pleural disease - paccm @ pitt€¦ · pleural disease meghan fitzpatrick, md pleural disease: ......
TRANSCRIPT

PleuralDisease
MeghanFitzpatrick,MD
PleuralDisease:Objec:ves
• Reviewtheanatomyandphysiologyofthepleuralspace
• Reviewdiagnosisandmanagementofcommondisordersofthepleura– Pleuraleffusion– Pneumothorax– PleuralTumors

PleuralAnatomy
• Visceralandparietalpleurasurroundthelungandlinethoraciccavity,respec:vely
• Singlelayerofmesothelialcells,withunderlyinglayerofconnec:ve:ssuecontainingvasculature,lympha:cs,nerves
NeJerF.AtlasofHumanAnatomy,2ndedi:on.1997,Plate200.

PleuralAnatomy
• Bothparietalandvisceralpleurainhumansaresuppliedbysystemiccircula:on
• Lympha:csarepresentinbothvisceralandparietalpleura,butfluidfromthepleuralspaceisprimarilyabsorbedbytheparietalpleurallympha:cs
• Painfibersarelocatedonparietalpleuraonly

PleuralPhysiology
• Pleuralspacepressureinaspontaneouslybreathingpersonisanega:vepressurespace(withexcep:onofduringforcedexhala:on)
cmH
2O
Liters
-5
-8
FRC
LungVolume
Intrapleuralpressure

PleuralPhysiology:FluidTransfer• 2-20mLoffluidineachpleuralspace,con:nuouslyfiltered
viapleuralcapillaries• Fluidflowforeverycapillarysystemcanbedescribedusing
theStarlingequa:onQf=Kf*[(PCAP-PPL)-σ(πCAP - πPL)]Qf:fluidflow(intopleuralspace)P:hydrosta:cpressures,π:onco:cpressuresKf:filtra:oncoefficient(capillarypermeability)σ:reflec:oncoefficient(abilityofthecapillarytoretainsolute)

Filtration:Qf=Kf*[(PCAP-PPL)-σ(πCAP - πPL)]
πPL:+5Kf
Kfσ
σ
πCAP : +34
PCAP:+26PPL:-5
PLEURALcapillariesNeteffectslightnetposi:vefiltra:onintopleuralspace

ParietalPleuralLympha6csAbsorbFluid,Solute,andCellsfromthePleuralSpace
πPL:+5Kf
Kfσ
σ
πCAP : +34
PCAP:+26PPL:-5

WhatLeadstoExcessPleuralFluidCollec:on?
• Mul:pleMechanisms…

Filtration:Qf=Kf*[(PCAP-PPL)-σ(πCAP - πPL)]
Kf
Kf
Kf
Kf
Kf
Kf
πCAP πPL
PCAP PPL
IncreasedPleuralCapillaryPermeability:• PleuralInflamma:on• Infec:on• Connec:veTissueDisease• Malignancy
Filtration:Qf=Kf*[(PCAP-PPL)-σ(πCAP - πPL)]
Kf
Kf
Kf
Kf
Kf
Kf
êπCAP πPL
PCAP PPL
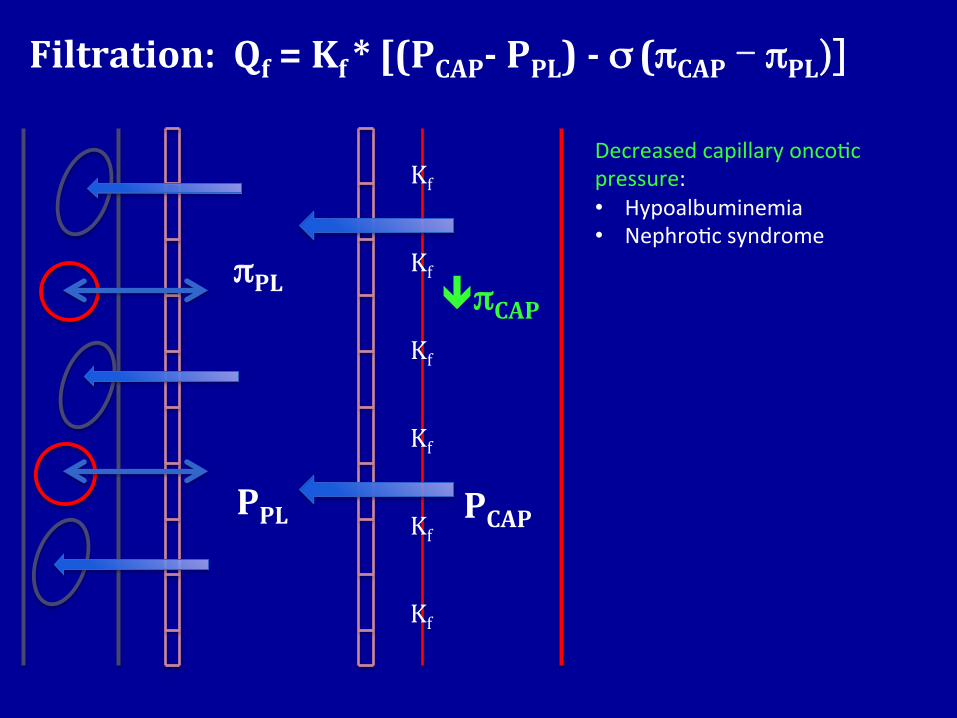
Decreasedcapillaryonco:cpressure:• Hypoalbuminemia• Nephro:csyndrome

Filtration:Qf=Kf*[(PCAP-PPL)-σ(πCAP - πPL)]
Kf
Kf
Kf
Kf
Kf
Kf
πCAP éπPL
PCAP PPL
Increasedpleuralonco:cpressure:• notusuallysignificant• occasionallywithhemothorax
Filtration:Qf=Kf*[(PCAP-PPL)-σ(πCAP - πPL)]
Kf
Kf
Kf
Kf
Kf
Kf
πCAP πPL
éPCAP PPL
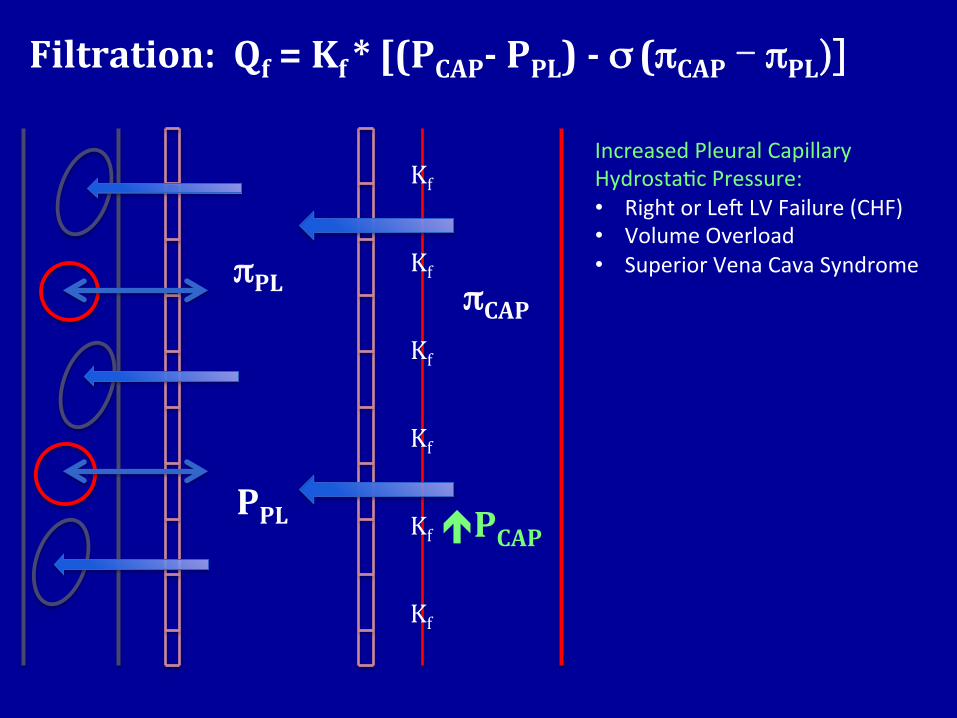
IncreasedPleuralCapillaryHydrosta:cPressure:• RightorLedLVFailure(CHF)• VolumeOverload• SuperiorVenaCavaSyndrome

Filtration:Qf=Kf*[(PCAP-PPL)-σ(πCAP - πPL)]
Kf
Kf
Kf
Kf
Kf
Kf
πCAP πPL
PCAP êPPL
Decreasedpleuralhydrosta:cpressure:• Lungatelectasis

Filtration:Qf=Kf*[(PCAP-PI)-σ(πCAP - πI)]
πI
PI
Kf
σ
πCAP
PCAP
PULMONARYcapillaries
inters::um
Increasedinters::alfluidoverwhelmingtheclearanceofthepulmonarylympha:cs• Highpressureorhighpermeability
pulmonaryedema(CHF,pneumonia,ARDS,VolumeOverload,etc.
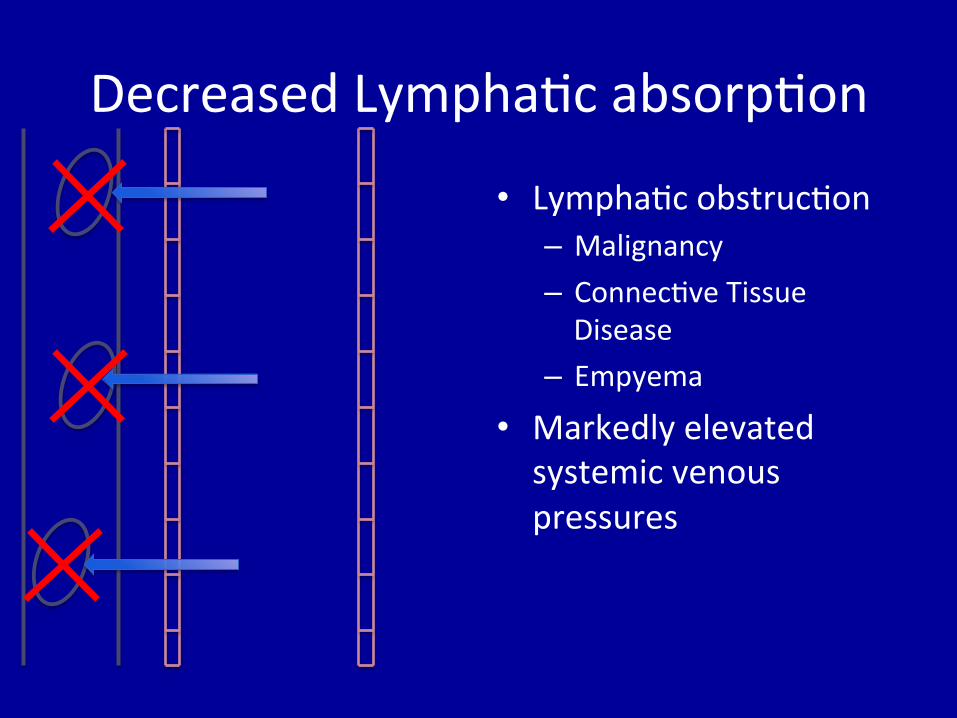
DecreasedLympha:cabsorp:on
• Lympha:cobstruc:on– Malignancy– Connec:veTissueDisease
– Empyema
• Markedlyelevatedsystemicvenouspressures

PleuralEffusionPathogenesis:Summary
Mul:pleMechanisms:1) Increasedpulmonaryinters::alfluidfrom
alveolar/pulmonarycapillaryleak(pulmonarycircula:on)intointers::alspacesoflung,thenintothepleuralspace
2) Pleuralcapillary(systemiccircula:on)Starlingchanges
3) Obstruc:onofparietallympha:cdrainage4) Breachofpleuralspacetoanotherfluid-filled
compartment

PleuralEffusionClinical:Background
• Morethan1,000,000casesannuallyinU.S.
• Physicalexamfindingsreflectfluidinterposedbetweenthechestwallandthelung:dullnesstopercussion,decreasedtac:lefremitus,diminishedbreathsounds
• AppearsonCXRatavolumeof200mLinPAprojec:onand50mLonlateral–decubitusviews,ultrasound,orCTenhancedetec:on
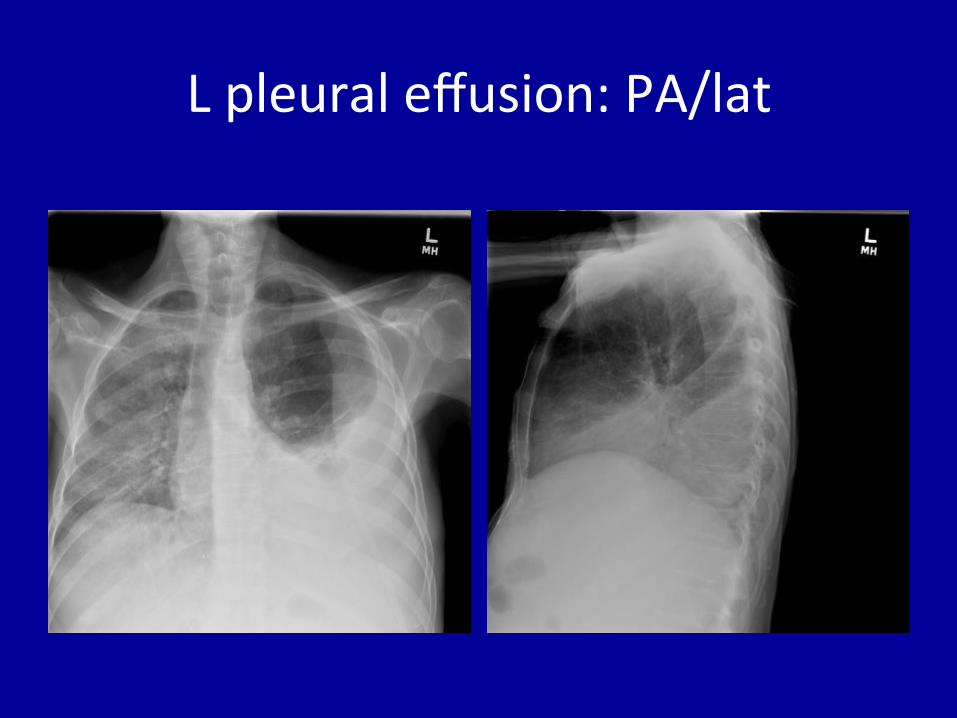
Lpleuraleffusion:PA/lat
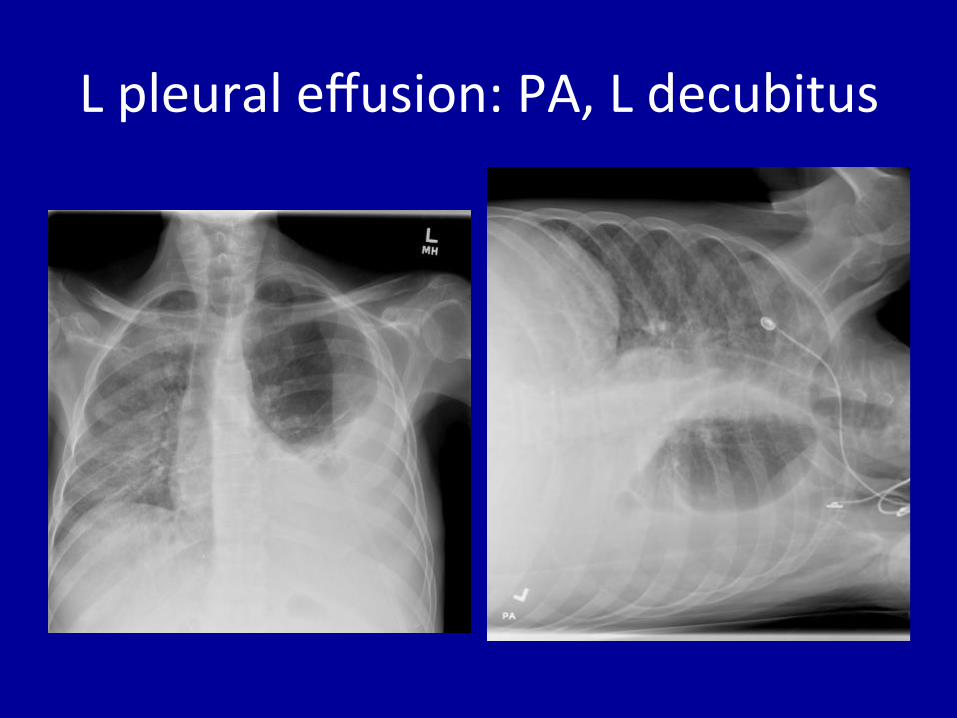
Lpleuraleffusion:PA,Ldecubitus

Case1:76yomalewithdyspnea
• Progressivedyspneafollowingaor:cvalvesurgery
• Peripheraledemanotedathip
• Generalizedweakness,failuretothrive

Case1:76yomalewithdyspnea
• Diagnos:cthoracentesisforfluidanalysis,withassociatedbloodwork
– Fluidprotein=1.6,FluidLDH=54– Serumprotein=6.1,SerumLDH=132
• Howisthefluidcharacterized?A. ExudateB. Transudate

TransudatevExudate
• Transudatesresultfromasystemicprocess(mostcommonlyCHF,hepa:cdisease,andrenaldisease)intheseongofnormalpleuraandrarelyrequirefurtherdiagnos:ctes:ngofthepleuralfluid
• Exudatesdevelopinseongoflungand/orpleuralpathology

TransudateversusExudate
• Importanttodifferen:ate– Narrowsdifferen:aldiagnosis– Exudateindicatesneedforfurtherdiagnos:ctes:ngofthepleuralfluid
• Light’sCriteria(onlyneed1)1. PleuralProtein:SerumProtein>0.52. PleuralLDH:SerumLDH>0.63. PleuralLDH>2/3ofUpperLimitNormalSerum

Case1:76yomalewithdyspnea
1. PleuralProtein:SerumProtein>0.5• 1.6/6.1=0.26
2. PleuralLDH:SerumLDH>0.6• 54/132=0.41
3. PleuralLDH>2/3ofUpperLimitNormalSerum• ULNserum=171;54not>2/3
MeetsnoneofLight’sCriteria;thusisaTRANSUDATEandrequiresnofurtherfluidtes:ng

Transudate:LimitedDifferen:alCommon• Conges:veHeartFailure• Cirrhosis• Nephro:csyndrome• Hypoalbuminemia
LessCommon• PE(usuallyexudate)• Associatedwithperitoneal
dialysis• Urinothorax• CSFLeak
• Treatment:Treatunderlyingcause• Mayrequiredrainageifverylarge,butlikelyto
recurifunderlyingcausenotaddressed.
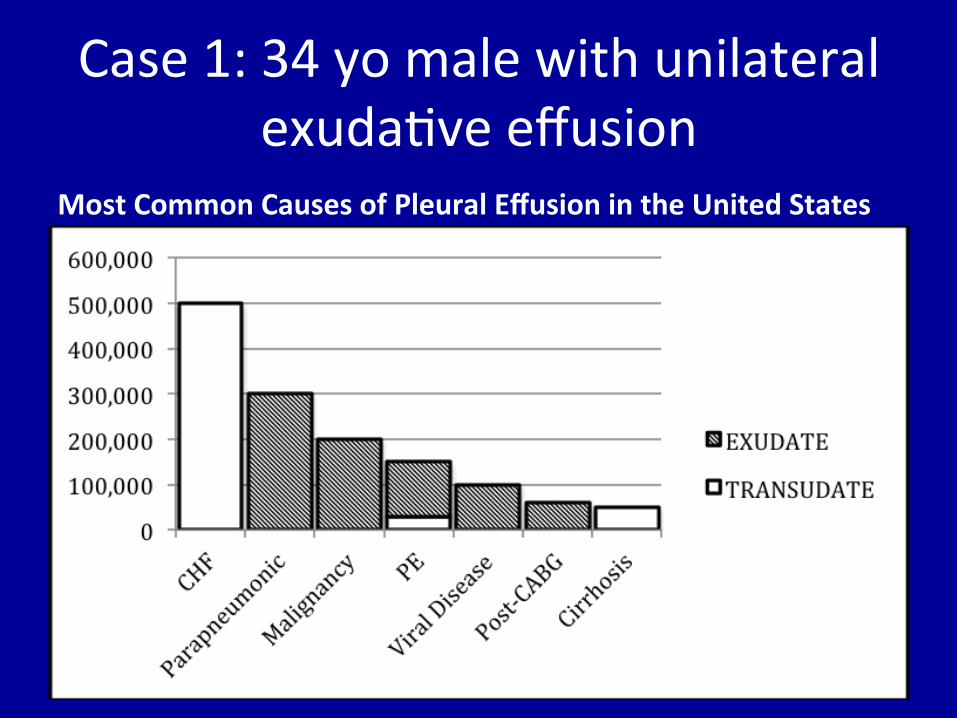
Case1:34yomalewithunilateralexuda:veeffusion
MostCommonCausesofPleuralEffusionintheUnitedStates

Case1:76yomalewithdyspnea

Case2:34yomalewithdyspnea
• 2weeksofworseningdyspneaonexer:on
• IntermiJentcoughproduc:veofbrownsputum,Rsidedchestpain
• Fevers,chills,anorexia• Recenthospitaliza:onforintoxica:on

Case2:34yomalewithdyspnea
• Diagnos:cthoracentesisforfluidanalysis,withbloodwork
– Fluidprotein=3,FluidLDH=12,000– Serumprotein=7,SerumLDH=246
• Howisthefluidcharacterized?A. ExudateB. Transudate

Case2:34yomalewithdyspnea
1. PleuralProtein:SerumProtein>0.5• 3/7=0.43
2. PleuralLDH:SerumLDH>0.6• 12,000/246=48
3. PleuralLDH>2/3ofUpperLimitNormalSerum• 12,000>>>>171
Meets2of3ofLight’sCriteria(onlyneededone);thusisanEXUDATEandrequiresfurtherdiagnos:ctes:ng

Case2:34yomalewithunilateralexuda:veeffusion
• Whatisthemostlikelycauseofhisexuda:veeffusion?
A. PneumoniaB. PulmonaryEmbolismC. MalignancyD. Conges:veHeartFailure

Case1:34yomalewithunilateralexuda:veeffusion
MostCommonCausesofPleuralEffusionintheUnitedStates

ParapneumonicEffusion• Mostcommoncauseofexuda:veeffusioninUnitedStates
• Complicates40-60%ofbacterialpneumonia• Parapneumoniceffusion,especiallyempyema,associatedwithincreasedmortality
• CommonOrganisms:– CAP:Streptococcus,Staphylococcus,anaerobes(Fusobacterium,Bacteroides,Peptostrepococcus)
– HCAP:Staph(MRSA),gram-nega:veaerobes(E.coli,Psuedomonas,Klebsiella)
• Highermortalitywithgram-nega:ves,Staph,andhospital-acquired

Case2:34yomalewithunilateralexuda:veeffusion
• Youobtainfurtherappropriatefluidstudiesinyourpa:ent,resul:ngwiththefollowing:– appearance:purulent– pH=7.0;glucose<10,WBC=unobtainable;gramstain:manyWBC,feworganisms
– cytology:nega:ve,AFB:nega:ve• Whatistheclassifica:onofthiseffusion?
A. UncomplicatedparapneumonicB. ComplicatedparapneumonicC. Empyema

Classifica:onofParapneumonicEffusion Uncomplicated Complicated Empyema
Imagingcharacteristics Free-7lowing Loculated,septated,orwithassociatedpleuralthickening.Mayalsobefree-7lowing;imagingcharacteristicsdonotruleoutcomplicatedeffusion
Anyofthecharacteristicsofcomplicated,ordense7luid/airloculessuggestiveofpus
Appearance Frankpus
Gramstain/Culture Negative Maybepositive +/-positivegramstain,culturemaybepositive
pH >7.2 <7.2 <7.0
Glucose >60 <60 <60
LDH <3XserumUNL >3XserumUNL >3XserumUNL(usuallyveryhigh)
• Cannotdifferen:ateuncomplicatedfromcomplicatedeffusionwithoutsamplingthefluid.
• Parapneumoniceffusionsofadequatesize(>10mmondecubitusfilm)mustbesampled,andcomplicatedparapneumoniceffusionsmustbedrained.
• Don’tforgetANTIBIOTICS!
REQUIREDRAINAGE

Case2:34yomalewithempyema

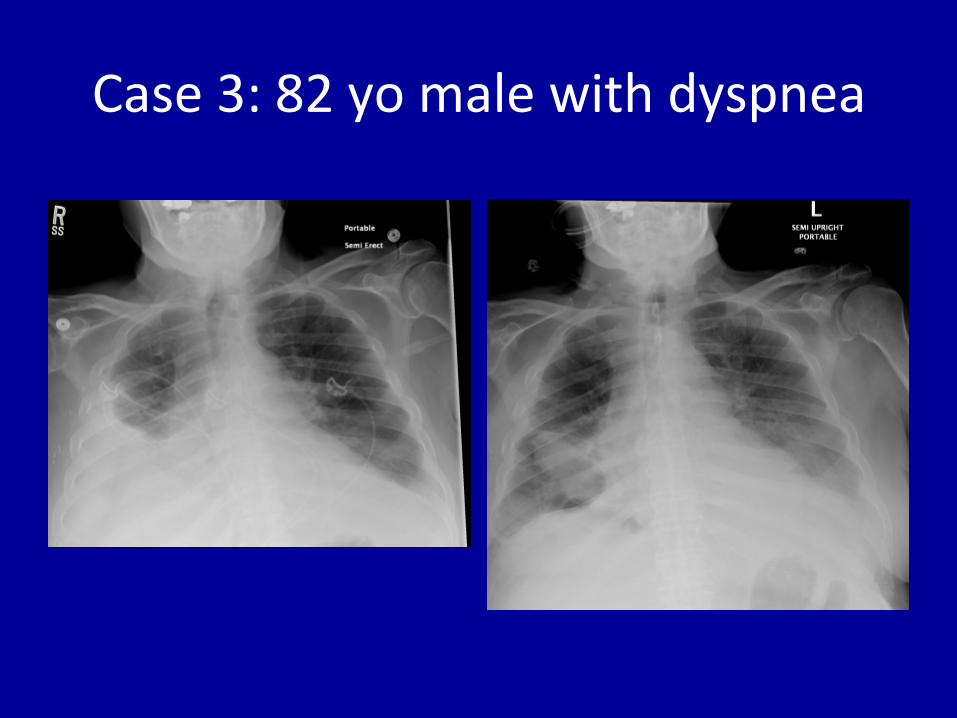
Case3:82yomalewithdyspnea
• Subacuteonsetofdyspneaonexer:on,nowatrest
• Fa:guedandfrail• HistoriesincludeRbreastcancer,CHF,andgallstonerequiringbiliarysurgery2monthspriortoadmission

Case3:82yomalewithdyspnea
• Diagnos:cthoracentesisforfluidanalysis,withbloodwork
– Fluidprotein=5.5,FluidLDH=148– Serumprotein=7.1,SerumLDH=139
• Exudate–nowwhat?

Undifferen:atedexudate:Rou:neStudies
Study IndicationAppearance Frankpus:empyema
Frankblood:possiblehemothorax(sendHct)Milky:chylothorax
CultureandGramStain EvalInfection.Sendinculturebottles
Cytology EvalMalignancy
CellCountandDifferential Seenextslide
GlucoseLevel <60indicatesinfection,malignancy,orrheumatoideffusion
pH <7.2indicatescomplicatedinfection,malignancy,rheumatoideffusion,esophagealleak

Exudate:CellCountGeneralCharacteristic PossibleDifferential
Macrophage-predominant(~75%) Normal
Neutrophil-predominant:Acutein7lammation
PneumoniaPulmonaryEmbolismSubdiaphragmaticAbscessAcuteTBConnectiveTissueDisease(Acute)
Lymphocyte-predominant:Chronicin7lammation
MalignancyConnectiveTissueDisease(Chronic)ChronicTB
Eosinophilia(>10%Eos):Non-speci7ic
Drug-inducedPneumothoraxMalignancyInfectionParasiticDisease

Undifferen:atedexudate:Rou:neStudies:Ourpa:ent
Study IndicationAppearance Orange-yellow,viscous
CultureandGramStain Negative
Cytology Pending
CellCountandDifferential Seenextslide
GlucoseLevel 79(<60indicatesinfection,malignancy,orrheumatoideffusion)
pH Notobtained(<7.2indicatescomplicatedinfection,malignancy,rheumatoideffusion,esophagealleak)

Exudate:CellCount–OurPa:ent
GeneralCharacteristic PossibleDifferential
Macrophage-predominant(~75%) Normal
Neutrophil-predominant:Acutein7lammation
PneumoniaPulmonaryEmbolismSubdiaphragmaticAbscessAcuteTBConnectiveTissueDisease(Acute)
Lymphocyte-predominant:Chronicin7lammation
MalignancyConnectiveTissueDisease(Chronic)ChronicTB
Eosinophilia(>10%Eos):Non-speci7ic
Drug-inducedPneumothoraxMalignancyInfectionParasiticDisease
WBCCount=400;76%L,14%M,8%N,1%E
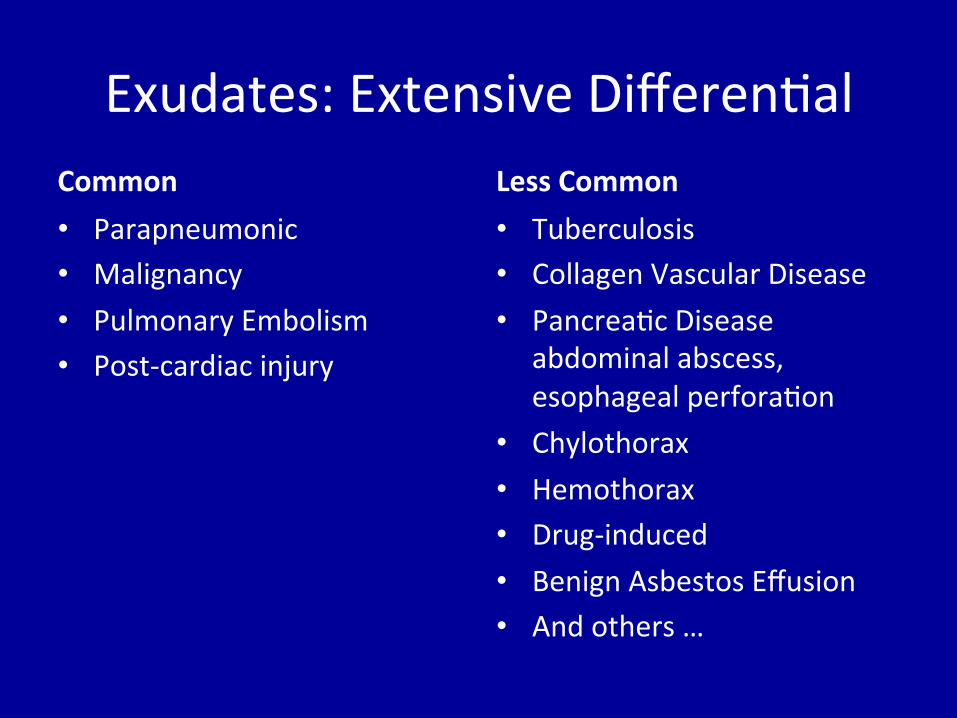
Exudates:ExtensiveDifferen:alCommon• Parapneumonic• Malignancy• PulmonaryEmbolism• Post-cardiacinjury
LessCommon• Tuberculosis• CollagenVascularDisease• Pancrea:cDisease
abdominalabscess,esophagealperfora:on
• Chylothorax• Hemothorax• Drug-induced• BenignAsbestosEffusion• Andothers…

Case3:82yomalewithdyspnea
• Whatfurtherstudieswouldyouobtain?A. AmylaseB. TotalbilirubinC. RheumatoidfactorD. AdenosinedeaminaseE. CTangiogramF. Allofthese?G. Noneofthese,I’msavinghealthcaredollars

AncillaryPleuralFluidStudiesTest Indication
Adenosinedeaminase(ADA) Tuberculosis
Interferon-gamma Tuberculosis
Amylase Pancreaticdisease,esophagealrupture
Hematocrit >50%ofserumHct:hemothorax
RheumatoidFactor Rheumatoideffusion
TriglycerideLevel,Chylomicrons Trig>110&plueral:serumcholesterol<1.0:chylothoraxChylomicrons+ive:chylothorax
Creatinine Urinothorax(transudate)
β2-transferrin Cerebrospinal7luidleak;suspectifpatienthasaventriculoperitoneal(VP)shuntorrecentthoracicspinesurgery(transudate)
TotalBilirubin Biliary-pleural7istula

TreatmentofNon-Infec:ousExudate
• Treatunderlyingcause• Localtreatmentdependsonsymptoms;unlikecomplicatedparapneumoniceffusionorempyema,drainageisnotrequired
• Simpledrainage,indwellingpleuralcathether,orpleurodesismaybeusedtotreatasymptoma:ceffusion,dependingonunderlyingcause
Case3:82yomalewithdyspnea

Pneumothorax
• Airinthepleuralspace(entersviabreachofchestwallorlung)
• Presen:ngfeatures:chestpain&dyspnea
• Examfindings:nofremitus,diminishedbreathsounds,hyper-resonantpercussionnote
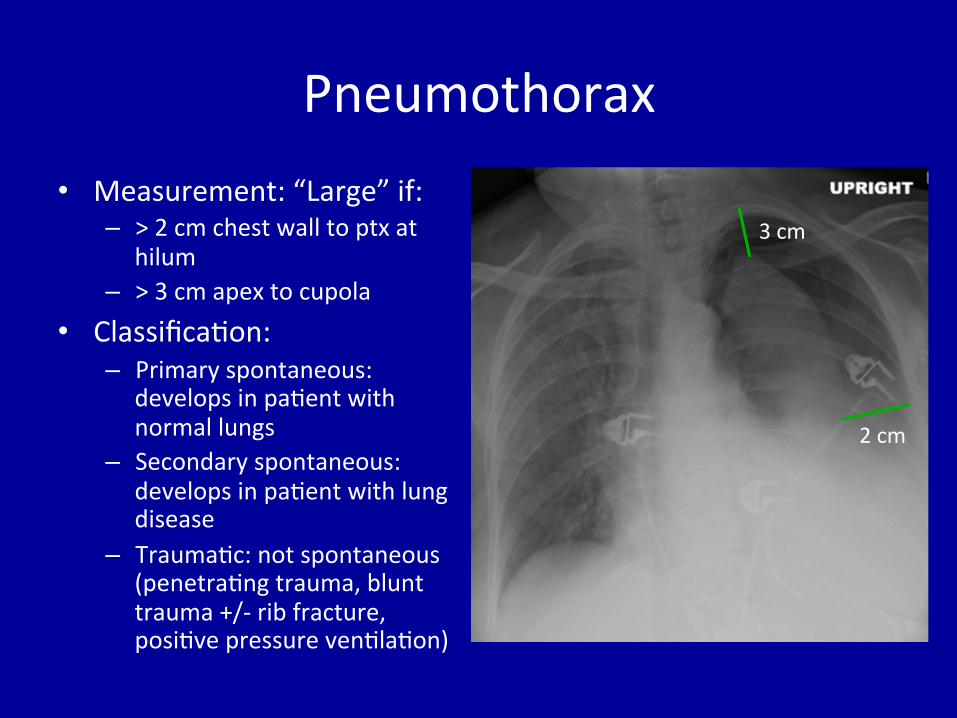
Pneumothorax• Measurement:“Large”if:
– >2cmchestwalltoptxathilum
– >3cmapextocupola• Classifica:on:
– Primaryspontaneous:developsinpa:entwithnormallungs
– Secondaryspontaneous:developsinpa:entwithlungdisease
– Trauma:c:notspontaneous(penetra:ngtrauma,blunttrauma+/-ribfracture,posi:vepressureven:la:on)
3cm
2cm

Pneumothorax:PrimarySpontaneous
• Spontaneousptxinpa:entwithnormallungs• Riskfactors:– CigareJesmoking– Malesex– Tallthinhabitus– Gene:cpredisposi:on(Marfan’s,Ehlers-Danlos,A1AT)

Pneumothorax:PrimarySpontaneous
• Pathogenesis:Possiblyruptureofsubpleuralblebs
• Treatment:dependsonsizeandsymptoms– Observa:on(verysmallptx,minimalsx)– Supplementaloxygen– Simpleaspira:on+/-indwellingtubeplacement– Sclerotherapyorsurgicalmanagement

Pneumothorax:SecondarySpontaneous
• Spontaneousptxinpa:entwithunderlyinglungdisease(COPD,lungcancer,fibrosis,bronchiectasis,etc)
• Poorlytoleratedduetolackofreserveforgasexchange;associatedwith>10%mortality
• Pathogenesis:abnormalparenchyma• Treatment:– Indwellingcatheterplacement– Surgicalmanagementorsclerotherapy,usuallyofferedwithini:aleventtopreventrecurrence

RecurrentPneumothorax
• Recurrenceratesrangefrom30-55%andarehigherinsecondarypneumothorax
• RiskFactors:Smoking,tall/thinhabitus• Sclerotherapyorsurgicalmanagementusuallypursuedat:meoffirstsecondarypneumothoraxd/thighriskofrecurrence
• Similarinterven:onspursuedforprimarypneumothoraxat:meoffirstrecurrence
IatrogenicPneumothorax:MechanicalVen:la:on
• MVdeliversposi:vepressureven:la:ontotherespiratorysystem,usuallyinseongofunderlyingparenchymaldisease
• Riskfactors:decreasedpulmonarycompliance,increasedpeakormeanairwaypressures(ex:ARDS)->leadingtoruptureofdistendedalveoli

DeepSulcusinSupineCXR

TensionPneumothorax
• Life-threateningemergency
• Riskfactors:posi:ve-pressureven:la:on• Pathophysiology:“One-wayvalve”phenomenon:airenterspleuralspaceandcan’texit

TensionPneumothorax
• Resultsinprogressivelyposi:vepleuralpressuremaintainedthroughouttherespiratorycycle
• Posi:vepleuralpressurecompromisesvenousreturnanddecreasescardiacoutput;ul:matelyprogressestoobstruc:veshockandcardiacarrest
NeJermedicalillustra:onusedwithpermissionofElsevier.Allrightsreserved.

TensionPneumothorax• Classicexamfindings:elevated
JVP,absentbreathsoundsonaffectedside,trachealshidawayfromaffectedside.Neednotallbepresent
• Treatment:mustallowposi:vepleuralpressuretoescapetolowerpressureenvironment(atmosphericpressure)->“decompression”ofthepleuralspace– needlethoracostomy– tubethoracotomy
NeJermedicalillustra:onusedwithpermissionofElsevier.Allrightsreserved.
PleuralTumors
• Metasta:corprimary• Frequentlyassociatedwitheffusion
• Metasta:cinvolvementmostcommonlyfrom3primaries:– LungCancer– BreastCancer– HematologicMalignancy(Lymphoma,Leukemia)

PrimaryPleuralTumors
• Rare:Solitaryfibroustumorofthepleura(mesenchymalorigin),usuallybenign
• Morecommon:MalignantPleuralMesothelioma
MalignantPleuralMesothelioma
• Epidemiology:U.S.incidence~10permillion,with~2500U.S.deaths/year,decliningduetodecreaseinasbestosexposure
• RiskFactors:Asbestosfiberexposure(carpentry,plumbing,ship-building,pipe-fiong,brakework,insula:on).Prolongedlatencyperiod–20-40yearsfrom:meofexposure.– 80%ofmesotheliomacasesarerelatedtoasbestos– Developsin~10%ofpersonswithexposurehistory

MalignantPleuralMesothelioma
www.cdc.gov.MMWRWeeklyReports2009:58(15);393-396.AccessedOctober2015.f/cc:fibers/cubiccen:meter;averagedoveran8-hourshid,limitsperOSHA

MalignantPleuralMesothelioma
• Clinicalfindings:chestpain,dyspnea,pleuralthickeningonchestimaging,+/-pleuralplaques,frequentlyeffusion
• Diagnosis:Requirespleuralbiopsy
• Histology:Maybeepitheliod,sarcomatoid,ormixed hJp://radiopaedia.org/encyclopaedia/cases/all
Credit:DrAhmedAbdRabou

MalignantPleuralMesothelioma• Staging:
– T1:ipsilateralpleura(parietalonly:T1a;visceral:T1b)withoutdeepextension– T2:involvesen:reipsilateralpleuraandextendstodiaphragmorlung– T3:locallyadvanced(mayinvolvefascia,medias:nalfat,chestwall,par:al
pericardium)but“poten:allyresectable”– T4:unresectable:contralateralpleura,transmuralpericardium,medias:nal
organs,peritoneum,diffuseextensionthroughchestwall
– N0:Nonodes– N1:ipsilateralhilar/bronchopulmonarynodes– N2:subcarinal,ipsilateralmedias:nal,nodes– N3:contralateralnodes
– M0:nomets– M1:mets

MalignantPleuralMesothelioma
• Treatment:Primaryfocusispallia:onofdyspneaandchestwallpain– Pleurodesis– Surgical(radicalpleurectomyanddecor:ca:on,extrapleuralpneumonectomy)–selectedcases,notconsideredstandardofcare
– Chemotherapy(pemetrexedandcispla:n)– +/-Radia:on
• Prognosis:poor,mediansurvival8-12monthsfromdiagnosis.– Worseprognos:cfactors:olderage,worseperformancestatus,non-epithelioidhistology,malegender,leukocytosis
• Survivalbenefitsoftreatmentareunconvincinginmostpa:ents