planning members kathi ayers, rn. msn, trauma program manager, sharp san diego bruce barton, agency...
TRANSCRIPT


Planning Members Kathi Ayers, RN. MSN, Trauma Program Manager, Sharp San Diego
Bruce Barton, Agency Director, Riverside EMSRaul Coimbra, Chief Division of Trauma/Burns UCSD Medical Center (Lead)
Brent Eastman, Chief Medical Officer Scripps HealthLes Gardina, QA Specialist San Diego EMS
Chris Van Gorder, President and CEO Scripps HealthVirginia Hastings, Executive Director, Inland Counties EMS Agency Dorothy Kelley, Trauma Services Director Scripps Mercy Hospital
Ryan Kelley, Agency Director, Imperial CountyCynthia Marlin-Stoll, Riverside County Department of Public Health
Sue Cox, Director of Trauma Services, Rady’s Children’s HospitalSharon Pacyna, RN, MPH, Trauma Program Manager, UCSD
Facilitators:Bonnie Sinz, Chief EMS Systems Division EMSA
Johnathan Jones, State Trauma Coordinator, EMSA
Region #5 – Interim Regional Trauma Coordinating Committee
Structure
Steering Committee– Triage Subcommittee– Performance Improvement Subcommittee– Repatriation Subcommittee– Funding Subcommittee

Achievements
Monthly Conference Calls• Steering Committee
Two Regional Summit Meetings• Temecula, January 2009• Palm Springs, June 2009• Loma Linda – planned for February 2010

Regional Representation
• All Trauma Centers (Level I, II, IV, Pediatric)• 4 LEMSAs• Pre-hospital Agencies (Ground and Aeromedical)• Fire Agencies• State of California Department of Corrections and
Rehabilitation • CHP• Hospital Associations• Registrars
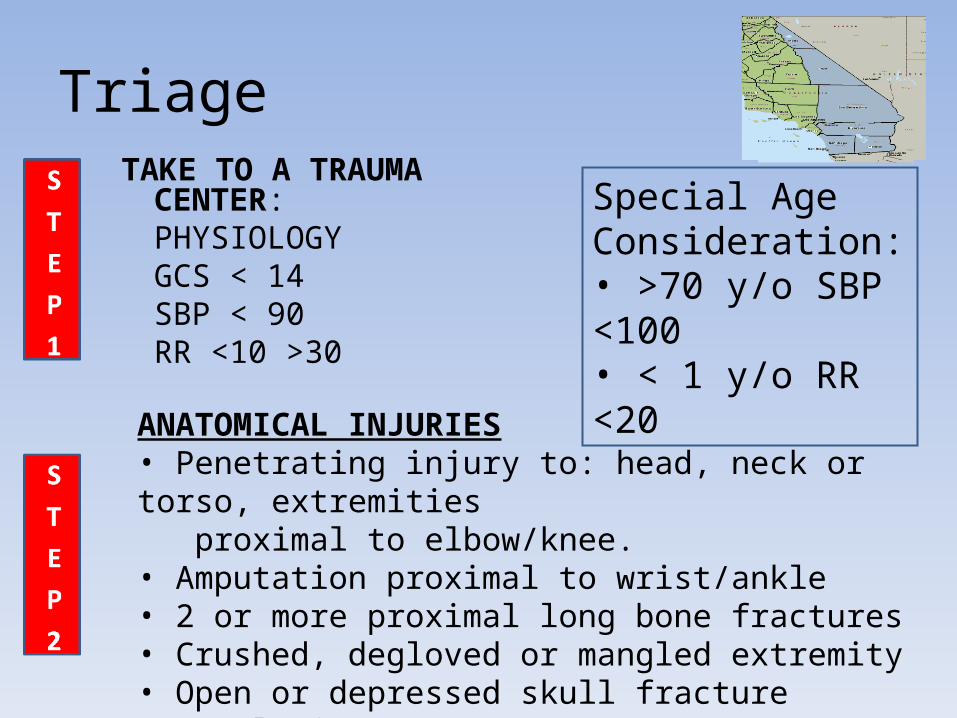
TriageTAKE TO A TRAUMA CENTER:
PHYSIOLOGY GCS < 14SBP < 90RR <10 >30
Special Age Consideration:• >70 y/o SBP <100• < 1 y/o RR <20
ANATOMICAL INJURIES• Penetrating injury to: head, neck or torso, extremities proximal to elbow/knee.• Amputation proximal to wrist/ankle• 2 or more proximal long bone fractures• Crushed, degloved or mangled extremity• Open or depressed skull fracture• Paralysis

Triage continued
IF PATIENT DOES NOT MEET ANY OF THE ABOVE CONSIDER TAKING TO A TRAUMA CENTER
• Falls > 20 ft– Peds* fall > 10 feet or 3 times height of child
• High risk auto crash – Intrusion > 12” driver side, >18” any side– Death in same passenger compartment– Auto vs pedestrian/cyclist thrown or run over w/ significant impact, >20mph

Triage continued
SPECIAL CONSIDERATIONS• Very young / very old
– Adults > 70 years– Peds – consider a pediatric trauma center
• Anticoagulation therapy (Plavix, ASA, Coumadin)• Time sensitive extremity injury• Pregnancy > 20 weeks• Burns
– With trauma to a trauma center– Without trauma to a burn center

PI Successes and Challenges
Successes• Consensus to submit trauma data to CEMSIS • Examine consistency of intra-county data
element definitions• Conduct intra-county data collectionChallenge• Time required to participate in a constructive
manner
PI Goals
• Apply audit filters to compare intra-county outcomes and practice patterns
• Interfacility Transfer Survey – process obstacles/facilitators
• Develop Practice Guidelines for Open Fractures (adult/pediatric)
• Develop Fracture Decision Tree

Repatriation Goals• Identify 5 primary placement/repatriation barriers
• Define categories of “difficult placement patients” (e.g. dialysis, behavior problem, non-documented, homeless etc.)
• Develop a survey for SE RTCC trauma centers to identify current repatriation practices and tracking processes for difficult placement patients
• Identify Trauma Center fiscal and discharge planning representatives for participation on redesigned committee focused on patient placement

Repatriation Successes
• Developed a Survey and distributed it to all SE RTCC Trauma Centers. Questionnaire targeted current methods of identifying and tracking difficult to place trauma patients.
• Contacted Trauma Center’s fiscal personnel and discharge planners for inclusion in Repatriation subcommittee activities.
Repatriation Challenges• Identify and overcome system barriers to placement
in Long Term Care facilities
• Quantify “difficult placement patients” in subcategories (e.g. dialysis, behavior problem, non-documented, homeless etc.)
• Create a collective vision for alternative solutions to regional repatriation issues
• Obtain cooperation of Trauma Centers to share financial information to track patient costs

Funding Task Force• Bruce Barton, Administrator
Riverside County EMS Agency
• Virginia Hastings, Executive DirectorInland Counties EMS Agency
• Ryan Kelley, AdministratorImperial County EMS Agency
• Marcy Metz, AdministratorSan Diego County EMS Agency

Funding• Funding for hospitals and physicians may be a key
factor in successful regionalization of trauma systems
• A complete discussion of funding must include repatriation opportunities/responsibilities
• Traditional funding sources for uncompensated care generally come through counties
• Any reappropriation of county funding must be approved by our various Boards of Supervisors/Governing Boards

Funding Goals and Objectives• Work with county budget analysts to discuss current
revenue streams that are generally used to pay for MIA/indigent/uncompensated care
• Using trauma registries, identify patients that cross county/state lines
• Identify payor source for those patients• Identify county/state/country of incident when
possible• Aggregate patient charges when available • Collect and analyze trauma financial data that can be
utilized to garner funding in the legislature • Develop blueprint for integrated, well developed
trauma systems.

Funding Challenges
• SURPRISE !!!
• OBSTACLES
• WE ALL DO THINGS DIFFERENTLY !

Overall Goals
• Establish a Region-Wide QI Meeting
• Interface with other RTCCs
• Disaster Planning

How our region can foster California’s State Trauma System
• Identifying and Standardizing Best Practices
• Developing Region-Wide QI Meeting
• Establishing Inter-County Communication Channels