physical)therapy)) ! ! plan)of)treatment!!
TRANSCRIPT
Physical Therapy Plan of Treatment
Patient’s Last Name First Name
MI HICN XXX-‐XX-‐
Provider Name LifeCare of Florida
Provider No
Onset Date SOC Date
Primary Diagnosis Treatment Diagnosis
Reason for Referral/Symptom Onset The Interview was completed with Patient Spouse Caregiver Other: ________________________________________________ Patient is _______ Years of Age and resides in a Home Apt/Condo ILF ALF Other: ________________________________________ Home is Accessible Not Accessible Has Steps _____ To Enter or _____ In Home Concerns: ________________________________________________________________________________________________________________ The patient lives: Alone or With: Spouse Family FT Caregiver PT Caregiver ____________________________________ hours/days)
Who Currently Helps with ADLs? _____________________________________________________________________________________________ Summary: Patient presents with a history of _____ Low _____ Moderate _____ High Complexity
Body Systems Affected: Skeletal Muscular Nervous Cardio-‐Respiratory Lymphatic Other: _____________________
Body Regions Affected: Multiple Sites/Systemic Dominant Side: R L
Right Shoulder Elbow/Upper Arm Wrist/Forearm Fingers & Hand Hip Knee/Lower Leg Ankle/Foot
Left Shoulder Elbow/Upper Arm Wrist/Forearm Fingers & Hand Hip Knee/Lower Leg Ankle/Foot
Other: Head Cervical Spine Thoracic Spine Lumbar Spine Ribs
Co-‐Morbid Medical Complexities: (Conditions which directly and significantly impact the patient’s level of function) No Yes (Describe):
Additional Medical Hx / Medications
Injury & Fall History Patient has had (Check all that apply): Loss of Balance/Near Falls Falls w/out Injury Falls with Injury
If Injury Occurred: When (date): ____________________ Location: ______________________________ Activity: ________________________
Injury: __________________________________________________ Is this the condition for which skilled therapy was ordered? No Yes
Rehab History Patient Has Not or HAS received PT OT SLP in the past 12 months, Therapy was for current or previous condition.
Describe: _________________________________________________________________________________________________________________
Prior Level of Function Independent OR Required Assistance (Describe)

Patient’s Last Name First Name
MI HICN
Current Impairments & Functional Impact
Body Functions Affected: Sensory Functions & Pain Neuro-‐Musculoskeletal & Movement CardioRespiratory/Hematological Mental Voice & Speech Skin & Related Digestive/Metabolic/Endocrine Genitourinary & Reproductive
Resulting Activity & Participation Restrictions: Balance Transfers Mobility in Home Mobility in Community Self Care/ADLs IADLS Learning & Applying Knowledge
General Tasks & Demands Communication Interpersonal Relationships Community/Social/Civic Life Being Alone
Additional Complexities: Advanced Age Time Since Onset Significant Co-‐Morbidities Fall Risk Lack/Limited Caregiver Safety in Home
Poor Vision HOH Cognitive Status Speech/Communication Bowel/Bladder Motivation Other: ______________
Primary G-‐Code The Primary G-‐Code Category for which therapy will be rendered is: _______________________________________________________________
Patient’s Admit Impairment Level is: __________________________________ with a Goal of ____________________________________________
Physical Therapy Plan of Care Recommended # of Skilled Therapy Visits: ___________ Visits Frequency: _________/week Duration: ____________ hours/visit Certification Period: Start: ________________________ End: ___________________ (Max 90 Days) Rehabilitation Potential: Excellent Good Fair Poor Long Term Goals: (Number Each Goal)
Skilled Intervention to Include: 97110 Therapeutic Exercise 97140 Manual Therapy
97112 Neuromuscular Re-‐Education 97542 Wheelchair Training
97116 Gait Training 97761 Prosthetic Training
Other: _______________________________________________________________________________________________________________ Precautions/Contraindications: ___________________________________________________________________________________________
Additional Recommendations: OT Evaluation SLP Evaluation Adaptive Equipment: ___________________________________________________________________ Medical Follow-‐Up For: _________________________________________________________________________________________________ Other: _______________________________________________________________________________________________________________
Professionals Establishing This Plan of Care Therapist Name & Credentials (Please Print) ______________________________________________________
Therapist Signature X_____________________________________________________
Date ____________________
As of the date of this evaluation, I certify the pertinent medical history and the need for skilled services that have been completed in consultation with the evaluating therapist under this plan.
Physician Name (Please Print) ___________________________________________________
Physician Signature X____________________________________________________
Date ____________________
Physical Therapy Plan of Treatment – Page 2

Patient’s Last Name First Name
MI HICN XXX-‐XX-‐
Diagnosis: SOC Date
Evaluating Therapist:
Musculoskeletal Evaluation Assessment Of: Cervical Spine Lumbar Spine Upper Body Lower Body Other: ______________________________________
Symptoms/Complaints:
Pain ___ None or: ____/10 Average ____/10 Worst ____/10 Best
ROM: WFL or Impaired
MMT: WFL or Impaired
Muscle Tone: WFL or Impaired: Flaccid Hypotonic Hypertonic
Sensation: WFL or Impaired for: Light Touch Pain Proprioception
Edema: Not Present or Present
Palpation: N/A or Describe Below
Special Tests: None or Describe Below
Endurance: Good Fair Poor (Describe Activity Tolerance in Minutes)
Posture: No Abnormality or Impaired
Deviations: Kyphosis Lordosis Scoliosis Forward Head Protracted Shoulders Leg Length Discrepancy
Other Pertinent Findings:
Physical Therapy Evaluation

Patient’s Last Name First Name
MI HICN XXX-‐XX-‐
Gait: WFL for Pattern & Distance or Impaired (Check All That Apply) Weight Bearing Status: FWB WBAT TTWB PWB _________________________________________________________________
Deviations: ê Heel-‐Toe Gait ê BOS LOB Antalgic Shuffling Festinating Waddling Slow Cadence Fast Cadence
Assistive Devices: Standard Cane Quad Cane 3WW 4WW Crutches WheelChair Other:
Ambulatory Capacity: ________ Feet Independent or With Assistance: ___________________________________________________
Additional Safety Issues: N/A or Furniture Walks Narrow Corners/Places Unsafe/Inappropriate AD Other: ___________________
Functional Tests & Measurements Tinetti Gait/Balance BERG Functional Reach Test NDI Oswestry OPTIMAL
Other: _______________________________________________________________________________________________________________
Test Results: Score: ____________ Interpretation: ________________________________________________________________________
Functional Performance Evaluation
I = (7) Indep/Safe SBA = (6)1-‐19% Assist CGA= (5)20-‐39% Min=(4)40-‐59% Mod=(3)60-‐79% Max=(2)80-‐99% Total= (1)100%
Mobility: I SBA CGA Min Mod Max Total Comments
Bed Mobility _____ _____ _____ _____ _____ _____ _____
Rolling _____ _____ _____ _____ _____ _____ _____
Scooting _____ _____ _____ _____ _____ _____ _____
Supine to Sit _____ _____ _____ _____ _____ _____ _____
Stair Climb Check if Stairs in Home _____ _____ _____ _____ _____ _____ _____
Balance: I SBA CGA Min Mod Max Total Comments Static Seated Balance _____ _____ _____ _____ _____ _____ _____ Dynamic Seated Balance _____ _____ _____ _____ _____ _____ _____ Static Stand _____ _____ _____ _____ _____ _____ _____ Dynamic Stand _____ _____ _____ _____ _____ _____ _____ Challenged _____ _____ _____ _____ _____ _____ _____
Transfers: I SBA CGA Min Mod Max Total Comments
Sit to Stand _____ _____ _____ _____ _____ _____ _____
Bed to Chair _____ _____ _____ _____ _____ _____ _____
Toilet _____ _____ _____ _____ _____ _____ _____
Shower _____ _____ _____ _____ _____ _____ _____
Car _____ _____ _____ _____ _____ _____ _____
Sphere of Mobility: I SBA CGA Min Mod Max Total Comments
Level 1: In room and home _____ _____ _____ _____ _____ _____ _____
Level 2: Just outside of home (e.g., mailbox) _____ _____ _____ _____ _____ _____ _____
Level 3: Within immediate neighborhood _____ _____ _____ _____ _____ _____ _____
Level 4: Community Distances _____ _____ _____ _____ _____ _____ _____
Level 5: All travel/excursions _____ _____ _____ _____ _____ _____ _____
Other I SBA CGA Min Mod Max Total Comments
_________________________________ _____ _____ _____ _____ _____ _____ _____
_________________________________ _____ _____ _____ _____ _____ _____ _____
_________________________________ _____ _____ _____ _____ _____ _____ _____
_________________________________ _____ _____ _____ _____ _____ _____ _____
_________________________________ _____ _____ _____ _____ _____ _____ _____

LifeCare Therapy Services
Rehabi l i ta t ion Therapy and Disease Management
Tinetti Gait & Balance Assessment
Patient’s Last Name First Name
MI HICN
BALANCE – Patient is seated in hard, armless chair.
Eval PR PR PR D/C
Sitting Balance 0= Leans or Slides in Chair 1= Steady/Safe
Rises from Chair 0=Unable to do without help 1=Able, uses arms to help 2=Able without use of arms
Attempts to Rise 0=Unable to do without help 1=Able, requires >1 attempt 2=Able to rise, first attempt
Immediate Stand Balance
0=Unsteady (staggers, moves feet, trunk sway) 1=Steady with walker/support 2=Steady without walker or other support
Standing Balance 0=Unsteady (staggers, moves feet, trunk sway) 1=Steady but wide stance (medial heels>4” apart or other support 2=Narrow stance without support
Nudged 0=Begins to fall =Staggers, grabs/catches self 2=Steady
Eyes Closed 0=Unsteady 1=Steady
Turn 360 Degrees 0=Discontinuous Steps 1=Continuous Steps
0=Unsteady (grabs/staggers) 1=Steady
Sitting Down 0=Unsafe (misjudges distance, falls into chair) 1=Uses arms or not a smooth motion 2=Safe, smooth motion
Balance Score (/16)
GAIT: Patient stands with examiner and walks first at “usual” pace and then back at a rapid but safe pace using usual walking aids.
Initiation of Gait 0=Any hesitancy or multiple attempts 1=No hesitancy
Step Length & Height
Right Swing Foot 0=Does not pass left 1=Pass left stance foot
0=Left foot does not clear floor 1=Left foot completely clears floor
Left Swing Foot 0=Does not pass right 1=Pass right stance foot
0=Left foot does not clear floor 1=Left foot completely clears floor
Step Symmetry 0=Right and left step length not equal 1=Right and left step length appear equal
Step Continuity 0=Stopping or discontinuity between steps 1=Steps appear continuous
Path 0=Marked deviation 1=Mild/moderate deviation or uses walking aid 2=Straight without walking aid
Trunk 0=Marked sway or uses walking aid 1=No sway, but knees flexed or spreads arm 2=No sway, no flexion/use of arms and no walking aid
Walking Time 0=Heels apart 1=Heels almost touch
Gait Score (/12)
Gait + Balance Score (/28)
≤ 18 = High Fall Risk 19-‐24 = Moderate Fall Risk ≥ 25 = Low Fall Risk

Physical Therapy Encounter Note
Patient’s Last Name First Name
MI HICN
Provider Name LifeCare of Florida
Provider No
SOC Date Date of Visit
Primary Diagnosis(es) Treatment Diagnosis(es)
Therapist Assistant (If Applicable)
Services Rendered: Intake Initial Evaluation Skilled Therapy Other: ______________________________________________________________
Billing & Coding Summary
Intake Information __________ Time _________ Units
97161 PT Eval LOW
__________ Time _________ Units
97162 PT Eval MODERATE
__________ Time _________ Units
97163 PT Eval HIGH
__________ Time _________ Units
97110 Therapeutic Exercise
__________ Time _________ Units
97112 Neuromuscular Re-‐Education
__________ Time _________ Units
97116 Gait Training __________ Time _________ Units
97140 Manual Therapy
__________ Time _________ Units
Other: __________________________
__________ Time _________ Units
Total Time (Minutes)
Total Units
Therapist Name & Credentials (Please Print) ___________________________________________________
Therapist Signature X____________________________________________________
Date ____________________
Evaluation Coding Guidelines Low Complexity Moderate Complexity High Complexity
Personal factors and/or comorbidities that impact POC None 1-‐2 Factors 3 or More Factors
Objective tests and measurements performed 1-‐2 3 or More 4 or More
Clinical presentation Stable / Uncomplicated Evolving Unstable / Unpredictable
Typical face-‐to-‐face time with patient/family 20 Minutes 30 Minutes 45 Minutes
Patient’s Last Name First Name
MI HICN XXX-‐XX-‐
Therapist: Onset Date SOC Date
Primary Diagnosis:
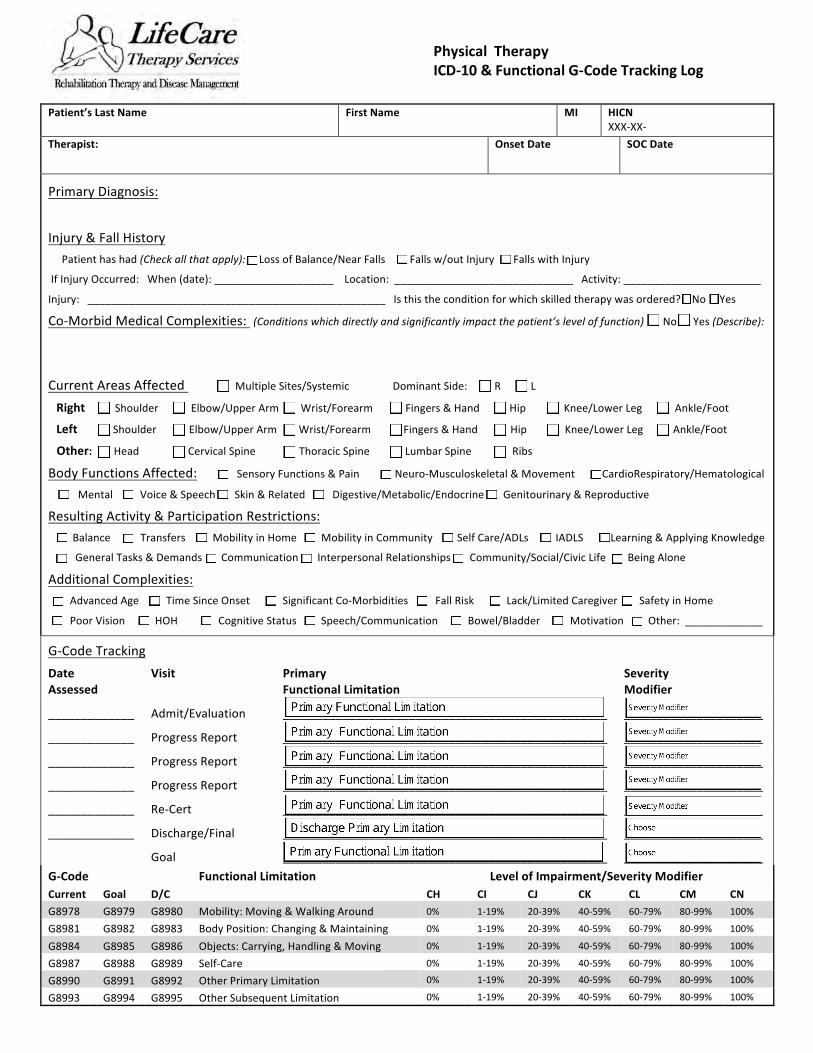
Injury & Fall History Patient has had (Check all that apply): Loss of Balance/Near Falls Falls w/out Injury Falls with Injury
If Injury Occurred: When (date): ____________________ Location: ______________________________ Activity: _______________________
Injury: __________________________________________________ Is this the condition for which skilled therapy was ordered? No Yes
Co-‐Morbid Medical Complexities: (Conditions which directly and significantly impact the patient’s level of function) No Yes (Describe):
Current Areas Affected Multiple Sites/Systemic Dominant Side: R L
Right Shoulder Elbow/Upper Arm Wrist/Forearm Fingers & Hand Hip Knee/Lower Leg Ankle/Foot
Left Shoulder Elbow/Upper Arm Wrist/Forearm Fingers & Hand Hip Knee/Lower Leg Ankle/Foot
Other: Head Cervical Spine Thoracic Spine Lumbar Spine Ribs
Body Functions Affected: Sensory Functions & Pain Neuro-‐Musculoskeletal & Movement CardioRespiratory/Hematological Mental Voice & Speech Skin & Related Digestive/Metabolic/Endocrine Genitourinary & Reproductive
Resulting Activity & Participation Restrictions: Balance Transfers Mobility in Home Mobility in Community Self Care/ADLs IADLS Learning & Applying Knowledge
General Tasks & Demands Communication Interpersonal Relationships Community/Social/Civic Life Being Alone
Additional Complexities: Advanced Age Time Since Onset Significant Co-‐Morbidities Fall Risk Lack/Limited Caregiver Safety in Home
Poor Vision HOH Cognitive Status Speech/Communication Bowel/Bladder Motivation Other: _____________
G-‐Code Tracking Date Assessed
Visit Primary Functional Limitation
Severity Modifier
_____________ Admit/Evaluation _________________________________________________ _____________________
_____________ Progress Report _________________________________________________ _____________________
_____________ Progress Report _________________________________________________ _____________________
_____________ Progress Report _________________________________________________ _____________________
_____________ Re-‐Cert _________________________________________________ _____________________
_____________ Discharge/Final _________________________________________________ _____________________
Goal _________________________________________________ _____________________ G-‐Code Functional Limitation Level of Impairment/Severity Modifier Current Goal D/C CH CI CJ CK CL CM CN G8978 G8979 G8980 Mobility: Moving & Walking Around 0% 1-‐19% 20-‐39% 40-‐59% 60-‐79% 80-‐99% 100%
G8981 G8982 G8983 Body Position: Changing & Maintaining 0% 1-‐19% 20-‐39% 40-‐59% 60-‐79% 80-‐99% 100%
G8984 G8985 G8986 Objects: Carrying, Handling & Moving 0% 1-‐19% 20-‐39% 40-‐59% 60-‐79% 80-‐99% 100%
G8987 G8988 G8989 Self-‐Care 0% 1-‐19% 20-‐39% 40-‐59% 60-‐79% 80-‐99% 100%
G8990 G8991 G8992 Other Primary Limitation 0% 1-‐19% 20-‐39% 40-‐59% 60-‐79% 80-‐99% 100%
G8993 G8994 G8995 Other Subsequent Limitation 0% 1-‐19% 20-‐39% 40-‐59% 60-‐79% 80-‐99% 100%
Physical Therapy ICD-‐10 & Functional G-‐Code Tracking Log

LifeCare Therapy Services
Rehabi l i ta t ion Therapy and Disease Management
Revised: 01/2014
Patient’s Last Name First Name
MI HICN
Provider Name LifeCare of Florida
Provider No
Onset Date SOC Date (Evaluation Date)
Certification Period
From:
To:
# of Visits to Date Report Period
From:
To: Primary Diagnosis(es) Treatment Diagnosis(es)
Therapist Assistant (If Applicable)
Summary of Progress LTG Admission Status Current Status LTG #1
Met
LTG #2
Met
LTG #3
Met
LTG #4
Met
LTG #5
Met
G-‐CODE
Conclusions Patient has made appropriate progress toward rehabilitation goals and continued functional improvement is expected
Patient has experienced a delay/setback (Explain)
Other: _______________________________________________________________________________________________________________________________
Additional Comments
Recommendations Continue POC or Modify POC (Describe): ________________________________________________________________________________________________
Other: ______________________________________________________________________________________________________________________________
Professional Establishing This Progress Report _________________________________________________________ Therapist Name & Credentials (Please Print)
_______________________________________________________ ___________________ Therapist Signature Date
Physical Therapy Supervisory Progress Report
Physical Therapy Encounter Note
Re-‐Evaluation Coding Requirements:
• An examination including a review of history and use of standardized tests and measures is required AND; • Revised plan of care using a standardized patient assessment instrument and/or measurement assessment of functional outcome. • Typical time, 20 minutes face-‐to-‐face.
Patient’s Last Name First Name
MI HICN
Provider Name LifeCare of Florida
Provider No
SOC Date Date of Visit
Primary Diagnosis(es) Treatment Diagnosis(es)
Therapist Assistant (If Applicable)
Services Rendered: Re-‐Evaluation Progress/Sup Visit Discharge Assessment Skilled Therapy Other: _______________________________
Billing & Coding Summary
Intake Information
__________ Time _________ Units
97164 PT Re-‐Evaluation (20 Min)
__________ Time _________ Units
97110 Therapeutic Exercise
__________ Time _________ Units
97112 Neuromuscular Re-‐Education
__________ Time _________ Units
97116 Gait Training
__________ Time _________ Units
97140 Manual Therapy
__________ Time _________ Units
Other: __________________________
__________ Time _________ Units
Total Time (Minutes)
Total Units
Therapist Name & Credentials (Please Print) ___________________________________________________
Therapist Signature X____________________________________________________
Date ____________________

LifeCare Therapy Services
Rehabi l i ta t ion Therapy and Disease Management
Revised: 01/2014
Patient’s Last Name First Name
MI HICN
Provider Name LifeCare of Florida
Provider No
Onset Date SOC Date (Evaluation Date)
Certification Period
From:
To:
# of Visits to Date Report Period
From:
To: Primary Diagnosis(es) Treatment Diagnosis(es)
Therapist Assistant (If Applicable)
Summary of Progress LTG Admission Status Current Status LTG #1
Met
LTG #2
Met
LTG #3
Met
LTG #4
Met
LTG #5
Met
G-‐CODE
Conclusions Patient has made appropriate progress toward rehabilitation goals and continued functional improvement is expected
Patient has experienced a delay/setback (Explain)
Other: _______________________________________________________________________________________________________________________________
Additional Comments
Recommendations Continue POC or Modify POC (Describe): ________________________________________________________________________________________________
Other: ______________________________________________________________________________________________________________________________
Professional Establishing This Progress Report _________________________________________________________ Therapist Name & Credentials (Please Print)
_______________________________________________________ ___________________ Therapist Signature Date
Physical Therapy Supervisory Progress Report

Physical Therapy Encounter Note
Re-‐Evaluation Coding Requirements:
• An examination including a review of history and use of standardized tests and measures is required AND; • Revised plan of care using a standardized patient assessment instrument and/or measurement assessment of functional outcome. • Typical time, 20 minutes face-‐to-‐face.
Patient’s Last Name First Name
MI HICN
Provider Name LifeCare of Florida
Provider No
SOC Date Date of Visit
Primary Diagnosis(es) Treatment Diagnosis(es)
Therapist Assistant (If Applicable)
Services Rendered: Re-‐Evaluation Progress/Sup Visit Discharge Assessment Skilled Therapy Other: _______________________________
Billing & Coding Summary
Intake Information
__________ Time _________ Units
97164 PT Re-‐Evaluation (20 Min)
__________ Time _________ Units
97110 Therapeutic Exercise
__________ Time _________ Units
97112 Neuromuscular Re-‐Education
__________ Time _________ Units
97116 Gait Training
__________ Time _________ Units
97140 Manual Therapy
__________ Time _________ Units
Other: __________________________
__________ Time _________ Units
Total Time (Minutes)
Total Units
Therapist Name & Credentials (Please Print) ___________________________________________________
Therapist Signature X____________________________________________________
Date ____________________

LifeCare Therapy Services
Rehabi l i ta t ion Therapy and Disease Management
Revised: 01/2014
Patient’s Last Name First Name
MI HICN
Provider Name LifeCare of Florida
Provider No
Onset Date SOC Date (Evaluation Date)
Certification Period
From:
To:
# of Visits to Date Report Period
From:
To: Primary Diagnosis(es) Treatment Diagnosis(es)
Therapist Assistant (If Applicable)
Summary of Progress LTG Admission Status Current Status LTG #1
Met
LTG #2
Met
LTG #3
Met
LTG #4
Met
LTG #5
Met
G-‐CODE
Conclusions Patient has made appropriate progress toward rehabilitation goals and continued functional improvement is expected
Patient has experienced a delay/setback (Explain)
Other: _______________________________________________________________________________________________________________________________
Additional Comments
Recommendations Continue POC or Modify POC (Describe): ________________________________________________________________________________________________
Other: ______________________________________________________________________________________________________________________________
Professional Establishing This Progress Report _________________________________________________________ Therapist Name & Credentials (Please Print)
_______________________________________________________ ___________________ Therapist Signature Date
Physical Therapy Supervisory Progress Report

Physical Therapy Encounter Note
Re-‐Evaluation Coding Requirements:
• An examination including a review of history and use of standardized tests and measures is required AND; • Revised plan of care using a standardized patient assessment instrument and/or measurement assessment of functional outcome. • Typical time, 20 minutes face-‐to-‐face.
Patient’s Last Name First Name
MI HICN
Provider Name LifeCare of Florida
Provider No
SOC Date Date of Visit
Primary Diagnosis(es) Treatment Diagnosis(es)
Therapist Assistant (If Applicable)
Services Rendered: Re-‐Evaluation Progress/Sup Visit Discharge Assessment Skilled Therapy Other: _______________________________
Billing & Coding Summary
Intake Information
__________ Time _________ Units
97164 PT Re-‐Evaluation (20 Min)
__________ Time _________ Units
97110 Therapeutic Exercise
__________ Time _________ Units
97112 Neuromuscular Re-‐Education
__________ Time _________ Units
97116 Gait Training
__________ Time _________ Units
97140 Manual Therapy
__________ Time _________ Units
Other: __________________________
__________ Time _________ Units
Total Time (Minutes)
Total Units
Therapist Name & Credentials (Please Print) ___________________________________________________
Therapist Signature X____________________________________________________
Date ____________________

LifeCare Therapy Services
Rehabi l i ta t ion Therapy and Disease Management
PT Re-‐Certification of the Plan of Care Revised: 01/2013
Physical Therapy Re-‐Certification of the Plan of Care
Patient’s Last Name First Name
MI HICN
XXX-‐XX-‐ Provider Name LifeCare of Florida
Provider No Onset Date SOC Date Date of ReCert Request
Primary Diagnosis(es) Treatment Diagnosis(es)
This Re-‐Certification is To: Complete the Initial Plan of Care (No additional therapy visits are needed; only an extension of the Certification Period). Extend the initial plan of care to provide continued skilled therapy to reach the goals (additional therapy visits are requested). Revise the POC due to a substantial change in the patient’s condition (additional therapy visits are requested).
Rationale:
G-‐Code with Severity Modifier (Impairment) Current Status Projected/Goal Status
Code/Descriptor Impairment Level Code/Descriptor Impairment Level
Physical Therapy Updated Plan of Care # of Visits to Complete Skilled POC __________Visits Frequency: _________/week Duration: __________ hours/visit Re-‐Certification Period: Start: __________________ End: _____________________ (Max 30 days)
Rehabilitation Potential: Excellent Good Fair Guarded Poor Long Term Goals: No Change OR Revised/Updated Goals Below: (Number each goal) Skilled Intervention to Include 97110 Therapeutic Exercise 97112 Neuromuscular Re-‐Education 97116 Gait Training 97140 Manual Therapy 97542 Wheelchair Training 97761 Prosthetic Training Other: _____________________________________________________________________________________________________________________________
Additional Recommendations Medical Follow-‐Up For: ________________________________________________________________________________________________________________ Other: ______________________________________________________________________________________________________________________________
Professionals Establishing This Plan of Care Therapist Name & Credentials (Please Print) ______________________________________________________
Therapist Signature X_____________________________________________________
Date ____________________
I certify the need for skilled therapy services as described in this Updated Plan of Care that has that have been completed in consultation with the evaluating therapist under this plan.
Physician Name (Please Print) ___________________________________________________
Physician Signature X____________________________________________________
Date ____________________

LifeCare Therapy Services
Rehabi l i ta t ion Therapy and Disease Management
Revised: 01/2014
Patient’s Last Name First Name
MI HICN
Provider Name LifeCare of Florida
Provider No
Onset Date SOC Date (Evaluation Date)
Certification Period
From:
To:
# of Visits to Date Date of Discharge
Primary Diagnosis(es) Treatment Diagnosis(es)
Therapist Assistant (If Applicable)
Discharge/Outcome LTG Admission Status Discharge Status LTG #1
Met
LTG #2
Met
LTG #3
Met
LTG #4
Met
LTG #5
Met
G-‐CODE
Reason For Discharge Goal Attainment Maximum Benefit Failure to Respond/Plateau
Patient Request (Explain): _______________________________________________________________________________________________________________
Patient No Longer Able to Participate: ____________________________________________________________________________________________________
Additional Comments
Recommendations Home Program As Assigned Medical Follow-‐Up Other: _______________________________________________________________________________
Professional Establishing This Progress Report _________________________________________________________ Therapist Name & Credentials (Please Print)
_______________________________________________________ ___________________ Therapist Signature Date
Physical Therapy Discharge Summary
Physical Therapy Encounter Note
Re-‐Evaluation Coding Requirements:
• An examination including a review of history and use of standardized tests and measures is required AND; • Revised plan of care using a standardized patient assessment instrument and/or measurement assessment of functional outcome. • Typical time, 20 minutes face-‐to-‐face.
Patient’s Last Name First Name
MI HICN
Provider Name LifeCare of Florida
Provider No
SOC Date Date of Visit
Primary Diagnosis(es) Treatment Diagnosis(es)
Therapist Assistant (If Applicable)
Services Rendered: Re-‐Evaluation Progress/Sup Visit Discharge Assessment Skilled Therapy Other: _______________________________
Billing & Coding Summary
Intake Information
__________ Time _________ Units
97164 PT Re-‐Evaluation (20 Min)
__________ Time _________ Units
97110 Therapeutic Exercise
__________ Time _________ Units
97112 Neuromuscular Re-‐Education
__________ Time _________ Units
97116 Gait Training
__________ Time _________ Units
97140 Manual Therapy
__________ Time _________ Units
Other: __________________________
__________ Time _________ Units
Total Time (Minutes)
Total Units
Therapist Name & Credentials (Please Print) ___________________________________________________
Therapist Signature X____________________________________________________
Date ____________________