positive deviance: innovative responses to healthcare reform
DESCRIPTION
Positive Deviance: Innovative Responses to Healthcare Reform. Dr. Rick Cartor, Director, ChD, LLC HR/OD Consultant @ BB&T Insurance Louisville, KY. Positive Deviance: Innovative Responses to Healthcare Reform. Outline and Goals The HCR context - PowerPoint PPT PresentationTRANSCRIPT

Positive Deviance: Innovative Responses to Healthcare Reform
Dr. Rick Cartor, Director, ChD, LLC HR/OD Consultant @ BB&T Insurance
Louisville, KY
http://rickcartor.wordpress.com 1

Positive Deviance: Innovative Responses to Healthcare Reform
1. Outline and Goals2. The HCR context3. Key Player Responses: Payers, Providers, Users4. Users: Obstacles to Innovation
– Overcoming the Obstacles
http://rickcartor.wordpress.com 2

http://rickcartor.wordpress.com 3
NOT-a thorough review of PPACA-a debate on PPACA merits-a how to for specific mandates-a how to for being deviant
Positive Deviance: Innovative Responses to Healthcare Reform
The GOALS of this session are: 1. understand how key players are responding to healthcare
reform so employers can find ways to survive and thrive2. enable participants to recognize and overcome common
obstacles to innovative solutions in healthcare benefit design.

Positive Deviance
…the observation that in any community, there are people whose uncommon but successful behaviors or strategies enable them to find better solutions to a problem than their peers, despite facing similar challenges and having no extra resources or knowledge than their peers.
http://rickcartor.wordpress.com 4
E.g.: Malnourished children Viet Nam; Pregnancy in Uganda, Hand washing (MDs) From: Positive Deviance, Appreciative Inquiry, Switch, Checklist Manifesto
“Necessity is the mother
of invention.”
There are many in thissimilar situation
Resist the tendency to act alone
http://rickcartor.wordpress.com 5
-exceptional complexity -ongoing requirements-a likely increase in costs -ambiguous terms -unique exceptions -shifting deadlines -penalties for errors-few (or no) experts -increased auditing
The “Similar Challenge”

But not identical!
States “high quality affordable care”
SOLUTIONS VARY….• Population (size, demographics)• Geography (size, concentration) • Politics / philosophy re: state/fed • Economic condition• Healthcare history (current status) • Healthcare governance and regulations • Insurance laws / regulations• Penchant for Innovation
The “Similar Challenge”
But the key players remain the same – and
are each adapting

7
$-Payer
+ Provider User / group

8
$-Payer
Diversify:New products / M&A• stop loss; level premium• ASO/TPA• Data salesMedical management• IT services (exchanges)• Wellness programs• Care & Clinics• Telemed / kiosks• DM
Retail:• Indiv / small group• 90+% covered• 50% fewer via broker• ¾ direct to consumer• Bare minimum / EB• States’ M&M
Cost:1. Relationshipsa. Provider focused:
• Collab w providers• Shift risk: Pay for Perf
• Outcome based• ACOs / Med Homes
• Narrow Networks
b. Member focused:• Modify behaviors
PreventiveTransparencyRx tiers2. Admin costs
• Technology: Auto enroll; • adjudication, portals
• Simplify for exchanges• Outsource / offshore

2011 2019Not covered 49 27 -22Medicaid 48 59 +11Medicare 48 60 +12Individual 18 31 +13Employer 145 157 +12Total 308 334 +26

Younger, more male & whiteLess obese, more smokers & drinkers

11
+ Provider
Quality, Cost OutcomesDirect Employer contactPopulation management ACO / PCMH/ PCP nets On site clinics Managed Care / Integrated carePhysician practices Networks, narrowPhysician extenders / PA
Related Diversific• Wellness• Biomets • Lab work• Targeted DM• TPA• HCIT• EAPs
New entrants: WalMart, mini-clinics, Primary Care clinics,Wellness & biometrics,MD2U, DM,Labs (franchises!)

12User / group
FTE/PTE: hours
INCREASE PREVENTIONEncouraging Essential benefitsWellness
Premium incentives for employees
Carrot / stickRewards for P’ then resultsdrawings vs. rewardscontestsOnsite coaches (w + DM)
Chronic costs/ non-adherenceOn site near site / shared solo clinics
Primary care externedersReduce ICC & ER
Telemedicine and KiosksMedical homesPolicies / Reward redesigns
Hiring practicesfood on site, fit bits, clubs,On site fitnessRewards for PCPDEPENDENT AUDITSPURCHASING COALITIONSTRANSPARENCY TOOLS
ATTN TO PROVIDERS AND PAYERS
PROVIDER CONCESSIONSPremium rebates Premium discounts (W, PCC, etc)Related discounts (LTD for PCC)TPA/ASOSelf-funding Lower stop loss (spec/agg)
Level premium
PARTNERSHIPSConsultants v brokerData demands analyticsManaged care / Population
management / ACO BC3Inpatient Care:
Narrow networks, tiers, steerPass through Rx; tiers, incentives
mail, generics, partner, unbundle
COMMUNITY RATING: associations, captives; private exchanges
<4950-100101+

http://rickcartor.wordpress.com 13
15 MISTAKEN Beliefsthat KILL innovative healthcare benefit
design within
Beliefs and Assumptions about:
(A) Healthcare in general(B) How to find a solution(C) How to implement a solution
User groups

http://rickcartor.wordpress.com 14
1. U.S. healthcare is unfixable2. There are no good solutions3. Healthcare decisions are separate from…4. SSDD
MISTAKEN BELIEFS & ASSUMPTIONS ABOUT…
(A) HEALTH CARE IN GENERAL
http://rickcartor.wordpress.com 15
5. In bounds & out of bounds6. Criteria: unclear, unstated, assumed...7. We have to think in 12 month cycles8. We have to settle for insufficient data9. We have no partners - but many adversaries10. “Innovative” = high risk
• Uncommon, Fast Follow, Early Adopter, 11. Things will settle down soon…one answer
MISTAKEN BELIEFS & ASSUMPTIONS ABOUT…
(B) HOW TO FIND A SOLUTION
http://rickcartor.wordpress.com 16
12. I will never be able to convince...13. It won't work here / for us because... 14. We already…15. We tried that one time...
I don’t have the time
MISTAKEN BELIEFS & ASSUMPTIONS ABOUT…
(C) IMPLEMENTING THE SOLUTION

To achieve innovative benefit design within an organization you must expect &
overcome the 15 Killers
http://rickcartor.wordpress.com

A Method to Overcome the 15 Killers
http://rickcartor.wordpress.com
SeekStructure& Steal
http://rickcartor.wordpress.com
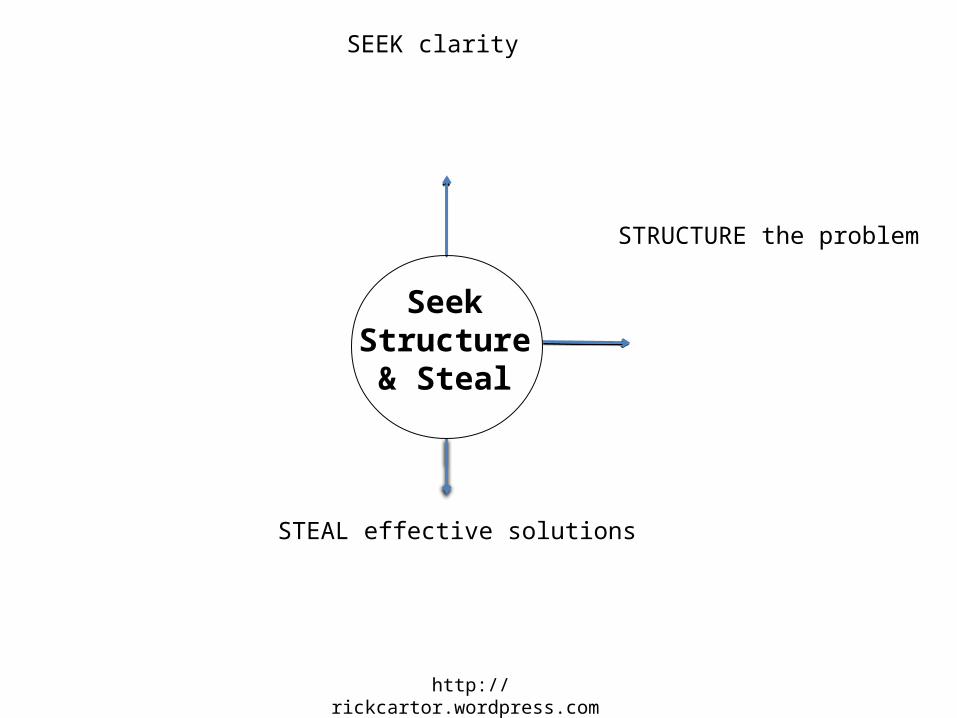
SeekStructure& Steal
SEEK clarity
STRUCTURE the problem
STEAL effective solutions

http://rickcartor.wordpress.com
SeekStructure& Steal
SEEK clarity on criteria
= Set Objectives / goals
STRUCTURE the problem
STEAL effective solutions
Our values? Goals / strategy?Talent management strategy? Comp philosophy? Role of EB?

http://rickcartor.wordpress.com
SeekStructure& Steal
STRUCTURE the problem:Small groupIdeal (goal) – Current = Gap -Problem statement (time) -Gather data
SEEK clarity on criteria
= Set Objectives / goals
Our values? Goals / strategy?Talent management strategy? Comp philosophy? Role of EB?

http://rickcartor.wordpress.com
SeekStructure& Steal
STRUCTURE the problem:Small groupIdeal (goal) – Current = Gap -Problem statement (time) -Gather data
Potential solutions
a. Generate (Brainstorm, etc.)b. STEAL effective solutions
Positive Deviance
SEEK clarity on criteria
= Set Objectives / goals
Our values? Goals / strategy?Talent management strategy? Comp philosophy? Role of EB?

Positive Deviance
…the observation that in any community, there are people whose uncommon but successful behaviors or strategies enable them to find better solutions to a problem than their peers, despite facing similar challenges and having no extra resources or knowledge than their peers.
http://rickcartor.wordpress.com 23

POSITIVE DEVIANCE
• Best for complex non technical problems where solutions depend on behavioral / social change
• HEALTHCARE BENEFIT INNOVATIONS: - NOT exact PD application + Steps & lessons
Steps & Details• DEFINE
– The problem (causes, challenges, constraints, current practices, desired outcomes)
• DETERMINE – Find [true] PDs’
• DISCOVER– uncommon, successful behaviors– similar to behavioral interview discipline
----------------------------------------------------DECISION TO PROCEED / APPLY THIS
SOLUTION----------------------------------------------------
• DESIGN– develop plan of action, practice,
activities, involvement • EVALUATE / MONITOR
– Keep group involvement, commitment
Use group / participant approach to finding, learning
Carefully match the situation / context
Respect / tap the collective expertise in the PD groupAssume that making it work is in the details
Ask open ended Qs, probe, follow upEncourage stories, information, details, visualsUse silence, don’t end, move on or sum too fastFocus on behaviors/actions, details
Goal: learn “HOW” not “WHAT” or “WHY”

Steps & Details• DEFINE
– The problem (causes, challenges, constraints, current practices, desired outcomes)
• DETERMINE – Find [true] PDs’
• DISCOVER– uncommon, successful behaviors– similar to behavioral interview discipline
----------------------------------------------------DECISION TO PROCEED / APPLY THIS
SOLUTION----------------------------------------------------
• DESIGN– develop plan of action, practice,
activities, involvement • EVALUATE / MONITOR
– Keep group involvement, commitment
Use group / participant approach to finding, learning
Carefully match the situation / context
Respect / tap the collective expertise in the PD groupAssume that making it work is in the details
Ask open ended Qs, probe, follow upEncourage stories, information, details, visualsUse silence, don’t end, move on or sum too fastFocus on behaviors/actions, details
Goal: learn “HOW” not “WHAT” or “WHY”

Steps & Details• DEFINE
– The problem (causes, challenges, constraints, current practices, desired outcomes)
• DETERMINE – Find [true] PDs’
• DISCOVER– uncommon, successful behaviors– similar to behavioral interview discipline
----------------------------------------------------DECISION TO PROCEED / APPLY THIS
SOLUTION----------------------------------------------------
• DESIGN– develop plan of action, practice,
activities, involvement • EVALUATE / MONITOR
– Keep group involvement, commitment
Use group / participant approach to finding, learning
Carefully match the situation / context
Respect / tap the collective expertise in the PD groupAssume that making it work is in the details
Ask open ended Qs, probe, follow upEncourage stories, information, details, visualsUse silence, don’t end, move on or sum too fastFocus on behaviors/actions, details
Goal: learn “HOW” not “WHAT” or “WHY”

Steps & Details• DEFINE
– The problem (causes, challenges, constraints, current practices, desired outcomes)
• DETERMINE – Find [true] PDs’
• DISCOVER– uncommon, successful behaviors– similar to behavioral interview discipline
----------------------------------------------------DECISION TO PROCEED / APPLY THIS
SOLUTION----------------------------------------------------
• DESIGN– develop plan of action, practice,
activities, involvement • EVALUATE / MONITOR
– Keep group involvement, commitment
Use group / participant approach to finding, learning
Carefully match the situation / context
Respect / tap the collective expertise in the PD groupAssume that making it work is in the details
Ask open ended Qs, probe, follow upEncourage stories, information, details, visualsUse silence, don’t end, move on or sum too fastFocus on behaviors/actions, details
Goal: learn “HOW” not “WHAT” or “WHY”

http://rickcartor.wordpress.com
SeekStructure& Steal
STRUCTURE the problem:Small groupIdeal (goal) – Current = Gap -Problem statement (time) -Gather data
Potential solutions
a. Generate (Brainstorm, etc.)b. STEAL effective solutions
Positive Deviance:
Monitor & Compare
Implement (pilot?)
Evaluate & Select
SEEK clarity on criteria
= Set Objectives / goals
Our values? Goals / strategy?Talent management strategy? Comp philosophy? Role of EB?

Good sources of related content
http://rickcartor.wordpress.com 30
Cartor, Rick. 2013. What I’ve Learned So Far. http://rickcartor.wordpress.comCooperrider, DL and Whitney, D. (2010) The Appreciative Inquiry HandbookGoldhill, David (2013) Catastrophic Care: How American Health Care Killed My
Father--and How We Can Fix It Heath, C. & Heath, D. (2010) Switch: How to Change Things when Change is HardHerzlinger, Regina. (2007) Who Killed Health Care?: America's $2 Trillion Medical
Problem - and the Consumer-Driven Cure National Business Coalition on Health http://www.nbch.org/National Business Group on Health, http://www.businessgrouphealth.org/ Pascale Richard; Sternin, Jerry and Sternin, Monique (2010) The Power of Positive
Deviance: How Unlikely Innovators Solve the World's Toughest Problems Potter, Wendall. (2011) Deadly SpinStarfield, Barbara, Johns Hopkins University. Miscellaneous articles and booksThaler, Richard H. & Sunstein, Cass R. (2009) Nudge: Improving Decisions About
Health, Wealth, and Happiness

http://rickcartor.wordpress.com 31
The GOALS of this session are: 1. understand how key players are responding to healthcare
reform so employers can find ways to survive and thrive2. enable participants to recognize and overcome common
obstacles to innovative solutions in healthcare benefit design.
NOT-a thorough review of PPACA-a debate on PPACA merits-a how to for specific mandates-a how to for being deviant
Positive Deviance: Innovative Responses to Healthcare Reform
Positive Deviance: Innovative Responses to Healthcare Reform
Dr. Rick Cartor, Director, ChD, LLC HR/OD Consultant @ BB&T Insurance
Louisville, KY
http://rickcartor.wordpress.com 32