plain films radiographs pa and lateral views ct chest
TRANSCRIPT

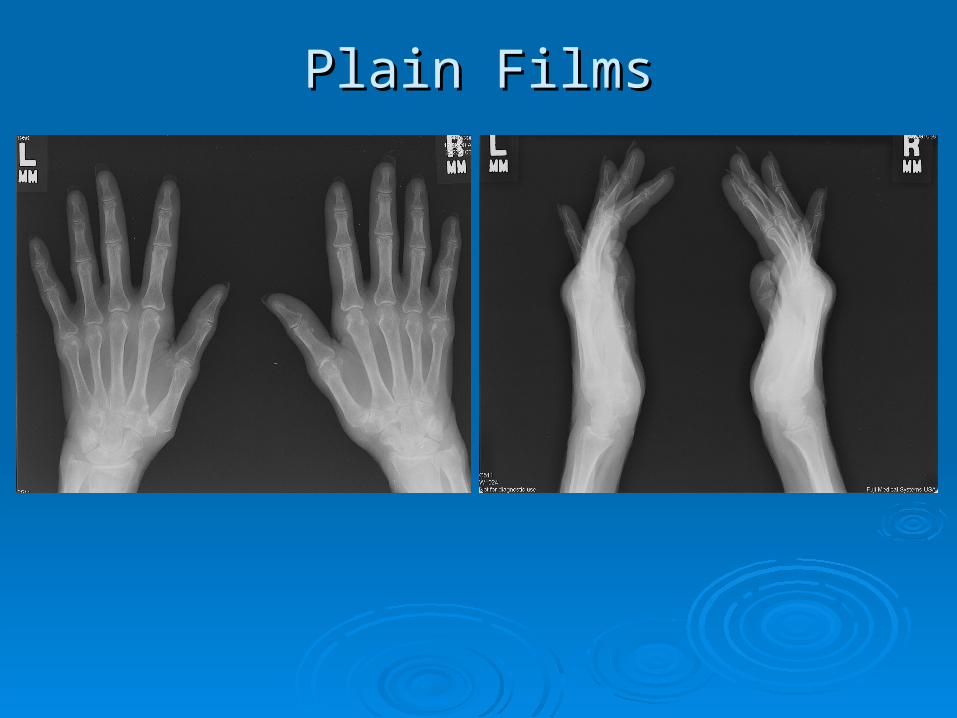
Plain FilmsPlain Films
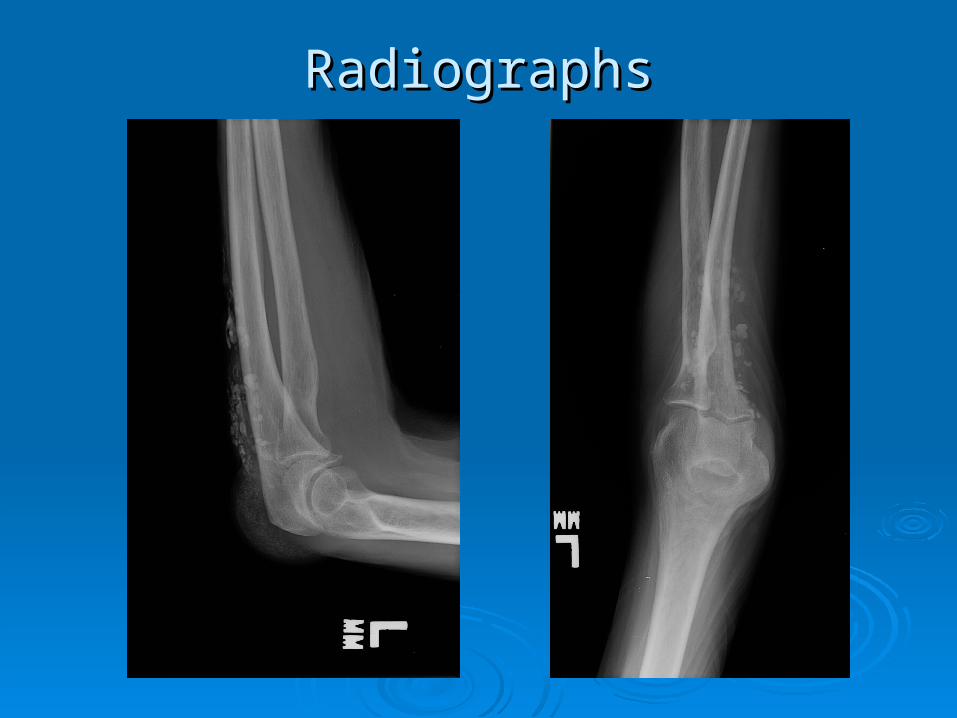
RadiographsRadiographs
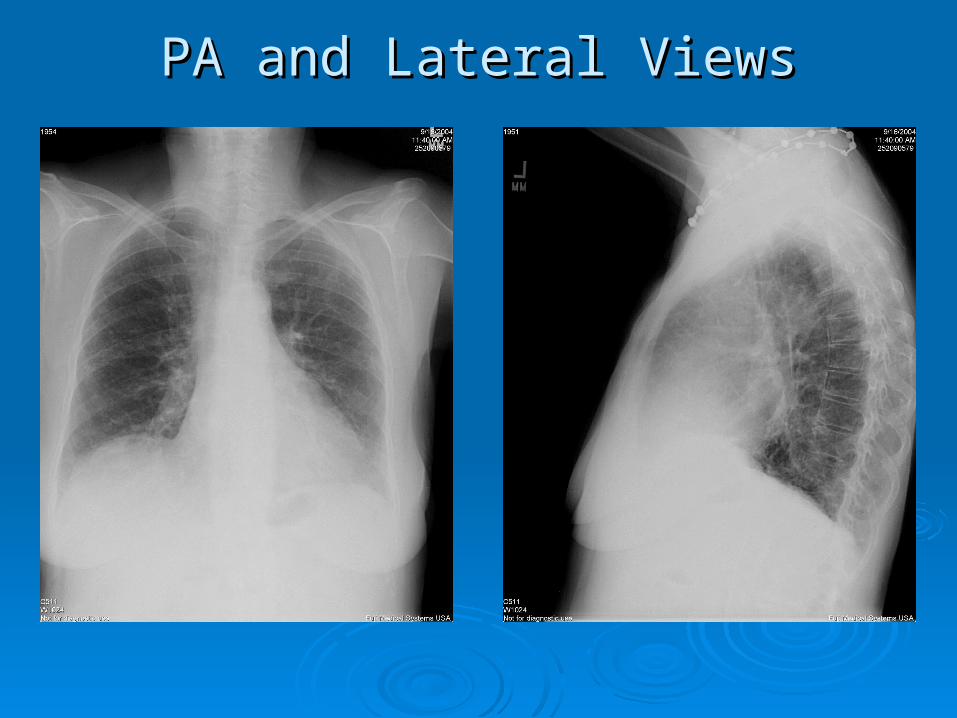
PA and Lateral ViewsPA and Lateral Views

CT ChestCT Chest


Polymyositis Overlap Syndromes, Polymyositis Overlap Syndromes, Anti-Synthetase SyndromeAnti-Synthetase Syndrome

EpidemiologyEpidemiology
DM/PM Syndrome affects mostly adults with a DM/PM Syndrome affects mostly adults with a female:male ratio of 3:1female:male ratio of 3:1
Relative prevalence exhibits regional latitude Relative prevalence exhibits regional latitude in Europe increasing from North (Iceland; in Europe increasing from North (Iceland; RP:0.08) to South (Greece; RP:0.56) (RP:0.08) to South (Greece; RP:0.56) (Hengstman, Hengstman,
van Venrooij et al. Ann. Rheum. Dis. ; 2000van Venrooij et al. Ann. Rheum. Dis. ; 2000) ) Jo-1 antibodies are correlated with HLA-DR3 Jo-1 antibodies are correlated with HLA-DR3
in Caucasiansin Caucasians Prevalence of antisynthetase antibodies is 20-Prevalence of antisynthetase antibodies is 20-
40% in patients with DM/PM40% in patients with DM/PM

Thought to have precedent viral exposure Thought to have precedent viral exposure leading to persistent presence of auto-leading to persistent presence of auto-antigens (molecular mimicry)antigens (molecular mimicry)
UV-B is thought to play a role given UV-B is thought to play a role given prevalence in European countries along prevalence in European countries along latitude. latitude. UV-B stimulates dermal expression of TNF-UV-B stimulates dermal expression of TNF-
alpha and other type-1 cytokinesalpha and other type-1 cytokines Spectrum includes both humoral mediated Spectrum includes both humoral mediated
(DM) and cell mediated (CD8+ cytotoxic (DM) and cell mediated (CD8+ cytotoxic cells in PM) mechanismscells in PM) mechanisms
Due to these different mechanisms, both Due to these different mechanisms, both DM, PM, and the overlap syndromes have DM, PM, and the overlap syndromes have differing responses to anti-inflammatory differing responses to anti-inflammatory agentsagents
PathophysiologyPathophysiology

FeaturesFeatures Raynaud’sRaynaud’s Proximal muscle weakness vs. combined proximal Proximal muscle weakness vs. combined proximal
and distal weakness in inclusion body myositisand distal weakness in inclusion body myositis PhotodermatitisPhotodermatitis Mechanic’s handsMechanic’s hands Elevated inflammatory markers, variable elevations in Elevated inflammatory markers, variable elevations in
CKCK Capillary dilation with periungal inflammationCapillary dilation with periungal inflammation May have amyopathic diseaseMay have amyopathic disease Subcutaneous calcinosis (anti-synthetase syndrome)Subcutaneous calcinosis (anti-synthetase syndrome) Interstitial Lung Disease (anti-synthetase syndrome)Interstitial Lung Disease (anti-synthetase syndrome) Symmetric, deforming (but not erosive) polyarthritis Symmetric, deforming (but not erosive) polyarthritis
(anti-synthetase syndrome)(anti-synthetase syndrome)
Clinical PresentationClinical Presentation

Physical Exam FindingsPhysical Exam Findings
Adapted from Targoff et alAdapted from Targoff et al

Physical Exam FindingsPhysical Exam Findings
Adapted from Targoff et alAdapted from Targoff et al

Physical Exam FindingsPhysical Exam Findings
Adapted from Targoff et alAdapted from Targoff et al

AutoantibodiesAutoantibodies
Note that 40% of Note that 40% of these DM/PM/Overlap these DM/PM/Overlap patients have patients have detectable antibodies. detectable antibodies. Clinical presentation Clinical presentation and muscle biopsy and muscle biopsy then becomes then becomes paramount.paramount.
+ ANA in 80% of + ANA in 80% of cases, don’t discount cases, don’t discount a negative ANAa negative ANA
DiseaseDisease
EntityEntity
Auto-Auto-antibodyantibody
DermatomyositDermatomyositisis
Anti-Mi2Anti-Mi2
PolymyositisPolymyositis Anti-SRPAnti-SRP
Polymyositis-Polymyositis-SclerodermaScleroderma
Anti-PM-Anti-PM-SclScl
DM/PM, DM/PM, Polyarthritis, Polyarthritis,
ILD ILD
Jo-1/anti-Jo-1/anti-synthetasesynthetase
DM/SLEDM/SLE RNPRNP

ANA PatternsANA Patterns
+ ANA, Speckled pattern. DM/PM + ANA, Speckled pattern. DM/PM (anti-Mi2 and SRP antibodies)(anti-Mi2 and SRP antibodies)
+ ANA, nucleolar pattern. Overlap + ANA, nucleolar pattern. Overlap of PM with Scleroderma (anti-PM-of PM with Scleroderma (anti-PM-Scl)Scl)
Negative ANA, cytoplasmic Negative ANA, cytoplasmic pattern. Anti-synthetase pattern. Anti-synthetase syndromessyndromes

Anti-Synthetase antibodiesAnti-Synthetase antibodies These autoantibodies are These autoantibodies are
directed towards aminoacyl-directed towards aminoacyl-tRNA synthetases tRNA synthetases (responsible for transfer of (responsible for transfer of AA to conjugate transfer AA to conjugate transfer RNAs)RNAs)
These are found in the These are found in the cytoplasm, therefore ANA cytoplasm, therefore ANA stains are cytoplasmic and stains are cytoplasmic and are thus reported as are thus reported as negative (20% of all negative (20% of all inflammatory myopathies) inflammatory myopathies)
AntigenAntigen Auto-Auto-antibodyantibody
Histidyl-Histidyl-tRNA tRNA
synthetase synthetase
Jo-1 Jo-1
Threonyl-Threonyl-tRNA tRNA
PL-7 PL-7
Alanyl-tRNA Alanyl-tRNA PL-12 PL-12
Isoleucyl-Isoleucyl-tRNA tRNA
OJ OJ
Glycyl-tRNA Glycyl-tRNA EJ EJ
Anti-Synthetase SyndromeAnti-Synthetase Syndrome

Clinical ManifestationClinical Manifestation Patients with Patients with
antisynthetase syndrome antisynthetase syndrome typically present with two typically present with two or more components of or more components of myositis, ILD, and joint myositis, ILD, and joint involvementinvolvement
ILD may occur in ILD may occur in absence of myositis, absence of myositis, particularly associated particularly associated with PL-12 with PL-12 autoantibodies (autoantibodies (Friedman, Friedman,
Targoff, Arnett. Semin Arthritis Rheum; 1996Targoff, Arnett. Semin Arthritis Rheum; 1996))
Clinical Clinical manifestationmanifestation
PrevalencePrevalence
Myositis Myositis 90%90%
Interstitial lung Interstitial lung disease (ILD)disease (ILD) 60%60%
Arthritis Arthritis 50-90%50-90%
Raynaud's Raynaud's 40%40%
Fever Fever 20%20%
Anti-Synthetase SyndromeAnti-Synthetase Syndrome

Physical therapy and an active exercise regimenPhysical therapy and an active exercise regimen Corticosteroids 1mg/kg/day with good success Corticosteroids 1mg/kg/day with good success
(remission rates of 25-68% achieved)(remission rates of 25-68% achieved) Non-steroidals (methotrexate .3mg/kg/week, Non-steroidals (methotrexate .3mg/kg/week,
azathioprine 2.5mg/kg/day, cyclophosphamide azathioprine 2.5mg/kg/day, cyclophosphamide 3mg/kg/day) used with mild-moderate success3mg/kg/day) used with mild-moderate success
Use IVIG in refractory casesUse IVIG in refractory cases Case reports describe use of Rituximab in Case reports describe use of Rituximab in
refractory casesrefractory cases
TreatmentTreatment

In older patients, consider occult In older patients, consider occult malignancy workupmalignancy workup
Non-Hodgkin’s Lymphoma associated Non-Hodgkin’s Lymphoma associated with DM/PMwith DM/PM
May order DEXA scan given prolonged May order DEXA scan given prolonged course of corticosteroidscourse of corticosteroids
Complications can include steroid Complications can include steroid induced myopathy (progressive induced myopathy (progressive weakness with improved CK)weakness with improved CK)
Most common cause of mortality = Most common cause of mortality = complications from ILD leading to complications from ILD leading to pulmonary HTN and hypoxiapulmonary HTN and hypoxia
ConsiderationsConsiderations

Gratuitous photosGratuitous photos

ReferencesReferences Hengstman GJD, van Venrooij WJ, Vencovsky J, Moutsopoulos HM, van Engelen Hengstman GJD, van Venrooij WJ, Vencovsky J, Moutsopoulos HM, van Engelen
BGM. The relative prevalence of dermatomyositis and polymyositis in Europe exhibits BGM. The relative prevalence of dermatomyositis and polymyositis in Europe exhibits a latitudinal gradient. Ann. Rheum. Dis. 59:141-142; 2000. a latitudinal gradient. Ann. Rheum. Dis. 59:141-142; 2000.
Plotz PH, Targoff I. Myositis associated antigens. Aminoacyl-tRNA synthetases. In : Plotz PH, Targoff I. Myositis associated antigens. Aminoacyl-tRNA synthetases. In : Manual of Biological Markers of Disease. Eds,WJ Van venrooij and R Maini. Kluwer Manual of Biological Markers of Disease. Eds,WJ Van venrooij and R Maini. Kluwer Academic Publications. The Netherlands. pp B6.1: 1-18; 1994. Academic Publications. The Netherlands. pp B6.1: 1-18; 1994.
Love LA, Leff RL, Fraser DD, Targoff IN, Dalakas M, Plotz PH, Miller FW. A new Love LA, Leff RL, Fraser DD, Targoff IN, Dalakas M, Plotz PH, Miller FW. A new approach to the classification of idiopathic inflammatory myopathy: myositis-specific approach to the classification of idiopathic inflammatory myopathy: myositis-specific autoantibodies define useful homogeneous patient groups. Medicine (Baltimore) autoantibodies define useful homogeneous patient groups. Medicine (Baltimore) 70:360-74; 1991. 70:360-74; 1991.
Friedman AW, Targoff IN, Arnett FC. Interstitial lung disease with autoantibodies Friedman AW, Targoff IN, Arnett FC. Interstitial lung disease with autoantibodies against aminoacyl-tRNA synthetases in the absence of clinically apparent myositis. against aminoacyl-tRNA synthetases in the absence of clinically apparent myositis. Semin Arthritis Rheum 26:459-67; 1996. Semin Arthritis Rheum 26:459-67; 1996.
Grathwohl KW, Thompson JW, Riordan KK, Roth BJ, Dillard TA. Digital clubbing Grathwohl KW, Thompson JW, Riordan KK, Roth BJ, Dillard TA. Digital clubbing associated with polymyositis and interstitial lung disease. Chest 108:1751-2; 1995. associated with polymyositis and interstitial lung disease. Chest 108:1751-2; 1995.
Kalenian M, Zweiman B Inflammatory myopathy, bronchiolitis obliterans/organizing Kalenian M, Zweiman B Inflammatory myopathy, bronchiolitis obliterans/organizing pneumonia, and anti-Jo-1 antibodies: an interesting association. Clin Diagn Lab pneumonia, and anti-Jo-1 antibodies: an interesting association. Clin Diagn Lab Immunol 4:236-40;1997. Immunol 4:236-40;1997.
Targoff IN, Arnett FC Clinical manifestations in patients with antibody to PL-12 Targoff IN, Arnett FC Clinical manifestations in patients with antibody to PL-12 antigen (alanyl-tRNA synthetase). Am J Med 88:241-51; 1990. antigen (alanyl-tRNA synthetase). Am J Med 88:241-51; 1990.
Lee W, Zimmermann B 3rd, Lally EV.Relapse of polymyositis after prolonged Lee W, Zimmermann B 3rd, Lally EV.Relapse of polymyositis after prolonged remission. J.Rheumatol 24:1641-4; 1997. remission. J.Rheumatol 24:1641-4; 1997.
Dalakas MC. Current treatment of the inflammatory myopathies. Curr Opin Dalakas MC. Current treatment of the inflammatory myopathies. Curr Opin Rheumatol 6:595-601; 1994.Rheumatol 6:595-601; 1994.