pl ce live 0512 short guide -...
TRANSCRIPT

−This handout accompanies the related articles published in−
PHARMACIST’S LETTER / PRESCRIBER’S LETTER May 2012 ~ Volume 28 ~ Number 5
More. . . Copyright © 2012 by Therapeutic Research Center
Pharmacist’s Letter / Prescriber’s Letter ~ P.O. Box 8190, Stockton, CA 95208 ~ Phone: 209-472-2240 ~ Fax: 209-472-2249 www.pharmacistsletter.com ~ www.prescribersletter.com
following
PL CE LIVE May 2012
Long Guide
ANTITHROMBOTICS
You’ll see more patients taking Brilinta (ticagrelor) for acute coronary
syndrome.
These patients usually get clopidogrel (Plavix, etc)...but now guidelines
suggest Brilinta over clopidogrel.
Brilinta is more effective...with a similar bleeding risk.
Brilinta prevents about 11 more cardiovascular deaths, 11 more heart
attacks, and 6 more stent thromboses than clopidogrel...for every 1000 acute
coronary syndrome patients treated for up to one year.
But Brilinta has downsides...possible dyspnea and twice-daily dosing instead
of once daily. Plus clopidogrel will cost less when generics come out in May.
Recommend taking just 81 mg/day of aspirin with Brilinta. Explain that
higher aspirin doses may make Brilinta less effective.
Clopidogrel will still be used a lot...especially now that prices are coming
down.
The controversy about using clopidogrel with PPIs will subside. When a PPI
is needed, recommend lansoprazole, dexlansoprazole, or pantoprazole...these are
less likely to interact.
Suggest clopidogrel if patients need an anticoagulant...we have more
experience using clopidogrel with warfarin.
Effient (prasugrel) will be used as an alternative to clopidogrel or
Brilinta for acute coronary syndrome.
It’s more effective than clopidogrel...but causes more bleeding.
Avoid Effient in most patients over age 75 and those with a previous stroke
or TIA...due to a higher bleeding risk.
To hear a great discussion of the pros and cons of these antiplatelets...and
what dose of aspirin to use with them...go to our PL Detail-Document to listen to
PL VOICES. You’ll hear an author of the latest Chest antithrombotic guidelines
talking with our team.
Also see our PL Chart, Comparison of Oral Antithrombotics, for antiplatelet
indications, dosing, interactions, and more.
Go to the Which Antiplatelet Drug to Add to Aspirin for Acute Coronary Syndrome
Detail-Document.
DISCUSSION POINTS LEARN MORE ABOUT THIS POINT... (Just click on the link for access!)
How the antiplatelet drugs stack up August 2011 Article – Brilinta, a new antiplatelet drug
Whether Plavix (clopidogrel) interacts with PPIs January 2012 Article – Reps will promote Dexilant (dexlansoprazole) for patients on Plavix (clopidogrel) who need a PPI

PL Detail-Document #271001 −This PL Detail-Document gives subscribers
additional insight related to the Recommendations published in−
PHARMACIST’S LETTER / PRESCRIBER’S LETTER October 2011
More. . . Copyright © 2011 by Therapeutic Research Center
P.O. Box 8190, Stockton, CA 95208 ~ Phone: 209-472-2240 ~ Fax: 209-472-2249 www.pharmacistsletter.com ~ www.prescribersletter.com ~ www.pharmacytechniciansletter.com
Comparison of Oral Antithrombotics (Last modified February 2012)
The recent proliferation of oral anticoagulants and antiplatelet agents has health care professionals questioning how to choose among them. The
newest anticoagulants are dabigatran (Pradaxa, Pradax [Canada]) and rivaroxaban (Xarelto). Also look for the direct factor Xa inhibitor apixaban
possibly in 2012, and edoxaban and betrixaban in the next few years. The following chart compares the indications, clinical benefit, antidotes,
washout, and other therapeutic considerations for these agents.
Abbreviations: ACS = acute coronary syndrome; ADP = adenosine diphosphate; A fib = atrial fibrillation; AV = arteriovenous; AWP = average
wholesale price; BID = twice daily; CAD = coronary artery disease; DVT = deep vein thrombosis; LMWH = low molecular weight heparin; LVD =
left ventricular dysfunction; MI = myocardial infarction; PE = pulmonary embolism; STEMI = ST segment elevation myocardial infarction; TIA =
transient ischemic attack; VTE = venous thromboembolism
Drug: Mechanism
Cost of 30-day
supplya
Approved Indications
(Usual Maintenance Dose)b
Clinical Benefit In…c
Antidote/
pre-op, pre-
procedure
washout (if
indicated)
Therapeutic
Considerations
ANTICOAGULANTS
Apixaban (Eliquis):
direct factor Xa
inhibitor1
(2.5 mg BID)
Canada: $120
Continued…
U.S.:
Investigational
Canada:69
VTE prevention post-hip or knee
replacement (2.5 mg twice daily for
32 to 38 days [hip] or 10 to 14 days
[knee], starting 12 to 24 hrs post-op)
A fib (off-label): at least as effective
as warfarin for stroke prevention,
systemic embolism, death; less major
bleeding1
Post-hip/knee replacement: at least as
effective as enoxaparin for preventing
VTE; comparable bleeding2,3
No specific
antidote Requires BID dosing.
69
For every 1000 A fib
patients treated for 1.8
years, apixaban prevents
six more strokes, 15 major
bleeds, and eight deaths
compared to warfarin.1
Caution if CrCl 15 to
29 mL/min, but no dosage
adjustment necessary. Not
recommended if CrCl
<15 mL/min.69
Contraindicated in severe

−This handout accompanies the related articles published in−
PHARMACIST’S LETTER / PRESCRIBER’S LETTER May 2012 ~ Volume 28 ~ Number 5
More. . . Copyright © 2012 by Therapeutic Research Center
Pharmacist’s Letter / Prescriber’s Letter ~ P.O. Box 8190, Stockton, CA 95208 ~ Phone: 209-472-2240 ~ Fax: 209-472-2249 www.pharmacistsletter.com ~ www.prescribersletter.com
following
PL CE LIVE May 2012
Long Guide
Pharmacist's Letter; August 2011; Vol: 27
New Drug Brilinta
You'll hear lots of buzz about Brilinta, a new antiplatelet drug. Brilinta (ticagrelor) will compete with Plavix (clopidogrel) and Effient (prasugrel)...for acute coronary syndrome
or after a stent. Plavix will still lead the pack...for a while. It was the first one approved and is used the most. But it's not perfect. Plavix has a delayed onset and variable response...because it has to be activated by cytochrome P450
enzymes in the liver. Effient is more effective than Plavix...but causes more bleeding. That's why it's not for patients with a prior
stroke or TIA, or over 75. Brilinta seems to be more effective than Plavix for acute coronary syndrome...and has a similar risk of major
bleeding in most cases. For every 1000 patients with acute coronary syndrome treated for up to one year, Brilinta prevents 11 more CV
deaths, 11 more heart attacks, and at least 6 more stent thromboses compared to Plavix. But these benefits are only seen with lower doses of aspirin. Tell patients to take Brilinta with 81 mg/day of
aspirin. Explain that doses over 100 mg/day may reduce Brilinta's efficacy. Brilinta has a faster onset than Plavix or Effient...because it's not a prodrug. It also wears off faster because it
binds to platelets REVERSIBLY...instead of permanently like Plavix and Effient. You'll hear this is an advantage in acute settings in case a patient needs surgery...but both Brilinta and Plavix
need to be stopped 5 days before surgery. Brilinta's short duration may be a disadvantage in the long run because it's taken twice a day...instead of once
a day like the others. Continue to recommend Plavix first for most patients...especially when the generic comes out (again) next
year. Caution against combining Brilinta with strong 3A4 inhibitors or inducers. Also don't exceed 40 mg/day for
simvastatin or lovastatin. Alert patients that Brilinta may cause shortness of breath...especially the first week. Suggest switching to Plavix
or Effient if it's severe or persistent.

More. . . Copyright © 2012 by Therapeutic Research Center
Pharmacist’s Letter / Prescriber’s Letter ~ P.O. Box 8190, Stockton, CA 95208 ~ Phone: 209-472-2240 ~ Fax: 209-472-2249 www.pharmacistsletter.com ~ www.prescribersletter.com
WOMEN’S HEALTH
Drug reps will promote Natazia for heavy menstrual bleeding.
Natazia (estradiol/dienogest) is the first oral contraceptive approved for
chronic menorrhagia...but other OCs are also effective.
Many women start with an NSAID to reduce cramps and bleeding...then go to
an OC if an NSAID isn’t enough for bleeding.
Heavy menstrual bleeding is often due to a hormone imbalance...especially
too little progesterone.
Natazia and other combo OCs reduce blood loss by about 50% in women with
heavy menstrual bleeding.
Explain that it’s not necessary to use Natazia. It costs more than generic
OCs...and handling missed pills is more complicated.
Suggest using a progestin-only contraceptive (Depo-Provera, etc) if a combo
OC isn’t appropriate. But explain that Depo-Provera might cause light, irregular
bleeding and weight gain.
Recommend Mirena (levonorgestrel IUD) for more severe cases. Explain that
it can reduce blood loss by 90% or more.
Suggest Lysteda (tranexamic acid) if a contraceptive isn’t desired. But
point out that it costs more and seems less effective.
Go to the Treatment of Menorrhagia Detail-Document.
DISCUSSION POINTS LEARN MORE ABOUT THIS POINT... (Just click on the link for access!)
Management of heavy menstrual bleeding August 2010 Article – new oral antifibrinolytic product for heavy menstrual bleeding called Lysteda (lye-STED-a)
Differences between the oral contraceptives December 2007 Article – how to choose the right oral contraceptive July 2010 Article – new oral contraceptive called Natazia (estradiol valerate/dienogest)

Detail-Document #231207
More. . . Copyright © 2007 by Therapeutic Research Center
Pharmacist’s Letter / Prescriber’s Letter ~ P.O. Box 8190, Stockton, CA 95208 ~ Phone: 209-472-2240 ~ Fax: 209-472-2249 www.pharmacistsletter.com ~ www.prescribersletter.com
ORAL CONTRACEPTIVES (Full update June 2010; last modified November 2010)
Productsa Manufacturer Estrogen Progestin Comments LOW-DOSE MONOPHASIC PILLS Aviane-28 Lessina Lutera Sronyx
Teva Teva Watson Watson
EE 20 mcg Levonorgestrel 0.1 mg Low estrogen; low progestin; low androgen.14 Low estrogen dose may cause more spotting and less margin of error for missed pills. Good choice to minimize risk of estrogen side effects like nausea, breast tenderness, etc.6
Junel 1/20 Junel Fe 1/20 Loestrin-21 1/20 Loestrin Fe 1/20 Microgestin 1/20 Microgestin Fe 1/20
Teva Teva Warner Chilcott Warner Chilcott Watson Watson
EE 20 mcg Norethindrone 1 mg Low estrogen; high progestin; medium androgen.13, 14 Low estrogen dose may cause more spotting and less margin of error for missed pills. Good choice to minimize risk of estrogen side effects like nausea, breast tenderness, etc.6
Levora Nordette-28 Portia-28
Watson Duramed/Teva Teva
EE 30 mcg Levonorgestrel 0.15 mg Low estrogen; medium progestin; medium/high androgen.13, 14 Good choice to minimize estrogen side effects like nausea, breast tenderness, etc. Good choice to minimize spotting and/or breakthrough bleeding.6
Cryselle-28 Low-Ogestrel-21 Low-Ogestrel-28 Lo/Ovral-28
Teva Watson Watson Wyeth
EE 30 mcg Norgestrel 0.3 mg Low estrogen; medium progestin; medium/high androgen.13, 14 Good choice to minimize estrogen side effects like nausea, breast tenderness, etc; and to minimize spotting and/or breakthrough bleeding.6
Junel 1.5/30 Junel Fe 1.5/30 Loestrin 1.5/30-21 Loestrin Fe 1.5/30 Microgestin 1.5/30 Microgestin Fe 1.5/30
Teva Teva Warner Chilcott Warner Chilcott Watson Watson
EE 30 mcg Norethindrone acetate 1.5 mg Low estrogen; high progestin; high androgen.13, 14 Good choice to minimize estrogen side effects like nausea, breast tenderness, etc.6
Apri Desogen Ortho-Cept Reclipsen Solia
Teva Organon Ortho Watson Prasco
EE 30 mcg Desogestrel 0.15 mg Low estrogen; high progestin; low androgen.13, 14 Increased risk of DVT with desogestrel over other progestins (controversial data).1 Good choice to minimize spotting and/or breakthrough bleeding; and to minimize androgenic effects. Has favorable lipid profile. 6

−This handout accompanies the related articles published in−
PHARMACIST’S LETTER / PRESCRIBER’S LETTER May 2012 ~ Volume 28 ~ Number 5
More. . . Copyright © 2012 by Therapeutic Research Center
Pharmacist’s Letter / Prescriber’s Letter ~ P.O. Box 8190, Stockton, CA 95208 ~ Phone: 209-472-2240 ~ Fax: 209-472-2249 www.pharmacistsletter.com ~ www.prescribersletter.com
following
PL CE LIVE May 2012
Long Guide
Pharmacist's Letter; July 2010; Vol: 26
Women's Health
Reps will promote a new oral contraceptive called Natazia (estradiol valerate/dienogest). They will point out that it's the first OC to contain estradiol instead of ethinyl estradiol, the synthetic estrogen in
most OCs. The hope is that estradiol will be better tolerated...but there's no proof that this is true. Natazia also contains a new progestin called dienogest. Dienogest has anti-androgenic effects like drospirenone (Yaz, etc)...but without the risk of hyperkalemia. Natazia has a unique four-phase dosing regimen...the estradiol dose steps down and dienogest dose steps up
during the cycle...to help avoid breakthrough bleeding. And instead of the usual 7-day hormone free interval, Natazia has 4 estrogen-only tabs plus 2 inert tabs. Tell women they MIGHT have less withdrawal bleeding with Natazia than with other OCs...due to the stepped
regimen and new progestin. Suggest starting with a generic monophasic OC (Levora, etc) for most women...especially if they want to skip
the placebo tabs to avoid periods. Save Natazia for women who need another option and might benefit from a more anti-androgenic pill. Use our new Comparison of Oral Contraceptives chart to identify similar products. Help your techs avoid med
errors by using our Technician Training Tutorial: Dispensing Oral Contraceptives.

More. . . Copyright © 2012 by Therapeutic Research Center
Pharmacist’s Letter / Prescriber’s Letter ~ P.O. Box 8190, Stockton, CA 95208 ~ Phone: 209-472-2240 ~ Fax: 209-472-2249 www.pharmacistsletter.com ~ www.prescribersletter.com
ALZHEIMER’S
You’ll hear more debate about whether cholinesterase inhibitors (donepezil,
etc) or memantine (Namenda) are beneficial for Alzheimer’s.
A cholinesterase inhibitor is often started for mild to moderate
Alzheimer’s...then memantine is added when a patient gets worse.
But these meds aren’t very effective...and new evidence suggests the combo
isn’t better than a cholinesterase inhibitor alone.
Only 1 in 12 patients on a cholinesterase inhibitor show any improvement.
Plus 1 in 12 patients have significant side effects...mostly GI problems, but
bradycardia and fainting are also possible.
Suggest a cholinesterase inhibitor first for mild to moderate Alzheimer’s
if the patient or family wants to try drug therapy.
Don’t suggest memantine for milder cases...it’s not beneficial.
Suggest switching to memantine for moderate to severe disease if a
cholinesterase inhibitor causes too many side effects. Memantine is often better
tolerated.
Think twice before recommending adding memantine to a cholinesterase
inhibitor when patients worsen. Memantine is not likely to add much
benefit...and it costs over $200 a month.
Discourage using Aricept 23 mg. It doesn’t work better than the 10 mg dose
to improve overall function...but it causes more GI effects.
Help set realistic expectations. Reinforce that drugs only turn back the
symptom clock a bit...the rate of cognitive and functional decline doesn’t
change. Explain that there’s not good evidence that dementia drugs delay nursing
home placement.
Suggest stopping drug therapy if there’s no detectable benefit by 3 to 6
months...side effects are a problem...or the patient is so severely affected
they’re bedridden, incontinent, nonverbal, etc.
Suggest tapering the drug over 4 weeks to reduce possible discontinuation
symptoms.
Emphasize nonpharmacologic interventions...maintaining a stable, low stress
environment...daytime engagement to maintain sleep-wake cycles...avoiding noise
and glare...and providing security objects.
To hear our experts discuss the appropriate use of drugs for Alzheimer’s,
go to our PL Detail-Document and listen to PL VOICES.
Go to the When and How to Use Drugs for Alzheimer's Disease Detail-Document.
DISCUSSION POINTS LEARN MORE ABOUT THIS POINT... (Just click on the link for access!)
How to manage Alzheimer’s May 2008 Article – whether dementia drugs are worth using October 2006 Article – what is useful to slow the progression of dementia due to Alzheimer's
Side effects of Alzheimer’s meds July 2009 Article – increased risk of slow heart rate and fainting in patients taking cholinesterase inhibitors

−This handout accompanies the related articles published in−
PHARMACIST’S LETTER / PRESCRIBER’S LETTER May 2012 ~ Volume 28 ~ Number 5
More. . . Copyright © 2012 by Therapeutic Research Center
Pharmacist’s Letter / Prescriber’s Letter ~ P.O. Box 8190, Stockton, CA 95208 ~ Phone: 209-472-2240 ~ Fax: 209-472-2249 www.pharmacistsletter.com ~ www.prescribersletter.com
following
PL CE LIVE May 2012
Long Guide
Pharmacist's Letter; May 2008; Vol: 24
Neurology / Psychiatry
There's controversy over whether dementia drugs are worth using. Lots of dementia patients are put on cholinesterase inhibitors or memantine in the hope of improving cognition
and functioning. But these drugs are only modestly effective...at best. Now the American College of Physicians and American Academy of Family Physicians are questioning their
routine use for dementia. Only 1 in 12 patients get any improvement with cholinesterase inhibitors...about the same number get adverse
effects. Ask whether therapy provides any meaningful improvement...and if it's worth the nausea, diarrhea, and other
side effects. Check that these patients are not taking meds that can make things worse. Drugs with anticholinergic effects
can increase the risk of cognitive impairment, falls, and delirium in older patients. Watch especially for older antihistamines (diphenhydramine, etc), drugs for overactive bladder (oxybutynin, etc),
tricyclics, and muscle relaxants (carisoprodol, etc). See our Detail-Document for our chart of drugs to avoid in patients with dementia...and suggestions for better
alternatives.

Cholinesterase Inhibitors for Dementia
Prepared for the subscribers of
Pharmacist’s Letter / Prescriber’s Letter to give to their patients. Copyright © 2009 by Therapeutic Research Center
www.pharmacistsletter.com ~ www.prescribersletter.com
What are cholinesterase inhibitors? Cholinesterase inhibitors are used to treat Alzheimer’s disease and other dementias. Cholinesterase inhibitors block the breakdown of a chemical in the brain called acetylcholine. Acetylcholine is involved in remembering things and thinking clearly. Examples of cholinesterase inhibitors are donepezil (Aricept) tablets; rivastigmine (Exelon) patches, capsules, and oral solution; and galantamine (Razadyne [U.S.], Reminyl [Canada]) capsules, tablets, and oral solution (U.S. only).
What kinds of benefits can I expect from cholinesterase inhibitors? Cholinesterase inhibitors are not a cure for dementia. But they may improve some symptoms or keep them from worsening. Cholinesterase inhibitors may somewhat improve thinking, memory, speech, interest, motivation, social interaction, self-care activities, or agitation. But most patients do not benefit. Only one in twelve patients improves with a cholinesterase inhibitor. There is no way to predict if or how a patient will respond to treatment with a cholinesterase inhibitor. And there is no way to know how long the benefit will last.
What are the side effects of cholinesterase inhibitors? One in twelve patients will experience a side effect from a cholinesterase inhibitor. Common side effects of the cholinesterase inhibitors include nausea, vomiting, and diarrhea. These side effects may improve over a few weeks. Starting with a low dose for several weeks and taking the cholinesterase inhibitor with food may reduce these side effects. A medication might be prescribed to treat nausea. Trying a different cholinesterase inhibitor or the rivastigmine patch may help. A more serious side effect of the cholinesterase inhibitors is slow heart rate, which can lead to falls and hip fracture.
What are some other things to consider? Some common medications can worsen dementia symptoms and decrease the effect of cholinesterase inhibitors. These include certain medications for depression, anxiety, pain, and urine incontinence, and muscle relaxants and antihistamines. Work with your prescriber and pharmacist to identify any such medications. It may be possible for your prescriber to substitute a similar medication that won’t affect your cholinesterase inhibitor. In making the decision to try a cholinesterase inhibitor, consider potential benefit, potential side effects, cost, quality of life, and treatment goals. For example, if quality of life is poor, treatment may not be a good goal, especially if side effects occur. Discuss treatment goals with your prescriber, and write them down for future reference.
How long should treatment with a cholinesterase inhibitor be continued? Benefits should be seen within three to six months. If benefit is seen, the cholinesterase inhibitor can be continued until it seems to no longer be helping, or the side effects outweigh the benefits.
Where can I get more information about dementia and caring for a patient with dementia? Multiple resources are available in both the U.S. and Canada. Examples include The Alzheimer’s Association (U.S.) (www.alz.org or 1-800-272-3900) and Alzheimer Society (Canada) (www.alzheimer.ca or 1-800-616-8816).
More. . . Copyright © 2012 by Therapeutic Research Center
Pharmacist’s Letter / Prescriber’s Letter ~ P.O. Box 8190, Stockton, CA 95208 ~ Phone: 209-472-2240 ~ Fax: 209-472-2249 www.pharmacistsletter.com ~ www.prescribersletter.com
STATINS
Statin patients will get fewer liver function tests.
Patients often get liver enzymes checked when starting a statin...with dose
increases...and then once or twice a year. This routine monitoring costs over $3
billion/yr...and is NOT helpful. Point out that new labeling NO longer recommends
routine monitoring during therapy.
Statins can increase liver enzymes...but it’s usually transient.
Any serious liver injury due to statins is idiosyncratic...and therefore
isn’t picked up with routine monitoring.
And liver failure itself is very rare...if it happens at all.
There’s only about one case of liver failure for every million patients per
year on a statin...the same as for people not on a statin.
Tell patients the new recommendation is to check liver enzymes BEFORE
starting a statin...and then only if they have symptoms, such as unexplained
nausea, abdominal pain, or jaundice.
Explain that statins are okay in patients with elevated liver enzymes due to
CHRONIC, stable liver disease...especially nonalcoholic fatty liver disease. In
this case, statins may actually LOWER liver enzymes...possibly by decreasing
inflammation.
On the other hand, recommend avoiding statins in patients with ACUTE liver
failure or decompensated cirrhosis.
To hear a great discussion about why routine monitoring isn’t helpful...and
whether it’s ever necessary to stop a statin due to high liver enzymes...go to our
PL Detail-Document for our PL VOICES segment.
Also see our updated PL Chart, Characteristics of the Various Statins, for
lipid lowering, monitoring, renal dosing, etc.
Go to the When to Monitor Liver Enzymes for Patients Taking Statins Detail-
Document.
DISCUSSION POINTS LEARN MORE ABOUT THIS POINT... (Just click on the link for access!)
Whether statins cause liver toxicity January 2011 Article – whether it's okay for patients with elevated liver enzymes to take a statin Detail-Doc 280405 – Update on Statin Risks
Which labs to monitor in patients taking statins Detail-Doc 260704 – Recommended Lab Monitoring for Common Medications Detail-Doc 280502 – Characteristics of the Various Statins

More. . . Copyright © 2012 by Therapeutic Research Center
P.O. Box 8190, Stockton, CA 95208 ~ Phone: 209-472-2240 ~ Fax: 209-472-2249 www.pharmacistsletter.com ~ www.prescribersletter.com ~ www.pharmacytechniciansletter.com
PL Detail-Document #280405 −This PL Detail-Document gives subscribers
additional insight related to the Recommendations published in− PHARMACIST’S LETTER / PRESCRIBER’S LETTER
April 2012
Update on Statin Risks
The U.S. Food and Drug Administration (FDA) has approved important safety label changes for the class of cholesterol-lowering drugs known as statins. These changes were made to provide the public with more information for the safe and effective use of statins and are based on FDA’s comprehensive review of the statin class of drugs (see Data Summary below). The changes include the following:
Monitoring Liver Enzymes
Labels have been revised to remove the need for routine periodic monitoring of liver enzymes in patients taking statins. The labels now recommend that liver enzyme tests should be performed before starting statin therapy and as clinically indicated thereafter. FDA has concluded that serious liver injury with statins is rare and unpredictable in individual patients, and that routine periodic monitoring of liver enzymes does not appear to be effective in detecting or preventing serious liver injury. Adverse Event Information
Information about the potential for generally non-serious and reversible cognitive side effects (memory loss, confusion, etc) and reports of increased blood sugar and glycosylated hemoglobin (A1C) levels has been added to the statin labels. FDA continues to believe that the cardiovascular benefits of statins outweigh these small increased risks.
Drug Interactions
The [U.S.] lovastatin label has been extensively updated with new contraindications (situations when the drug should not be used) and dose limitations when it is taken with certain medicines that can increase the risk for muscle injury.
Health care professionals should refer to the drug labels for the latest recommendations for prescribing statins (also see Additional
Information for Health Care Professionals below). Patients should contact their health care professional if they have any questions or concerns about statins. Additional Information for Patients • The statin drug labels have been revised to
provide patients with more information on the safe and effective use of statins. Patients should be aware of the following information: 1. There have been rare reports of serious
liver problems in patients taking statins. Patients should notify their health care professional right away if they have the following symptoms: unusual fatigue or weakness; loss of appetite; upper belly pain; dark-colored urine; or yellowing of the skin or the whites of the eyes.
2. Memory loss and confusion have been reported with statin use. These reported events were generally not serious and went away once the drug was no longer being taken.
3. Increases in blood sugar levels have been reported with statin use.
4. Certain medicines should never be taken (are contraindicated) with lovastatin (Mevacor).
• Patients should contact their health care professional if they have any questions or concerns about statins.
Additional Information for Health Care Professionals • Health care professionals should perform liver
enzyme tests before initiating statin therapy in patients and as clinically indicated thereafter. If serious liver injury with clinical symptoms and/or hyperbilirubinemia or jaundice occurs during treatment, therapy should be interrupted. If an alternate etiology is not found, the statin should not be restarted.
Detail-Document #260704
−This Detail-Document accompanies the related article published in−
PHARMACIST’S LETTER / PRESCRIBER’S LETTER July 2010 ~ Volume 26 ~ Number 260704
More. . . Copyright © 2010 by Therapeutic Research Center
Pharmacist’s Letter / Prescriber’s Letter ~ P.O. Box 8190, Stockton, CA 95208 ~ Phone: 209-472-2240 ~ Fax: 209-472-2249 www.pharmacistsletter.com ~ www.prescribersletter.com
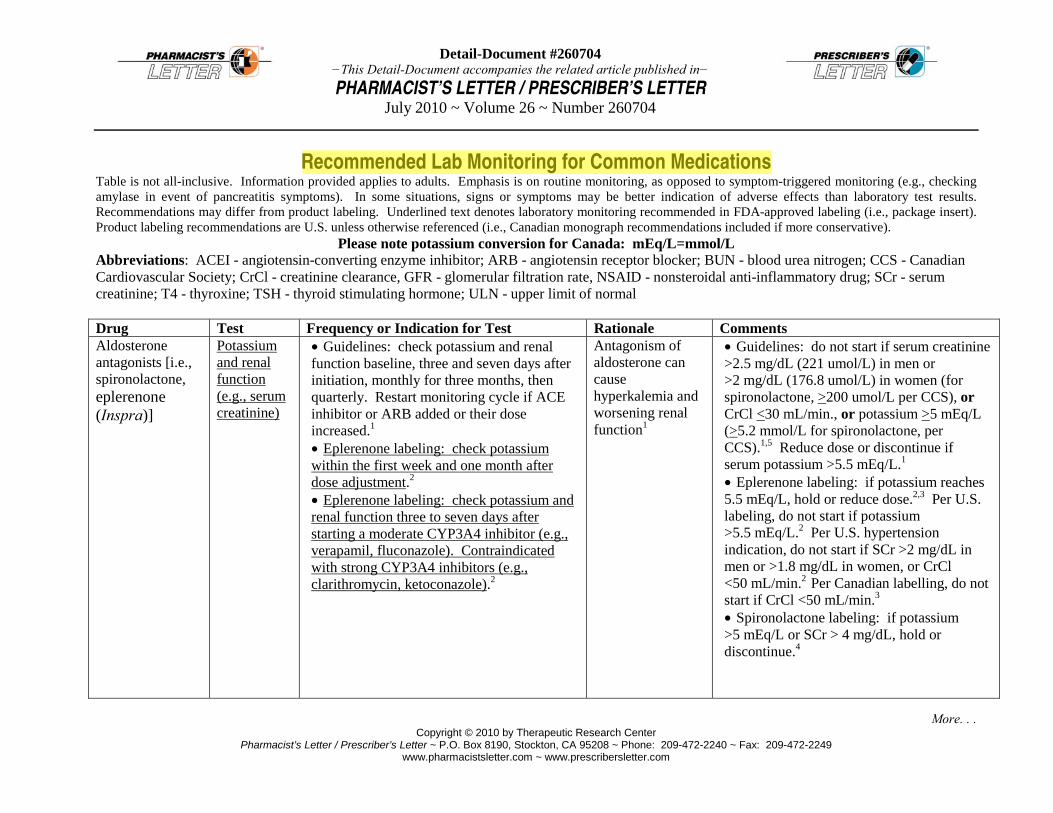
Recommended Lab Monitoring for Common Medications Table is not all-inclusive. Information provided applies to adults. Emphasis is on routine monitoring, as opposed to symptom-triggered monitoring (e.g., checking amylase in event of pancreatitis symptoms). In some situations, signs or symptoms may be better indication of adverse effects than laboratory test results. Recommendations may differ from product labeling. Underlined text denotes laboratory monitoring recommended in FDA-approved labeling (i.e., package insert). Product labeling recommendations are U.S. unless otherwise referenced (i.e., Canadian monograph recommendations included if more conservative).
Please note potassium conversion for Canada: mEq/L=mmol/L Abbreviations: ACEI - angiotensin-converting enzyme inhibitor; ARB - angiotensin receptor blocker; BUN - blood urea nitrogen; CCS - Canadian Cardiovascular Society; CrCl - creatinine clearance, GFR - glomerular filtration rate, NSAID - nonsteroidal anti-inflammatory drug; SCr - serum creatinine; T4 - thyroxine; TSH - thyroid stimulating hormone; ULN - upper limit of normal Drug Test Frequency or Indication for Test Rationale Comments Aldosterone antagonists [i.e., spironolactone, eplerenone (Inspra)]
Potassium and renal function (e.g., serum creatinine)
• Guidelines: check potassium and renal function baseline, three and seven days after initiation, monthly for three months, then quarterly. Restart monitoring cycle if ACE inhibitor or ARB added or their dose increased.1 • Eplerenone labeling: check potassium within the first week and one month after dose adjustment.2 • Eplerenone labeling: check potassium and renal function three to seven days after starting a moderate CYP3A4 inhibitor (e.g., verapamil, fluconazole). Contraindicated with strong CYP3A4 inhibitors (e.g., clarithromycin, ketoconazole).2
Antagonism of aldosterone can cause hyperkalemia and worsening renal function1
• Guidelines: do not start if serum creatinine >2.5 mg/dL (221 umol/L) in men or >2 mg/dL (176.8 umol/L) in women (for spironolactone, >200 umol/L per CCS), or CrCl <30 mL/min., or potassium >5 mEq/L (>5.2 mmol/L for spironolactone, per CCS).1,5 Reduce dose or discontinue if serum potassium >5.5 mEq/L.1 • Eplerenone labeling: if potassium reaches 5.5 mEq/L, hold or reduce dose.2,3 Per U.S. labeling, do not start if potassium >5.5 mEq/L.2 Per U.S. hypertension indication, do not start if SCr >2 mg/dL in men or >1.8 mg/dL in women, or CrCl <50 mL/min.2 Per Canadian labelling, do not start if CrCl <50 mL/min.3 • Spironolactone labeling: if potassium >5 mEq/L or SCr > 4 mg/dL, hold or discontinue.4

Copyright © 2012 by Therapeutic Research Center
Pharmacist’s Letter / Prescriber’s Letter ~ P.O. Box 8190, Stockton, CA 95208 ~ Phone: 209-472-2240 ~ Fax: 209-472-2249 www.pharmacistsletter.com ~ www.prescribersletter.com
INSOMNIA
Reps will promote Intermezzo (in-ter-MET-zoe), a new low-dose zolpidem
for middle-of-the-night awakening.
You’ll hear it’s the first drug approved for middle-of-the-night
awakening...but zaleplon (Sonata) is already used this way. Both are short-
acting and last about 4 hours.
Intermezzo will cost about $220 for 30 sublingual tablets...compared to
about $20 for generic zaleplon.
Watch for gender-specific dosing for Intermezzo.
Recommend Intermezzo 3.5 mg for men...and 1.75 mg for women, seniors, and
patients with hepatic impairment.
Women and seniors metabolize zolpidem more slowly than younger men...so
the lower dose helps ensure that the drug won’t last too long.
Also use the lower dose for patients who use CNS depressants...opioids,
tricyclics, or alcohol.
Caution patients not to take Intermezzo unless they have at least 4 hours
before they need to get up.
Advise them NOT to use Intermezzo if they used another hypnotic earlier
in the night. Suggest regular zolpidem (Ambien, etc) or eszopiclone (Lunesta)
if needed for both sleep onset and maintenance.
Discourage overuse of sleeping pills. Explain that cognitive and
behavioral therapy is the best bet for long-term improvement...without the risk
of cognitive or physical impairment.
To hear a fascinating, and sometimes heated, debate about the
safety of sleep meds, go to our PL Detail-Document and click on PL VOICES.
Feel free to use our PL Patient Education Handout, Strategies for a Good
Night’s Sleep. If meds are needed, see our PL Chart, Comparison of Insomnia
Treatments, for onset, duration, and more.