post graduate dept of radiodiagnosis ppt.pdfreduction enema •successful when flow moves ... barium...
TRANSCRIPT

DR JAIKISHOR JOTHIRAJ MD
POST GRADUATE DEPT OF RADIODIAGNOSIS
• YASHODAMMAL 70 YRS OD LADY had
• C/o diffuse lower abdominal pain ‐20 days• h/o blood in stools ‐4 days • h/o vomiting ‐2 days • h/o burning micturation +ve• h/o abdominal surgery 30 yrs back • Not a k/c/o DM/HT/BA

• O/E
• No guarding
• No rigidity
• No distention
• No blood in P/R
• AMOEBIC COLITIS ??

USG – TARGET SIGN +VEBOWEL with in BOWEL appearancePROBE tenderness + vepseudo kidney sign +ve
UGI‐ENDOSCOPY –normal
Chest x‐ray pa—no free air under diaphragm
X‐ray abdomen erect –dilated small bowel,withmultiple air fluid levels & gaseous distention of proximal colon
CT‐well defined fat density [‐100 to ‐120 hu] lesions of size 4.2 3.8 cms noted within lumen of sigmoidcolon with telescoping of sigmoid loops

Target Sign
Central hyperechoic region (C) surrounded by hypoechoic and homogeneous edge (bowel wall)
DDX –TARGET SIGN
1.APPPENDICULAR MASS
2.LEIOMYOMA
3.MELANOMA RECTUM
4.LYMPHOMA
5.ENCEPHALOID CA
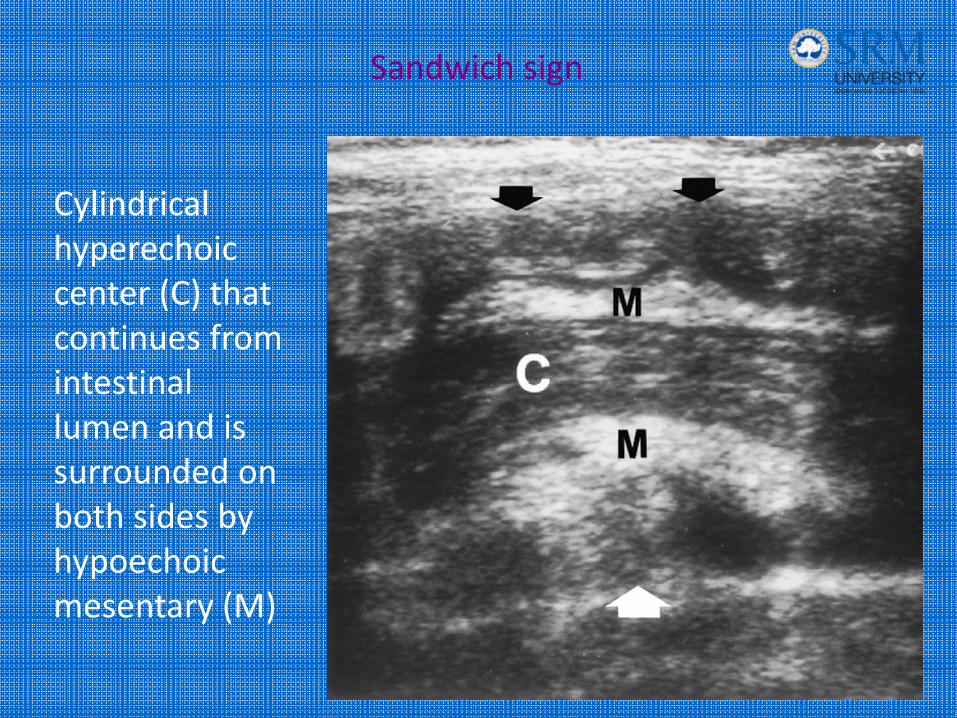
Sandwich sign
Cylindrical hyperechoic center (C) that continues from intestinal lumen and is surrounded on both sides by hypoechoic mesentary (M)


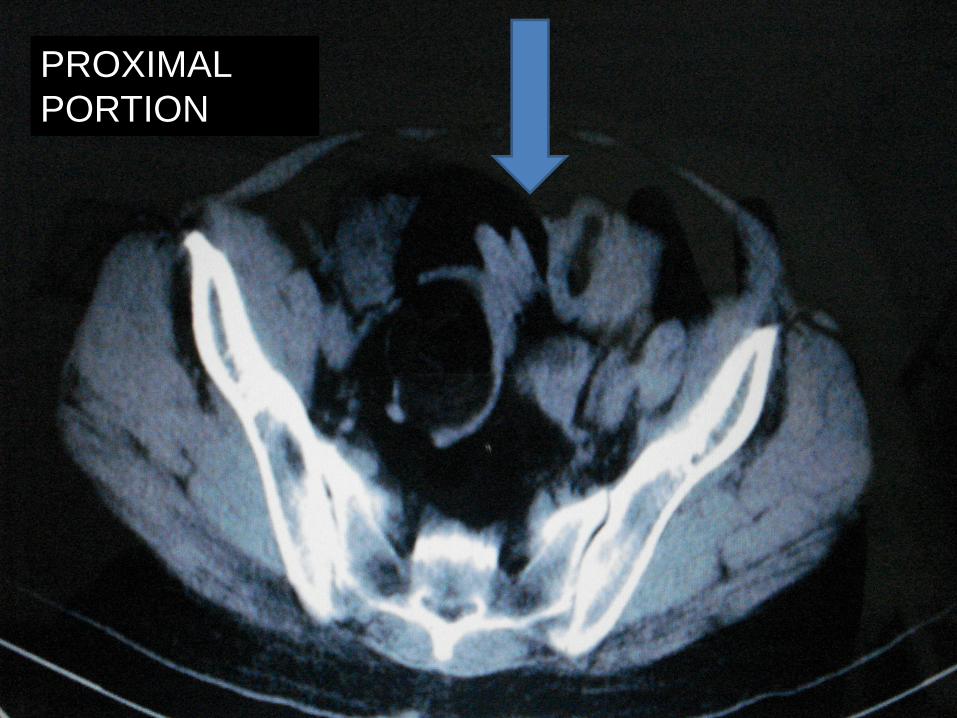
PROXIMAL PORTION



Distal endDISTAL END

axr
• Absence of bowel gas in the area
• Rounded soft tissue mass
• Crescent of air at the apex of an intussusception
• Target sign

Created by gas trapped between two layers of intestinal wall
Where is the target sign?

Where is the
crescent sign?
Created by gas surrounding invagination

COLONOSCOPY REPORT
• Globular mass seen in the lumen of the rectum which on inflation retracted back upto sigmoid
• Scope could not be passed further
• Rectal mucosa appears normal
• POLYPOIDAL MASS ‐ ? LIPOMA
• INTUSSUSCEPTING from sigmoid rectum

DIAGNOSIS
• SIGMOID colon lipoma acting as a lead point for intussusception

Just as a refresher…

What is IS?• 1 portion of the small bowel invaginating into the distal portion of small
bowel, pulled in by peristalasis
• Type of intussusception depends on segment of bowel that is involved – Starting at the ileocolic junction ileocolic intussusception
Intussusceptum=proximal portion
Intussuscipen=distal portion

ETIOLOGY
• WEANING PERIOD
• VIRAL GASTRO‐ENTERITIS {rota,polio}
• INFLAMMATION & ENLARGEMENT OF LYMPHOID TISSUE ‐‐‐‐PAEYER’S PATCHES
• Neoplasam
• Gastro‐jejunal & naso‐jejunal feeding tubes
• 5‐10% ‐‐‐meckel’s diverticulum,polyps,lymphomas,duplication cysts

Classic Triad
Colicky abdominal pain
‐pulling knees up to abdomen
Abdominal Mass‐sausage shaped
“Currant Jelly” bloody stools
•Multiple studies have shown that classic triad is only present in 20‐50%•70% found to have 2 sx•9% found to have 1 sx

Classification
• Intraluminal
• Intramural
• Extraluminal
• Ileo‐colic
• Ileo‐ileo‐colic
• Colo‐colic
• Ileo‐ileal
• Gastro‐colic
• Primary
• Secondary

Colo-colic

OPERATIVE FINDINGS
• Intra abdominal adhesions
• Submucosal lipoma in sigmoid colon
• Rest of intra abdominal areas –normal





In a nutshell…
Base your next move on CLINICAL SUSPICION…
IF LOW suspicion AXR
‐if negative, unlikely to be IS
IF MEDIUM suspicion AXR US
‐if US negative, unlikely to be IS
IF HIGH suspicion, you can skip AXR and proceed directly to US
for confirmative CT contrast

Treatment
17% of IS spontaneously reduce
1st – NPO, IV fluids, NG tube2nd – surgery consult
Otherwise, tx by reduction enemas or surgery
Reduction Enema•Successful when flow moves into ileum•Pt is under sedation•Disadvantages – missed lead points, higher recurrence rate, perforation, and radiation exposure•But benefits outweigh risks –less invasive than surgery, faster
recoverySurgery•Indications – irreducible by enema, necrotic IS, age, long duration of sx, SBO, or clinical signs/sx of peritonitis or bowel infarction

Enema‐3 types
• Pneumatic
• Hydrostatic
• Barium
• Succesful reduction ‐‐‐disappearance of mass & flooding of air into the small bowel

Pneumatic Enema: Before and After


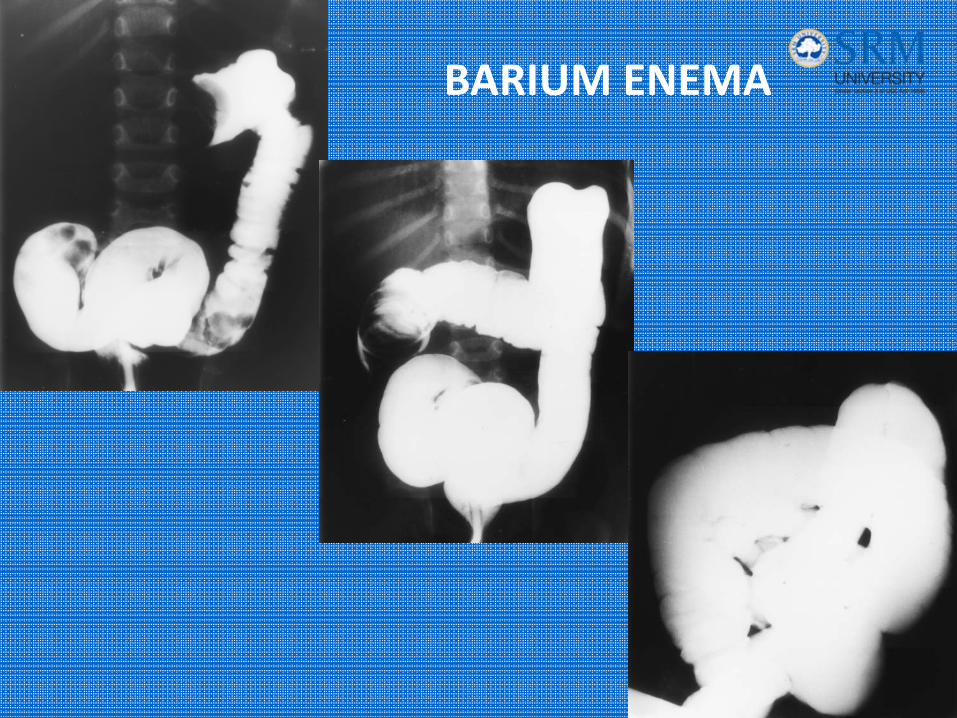
BARIUM ENEMA

risk
• Inducing /uncovering a pre‐existing perforation
• Tension pneumoperitoneum
• Respiratory & haemodynamic instability
• Hydrostatic enema‐‐‐‐‐rapid fluid shifts if iso‐osmolar concenteration not used
• Barium enema –
P i i i & f i