plan of action forms - southern 7 health department
TRANSCRIPT

0
Southern Seven Head Start/Early
Head Start Plan of Action Forms
Grantee and delegate agencies operating center-based programs must establish and implement policies and procedures to respond to medical and dental health emergencies with which all staff are familiar and trained.
Compiled By the Health & Nutrition Specialist Last Updated: July, 2018

1
Table of Contents
Plan of Action: Asthma/Breathing Difficulties .................................................................................. 2
Plan of Action: Allergy ................................................................................................................... 7
Plan of Action: Diabetes .............................................................................................................. 15
Hyperglycemia: ....................................................................................................................... 16
Hypoglycemia: ......................................................................................................................... 16
Plan of Action: Seizures ............................................................................................................... 22
Other Health Conditions: ............................................................................................................. 26
Works Cited ................................................................................................................................ 30

2
Plan of Action: Asthma/Breathing Difficulties
Asthma is a chronic inflammatory disease of the respiratory system that causes the airways of the
lungs to swell, tighten and constrict. During an asthma episode three things can happen:
Swelling of the airways (inflammation)
Squeezing: the air passages are squeezed together by the muscles that surround the outside
of each airway (constriction)
Clogging: the mucus blocks the airways and thus allows less air to pass through the airways
This combination of swelling, squeezing, and clogging dramatically reduces the size of the airways.
Quick Facts
Asthma is one of the most common chronic diseases nationwide, impacting the lives and
families of over 7 million children.
Asthma is the third-ranking cause of hospitalization among children under 15.
An average of one out of every 10 school-aged children has asthma.
10.5 million school days are missed each year due to asthma.
Checklist
Have parent/guardian fill out and sign Southern Seven Head Start/Early Head Start Asthma
Plan of Action Form.
If medication may be needed fill out Medication Administration Form located on the back of
the Asthma Action Plan.
If asthma attack occurs follow procedure outlined in your site’s Emergency/Medical
Management Plan.
Afterwards complete the Symptom Record Form, send a copy to the Health & Nutrition
Specialist and file the original at your center.
3
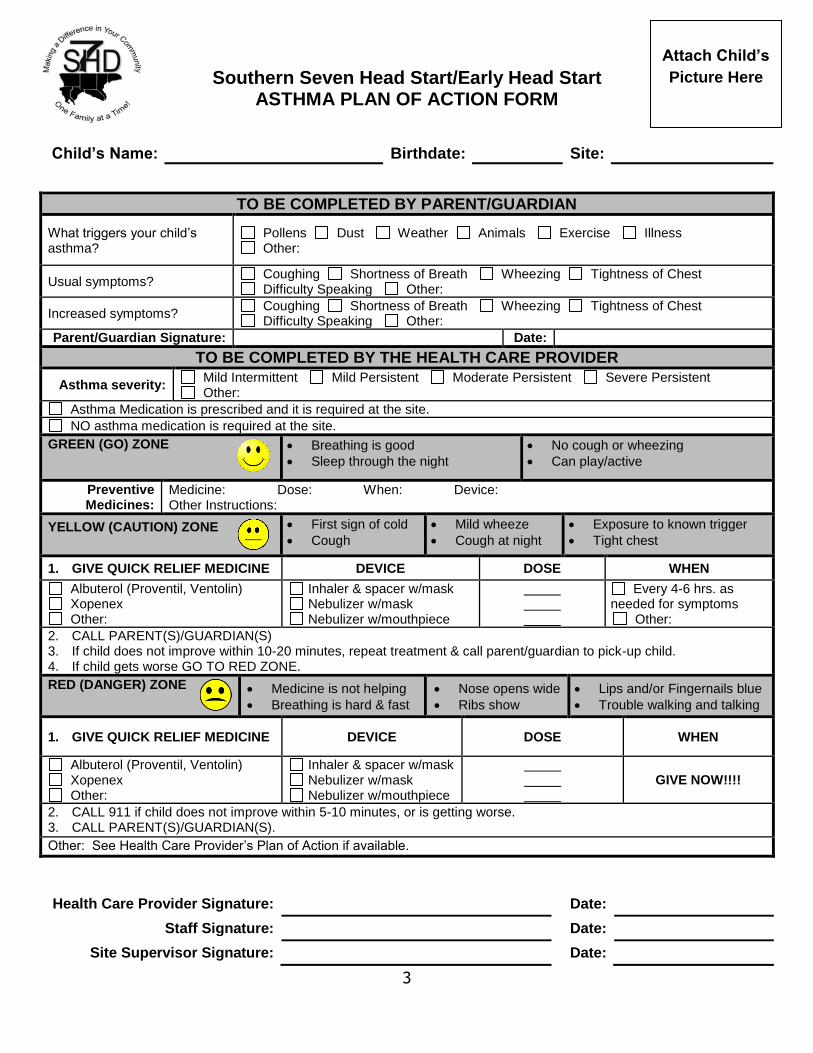
Southern Seven Head Start/Early Head Start ASTHMA PLAN OF ACTION FORM
Child’s Name: Birthdate: Site:
TO BE COMPLETED BY PARENT/GUARDIAN
What triggers your child’s asthma?
Pollens Dust Weather Animals Exercise Illness Other:
Usual symptoms? Coughing Shortness of Breath Wheezing Tightness of Chest Difficulty Speaking Other:
Increased symptoms? Coughing Shortness of Breath Wheezing Tightness of Chest Difficulty Speaking Other:
Parent/Guardian Signature: Date:
TO BE COMPLETED BY THE HEALTH CARE PROVIDER
Asthma severity: Mild Intermittent Mild Persistent Moderate Persistent Severe Persistent Other:
Asthma Medication is prescribed and it is required at the site.
NO asthma medication is required at the site.
GREEN (GO) ZONE Breathing is good
Sleep through the night
No cough or wheezing
Can play/active
Preventive Medicines:
Medicine: Dose: When: Device: Other Instructions:
YELLOW (CAUTION) ZONE First sign of cold
Cough
Mild wheeze
Cough at night
Exposure to known trigger
Tight chest
1. GIVE QUICK RELIEF MEDICINE DEVICE DOSE WHEN
Albuterol (Proventil, Ventolin) Xopenex Other:
Inhaler & spacer w/mask Nebulizer w/mask Nebulizer w/mouthpiece
Every 4-6 hrs. as needed for symptoms
Other:
2. CALL PARENT(S)/GUARDIAN(S) 3. If child does not improve within 10-20 minutes, repeat treatment & call parent/guardian to pick-up child. 4. If child gets worse GO TO RED ZONE.
RED (DANGER) ZONE Medicine is not helping
Breathing is hard & fast
Nose opens wide
Ribs show
Lips and/or Fingernails blue
Trouble walking and talking
1. GIVE QUICK RELIEF MEDICINE DEVICE DOSE WHEN
Albuterol (Proventil, Ventolin) Xopenex Other:
Inhaler & spacer w/mask Nebulizer w/mask Nebulizer w/mouthpiece
GIVE NOW!!!!
2. CALL 911 if child does not improve within 5-10 minutes, or is getting worse. 3. CALL PARENT(S)/GUARDIAN(S).
Other: See Health Care Provider’s Plan of Action if available.
Health Care Provider Signature: Date:
Staff Signature: Date:
Site Supervisor Signature: Date:
Attach Child’s
Picture Here

4
Southern Seven Head Start/Early Head Start PARENT/GUARDIAN’S REQUEST
FOR MEDICATION ADMINISTRATION
All Medication Must Be In The Original Container!
CHILD’S INFORMATION
Name:
Address:
PARENT/GUARDIAN INFORMATION
Mother’s Name: Phone #: Work #:
Address:
Father’s Name: Phone #: Work #:
Address:
ADDITIONAL EMERGENCY CONTACT
Name: Relationship: Phone #:
PHYSICIAN INFORMATION
Name: Phone #:
Office Address:
PRESCRIPTION INFORMATION
Pharmacy: Date:
Prescription Number: Diagnosis:
Drug: Dosage:
Frequency of Administration:
Directions for Administration:
Possible Side Effects:
I hereby request Head Start to administer the above medication to my child ______________________. I will hold and save the Head Start Program from and against any and all actions or cause of action, claims, demands, and liabilities, loss, damage, or expense of whatsoever kind and nature which the Head Start Program shall or may at any time sustain or incur by reason or in consequence of the administrating of the medication to my child.
Parent/Guardian’s Signature: Date:
Staff Signature: Date:
Site Supervisor Signature: Date:

5

6
Asthma/Breathing Difficulties Management Plan
STAY CALM: Don’t Panic. Getting upset only makes things worse.
Remove child from area of trigger and have child sit upright.
Encourage use of deep breathing and relaxation exercises to avoid panic.
Designate 2 individuals to care for child in a private area. Never leave the child alone.
Use the Asthma Action Plan.
Take medicines as directed: Take quick-relief medicine if breathing is labored. No medication
is to be given unless the child has a PRN inhaler or nebulizer.
Child should respond to treatment within 15-20 minutes.
If NO change is observed or breathing becomes significantly worse, call for emergency help
and contact parent immediately.
Make sure someone reassures the children that were present when the attack began and
incorporate the experience into a health lesson.
Seek Immediate Emergency Care If:
! Coughs constantly
! Is unable to speak in complete sentences without taking a breath
! Has lips, nails, mucous membranes that are gray or blue
! Demonstrates severe retractions and/or nasal flaring
! Is vomiting persistently
! Has pulse of greater than 120 per minute
! Has respirations of greater than 30 per minute
! Is severely restless
! Shows no improvements after 15 minutes

7
Plan of Action: Allergy
The job of the body’s immune system is to identify and destroy germs (such as bacteria or viruses)
that make you sick. A food allergy results when the immune system mistakenly targets a harmless
food protein – an allergen – as a threat and attacks it.
Although nearly any food is capable of causing an allergic reaction, only eight foods account for 90
percent of all food-allergic reactions in the United States. These foods are:
Peanut
Tree nuts
Milk
Egg
Wheat
Soy
Fish
Shellfish
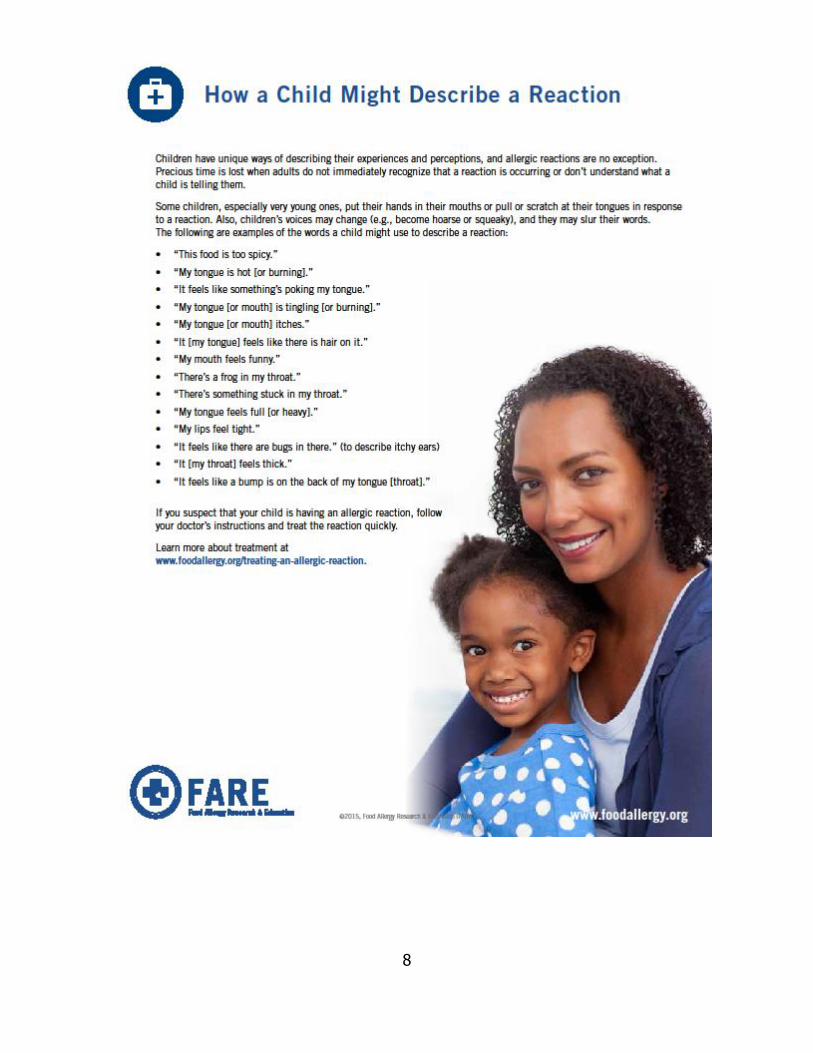
Symptoms typically appear within minutes to several hours after eating the food to
which you are allergic. Keep in mind that children may communicate their symptoms in
a different manner than adults.
Mild symptoms may include one or more of the following:
Hives (reddish, swollen, itchy
areas on the skin)
Eczema (a persistent dry, itchy
rash)
Redness of the skin or around the
eyes
Itchy mouth or ear canal
Nausea or vomiting
Diarrhea
Stomach pain
Nasal congestion or a runny nose
Sneezing
Slight, dry cough
Odd taste in mouth
Uterine contractions
Severe symptoms may include one or more of the following:
Obstructive swelling of the lips,
tongue, and/or throat
Trouble swallowing
Shortness of breath or wheezing
Turning blue
Drop in blood pressure (feeling
faint, confused, weak, passing
out)
Loss of consciousness
Chest pain
A weak or “thread” pulse
Sense of “impending doom”
8

9
Anaphylaxis
Anaphylaxis is an extreme and severe allergic reaction. The whole body is affected, often within minutes of exposure to the substance which causes the allergic reaction (allergen) but sometimes after hours. During anaphylaxis, allergic symptoms can affect several areas of the body and may threaten breathing and blood circulation. Food allergy is the most common cause of anaphylaxis,
although several other allergens – insect stings, medications, or latex – are other potential triggers.
Epinephrine (adrenaline) is a medication that can reverse the severe symptoms of anaphylaxis. It is given as a “shot” and is available as a self-injector, also known as an epinephrine auto-injector, that can be carried and used if needed. Epinephrine is a highly effective medication, but it must be administered promptly during anaphylaxis to be most effective. Delays can result in death in as little as 30 minutes. Even if epinephrine is administered promptly and symptoms seem to subside completely, the individual who was treated with epinephrine should always be taken to the emergency room for further evaluation and treatment.
Quick Facts
Food allergy is a serious medical condition affecting up to 15 million people in the United
States, including 1 in 13 children.
In the U.S., food allergy symptoms send someone to the emergency room every three
minutes.
People who have both asthma and a food allergy are at greater risk for anaphylaxis.
Checklist
Have parent/guardian fill out and sign Southern Seven Head Start/Early Head Start Allergy
Plan of Action Form.
If anaphylaxis is a possibility FARE Food Allergy & Anaphylaxis Emergency Care Plan may be
needed. Contact Health & Nutrition Specialist for further instruction.
If medication may be needed have parent fill out Parent/Guardian’s Request for Medication
Administration Form.
If an allergic reaction occurs follow procedure outlined in your site’s Emergency/Medical
Management Plan.
Afterwards, complete Symptom Record Form, send a copy to the Health & Nutrition Specialist,
and file the original at your center.

10
Southern Seven Head Start/Early Head Start ALLERGY PLAN OF ACTION FORM
Child’s Name: Birthdate: Site:
TO BE COMPLETED BY THE HEALTH CARE PROVIDER
What things cause this child’s allergic reaction?
MILD SYMPTOMS Nose – Itchy or runny nose, sneezing Mouth – Itchy mouth
Skin – A few hives, mild itch Gut – Mild nausea or discomfort
Other:
ACTION FOR MILD SYMPTOMS
1. Give: Rx Antihistamine Other:
2. Call parent/guardian.
3. If condition does not improve within 10 minutes follow the Action for Severe Symptoms below. *For Mild Symptoms from more than one system area, give Epinephrine.
SEVERE SYMPTOMS Lung – Shortness of breath, wheezing, repetitive cough
Heart – Pale or bluish skin, faintness, weak pulse, dizziness
Throat – Tight or hoarse throat, trouble breathing or swallowing
Mouth – Significant swelling of the tongue or lips
Skin – Many hives over body, widespread redness
Gut – Repetitive vomiting, severe diarrhea
Other:
ACTION FOR SEVERE SYMPTOMS
1. Give: Epinephrine Other:
2. Call 911.
3. Call parent/guardian.
Is anaphylaxis a possibility? Yes No
Medications AT SCHOOL? Yes No If yes, what medications? Epinephrine Rx Antihistamine Other:
Other: See Health Care Provider’s Plan of Action if available.
Health Care Provider Signature: Date:
Parent/Guardian Signature: Date:
Staff Signature: Date:
Site Supervisor Signature: Date:
Attach Child’s
Picture Here

11
Southern Seven Head Start/Early Head Start PARENT/GUARDIAN’S REQUEST
FOR MEDICATION ADMINISTRATION
All Medication Must Be In The Original Container!
CHILD’S INFORMATION
Name:
Address:
PARENT/GUARDIAN INFORMATION
Mother’s Name: Phone #: Work #:
Address:
Father’s Name: Phone #: Work #:
Address:
ADDITIONAL EMERGENCY CONTACT
Name: Relationship: Phone #:
PHYSICIAN INFORMATION
Name: Phone #:
Office Address:
PRESCRIPTION INFORMATION
Pharmacy: Date:
Prescription Number: Diagnosis:
Drug: Dosage:
Frequency of Administration:
Directions for Administration:
Possible Side Effects:
I hereby request Head Start to administer the above medication to my child ______________________. I will hold and save the Head Start Program from and against any and all actions or cause of action, claims, demands, and liabilities, loss, damage, or expense of whatsoever kind and nature which the Head Start Program shall or may at any time sustain or incur by reason or in consequence of the administrating of the medication to my child.
Parent/Guardian’s Signature: Date:
Staff Signature: Date:
Site Supervisor Signature: Date:

12

13

14
Allergic Reaction/Anaphylaxis Management Plan
STAY CALM: Don’t Panic. Getting upset only makes things worse.
Follow Allergy Action Plan.
Mild Symptoms:
o Antihistamines may be given if ordered by a healthcare provider. No medication is to be
given unless the child has a PRN on file.
o Stay with child and alert emergency contacts.
o Watch child closely for changes. If symptoms worsen, administer epinephrine
immediately and call 911.
Severe Symptoms:
o Inject Epinephrine Immediately.
o Call 911 – Tell them the child is having anaphylaxis and may need more epinephrine
when they arrive.
o Consider giving additional medications following epinephrine if child has PRN for
antihistamine or inhaler.
o Lay child flat, raise legs and keep warm. If breathing is labored or they are vomiting, let
them sit up or lie on their side.
o IF SYMPTOMS DO NOT IMPROVE OR SYMPTOMS RETURN – MORE DOSES OF
EPINEPHRINE CAN BE GIVEN ABOUT 5 MINUTES OR MORE AFTER THE LAST DOSE.
o Alert Emergency Contacts.
o Transport to ER even is symptoms resolve.
Make sure someone reassures the children that were present when the attack began and
incorporate the experience into a health lesson.
Severe Symptoms
! Short of breath, wheezing, or repetitive cough
! Pale, blue, faint, weak pulse, or dizzy
! Throat is tight, horse, or has trouble breathing/swallowing
! Mouth has significant swelling of the tongue and/or lips
! Skin has many hives over body or widespread redness
! Repetitive vomiting or severe diarrhea
! Feeling something bad is about to happen, anxiety, and confusion
! Or a combination of symptoms from different areas

15
Plan of Action: Diabetes
Diabetes is a problem with the body that causes blood glucose (sugar) levels to rise higher than
normal. This is also called hyperglycemia.
Type I Diabetes: Type 1 diabetes is usually diagnosed in children and young adults, and was
previously known as juvenile diabetes. Only 5% of people with diabetes have this form of the
disease. In type 1 diabetes, the body does not produce insulin. Insulin is a hormone that is needed to
convert sugar, starches and other food into energy needed for daily life.
At its core, proper type 1 diabetes management is composed of a handful of elements: blood glucose
control and insulin management, exercise, nutrition and support.
Medication: Type I Diabetes requires multiple daily injections with insulin pens or syringes or
an insulin pump.
Exercise: With type 1, it’s very important to balance insulin doses with the food eaten and the
activity performed. Sometimes people experience a drop in blood glucose during or after
exercise, so it is very important to monitor blood glucose, take proper precautions, and be
prepared to treat hypoglycemia (low blood glucose).
Nutrition: How much and what type of carbohydrate foods are important for managing
diabetes. The balance between how much insulin is in the body and the carbohydrate eaten
makes a difference in blood glucose levels. Most diabetics have individual meal plans that need
to be followed.
Type II Diabetes: Type 2 diabetes is the most common form of diabetes. In Type 2 diabetes the
body does not use insulin properly. This is called insulin resistance. At first, the pancreas makes extra
insulin to make up for it. But, over time it isn’t able to keep up and can’t make enough insulin to keep
blood glucose at normal levels. Management of Type 2 Diabetes includes healthy eating, regular
exercise, blood glucose monitoring, and sometime medication. Some people who have type 2
diabetes can achieve their target blood sugar levels with diet and exercise alone, but many also need
diabetes medications or insulin therapy.

16
Quick Facts
Type 1 diabetes can also be called insulin-dependent diabetes because people with type 1
must take insulin in order to live.
With tight blood glucose control, a person with diabetes can avoid many of the short- and
long-term complications associated with diabetes.
Hyperglycemia:
Hyperglycemia is the technical term for high blood glucose (blood sugar). High blood glucose
happens when the body has too little insulin or when the body can't use insulin properly.
The signs and symptoms include the following:
High blood glucose
High levels of sugar in the urine
Frequent Urination
Increased Thirst
Dry Mouth
Tired
Hunger
Headache
Ketones in Urine
*If symptoms persist they can lead to nausea, vomiting, stomach pain, and fruit
smelling breath
Hypoglycemia:
Hypoglycemia is a condition characterized by abnormally low blood glucose (blood
sugar) levels, usually less than 70 mg/dl. However, it is important talk with a child’s
parent/guardian about individual blood glucose targets, and what level is too low that
specific child.
Signs and Symptoms of Hypoglycemia (happen quickly):
Shakiness Nervousness or anxiety
Sweating, chills and clamminess
Irritability or impatience
Confusion, including delirium
Rapid/fast heartbeat
Lightheadedness or dizziness
Hunger and nausea
Sleepiness
Blurred/impaired vision
Tingling or numbness in the lips
or tongue
Headaches
Weakness or fatigue
Anger, stubbornness, or sadness
Lack of coordination
Nightmares or crying out during
sleep
Seizures
Unconsciousness

17
Checklist
Have parent/guardian fill out and sign Southern Seven Head Start/Early Head Start Diabetes
Plan of Action Form, Hyperglycemia Plan of Action Form, and Hypoglycemia Plan of Action
Form.
Contact the Health & Nutrition Specialist to schedule a diabetes training for site staff
If medication may be needed have parent fill out Parent/Guardian’s Request for Medication
Administration Form
If hypoglycemia or hyperglycemia occurs follow procedure in plans
Afterwards, complete Symptom Record Form, send a copy to the Health & Nutrition Specialist,
and file the original at your center

18
Southern Seven Head Start/Early Head Start DIABETES PLAN OF ACTION FORM
Child’s Name: Site:
1) Diagnosis: Type I Diabetes Type II Diabetes Pre-Diabetes
Other Condition Requiring Glucose Monitoring:
2) When should blood sugar monitoring be done?
As needed for signs/symptoms of low or high blood sugar
Before Feeding
As needed for signs/symptoms of illness
Other:
3) Diet Requirements:
No Concentrated Sweet Diet
Carbohydrate Count: carbs/meal
Other:
Does the child require a SCHEDULED snack at any time during the school
day? Yes No
If yes, do they need insulin with the snack? Yes No
How many units of insulin? Other: See Health Care Provider’s Plan of Action if available.
Plan of Action:
Health Care Provider Signature: Date:
Parent/Guardian Signature: Date:
Staff Signature: Date:
Site Supervisor Signature: Date:
Attach Child’s
Picture Here

19
Southern Seven Head Start/Early Head Start HYPERGYLCEMIA (HIGH BLOOD SUGAR)
PLAN OF ACTION FORM
Child’s Name: Site:
Signs & Symptoms:
dry mouth; increased urination; tired; thirsty; sores or infections that will not heal; hungry; sleepy; dry, itchy skin; headache *If symptoms persist, they can lead to nausea, vomiting, stomach pain, fruity smelling breath
High Blood Sugar for this Child Requiring the Following Interventions is Greater Than: (Fill in the number)
Interventions:
Encourage extra liquids without sugar such as water. No extra juice or milk.
Allow frequent trips to the restroom.
Ketone monitoring: (If child is positive for ketones, MUST notify parent/guardian)
Other: Other: See Health Care Provider’s Plan of Action if available.
Plan of Action:
Health Care Provider Signature: Date:
Parent/Guardian Signature: Date:
Staff Signature: Date:
Site Supervisor Signature: Date:
Attach Child’s
Picture Here
20
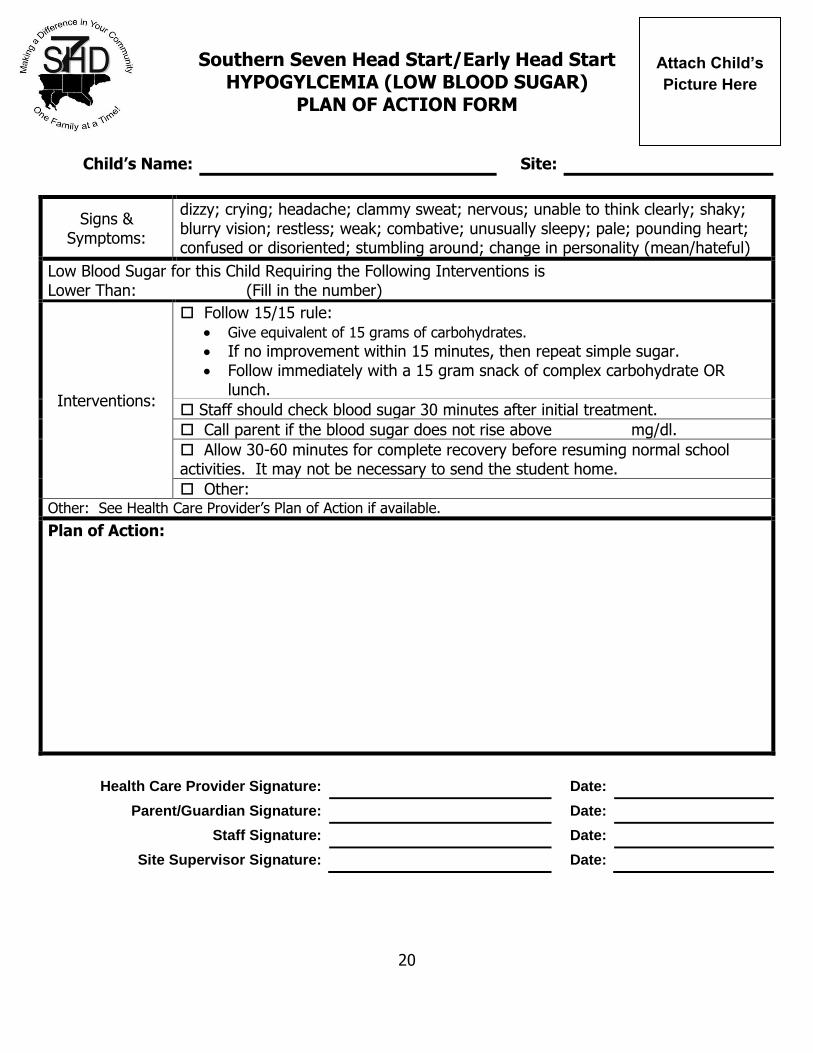
Southern Seven Head Start/Early Head Start HYPOGYLCEMIA (LOW BLOOD SUGAR)
PLAN OF ACTION FORM
Child’s Name: Site:
Signs & Symptoms:
dizzy; crying; headache; clammy sweat; nervous; unable to think clearly; shaky; blurry vision; restless; weak; combative; unusually sleepy; pale; pounding heart; confused or disoriented; stumbling around; change in personality (mean/hateful)
Low Blood Sugar for this Child Requiring the Following Interventions is Lower Than: (Fill in the number)
Interventions:
Follow 15/15 rule: Give equivalent of 15 grams of carbohydrates. If no improvement within 15 minutes, then repeat simple sugar. Follow immediately with a 15 gram snack of complex carbohydrate OR
lunch.
Staff should check blood sugar 30 minutes after initial treatment.
Call parent if the blood sugar does not rise above mg/dl.
Allow 30-60 minutes for complete recovery before resuming normal school activities. It may not be necessary to send the student home.
Other: Other: See Health Care Provider’s Plan of Action if available.
Plan of Action:
Health Care Provider Signature: Date:
Parent/Guardian Signature: Date:
Staff Signature: Date:
Site Supervisor Signature: Date:
Attach Child’s
Picture Here

21
Hyperglycemia Management Plan
STAY CALM: Don’t Panic. Getting upset only makes things worse.
Follow Hyperglycemia Treatment steps listed in child’s action plan
If child uses a pump, check to see if pump is connected properly and functioning.
Give child plenty of water to drink.
Allow extra trips to the restroom.
Re-check glucose every 2 hours to determine if glucose is reaching normal level.
Restrict physical activity.
Notify parent/guardian immediately if ketones are present.
Moderate Hypoglycemia Management Plan
STAY CALM: Don’t Panic. Getting upset only makes things worse.
Provide simple sugar equal to grams of carbohydrates in child’s action plan.
Wait 15 minutes.
Recheck blood glucose level.
Repeat if blood glucose level is still low.
Follow immediately with a 15 gram complex carbohydrate snack or next meal.
Contact the student’s parents/guardian.
Severe Hypoglycemia Management Plan
STAY CALM: Don’t Panic. Getting upset only makes things worse.
Position the student on his or her side.
Do not attempt to give anything by mouth.
Follow child’s action plan.
While treating, have another person call 911 (Emergency Medical Services).
Contact the student’s parents/guardian.
Stay with the student until Emergency Medical Services arrive.
Hypoglycemia Severe Symptoms
! Inability to eat or drink
! Unconscious
! Unresponsive
! Seizure activity or Convulsions

22
Plan of Action: Seizures
Seizures are caused by abnormal electrical activity in the brain. Someone having a seizure might
collapse, shake uncontrollably, or have another brief disturbance in brain function, often with a loss
of or change in consciousness.
Seizures can be frightening, but most last only a few minutes, stop on their own, and are not life
threatening.
Seizures that happen more than once or over and over might indicate the ongoing condition epilepsy.
Some children under 5 years old have febrile seizures, which can develop during a medium or high
fever — usually above 100.4°F (38°C). While terrifying to parents, these seizures are usually brief
and rarely cause any serious or long-term problems.
Quick Facts
You can’t swallow your tongue during a seizure. It's physically impossible.
You should NEVER force something into the mouth of someone having a seizure.
Epilepsy is NOT rare. There are more than twice as many people with epilepsy in the US as the
number of people with cerebral palsy (500,000), muscular dystrophy (250,000), multiple
sclerosis (350,000), and cystic fibrosis (30,000) combined.
Checklist
Have parent/guardian fill out and sign Southern Seven Head Start/Early Head Start Seizure
Plan of Action Form
If medication may be needed fill out the Medication Administration Form located on the back
of the Seizure Plan of Action form.
If seizure occurs follow procedure outlined in your site’s Emergency/Medical Management Plan
Afterwards, complete Symptom Record Form, send a copy to the Health & Nutrition Specialist,
and file the original at your center

23
Southern Seven Head Start/Early Head Start SEIZURES PLAN OF ACTION FORM
Child’s Name: Birthdate: Site:
TO BE COMPLETED BY THE HEALTH CARE PROVIDER
Type of Seizure Length Frequency Description
For Febrile Seizure: If child has a temperature of degrees Fahrenheit or higher then administer fever reducing medication per instruction on the Authorization to Administer Prescription Medication form and call parent to pick-up.
Possible triggers or warning signs:
SEIZURE FIRST AID
Stay calm and track time Keep child safe Do not restrain Do not put anything in mouth Stay with child until fully conscious Record seizure in log
Protect head (tonic-clonic) Keep airway open/watch breathing (tonic-clonic)
Turn child on side (tonic-clonic)
SEIZURE ACTION PLAN
1. Notify parent or emergency contact if unable to reach call 911.
2. Administer emergency medications as indicated if applicable.
3. Other: See Health Care Provider’s Plan of Action if available.
A SEIZURE IS GENERALLY CONSIDERED AN EMERGENCY WHEN:
Convulsive (tonic-clonic) seizure lasts longer than 5 minutes.
Student has repeated seizures without regaining consciousness.
Student is injured or has diabetes.
Student has a first-time seizure.
Student has breathing difficulties.
Health Care Provider Signature: Date:
Parent/Guardian Signature: Date:
Staff Signature: Date:
Site Supervisor Signature: Date:
Attach Child’s
Picture Here

24
Southern Seven Head Start/Early Head Start PARENT/GUARDIAN’S REQUEST
FOR MEDICATION ADMINISTRATION
All Medication Must Be In The Original Container!
CHILD’S INFORMATION
Name:
Address:
PARENT/GUARDIAN INFORMATION
Mother’s Name: Phone #: Work #:
Address:
Father’s Name: Phone #: Work #:
Address:
ADDITIONAL EMERGENCY CONTACT
Name: Relationship: Phone #:
PHYSICIAN INFORMATION
Name: Phone #:
Office Address:
PRESCRIPTION INFORMATION
Pharmacy: Date:
Prescription Number: Diagnosis:
Drug: Dosage:
Frequency of Administration:
Directions for Administration:
Possible Side Effects:
I hereby request Head Start to administer the above medication to my child ______________________. I will hold and save the Head Start Program from and against any and all actions or cause of action, claims, demands, and liabilities, loss, damage, or expense of whatsoever kind and nature which the Head Start Program shall or may at any time sustain or incur by reason or in consequence of the administrating of the medication to my child.
Parent/Guardian’s Signature: Date:
Staff Signature: Date:
Site Supervisor Signature: Date:

25
Seizure Management Plan
If Generalized Seizure Occurs:
If falling, assist student to floor, turn to side.
Loosen clothing at neck and waist; protect head from injury.
Clear away furniture and other objects from area.
Have another classroom adult direct students away from area.
Time the seizure.
Allow seizure to run its course; DO NOT restrain or insert anything into student’s
Do not try to stop purposeless behavior.
During a general or grand mal seizure expect to see pale or bluish discoloration of the skin or
lips. Expect to hear noisy breathing.
If Smaller Seizure Occurs: (lip smacking, behavior outburst, staring, twitching of mouth/hands)
Assist student to comfortable, sitting position.
Time the seizure.
Stay with student, speak gently, and help student get back on task following seizure.
Seizure Is Considered An Emergency When:
! A convulsive (tonic-clonic) seizure lasts longer than 5 minutes
! There are repeated seizures without regaining consciousness
! It’s a first-time seizure
! The child is injured or has diabetes
! The child has breathing difficulties
! The seizure is in water

26
Other Health Conditions:
Checklist
Have parent/guardian fill out and sign Southern Seven Head Start/Early Head Start Other
Health Conditions Plan of Action Form
If medication may be needed have parent fill out Parent/Guardian’s Request for Medication
Administration Form
If an incidence occurs related to the specific condition(s) follow the Plan of Action.
Afterwards, complete Symptom Record Form, send a copy to the Health & Nutrition Specialist,
and file the original at your center
27
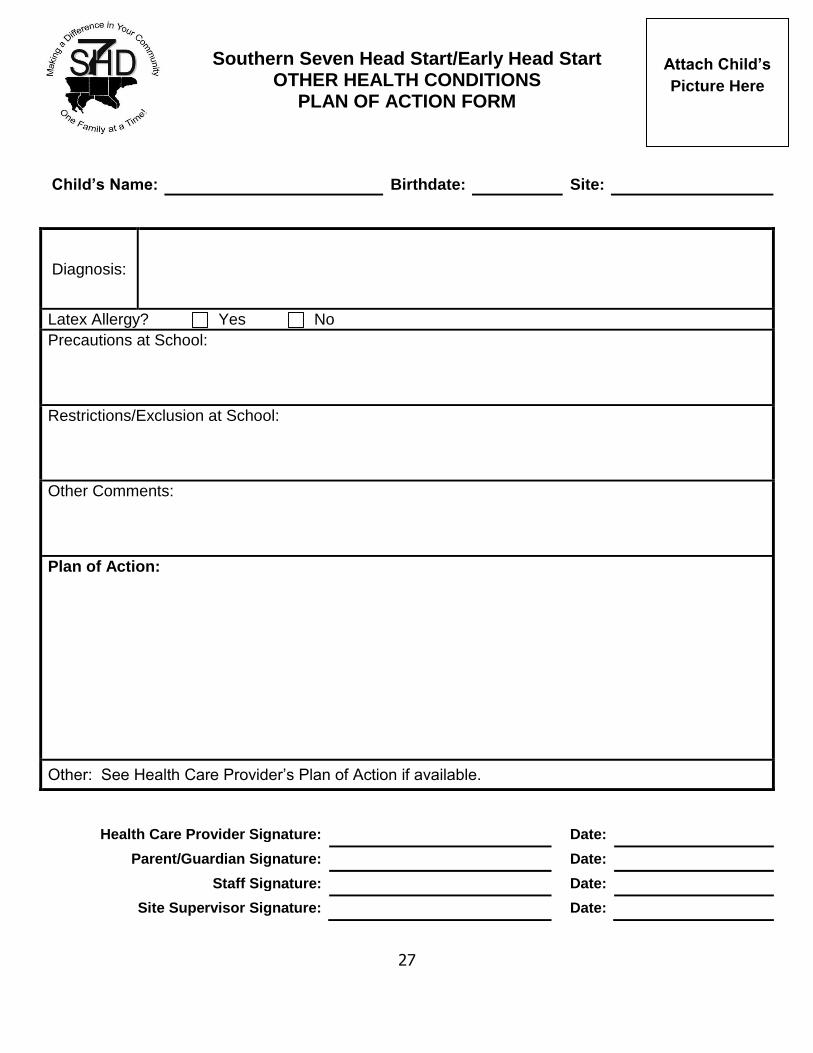
Southern Seven Head Start/Early Head Start OTHER HEALTH CONDITIONS
PLAN OF ACTION FORM
Child’s Name: Birthdate: Site:
Diagnosis:
Latex Allergy? Yes No
Precautions at School:
Restrictions/Exclusion at School:
Other Comments:
Plan of Action:
Other: See Health Care Provider’s Plan of Action if available.
Health Care Provider Signature: Date:
Parent/Guardian Signature: Date:
Staff Signature: Date:
Site Supervisor Signature: Date:
Attach Child’s
Picture Here

28
Southern Seven Head Start/Early Head Start PARENT/GUARDIAN’S REQUEST
FOR MEDICATION ADMINISTRATION
All Medication Must Be In The Original Container!
CHILD’S INFORMATION
Name:
Address:
PARENT/GUARDIAN INFORMATION
Mother’s Name: Phone #: Work #:
Address:
Father’s Name: Phone #: Work #:
Address:
ADDITIONAL EMERGENCY CONTACT
Name: Relationship: Phone #:
PHYSICIAN INFORMATION
Name: Phone #:
Office Address:
PRESCRIPTION INFORMATION
Pharmacy: Date:
Prescription Number: Diagnosis:
Drug: Dosage:
Frequency of Administration:
Directions for Administration:
Possible Side Effects:
I hereby request Head Start to administer the above medication to my child ______________________. I will hold and save the Head Start Program from and against any and all actions or cause of action, claims, demands, and liabilities, loss, damage, or expense of whatsoever kind and nature which the Head Start Program shall or may at any time sustain or incur by reason or in consequence of the administrating of the medication to my child.
Parent/Guardian’s Signature: Date:
Staff Signature: Date:
Site Supervisor Signature: Date:

29
Southern Seven Head Start/Early Head Start SYMPTOM RECORD
Child’s Name: Date:
MAIN SYMPTOM:
When did it began? How long has it lasted?
How much? How often?
Is it staying constant, getting better or worse?
OTHER SYMPTOMS/COMPLAINTS:
General appearance (ie. comfort, mood, behavior, activity level, appetite):
CHECK () THE SYMPTOMS
Breathing: coughing wheezing breathing fast difficulty breathing other:
Skin: pale flushed rash sores swelling bruises itchiness other:
Vomiting (number of times): Diarrhea (number of times): Urine:
Eyes: pink/red watery discharge crusty swollen other:
Nose: congested runny other:
Ears: pulling at ears discharge other:
Mouth: sores drooling difficulty swallowing other:
Odors (ie. Breath, stool):
Temperature: axillary oral rectal other:
WHAT HAS BEEN DONE
Comfort: Rest:
Liquids Name: Amount: Time:
Food Name: Amount: Time:
Medications (see medication administration procedure)
Name: Amount: Time:
Emergency measures:
Who was called and when (ie. parent/guardian, emergency contact person, health consultant, child’s health provider, emergency medical services)?
Signature: Date:

30
Works Cited
American Diabetes Association. (2015). ADA. Retrieved from American Diabetes Assocation:
http://www.diabetes.org
American Lung Associate. (2015). Learning More About Asthma. Retrieved from American Lung
Association: Fighting for Air: http://www.lung.org/lung-disease/asthma/learning-more-about-
asthma/
Food Allergy & Research Education. (2015). FARE. Retrieved from Food Allergy & Anaphylaxis
Emergency Care Plan: https://www.foodallergy.org/faap
Kid's Health. (2015). Seizure Basics. Retrieved from Kid's Health:
http://kidshealth.org/parent/firstaid_safe/emergencies/seizure.html#
National Heart, Lung, & Blood Institute. (2007). NIH. Retrieved from Asthma Action Plan:
https://www.nhlbi.nih.gov/files/docs/public/lung/asthma_actplan.pdf
PPMD. (n.d.). Seizure Action Plan for Schools. Retrieved from Parent's Place of Maryland:
http://ppmd.org/wp-content/uploads/2014/03/WritableSeizure_Action_Plan.pdf