physiology, lecture 6, gas exchange (lecture notes)
DESCRIPTION
Physiology, Lecture 6, Gas Exchange (Lecture Notes)TRANSCRIPT

1

الرحيم الرحمن الله بسمDate : 11-10-2010Physio 6th lec
Subject: gas exchange
The doctor mentioned that his office hours are : Mon , wed : 12-2 pmSun , tue , thu : 10-11 pm
***the doctor will be busy(in a meeting) during the last two working days before the exam so manage to step by his office any time earlier.
In the last lecture we started our talk about respiratory system we said the respiratory system is divided into two major parts:
*Air conducting channels ; their function just to conduct the air from outside inside
*Alveolar spaces (or the lungs spaces) and the major function of it to transport or to exchange the Oxygen and carbon dioxide through the respiratory membrane.
Now, what's the respiratory membrane ?, what does it contain? It contains epithelial cells of the alveoli ,type one alveolar cells , and endothelial cells of capillaries in and a space separate them . this is the alveolar membrane ,this is the membrane through which the oxygen should cross from the alveoli to the RBC's .and it's the same membrane carbon dioxide should
cross from blood to alveoli.
And we've also discussed the types of muscles we have for respiration ; the major inspiratory ,major expiratory ,accessory inspiratory muscles which help us to do the forceful breathing ,and also we discussed the mechanism of the
respiratory cycle.
What's the respiratory cycle? It is the inspiration and expiration . and we said that the normal quiet breathing is just inspiration nothing more .just you inspire and after that you do the
relaxation of the muscles and that will cause the normal quiet expiration. But, if you need more oxygen if you need more breathing you have to use extra muscles and then you start to do the inspiration ,expiration forcefully.
In both cases, when you breathe normally you take small amount of air the amount that we need for our basic physiological functions ,but if we need sth more ,more exercises ,stress then you have to use active inspiration ,active
expiration… "In normal quiet breathing the only active part is the inspiration ,the expiration
is passive " because it's just a relaxation of the muscles."
2

In this lecture we will continue discussing that mechanism by talking about a phenomenon called " the elasticity behavior of the lungs" ;how the lungs behave in their elasticity.
what is the elasticity? the elasticity is the stretchability in the lungs.
how easy you can fill your lungs with air? under normal conditions we mentioned its very easy. we only consume 3% of the total energy per day .but if we have a sickness or a disease in the respiratory system this 3% it might exceed 20% up to 30% to 40% and it can reach 90%.
So, in physiological condition the breathing is very easy and simple ,why is that ?
There are many factors ;one of them and the simplest one "we discussed different pressures in the respiratory system " we said that there is a pressure
inside the alveoli and it's called "alveolar pressure." *We said that this pressure could be (0)and zero means it's equal to
atmospheric pressure. *or it could be minus during inspiration ; under normal quiet breathing it
reaches up to (-1)mm hg not that much ,in other words if I want to take inspiration and I'm normal I need only (-1)mm hg difference to get that amount of air "I don’t need more because I don’t want to spend energy for breathing
and this is a gift from god."
*and during normal expiration it could be (+1).
We said that alveolar pressure could be (-1, 0 , +1) if we go to the pleural space which is the coated compartment around the lungs and it has minus pressure and it equals to (-4) during quiet normal breathing , while you are doing the inspiration this (-4) becomes (-8) .so the intrapleural pressure normally it's minus ,it's more minus during inspiration, and it's more and more minus during
forceful inspiration.
Now, the TRANSMURAL pressure is the difference between the alveolar pressure and the pleural pressure , the transmural pressure is also minus ,because when we are talking about pleural pressure which is minus (-3 , -4 , -5 …) and alveolar pressure either (-1, 0 , +1 ) so the difference will be
always minus …..why ?
firstly the normal quiet breathing pleural pressure (-4)alveolar pressure (0)
so the transmural pressure (0- -4= +4 )
during inspiration pleural pressure (-5or -6)alveolar pressure (-1)
3
so the transmural pressure (-1- -6= +5 ) during expiration pleural pressure (-3,-2)alveolar pressure (+1)so the transmural pressure (+1- -2= +3 )
So what's the +3,+4,+5 ? this the pressure of the air inside the lungs , the more the pressure the more air inside your lungs.
Now lets go back to the behavior of the lung "the elasticity; how easy you can fill your lungs with air " ,and you know the rubber structure it's a stretchable structure you can stretch it and when you leave it ,it goes back to normal
position. Now, lets remember our childhood when you have a balloon to blow ,when you bought these balloons and you start to blow them it wasn't easy to blow them Because you were very small , you always asked your older brother or sister to do the first blow .and after a while if you take that balloon it becomes easier to
blow air inside it because the stretchability is now much easier.
Now, the balloon when it is blown for the first time it was very strong but after being stretched and inflated the strength of the rubber is less so, what we say here; when its easy to blow the balloon its compliance is much higher but when its rigid to blow it ,its compliance is very low.
So, what's the definition of the compliance ? the compliance definition is how much air you can inflate any compartment compared to how much difference in pressure you created after blowing . in other words when we applied that to lungs , how many mm hg difference in the pressure I need to fill my lungs with 100 ml of air if I need 1mm hg this means the compliance is equal to1mm hg to fill with 100 ml of air , and if I want to fill my lungs with 200 ml and I created only 1mm hg ,so its much easier now to fill my lung with 200 ml with the same amount of pressure so the compliance of the 2nd situation is higher than the
compliance of the 1st one .
Now, lets talk in numbers.…… What is the normal compliance of our lungs around 200mm per mm hg ; so each 1mm hg able to fill your lungs with 200ml of air, if I created 2mm hg I’ll fill 400 ml of air . because I double the amount of air by inflating my lungs with
extra1mm hg ,so this is the compliance of normal lung.
And because our lungs are located in the chest if I want to fill my lungs while they are in my chest it's not easy because I have to fill them and at the same time I have to stretch the thorax (the ribs ,the skin, and the muscles ) so if you calculate the compliance of the lungs under normal condition , in human being it will be 110 ml per 1mm hg because I have to spend another effort to inflate the chest layers not only the lungs . so if you take the lungs out side you can fill them with 200ml per 1mm hg but if you put them back to the chest with that amount of pressure you only fill it with 110 ml air.
4

Now lets discuss why its easy and simple to fill your lungs with air ? Lets think what is going on when we inflate our lungs , we have to push the air inside and to inflate the lungs tissue so, what are the forces opposing that air
filling? The first force is the elasticity of the tissue which is the rubber if you stretch it they don’t accept that they go back to the normal position, so the same is applied to the lungs ;lungs tissues if you fill them they will be filled but you have to push pressure , why? To over come the elasticity of the tissues .this elasticity of the tissue comes because there is a lot of elastin in the structure of the alveoli, and you know the elastin is fibers when you stretch it ,it goes back to
the normal position.
So, the elastin is one of the forces against the air filling this is number 1. the second force is the same elasticity behavior of the chest layers it's not easy to push the chest layers in both directions anterior and posterior; vertically without facing a force from the muscles ,the skin and the tissues so this is one of the forces against inflating the lungs , they opposing the inflation ; they try to
collapse the lungs.
There is another force "the third force" which is very important and its called the surface tension ,I think this phenomenon you should know from other subjects .it is a phenomenon of the water where ever the water interface the air , the molecules of water they have attraction between each other this attraction called the surface tension now lets go deep inside the lung and we
have about 3 million of (alveolus).
Always "under normal conditions" there is a water layer coated in the internal surface of the alveolus this water is very thin now you will learn another term in medicine, it's not acceptable to have dry alveolus and it's not acceptable to have wet alveolus too, what I mean by that, it is not accepted to have no water inside the alveolus and also it is not accepted to have full water inside the alveolus.We have to have only a film coated water in the internal surface.So it's wet " but not full of water or even partially of water", now these molecules of water because they are close to each other they have a power attraction ,attract to each other , this attractions it will force a power the direction of this force is the center of the alveoli so this force against the filling. in order to fill the alveolus I have to overcome this alveolus plus the elastin power which related to elastin and the tissue so the main two forces which opposing the inspiration or the air filling (the inflation)
are -: The elasticity.*
The surface tension.*
5

The most powerful one is the surface tension, surface tension will take 2/3 of the power so if I have to spend 3 mm hg to fill that alveolus with air 2mm hg will be overcoming the surface tension and 1 mm hg will overcome the elasticity so the surface tension because it's too powerful and normally it's equal about 13 – 15mm hg, imagine we are talking about different pressure to overcome this surface tension equal13 mm hg and few minutes ago what I was talking about (one mm hg ) is enough to do the respiratory movement so how we overcome that 13 mm hg , there is a special chemicals secreted by the type 2 alveoli, you remember.
When I discussed the alveolus structure I said there's type1 alveolus cells and type 2 alveolar cells.I said type 1 is the structure of epithelial cell or the layer of the alveolus, but type 2 they are special secreted cells they secrete chemical called surfactant.Now if you go back to water molecules attraction which is due to have two water molecules close to each other, surfactant is lipid and protein mixture , if it's secreted it will create a space between water molecule it will separate the water molecule from each other if you do so you'll decrease the attraction between molecule so the surfactants function is to decrease the surface tension and in our body this surfactant it will decrease the surface tension significantly .instead of 13 it goes to back to 2 or 1 , now if we have the surfactant if it is secreted in the alveoli and I told you before that the structure of the alveoli is opened to each other . They are small , medium, and large size now all of them they have that layer of water and all of the in their structure there is a secretion of surfactant and the cell type(2) will secrete the surfactant and it will be coated the whole surface area .Surface tension is inversely proportional to the diameter of the compartment , the smaller the compartment the more the surface tension inside that compartment .and its obvious, logical because when we are talking about small compartment we are talking about less distance between water molecules , and less distance leads to more attraction , and from here the surface tension in the small alveolus will be the highest ,the surface tension in the medium will be medium and in the high will be less.
Look back to the secretion of surfactant ,when its secreted in each alveolus and it will be spreaded all over the surface area in the biggest alveolus the amount of the surfactant compared to the surface area is less because if you have one drop of surfactant and you have to clean the whole surface area in the bigger will have lowest amount, whereas in the smaller alveolus you have the same drop of surfactant but small surface area so the concentration of surfactant in the small alveoli will be more than in the medium and in the medium will be more than in the biggest , why is that ? because surface tension in the smallest alveoli is the highest, so we need more surfactant to overcome that, in the biggest alveolus we need a little bit of surfactant, by the end of that effect (the effect of surfactant) the surface tension effect in the small or the medium or the large one will be almost the same because the decrease in the smallest will be high, the decrease in the medium will be
medium, and the decrease in the large one will be low.
6

The first sign we consider that the newborn is alive is the first cry "the first cry means the first inspiration", why it's so loud? Why the baby is crying? Because the first breath is the first very strong inspirations movement.Why is that?
Because the surface tension stills high and the alveoli all of them are collapsed and we need to inflate them.It needs a huge energy and this should come from that newborn and he is able to it. Most of us were able to do it, some of us were not able to do it we
call that
"newborn respiratory distress syndrome"
What's that?If the newborn is premature ,premature means that he came out without full maturation of physiology.One of the almost important factors in maturation of respiratory system is the secretion of surfactant and it starts from the seventh month of pregnancy, the type2 cells start to secret surfactant starting from the seventh month of pregnancy, if that newborn is premature that means the amount of surfactant secreted is not enough to decrease the surface tension, the major powerful force against the inflation against the inspiration. So when he comes out he wants to breathe, the inspiratory muscles will be contracted and the accessory muscle will be contracted " to the maximum " ,but these forceful movement does not equal to the surface tension which is very high ,why? Because the surfactant is not there ,if the baby is not able to breathe we call this "syndrome ", and if we wait he will die , nowadays we have a surfactant as a drug it's available in hospitals <in such case > this newborn will be given a surfactant directly to the respiratory system , after the drug is given to the newborn and within seconds in front of your eyes you'll see that the newborn who was not able to breathe who was almost dieing just relieve and start to breathe , because we added surfactant to the alveolar system and it spreaded all over the water layer and it decreases the surface tension ,but because giving that surfactant is temporary treatment and it doesn’t remain there we have to follow the treatment for few days by giving other drugs which increase the development of the type 2 alveolar
cells to secrete the surfactant .
pneumothorax:
Normally , air does not enter the pleural cavity , because there is no communication between the cavity and either the atmosphere or the
7

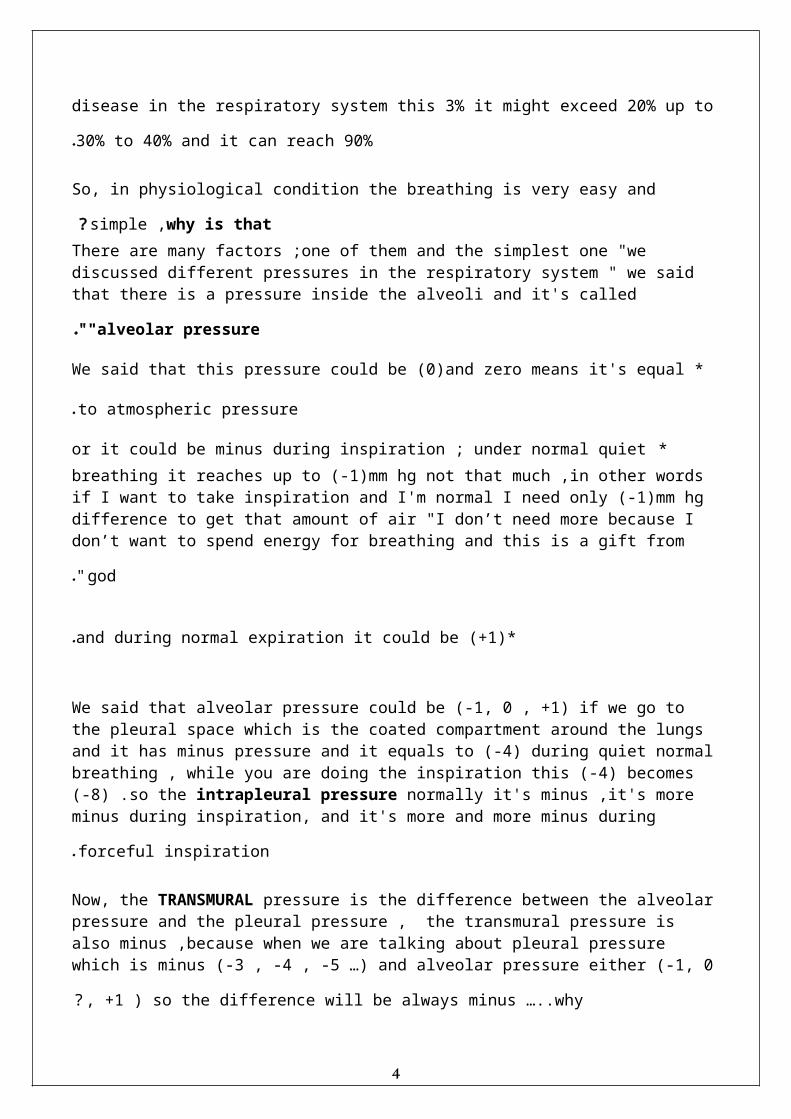
alveoli . however , there are some abnormalities could happen in our life where we can get some holes or penetration in the chest wall or in the lungs , this pneumonia ( this abnormalities )is called Pneumothorax ( " air in the chest " ) : is a collection of gas in the pleural cavity of the chest between the lungs and the chest wall , so a transmural pressure gradient no longer exists across the lung wall , with no force present to stretch the lung leading to collapsing of this lung.
this picture shows the anatomy of
the normal chest ,lungs and the pleural cavity.
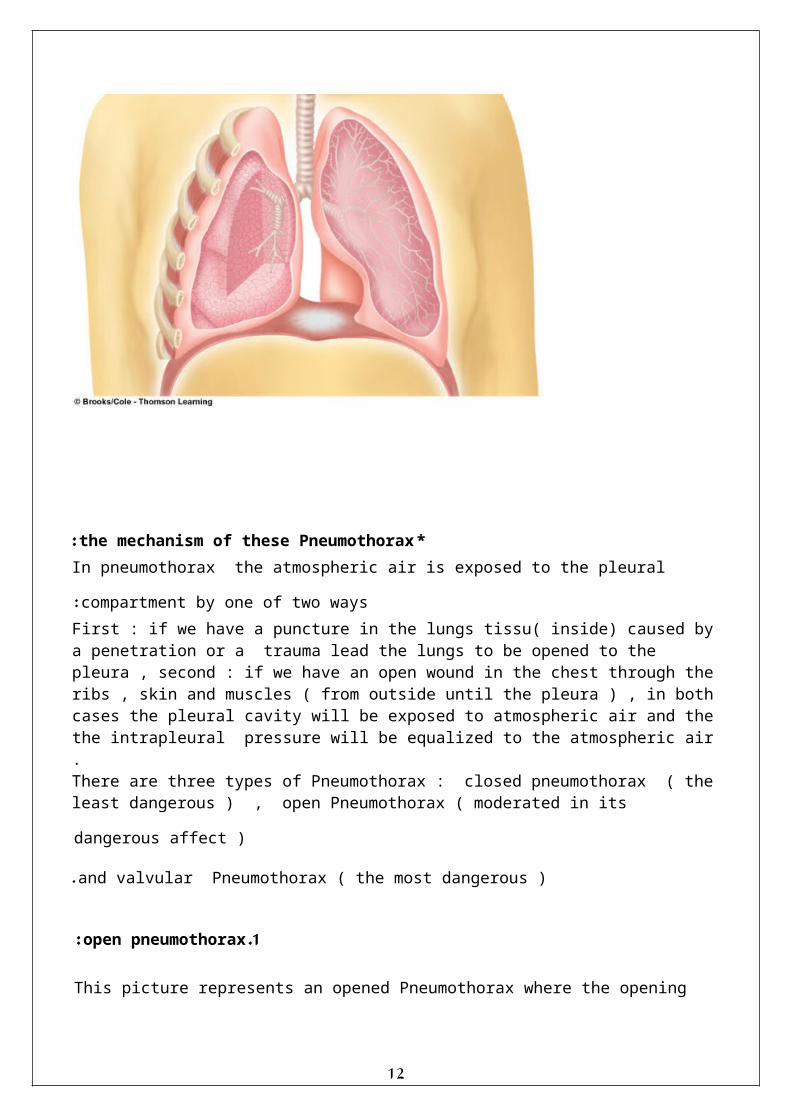
*the mechanism of these Pneumothorax: In pneumothorax the atmospheric air is exposed to the pleural compartment by
one of two ways : First : if we have a puncture in the lungs tissu( inside) caused by a penetration or a trauma lead the lungs to be opened to the pleura , second : if we have an open wound in the chest through the ribs , skin and muscles ( from outside until the pleura ) , in both cases the pleural cavity will be exposed to atmospheric air and the the intrapleural pressure will be equalized to the atmospheric air .There are three types of Pneumothorax : closed pneumothorax ( the least dangerous ) , open Pneumothorax ( moderated in its dangerous affect )
and valvular Pneumothorax ( the most dangerous ).
8

1 .open pneumothorax : This picture represents an opened Pneumothorax where the opening
could be from outside (from the chest layer) or e from the lung's side ( represented by an opening in the lung ) , in either way the pressure inside the pleura is zero pressure ( 760 mmhg ) . when the open pneumothorax is inside the lungs ( not the chest ) the air the comes from the air conducting channels during inspiration will pass the lungs to the pleural cavity and that will cause the lungs to collapse and by expiration it gets out from the same opening(wound )in the lungs to the air conducting channels . by this way , the air that gets inside is not exposed to the alveolar surface area and no gas exchange happens (so that will just fill the pleural cavity which has no function of gas exchanging and it will go back outside ) and the the defected side will be filled with air without taking the oxygen nor expelling co2
efficiently.
2 .closed pneumothorax:
Normally , and during inspiration and contraction of the respiratory muscles the chest layer raises up and because it has a closed pleura it will suck the lung with it and fill it with air . however , in this type of pneumothorax the opening (wound ) is in the chest and reaches to the lung and during inspiration of this defected area the air from atmosphere will go inside the pleura from this wound , so the chest will be full with pleural cavity with air and the lungs will be
collapsed inside.
9

More about the mechanism of this type : there's a small opening in the lungs ( caused by a wound coming from the chest layer ) , so when you start to inspire with that wound it will open a hole and the air will go out , after a while this small opening will be closed by it self because as a protection for our homeostasis there's a healing of that wound , so its not open during the second and third inspiration and so on , although is closes we still call it a pneumothorax because a portion of air gets out from the lungs to the pleura space and by pneumothorax we have some of air in it and after a while it'll be painful and the patient will feel a huge pain , if the amount of air got to the pleura is small nothing is done to the patient because this small amount will be absorbed by the tissues after few days and everything will go back to normal , if the amount of the air is huge and the patient can't tolerate the pain we can do a puncture through the chest to take out that collection of air in the pleura then
we close that puncture.
3.The valvular pneumothorax : it’s the most dangerous type, valvular means it has a valve ( a structure that opens in one direction but closes in the other direction ) , if there's an open pneumothorax inside the lung caused by a wound that has such structure ( a valve like structure ) in the defected area , inspiration will cause the air to come inside the lungs and it will raise that valve up and the air will go out in the pleural cavity , after inspiration comes the expiratory movement in which the chest and lungs are depressed and that will lead the valve structure to go down and closes the open pneumothorax , so during inspiration portion of air goes outside the lungs to the pleural cavity , during expiration the valve will close the opening and the air will remain in the
pleural cavity .
10

)remember that in open pneumothorax : during inspiration the air out to the pleura and during expiration the air inside the lung outside the chest and it will
leave the pleural cavity , ( here during inspiration some air is added to the pleura and during expiration its not lost ! so if we had 10 ml of air inside the pleura in the first respiratory cycle , in the second one we'll add another 10 ml to that 10 ml and so we'll have 20 ml and so on , by continuing breathing more and more air will be added in the pleura , and that's verrrry dangerous because this amount of air in the pleura depresses that lung again and again until its small ( collapsed ) and even when its small during inspiration another amount of air is added and that will cause the defected area in one side ( one lung ) to push the other normal side which will increase the pressure on the heart and on that other side , and if no treatment is done the patient with this condition will die , and its one of the emergency cases in medicine where there's no time to wait at all ! if the physician is sure that the diagnosis is a valvular pneumothorax he has to do a small medical procedure which is to create an open pneumothorax to that patient by making a small hole between ribs by a needle or any available sharp tool ( like a knife or so ! :P ) and so the collected air in the pleura will go out by the opening in the chest was created by the physician and the patient will survive and then he can be transported to the hospital to get the
surgical treatment for his condition.
Lungs volume & capacities :
We need oxygen all the time but not with the same amount that's why we need to have different volumes in our lungs , because suppose we have an x amount of oxygen in our lungs , sometimes we need double x or triple x and someties
we only need half of the x amount , these different volumes of the lungs are : 1.tidal volume TV : the amount of air taken by respiratory cycle under normal
breathing ( that's when you'r setting for example ) , if you don't concentrate on your breathing pattern the amount of air taking by normal inspiration and quiet
expiration is called the tidal volume. And this amount for a healthy adult 70 KG human male is 500 ml , in female it is
a little bit less than that.
2. Inspiratory reserve volume: sometimes we need more than the TV so there's another volume in the
structure of respiratory system called " Inspiratory reserve volume" )it's reserved for our benefit ( its there but you don't use it unless you need it
and it's 3000 ml ( 3 liters of air , six times the tidal volume ) . so under normal condition we need x amount of oxygen , if we need more we can increase that
amount by six times by using inspiratory reserve volume . So , inspiratory reserve volume : the maximum amount of air can be inspired after normal quiet inspiration ( after taking the tidal volume the major and accessory inspiratory muscles contract to the maximum to get extra amount of air from atmosphere to get inside the lungs ) , and so it’s the this maximum amount of air will be inspired by forceful inspiration after normal inspiration
(IRV) .
3. inspiratory capacity:
11
If we add the tidal volume to the Inspiratory reserve volume we get the result of what is called inspiratory capacity which is not equal to the volume of the lung but to two or more of the volumes of the lungs , its definition is (the IC ) : it's the maximum amount of air person can inspire by forceful inspiration after normal expiration ( the tidal volume is out , the inspiratory reserve volume is out and its always out there and we don't take it inside unless we need it , and then we do forceful inspiration and by doing so we take the TVand then the IRV
to get the IC ).
4. Expiratory reserve volume (ERV): :sometime when you're breathing normally ( while setting for example ) you
feel that you need to inspire deep in and to expire deep out , its not because you need more oxygen but because inside your lungs , after a while , the alveolar compartment will have more co2 , so what usually happens is you expire out the tidal volume and take a new tidal volume ( expelling co2 out and taking atmospheric air which is rich in oxygen ) , sometimes when the amount of co2 in th lung is increased which is not acceptable to happen we have the ability to do a forceful expiration after quiet expiration ( we expel out the tidal volume and after that our muscles are able to push your chest more and to get more air outside ) , this volume of air which can be expelled from the lungs by forceful expiration after normal expiration is called the Expiratory reserve volume . ( 1000 ml = 10 liters ) so by doing the ERV you clean your internal
respiratory system . The doctor said to explain this one more time : there's always one liter of air in your lung , you don't use it , its there , you take half a liter of air from outside and you return it back , sometimes when this one liter is somehow gets dirty with co2 or other particles , you are able to do the ERV out , when its out ( this
alveolar air is out ) you get back the atmospheric air which is good .
5. the residual volume: No matter how much you do your forceful expiration , no matter how much you push your chest , by doing forceful expiration you'll spell air outside but always you will still have volume of air inside your lungs , this volume of air ( the minimum amount of air remaining in your lungs – I'm not inspiring or expiring it – after forceful expiration is called the residual volume RV ) and its 1.2 liters and it has many functions : mainly to keep the blood going through the respiratory system and taking oxygen because if I can expel that amount of air out I'll collapse the lungs completely and they'll be empty from air , if that happens the blood flow will cross the lungs without taking oxygen and its also
important to maintain the normal shape of the chest ( not collapsing it ) .
6 . Functional residual capacity ( FRC ): volume in lungs at the end of quite passive expiration.
after quiet passive expiration means : taking the tidal volume by inspiration and taking out the tidal volume by passive normal expiration at that point
12

there are still two volumes inside the lungs : the residual volume – which is always there and you can’t expel it out and the expiratory reserve volume and
its there because I didn’t do a forceful expiration so : the sum of residual volume + the expiratory reserve volume =
functional residual capacity ( 1.2 + 1 = 2.2 liter ).
7 . vital capacity: its equal to tidal volume + inspiratory reserve volume + expiratory reserve
volume . ( 500+3000+1000 = 4500 ml ) 4.5 liter .
and its called so ( vital ) because it can be used ; inspiratory reserve volume I can breath it , tidal volume I always use it , expiratory reserve volume I can expel it out , so by being able to use these three wether in taking the air in or
out they're for my benefit. the definition : the maximum amount of air a person can inspire after forceful expiration expiring the tidal volume and the ERV now the three volumes of vital capacity are out – coz IRV is originally out - and the remaining in the lungs is only the residual volume , then the person starts to inspire forcefully he'll take the EV then the tidal volume then the IRV and by doing so a person will have a new fresh air from atmosphere inside my lungs to use it . so it’s the maximum amount of air that you can take it in by forceful inspiration and expel it
out by forceful expiration.
8 . total lung capacity: it’s the whole volumes all together RV , IRV , ERV and TV , its about 5.7 liters of
air.
9 .Forced expiratory volume in 1 sec: its important in medicine , if I ask a person to do a forceful inspiration , he will get inside his lungs the whole things : ( total lung capacity ) , if I ask him to expire that forcefully he will expel out the vital capacity because the residual volume can't be expelled , by doing so if I ask the person to do that forceful expiration under normal condition , in the first second of expiration , he'll expel 80% of the whole air inside your lung that he inspired , and the remaining 20% will be expelled by the sec and third and fourth second of breathing , remember : in normal breathing you breath in and out 12 times per minute , so 5 seconds for they whole cycle of inspiration and expiration , but for forceful inspiration and expiration its more than that , so if we say that forceful expiration is 4 to 5 seconds , in the first second , you'll expel 80% of the vital capacity , and this is the normal situation if its lower then its pathological ,
especially with the smokers they will not be able to expel 80% of VC .
The student questions: The questions weren't that clear , but we put the answers here :
13

-one of the students asked a question about the total lung capacity and the doctor answered : when you are setting by the end of your inspiration you have tidal volume , inspiratory reserve volume and residual volume . IRV is always outside , its not inside your lungs , but your lungs are able to have it by stretching to get it inside , so the only volume which is always out is the IRV , tidal volume its always in ( by inspiration ) and out ( by expiration ) , Expiratory reserve volume is always in but you can get it out whenever you need to , so
not all the volumes are inside the lungs. -another student asked : what about the yawning ?
The doc answered : it’s the same it’s a deep breath u need it whenever inside the lung there's contamination so you want to expel that to take fresh air inside , and about the relation between that and sleeping its still an unanswered
question for the scientists. -and then another student asked a question , the doctor answered : risdual
volume has nothing to do with vital capacity , the amount of air expelled outside is the vital capacity , 80% of it will be in the 1st sec and 20 % of the vital capacity ( not the residual volume ) will be in the remaining seconds . and then the student asked why ? and the doctor said : "you wanna know why ?! then set another 10 mins !! " … but the lecture time was already done :P
الله* هدانا أن لوال لتنهتدي كنا ما و لهذا هدانا الذي *الحمدلله
و توكلت عليه بالله إال توفيقي ما و إياه علمتني ما استودعك إني اللهم(: ألنفسكم الدعاء تنسو ال و.) آمين أنيب إليه
Best of luck to you all, Shouroq alalmeh شروق عاللمة
Aya alaaliاية علعالي
14