pitfalls in critical care - welcome to...
TRANSCRIPT
Ten Pitfalls in Intensive Care
Critical Care Two Working Principles
1. Critical illness is precipitated by specific disease. The first working principle is to rapidly identify and limit or reverse the triggering disease.
2. The second working principle is to keep the patient alive using default ICU therapies till disease is reversed & the body heals itself.
– Mechanical Ventilation
– Vasoactive medications
– Renal Replacement Therapy

Critical Care Other Aspects
• Other Aspects • Infection control, nutrition, nursing, physiotherapy
• Safety & comfort ICU measures
• Ensure appropriate protocols, documentation, staffing & organization
• Wait for recovery, wean & discharge
• Prevent common pitfalls & hopefully improve clinical outcomes

Pitfall 1: Case Scenario
• A 75-year-old gentleman presents to ER
• 5 day history of fever and productive cough
• He looks unwell, is tachycardic and tachypneic with a systolic blood pressure of 85 mmHg
• Intravenous fluids are commenced and appropriate investigations sent
• Right basal consolidation on the chest X-ray confirms a diagnosis of community-acquired pneumonia
• After 2 liters of intravenous fluids the patient remains hypotensive

Pitfall 1: Case Scenario
• Transferred to ICU
– Standard monitoring instituted
– An internal jugular vein inserted: CVP - 12 mmHg
– Hypotension persists, noradrenaline started
– Drugs are written up and ordered
• What was the Pitfall?

Pitfall No. 1: Delayed Definitive Treatment
• There is no mention of antibiotic administration
• The single most important determinant of outcome in septic shock is the time in which the correct antibiotic is given, after the onset of hypotension
• Additional source control if needed

(Crit Care Med 2006; 34:1589–1596)
Other (Early) Antibiotic Literature
Positive Trials • Yokota PKOPLoS ONE 9(11):
e104475. doi:10.1371/journal.pone.0104475
• Ricard Ferrer, Crit Care Med 2014; 42:1749–1755
• Weiss Crit Care Med 2014; 42:2409–2417 – Paediatrics
Negative Trials • Antonia L. American Journal of
Emergency Medicine 32 (2014) 7
• Bas de Groot, Critical Care 2015, 19:194
• BASIC. J Antimicrob Chemother 2010; 65: 1276
• Stephen W. Shock, vol. 42, no. 3, pp. 185y191, 2014
• Hranjec T, Lancet Infect Dis. 2012:17:774-780
• Sterling (Crit Care Med 2015; 43:1907–1915)
Other Early Antibiotic Literature: Interpretation
• Early & appropriate antibiotics save lives in primary & severe sepsis
• Evidence lacking
– Secondary sepsis
– Less severe infections (without hypotension)
– Studies with poor microbiological correlation

Pitfall 1: Delayed Treatment
• Time is tissue
–Rapid resuscitation
–Rapid identification of precipitating illness
–Rapid reversal of precipitating illness
Pitfall No. 2
Forgetting this Person

Ignaz Philipp Semmelweis 1818-65
…in the whole history of medicine there is only one Semmelweis in the magnitude of his services to Mankind, and in the depth of his sufferings from contemporary jealous stupidity and ingratitude.
Sir William Sinclair (1909)


Death of his friend Kolletschka, Professor of Forensic Pathology
• 'In the course of a post-mortem examination he was pricked in the finger by one of his pupils with a knife.... ……….. and he died from pleurisy, pericarditis, peritonitis and meningitis………
• it rushed into my mind with irresistible clearness that the disease from which Kolletschka had died was identical with that from which I had seen so many hundreds of lying-in women die…
Ignaz Philipp Semmelweis 1818-65
• He began, in May 1847, to use chlorinated lime with which every student was required to wash his hands before making an examination
• At the time of the introduction of this measure, the mortality rate stood at 12%
• Following it the mortality fell to 3%
• Next year: Mortality = 1.27%.( 45 of 3,556)
• Later moved to Budapest & introduced the practice

Is Hand Washing The Most Important Aspect of Infection Prevention
Vienna
• 12%
– Historic controls
• 3%
– 1st year of hand washing
• 1.3%
– Next year
Budapest
• < 1%
– St Roque Hospital:
• At times > 13%
– Contemporary controls in “splendid university clinics throughout the empire”
Hand Washing: The Choice is Yours
• Mortality benefit in healthy young post-partum females: ~1 vs. 10-11%
– RR = 0.1 (10%) & RRR = 0.9 (90%)
– ARR = 10% & NNT = 10
• Cost & Risk: Negligible
Pitfall No. 2: Poor Infection Control
• Most critically ill patients no longer die early in their illness due to refractory shock • They are resuscitated with standard techniques & many remain
in multi-organ dysfunction
• Each episode of secondary sepsis increases the chance of death
• After rapid eradication of the primary focus of illness, prevention of secondary sepsis may be the most effective method of improving outcomes
• Be obsessive about implementing basic IC practices – Hand washing before patient and device contact – Full barrier precautions for invasive procedures
Pitfalls No. 3, 4 & 5
• Patient stabilizes but not better • Open ICU Scenario
– Multiple specialists give multiple inputs – Inputs very inconsistent – Management changes depending on which
consultant seen most recently
• Closed ICU Scenario – Different Intensivists cover over different periods – Each has own practices patters – Patient care varies depending on rota!!!!
• Question: What are the Pitfalls?

Pitfalls No. 3, 4 & 5
Pitfalls No. 3, 4 & 5
• Near universal problem of varying practice patterns by different ICU & consulting physicians
• The best way to improve uniform yet effective care is for all to agree to practice Evidence Based Medicine
– To focus on clinical outcomes in ICU patients
– Avoid using too many unproven therapies
• Necessary to be updated with medical literature
– Especially RCTs and meta-analysis using mortality as the primary outcome
• ICUs need Direction & Leadership

PITFALL NO. 3
Failure to use EBM For Standards Life Support Techniques In ICU
EBM for Basic Intensive Care Therapies
• Haemodynamics
– BP Target
– Choice of Fluids
– Choice of Vasoactive drugs
– Early Resuscitation: EGDT
• Ventilation
– ARDS
• Renal Replacement Therapy
BP Targets & Choice of Fluids
• BP Target – SEPSISPAM (NEJM - March 18, 2014)
• Choice of Fluids • SAFE N Engl J Med 2004;350:2247-56 • FEAST N Engl J Med 2011;364:2483-95 • CRYSTMAS study. Crit Care 2012, 16:R94. doi:10.1186/cc11358 • 6S (Scandinavian Starch for Severe Sepsis/Septic Shock) trial) N
Engl J Med 2012. DOI: 10.1056/NEJMoa1204242. • CHEST N Engl J Med 2012;367:1901-1911. • CRISTAL JAMA 2013;310:1809–1817. • ALBIOS (March 18, 2014, at NEJM.org. ) • SPLIT JAMA 2015

Choice of Vaso-Active Agents
• Annane D, Vignon P, Renault A, et al. Norepinephrine plus dobutamine versus epinephrine alone for management of septic shock: a randomised trial. Lancet 2007;370:676-84.
• Myburgh JA, Higgins A, Jovanovska A, Lipman J, Ramakrishnan N, Santamaria J. A comparison of epinephrine and norepinephrine in critically ill patients. Intensive care medicine 2008;34:2226-34.
• Russell JA, Walley KR, Singer J, et al. Vasopressin versus norepinephrine infusion in patients with septic shock. N Engl J Med 2008;358:877-87.
• De Backer D, Biston P, Devriendt J, et al. Comparison of dopamine and norepinephrine in the treatment of shock. N Engl J Med 2010;362:779-89.
• Meta-Analysis PLOS ONE | DOI:10.1371/journal.pone.0129305 August 3, 2015

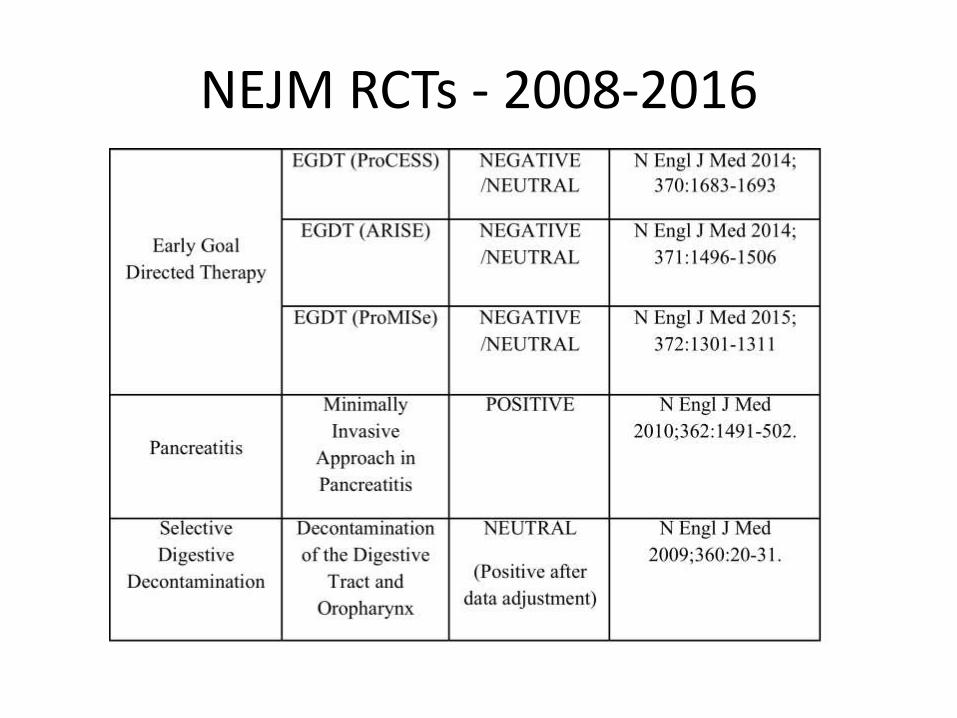
Early Resuscitation: EGDT
• The ProCESS Investigators. A Randomized Trial of Protocol-Based Care for Early Septic Shock. N Engl J Med 2014; 370:1683-1693
• The ARISE Investigators and the ANZICS Clinical Trials Group. Goal-Directed Resuscitation for Patients with Early Septic Shock. N Engl J Med 2014; 371:1496-1506
• The ProMISe Trial Investigators. Trial of Early, Goal-Directed Resuscitation for Septic Shock. N Engl J Med 2015; 372:1301-1311

Basic ICU Therapy: Haemodynamics What does the Literature Show
• BP Targets (With perfusion maintained)
– Septic shock: MBP > 65 mmHg
• Previous HT > 80-85 mmHg
• Choice of Fluids
– Crystalloids and colloids are associated with similar outcomes
– Avoid starch solutions in renal injury or severe sepsis
– Routine replacement of albumin is not useful
• ? in severe sepsis sub group analysis
• ? Useful in a meta-analysis
– Buffered solutions & saline have similar clinical outcomes
Basic ICU Therapy: Haemodynamics What does the Literature Show
• Vaso-Active Agents
– Catecholamines seem equivalent for major outcomes
– Safety profile and efficacy of Noradrenaline may be best overall and in cardiac patients
– Vasopressin in low fixed dose is a safe and effective second line alternative drug
• EGDT is similar to Early Standard Therapy
RESPIRATORY SUPPORT
How Should We Ventilate Patients With ARDS


RENAL SUPPORT
Which Modality
How Much
How Early
RRT: Which Modality? HD vs CRRT: 4 RCTs
• Mehta RL et al. A randomized clinical trial of continuous versus intermittent dialysis for acute renal failure. Kidney International (2001);60:1154 - 63.
• Uchino S et al Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators . Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA 2005; 294: 813–818.
• Vinsonneau C, et al. Continuous venovenous haemodiafiltration versus intermittent haemodialysis for acute renal failure in patients with multiple-organ dysfunction syndrome: a multicentre randomised trial. Lancet 2006, 368:379-385.
• Lins R, Elseviers M, Van der Niepen P, Hoste E, Malbrain ML, Damas P, Devriendt J.; SHARF Investigators: Intermittent versus continuous renal replacement therapy for acute kidney injury patients admitted to the intensive care unit: Results of a randomized clinical trial. Nephrol Dial Transplant 24: 512–518, 2009
RRT: How Much? High vs Standard Dose / Intensity: 2 Large RCTs
• Initial (Ronco) Trial showed high dose CRRT has mortality benefit
• Two subsequent larger RCTS failed to show benefit
• RENAL Trial Intensity of continuous renal-replacement therapy in critically ill patients. N Engl J Med. 2009 Oct 22;361(17):1627-38.
• VA/NIH ATN Trial. Intensity of renal support in critically ill patients with acute kidney injury. N Engl J Med. 2008 Jul 3;359(1):7-20

RRT: How Early Early versus Late: 4 Large RCTs
• Initial small studies
– Benefit in cardiac surgery patients
• Two later studies (early & intense RRT) were negative – Ronco C et al. Early isovolaemic haemofiltration in oliguric patients
with septic shock. Intensive Care Med (2006) 32:80–86
– Bouman CS, Oudemans-Van Straaten HM, Tijssen JG, Zandstra DF, Kesecioglu J. Effects of early high-volume continuous venovenous hemofiltration on survival and recovery of renal function in intensive care patients with acute renal failure: A prospective, randomized trial. Crit Care Med. 2002 Oct;30(10):2205-11.
Renal Replacement Therapy Early versus Late: 2 Meta-Analysis
• Earlier Meta-analysis Critical Care 2011;15:R72.
– Suggest benefit, but significant heterogenity
• Recent Meta-analysis Critical Care (2016) 20:122
– High Quality Studies only
• no overall or subgroup benefit, either for mortality or for duration of illness or hospitalization.
– Low quality studies showed benefit

Renal Replacement Therapy: Early versus Late: 2 Newer RCTs: AKIKI vs ELAIN
AKIKIn=620 ELAINn=231CaseMix 80%Medical
20%Surgical20%Medical80%Surgical
Design Multi-center31FrenchSites
Singlecenter1GermanSite
SeveritySOFA(Early&Late)
10.9&10.8 15.6&16
RRT IHD&/orCRRT OnlyCVVHDF
EarlyInitiation KDIGO3(1) KDIGO2(2)LateInitiation Conventionalcriteria(3) In12hoursofKDIGO3
LateInitiationDidnotreceiveRRT
49% 9%
Primaryendpoint 60daymortality 90mortality
Outcome:Mortality(EarlyvsLate)
150/311(48.5%)vs153/308(49.7%)
44/112(39.3%)vs65/119(54.7%)
HazardRatio(95%CI)&Pvalue
1.03(0.82–1.29)p=0.079
0.66(0.45to0.97)p=0.03
Statistics:Poweredat(for5%Significance)
90% 80%
Statistics:PoweredtodetectanAbsoluteriskreductionfromapresumedbaselineof55%
15% 18%
Statistics:FragilityIndex(4)
-21(5) +3(6)
RRT- Current Evidence
• HD & CRRT appear to have similar clinical outcomes
– ? Less renal loss with CRRT
• Standard intensity and high intensity RRT appear to have similar outcomes
– Earlier small studies showed benefit
• The timing of initiation of RRT is unclear
– Two Meta-Analysis: Earlier shows benefit, significant heterogenity, later shows no benefit
– Two recent RCTs. One showed benefit
– Two RCT on going (STARRT-AKI, & IDEAL-ICU trial )
Pitfall No. 4: Chasing the Wrong Target
Physiology Outcome
• Vital Parameters
• Haemodynamic parameters
• Ventilatory parameters
• Laboratory investigations – Haematology
– Biochemistry
– Microbiology
• Imaging
• Scoring systems
Clinical Outcome
1. Mortality (all cause) – ICU / Hospital
– Time point
2. Severity – Less invasive intervention
– Less duration
– Less distress or discomfort
3. Recovery – Shorter duration for recovery
– Full return of function
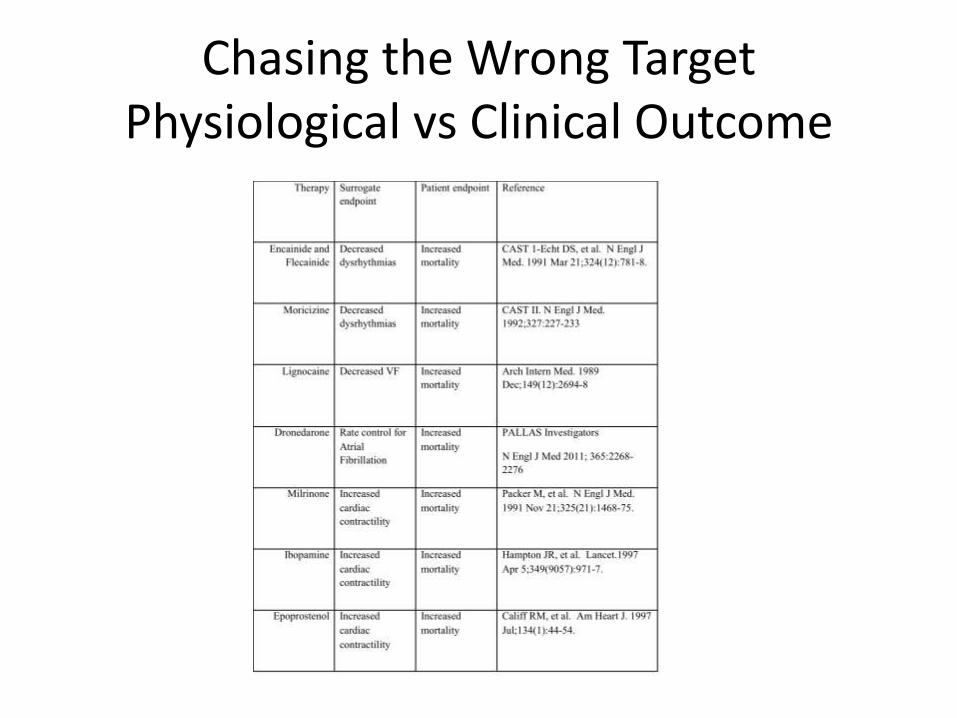
Chasing the Wrong Target Physiological vs Clinical Outcome
• Nitric Oxide is the physiological vasodilator – Dys-regulation in sepsis contributes to the shock state
– Physiologically plausible to inhibit it in septic shock
• NO-Synthase inhibitor (NG-methyl-L-arginine hydrochloride)
• First RCT: Endpoint- Resolution of shock. (CCM 2004; 32:1–12) – Promotes resolution of shock
– Acceptable safety profile
• Second RCT Endpoint- Mortality (CCM 2004; 32:21–30) – Higher 28 day mortality (59 vs 49%. P<0.01)
– Trial stopped early by the independent data safety monitoring board

Chasing the Wrong Target Physiological vs Clinical Outcome
• "The scientist is not a person who gives the right answers, he is one who asks the right questions." Claude Lévi-Strauss. French philosopher
• In Critical Care – The Right Question: which therapies improve clinical
outcomes?
– The Wrong Question: which therapies improve physiological parameters?

Chasing the Wrong Target Physiological vs Clinical Outcome

Chasing the Wrong Target Physiological vs Clinical Outcome
Chasing the Wrong Target Physiological vs Clinical Outcome

Chasing the Wrong Target Physiological vs Clinical Outcome

Cherry Picking Trials?
He uses statistics as a drunken man uses lamp posts –
for support rather than for illumination." -
Andrew Lang
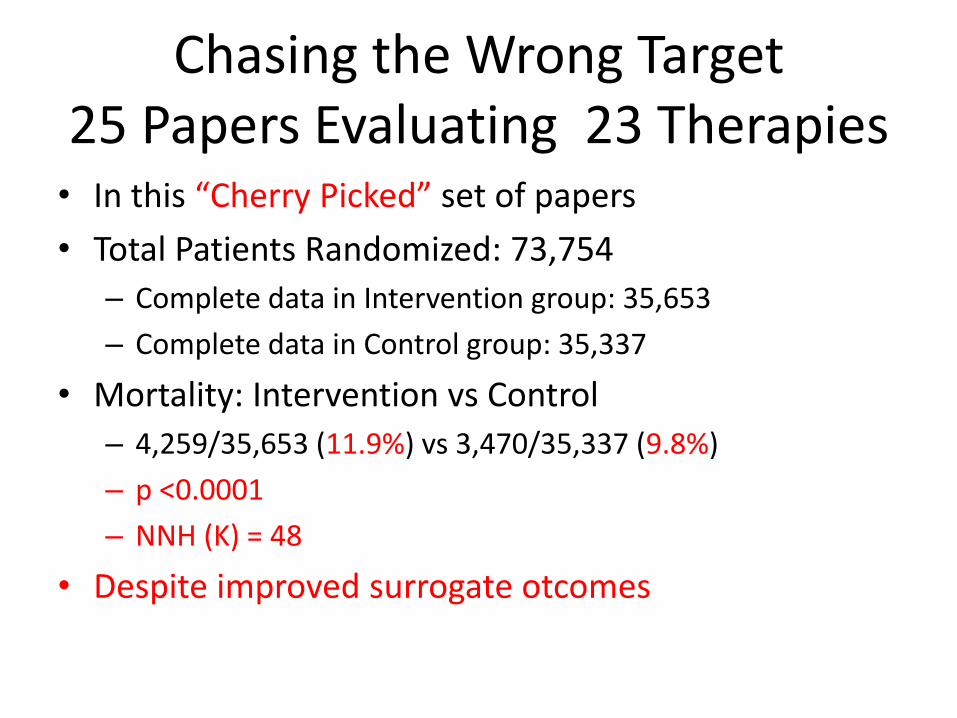
Chasing the Wrong Target 25 Papers Evaluating 23 Therapies • In this “Cherry Picked” set of papers
• Total Patients Randomized: 73,754
– Complete data in Intervention group: 35,653
– Complete data in Control group: 35,337
• Mortality: Intervention vs Control
– 4,259/35,653 (11.9%) vs 3,470/35,337 (9.8%)
– p <0.0001
– NNH (K) = 48
• Despite improved surrogate otcomes

Pitfall No. 4: Chasing the Wrong Target
• It is not a pitfall to target physiological goals in the practice of critical care
• It becomes a pitfall when we assume that the correction of these factors will unquestionably lead to better clinical outcomes
Pitfall no. 5: Can Less Be More?
It takes a lot of hard work to make
something simple, to truly understand
the underlying challenges and come
up with elegant solutions. Simplicity
isn’t a style. It’s not just minimalism or
absence of clutter. It involves digging
through the depth of complexity. To
be truly simple, you have to go really
deep, to understand the essence in
order to get rid of the parts that are
not essential.
Steve Jobs

Pitfall no. 5: Can Less Be More?
• The Hypothesis: Will a Restrictive approach, compared to a Liberal approach, result in better clinical outcomes in intensive care patients.
• The Liberal Approach:
– Use all the proven therapies
– Use all other plausible therapies
• The Restrictive Approach:
– Limiting routine therapies to proven ones
– Selectively and judiciously use other techniques based on clinical evaluation of the individual patient
Can Less be More? An Illustrative Example
• Early palliative care for patients with metastatic non–small-cell lung cancer. N Engl J Med 2010;363:733–42.
• Metastatic non–small cell lung cancer
• Early vs late referral to palliative care

Can Less be More? An Illustrative Example
• Part of the palliative care management was the documentation of preferences ICU at the end of life
– More patients in the early palliative care group had documented their preferences than those in the standard care group.
• More patients in the standard treatment group received aggressive ICU care than those in the palliative care group
– The median survival was higher in those receiving palliative care and less ICU therapy.
Can Less be More?
• O2 therapy
• Adrenaline & hypothermia in CPR (OH)
• Blood transfusion
• Nutrition
• Sugar control
• DVT prophylaxis
• Steroids
• VOMIT
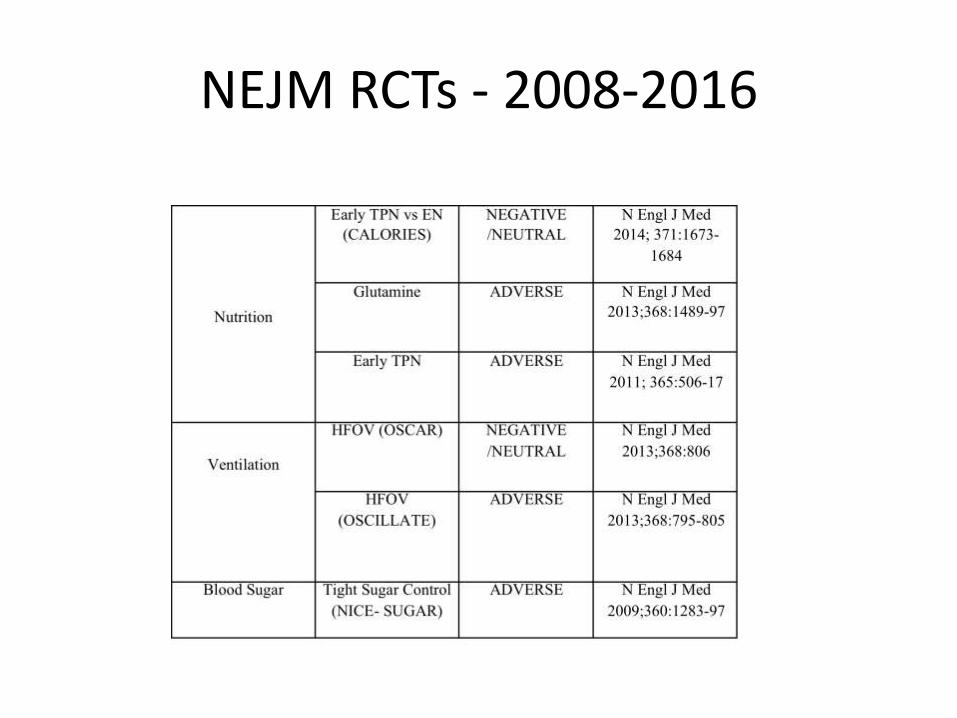
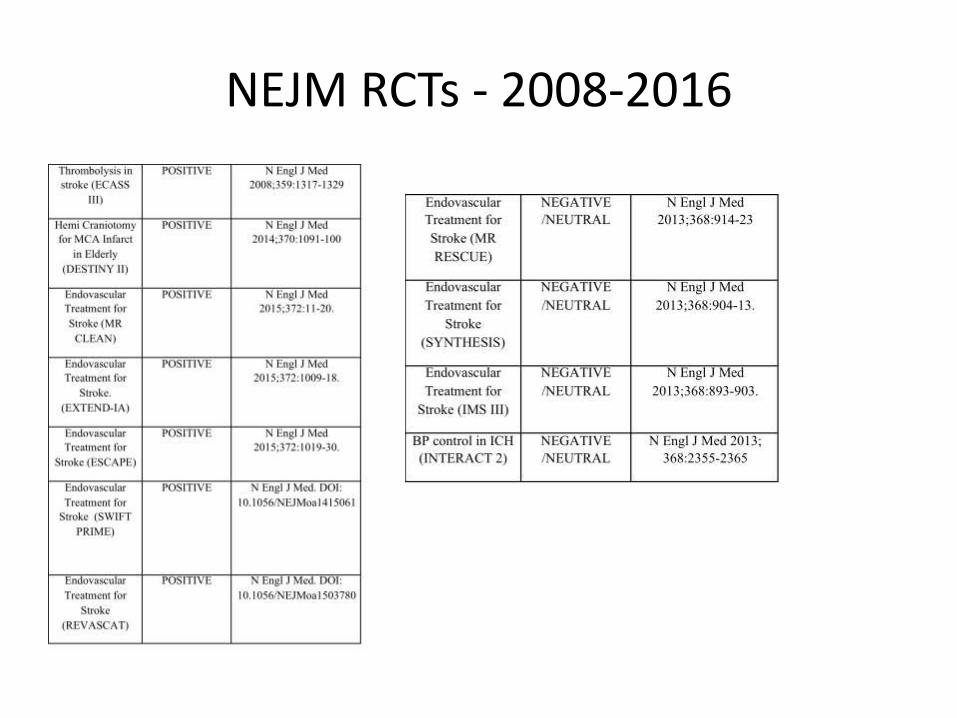
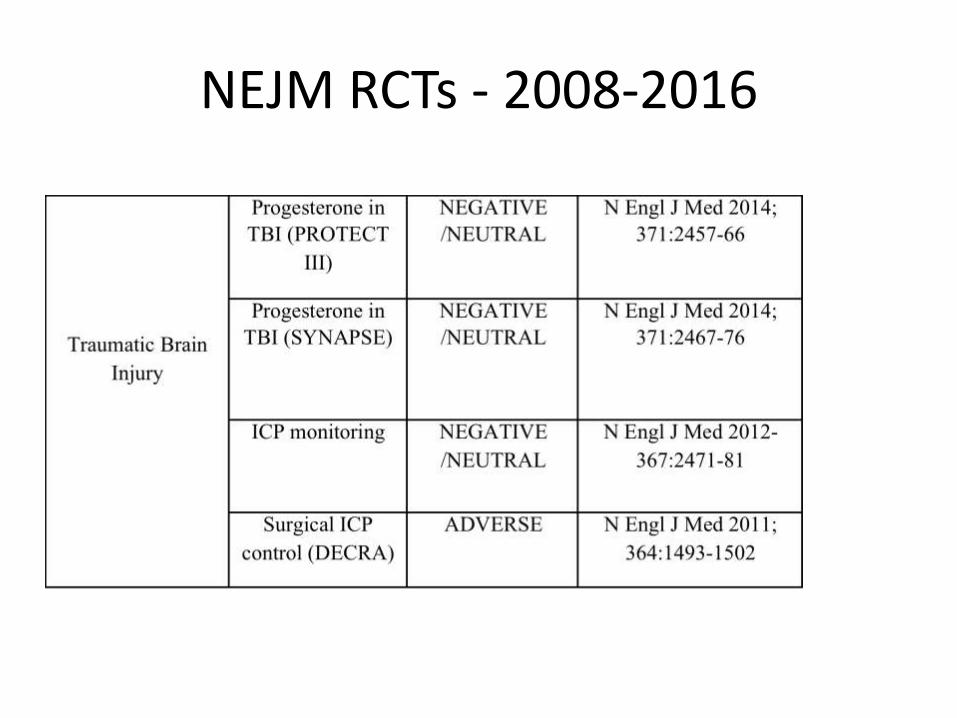
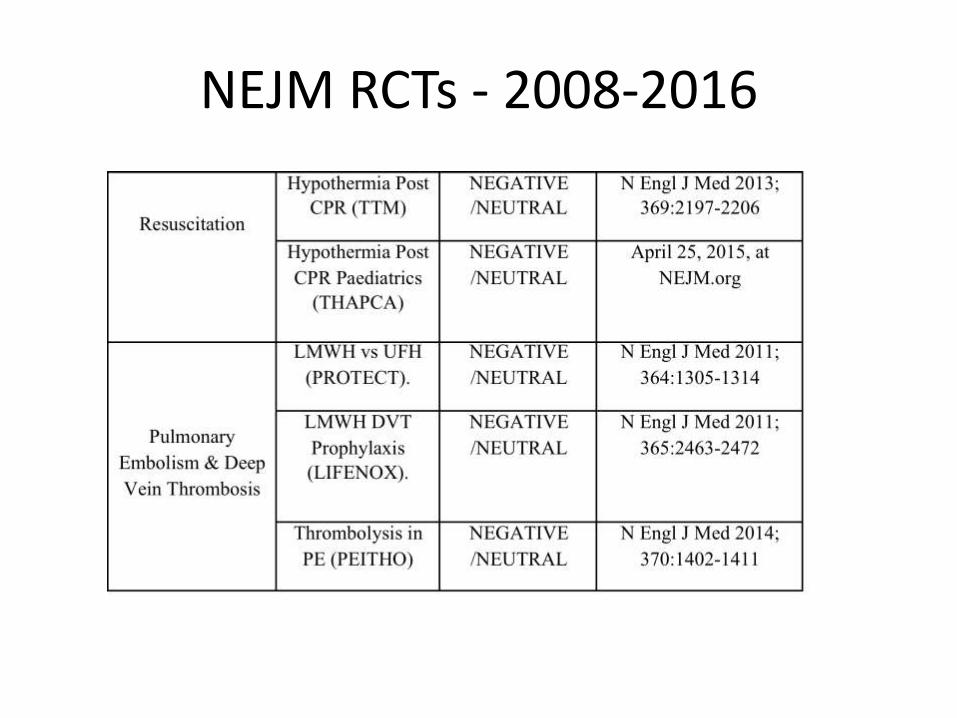
A Snapshot of NEJM RCTs 2008-2016
• A Review of all NEJM Critical Care & Acute Care Related large RCTs
– Most with Mortality as the primary end point
• How Many were Positive, Neutral or Adverse
– Allows evaluating of our understanding of underlying pathophysiology

NEJM RCTs - 2008-2016
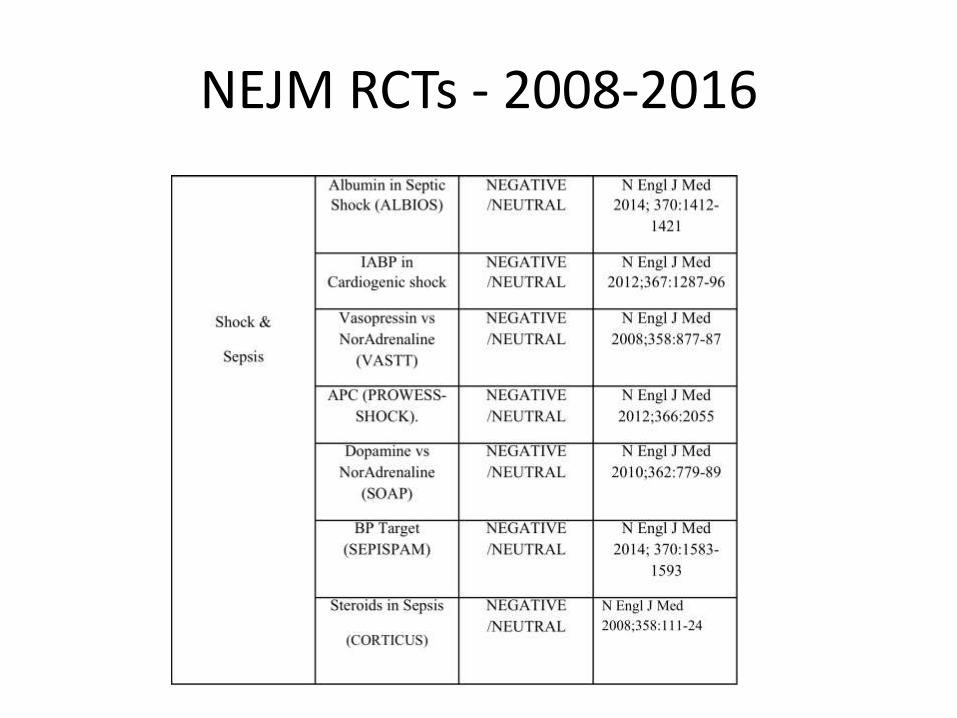
NEJM RCTs - 2008-2016
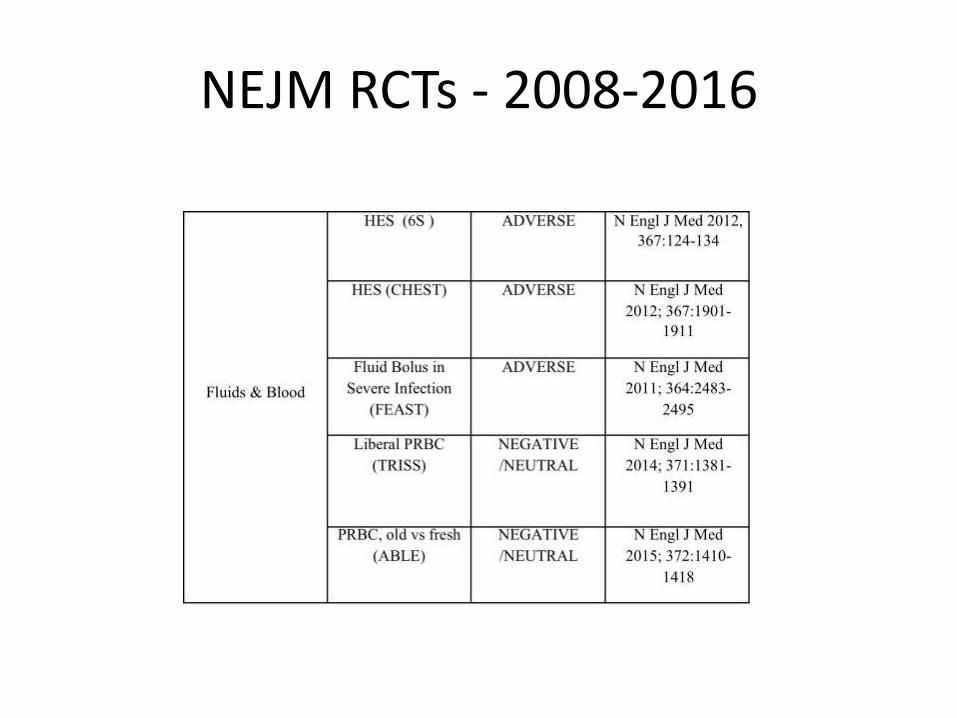
NEJM RCTs - 2008-2016
NEJM RCTs - 2008-2016
NEJM RCTs - 2008-2016
NEJM RCTs - 2008-2016
NEJM RCTs - 2008-2016
NEJM RCTs - 2008-2016
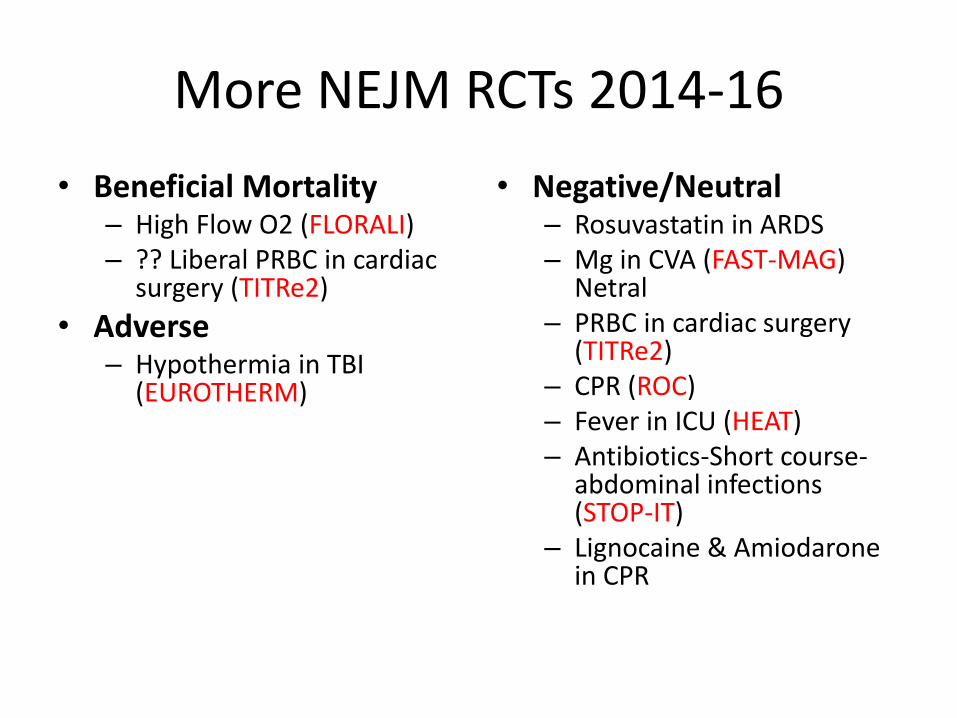
More NEJM RCTs 2014-16
• Beneficial Mortality – High Flow O2 (FLORALI) – ?? Liberal PRBC in cardiac
surgery (TITRe2)
• Adverse – Hypothermia in TBI
(EUROTHERM)
• Negative/Neutral – Rosuvastatin in ARDS – Mg in CVA (FAST-MAG)
Netral – PRBC in cardiac surgery
(TITRe2) – CPR (ROC) – Fever in ICU (HEAT) – Antibiotics-Short course-
abdominal infections (STOP-IT)
– Lignocaine & Amiodarone in CPR
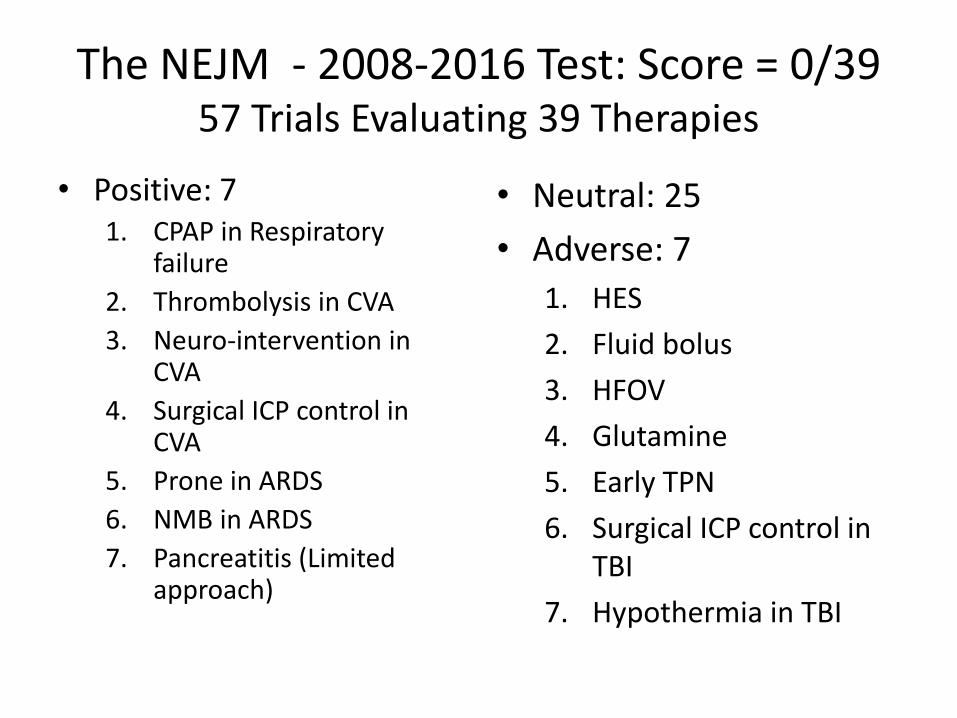
The NEJM - 2008-2016 Test: Score = 0/39 57 Trials Evaluating 39 Therapies
• Positive: 7 1. CPAP in Respiratory
failure
2. Thrombolysis in CVA
3. Neuro-intervention in CVA
4. Surgical ICP control in CVA
5. Prone in ARDS
6. NMB in ARDS
7. Pancreatitis (Limited approach)
• Neutral: 25
• Adverse: 7
1. HES
2. Fluid bolus
3. HFOV
4. Glutamine
5. Early TPN
6. Surgical ICP control in TBI
7. Hypothermia in TBI
Cherry Picking Trials?
He uses statistics as a drunken man uses lamp posts –
for support rather than for illumination." -
Andrew Lang

The NEJM 2008-2016 Test 57 Trials Evaluating 39 Therapies
• Total Patients Randomized: 112,532
– Complete data in Intervention group: 56,427
– Complete data in Control group: 51,221
• Mortality: Intervention vs Control
– 24,860/56,427 (44.1%) vs 19,968/51,221 (39%)
– p <0.0001
– NNH (K) = 20
• This is not a “Cherry Picked” list of RCTs
Pitfall No. 6,7 & 8
• The patient has stabilized and is showing signs of recovery
– The inotropes are off & patient is awake and alert on PSV
• Staff shortage
– Additionally, a few have left for NABH mock CPR drill
• There was no nurse in the patients’ cubicle
– Patient self extubated deteriorated-->Intubation
– Malfunctioning laryngoscope & suction arrested
– CPR
• Patient stabilizes but unresponsive

Pitfall No. 6,7 & 8
• The ICU consultant is then informed about the event
• The primary consultant is unable to find any notes
– Asks for 100% O2 & neurologist opinion
• Neurologist asks for MRI
– Patient recovers consciousness- but neurologist not contactable
– Patient deteriorates in MRI needing inotropes
– He then stabilizes over the next 48-72 hours
• What are the Pitfalls?

Pitfall No. 6,7 & 8
Pitfall No. 6,7 & 8
• Inadequate ICU Infrastructure
– Failure to appropriately use protocols & guidelines
– Inadequate communication & documentation
– Inadequate Staffing
• Intensivist must ensure the above

Protocols & Guidelines
• The Good: Strong safety measures prevent errors
• The Bad: Clinicians are pressurized to follow practices they do not believe
• The Ugly: Documentation of worse outcomes when blindly & unquestioningly following guidelines
• The Pragmatic: Guideline On How To Use Guidelines
Guideline On How To Use Guidelines!!!!! The Pragmatic
• “Evidence Free” recommendations
– Obsessively follow safety guidelines
– Largely follow guidelines based on high quality EBM
• Large RCTs with clinical endpoints
– Resist slavishly following guidelines based on poor quality EBM (> 50-75% of most guidelines)
Pitfall No 7: Poor Communication & Documentation
• Clear communication Between ICU Doctors, Nurses, Respiratory Technicians, & other ICU staff as well as primary & referred specialties
– Main diagnosis
– Physiological status
– Test reports
– Investigations awaited
– Treatment
– Plan for the day

Pitfall No. 8: Staffing & Organization
Crit Care Med 2014; 42:344–356
(Crit Care Med 2014; 42:344–356)
• Design: We surveyed 69 ICUs about organization, size, volume, staffing, processes of care, use of protocols, and annual ICU mortality
• Conclusions: In a sample of 69 ICUs, a daily plan of care review and a lower bed-to-nurse ratio were both associated with a lower annual ICU mortality
Pitfall No. 6,7 & 8
Don’t Be Sloppy
Pitfall No. 9
• Scenario 1: Patient recovers over the next 3-4 weeks
– He is observed in ICU and later transferred to the ward
– He is weak and poorly mobile, advised to rest
• Discharged home
– Started on a physiotherapy program
• 3 months to become physically functional
• Another three months to go back to his job
• What was the Pitfall?

Pitfall No. 9: Inadequate or Delayed Rehabilitation
The Muscle Is The Forgotten Organ Of ICU
The Post ICU Syndrome
• Prolonged disability ( even at 5 years) – (Herridge N Engl J Med 2011;364:1293–304.)
• Renal Loss – (BEST. JAMA 2005;294: 813–8)
• Higher Cardio & Cerebro Vascular events & mortality – (Yende Am J Respir Crit Care Med 2014;189:1065–74)
• Neuro-psychiatric dysfunction
– Pandharipande N Engl J Med 2013;369:1306–16.
• ICU Acquired Weakness & CIP-CIM
– Lancet Neurol 2011;10:931-41

Important Rehabilitation Studies
• Lancet 2009;373:1874 • Int J Rehabilitation Res 2011; 34: 336 • American Journal of Respiratory and Critical Care
Medicine Volume 190 Number 4 | August 15 2014 • Chest 2013;144:1469–80. • Br J Anaesthes 2014; doi:10.1093/bja/aeu051 • TEAM study. Critical Care (2015) 19:81 • J Crit Care 2015; 30: 13–18 • RECOVER -JAMA Intern Med 2015;175: 901–910.
• Peter E. Morris. JAMA. 2016;315(24):2694-2702.
Summary of Studies
• Physical therapy is effective in hastening recovery – Not better final outcome
• More effective if started earlier
• It is probably not being done as much as is necessary
• Needs to be encouraged in and after ICU
• Should be graded, supervised & multifaceted
• Only exercise associated with improved Physical Fitness
Summary of RCTs
• Lancet 2009;373:1874 – A strategy for whole-body rehabilitation—consisting of interruption of
sedation and physical and occupational therapy in the earliest days of critical illness—was safe and well tolerated, and resulted in better functional outcomes at hospital discharge, a shorter duration of delirium, and more ventilator-free days compared with standard care.
• RECOVER -JAMA Intern Med 2015;175: 901–910.
– Following ICU discharge: Standard vs individualized physiotherapy had similar outcomes
• Peter E. Morris. JAMA. 2016;315(24):2694-2702.
– “Standard rehab” vs “Usual ICU care” Similar outcomes
• Better physicial status at 6 months
Pitfall No. 10
• Scenario 2: Patient does not improve. History of COPD, Alzheimer's with aspiration & minimally mobile for 3-6 months.
• Continue with inotropes & ventilator • Becomes anuric & & dialysis started • 3 episodes of CPR. Resuscitated each time
• Relatives request treatment be stopped • Told it was unethical & that euthanasia was illegal • Suggested to take home LAMA (Left Against Medical
Advice)
• What is the Pitfall?
Quality of Terminal
Phase of Life
Quantity of Terminal
Phase of Life
Pitfall No. 10: Absence of EoL Care Plan

Pitfall No. 10: No plan for EoL Care
• Communication is the Key
• Consider Socio-Cultural issues
• Act within the law
• Be primarily guided by medical ethics
– Beneficence
– Non-Maleficence
– Autonomy
– Distributive Justice
Pitfall No. 10: ICU at EOL
• Change focus from physiology & prolonging the dying process to ensuring comfort – Pain
– Dyspnea
– Secretions
– Bladder-bowel, skin & eye care
– Ensure dignity
– Ensure autonomy
– Ensure family access

Summary

Shameless Plug (Available on Amazon - Kindle)
Summary
• Pitfall No. 1: Delay in giving antibiotics in Septic Shock – Delay in either reversal of disease or in resuscitation
• Pitfall No. 2: Poor Hand washing and Infection Control Practices
• Pitfall No. 3: Eminence instead of Evidence based medicine for standard ICU therapies
• Pitfall No. 4: Wrong Therapeutic target – Physiological targets instead of Clinical Outcomes
• Pitfall No. 5: Doing too much. Can Less be More?

Summary
• Pitfall No. 6: Inadequate or inappropriate use of protocols & guidelines
• Pitfall No. 7: Inadequate communication & documentation
• Pitfall No. 8 Inadequate staffing
• Pitfall No. 9: Inadequate or delayed rehabilitation
• Pitfall No. 10: Absence of EoL care planning

Concluding Thought
• An ability to evaluate EBM is part of the job of being a doctor & looking after patients
– Large RCTs & Meta-analysis using clinical end points in ICU patients
• Familiarity with emerging literature needed to guide clinical decisions
• Hopefully, constantly evaluating and modifying practices based on emerging evidence will improve clinical outcomes in our ICU patients