platelet transfusions · 2020-01-11 · •thrombocytopenia is defined as a platelet count less...
TRANSCRIPT

Platelet Transfusions
Dr Vinay H joshi MD, DM,
Fellowship NICU, PICU & Cardiac ICU
(University Of Sydney & Toronto)
Cloudnine Hospital, Mumbai
SRCC Children’s Hospital, Mumbai

Case
• 26 wks, 700gms, severe PIH, day6, on CPAP, intermittent apneas, platelets 60000/cmm
• 26 wks, 700 gms, severe HMD, day 6, sepsis, ventilated, 2 mm PDA, platelets 55000
• 26 weeks, 700gms, day 6, on CPAP, partial feeds, platelets 25000/cmm

• Thrombocytopenia is defined as a platelet count less than 1.5 lacs/cmm
• 2nd most common (after anemia) hematologic disorder of infants admitted to NICUs
• Incidence:
• 18-35% of all NICU patients
• 70% of ELBW infants (< 1000gms)
• 80% in < 600 gms

Classification of Thrombocytopenia
• Timing
• Early- within 3 days
• Late- > 4 days
• Severity
• Mild- 1.5- 1 lac/cmm
• Moderate- 1 lac- 50000/cmm
• Severe- < 50000/cmm

Causes of Thrombocytopenia

Thrombocytopenia and Risk Of Serious Hemorrhage in PT infants??
Andrew et al. 1992
• Thrombocytopenic infants, 2 ½ times more likely to bleed than non-thrombocytopenic infants
• Among VLBW infants, thrombocytopenia was associated with higher incidence of severe bleeding (IVH Grade III/IV) (44% Vs 16%)
Prematurity IVH

• The incidence and severity of thrombocytopenia is inversely proportional to the GA
• The smallest and most premature infants have the highest incidence of bleeding/IVH
• ~ 30% of ELBW babies have IVH, usually developed in the first week of life

Platelet transfusions Vs platelet count
• So it is accepted that these babies should receive platelets at higher threshold levels (Vs children and adults)

Transfusion practices in Europe and NA Cremer et al Transfusion 2011
Normal PT Sepsis l PT

Are we doing it right?
• Timing and thresholds are right?
• Platelet transfusions – the only way to prevent IVH in PT/ELBW neonates?
• Do platelet transfusions really reduce the risk of bleeding?
• Are we causing more harm by UNNECESSARY platelet transfusions?

Andrew et al 1993
• Randomized controlled trial
• 152 VLBW infants, mild to moderate thrombocytopenia, first week of life
• Two thresholds, > 1.5 lacs/cmm Vs60000/cmm
• No difference in IVH (28% Vs 26%)
• Limitation: Babies with severe thrombocytopenia and > 7 days excluded
No added benefit of maintaining platelet levels > 50000/cmm Vs > 1,50000

PlaNeT-1 study- Stanworth et alPediatrics 2009
• Prospective, multicenter Observational study
• 25% of thromboctopenia, platelets < 60,000/cmm
• 9% of above patients experienced severe IVH
• 87% patients < 28 weeks and 87% occurred within first 2 weeks of life
• Secondary analysis showed babies who received platelets had fewer minor bleeds (Vs those who did not receive platelets)

Nadir platelets were similar in NO Bleed, SMALL Bleed and SEVERE bleed

• Von Linden et al
• Liberal Vs restricted platelet transfusion
• No difference in the incidence of bleeding

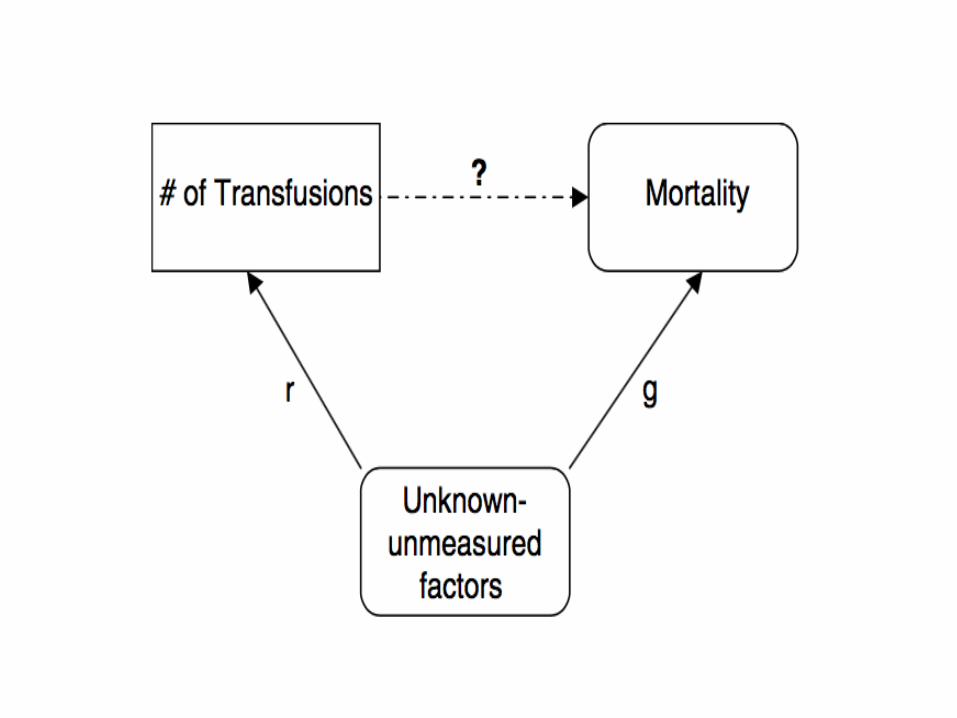
So is it the combination of thrombocytopenia with other factors
(clinical and lab) more predictive of risk for bleeding?

Factors contributing to IVH
• Fragile, vascularized and ill supported germinal matrix
• Fluctuations of hemodynamics-hypotension, PDA, volume boluses, ionotropes etc
• Sick infants (NEC, DIC)

PlaNeT 2 MATISSE Collaborators

PlaNeT 2 MATISSE Collaborators
• RCT, multicenter
• Platelet transfusion; High threshold- 50,000 VsLow threshold 25,000
• 660 patients, median GA 26.6wks, BWt740gms
• Primary outcomes: Death or major bleed within 28 days of randomization

Results
• Platelet Tx: 90% babies in high threshold group Vs 53% in low threshold group
• Major bleed or death: 26% in high threshold Vs19% in low threshold group (CI 1.06- 2.32, p= 0.02)
• Secondary outcomes: Higher BPD in high threshold group compared to low threshold group (63% Vs 54%, OR 1.54)
• Adverse outcomes: No difference between the groups


From available literatureConclusion…
• Limited evidence to suggest causal relationship between platelet levels and serious IVH
• No additional benefit of prophylactic transfusions to maintain higher platelet counts
• Strongest predictors of serious bleeding were:
• GA < 28 weeks
• Post-natal age < 10 days
• Severe sepsis/ NEC

• Prophylactic platelet transfusions (for higher thresholds) can increase mortality, IVH and BPD
From available literaturConclusion…

Do platelet transfusions increase mortality???

Harmful effects of platelet transfusions
• Infections: bacterial, viral, CMV
• Inflammation: the supernatant fluid contains inflammatory mediators (VEGF, PAF, IL-6, IL-8)
• GVHD- immunocompromised
• TRALI
• Tilting towards prothrombotic state (adult platelets)
• Volume overload

Transfusion Related Acute Lung Injury(TRALI)
• Potentially Life threatening complication of blood transfusion
• In adults, reported mortality ~ 5-10%
• Manifests in the form acute respiratory distress requiring escalation of respiraotrysupport
• Two Hit theory: Neutrophils and HLA

29
16
6
0
5
10
15
20
25
30
Nu
mb
er o
f
ep
iso
de
s
Any One
criterion
Any Two
criteria
All Three
criteria
Criteria: FiO2 > 10%, MAP >2,
New mode of ventilation
TRALI Episodes by Number of Diagnostic Criteria
Does Transfusion Related Acute Lung Injury (TRALI) Occur In Newborns
V Joshi1, P Joshi1, K Webert2, J Cairnie1, N Heddle2, T Sabourin1, M Blajchman2 and H Kirpalani1
Department of Neonatology1 and Transfusion Medicine2, McMaster Children’s Hospital, Hamilton, ON, Canada
Background
• TRALI is a potentially
life-threatening complication of blood
transfusion in adults. (Incidence-1:5000
transfusions).
• The reported mortality is approximately
5-10% of TRALI cases.
• Only two cases of TRALI occurring in
neonates have been reported in
literature1,2.
Objectives
• To determine if TRALI occurs in
neonates;
• If it occurs, to estimate its incidence.
Design/Methods
• In a level III NICU, we prospectively
observed all consecutive newborns who
received a blood product transfusion
from June 2005 to October 2005.
• As this was a pilot study to establish
whether the phenomenon might exist, we
formed a convenience sample of 200
consecutive blood product transfusions.
• Information recorded: patient
demographics, blood component
received, indication for blood component
therapy and cardio-respiratory status (4
hours prior to and 6 hours post-
transfusion).
We defined TRALI as present if,
compared to the average 4 hours
pre-transfusion, any of the following
events occurred in the 6 hours
following the start of the transfusion:
(i) An increase in FiO2 of >10% for
>15 minutes;
(ii) An increase in mean airway
pressure of >2 cm H2O;
(iii) A new mode of ventilation
initiated by a worsening lung
condition (increased frequency of
apnea with bradycardia; or RR
increase by >10/min).
Results• 200 blood products were
administered to 75 newborn infants
(2.6 per infant).
• 30 received a single transfusion and
45 babies received multiple
transfusions.
• TRALI was seen in 29 transfusion
episodes (15%). Of these, 23 episodes
were associated with PRBC, 4 with
platelets, and 2 with FFP.
Type of Blood Product Transfused
4%(8) 3% (5)
73%(148)
20%(39)
PRBC
Platelets
FFP
Others
Mean (SD) FiO2 requirement in the 16 babies who had a change of >10% FiO2
4 hrs pre-
transfusion
Start of transfusion Peak of FiO2 rise after
start of transfusion
6 hours post-
transfusion
42.6 (13.3)† 44.3 (17.7) †*
p† >0.05
72.7 (22.2) *#
p *=0.0004
47.2 (20.3) #
p # =0.009
0
20
40
60
80
100
120
-4 -3 -2 -1 0 1 2 3 4 5 6 7
Time in ho urs
FiO
2 %
TRALI Episodes With Increase In FiO2 By > 10%
Conclusion15% incidence of TRALI was noted in
our study as diagnosed by predefined
criteria.
Future directionSince this study was from a single
institution, a multi-center evaluation
would help confirm this is a true entity
in newborns.References1. O’Connor JC, Strauss RG, Goeken NE, Knox LB. A near-fatal reaction during granulocyte transfusion of a neonate. Transfusion 1988; 28:173-176.2. Gloster ES, Ranu S, Wang Y. Transfusion related acute lung injury (TRALI) type reaction in a neonate. Transfusion 2004; 44; supplement 108 A, SP263.
Fig.1.
Table.1.
Fig.2.
Fig.3.
Total Transfusions 200 TRALI like episodes 29 (15%)
Packed Red cells 148 (74%) 23 (16%)
Platelets 39 (20%) 4 (10%)
Fresh Frozen Plasma 8 (4%) 2 (25%)
Others 5 (2.5%) Nil

• Platelet transfusions associated with highest incidence of complications among all components
(Slonim AD. Transfusion 2008,
Stainsby D. UK SHOT scheme Br J Hematol 2008)
• Strong association between number of platelet transfusions and increased neonatal morbidity and mortality (Del Vecchio 2001, Garcia MG 2001, BonifacioL 2007, Kenton AB 2005)

Limitation of the definition
• Can we use same conventional cut offs to define thrombocytopenia in preterm infants?
• Is it really thrombocytopenia? Or normal values for PT/ELBW infants?

Weidmeier SE et al 2009, 47,000newborns, 22-42 weeks GA
Mean
95th centile
5th centile
Need to redefine thrombocytopenia in PT/ELBW infants
1.041.25

Summary
• Preterm thrombocytopenia needs better definition, reference range
• No correlation found between platelet transfusion and timing of IVH
• Prophylactic administration of platelets did not prevent/reduce IVH
• Platelet transfusions are associated with complications (infection, inflammation, TRALI)
• Keeping higher thresholds for platelet transfusion was associated with increased mortality, IVH and BPD

So we infer…..
• Need to shift towards restricted (Lesser) platelet transfusion practice in babies without significant bleeding within last 72 hours
So let’s think think think …before reaching out for that platelet bag!!

Thank You