portsmouth hospitals nhs trust dr david prytherch and dr jim briggs health care computing group...
Post on 22-Dec-2015
219 views
TRANSCRIPT

Portsmouth HospitalsNHS Trust
Dr David Prytherch and Dr Jim BriggsHealth Care Computing GroupUniversity of Portsmouth
Mr Paul Weaver and Dr Paul Schmidt, University of Portsmouth
Professor Gary Smith, Portsmouth Hospitals NHS Trust, University of Bournemouth
Measuring clinical performance using routinely collected clinical data.

Portsmouth HospitalsNHS Trust
………Hospitals and the NHS could tell you about throughput (number of patients treated), bed occupancy (the proportion of beds occupied in the hospital), and, latterly, the costs involved. But, generally speaking, quality of outcome was a closed book.
Why look at Clinical Outcomes?
At national level, the indicators of performance should be comprehensible to the public as well as to healthcare professionals. They should be fewer and of high quality, rather than numerous but of questionable or variable quality.
Why Mortality?
“Learning from Bristol”:The Report of the Public Inquiry into children’s heart surgery at the Bristol Royal Infirmary 1984 to 1995. I Kennedy, HMSO 2001

Portsmouth HospitalsNHS Trust
…… Variables such as case mix and where possible, in the case of surgery, operative risk must be allowed for, so that, wherever feasible, it is possible to compare like with like.
“Learning from Bristol”:The Report of the Public Inquiry into children’s heart surgery at the Bristol Royal Infirmary 1984 to 1995. I Kennedy, HMSO 2001
Why case-mix adjust?
For the future the multiple methods and systems for collecting data must be reduced. Data must be collected as the by-product of clinical care.
How to collect the data?

Portsmouth HospitalsNHS Trust
Measuring Clinical Performance
How do you measure clinical performance?
You need to know what you expect – predicted outcomes. Compare predicted with reported.
How do you predict outcomes?
Case mix adjusted models
Why case mix adjust?
To gain clinician engagementTo answer “my results are worse than … because my patients are sicker”
Essentially it provides a ruler

Portsmouth HospitalsNHS Trust
How do you case mix adjust?
Use clinical data that encapsulates the physiological state of the patient
Use this to predict a risk of “adverse outcome”
Trick is to collect necessary data in the clinical environment

Portsmouth HospitalsNHS Trust
Aim of study was to see if data stored in core hospital systems could be used to predict (case mix adjust) clinical outcomes.
Data from: PASBiochemistry and Haematology modules of pathology system
Data already collected / exists. No additional administrative or clinical burden.
BHOM: Biochemistry and Haematology Outcome Modelling

Portsmouth HospitalsNHS Trust
results adapted from: The use of routine laboratory data to predict in-hospital death in medical admissionsD R Prytherch, J S Sirl, P Schmidt, P I Featherstone, P C Weaver, G B
Smith. Resuscitation 2005; 66: 203-207
First demonstration of outcome prediction for General MedicineData from PAS and Biochemistryand Haematology modules of pathology system
1st January 2001 - 31st December 2001
9497 discharges from GM with necessary dataModel developed from Q1 and applied prospectively against Q2, Q3 and Q4
e.g., BHOM in General Medicine

Portsmouth HospitalsNHS Trust
•Urea•Albumin•Creatinine•Na•K•Haemoglobin•White Cell Count•Age on admission•Sex•Mode of admission•Mortality at discharge
Data items used in models for General Medicine:

Portsmouth HospitalsNHS Trust
Risk (%) Dis-charges
Mean Risk (%)
Predicted Deaths
Reported Deaths
2
0 to 5 1279 2.27 29 35 1.27
>5 to 7.5 265 6.49 17 20 0.48
>7.5 to 10 321 8.86 28 24 0.76
>10 to 12.5
164 11.48 19 20 0.08
>12.5 to 15
169 14.00 24 31 2.65
>15 to 20 154 17.78 27 28 0.02
>20 to 25 72 22.90 16 14 0.49
>25 to 33 78 28.69 22 20 0.36
>33 to 50 28 40.25 11 8 1.59
>50 to 100 14 64.21 9 8 0.31
0 to 100 2544 8.01 204 208 8.00
2 = 8.00
10 d.f
P = 0.63
no evidence of lack of fit
c-index=0.757
General Medicine StudyFinal 3 month period 1st October – 31st December 2001

Portsmouth HospitalsNHS Trust
General Medicine - Mortality at Discharge
Monthly, J anuary 1998 to December 2001
0
20
40
60
80
100
120
Predicteddeaths
Reporteddeaths
p-value
(prospective)
45 df = 0.11
General Medicine StudyTotal Mortality through time – 1st January 1998 to 31st December 2001 (37283 discharges)

Portsmouth HospitalsNHS Trust
Excess of reported vs predicted deaths per month in General Medicine Jan 98 to December 2001
-20
-15
-10
-5
0
5
10
15
20
25
30
01-9
8
03-9
8
05-9
8
07-9
8
09-9
8
11-9
8
01-9
9
03-9
9
05-9
9
07-9
9
09-9
9
11-9
9
01-0
0
03-0
0
05-0
0
07-0
0
09-0
0
11-0
0
01-0
1
03-0
1
05-0
1
07-0
1
09-0
1
11-0
1
December 99 and January 2000 show statistically significant excess. Bed availability problems and flu.
Use to identify periods when performance deviates from norm
Portsmouth HospitalsNHS Trust
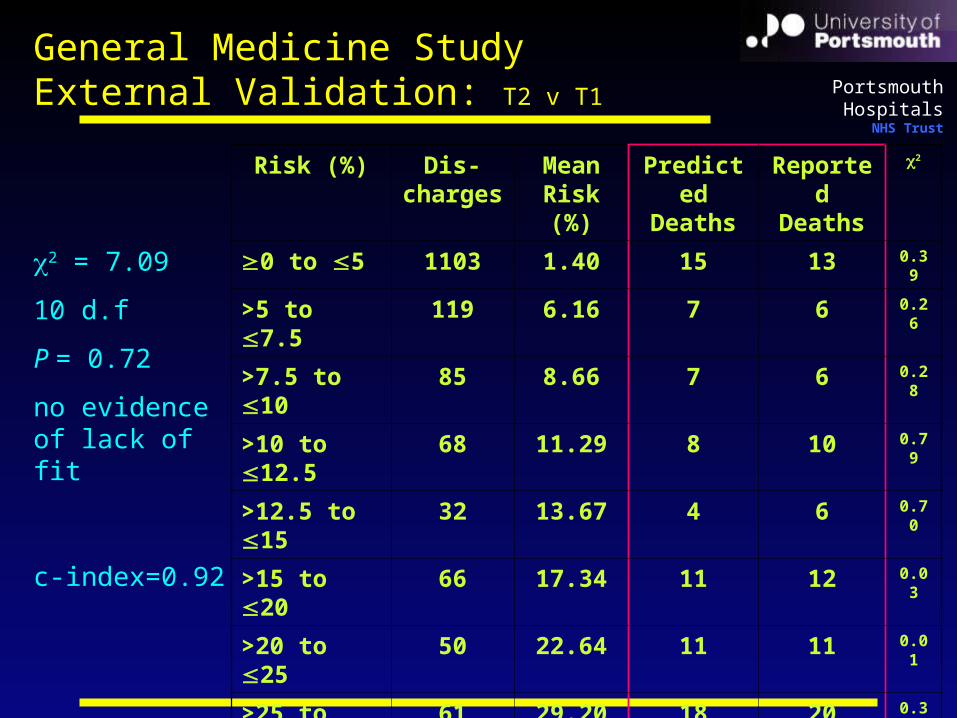
Risk (%) Dis-charges
Mean Risk (%)
Predicted Deaths
Reported Deaths
2
0 to 5 1103 1.40 15 13 0.39
>5 to 7.5 119 6.16 7 6 0.26
>7.5 to 10 85 8.66 7 6 0.28
>10 to 12.5
68 11.29 8 10 0.79
>12.5 to 15
32 13.67 4 6 0.70
>15 to 20 66 17.34 11 12 0.03
>20 to 25 50 22.64 11 11 0.01
>25 to 33 61 29.20 18 20 0.38
>33 to 50 90 40.71 37 36 0.02
>50 to 100 93 74.58 69 78 4.24
0 to 100 1767 10.68 189 198 7.09
2 = 7.09
10 d.f
P = 0.72
no evidence of lack of fit
c-index=0.92
General Medicine StudyExternal Validation: T2 v T1

Portsmouth HospitalsNHS Trust
Clinical data obtained from a single venesection
Clinical data are used operationally in care of individuals
All data already stored on hospital core IT systems - no “extra” effort is required to collect data
Clinical data used are subject to extensive quality assurance
Key points: 1

Portsmouth HospitalsNHS Trust
Case mix adjusted and uses high quality data trusted by clinicians (no coded data) – more likely to win clinical acceptance
Data immediately available to inform decisions
Cannot be “gamed”
Performance and surveillance tool
Key points: 2

Portsmouth HospitalsNHS Trust
National Application of BHOM
Vascular Society of Great Britain and Ireland National Vascular Database (Risk adjusted predictive models of death after index arterial operations using a minimal data set.D R Prytherch, BMF Ridler, S Ashley on behalf of the Audit and Research Committee VSGBI, Br J Surg 2005; 92: 714-718)
NCEPOD (National Confidential Enquiry into
Patient Outcome and Death) study into Abdominal Aortic Aneurysm www.ncepod.org.uk

Portsmouth HospitalsNHS Trust
Portsmouth NHS R&D Consortium
Portsmouth Hospitals NHS Trust
University of Portsmouth
Sources of funding