polypoid cystitis -...
TRANSCRIPT

path. microbiol. scand. Sect. A, 87: 179-184, 1979.
POLYPOID CYSTITIS
.. A Catheter Associated Lesion of the Human Bladder
PETER EKELUND and SONNY JOHANSSON
Geriatric clinic I, Vasa hospital and Department of Pathology II, Sablgren's hospital, University of
Goteborg, Goteborg, Sweden
Ekelund, P. & Johansson, S. Polypoid cystitis, a catheter associated lesion of the human bladder. Acta
path. microbial. scand. Sect. A, 87: 179-184, 1979.
Histopathological examination of the urinary bladders of 63 patients dying in a geriatric clinic was
performed. In 40 of 51 patients who had been treated with a urinary catheter, histological changes of
polypoid cystitis were found. In 34 of the bladders the lesion engaged the posterior wall which
corresponds to the localization of the tip of the catheter. The frequency of polypoid cystitis increased
with increasing time of catheter treatment and reached its peak. by three months. After that time the
frequency was relatively constant. The frequency of polypoid cystitis seemed not to be influenced by
bacterial urinary tract infection. Urothelial atypia was not seen after catheter treatment.
Key words: Urinary bladder; catheter; polypoid cystitis.
Sonny Johansson, Department of Pathology 11, University of Goteborg, Sahlgren's hospital. S-413 45
Goteborg, Sweden.
IJ.xi.78 Accepted 5,xii.78
A number of inflammatory and reactive lesions a characteristic histological appearance in the
bladder have been described, e.g. cystitis and glandularis, follicular cystitis, interstitial
radiation cystitis, giant cell cystitis, and
malakoplakia (/(oss I974). Polypoid cystitis is a term used by Friedman & Ash (1959) for a vesical growth which may simulate neoplaSf!l macroscopi
but was considered to be inflammatory, "A'""''A.,.,,.and reactive in origin, They illustrated
a case in a 23-year-old man without apparent cause, which Koss (1974) considered to be exceptional. The
study is a histopathological examination of the urinary bladder from 63 consecutive patients
dying in a geriatric clinic.
MATERIAL AND METHODS
Se.>; a11d age: Thlrty-four of the patients were males :and
29 females, with a mean age of 79 years (range 45- 99).
Twelve of the patients had never been treated with a
urinary catheter, the remaining patients had used
catheters for varying lengths of time. The charts and the
clinical records were examined with particular reference
to diseases of tile minary tract, especially urinary tract
infection.
Morplzological methods: Thirty minutes after the patients
were declared dead by a physician, the urinary bladder
was filled with I SO cc 4 per cent formaldehyde solution
in order to achieve acceptable histological fixation. The
pelvic organs were removed en bloc, the urinary bladder
was bisected and inspected, and multiple sections were
taken from the urethra and prostate, trigone, posterior
wall, dome, and left and right lateral walls. Five )lm
sections were stained with hematoxylin and eosin and
according to Weigert-vanGieson.
RESULTS
Clinical results: The patients were old and had often
several major diseases, e.g. 19 of them had malignant tumours in a terminal stage, and 33 patients suffered from cardiovascular diseases inclu
ding diabetes, hypertension and cerebral hemorr hage or infarction.
179

a .
TABLE I .The Correlation between Time ofCMheter Treatment and Incidence of Urinary Tract Infection in 63 Patie1115
Urinary tract
infection
T€
Time of catheter treatment (months) m
ol
0 <I 1-3 3--6 6-12 12-24 >24 Total
tr Negative 9 6(4) 3(3) I(I) I(I) 0 0 20
Positive 3 7(4) 7(6) 4(3) 6(4) 8(7) 8(7) 43
Total 12 13 10 5 7 8 8 63
The numbers within brackets indicate patients with polypoid cystitis.
TABLE 2. The Frequency of Di[{ere/11 Histopat/w/ogica/ Changes of the Urinary Bladder and Prostate in 63 Patienls after Different Times of Catheter Treatmew
Time of catheter treatment (months)
o!
ir p;
IT
tt b;
c:
tv. u
p
I
fl
tl
..
Morphological
0
<I 1-3
3--6
6-12
12-24
>24
lesion n = 12 n ::: 13 n = 10 n :::: 5 n = 7 n =8 n=8
Polypoid cystitis
8
9
4
5
1
7
von Brunn's nest 5
5 5
2 4
J
4
t Severe inflammation ...
,. with contracted bladder
2 3 4
Diverticuli
2
3
Squamous
metaplasia 2 2
Bladder calculi
Follicular
cystitis
Benign prostatic
hyperplasia 6 6 3 3 4 3
Prostatic
adenocarcinoma 2 2 3
»Normal(( bladder 7
2
180

! .
Traer bifecrioll in 63 Patients
tts)
-24 >24 Total
0 0 20
:7) 8(7} 43
8 63
and Prostate in 63 Patients
1 2-24 >24
n=8 n=8
7 7
3 4
In 43 patients urinary tract infection was recorded (positive urine cultures or urine sediment), and in 20 patients this could not be verified. Three of 12 patients who had not been treated with a Foley catheter bad bacterial urinary tract infection. Table
1 gives the correlation between time of catheter treatment and urinary tract infection. TM incidence of urinary tract infection seems to increase with
.increasing time of catheter treatment. AU the patients who had had a urinary catheter for 12 months or more had urinary tract infection. Nine of the II catheter treated patients without evidence of bacterial urinary tract i11fection had polypoid cystitis. Morphological results: Macroscopical lesions of the urinary bladder were seen in twelve cases. The pathological area exhibited polypoid or bullous lesions up to 0.5 em in diameter. The mucosa appeared oedematous and often hemorrhagic. The frequency of different histopathological changes of the urinary bladder and prostate is given in Table 2.
Altogether, polypoid cystitis (see below) was found in 40 bladders: 22 men and 18 women.In 28 of the patients the lesion was only microscopical. TI1e frequency and localization of polypoid cystitis is given inTable 3. Thus in 34/40 cases the polypoid cystitis involved the posterior wall (Fig. 1). All U1e three patients who had involvement of the entire bladder had been using callieters for more than six months. Polypoid cystitis was not found in any of the patients who had not been using a urinary catheter.
Microscopically the lesions were polypoid, some times bullous or papillary (Figs. 2-4). Urothelial hyperplasia of mild deg.ree was frequently found,
and the urotheliom often contained small micro abscesses. The underlining lamina propria was oedematous, often willi abundant inflammatory cells, particularly polymorphous leucocytes and lymphocytes. In association with the oedematous areas, an increased number of capillaries and . ' sometimes larger ectatic vessels were seen. Signs of recent and old hemorrhage were also common (Fig.
4
3
4 3
3
Fig. 1. Localization of the tip of the catheter in the posterior wall.
181 l .;
Greg
D:20091104092731-05'00'11/4/2009 9:27:31 AM
-------------------------------------
------- showing direct
contact with catheter tip

Fig. 2. Combined oolypoid and papillary lesion after 4 months of catheter treatment. Hrx & eo x 90.
Fig.
mics cath
5).
bee1
tl\01
witl (Fig
Th catl
cal mo blao
Th1
lar: anc
cap inil lesi bee
Fig. 3. BuUous lesion with urothelfal hyperplasia, prt>minent oedema, and mild inflammation after 2 months of ye<
catheter treatment. Htx & eo x 120. J (IS
1 82
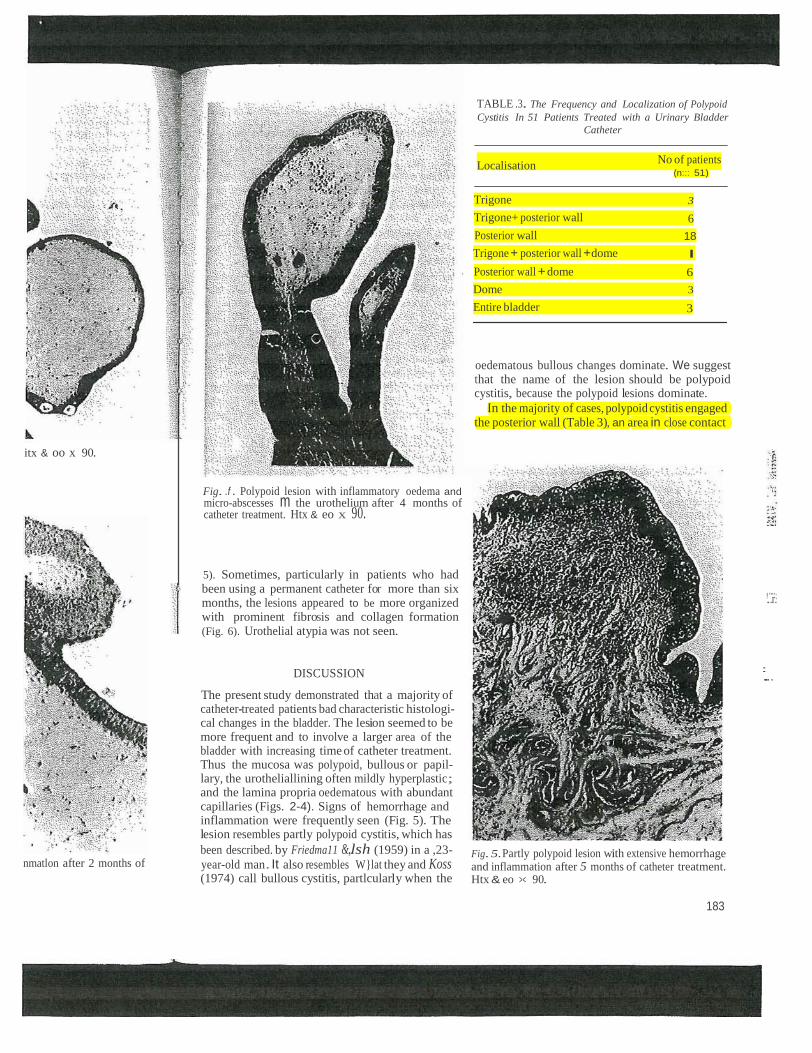
TABLE .3. The Frequency and Localization of Polypoid
Cystitis In 51 Patients Treated with a Urinary Bladder
Catheter
Localisation No of patients
(n::: 51)
Trigone 3
Trigone+ posterior wall 6
Posterior wall 18
Trigone + posterior wall +dome I
Posterior wall + dome 6
Dome 3
Entire bladder 3
oedematous bullous changes dominate. We suggest that the name of the lesion should be polypoid cystitis, because the polypoid lesions dominate.
In the majority of cases, polypoid cystitis engaged the posterior wall (Table 3), an area in close contact
itx & oo x 90.
Fig. .f . Polypoid lesion with inflammatory oedema and micro-abscesses m the urothelium after 4 months of catheter treatment. Htx & eo x 90.
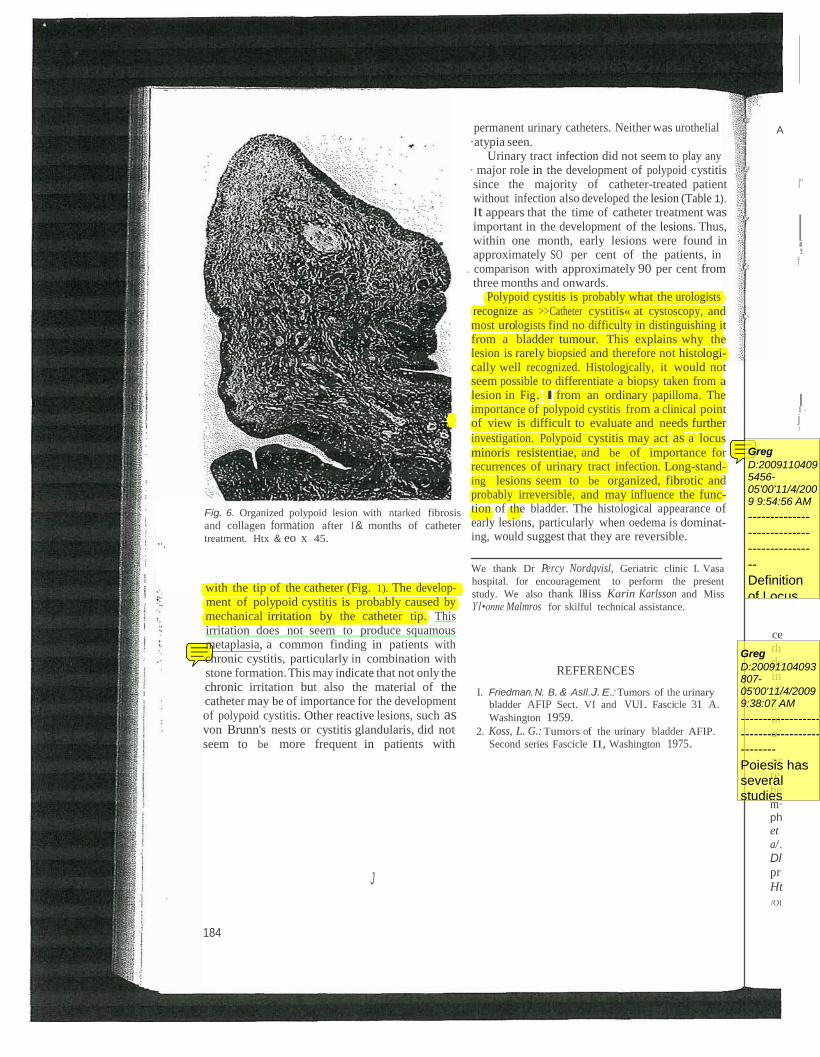
5). Sometimes, particularly in patients who had been using a permanent catheter for more than six months, the lesions appeared to be more organized with prominent fibrosis and collagen formation (Fig. 6). Urothelial atypia was not seen.
!.".r''.;
nmatlon after 2 months of
DISCUSSION
The present study demonstrated that a majority of catheter-treated patients bad characteristic histologi cal changes in the bladder. The lesion seemed to be more frequent and to involve a larger area of the bladder with increasing time of catheter treatment. Thus the mucosa was polypoid, bullous or papil lary, the urotheliallining often mildly hyperplastic; and the lamina propria oedematous with abundant capillaries (Figs. 2-4). Signs of hemorrhage and inflammation were frequently seen (Fig. 5). The lesion resembles partly polypoid cystitis, which has
been described. by Friedma11 &,..lsh (1959) in a ,23-
year-old man. It also resembles W}lat they and Koss (1974) call bullous cystitis, partlcularly when the
Fig. 5.Partly polypoid lesion with extensive hemorrhage and inflammation after 5 months of catheter treatment. Htx & eo >< 90.
183
.=...
I
··.
Fig. 6. Organized polypoid lesion with ntarked fibrosis
and collagen formation after I & months of catheter treatment. Htx & eo x 45.
with the tip of the catheter (Fig. 1). The develop ment of polypoid cystitis is probably caused by mechanical irritation by the catheter tip. This irritation does not seem to produce squamous metaplasia, a common finding in patients with chronic cystitis, particularly in combination with stone formation. This may indicate that not only the chronic irritation but also the material of the catheter may be of importance for the development
of polypoid cystitis. Other reactive lesions, such as von Brunn's nests or cystitis glandularis, did not
seem to be more frequent in patients with
J
184
permanent urinary catheters. Neither was urothelial
·atypia seen. Urinary tract infection did not seem to play any
· major role in the development of polypoid cystitis since the majority of catheter-treated patient without infection also developed the lesion (Table 1).
It appears that the time of catheter treatment was important in the development of the lesions. Thus, within one month, early lesions were found in approximately SO per cent of the patients, in
. comparison with approximately 90 per cent from three months and onwards.
Polypoid cystitis is probably what the urologists
recognize as >>Catheter cystitis« at cystoscopy, and most urologists find no difficulty in distinguishing it from a bladder tumour. This explains why the lesion is rarely biopsied and therefore not histologi cally well recognized. Histologjcally, it would not seem possible to differentiate a biopsy taken from a
lesion in Fig. I from an ordinary papilloma. The importance of polypoid cystitis from a clinical point of view is difficult to evaluate and needs further
investigation. Polypoid cystitis may act as a locus
minoris resistentiae, and be of importance for recurrences of urinary tract infection. Long-stand ing lesions seem to be organized, fibrotic and probably irreversible, and may influence the func tion of the bladder. The histological appearance of early lesions, particularly when oedema is dominat ing, would suggest that they are reversible.
We thank Dr Percy Nordqvisl, Geriatric clinic I. Vasa
hospital. for encouragement to perform the present
study. We also thank ll•liss Karin Karlsson and Miss
Y1•onne Malmros for skilful technical assistance.
REFERENCES
I. Friedman. N. B. & Asll.J. E.: Tumors of the urinary
bladder AFIP Sect. VI and VUI. Fascicle 31 A.
Washington 1959. 2. Koss, L. G.: Tumors of the urinary bladder AFIP.
Second series Fascicle II, Washington 1975.
A
I"
i !
f
I I· j 1
ce
th de in
(C
h< in
a/ pr
re·
be
m· ph
et
a/ .
Dl
pr
Ht
/Ol
Greg
D:20091104093807-05'00'11/4/2009 9:38:07 AM
--------------------------------------------
Poiesis has several studies which confirm to the contrary that catheters increase bladder cancer by 8-10%
Greg
D:20091104095456-05'00'11/4/2009 9:54:56 AM
--------------
--------------
--------------
--
Definition
of Locus
minoris
resistentia
e
Locus
minoris
resistentiae
: Latin
meaning a
place of
less
resistance.
A locus
minoris
resistentiae
offers little
resistance
to
microorgani
sms. For
example, a
damaged
heart valve
acts as a
locus
minoris
resistentiae
, a place
where any
bacteria in