placement of fiber prefabricated or custom made posts affects the 3
TRANSCRIPT

Placement of fiber prefabricated or custom made posts affects the 3-yearsurvival of endodontically treated premolarsMARIA CRYSANTICAGIDIACO,MD,DDS,PHD, FRANKLINGARCIA-GODOY,DDS,MS,ALESSANDROVICHI, DDS,PHD,SIMONEGRANDINI,DDS,MS,PHD,CECILIA GORACCI, DDS,MS,PHD& MARCO FERRARI, MD,DDS,PHD
ABSTRACT:Purpose: To assess whether the amount of residual coronal dentin and the placement of a prefabricated (DTLight Post)(LP) or a customized fiber post (Ever Stick Post)(ES) have a significant influence on the 3-year survival ofendodontically treated premolars. Methods: A sample of 345 patients provided six groups of 60 premolars in need ofendodontic treatment. Groups were defined based on the amount of dentin left at the coronal level after endodontic treatmentand before abutment build-up. Within each group teeth were randomly divided into three subgroups (n=20). In Subgroup A,no root canal retention was provided for the coronal restoration. In Subgroups Band C, LP and ES, respectively, were placedinside the root canal. All the teeth were finally restored with a single unit metal-ceramic crown. Results: Data were notaffected by any loss to follow-up. The overall 36-month survival rate of crowned endodontically treated premolars was76.7%. The lowest survival rate was recorded for teeth restored without any root canal retention (62.5%). Teeth restoredwith LP had a survival rate higher (90.9%) than those restored with ES (76.7%). The Cox regression analysis showed thatthe presence of root canal retention was a significant factor for survival (P< 0.05). The decrease in failure risk was higher inteeth restored with LP (HR= 0.1; 95% CI for HR= 0.09 to 0.34; P< 0.001) than when using ES (HR= 0.5; 95% CI for HR=0.3 to' 0.7; P= 0.003). Teeth retaining one (HR= 0.3; 95% CI for HR= 0.2 to 0.7; P= 0.003), two (HR= 0.2; 95% CI for HR=0.1 to 0.5; P< 0.001), or three coronal walls (HR= 0.1; 95% CI for HR= 0.05 to 0.3; P< 0.001) had a significantly lowerfailure risk than teeth deprived even of the ferrule effect. Similar failure risks existed for teeth missing all the coronal wallsregardless of the presence or absence of a ferrule effect (P> 0.05). Interaction terms were not significant (P> 0.05). Postplacement and the amount of residual coronal dentin affected the 3-year survival of endodontically treated premolars. (Am JDent 2008;21: 179-184).
CLINICALSIGNIFICANCE:To obtain the highest success rate, endodontically treated premolar~; sh'auld be restored with afiber post and a complete crown. The "ferrule" structure has a direct influence on the clinical success rate.
18J: Prof. Dr. Marco Ferr~, Department of Oral Sciences, Policlinico Le Scotte, Viale Bracci, Siena 53100, Italy. E-I8J:[email protected] \ ,.
A new approach to the restoration of endodontically treatedteeth has been prompted by the introduction of fiber-reinforcedcomposite (FRC) posts. 1,2With an elastic behavior more closelyresembling that of dentin, fiber posts have limited the occur-rence of irreparable root fractures as compared with metallicpostS?-5 Moreover, higher fracture resistance and more favor-able failure patterns were reported in vitro for teeth restored withFRC posts than in the absence of any root canal retention.2.6-8
The survival of root treated teeth has been assessed inseveral retrospectivel,9-11 and prospective12-18 clinical studies.Failure rates ranging from the 8% of carbon fiber posts dver an8-year observation period irr'a retrospective study,IJto tile 12%of glass fiber posts -iI!-a 2-year prospective investigationl6 havebeen recorded. Differences in study design, inclusion criteria,number of observed patients, and observation periods may haveaccounted for dissimilarities in the results.
Variables such as tooth tYpe and position within the dentalarch in relation to the occlusal forces,16,17 the presence ofproximal contacts,19 and the type of the final restoration20 hasbeen found to have an effect on the longevity of root treatedteeth. Additionally, the amount of coronal residual structure hasbeen recognized as critical to the survival probability of pulplessteeth. 10,15-18In particular, the contribution to mechanicalproperties of preserving a 2 mm high dentin collar, the so-called"ferrule effect", has been emphasized.21.24
Recently, as an alternative to metallic and prefabricated fiber
posts, FRC materials have been proposed for constructingcustom made postS?5-3o The fiber bundles can be adapteddirectly into the post space, so as to obtain a customized post,
hi h· h dh' 1 1 d S l' . 253132 d'w C IS t en a eSlve y ute. evera zn Vitro " stu leshave investigated the mechanical properties and indications ofthese FRC materials.
However, no clinical study has so far assessed whether teethrestored with such custom-made posts have a significantlydifferent clinical outcome in comparison with teeth restored withFRC prefabricated posts or without any root canal retention.
Therefore, the present study prospectively evaluated the 3-year clinical behavior of root-treated premolars with varyingdegrees of coronal tissue loss that were restored with DT Lightposta posts, EverStickb fibers or without any root canal retention.All the teeth were fmally covered with a prosthetic crown. Thetested null hypothesis was that neither the amount of residualcoronal dentin nor the placement of a prefabricated or custom-ized FRC post in the root canal significantly affected the 3-yearsurvival of endodontically treated and crowned premolars.
Materials and MethodsA total of 345 patients who consecutively presented at a
private dental office for receiving endodontic treatment andrestoration of premolars provided six groups of 40 teeth each.No more than two teeth per patient were considered for thestudy. Informed written consent was obtained from the patientsafter they had received clear explanation of the purpose of thetrial, according to a protocol preliminarily approved by the

Instrument the root canals with K-files (#08-10-15)and Flexmaster (#15-20-25-30-35-40 VDW),mounted on an electric handpiece (Endo ITprofessional), having established the workinglength at I mm above the radiographic apex.
Condense the gutta-percha using the continuous wave technique up to 4 to 5 mm fromthe apex with a System B heat source 5 mm from the apex with a System B heat source
In between instrumentations irrigate with 3 mL of 5.25%sodium hypochlorite using a long 27-gauge needle.
Use deionized water as the final rinse, and maintainpatency of the c:tn~l with a # 10 K-file.
Subgroup BApply Caulk 34% Tooth Conditioner Gelto the post space.After 15 seconds, rinse with water.Remove the excess water with an air blast.With paper points remove the residualmoisture without desiccating the etcheddentin surface.
Subgroup CApply Bisco 37% phosphoric gel to the postspace. After 15 seconds rinse with water.Remove the excess water with an air bla,st'.-With paper points remove the residualmoisture without desiccating the etcned dentinsurface. "
Mix I or 2 drops of Prime&Bond NTadhesive with the same amount ofSelf-Cure Activator for 1-2 secondswith a clean brush tip.Apply the adhesive/activator solution to thepost space with a microbrush. After 20seconds, remove the excess solution from thepost space with an air blast and paper points.
Coat the post surface with a layer of adhesive/activator solution and gently air-dry for 5seconds. If the post surface does not appearuniformly shiny, apply a second layer andgently air-dry again.
Apply Primer B with a microbrush. After 20seconds, remove the excess solution from theFost space with an air blast and paper points.Apply the unfilled resin with a microbrush andthen air dry and remove the excess with a cleanpaper point.
Mix equal amounts of Calibra base catalyst.Apply the mixture onto the post surface with aspatula and into the post space with a lentulo spiral.Seat the post and remove the excess cement.Light-cure through the post for 10 seconds with ahigh power LED curing light (SmartLite PS).
Mix equal amounts of BisCore base and catalystApply the mixture onto the post surface with aspatula and into the post space with a lentulo spiral.Seat the post and remove the excess cement.Leave the luting material undisturbed for 5 minutes.
Institutional Review Board of the University of Siena, Italy.Patients' ages ranged from 18-76 years, with an average of 58years. The selected teeth needed to be in occlusal function with anatural tooth and in interproximal contact with two adjacentnatural teeth. If the teeth had already been endodonticallytreated, the inclusion criteria of symptom-free root canal fillingand a minimum apical seal of 4 mm, without any periapicallesion on the X-ray, had to be met by the tooth to be restored.Clinical procedures were performed by the same operator.Groups were defined as follows, based on the amount of dentinleft at the coronal level after endodontic treatment and beforeabutment preparation: .. ,.' ,-
Group 1. All the EClronalwalls were present (Fig. 1A);
Group 2. Three coronal walls were retained (Fig. IE);Group 3. Two coronal walls were preserved (Fig. 1C);Group 4. Only one coronal wall was left intact (Fig. lD);
Group 5. Ferrule effect: no coronal wall was retained, although acollar of dentin at least 2 mm in height, as measured with aperiodontal probe, was preserved circumferentially;Group 6. No ferrule effect: no coronal wall was retained, andless than 2 mm of dentin was present circumferentially.
Within each group three equally sized subgroups (n=20)were randomly formed:
Subgroup A. No root canal post was placed;
Fig. I. Schematic representations of the varying degrees of hard tissue loss thatthe tested premolars may exhibit at completion of endodontic treatment. Thedarker area represents the missing structure in the conditions referred to as A.four coronal walls retained, B. three walls left, C. two walls maintained, D. onlyone coronal wall preserved.

No Post DT Light Post Stick Tech fibers TotalResidual coronal dentin (Subgroup A) (Subgroup B) (Subgroup C) (per group)
Group I. Four coronal walls 0/20 0/20 0/20 0/60
Group 2. Three coronal walls 4/20 (20%) 0/20 2/20 (10%) 6/60 (10%)
Group 3. Two coronal walls 7/20 (35%) 0120 4120 (20%) 11/60 (18.3%)Group 4. One coronal wall 8/20 (40%) 1/20 (5%) 6120 (30%) 15/60 (25%)
Grou p 5. Ferrule effect 12/20 (60%) 4/20 (20%) 7/20 (35%) 23/60 (38.3%)
Group 6. No ferrule 14/20 (70%) 6/20 (30%) 9/20 (45%) 29/60 (48.3%)
Total (per SUbgr9~) 45/120 (37.5%) 11/120 (9.1%) 28/120 (23.3%) Grand Total 84/360 (23.3%)
Subgroup B. DT Light Posts were used to provide retention tothe coronal restorations;
Subgroup C. EverStick fibers were adapted into the post spaceto obtain a customized FRC post.
For all the teeth the final restoration was a single unit metal-ceramic crown.
Clinical procedures - Tables 1 and 2 respectively summarize theprocedures for root canal treatment and post luting.
In the teeth to be restored with a post (Subgroups Band q,at least 24 hours after endodontic treatment, the gutta-perchawas removed with Gates Glidden drillsc for a length of 7-8 mm,leaving at least 4 mm of intact apical seal.
For the DT Light Posts, the size (1, 2, or 3) that best fit thedowel space was chosen. The post was tried-in and consequentlyshortened with a diamond bur.
Prime&Bond NT Dual Cure':.adhes-i:vesystem was used incombination with the dual-cur~ resin cement Calibrac followingmanufacturer's instructions. The abutment portiOifwas built upusing XFlowc flowable composite and CerarnXc microhybridcomposite.
EverStick fiber bundles were adapted into the dowel space,cured, removed from the root as per manufacturer's instruc-tions.29 The custom-made posts were then adhesively luted withAll Bond 2 and Bis-Core.d Bis-Core was also used for abutmentbuild-up. The crown preparation varied from a full chamfer witha bevel interproximally and lingually, to a feather finish, de-pending on the height and thickness of the remaining dentin.Single unit porcelain fused-to-metal crowns were fabricated.
Evaluation parameters - Patients were recalled after 1,6, 12 and24 months for clinical and radiographic examinations. Periapicalradiographs were taken.,with modified parallel. technique andUltra-Speed fIlms,· and examined at x5 magnification. Thefollowing events:::""wereconsidered as failures: post debonding,post fracture, vertical or horizontal root fracture, failure of thecore portion requiring a new coronal restoration, displacementof the crown, endodontic and periradicular conditions requiringendodontic retreatment. Evaluation of success or failure wasindependently performed by two examiners other than theoperator.
Statistical analysis - For descriptive purposes, Kaplan-Meierplots were constructed by subgroup (Fig. 2A), and by subgroupwithin each group (Fig. 2B-F).
The Cox regression analysis was applied in order to assessthe influence on failure rate of the type of restoration (no post!DT Light PostlEverStick Post), the amount of residual coronal
dentin, and the interaction between the two variables. The levelof significance was set at P< 0.05.
ResultsTable 3 reports frequencies and percentages of the failures
occurred over the 36-month observation period. Data were notaffected by any loss to follow-up. The overall 36-month survivalrate of crowned endodontically treated premolars was 76.7%.The lowest survival rate was recorded for teeth restored withoutany root canal retention (Subgroup A, 62.5%). Teeth restoredwith DT Light Posts (Subgroup B) had a 3-year survival ratehigher (90.9%) than those restored with EverStick fibers(Subgroup C, 76.7%).
In the presence of a post, no root fracture or failure of theabutment portion was recorded; all the failure events were due topost debonding, and occurred in teeth that presented with areduced amount of residual dentin, with one wall at the mostremaining at the coronal level.
For the sample teeth restored without a post, 13 rootfractures and 32 crown displacements were observed. WhenEveryStick fibers were used, dislodgement of the crown androot fractures were the reasons for failures. The majority ofcrown dislodgements and all the root fractures occurred in teethwhere the remaining coronal structure before abutment build-upwas reduced to one or two residual walls at the most. All theteeth that exhibited four walls at the end of endodontic treatmentsurvived the 3 years of clinical service, regardless of therestorative procedure including or omitting the placement of apost (Table 2).
For all of the premolars that experienced post debonding, thepost was luted again and the teeth were maintained in clinicalservice. As for the cases of failed endodontic treatment, all theteeth presented with asymptomatic periapical lesions. Endodon-tic retreatment was performed and the teeth were restored toclinical service. All the root fractures but three were fatalfailures. Thus, in cases of no ferrule structure remained, througha periodontal surgery intervention (crown lengthening), fiberpost insertion and placement of new crowns, it was possible tobring the tooth back to function. Conversely, all the otherfractured roots had to be extracted.
The Cox regression analysis (limited to Groups 2-6), showedthat with the exclusion of teeth retaining four intact walls, allsurvived related to the restorative procedure. The model showedthat the presence of root canal retention was a significant factorfor survival (P< 0.05).
The decrease in failure risk was higher in teeth restored withprefabricated posts (hazard ratio, HR= 0.1; 95% CI for HR= 0.09
@ No ferrule1,0 ... ®+
I .. 1,0 :to'-___+ t + I
,8 +,8
+
+,8 - -
DTUQht Post ,6 OT Light Post
1ii +OT Light Post-eensored + +OT Light Post-censored
> ,4 -- Iii -'~
o Ever Stick post > ,4o Bier Stick post::J 0 '2:Vl ~
Q) + Ever Stick post :J> (/) + Bier Stick post
~ ,2 -censored Q)
~ > ,2 -censored
E oNo post ~::J :5 oNo postU
+No post-eensored E0,0 :J
0 6 12 18 24 30 36 () 0,0 +No post-censored
0 6 12 18 24 30 36Months
Months
F~rrule effect 1 coronal wall© 1,0 r+ @ 1,0
~+ •I I
+ 1 +,8 ,8 +
++
- ,6 -or Light Post,6 +
OT Light Post ~; ,-+OT Light Post-censored +OT Light Post-censored
Iii - Iii ->> 4 o Bier Stick post '2: ,4o Bier Stick post'2: . .' - :J:J
+ Evel'Stick post(/) + Bier Stick post(/)Q)
Q) .::: -censored,~ 2 -censored ,2ro '0' ro~ ,
aNa post :5 oNo post
E I E:J :J + No post-censored() 0 +No post-censored () 0,0
0 6 12 18 24 30 36 0 6 12 18 24 30 36
Months Months
®2 coronal walls 3 coronal walls
1,0 r+ CD...I 1 1,00 0+ + + I I
+I + +
,8 + +,80
-.6 OT Light Post -,60 OT Light Post, + OT Light Post~ns;orel!.
Iii - + OT Light Post-censored> 4 o Ever Stick post'2: Iii -:J
.. > 40 o Bier Stick post(/) + Ever Stick post '2:Q) :J.~ 2 -censored (/) ,. Bier Stick post
ro Q)
:5 o No post > 20 -censored
E.. ~
:J -INo post-censored :5 o No post() 0 E
0 6 12 18 24 30 36 :J 00 + No post-censored()
Months0 6 12 18 24 30 36
. ' "
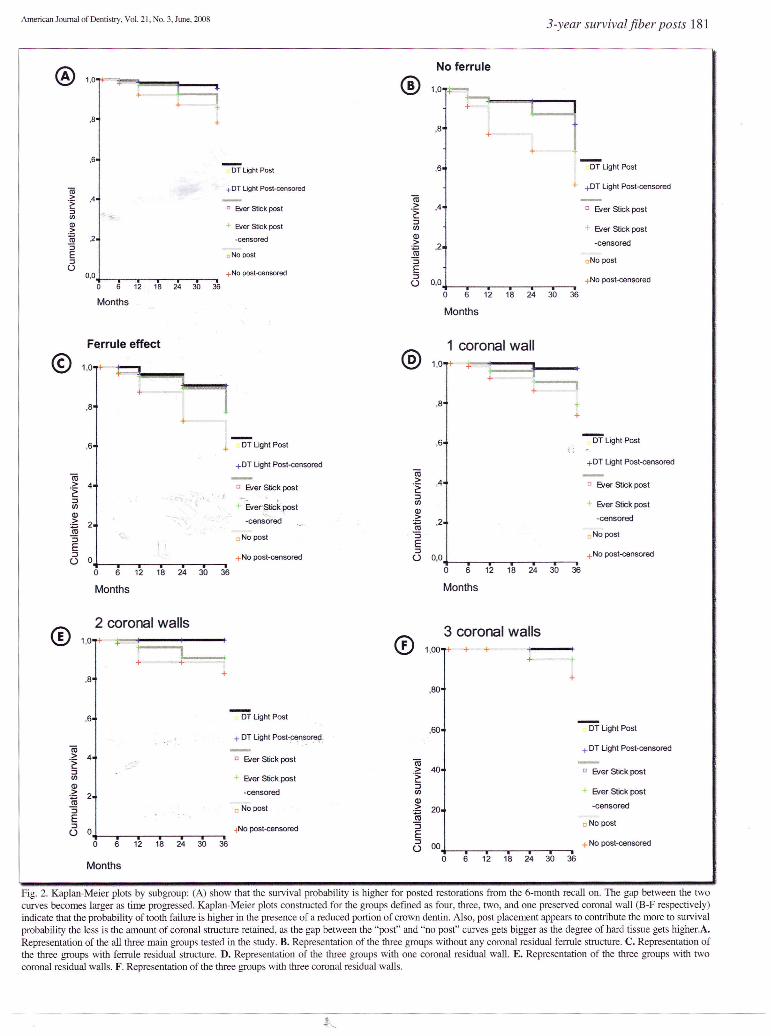
Fig. 2. Kaplan-Meier plots by subgroup: (A) show that the survival probability is higher for posted restorations from the 6-month recall on. The gap between the twocurves becomes larger as time progressed. Kaplan-Meier plots constructed for the groups defmed as four, three, two, and one preserved coronal wall (B-F respectively)indicate that the probability of tooth failure is higher in the presence of a reduced portion of crown dentin. Also, post placement appears to contribute the more to survivalprobability the less is the amount of coronal structure retained, as the gap between the "post" and "no post" curves gets bigger as the degree of hard tissue gets higher.A.Representation of the all three main groups tested in the study. B. Representation of the three groups without any coronal residual ferrule structure. C. Representation ofthe three groups with ferrule residual structure. D. Representation of the three groups with one coronal residual wall. E. Representation of the three groups with twocoronal residual walls. F. Representation of the three groups with three coronal residual walls.

to 0.34; P< 0.001) than when using customized posts (HR= 0.5;95% CI for HR= 0.3 to 0.7; P= 0.003). Teeth retaining one(HR=O.3; 95% CI for HR= 0.2 to 0.7; P= 0.003), two (HR=O.2;95% CI for HR= 0.1 to 0.5; P< 0.001), or three coronal walls(HR= 0.1; 95% CI for HR= 0.05 to 0.3; P< 0.001) had asignificantly lower failure risk than teeth deprived even of theferrule effect. Similar failure risks existed for teeth missing all thecoronal walls regardless of the presence or absence of a ferruleeffect (P> 0.05). Interaction terms were not significant (P> 0.05).
Discussion
Following the protocol of a previous 2-year prospectiveclinical trial,33 the study was designed to verify whether thedegree of coronal tissue loss and the placement of a root canalpost or a custom post had an influence on failure-free time ofroot treated teeth. To this purpose, a point was made ofstandardizing as much as possible other v~ables that can affectthe clinical service, such as tooth type and function in the dentalarch (only premolars with natural teeth as adjacent andantagonist elements), as well as type of the final restoration(single unit porcelain metal crowns).
The restorative procedure that yielded the greatest survivalprobability was the placement of the prefabricated fiber post(DT Light Post). Specifically with Light Posts, a reduced proba-bility of crown dislodgement was noticed and the occurrence ofroot fractures was prevented over the 3-year observation period.Also, the fracture resistance of these posts stood the test ofclinical service, as no such failure was reported. As a matter offact, for this type of fiber post a relatively~higJ;ffatigue resistancehad previously been recordec\ in vitro,34 in;·cornparison withother posts that also performed less satisfactorily clinlcally.16
Also Ever Stick fiberS contributed to prolong the failure-freetime of endodontically treated premolars, in comparison withteeth restored without any root canal retention. Nevertheless, theprotective role of Ever Stick fibers was less effective than that ofDT Light Posts, showing a higher percentage of failures.
A possible explanation for the more convincing clinical out-come of DT Light Posts may reside in the superior mechanicalproperties of this prefabricated post. Although Light Post andEver Stick posts have never been directly compared before, inprevious fatigue and fracture resistance studies34,35Light Postsoutperformed another prefabricated post (Parapost FiberWhite\ that, according to Fokkinga et al,2 exhibited a fracturebehavior similar to EverS.tick fibers. To the impr()ve!Jlent inmechanical properties of Light Posts, the manufacturilig· step offiber pre-stressing may have contributed. This procedure, whichis unique to this type of post, involves soaking in the resin fibersthat are pre-stressed in tension. On the final cure of the resin, thetension in the fibers is. released and, consequently, the resinsurface is left under compression, enabling the post to favorablyabsorb tensile stress during function.
Concerning the role of residual coronal dentin, indicationscan be found in the literature that the survival of restoredpulpless premolars is greatly affected by the amount of crownstructure preserved.16,17,21-24,33The present study's fmdings areconfirmatory in this regard. All failures such as post debondingand fractures of non-posted roots occurred with those havingonly one wall or less coronal structure. Particularly, the loss ofany ferrule effect appeared to place the restored tooth under a
statistically significant higher risk of failure than when one ormore coronal walls were retained.
Moreover, Kaplan-Meier plots suggested the contribution ofpost placement to tooth survival to become more effective withtime and with decreasing amounts of preserved crown structure(Fig. 2B). Nevertheless, between factor interactions were notsignificant according to the Cox model. An alternative ex-planation for this lack of significance may reside in therelatively low overall failure rate of restored root filledpremolars. Collection of longer-term data is still being pursuedwith the expectation of further strengthening the evidence so farprovided regarding the role of the ferrule. Also, the outcome ofother tooth types should be evaluated under the same experi-mental conditions. The limitation of the present study to pre-molars only, although justified by the need for standardization,inevitably affects the external validity of the findings.
Concerning the failures of endodontic treatment, in all thecases they were accompanied by a loss of the seal due to crowndislodgement or post debonding, possibly leading to root canalreinfection.36,37
In conclusion, over a 3-year observation period, the place-ment of prefabricated or customized posts was shown to providea significant contribution to the survival of pulpless restoredpremolars. This contribution was more effective for DT LightPosts than for Ever Stick posts. Irrespective of the restorativeprocedure, preservation of at least one coronal wall significantlyreduced the failure risk. Longer-term data are expected to furtherstrengthen the evidence regarding the protective role of thedentin ferrule.
a. RTD, St Egreve, France.b. Stick Tech Ltd, Turku, Finland.c. Denstply Ltd, Kostanz, Germany.d. Bisco, Schaumburg, IL, USAe Eastman Kodak Co., Rochester, NY, USA.f ColtenelWhaiedent Inc., Altstiitten, Switzerland.
Dr. Cagidiaco, Dr. Vichi, Dr. Grandini, and Dr. Goracci are Assistant Professors,and Dr. Ferrari is Professor and Dean, School of Dental Medicine, University ofSiena, Italy. Dr. Franklin Garcia-Godoy is Professor and Associate Dean forResearch, Director, Bioscience Research Center, College of Dental Medicine,Nova Southeastern University, Fort Lauderdale, Florida, and Senior ClinicalInvestigator, The Forsyth Institute, Boston, Massachuseus, USA.
I. Ferrari M, Vichi A, Garcia-Godoy F. Clinical evaluation of fiber-reinforcedepoxy resin posts and cast post and cores Am J Dent 2000;23(Sp ls)15B-18B.
2. Fokkinga WA, Le Bell AN!, Kreulen CM, Lassila LV, Vallittu PK,Creugers NH. Ex vivo fracture resistance of direct resin compositecomplete crowns with and without posts on maxillary premolars. IntEndod J 2005;38:230-237.
3. Akkayan B, Gulmez T. Resistance to fracture of endodontically treated teethrestored with different post systems. J Prosthet Dent 2002;87:431-437.
4. Schwartz RS, Robbins JW. Post placement and restoration of endodonticallytreated teeth: A literature review. J Endod 2004;30:289-30 I.
5. Le Bell A-M, Lassila LVl, Kangasniemi I, Vallittu P. Bonding of fibre-reinforced composite post to root canal dentin. J Dent 2005;33:533-539.
6. Salameh Z, Sorrentino R, Papacchini F, Ounsi HF, Tashkandi E, Goracci C,Ferrari M. Effect of fiber post and resin core restorations on fractureresistance and pattern of endodontically treated mandibular molars. J Endod2006;32:752-755.
7. Sorrentino R, Monticelli F, Goracci C, Zarone F, Tay FR, Ferrari M.Effect of post and core restorations on the resistance to fracture ofendodontically treated maxillary premolars in different restorative sys-tems. J Adhes Dent (In press).
8. Sorrentino R, Monticelli F, Goracci C, Zarone F, Tay FR, Ferrari M. Effectof post retained composite restorations on the resistance to fracture ofendodontically treated teeth related to the amount of coronal residual struc-

ture. Am J Dem2007;20:269-274.9. Fredriksson M, Astback J, Pamenius M, Arvidson K. A retrospective study
of 236 patients with teeth restored by carbon fiber-reinforced epoxy resinposts. J Prosthet Dent 1998;80:151-157.
10. Ferrari M, Vichi A, Mannocci F, Mason PN. Retrospective study of theclinical performance of fiber posts Am J Dent 2000; I3 (Spec Iss): 9B-13B.
II. Ferrari M, Cagidiaco MC, Goracci C, Vichi A, Mason PN, Tay FR. Longterm retrospective study of the clinical performance of fiber posts. Am JDent 2007;20:287-291.
12. Glazer B. Restoration of endodontically treated teeth with carbon fibre posts.A prospective study. J Can Den Assoc 2000;66:613-618.
13. Mannocci F, Bertelli E, Sherriff M, Watson TF, Ford TR. Three-yearclinical comparison of survival of endodontically treated teeth restored witheither full cast coverage or with direct composite restoration. J Prosthet Dent2002;88:297-301.
14. Malferrari S, Monaco C, Scotti R. Clinical evaluation of teeth restored withquartz fiber-reinforced epoxy resin posts. 1m J Prosthod 2003;16:39-44.
15. Monticelli F, Grandini S, Goracci C, Ferrari M. Clinical behavior oftranslucent-fiber posts: A 2-year prospective study. 1m J Prosthod2003; 16:593-596.
16. Naumann M, Blankenstein F, Dietrich T. Survival of glass fibre reinforcedcomposite post restorations after 2 years. An observational clinical study. JDem2005;33:305-312.
17. Naumann M, Blankenstein F, Kiessling S, Dietrich T. Risk factors for failureof glass fiber-reinforced composite post restorations: A prospectiveobservational clinical study. Eur J Oral Sci 2005;lI3:519-524.
18. Cagidiaco MC, Radovic I, Simonetti M, Tay FR, Marco Ferrari M. Clinicalperformance of fiber post restorations in endodontically treated teeth. 2 yearresults. 1m J Prosthod 2007; 20: 293-298
19. Caplan DJ, Kolker J, Rivera EM, Walton RE. Relationship between numberof proximal contacts and survival of root canal treated teeth. Int Endod J2002;35:193-199.
20. Aquilino SA, Caplan DJ. Relationship between crown placement and thesurvival of endodontically treated teeth. J Prosthet Dent 2002;87:256-263.
21. Stankiewicz NR, Wilson PRo The ferrule effect: A literature review. IntEndod J 2002;35:575-581. _
22. Akkayan B. An in vitro study evaluating me efft(ct of ferrule length onfracture resistance of endodontically treated teeth restored with fiber-reinforced and zirconia dowel systems. J Prosthet Dent 2004;92: 155-162.
23. Tan PL, Aquilino SA, Qratton DG, Stanford CM, Tan SC, Johnson WT,Dawson D. In vitro fracture resistance of endodontically treated centralincisors with varying ferrule heights and configurations. J ProsthetDent2005;93:331-336.
24. Pereira JR, de Omelas F, Conti PCR, do Valle AL. Effect of crown ferrule
on the fracture resistance of endodontically treated teeth restored withprefabricated posts. J Prosthet Dent 2006;95:50-54.
25. Lassila LVJ, Tanner J, Le Bell A-M, Narva K, Vallittu PK. Flexuralproperties of fiber reinforced root canal posts. Dent Mater 2004;20:29-36.
26. Mannocci F, Sheriff M, Watson TF, Vallittu PK. Penetration of bondingresins into fibre-reinforced composite posts: A confocal microscopic study.Int Endod 12005;38:46-51.
27. Fokkinga WA, Kreulen CM, LeBell-Ronnlof A-M, Lassila LVJ, VallittuPK, Creugers NHJ. In vitro fracture behavior of maxillary premolars withmetal crowns and several post-and-core systems. Eur J Oral Sci2006; 114:250-256.
28. Fokkinga WA, Kreulen CM, Vallittu PK, Creugers NH. A structuredanalysis of in vitro failure loads and failure modes of fiber, metal, andceramic post-and-core systems Int J Prosthod 2004;17:476-482.
29. Fokkinga WA, Kreulen CM, LeBell-Ronnlof A-M, Lassila LVJ, VallittuPK, Creugers NHJ. Fracture behavior of structurally compromised non-vitalmaxillary premolars restored using experimental fiber reinforced compositecrowns. Am J Dent 2006;19:326-32.
30. Kalkan M, Usumez A, Ozturk N, Belli S, Eskitascioglu G. Bond strengthbetween root dentin and three glass-fiber post systems. J Prosthet Dent2006;96:41-6.
31. Bouillaguet S, Schutt A, Alander P, Schwaller P, Buerki G, Michler J,Cattani-Lorente M, Vallittu PK, Krejci I. Hydrothermal and mechanicalstresses degrade fiber-matrix interfacial bond strength in dental fiber-reinforced composites. J Biomed Mater Res Part B: Appl Biomater2006;76B:98-105.
32. Garoushi S, Lassila LVJ, Tezvergil A, Vallittu PK. Static and fatiguecompression test for particulate filler composite resin with fiber-reinforcedcomposite substructure. Dent Mater 2007;23: 17-23
33. Ferrari M, Cagidiaco MC, Grandini S, De Sanctis M, Goracci C. Postplacement affects survival of endodontically treated teeth. J Dent Res 2007;86: 729-734.
34. Grandini S, Goracci C, Monticelli F, Tay FR, Ferrari M. Fatigue resistanceand structural characteristics of fiber posts: three-point bending test andSEM evaluation. Dent Mater 2005;21:75-82.
35. Seefeld F, Wenz H-J, Lugwig K, Kern M. Resistance to fracture andstructural characteristics of different fiber reinforced post systems. DemMarer 2007; 23: 265-71.
36. Ray HA, Trope M. Periapical status of endodontically treated teeth inrelation to the technical quality of thee root filling and the coronalrestoration. lilt Endod J 1995;28:12-18.
37. Tronstad L, Asbjomsen K, Doving L, Pedersen I, Eriksen HM. Influence ofcoronal restorations on the periapical health of endodontically treated teeth.Endod Dent TraumatoI2000; 16:18-21.