poster session iii 2006
TRANSCRIPT

P2-72
Echocardiographic Guidance of Percutaneous Mitral Valve Repair with the Evalve System: Lessons Learned from EVEREST I
Frank E Silvestry1, Howard C Herrmann1, L Leonardo Rodriguez2, William J Stewart2, Shunichi Homma3, Alan Zunamon4, Randolph P Martin5, Kimberly Krabill6, Elyse Foster7, Ted Feldman4, Susan E Wiegers1
1Hospital of the University of Pennsylvania, Philadelphia, PA;2Cleveland Clinic Foundation, Cleveland, OH;3Columbia Presbyterian Hospital, NYC, NY;4EvanstonHospital, Evanston, IL;5Emory University Hospital, Atlanta, GA;6Swedish Medical Center, Seattle, WA;7UCSF Medical Center, San Francisco, CA
Background: Percutaneous repair of mitral regurgitation (MR) is an increasingly attractive alternative to cardiac surgery. We report our experience with echo guidance of this procedure in the first 47 patients enrolled in EVEREST I.Methods: A catheter-based transseptal system is used to deliver and attach a clip to the mitral valve leaflets, replicating surgical edge-to-edge repair for mitral regurgitation. The system (Evalve) uses a steerable guide catheter to precisely and iteratively position a clip that approximates the middle anterior and posterior leaflet scallops of the valve, creating edge-to-edge mitral valve repair. This requires precise manipulation of the clip, using primarily echocardiographic guidance aided by fluoroscopy. A unique and intense collaboration between echocardiographer and interventionalist is required for successful placement of the repair system. This requires continuous online monitoring during all aspects of the procedure. A streamlined imaging approach was developed for this trial, that uses standardized vocabulary and predetermined TEE views to optimize collaboration between interventionalist and echocardiographer.Results: A standard vocabulary based on internal mitral valve landmarks was used to optimize communication between echocardiographers and interventionalists. Echo provides online procedural guidance, immediate monitoring of the degree of MR and transmitral gradients (pre and post clip deployment), allowing iterative repositioning of the clip (all patients), and placement of a second clip (11 patients). Four primary TEE views are used: 1) short axis view at the base of the heart to determine transseptal position, system translation, and avoid contact with the lateral atrial structures; 2) Mid esophageal (ME) intercommissural view at to determine medial-lateral angulation and axial translation of the delivery system; 3) the ME long axis view to determine anterior-posterior angulation, and to align the system parallel to the direction of antegrade mitral inflow; and 4) trans-gastric short axis view (or transthoracic parasternal short axis, if necessary) for the alignment of the clip arms perpendicular to the line of coaptation.Conclusions: 1) TEE is essential for guiding catheter based edge-to-edge repair with the Evalve system. 2) A streamlined imaging approach was developed for the trial using standardized imaging views and a common vocabulary, which shortened procedure times for efficient placement and deployment of the clip, and facilitates effective collaboration between interventionalist and echocardiographer.
P3-01
Prevalence of Intraventricular Mechanical Dyssynchrony in a Heart Failure Population; A Comparison of Four Techniques
Julian M Castro, Gail Doyle, Leighton Kearney, Tracey Muir, Piyush Srivastava Austin Health, Melbourne, Australia
Background: Echocardiography has been advocated as a better predictor of mechanical dyssynchrony than the surface ECG. However, there is no consensus as to the best echocardiography method. This analysis compares 4 echocardiography methods for determining the prevalence of mechanical dyssynchrony in a heart failure populationMethods: Standard echocardiography according ASE guidelines was performed. Tissue Doppler was analysed offline using Echopac. Mechanical dyssynchrony was defined according to the method used: (1)M-mode: septal to posterior wall mechanical delay >130msec. Tissue Doppler: (2)Septal-lateral delay > 65msec; (3) Delay of any of the four basal segments greater than 65msec; (4) Standard deviation (sd) of twelve segment model > 32msec.Results: 62 patients referred from the heart failure clinic were studied (70 ± 12 years; 78% male, 70% ischaemic cardiomyopathy, 93% systolic dysfunction, 18% NYHA grade III-IV). Dyssynchrony was assessable in 37% of patients using Mmode and 93% using tissue Doppler. The basal 4 segment and 12 segment models produced similar rates of dyssynchrony, 63% and 60% respectively, that were higher than the Mmode and septolateral model. There was a strong and significant correlation between the tissue Doppler methods (See graph). However, the basal 4 and the 12 segment model identified different patients as having dyssynchrony (χ2: p<0.0001).
Conclusion: Tissue Doppler is more reliable for measuring mechanical dyssynchrony than Mmode. A 2 dimensional model is less sensitive than a 3 dimensional model. Both the 12 segment and basal 4 segment models produced similar rates of mechanical dyssynchrony, 60-63%, yet identified different subgroups.
P3-02
Regional Myocardial Mechanics in Patients with Septal and Apical Hypertrophic Cardiomyopathy
Hua Yang1, Shemy Carasso1, Mani A. Vannan2, Anna Woo1, Michal Jamorski1,Evelyn Rozenblyum1, E. Douglas Wigle1, Harry Rakowski1
1Toronto General Hospital, University of Toronto, Toronto, ON, Canada; 2Universityof California at Irvine, Orange, CA
Background: We used a novel B-mode angle-independent technique, Velocity Vector Imaging (VVI, Siemens Medical Solutions), to quantify left ventricular (LV) circumferential (circ) and longitudinal (longi) regional mechanics. We postulated that myocardial mechanics would be altered in hypertrophic cardiomyopathy (HCM) and related to the site of LV hypertrophy.Methods: 72 patients with HCM (27 apical HCM (ApHCM) and 45 septal HCM (SepHCM)) were compared with 25 normal age-matched subjects. Short axis measurements included global systolic (RAV-S, cm/s) and diastolic (RAV-D) rotational angle velocities, circ strain (C-Strain, %), and strain rate (C-SR, 1/s) at the LV basal, mid and apical segments. Apical 4-chamber measurements included regional longi strain (L-strain, %) and systolic and diastolic (L-SR-D, 1/s) strain rate at the LV basal, mid and apical segments of septal and lateral walls. One-way ANOVA was used with Post Hoc multiple comparisons between the three groups.Results: SepHCM had greater LV wall thickness in the basal (12.05±1.48 mm vs 19.53±5.25 mm, ApHCM vs SepHCM, p<0.0001) and mid (14.52±2.69 vs 17.8±7.09, p<0.05) septal, basal anterior (12.23±1.60 vs 16.45±3.97, p<0.0001) and basal lateral (11.01±1.21 vs 12.82±2.04, p<0.001) segments. As expected, ApHCM (from 15.67±3.81 to 17.29±2.10) had more thickness than SepHCM (from 10.90±2.34 to 13.62±3.59) in all apical segments (p<0.001 to p<0.0001). Rotational velocity of the mid LV segment in systole followed the basal direction in SepHCM and ApHCM, but followed the apical direction in the normal group. So the rotation equatorial plane (with zero rotation) was apically displaced in HCM patients. Apart from the above different patterns, the values of rotational velocities at mid segments varied between the three groups (table). Compared to the normal group, HCM groups had decreased average LV Longi diastolic strain rate and strain. Compared to ApHCM, SepHCM had higher LV circ systolic strain rate and strain at basal and mid segments.Conclusions: Myocardial mechanics were markedly abnormal in HCM patients. Circ strain and strain rate abnormalities vary with the location of LV hypertrophy. Both septal and apical HCM patients had decreased longi strain and strain rate and altered mid LV rotation, indicating a unique primary contraction abnormality.
Normal (1)(n=25) ApHCM (2)(n=27) SepHCM (3)(n=45) p value (1 vs 2) p value (1 vs 3) p value (2 vs3)Age 47.9±12.4 54.2±16.4 49.5±17.4 NS NS NSC-SR-S-base 1.19±0.39 1.13±0.31 1.44±0.52 NS NS 0.010C-SR-S-mid 1.39±0.40 1.33±0.39 1.58±0.51 NS NS 0.029C-strain-base 22.0±4.7 21.8±4.3 25.4±6.3 NS NS 0.036C-strain-mid 25.7±5.6 23.5±5.3 28.3±6.8 NS NS 0.003L-SR-D 1.16±0.39 0.87±0.32 0.86±0.35 0.004 0.001 NSL-Strain -21.0±3.1 -17.0±4.0 -16.9±4.18 <0.001 <0.001 NSRAV-S-mid -0.61±0.34 0.41±0.28 0.56±0.46 <0.001 <0.001 0.039RAV-D-mid 0.61±0.29 -0.35±0.26 -0.55±0.54 <0.001 <0.001 0.013
Poster Session IIIMonday, June 5, 2006
Presented: 11:30 am – 2:30 pmModerated: 12:30 pm – 2:30 pm
Moderated Posters:Cardiomyopathies, Ventricular and Atrial Function, Myocardial Tissue Imaging and Pericardial Diseases
– Posters P3-01 through P3-21
Posters:Myocardial Function – Posters P3-22
through P3-49Cardiomyopathies and Pericardial
Disease, Cardiac Mass/Tumor – Posters P3-50 through P3-71
3-D Echocardiography – Posters P3-72 through P3-82
Journal of the American Society of EchocardiographyVolume 19 Number 5 Abstracts 619

P3-03
Ratio of Transmitral Early Diastolic Velocity to Mitral Annular Early Diastolic Velocity Identifies Early-Stage Cardiac Involvement in Patients With Systemic Amyloidosis and Normal Wall Thickness
Ravi Lala, Ravin Davidoff, Martha Skinner, Frederick Ruberg Boston University Medical Center, Boston, MA
Background: The identification of early-stage cardiac involvement in systemic amyloidosis is challenging. Although numerous echocardiographic features of amyloid cardiomyopathy (AC) have been characterized, most are present in advanced disease when treatment options are limited. Thus, identification of markers of early AC may be useful in guiding therapy. Elevated levels of serum B-type natriuretic peptide (BNP) are strongly correlated to both the presence of AC and its prognosis. (Palladini et al, Circulation 2003). We sought to determine if sensitive hemodynamic echocardiographic measures might identify AC at an early-stage when wall thickness remains normal.Methods: Seventy consecutive patients with systemic AL amyloidosis and normal mean wall thickness (< 12 mm) by echocardiography but unknown AC were recruited following informed consent. All echocardiograms were performed in standard fashion and analyzed using a commercial workstation (XCelera, Philips Medical Systems). Mitral inflow and pulmonary venous Doppler, as well as mitral annular tissue Doppler measurements, were recorded. Baseline BNP levels were measured at the time of echocardiography. Comparisons were performed by two-tailed unpaired t-test and correlations examined by the Pearson method.Results: Overall systolic function was normal (LVEF=60.7 ± 4.9%). Cardiac amyloid involvement was suspected by a serum BNP level of greater than 100 pg/ml (Nordlinger, Am J Cardiol, 2005). Of the 70 records reviewed, 17 (24%) had a BNP level > 100 pg/ml and 53 (76%) had a BNP level < 100 pg/ml. Patients with a BNP level > 100 pg/ml had a higher E/E’ ratio (13.9 vs. 9.4, p < 0.0001) and greater wall thickness (10.6 mm vs. 9.7 mm, p < 0.01) as compared to those with a BNP level less than 100 pg/ml. While E/E‘ and BNP were significantly correlated (R=0.274, p=0.02), wall thickness and BNP were not (R=0.097, p=0.42). E wave deceleration time, E/A ratio, and pulmonary vein S/D ratio were not statistically different between the two groups. When patients with hypertension or renal failure in the higher BNP group were excluded (n=8), the difference in E/E‘ (14.2 vs 9.4, p<0.0001) and correlation between E/E‘ and BNP (R=0.491, p<0.001) persisted.Conclusion: This study suggests that E/E’ ratio, but not traditional hemodynamic measures, may be a marker for early-stage cardiac amyloidosis in patients with known systemic amyloidosis but without classical echocardiographic manifestations of cardiac involvement. In conjunction with BNP, E/E‘ may permit optimization of patient selection for aggressive stem cell-based chemotherapeutic regimens.
P3-04
Intra Pericardial Fluid Shifts and Doppler Correlation of Intra Pericardial Pressure in Cardiac Tamponade
Sangareddi Venkatesan1, R Alagesan2, G Gnanavel2, V Jaganathan2
1Madras Medical College, Chennai, India; 2Madras Medical College, Chennai, India
Back ground The definitive dignosis of cardiac tamponade(CT) in patients with large pericardial effusion(PE) remains a contentious issue.Aim Intra pericardial fluid in PE is in a dynamic state.We hypothesized that Doppler analysis of fluid shifts in large PE could predict CT and possibly correlate with Intra pericardial pressure(IPP).Methods The study population included 14 patients with large PE who presented to our institute . After clinical examination they underwent routine 2 D and Doppler echocardiography .7 patients had both clinical and echo evidence of tamponade 5 had neither clinical nor echo evidence of tamponade. 2 had echo evidence of tamponade but no clinical tamponde. All these patients underwent Intra pericardial Pulsed Doppler study.Good 2D images were obtained in apical 4 chamber or parasternal long axis view. The sample volume was placed in the area of maximum pericardial fluid accumulation . It was adjacent to the RV or LV free wall or apex. Pulse wave Doppler tracing gated with ECG was recorded . Patients with CT were taken up for pericardiocentesis with continuous IPP monitoring.Intra pericardial Doppler revealed two distinct velocity profiles. A negative systolic swing velocity (Vns) and a positive diastolic swing velocity (Vpd). The following parameters were measured. Peak velocity of Vpd and Vns. Total swing velocity Vns+Vpd ( VS) , Time to peak Vns (Vnt) , Vpd (Vpt) and Vns to Vpd ratio.The Doppler estimation of IPP was done by modified Bernoulli equation with Peak Vns and Vpd.Results In patients with tamponade, the mean Vns and Vpd were 1.6m/sec(r 1.3-2.2), 1.4m/sec(r 1.2-2.0) respectively .The mean (VS)was 2.6m/sec(2.5-3.2) The Vnt and Vpt were 38ms (r 30-60ms) 40msec(r 36-62ms) respectively. The Vns:Vpd was 1.2:1.In patients with large PE and no tamponade, the mean Vns and Vpd were .75(r.5-1.1) , .96m/sec(r.6-1.2) respectively. The mean ( VS) was 1.2m/sec(r 1.1-1.8). The Mean Vnt and Vst were 64msec (r 50-75ms), 70ms(r58-80ms) respectively The Vns:Vps was .8:1The mean estimated IPP in patients with was 9 mmhg (r 8-18). And the catheter measured IPP was 8mmhg(r 7-16) .In patients with large effusion and no tampondae the mean doppler derived IPP was 2mmhg(r 1-4) .A Vnt less than 40msec predicted a IPP of >10mmhg with 100% accuracy.Vns correlated well with IPP than Vpd.Conclusion There are distinct doppler velocity profiles inside the pericardial space in patients with large PE. The magnitude of combined systolic and diastolic swing velocities and a rapid negative systolic velocity can be a simple predictor of cardiac tamponade . It also has a good correlation with intra pericardial pressure .
P3-05
Quantitative Assessment of Left Atrial Function and Remodeling in Patients with Atrial Fibrillation by Tissue Doppler Strain and 2-Dimensional Strain Imaging
Kyoung Im Cho, Jeong Ho Park, Tae Ik Kim Maryknoll General Hospital, Busan, Republic of Korea
Background: Conservation of the normal atrial size and architecture by preventing structural atrial remodeling due to atrial fibrillation (AF) seems of prime importance for the future management of AF. 2-Dimensional strain is a novel technique that depicts regional deformation via frame-to-frame tracking of unique acoustic grayscale patterns within image. We attempted to assess the relevance of strain echocardiography for quantitative assessment of the left atrial (LA) status in AF. Methods: Tissue Doppler strain and 2-dimensional strain imaging were performed in 15 patients with chronic AF, 15 paroxysmal AF and 15 healthy age-matched controls using a GE vivid 7 dimension. LA diameter, LA volume index and mitral inflow parameters were measured by standard echocardiography. Longitudial peak strain was obtained from 2 different areas of the basal left atrial free wall and inter-atrial septum in the apical 4 chamber view by tissue Doppler strain. Mean peak systolic (Sm-SR), peak early diastolc (Em-SR) and peak late diastolic (Am-SR) strain rate were measured at the inter-atrial sepum in the apical 4 chamber view by 2-dimensional strain. Results: Peak strain, Sm-SR, Em-SR and Am-SR were significantly reduced in the AF group comparing normal, especially in the chronic AF group(Table 1). There were no significant differences in LA size and A wave velocity between PAF and normal groups, however, peak systolic strain/rate, Em-SR, Am-SR were significantly lower in paroxysmal AF group than normal. Conclusions: The lower values of atrial Sm-SR, Em-SR and Am-SR revealed that active contraction and passive stretching of LA wall may impair in some patients with PAF even before LA enlargement possibly because of atrial fibrosis and reduced compliance. Our results indicated that strain echocardiography enabled qualitatively precise LA contractile function and provided clinically useful information of LA function and remodeling.
Table 1:Parameters of 2-dimensional strain between groups Peak strain(%) Peak SR(s-1) Em-SR(s-1) Am-SR(s-1)Normal 48.15±17.85 3.03±0.60 -2.61±0.46 -2.44±0.31PAF 19.78±8.88* 1.38±0.58* -1.11±0.53* -1.46±0.71*
Chronic AF 8.25±4.66*,† 0.57±0.39*,† -0.82±0.52*,†
Values are mean±SD. PAF; paroxysmal AF, *: p<0.05 vs control, †: p<0.05 vs PAF
P3-06
Functional Correlates of Left Atrial Strain and Strain Rate by Velocity Vector Imaging
Maria J Eriksson, Christina Jarnert, Pernilla Jacobsson, Margareta Ring, Lars Rydén, Kenneth Caidahl, Anders Melcher Karolinska University Hospital, Stockholm, Sweden
Background: We applied a new 2-D based quantitative technique Velocity Vector Imaging (VVI) to evaluate the regional function of the left atrium (LA) in relation to established Doppler-derived indexes of diastolic function and LA volume changes in patients with Type 2 Diabetes.Methods: 29 consecutive patients with uncomplicated Type 2 Diabetes, mean age 59±7 years, with normal systolic left ventricular function and no hypertrophy, or mitral regurgitation, underwent Doppler-echo. LA wall deformation was evaluated by a new 2-D based technique VVI (Siemens, CA). Mitral inflow velocities (E and A wave) and tissue velocity in the septal part of the mitral annulus (É waves) were measured and E/A, and E/É ratios were calculated. VVI measurements included systolic strain (LA-Strain) and systolic (LA-SRs) for the septum (Sep), lateral wall (Lat) and the LA roof (Roof). LA ejection fraction (LA-EF) was calculated.Results: Mean values were: for the indexed LA volume 33±7 ml/m2, E/A 1.1±0.4, E/É 7.6±2.1 and LA EF 53±8%. Systolic velocity in the lateral and septal wall, and the LA roof were 3.2±0.9 cm/s, 2.9±0.9 cm/s and -0.4±0.5 cm/s and systolic strain 31±10%, 32±10% and 30±7%. E/É related to the LA Vol and LA EF (p<0.01). The LA-Strain and LA-SR measured in the Lat, Sep and Roof positions correlated significantly with E/A, E/É, LA-EF, but not with heart rate or the indexed LA volume. LA volume correlated only with the systolic LA velocity measured in the lateral wall.Conclusions: Strain and strain rate assessed by VVI for the septal and lateral wall, and the LA roof were related to established measures of diastolic left ventricular function in terms of E/A and E/E´ and LA emptying function, but not to the indexed LA volume. VVI provides a new insight into regional LA mechanics.
Journal of the American Society of Echocardiography620 Abstracts May 2006

P3-07
Exercise Capacity in Heart Failure Patients: Relationship with Diastolic Function and Left Atrial Performance
Ana Clara T Rodrigues, Linda Ueno, Geraldo Lorenzi-Filho, Carlos Eduardo Negrao, Wilson Mathias, Jr. Heart Institute - InCor, Sao Paulo - SP, Brazil
Peak oxygen uptake (VO2) is a strong predictor of hospitalization and death in chronic heart failure (HF). To assess the relation of exercise capacity to indexes of left ventricular (LV) and left atrial (LA) function in HF, 20 patients (17 male, aged 57± 7 years) underwent maximal symptom-limited treadmill exercise testing with measurement of peak VO2 and were divided into 3 groups according to Weber’s classification: Group I, VO2 > 20 ml/Kg/min, Group II, VO2 from 16 to 20 ml/kg/min, and Group III, VO2 from 10 to 15 ml/Kg/min. All patients had LV ejection fraction (EF) <0.45. M-mode and two-dimensional echocardiographic measurements were undertaken for LV mass and LA and LV volumes (apical 2 and 4 chamber views -Simpson’s rule), and LVEF and LA emptying fraction (LAEF) were derived. LAEF was given as the ratio of maximal (max) LA volume (vol) - minimal (min) LA vol/max LA vol. Transmitral Early (E) and late (A) velocities, E wave deceleration time (DT), isovolumic relaxation time, pulmonary venous flow, and basal lateral and septal mitral annular tissue Doppler velocity measurements were undertaken to assess LA and LV function. ANOVA was used to test the difference among groups. Results: VO2 max for groups I, II and III was 21.2 ± 0.6, 18.0±0.4 and 12.3±0.5 ml/Kg/min, respectively. Age, body surface area and etiology of HF did not differ among the groups, but heart rate was lower for group II. While LV diameters, mass, volumes, and EF(0.31±0.09, 0,32±0.07 and 0,22±0.09 respectively for groups I, II and III, p=NS) were similar, septal systolic (Sm) velocities showed lower values for group III. Doppler indexes of LV diastolic filling were also different, with Group III showing higher E waves and E/A ratio and a reduced DT, typical of restrictive filling. Additionally, group III exhibited evidence of LA failure, expressed by an increased LA min vol, resulting in a lower LAEF in Group III, and a decreased late (Am) lateral velocity. There was a significant but modest correlation between peak VO2 and measurements of cardiac performance, including LVEF(r= 0.49), LAEF (r=0.42), septal Sm (r =0.66) and lateral Am (r = 0.44). Conclusion: In patients with HF, impairment in exercise capacity may not be well related with LV dimensions or load dependent indexes of LV function, rather, it seems to be better predicted by diastolic indexes and LA performance.Echocardiographic variables for each heart failure group LAEF LA min E wave E/A Deceleration Septal Sm Lateral Am vol (ml) (cm/s) ratio time (ms) (cm/s) (cm/s)Group IN = 7 0.39±.09 40±16 65±20 0.9±0.4 200±50 5.5±1.1 7.6±2.7Group IIN = 7 0.47±.09 35±16 58±17 0.8±0.3 240±66 5.8±1.0 8.6±2.1Group IIIN = 6 0.31±0.13(*) 87±58 (*) 94±31 (*) 2.1±1.3(*) 152±42(*) 4.0±0.9 (*) 3.5±2.6 (*) (*)p = 0.04 (*)p=0.03 (*) p= 0.03 (*) p= 0.02 (*) p= 0.03 (*) p=0.008 (*) p = 0.005
P3-08
Atrial Fibrillation After Noncardiac Thoracic Surgery: Role of Echocardigraphy in Prediction and Prevention
Abu Shoyeb, Howard Weinstein, Nancy Roistacher, Barbara Spaltro, Galina Yusim, Richard M Steingart Memorial Sloan-Kettering Cancer Center, New York, NY
Background: Postoperative atrial fibrillation (POAF) is an important and common complication of noncardiac thoracic surgery. Limited data are available on the value of transthoracic echocardiography (TTE) in the management of patients (pts) at risk for POAF. Therefore, the predictive power of clinical and TTE variables on the incidence and prevention of POAF were investigated.Methods: Consecutive pts who underwent echocardiography < 6 months prior to intermediate and high risk noncardiac thoracic surgery were identified from an exercise echocardiographic database. Pts who were not in sinus rhythm before anesthesia were excluded. TTE and clinical variables, including the use of perioperative beta-blockers (PBB), were extracted from the electronic medical record. POAF was defined by telemetry or 12 lead ECG if it occurred before the 8th POD or discharge from the hospital. Logistic regression analysis and Fisher’s exact test were used for statistical analysis. Data are mean±SD.Results: A total of 229 pts were studied. Age was 68±11 yrs, 55% were men; 187 pts had lung surgery and 42 pts had esophageal surgery. Ninety one pts received PBB. Thirty pts (13.1%) developed POAF. Onset of POAF was 2.6±1.9 days after surgery. Results of logistic regression analysis for predictors of POAF are shown in the table
Predictors Odds Ratio 95% CI P valueAge ? 65 yrs 2.13 0.76 - 7.04 0.17Hx Smoking 2.24 0.76 - 8.29 0.18HTN 1.46 0.59 - 3.61 0.41Diabetes 1.51 0.44 - 4.74 0.41Hx CVA 1.65 0.35 - 6.63 0.50Hx. of AF 5.51 0.91 - 30.06 < 0.05LAE/LVH 2.60 1.09 - 6.55 < 0.05Rest EF <50% 5.37 0.53 - 56.49 0.13Beta-blockers 0.24 0.08 - 0.65 < 0.01
POAF was seen in 7.7% of pts receiving PBB Vs. 16.7% of pts not receiving PBB (p = 0.07). In the group with TTE LAE/LVH pts receiving PBB had significantly lower incidence of POAF (6.5% Vs 32%; p < 0.01) than pts who did not receive PBB. This benefit of PBB was not seen in the group without TTE LAE/LVH (8.9% vs. 7.9% with and without PBB; p = ns). (Fig)
Conclusion: A Hx of AF and the TTE variables LAE/LVH are more powerful predictors of POAF than other traditional risk factors. PBB reduce the incidence of POAF more effectively in pts with LAE/LVH. Thus, preoperative TTE is a potentially useful tool in gauging operative risk and planning preventative strategies in noncardiac thoracic surgery where the use of PBB may be of concern.
P3-09
Myocardial Performance Index Predicts Survival Rates in Patients with Chronic Renal Failure: Evidence for Diastolic Left Ventricular Dysfunction
Hiroshi Kato, Yuka Sugawara, Aki Kato, Yasuko Saito, Fumiko Abe, Junichi Hirai, Naomi Maekawa, Shinichiro Ishihara, Makoto Yamamoto Fukui Kosei Hospital, Fukui City, Japan
Background: We sought to clarify prognostic value of the myocardial performance index (MPI; also known as the Tei index) in patients with chronic renal failure (CRF). Methods:We prospectively performed pulse Doppler echocardiography and tissue Doppler imaging (TDI) in 50 consecutive CRF patients treated with maintenance hemodialysis (mean age ±SD, 69±13 years). MPI was calculated as the sum of isovolumic contraction time and relaxation time divided by ejection time. An MPI exceeding 0.45 was considered abnormal (“increased MPI”). Using TDI, we measured systolic LV myocardial velocities and early diastolic LV myocardial velocities adjacent to the mitral annulus. At 1 year follow-up, we compared all echocardiographic parameters between survivors and nonsurvivors. Results: Eleven patients (22%) died during the follow-up period. Comparison between survivors (n=39) and nonsurvivors (n=11) showed no statistically significant differences in LV mass index, LV end-diastolic volume, LV ejection fraction, or cardiac index. In contrast, nonsurvivors had significantly higher MPI than survivors (0.52±0.17 vs. 0.38±0.14, p<0.005). Diastolic LV myocardial velocity was significantly lower in nonsurvivors than in survivors (8.6±1.6 vs. 10.4±2.8 cm/s, p<0.05). At 1 year, patients with increased MPI had higher mortality rate than those with normal MPI (50% vs. 9%, p<0.005). Increased MPI predicted mortality during 1 year with sensitivity of 72%, specificity of 79%, and diagnostic accuracy of 78%. Multivariate analysis identified MPI as the only independent predictor of overall mortality (p<0.01). Furthermore, patients with increased MPI (n=16) had lower diastolic LV myocardial velocity (7.9±1.6 vs. 11.0±2.5 cm/s, p<0.0001), lower E wave velocity for transmitral flow (49±17 vs. 63±19 cm/s, p<0.05), and lower E/A ratio (0.58±0.19 vs. 0.76±0.22, p<0.01) than those with normal MPI (n=34). Conclusions: Among patients with CRF, MPI is a powerful predictor of clinical outcome and is superior to standard echocardiographic indexes. Patients with increased MPI have LV diastolic dysfunction associated with poor chances of survival over 1 year.
P3-10
Tissue Doppler Measurement at the Tricuspid Valve Annulus is Not Predictive of Right Atrial Pressure in Patients with Pulmonary Hypertension
Andrew M Kahn1, Ron Schnitzer1, Swaminatha Gurudevan2, Anthony N. DeMaria1,Daniel G. Blanchard1
1University of California, San Diego, CA;2University of California, Irvine, CA
Background: Peak early diastolic mitral inflow velocity (E) divided by tissue Doppler measurement of early mitral annular velocity (Em) has been shown to correlate well with mean left atrial pressure. An analogous measurement for the right heart has been shown to estimate mean right atrial pressure in patients without significant pulmonary hypertension; however it has not been validated for patients with pulmonary hypertension.Methods: We evaluated 44 consecutive patients with pulmonary hypertension undergoing preoperative evaluation for pulmonary thromboendarterectomy surgery. The right heart was imaged in the apical 4-chamber view. Peak early tricuspid valve inflow velocity (Et) and early diastolic tissue velocity at the lateral tricuspid annulus (Etm) were measured. The results were compared with direct measurements of right atrial (RA) pressures using fluid-filled catheters.
Results: Mean RA pressure was 10+7 mm Hg and mean systolic pulmonary artery pressure was 77+18 mm Hg. The quotient of Et divided by Etm correlated poorly with mean RA pressure (r=0.08, p=NS, Figure). This correlation remained poor and statistically insignificant even when the dataset was restricted to exclude patients with severe tricuspid regurgitation (r=0.09, p=NS) or to exclude those with moderate or severe tricuspid regurgitation (r=0.29, p=NS). In addition, peak Etm velocity
alone correlated poorly with right atrial pressure (r=0.15, p=NS).Conclusion: Unlike analogous measurements in patients without pulmonary hypertension, tissue Doppler measurements at the tricuspid valve annulus do not correlate with RA pressure in patients with pulmonary hypertension. This dichotomy may be due to effects of pulmonary hypertension on the structure, function, and relaxation dynamics of the right ventricle. Therefore the ratio of Et to Etm should not be used as an estimate of RA pressures in patients with pulmonary hypertension.
Journal of the American Society of EchocardiographyVolume 19 Number 5 Abstracts 621

P3-11
Diastolic Dysfunction and LA Enlargement are Responsible for Development of Functional Mitral Regurgitation in Dilated Cardiomyopathy : Not Vice Versa
Seong-Mi Park, Grace C Casaclang-Verzosa, Maurice E Sarano, Steve R Ommen, Patricia A Pellikka, Fletcher A Miller, Jae K Oh Mayo Clinic, Rochester, MN
Background : Functional mitral regurgitation (MR) is a frequent comorbidity in patients with advanced dilated cardiomyopathy (DCM) and is one of the strongest risk factors for prognosis. Different mechanisms have been proposed to account for MR in these patients. Not all DCM patients show significant MR or enlarged left atrum (LA) despite severe left ventricular (LV) dilatation. ACORN trial has provided an ideal opportunity to identify structural and functional parameters best correlated with the severity of MR in DCM.Methods : From the baseline echocardiographic results of Acorn cardiac support device trials, 144 patients (53 ± 13 years, 53% men) with DCM and sinus rhythm, but without organic mitral valve disease and ischemic heart disease were identified. All patients were stable and had optimal medical management. Echocardiographic parameters were measured off-line by the Echo Core Lab at Mayo Clinic. The severity of MR assessed by visual assessment of color flow imaging (Grade 0 to 4+). All parameters were indexed based on patient’s body surface area.Results : In all patients, the mean LVEF and LVEDV index were 25 ± 10 % and 135 ± 48 ml/m2.Eighty-six (60%) patients had significant MR ? 2+ (MR group). Tenting area, tenting height, tethering distance, LA volume, mitral annular diameter were larger in MR group, but there was no significant difference in LVEDV index and LVESV index (p=0.20 and p=0.38) between two groups. Tenting area showed good relation with MR severity (tenting area, r=0.50, p<0.001) and was most significantly correlated to mitral annular diameter (r=0.92, p<0.001) compared to other parameters (tenting height, r=0.27; tethering distance, r=0.43; LVESV index, r=0.27, p<0.01, LV sphericity, r=0.29, p<0.05). Moreover, mitral annular diameter showed a good correlation with LA volume (r=0.66, p<0.001) than LVESV index (r=0.27, p=0.005). The same correlation was found in no MR group (MR ? 1, LA volume, r=0.60, p<0.001; LVESV index, r=0.20, p>0.05). Additionally, LA volume was better correlated with LV diastolic dysfunction than LVEDV index (LA volume, r=0.58, p<0.001; LVEDV index, r=0.32, p=0.003).Conclusion : In advanced DCM, there was no significant difference in LV volume, but were differences in LA volume and mitral annular diameter between no MR and MR group. Mitral annular diameter and LA volume were closely related each other even in patients without significant MR. These findings suggest that increase in LA volume by more advanced diastolic dysfunction may have a major contribution to development of significant MR by augmentation of mitral annular dilatation in DCM.
P3-12
Comparison of a Novel Artificial Intelligence Echocardiographic Image Analysis System with Visual Assessment of Ejection Fraction by Expert and Novice Readers
Maxime Cannesson, Masaki Tanabe, Matthew S Suffoletto, Dennis M McNamara, John Gorcsan, III University of Pittsburgh, Pittsburgh, PA
Background: Visual assessment of ejection fraction (EF) is used often in clinical practice, but is subjective and requires training and experience.Methods: We studied 130 patients to test the hypothesis that a novel image analysis system using artificial intelligence pattern recognition programming (Auto EF, Siemens Corp), unlike previous automated border detection, is more reproducible and more accurate than visual EF. Auto EF incorporated pattern and shape recognition to automatically locate the left ventricle, track the endocardium, and calculate EF in < 15 sec from routine digital images. Results were independently compared with routine visual EF by blinded expert readers (n = 130) and visual EF by blinded novice readers with only 1 month of echo training (n = 60). Manually traced EF by biplane Simpson’s rule by a separate group of blinded investigators was used as the reference.Results: Auto EF correlated well with visual EF by expert readers (r=0.97, 5% limits of agreement), but intraobserver and interobserver variabilities in visual EF were greater than Auto EF: 1±4 % vs. 0.5±1 % and 10±6% vs. 1±2 %, respectively (p < 0.001). Visual EF by novice readers was less accurate, as expected (r=0.82, 19% limits of agreement) (LEFT Panels) while trainee-operated Auto EF had more favorable results (r=0.98, 7% limits of agreement) (RIGHT panels).Conclusions: Auto EF is more reproducible than visual EF by expert readers, more accurate than visual EF by novice readers, and has potential clinical applications.
P3-13
Left Atrial Volume is an Independent Predictor of Exercise Capacity in Patients with Isolated Diastolic Dysfunction
Hazel P Penafiel, Raymond Ching-Chiew Wong, Tiong Cheng Yeo National University Hospital, Singapore, Singapore
Background: Left atrial (LA) volume reflects left ventricular (LV) diastolic properties and is a marker of the severity and duration of diastolic dysfunction. LV diastolic dysfunction is an important determinant of exercise capacity in patients with normal LV systolic function. We hypothesize that LA volume predicts exercise capacity in patients with isolated LV diastolic dysfunction.Methods: We performed echocardiography and maximal exercise testing in 256 patients with normal LV systolic function (LVEF � 50%). Diastolic dysfunction was determined using on standard Doppler criteria. LA volume was measured using the ellipsoid method and maximum LA volume (Vol max) was indexed to the body surface area. Univariate and multivariate predictors of exercise capacity in patients with isolated diastolic dysfunction were then determined.Results: Mean age was 45 ± 15 years, with 73% male, 119 patients had diastolic dysfunction. Patients with diastolic dysfunction had higher indexed LA Vol max (20 ± 6 ml/m2 vs 18 ± 4 ml/m2, p = 0.004) and lower exercise capacity (10 ± 3 METs vs 12 ± 3 METs, p<0.001). Univariate predictors of exercise capacity were age, gender, LV mass index, mitral E/A, E wave deceleration time, ratio of early diastolic mitral inflow velocity to early diastolic mitral annular velocity (E/Ea), and indexed LA Vol max. On multivariate analysis, only age (p<0.001) and indexed LA Vol max (p = 0.003) were independent predictors of exercise capacity. Exercise capacity was similar in the patients with normal diastolic function and those with diastolic dysfunction and normal indexed LA Vol max . In contrast, patients with diastolic dysfunction and increased indexed LA Vol max had reduced exercise capacity (p = 0.002) (see figure).Conclusion: Indexed LA volume is an independent and reliable predictor of exercise capacity in patients with isolated diastolic dysfunction. In these patients, exercise capacity is reduced only if LA volume is increased.
P3-14
Tissue Doppler Imaging During Parabolic Flight to Evaluate Preload Independence of Left Ventricular Mitral Annular Velocity
Enrico G Caiani1, Masaki Takeuchi2, Lynn Weinert3, Pierre Vaida4, Roberto M Lang3
1Politecnico di Milano, Milano, Italy; 2Tane General Hospital, Osaka, Japan; 3University of Chicago, Chicago, IL; 4Université Bordeaux 2, Médecine Aérospatiale EA518, Bordeaux, France
Tissue Doppler imaging (TDI) has been recently proposed as a new approach to assess left ventricular (LV) diastolic function. However, the preload independence of the early diastolic mitral annular velocity (E’) measured by TDI still remains controversial. As parabolic flight represents a unique experimental setup to study the effects on the heart of reversible and repeatable acute non-pharmacologically induced variations in preload, our goal was to evaluate the preload independence of E’ to both the reduction and the increase of venous return occurring with changes in gravity during parabolic flight. Methods. TDI images were obtained in 10 normal unmedicated subjects (age 38±11 yrs) in an upright position during parabolic flights (Airbus A-300 Zero-G, CNES-ESA, Bordeaux, France) using a broad-band transducer (S3, Philips iE33). TDI image acquisition (apical 4-chamber long-axis view) of three consecutive beats was performed with breath-hold during normogravity (1G), the ascent phase of hypergravity (1.8G), and microgravity (0G). Data were stored and analyzed off-line (SQ, QLAB v. 4.2, Philips). For each gravity level, regional myocardial velocity curves in the basal inter-ventricular septum (IVS) and in the basal lateral (LAT) segments were reconstituted offline from the TDI color images, from which E’ and late diastolic mitral annular velocity (A’) were measured and averaged over three beats. Results. Both in the IVS and LAT segments, E’ increased significantly (p<0.01) in its absolute value at 0G, compared to 1G (IVS: from 3.45±0.98 cm/s at 1G to 6.45±1.62 cm/s at 0G; LAT: from 2.72±0.96 cm/s to 5.05±1.97 cm/s), while at 1.8G E’ did not change (IVS: 3.42±1.68 cm/s; LAT: 2.15±1.61 cm/s), compared to 1G. Conversely, both in the IVS and LAT segments, A’ did not change at 0G (IVS: from 3.5±1.6 cm/s at 1G to 4.8±1.4 cm/s at 0G; LAT: 3.1±1.1 cm/s at 1G to 3.1±1.2 cm/s at 0G) while it was significantly reduced at 1.8G (IVS: 2.8±1.6 cm/s; LAT: 2.4±1.1 cm/s) Conclusion.During parabolic flight, while a reduction in preload induced by hypergravity was found to influence late diastolic mitral annular velocity, E’ was significantly affected by the increase in preload elicited by 0G. This fact should be considered in the utilization of E’ and A’ in clinical practice.
Journal of the American Society of Echocardiography622 Abstracts May 2006

P3-15
Holdover of Postsystolic Thickening as a Sign of Ischemic Memory After Short Myocardial Ischemia
Ayumi Uranishi, Toshihiko Asanuma, Asuka Taniguchi, Kasumi Masuda, Kentaro Otani, Fuminobu Ishikura, Shintaro Beppu Division of Functional Diagnostic Science, Osaka University Graduate School of Medicine, Suita, Japan
Background: Regional myocardial function can be quantified by noninvasive ultrasonic strain analysis. Postsystolic thickening derived from ultrasonic strain analysis is a sensitive parameter for myocardial ischemia and this abnormal motion is also observed in stunned myocardium. However, it is still unclear how long postsystolic thickening continues after ischemia of short duration. We, therefore, sought to investigate the recovery from the postsystolic thickening after ischemia of short duration.Methods: Left anterior descending artery was occluded for 5 (n=8) or 15 (n=5) minutes in 13 open-chest dogs. In the Tissue Doppler mode using an Aplio ultrasound system (Toshiba), short-axis images were acquired at baseline, during occlusion and 120 minutes after reperfusion. Peak systolic strain (ε sys) and strain at mitral valve opening (ε mvo) were measured in the center of the risk area. Postsystolic strain was calculated as the subtraction of ε sys from ε mvo. Myocardial contrast echocardiography was performed for assessing the risk area.
Results: The extent of the risk area was almost identical between 5 minutes occlusion and 15 minutes occlusion groups (26.5±4.3% vs. 29.1±8.1%, p=0.52). Also peak systolic strain at the end of occlusion was not different between 5 minutes occlusion and 15 minutes occlusion groups (-8.4±9.9% vs. -4.0±10.6%, p=0.46). Peak systolic strain recovered immediately after reperfusion in the 5 minutes occlusion group, although it did not even 120 minutes after reperfusion in the 15 minutes occlusion group (fig.1). Postsystolic strain in the 5 minutes occlusion group, on the other hand, was postponed for 30 minutes after reperfusion, as in the 15 mimutes occlusion group (fig.2).Conclusion: Even if regional systolic function is recovered after short ischemia,
postsystolic thickening can be observed for relatively long time. The assessment of postsystolic strain may have possibility for ischemic memory imaging.
P3-16
Increased Myocardial Energy Expenditure in Patients with Chronic Kidney Disease on Hemodialysis: The Strong Heart Study
Daniel G Krauser1, Mary Jane Farr1, Jonathan N Bella1, Vitorio Palmieri1, Mary J Roman1, Jason G Umans2, Elisa T Lee3, Richard B Devereux1
1New York Presbyterian Hospital - Weill Cornell Medical Center, New York, NY; 2MedStar Research Institute, Washington, DC; 3Oklahoma University, Oklahoma City, OK
Introduction: Non-invasively derived myocardial energy expenditure (MEE) parallels the concept of tension-time index as a determinant of myocardial oxygen demand. Previous work has demonstrated that chronic volume overload from valvular regurgitation is associated with increased MEE, which may contribute to volume-related left ventricular (LV) dilation and subsequent dysfunction. Whether other high-output or volume overload states such as hemodialysis (HD) in patients with chronic kidney disease are associated with increased MEE is unknown.Methods: We examined 2,650 participants from the 2nd exam of the Strong Heart Study. Clinical and echocardiographic data were compared between HD and non-HD participants. LV MEE was estimated by 3.98 x 10-7 x (LV mass x end-systolic stress (ESS) x ejection time [g x kdyne/cm2 x sec]) x heart rate; named MEElvm and expressed in Kcal per minute, paralleling the tension-time index as a determinant of myocardial oxygen demand. Alternatively, MEE was estimated by the product 4.2 x 10-7 x Doppler stroke volume (SV) x ESS x ejection time x heart rate, named MEEsv. Multivariable regression analysis was used to determine the relationship between MEE and HD.Results: 120 (4.6%) patients had renal insufficiency defined as serum creatinine >/= 2 and 60 of these were on chronic HD. HD patients were more likely to have LV dysfunction, hypertension, diabetes, history of coronary heart disease or heart failure, and >1+ mitral regurgitation. HD patients had a higher pulse, LV mass, circumferential and meridional ESS, and pulse pressure. There was no difference in ejection time, fat-free mass, hemoglobin, significant aortic regurgitation, or SV between HD and non-HD groups. There was a stepwise increase in MEE between groups without significant renal dysfunction, with renal insufficiency, and those on HD (.16±.08 vs. .20±.11 vs. .32±.16 for MEElvm, P<0.01 for all comparisons; .10±.04 vs. .12±.06 vs. .15±.06 for MEEsv, P<0.01 for all comparisons). In multivariable regression analysis adjusting for relevant covariates, HD was independently associated with both increased MEElvm (β=0.17, p<0.001) and MEEsv (β=0.12, p<0.001). Other factors strongly associated with MEE included EF (β=-0.40, p<0.001), mean blood pressure (β=0.26, p<0.001), and fat-free body mass (β=0.40, p<0.001).Conclusion: In a population-based sample with a large prevalence of traditional risk factors, HD is independently associated with increased MEE. Further studies are required to determine whether this non-invasive measure predicts subsequent LV dysfunction and cardiovascular events in HD patients.
P3-17
Effects of Simulated High Altitude on Global and Regional Left Ventricular Performance and Filling Pressure
Jesper Kjaergaard1, Eric M Snyder1, Christian Hassager2, Thomas P Olson1, Jae K Oh1, Bruce D Johnson1
1Mayo Clinic College of Medicine, Rochester, MN;2Copenhagen University Hospital, Dept. of Cardiology, Copenhagen, Denmark
Background High Altitude Pulmonary Edema (HAPE) is believed to be a hydrostatic edema in part related to increased pulmonary capillary pressure caused by hypoxic pulmonary vasoconstriction. It is possible that elevated left atrial pressure may also contribute to the elevated pressures. This study investigated to impact of simulated high altitude on global and regional echocardiographic measures of LV performance and filling pressure.Methods Seventeen healthy individuals underwent a supine echocardiography study, including tissue Doppler of the septal Mitral annulus and basal segment, before and after an 18-hour overnight stay in a high altitude simulation tent at FiO2=12.3% (simulating 4000 m above sea level). Early and late Mitral flow velocities (E and A, resp.) and time intervals, as well as peak early myocardial relaxation velocity (e’) were recorded. MPI was calculated as the sum of isovolumic periods (IVCT and IVRT) divided by LV ejection time (LVET). RV systolic pressure was estimated form the Tricuspid regurgitation velocity.Results Compared to baseline, increases in the RV pressure (24±3 to 32±7 mmHg, p<0.0001) and in heart rate (60±10 to 68±14 bpm, p<0.01) were seen with hypoxia, whereas cardiac index and LV ejection fraction were unaffected (2.4±0.4 to 2.5±0.5 l/min/m2, NS and 61±4 to 60±6%, NS, respectively). A small decrease in mean arterial blood pressure was seen (91±8 to 87±7 mmHg, p<0.05). The regional basal myocardial velocity decreased slightly (7.3±0.6 to 6.8±0.7 cm/s, p<0.05), whereas no changes were seen in the strain (15±6 to 17±4 %, NS).The E velocity was unchanged and the A increased (75±14 to 71±13 cm/s, NS and 48±0 to 56 ±16 cm/s, p<0.05, resp.), whereas the e’ decreased significantly (11.5±2.9 to 9.0±2.3, p<0.0001). See Figure for data on the E/e’ and MPI. The IVRT increased significantly (55±31 to 87± msec, p<0.001) whereas the IVCT and LVET were unchanged.
Conclusion Simulated high altitude leads to decreasing LV performance with an accompanying increase in LV filling pressure. The significant changes in filling pattern and IVRT in the setting of normal and un-changed systolic function, indicates that hypoxia induces mild diastolic dysfunction, even in young healthy individuals.Supported by NIH grant
HL71478.
P3-18
Objective Assessment of Right Ventricular Systolic Function with Midventricular Systolic Strain in Patients with Acute Pulmonary Thromboembolism
Jae-Hyeong Park, Jae-Hwan Lee, Si-Wan Choi, Jin-Ok Jeong, Soo Jin Park, Min Su Lee, Yun Seon Park, In Whan Seong Chungnam National University Hospital, Daejeon, Republic of Korea
Background: Cor pulmonale is defined as the structural and functional alternation of the right ventricle (RV) caused by a primary disorder of the respiratory system. Although the majority of cor pulmonale has a chronic and slowly progressive course associated with chronic obstructive coronary disease (COPD), acute cor pulmonale can be complicated with acute pulmonary thromboembolism (PTE). We aimed to differentiate acute cor pulmonale from chronic cor pulmonale with strain analysis of RV.Patients and methods: From March 2005 to September 2005, total 23 patients, 12 consecutive patients with acute PTE (6 males, mean 67±9 years; range 44~75) and 11 consecutive patients with severe COPD (7 males, mean 63±14 years; range 34~77), were included. Echocardiographic data were assessed by Vivid 7 (GE Medical Systems, Waukesha, Wisconsin).Results: There was no statistical difference in age and gender in both groups. Tricuspid regurgitation maximal velocity (TR Vmax) (3.7±0.7 vs 3.7±0.3 m/sec, p=0.260) and myocardial performance index of RV (0.57±0.21 vs 0.70±0.14, p=0.091) were similar. However, mean RV EF (21.6±12.6% vs 33.7±7.6%, p=0.011) and fractional area change of RV (FACRV) (15.8±8.6 vs 26.4±6.6%, p=0.009) were more decreased in patient with acute PTE. Midventricular systolic strain of RV was significantly decreased in patients with acute PTE (-1.02±11.19 vs -20.05±8.9%, p<0.001). Regarding the midventricular systolic strain of RV in the detection of acute PTE by the receiver operating curve, the best sensitivity and specificity were obtained when -13.6% was applied as the criterion. Using this criterion (midventricular systolic strain of RV less than -13.6% for predicting an acute PTE), the sensitivity, specificity and accuracy were 91.7%, 81.8% and 87.0%, respectively.Conclusions: Analysis of midventricular systolic strain of RV using tissue Doppler techniques can give useful information in differentiation of acute PTE from chronic cor pulmonale complicated with COPD. This can reduce the use of other diagnostic studies including computerized tomographic scans in the emergency room.
Journal of the American Society of EchocardiographyVolume 19 Number 5 Abstracts 623
P3-19
Novel Assessment of Cardiac Dyssynchrony Using Variance of Dyssynchrony Vector on Tissue Doppler Imaging to Predict Reverse Remodeling
Takeshi Arita1, Brandon Fornwalt1, Dean Notabartolo2, Maria A Pernetz1, Stamatios Lerakis1, Stephens D Clements1, Dan Sorescu1, John D Merlino2, Randolph P Martin1, Angel R Leon2
1Emory University School of Medicine, Atlanta, GA;2The Carlyle Fraser Heart Center/Emory University School of Medicine, Atlanta, GA
Background Quantitation of intraventricular mechanical dyssynchrony may help predict response to cardiac resynchronization. Analyses of the standard deviation (SD) of time to peak systolic velocity (TPVs) across the LV reflect numerical variance but neglect spatial information on the direction of wall motion. The concept of vector assessment that provides magnitude of dyssynchrony and the spatial location of the most dyssynchronous segment may also predict response.Methods Patients (n=32) with advanced heart failure (age 66 ±10, NYHA 3.1±0.5, QRS width 173 ± 20.8msec, sinus rhythm 26(81%), EF 22.4±8.2%) underwent CRT-P or CRT-D implant with LV lead placement along the lateral wall. Echocardiography with tissue Doppler imaging (GE Vingmed) obtained on apical 4-, 3-, 2-chamber views pre-implant and 3month post-CRT assessed intraventricular dyssynchrony using three parameters: The SD of time to peak velocity in 12 segments, dispersion of TPVs in 12 segments and 4 basal segments , and the novel vector method that calculates the degree of dyssynchrony and the direction toward the most delayed segment. ROC analysis determined the cut-off value for the magnitude and direction of the net vector of dyssynchrony.
Results 19 patients (59%) demonstrated reverse remodeling (- DESV>15%). Baseline characteristics did not differ between responders
and nonresponders. Figure 1 plots the magnitude and direction of the net vector for each group. The predictive values for the parameters appear in table 1. Adopting a cut-off numerical value of 18.4 msec and a direction of the net vector less than -47 degrees with this novel method appears highly predictive and relatively advantageous over numerical assessments of time to peak velocity.Conclusion Vector-weighed variance method identifies the degree of dyssynchrony and the direction to the most delayed segment(s). Initial comparisons to scalar variance of time to peak velocity method might suggest superiority of the vector approach.
SD of 12 segments Dispersion of TPVs in Dispersion of TPVs Magnitude of vector Direction of vector Mag AND Mag OR (>34.4msec) 12 seg (>105msec) in basal 4 segments (>65msec) �18.4msec (Mag) �-47 (Dir) Dir DirSensitivity (%) 63 74 53 63 89 53 95Specificity (%) 38 15 46 62 62 92 31Positive Predictive Value 0.60 0.56 0.59 0.71 0.77 0.92 0.67Negative Predictive Value 0.42 0.29 0.40 0.53 0.80 0.60 0.80
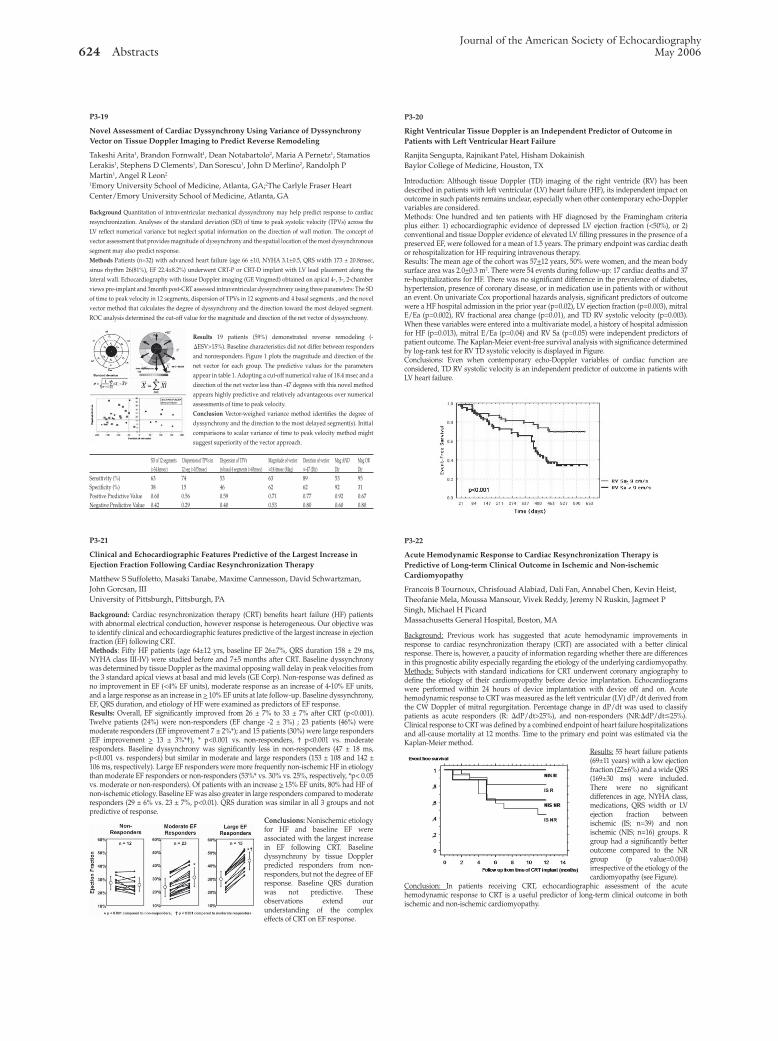
P3-20
Right Ventricular Tissue Doppler is an Independent Predictor of Outcome in Patients with Left Ventricular Heart Failure
Ranjita Sengupta, Rajnikant Patel, Hisham Dokainish Baylor College of Medicine, Houston, TX
Introduction: Although tissue Doppler (TD) imaging of the right ventricle (RV) has been described in patients with left ventricular (LV) heart failure (HF), its independent impact on outcome in such patients remains unclear, especially when other contemporary echo-Doppler variables are considered.Methods: One hundred and ten patients with HF diagnosed by the Framingham criteria plus either: 1) echocardiographic evidence of depressed LV ejection fraction (<50%), or 2) conventional and tissue Doppler evidence of elevated LV filling pressures in the presence of a preserved EF, were followed for a mean of 1.5 years. The primary endpoint was cardiac death or rehospitalization for HF requiring intravenous therapy.Results: The mean age of the cohort was 57+12 years, 50% were women, and the mean body surface area was 2.0+0.3 m2. There were 54 events during follow-up: 17 cardiac deaths and 37 re-hospitalizations for HF. There was no significant difference in the prevalence of diabetes, hypertension, presence of coronary disease, or in medication use in patients with or without an event. On univariate Cox proportional hazards analysis, significant predictors of outcome were a HF hospital admission in the prior year (p=0.02), LV ejection fraction (p=0.003), mitral E/Ea (p=0.002), RV fractional area change (p=0.01), and TD RV systolic velocity (p=0.003). When these variables were entered into a multivariate model, a history of hospital admission for HF (p=0.013), mitral E/Ea (p=0.04) and RV Sa (p=0.05) were independent predictors of patient outcome. The Kaplan-Meier event-free survival analysis with significance determined by log-rank test for RV TD systolic velocity is displayed in Figure.Conclusions: Even when contemporary echo-Doppler variables of cardiac function are considered, TD RV systolic velocity is an independent predictor of outcome in patients with LV heart failure.
P3-21
Clinical and Echocardiographic Features Predictive of the Largest Increase in Ejection Fraction Following Cardiac Resynchronization Therapy
Matthew S Suffoletto, Masaki Tanabe, Maxime Cannesson, David Schwartzman, John Gorcsan, III University of Pittsburgh, Pittsburgh, PA
Background: Cardiac resynchronization therapy (CRT) benefits heart failure (HF) patients with abnormal electrical conduction, however response is heterogeneous. Our objective was to identify clinical and echocardiographic features predictive of the largest increase in ejection fraction (EF) following CRT.Methods: Fifty HF patients (age 64±12 yrs, baseline EF 26±7%, QRS duration 158 ± 29 ms, NYHA class III-IV) were studied before and 7±5 months after CRT. Baseline dyssynchrony was determined by tissue Doppler as the maximal opposing wall delay in peak velocities from the 3 standard apical views at basal and mid levels (GE Corp). Non-response was defined as no improvement in EF (<4% EF units), moderate response as an increase of 4-10% EF units, and a large response as an increase in > 10% EF units at late follow-up. Baseline dyssynchrony, EF, QRS duration, and etiology of HF were examined as predictors of EF response.Results: Overall, EF significantly improved from 26 ± 7% to 33 ± 7% after CRT (p<0.001). Twelve patients (24%) were non-responders (EF change -2 ± 3%) ; 23 patients (46%) were moderate responders (EF improvement 7 ± 2%*); and 15 patients (30%) were large responders (EF improvement > 13 ± 3%*†), * p<0.001 vs. non-responders, † p<0.001 vs. moderate responders. Baseline dyssynchrony was significantly less in non-responders (47 ± 18 ms, p<0.001 vs. responders) but similar in moderate and large responders (153 ± 108 and 142 ± 106 ms, respectively). Large EF responders were more frequently non-ischemic HF in etiology than moderate EF responders or non-responders (53%* vs. 30% vs. 25%, respectively, *p< 0.05 vs. moderate or non-responders). Of patients with an increase > 15% EF units, 80% had HF of non-ischemic etiology. Baseline EF was also greater in large responders compared to moderate responders (29 ± 6% vs. 23 ± 7%, p<0.01). QRS duration was similar in all 3 groups and not predictive of response.
Conclusions: Nonischemic etiology for HF and baseline EF were associated with the largest increase in EF following CRT. Baseline dyssynchrony by tissue Doppler predicted responders from non-responders, but not the degree of EF response. Baseline QRS duration was not predictive. These observations extend our understanding of the complex effects of CRT on EF response.
P3-22
Acute Hemodynamic Response to Cardiac Resynchronization Therapy is Predictive of Long-term Clinical Outcome in Ischemic and Non-ischemic Cardiomyopathy
Francois B Tournoux, Chrisfouad Alabiad, Dali Fan, Annabel Chen, Kevin Heist, Theofanie Mela, Moussa Mansour, Vivek Reddy, Jeremy N Ruskin, Jagmeet P Singh, Michael H Picard Massachusetts General Hospital, Boston, MA
Background: Previous work has suggested that acute hemodynamic improvements in response to cardiac resynchronization therapy (CRT) are associated with a better clinical response. There is, however, a paucity of information regarding whether there are differences in this prognostic ability especially regarding the etiology of the underlying cardiomyopathy.Methods: Subjects with standard indications for CRT underwent coronary angiography to define the etiology of their cardiomyopathy before device implantation. Echocardiograms were performed within 24 hours of device implantation with device off and on. Acute hemodynamic response to CRT was measured as the left ventricular (LV) dP/dt derived from the CW Doppler of mitral regurgitation. Percentage change in dP/dt was used to classify patients as acute responders (R: DdP/dt>25%), and non-responders (NR:DdP/dt�25%). Clinical response to CRT was defined by a combined endpoint of heart failure hospitalizations and all-cause mortality at 12 months. Time to the primary end point was estimated via the Kaplan-Meier method.
Results: 55 heart failure patients (69±11 years) with a low ejection fraction (22±6%) and a wide QRS (169±30 ms) were included. There were no significant differences in age, NYHA class, medications, QRS width or LV ejection fraction between ischemic (IS; n=39) and non ischemic (NIS; n=16) groups. R group had a significantly better outcome compared to the NR group (p value=0.004) irrespective of the etiology of the cardiomyopathy (see Figure).
Conclusion: In patients receiving CRT, echocardiographic assessment of the acute hemodynamic response to CRT is a useful predictor of long-term clinical outcome in both ischemic and non-ischemic cardiomyopathy.
Journal of the American Society of Echocardiography624 Abstracts May 2006

P3-23
Acute and Chronic Effects of Continuous Positive Airway Pressure Therapy on Left Ventricular Systolic and Diastolic Function in Patients with Obstructive Sleep Apnea and Congestive Heart Failure
Ian G Burwash1, Chris B Johnson1, Keiichiro Yoshinaga1, Haissam Haddad1, Judith Leech2, Rob de Kemp1, Rob S Beanlands1
1University of Ottawa Heart Institute, Ottawa, ON, Canada; 2Sleep Medicine Centre, University of Ottawa, Ottawa, ON, Canada
Background: Obstructive sleep apnea (OSA) may contribute to the pathogenesis and progression of congestive heart failure (CHF). Nocturnal continuous positive airway pressure (CPAP) therapy can alleviate OSA and may have a role in the treatment of CHF patients. The purpose of this study was to investigate the acute and chronic effects of CPAP therapy on left ventricular systolic function, diastolic function and left ventricular filling pressures in patients with CHF and OSA.Methods: Seven patients with stable CHF (NYHA class 2 or 3 heart failure, LVEF<40%) and OSA (apnea-hypopnea index >15 events/hr, >80% obstructive events) underwent echocardiographic examinations at baseline (awake, before CPAP therapy), during acute CPAP therapy and after 6.9+3.3 weeks of nocturnal CPAP therapy (chronic CPAP therapy).Results: Acute CPAP therapy resulted in a decrease in stroke volume (44+15 vs. 50+14 mL, p=0.002) and LVEF (34.8+5.0 vs. 38.4+3.3 %, P=0.006) compared to baseline. There was no significant change in Ea (6.0+1.6 vs. 6.3+1.6 cm/s, p=NS), E/A ratio (1.05+0.79 vs. 1.00+0.67, p=NS) or E/Ea ratio (10.9+4.1 vs. 11.3+4.1, p=NS). In contrast, chronic CPAP therapy resulted in an increase in stroke volume (59+19 vs. 50+14 ml, p=0.07) and LVEF (43.4+4.8 vs. 38.4+3.3%, p=0.01) compared to baseline. The change in stroke volume and LVEF with chronic CPAP therapy was directly related to the baseline systemic vascular resistance index (r=0.78, p=0.037; and r=0.69, p=0.08, respectively). However, there was no significant change in Ea (6.2+1.2 vs. 6.3+1.6 cm/s, p=NS), E/A ratio (1.13+0.61 vs. 1.00+0.67, p= NS) or E/Ea ratio (12.1+2.7 vs. 11.3+4.1, p=NS).Conclusions: Acute CPAP therapy decreases stoke volume and LVEF in stable patients with CHF and OSA. In contrast, chronic CPAP therapy for 7 weeks improves left ventricular systolic function, but does not affect left ventricular diastolic function or left atrial pressure. The potential clinical implications of the discrepant effect of CPAP therapy on left ventricular systolic function and diastolic function in patients with CHF and OSA warrant further study.
P3-24
Lateral Mitral Annular Velocity Has the Best Correlation with Exercise Tolerance Regardless of Left Ventricular Systolic Function
Yasuyuki Hadano, Kazuya Murata, Nobuaki Tanaka, Eizo Akagawa, Takeo Tanaka, Hideki Kunichika, Masunori Matsuzaki Yamaguchi University, Ube, Japan
Background: The ratio of the transmitral early diastolic velocity (E) to the early diastolic velocity of the mitral annulus obtained by tissue Doppler imaging has been proposed for evaluating exercise tolerance. However, the impact of left ventricular ejection fraction (LVEF) on estimation of exercise tolerance using tissue Doppler imaging is unknown.Methods: We studied 66 consecutive patients with heart disease. All patients were in sinus rhythm and without atrial fibrillation, mitral stenosis, severe mitral regurgitation, or prosthetic mitral valve. Of the patients, 30 had LVEF > 50% and 36 had LVEF < 50%. We measured the transmitral E velocity by pulsed-wave Doppler and the early diastolic velocities of the lateral (LEa) and septal (SEa) mitral annulus by pulsed-wave tissue Doppler imaging; and then calculated the ratios of E to LEa and SEa. Immediately after echocardiography, we measured peak oxygen consumption and anaerobic threshold by cardiopulmonary exercise testing. The correlations of these Doppler indices with peak oxygen consumption or anaerobic threshold were evaluated in each group of LVEF > 50% and LVEF < 50%.Results: Nine (30%) of patients with LVEF > 50% and 26 (72%) of those with LVEF < 50% had a history of congestive heart failure. LVEF, left ventricular end-diastolic dimension, or left atrial dimension did not correlate with exercise tolerance in patients with preserved or impaired LVEF. Conventional Doppler indices correlated weakly with exercise tolerance in patients with LVEF > 50%. In patients with LVEF > 50%, E/LEa correlated well with peak oxygen consumption and anaerobic threshold (r = -0.62, r = -0.69, p < 0.001, respectively), however, E/SEa correlated modestly (r = -0.57, r = -0.60, p < 0.001, respectively). In patients with LVEF < 50%, E/LEa correlated well with peak oxygen consumption and anaerobic threshold (r = -0.72, r = -0.76, p < 0.001, respectively), and E/SEa also correlated well (r = -0.63, r = -0.63, p < 0.001, respectively).Conclusion: Evaluation of left ventricular diastolic function using tissue Doppler imaging was related to exercise tolerance in patients with both preserved and impaired LVEF. E/LEa obtained by tissue Doppler imaging has the best correlation with exercise tolerance, especially anaerobic threshold, and may be useful in the noninvasive estimation of exercise tolerance, regardless of LVEF.
P3-25
Radial Strain, Circumferential Strain, and Radial Displacement Depict Regional Dysfunction in a Swine Model of Myocardial Infarction
Jing Ping Sun, David Chou, Hsuan-Hung Chuang, Kai Wang, Jeanne Drinko, Allen Borowski, James D. Thomas, William J. Stewart The Cleveland Clinic Foundation, Cleveland, OH
Background: Tissue Doppler-derived strain and strain rate imaging has been used to demonstrate impairment of regional myocardial function in patients with cardiac diseases. However, this application has been largely limited to the evaluation of longitudinal myocardial function. The purpose of this study was to apply radial strain (RS), circumferential strain (CS) and wall thickening/radial displacement (RD) analysis in differentiating the infarct, adjacent and remote zones in a swine model of myocardial infarction (MI). Methods and Results: Seven pigs were subjected to myocardial infarction (MI) by occlusion of the left anterior descending coronary artery (LAD) and followed up for 8 weeks. Cine-loop images were acquired at three short-axis levels (base, mid and apex) of the left ventricle using a Vivid 7 machine (GE Medical Systems). Regional functions (CS, RS, RD and rotation) were compared between the infarct, adjacent and remote zones according to the territorial distribution of various coronary arteries (right coronary-RCA, left descending artery-LAD and left circumflex-LCX).
Circumferential Strain (%) Radial Strain (%) Radial Displacement (cm) RCA LAD LCX RCA LAD LCX RCA LAD LCXBaseline 15±3 13±3 11±4 34±17 31±16 44±24 3.9±1.3 2.9±0.8 4.3±1.2AMI 12±4 7±2** 9±3 32±16 12±7** 28±12 4±1.4 1.4±0.6** 2.9±0.8*4 weeks 13±4 7±2** 11±2 20±11 17±4* 25±16 3.6±1.6 1.8±0.7* 4.2±1.36 weeks 15±3 6±2** 13±6 33±10 14±4* 33±7 4.3±1.3 1.7±0.4** 5±28 weeks 13±3 6±1.6** 10±5 21±13 13±6* 25±11 3.4±1.9 1.3±1* 3.4±1.9
* vs Baseline p <0.05, ** vs Baseline p <0.01Conclusions: Myocardial dysfunction defined by radial strain, circumferential strain, and radial displacement was abnormal in LAD-territory segments, but normal in adjacent and remote zones. These novel methods of imaging segmental myocardial dysfunction may be useful in experimental and clinical diagnosis of myocardial ischemia and infarction.
P3-26
Abnormalities in the Index of Myocardial Performance in Patients with Left Ventricular Hypertrophy and Normal Ejection Fraction
Francis W Grzywacz, Alfred A Bove, Arnold Meshkov Temple University Hospital, Philadelphia, PA
BACKGROUND: Increased left ventricular mass is a strong risk factor for cardiovascular morbidity and mortality. Noninvasive markers identifying higher risk patients are lacking. The index of myocardial performance (IMP), an echocardiographic measurement, has been used to identify systolic and diastolic dysfunction. This study assessed the relationship of IMP to LV mass index (LVMI) in patients with normal LV ejection fraction (LVEF).METHODS: Echocardiography was performed on 75 pts with concentric LVH (= 11mm wall thickness) and normal LVEF (>50%), and 25 age-matched controls. IMP was calculated utilizing 3-5 different Doppler time intervals measured during mitral valve inflow and left ventricular outflow. Left ventricular mass was calculated using the M-Mode formula assuming cuboid geometry of the LV end diastolic diameter, interventricular septal thickness and posterior wall thickness.RESULTS: The LV mass (g) and LV mass index (g/m2) in the control patients (<11mm) were 227 ± 46 and 123 ± 23. Patients with mild (11-13mm), and moderate to severe (14-22mm) LVH patients revealed significant increases in LV mass (g) (343 ± 94 vs. 477 ± 110; p<0.001) and LV mass index (g/m2) (177 ± 41 vs. 243 ± 57; p<0.001). Patients with LVH demonstrated a higher IMP (0.50 ± 0.16 vs. 0.36 ± 0.05; p<0.001) than controls. Regression analysis revealed a correlation between increased LV mass (g) and IMP (R=0.59; p<0.001), and increased LVMI (g/m2) and IMP (R=0.56; p<0.001). This relationship was not explained by differences in the RR interval or age. Significant increases in the IMP were noted comparing normal, mild LVH, and moderate to severe LVH; (0.36 ± 0.05 vs. 0.46 ± 0.13 vs. 0.58 ± 0.18; p<0.005).CONCLUSIONS: The IMP is prolonged in patients with increased LVMI and normal LVEF. IMP may be useful to risk stratify such patients over extended time periods. Serial changes in IMP may help predict clinical outcomes, or provide support for more aggressive therapy to stabilize or reverse increased LV mass.
Journal of the American Society of EchocardiographyVolume 19 Number 5 Abstracts 625

P3-27
Vector Velocity Ultrasound Imaging of Radial and Rotational Motion Within Layers of the Left Ventricle
Petra S Niemann1, Helene Houle2, John Jackson2, Muhammad Ashraf1, Ling Hui1,Edward Hickey1, Xiao Kui Li1, David J Sahn1
1Oregon Health & Science University, Portland, OR;2Siemens Medical Solutions, Mountain View, CA
Background: The architecture of the left ventricle (LV) has been described as containing a myocardial band with a circumferential transverse band and oblique apical loop. Vector velocity imaging (VVI) is a new method for evaluating rotational velocity at different endocardial and myocardial layers of the LV. We studied LV mechanics in an open-chest pig model using VVI.Methods: Six anesthetized piglets (3-6.5 kg) were studied with an Acuson Sequoia ultrasound system and a 15L8 probe (14 MHz). Imaging was performed at transverse basal and oblique apical views. Heart rate was 60-80 bpm at baseline; RV/LV pacing was performed at 130 bpm. Rotational velocity was computed offline in LV endocardial and myocardial layers using VVI v30 (Siemens) software.Results: Rotational velocity differed significantly between subendocardial and mid myocardial layers of the LV (m 13.5 0/sec ± 5.39 and m 8.5 0/sec ± 3.76, p< 0.03). Ventricular rotation started in the endocardium near the septum and propagated to the outer layers. Time to peak rotation is 207 ms ± 151 in the subendocardium and 172 ms ± 80 in the mid myocardium. Radial inward velocity was highest in the endocarium in normal hearts with a significant decrease towards the outer layer (m 0.576 cm/sec ± 0.193 to m 0.453 cm/sec ± 0.137, p<0.03).Conclusion: VVI demonstrated peak rotational and radial velocity differences in the regions of the LV as well as between subendocardial and myocardial layers of the left ventricle.
P3-28
Biplanar Echocardiographic Strain Imaging Documents Improvement in LV Function in Patients with Ventricular Assist Device
Molly Thangaroopan, Shemy Carasso, Shelley Zieroth, Vivek Rao, Diego Delgado, Samuel Siu, Harry Rakowski, Heather Ross University Health Network, Toronto, ON, Canada
Background Ventricular assist device (VAD) support is used in the treatment of refractory heart failure. Conventional echocardiographic assessment of systolic and diastolic function in this patient population is limited due to poor imaging windows and subjective measurement of ejection fraction in a decompressed and asynchronously contracting left ventricle (LV). The assessment of myocardial mechanics by bi-planar strain imaging (SI) may provide a quantitative approach to the evaluation and follow-up of LV function (LVF) in patients (pts) supported with a VAD. We compared LV mechanics using strain imaging in heart failure pts immediately prior to and during VAD mechanical support.Methods LV short and long axis images acquired from 2D echo were analyzed offline to measure circumferential and longitudinal strain and strain rate using velocity vector imaging to track the endocardial border. Baseline and post-VAD EF and mean LVDD (LV diastolic dimension) were compared.Results 8 pts with non-ischemic cardiomyopathy requiring VAD support were studied. Mean age was 34 years (range 24-51). Median time from implant was 28 days (range 9-559). LVDD was reduced post VAD (63±11mm to 51± 13mm). Strain improved in 5 pts. LVF improved from severe to mild-moderate dysfunction on average in this subgroup. Strain S and E (diastolic) showed a similar pattern of improvement in both systolic and diastolic function. In the remaining 3 patients strain and LVF did not improve (2 died, 1 transplanted).
Conclusions This pilot study demonstrates the utility of strain imaging in the objective assessment of LV function in pts with VAD. SI provides supplementary data to conventional EF measurement since it can be obtained from limited studies, is less load dependent and may be a useful technique to identify responders to VAD support. Further studies are needed to determine whether this technique can be applied clinically as a predictor of LV recovery
P3-29
Right Ventricular Systolic Function is Not the Sole Determinant of Tricuspid Annular Motion
Angel Lopez-Candales, Navin Rajagopalan, Neil Saxena, Beth Gulyasy, Kathy Edelman, Raveen Bazaz Cardiovascular Institute University of Pittsburgh Medical Center, Pittsburgh, PA
Background: Maximal tricuspid annular plane systolic excursion (TAPSE) correlates well with right ventricular (RV) function; however, little is known regarding the effect of left ventricular (LV) systolic function on TAPSE.
Methods: TAPSE was examined in 206 patients (105 males, mean age 56 ± 17 years) with regards to RV (RV fractional area change 45 ± 19%) and LV (56 ± 17%) systolic function.Results: The mean TAPSE value for the 206 patients studied was 1.97 ± 0.72 cm. As seen in Figure1, (A) although a good correlation is seen between TAPSE and RVFAC in patients with normal RV systolic function but a reduced LV systolic function (r = 0.59); (B) an even stronger correlation is seen (r = 0.79) when patients have normal biventricular systolic function. Relative differences with regards to TAPSE values and biventricular function were noted. First, the highest TAPSE was found when both RV and LV systolic function were normal (2.46 ± 0.50 cm). Second, patients with a reduced RV systolic function had lower TAPSE (1.28 ± 0.48 cm; p< 0.0001). Third, patients with normal RV function but a reduced LV systolic function had TAPSE (1.91 ± 0.54 cm; p< 0.0001) values that were intermediate between those patients with both normal RV and LV and patients with an abnormal RV systolic function. Fourth, patients with biventricular dysfunction had the lowest TAPSE (1.16 ± 0.41 cm; p< 0.0001). The overall patient distribution in each group with relation to their biventricular function and TAPSE values is shown in Figure 2.Conclusions: Based on this data, it is important to realize that TAPSE is not only determined by RV
systolic function but also appears to be dependent on LV systolic function. In our analysis, TAPSE values less than 2.0 cm are associated with some degree of either RV or LV dysfunction, while values greater than 2.0 cm suggest normal biventricular systolic function.
P3-30
The Additive Value of Radial Strain Imaing to Routine M-Mode for Determining Dyssynchrony in Patients Evaluated for Resynchronization Therapy
Masaki Tanabe, Matthew S Suffoletto, Kaoru Dohi, David Schwartzman, John Gorcsan, III University of Pittsburgh, Pittsburgh, PA
Background: Septal-to-posterior wall motion delay (SPWMD) by M-mode echocardiography is one of the major tools for dyssynchrony analysis. However, recent publications and clinical experience have shown that M-mode SPWMD may not provide a reliable or accurate reflection of left ventricular (LV) dyssynchrony.Methods: Accordingly, the aim was to test the hypothesis that radial strain assessed by the new technique of Dyssynchrony Imaging (DI) (Toshiba Corp.) can have an additive value to routine M-Mode in determining SPWMD before CRT. Twenty five patients with left bundle branch block were studied at the mid-LV short axis view by both routine gray scale M-mode imaging and by DI using angle-corrected radial strain which color-codes time-to-peak radial strain. SPWMD was calculated independently as the time difference in peak inward septal and posterior wall motion by M-mode or the time difference in peak strain by DI, respectively.Results: Difficulties with routine M-mode analysis included 28% of patients with multiple septal inward motions (Figure below) and 12% with extremely flattened septal movement which made determination of the peak inward motion ambiguous. DI strain imaging demonstrated SPWMD more clearly than M-mode in 92%. The relationship of SPWMD using M-mode peak inward motion and SPWMD by strain was weak (r=0.446, p=0.025). However, when the M-mode peak matching the peak strain was selected (usually first inward motion), the correlation in SPWMD improved (r=0.87, p<0.001).
Conclusions: SPWMD by routine M-mode was ambiguous in 40% of patients with dyssynchrony due to its inability to separate active from passive motion. DI radial strain significantly improved determination of SPWMD analysis. This new technique has potential for clinical applications.
Journal of the American Society of Echocardiography626 Abstracts May 2006

P3-31
Index of Myocardial Performance as a Potential Objective Intraaortic Balloon Pump Weaning Tool in Patients with Low Cardiac Output Following Percutaneous Coronary Interventions
Marcos Daccarett, Patrick Alexander, Mark Sierra, Isaac Grinberg, Shukri David Providence Heart Institute, Southfield, MI
Background: Intraaortic Balloon Pump (IABP) devices are widely used during percutaneous coronary interventions (PCI) in patients requiring hemodynamic support. Currently objective parameters do not exist to determine effective weaning or termination of IABP support in these patients. The Index of Myocardial Performance (IMP) is a Doppler based variable that effectively incorporates systolic and diastolic time intervals expressed in global LV performance. Normal IMP values range in 0.39±0.05, and 0.59±0.10 in severe chronic systolic dysfunction. We intend to validate the IMP index as an indicator of systolic performance in patients requiring IABP support following PCI, and its role as a weaning parameter.Methods: Prospectively, 35 consecutive patients requiring IABP support following PCI were included. Isovolumic contraction (ICT), relaxation (IVRT) and ejection intervals (ET) (IMP=(ICT+IVRT)/ET) were measured using 2D Echocardiographic Doppler examination. On and off IABP support measurements were taken at baseline and every 24 hours to a up to 3 days post implantation. Clinical and IABP variables were obtained in an observational fashion. Doppler variables were recorded and separately analyzed by a blinded reader.Results: The average age was 66±3 years, 18 patients received IAPB support for 48 hours (51%) and 7 patients completed 72 hours (20%). The IMP on and off IABP after 24 hours was 0.47±0.11 and 0.67±0.14 (p<0.005) [27.2±18% difference], after 48 hours 0.47±0.13 and 0.58±0.12 (p<0.05) [17±14% difference], and 0.54±0.14 and 0.6±0.19 (p>0.38) after 72 hours [8.65±15% difference].
Conclusions: IMP is a sensitive, objective and reproducible method to monitor changes in LV dysfunction in patients requiring IABP support following PCI. Differences in IMP were larger and statistically significant on and off IABP during the first 24 hours post implantation. IABP support extending more than 48 hours post implantation failed to demonstrate a statistically significant
improvement in IMP. IMP can be potentially used as an adjunctive variable along with clinical monitoring during IABP weaning decision, but larger trials are needed to establish cutoff IMP values.
P3-32
Comparison of Doppler Echocardiography, Serum B-Type Natriuretic Peptide, Chest X-Ray and Physical Exam for the Estimation of Left Heart Filling Pressure
Daniel M Spevack, James Bowers, Anita Banerjee, Ashok Talreja, Eric Altman, Mark A Friedman, Michelle Bloom, Sanjay Doddamani, Divya Malhotra, Garet M Gordon, Kavita Patel, Linda Haramati, Hugo Spindola-Franco, Mark Menegus, Mark Greenberg Montefiore Medical Center, Bronx, NY
Background: Measurement of left heart filling pressures is clinically important for the diagnosis of congestive heart failure, predicting prognosis and guiding therapy. Invasive measurement of left ventricular pressure or pulmonary capillary wedge pressure is impractical for routine use outside the critical care setting. Physical examination, chest radiography (CXR), measurement of serum B-type natriuretic peptide (BNP) and Doppler echocardiography (DE) can be used to estimate left heart filling pressure non-invasively. We studied the accuracy of these diagnostic tests for estimating left heart filling pressure.Methods: Fifty-one patients in sinus rhythm without mitral stenosis underwent DE, CXR and BNP measurement within two hours of diagnostic left heart catheterization. Left ventricular diastolic pressure occurring immediately prior to atrial contraction (EDPpreA) was measured with fluid filled catheters at end-expiration. Pulse wave Doppler measurements of the mitral inflow and early lateral mitral annular tissue velocity (Em) were acquired at end-expiration. DE classification of EDPpreA was considered elevated (above 16 mmHg) when pseudo-normal or restrictive inflow patterns were seen. Em below 8 cm/s was used to distinguish pseudo-normal from normal mitral inflow pattern. Pulmonary vascular redistribution on CXR was used to classify EDPpreA as elevated. EDPpreA was considered elevated if BNP was above 60 pg/ml. Interpreters of DE and CXR were blinded to EDPpreA.Results: EDPpreA was elevated in fourteen patients (17-28 mmHg). The sensitivity and specificity for the detection of elevated EDPpreA were 79% and 89% for DE, 46% and 74% for CXR and 40% and 57% for BNP respectively. None of the patients had rales on physical examination. LVEDP did not correlate with E:Em ratio, peak E velocity or E deceleration time. All but seven patients had normal left ventricular ejection fractions.Conclusion: DE is an accurate non-invasive method for estimation of left heart filling pressure. The diagnostic accuracy of DE compares favorably to other non-invasive techniques.
P3-33
Longitudinal RV Strain Determined by Speckle-Tracking is Strongly Correlated to Pulmonary Arterial Pressure and Resistance in Systemic Sclerosis
Ahmed A Hassan, Madelon C Vonk, Madelijn H Sander, Arie P van Dijk Radboud University Medical Center, Nijmegen, The Netherlands
Introduction: Pulmonary hypertension (PHT) is an important complication of systemic sclerosis (SSc). To confirm the presence of pulmonary hypertension, right heart catheterization (RHC) is oligatory. Only recently myocardial strain parameters can be derived noninvasively by tracking the speckle formations in gray-scale echocardiographic images. Myocardial strain (S) is a dimensionless index of change in myocardial length while strain rate (SR) is the time derivative of strain with unit of per second (1/s).Aim: to assess right ventricular (RV) free wall S and SR for the detection of PHT.Setting: tertiary referral centre for pulmonary hypertension and scleroderma.Methods: In scleroderma patients, who underwent RHC, the RV free wall was imaged in the 4-chamber view using second harmonic imaging using Vivid 7 (GE, Horten, Norway).In the EchoPAC PC software package, 2D Strain was used for image analysis in the basal, middle and apical segments of the RV free wall. Longitudinal maximum systolic strain SL, maximum systolic strain rate Sr-s, maximum early filling strain rate Sr-E, late filling strain rate Sr-A and transverse (radial) maximum systolic displacement DT-s were derived. All patients underwent RHC measuring pulmonary arterial (PA) pressures, cardiac output and pulmonary vascular resistance (PVR).Results: 22 scleroderma patients age 59 + 12 yr, 15 female, were investigated. PHT was present in 18 patients (mean PA pressure 34 ± 13 mmHg) and absent in 4 patients (mean PA pressure 16 ± 2 mmHg). Only SL middle (-19 ± 11 % resp. -29 ± 5,6 %) , Sr-s apical (-1.81+0.63resp. -1.21+ 1.72 /s, p = 0.004) and Sr-A middle ( -1.48 + 0.77 resp. -1.65 + 0.28 /s, p= 0,03) differed significantly between PHT+ and PHT- patients. SL of the middle segment showed the strongest correlation with the diastolic PA pressure (Spearman rho = 0,672, SEE = 7,3 mmHg, p = 0,001), mean PA pressure (rho = 0,627, SEE = 11,7 mmHg, p = 0,002) and PVR ( rho = 0,677, SEE = 352,2 dynes.sec.cm-5 p =0,003).Conclusion: SL of the middle segment of the RV free wall is strongly correlated with PA pressures and PVR and might be used for PA pressure estimation.
P3-34
Right Ventricular Mechanics with Worsening Pulmonary Artery Pressures
Angel Lopez-Candales, Beth Gulyasy, Raveen Bazaz Cardiovascular Institute University of Pittsburgh Medical Center, Pittsburgh, PA
Background: Right ventricular (RV) fractional area change and tricuspid annular plane systolic excursion (TAPSE) are well-recognized methods in the assessment of RV mechanics. However, what is considered a normal range and how these variables are affected in pulmonary hypertension is not well characterized.Objective: To examine standard echocardiographic parameters used to determine RV performance and define RV areas, RV fractional area change and TAPSE in patients with varying degrees of pulmonary artery systolic pressures (PASP).Methods: RV end-systolic (RVESA) and end-diastolic areas (RVEDA), left ventricular (LV) systolic function, PASP and TAPSE were prospectively collected in 121 patients classified into three groups. Group I included 42 patients (mean age 48 ± 18 years, 24 males) had a PASP of 26 ± 5 mmHg, Group II included 45 patients (mean age 62 ± 14 years, 22 males) had a PASP of 51 ± 11 mmHg, and Group III included 34 patients (mean age 53 ± 15 years, 9 males) had a PASP of 100 ± 19 mmHg.Results: Characterization of the studied population according to their PASP allowed us to describe normal as well as abnormal range values for RVESA, RVEDA, RV fractional area change, and TAPSE as listed in Table 1. Of these echocardiographic parameters values, RVESA and RVEDA appear to most useful in allowing a more accurate discrimination between Groups I and II.Conclusions: Noninvasive recognition of early RV echocardiographic abnormalities as a result of pulmonary hypertension has always been somewhat difficult and controversial. The results of this analysis not only define normal values for different echocardiographic parameters used to assess RV performance but also characterize changes in these parameters with pulmonary hypertension. Furthermore, it appears that early changes in RVESA and RVEDA are the most useful and discriminatory echocardiographic variables to detect RV abnormalities in patients with mild to moderate elevations in PASP during a routine standard echocardiographic examination.
RV Data with Increasing PASPp value p value p value p value
Variable between groups Variable between groups Variable between groups Variable between groupsGroup 1 RVESA Group 1 RVEDA Group 1 RVFAC Group 1 TAPSE9 ± 4 ___ 19 ± 5 ___ 53 ± 12 ___ 2.4 ± .5 ___Group 2 RVESA Group 2 RVEDA Group 2 RVFAC Group 2 TAPSE13 ± 7 0.001 24 ± 7 0.001 46 ± 15 0.03 2.2 ± .8 0.05Group 3 RVESA Group 3 RVEDA Group 3 RVFAC Group 3 TAPSE26 ± 6 0.0001 35 ± 6 0.0001 26 ± 6 0.0001 1.4 ± .5 0.0001
Journal of the American Society of EchocardiographyVolume 19 Number 5 Abstracts 627

P3-35
Attenuated Increase in Tei Index With Advanced Congestive Heart Failure: Utility of Shortened Mitral E Deceleration Time
Kunitsugu Takasaki1, Yutaka Otsuji1, Eiji Kuwahara1, Toshinori Yuasa1, Takeshi Uemura1, Kenichi Nakashiki1, Kayoko Kubota1, Koichi Toyonaga2, Souki Lee2,Chuwa Tei1
1Department of Cardiovascular, Respiratory and Metabolic Medicine, Graduate School of Medicine, Kagoshima University, Kagoshima City, Japan; 2Department of Cardiology, Kagoshima City Hospital, Kagoshima City, Japan
Background: Tei index enables prediction of patients’ prognosis, however, only mild to moderate increase in Tei index despite severe congestive heart failure (CHF) (pseudonormalization) is also reported. The purpose of this study is to test the hypothesis that combination of shortened mitral E deceleration time to mild to moderate increase in Tei index may allow better evaluation of the hemodynamics.Methods: In 52 patients with anterior acute myocardial infarction (AMI), Tei index, mitral E deceleration time (DcT), and E/A were measured by Doppler echocardiography and pulmonary capillary wedge pressure (PCWP) was measured by catheterization.
Results: 1) Tei index showed significant positive correlation with PCWP (r=0.59, p<0.0001). 2) In all 21 patients with no clear increase in Tei index of � 0.50, PCWP was < 18 mmHg. 3) In 4 patients with advanced increase in Tei index of � 0.70, PCWP was 14 - 25 (21 ± 4) mmHg. 4) In 25 patients with mild to moderate increase in Tei index of 0.50 - 0.70, PCWP ranged from 3 to 39 mmHg. 5) In these 25 patients with mild to moderate increase in Tei index, mitral E DcT was significantly shorter and E/A was greater in 8 patients with PCWP � 18 mmHg compared to the remaining 17 patients (E DcT: 115 ± 33 vs. 155 ± 39 ms, p<0.01; E/A: 1.6 ± 0.7 vs. 1.0 ± 0.4,
p<0.01). In these 25 patients, diagnosis of PCWP � 18 mmHg by mitral E DcT <150 ms and E/A >1 had the sensitivity, specificity, and accuracy of 88, 82, and 84 %, respectively.Conclusion: Shortened mitral E DcT with E/A > 1 enables differentiation of only mild to moderate increase in Tei index with and without advanced CHF.
P3-36
Acute Response to Cardiac Resynchronization Therapy in Patients with Segmental Paradoxical Systolic Expansion Assessed by Strain Imaging
Hidekazu Tanaka, Hiroya Kawai, Maki Furuki, Kazuhiro Tatsumi, Toshiya Kataoka, Tetsuari Onishi, Mitsuhiro Yokoyama Kobe University Graduate School of Medicine, Kobe, Japan
Background: Tissue Doppler imaging-derived indices of time to peak systolic myocardial velocity have been used to assess left ventricular dyssynchrony. However, it is difficult to evaluate the magnitude of left ventricular dyssynchrony in patients with segmental paradoxical systolic expansion. The aim of this study is to investigate the acute response to cardiac resynchronization therapy (CRT) in patients with segmental paradoxical systolic expansion.Methods: We studied 22 patients with chronic heart failure (mean age was 69±9 years, left ventricular ejection fraction was 31±7%, QRS duration was 175±23msec, and New York Heart Association functional class III or IV), who underwent successful CRT. Standard echocardiography was performed before and after 5 to 7 days of CRT, and peak systolic strain was obtained from tissue Doppler imaging at the anterior, lateral, posterior, inferior, anteroseptal and posteroseptal walls at the level of the middle and basal-left ventricle from the apical views. Patients were divided into 2 groups with or without segmental reversed peak systolic strain (becoming positive, paradoxical systolic expansion) (Figure). The percent decrease in left ventricular end-systolic volume and the increase in left ventricular ejection fraction after CRT were determined as a marker of the acute response to CRT.Results: Seven patients had segmental reversed peak systolic strain. Acute improvement in hemodynamics, left ventricular end-systolic volume and ejection fraction were demonstrated in all patients. The decrease in left ventricular end-systolic volume (19±9% vs 9±5%, P<0.001) and increase in ejection fraction (16±6% vs 5±3%, P<0.001) in patients with segmental reversed peak systolic strain were significantly larger compared with patients without segmental reversed peak systolic strain.
Conclusions: This study demonstrates much greater extent of improvement in left ventricular volume and ejection fraction caused by CRT in patients with segmental paradoxical systolic expansion. Assessment of segmental paradoxical systolic expansion
using strain imaging might be useful for the prediction of beneficial effects in CRT as well as myocardial velocity indices to measure the degree of left ventricular dyssynchrony.
P3-37
Left Ventricular Midwall Fractional Shortening is Depressed Even in Patients with Well-Controlled Hypertension Compared with Normal Subjects
Hyung-Kwan Kim, Su-Yeon Choi, Jin-Shik Park, Yong-Jin Kim, Dae-Won Sohn, Byung-Hee Oh, Young-Bae Park, Yun-Shik Choi Seoul National University Hospital, Seoul, Republic of Korea
OBJECTIVES:Left ventricular midwall fractional shortening(LVmFS) is decreased and considered to have a prognostic implication in patients with hypertension. According to prior studies, anti-hypertensive treatment improved LVmFS with both regression of LV hypertrophy(LVH) and normalization of LV geometry in patients with mild hypertension. However, there is a paucity of data on LVmFS improvement in patients with well-controlled HTN in a real-world clinical practice, especially using current echocardiographic second harmonic imaging technique. Therefore, we wished to investigate this issue with echocardiographic machine equipped with second harmonic imaging capability.METHODS:LVmFS was evaluated in 80 patients with well-controlled HTN (<130/90mmHg in blood pressure for at least 1 year)(56±8years, 44 men) and 80 age- and sex-matched normal controls(58±8years, 36 men). LVH was defined as LV mass index�131mg/m2 in men and �110mg/m2 in women. Patients with both normal LV geometry ont the basis of relative wall thickness and normal LV mass index were separately analyzed.RESULTS:There was no difference in heart rate, gender proportion, LV endocardial FS and LV ejection fraction between the two groups. Body mass index(BMI) was slightly higher in patients with HTN(24.8±2.5kg/m2) vs. controls(23.4±2.4kg/m2)(p<0.001). LVmFS was significantly depressed in patients with hypertension vs. controls(25.5±3.4% vs. 23.3±3.9%, p=0.006). In separate analysis with patients with both normal LV geometry and normal LV mass index, LVmFS was again depressed (25.5±3.4% vs. 23.1±3.6%, p=0.003). Correction for BMI cannot alter this statistical significance.CONCLUSIONS:In contrast to registry data, LVmFS is depressed in patients with well-controlled hypertension relative to normal controls in a real-world clinical practice. Furthermore, LVmFS decrement is not normalized even in well-controlled hypertensive patients with both normal LV geometry and normal LV mass index.Clinical and echocardiographic features Normal controls (n=80) Hypertensive patients (n=80) P value
Age 56.3 ± 7.9 58.4 ± 9.0 0.12Systolic BP (mmHg) 108 ± 9 127 ± 10 < 0.01Diastolic BP (mmHg) 68 ± 8 77 ± 10 < 0.01Heart rate (bpm) 66 ± 10 68 ± 10 0.27BMI (kg/m2) 23.4 ± 2.4 24.8 ± 2.5 < 0.001Interventricular septal thickness (mm) 7.5 ± 1.2 9.5 ± 2.1 < 0.001LV posterior wall thickness (mm) 7.7 ± 1.1 9.5 ± 2.1 < 0.001LVEF (%) 63 ± 6 61 ± 7 0.13LV endocardial fractional shortening (%) 39.2 ± 5.0 38.0 ± 5.5 0.13LV midwall fractional shortening (%) 25.5 ± 3.4 23.8 ± 3.9 0.006Antihypertensive drugsα blockers ... 2 (2.7%) ...β blockers ... 15 (20.3%) ...Non-dihydropyridine calcium channel blockers ... 2 (2.7%) ...Dihydropyridine calcium channel blockers ... 34 (45.9%) ...Angiotensin converting enzyme inhibitors or Angiotensin receptor blockers ... 32 (43.2%) ...Thiazide diuretics ... 26 (34.7%) ...Aldactone ... 1 (1.4%) ...
P3-38
Correlation of Myocardial Energy Expenditure with Diastolic Dysfunction in a Large Population of American Indians: The Strong Heart Study
Rakesh K Mishra, Vittorio Palmieri, Lyle G. Best, Elisa T. Lee, James M. Galloway, Richard B. Devereux Weill Medical College-Cornell University, New York, NY
Introduction Left ventricular (LV) pressure and volume overload result in increased myocardial workload and oxygen consumption. Whether myocardial workload varies independently with degrees of diastolic dysfunction is not known.Methods We investigated the association of echo parameters of diastole with myocardial energy expenditure (MEE in calories/beat), an echo-derived estimate of myocardial workload calculated as the product of LV mass, end-systolic stress and ejection time, in 1016 American Indian participants greater than 45 years of age in the Strong Heart Study.Results Age 59±10, 64% women, hypertension in 51% and diabetes in 36%. In univariable analyses, MEE had significant positive associations with age and isovolumic relaxation time (IVRT) and a significant negative association with ejection fraction (EF; all p<0.05). There were no significant associations between MEE and mitral E/A ratio or E-wave deceleration time (DT). After adjustment for covariates, MEE retained its significant associations with age, IVRT and EF. We then examined the relationship of MEE with the three diastolic patterns: normal (0.6<E/A<1.5), abnormal relaxation (E/A<0.6), restrictive filling (E/A>1.5) (Table). Participants with restrictive filling had significantly shorter IVRT and DT and lower EF. In a general linear model, after adjustment for age and EF, MEE was significantly higher with restrictive filling than with normal or abnormal relaxation.
Study population Normal (n=1019) Abnormal relaxation (n=94) Restrictive (n=10)Age (yrs) 59±10 58±10 68±10* 56±10†
IVRT (msec) 84±13 83±13 87±15* 77±14†
DT (msec) 192±44 190±41 217±60* 166±44†
EF (%) 60±7 60±6 59±10 48±15*†
MEE (cal/beat) 3.00±1.42 2.95±1.29 3.20±2.15 5.57±2.70*†
* p<0.05 compared to normal; †p<0.05 compared to abnormal relaxation.Conclusions This study, for the first time, demonstrates that diastolic parameters are associated with MEE in a large population-based sample of adults with high prevalences of diabetes and hypertension. These findings suggest that some of the deleterious effects of diastolic dysfunction may be mediated by increased MEE with a concomitant increase in myocardial oxygen consumption.
Journal of the American Society of Echocardiography628 Abstracts May 2006

P3-39
Role of Tissue Doppler Echocardiography for the Diagnosis of Heart Transplantation Rejection
Marcos V C Resende, Marcelo L. C. Vieira, Wilson Mathias, Jr., Fernando Bacal, Edimar A. Bocchi Heart Institute HC FMUSP, Sao Paulo, Brazil
Background- Endomyocardial biopsy (EMB) is the gold standard method for the diagnosis of cellular rejection (CR). Tissue Doppler imaging (TDI) is a recent technique capable of selectively measuring cardiac function. We tested the hypothesis that multiregional TDI could detect CR � 3A after heart transplantation (HT).Methods and Results- Fifty four HT patients (pts) underwent 129 EMB and a TDI echocardiographic study within 24 hours. We compared the HT group versus a normal control group (13 pts), and HT patients who presented CR 3A with those who do not . We measured TDI systolic (S), early diastolic (E), late diastolic (A) velocities and E/A ratio on left ventricular annulus (an), basal (bas) and medium (mid) segment of septal (SEP), lateral (LAT), inferior (INF), anterior (ANT) and mid segment of posterior wall of LV; and on right ventricular annulus. The EMitral and ELATan velocity ratio was also obtained. HT patients showed CR �3A in 39/129 (30.2%) EMB. The best isolated predictor for the CR diagnose was ALATan, with sensivity of 76,3% and specifity of 73,8% (p= 0.001). In multivariate analysis, ALATan (p= 0.001), ASEPan (p= 0.002), E/A ratio LATan (p= 0.006), EMitral/ ELATan (p= 0.014), SINFan ( p= 0.009) and ELATmed (p= 0.042) predicted CR �3A. We obtained a score with sensivity of 88.2% and specificity of 75.4% (p= 0.001).Conclusion- Multiregional model based on TDI velocities could become a potential method to detect CR � 3A and function abnormalities after HT.
P3-40
Relationship Between Global and Regional Left Ventricular Systolic and Diastolic Function in Patients with Coronary Artery Disease Assessed by Strain Rate Imaging
Hidekazu Tanaka, Hiroya Kawai, Maki Furuki, Kazuhiro Tatsumi, Toshiya Kataoka, Tetsuari Onishi, Mitsuhiro Yokoyama Kobe University Graduate School of Medicine, Kobe, Japan
Background: Global left ventricular early diastolic filling is associated with global left ventricular systolic function. However the relationship between regional myocardial systolic and diastolic function has not been well characterized and whether regional myocardial diastolic function is associated with global diastolic function remains unknown. The present study aimed to assess the relationship between regional myocardial systolic and diastolic function in patients with coronary artery disease (CAD) using strain rate (SR) imaging. We also evaluated the relationship between SR imaging findings of regional myocardial diastolic function and conventional pulsed Doppler parameters of global left ventricular filling dynamics.Methods: We studied 45 patients with CAD (angina pectoris in 25, and prior myocardial infarction in 20) without myocardial ischemia. We performed conventional echocardiography and segmental peak SR in systole (SSR) and early diastole (ESR) were obtained from tissue Doppler imaging at the anterior, lateral, posterior, inferior, anteroseptal and posteroseptal walls at the level of the apical, middle and basal-left ventricle from the apical views.Results: We measured SR values in 701 of 810 possible segments obtained from the 45 patients. A significant positive correlation was observed between SSR and ESR in the entire segments (R=0.55, P<0.0001). In addition, we determined participant SSR was derived by dividing the summed of the SSR values by the number of interpretable segments for each patient, and participant ESR was also determined for each patient. Significant positive correlations were observed between participant SSR and left ventricular ejection fraction (R=0.85, P<0.0001), and participant ESR and peak early diastolic transmitral flow velocities (R=0.68, P<0.0001).Conclusions: Regional myocardial contraction and relaxation were clinical relevance in patients with CAD. Furthermore, global left ventricular early diastolic filling was associated with the degree of regional myocardial relaxation as well as systolic function.
P3-41
Clinical, Serum Cardiac Troponin T and Echocardiographic Evaluation for Prediction of Late Doxorubicin Cardiotoxicity
Marcelo G Paiva1, Sérgio Pettrilli2, Fábio C Doin1, Valdir A Moisés1, Adriana Cordovil1, Cristiano V Machado1, Manuel A Gil1, Orlando Campos1, Jose L Andrade1
1UNIFESP, São Paulo, Brazil; 2GRAAC, São Paulo, Brazil
OBJECTIVE: To evaluate whether clinical signs or syntoms of congestive heart failure, serial assessment of cardiac function by low dose dobutamine stress echocardiography (LDSE) and serum cardiac troponin T (cTnT) can predict doxorubicin (DOXO) cardiotoxicity.METHODS: Twenty six consecutive patients with osteosarcoma enrolled in the Brazilian osteosarcoma treatment group study 2000, were studied with LDSE (up to 5µg/kg/min). It was assessed systolic (shortening fraction-SF and contractile reserve-DSF) and diastolic function (transmitral Doppler inflow diastolic parameters) before chemotherapy, at 160 mg/m2 DOXO and greater than 160mg/m2 DOXO. cTnT were also measured before and during DOXO infusions and a cut-off abnormal value was defined as blood levels above 0,01ng/ml. Cardiotoxicity was defined as SF less than 30% assessed by rest echocardiogram 1 to 6 months after chemotherapy. Group A comprised those without cardiotoxicity (17 patients, 11 male, 14,3 ± 4,7 years) and group B included patients with a SF < 30% (9 patients, 6 male, 15,4 ± 3 years).RESULTS: Patients were submitted to a mean of 3,4 LDSE studies and 32,5 serum cTnT measurement. Only one patient (group B) presented clinical manifestation of cardiotoxicity. Patients with elevated serum cTnT were more frequent in higher DOXO dose (> 160mg/m2) in both groups but no statistical difference was found between them (46,2% vs 87,5%; p=0,06). Systolic and diastolic parameters were not significantly different between the two groups before chemotherapy. Resting SF showed lower values in group B only after 160mg/m2 DOXO (27% ± 2 and 34,1% ± 2, p < 0,01). LDSE SF and DSF were significantly lower in group B as compared to group A at DOXO dose 160mg/m2 (SF 36,1% ± 3,4 and DSF 2,1 ± 2,3 versus SF 45,2% ± 4,9 and DSF 9,4 ± 3; p < 0,01) as well as at DOXO dose greater than 160mg/m2 (SF30,3% ± 3 and DSF 3,1 ± 1,9 vs. SF40,8% ± 5,9 and DSF 7,2 ± 4,2; p < 0,01).CONCLUSION: This study suggests that LDSE is more reliable than cTnT and clinical evaluation for predicting future subclinical cardiotoxicity, even at lower doxorubicin dose.
P3-42
The Case for Echocardiographic Assessment of Volume Overload Beyond B-Type Natriuretic Peptide Levels
Sukesh Burjonroppa1, Pavlos Papavasilou1, Daniel Lenihan2
1University of Texas Health Science Center, Houston, TX;2MD Anderson Cancer Center, Houston, TX
Background: B type-natriuretic peptide (BNP) has been shown to be of diagnostic and prognostic significance in patients with clinical evidence of volume overload (VOL) and left ventricular systolic dysfunction. Echocardiography (Echo) utilizing Doppler tissue imaging of the Mitral annulus (DTI) is a validated method to derive pulmonary capillary wedge pressure (PCWP) and has been shown to correlate with BNP levels making a case for a simple blood test to measure the wedge pressure. However, marked elevations of BNP have been noted without VOL. Thus, we hypothesized that elevated BNP levels may reflect non-specific neuro-humoral activation due to multiple co-morbidities rather than due to VOL confirmed clinically or with Echo-derived PCWP.Methods: Over a one-year period, all patients admitted with BNP levels greater than 1000 pg/ml were identified and the demographics, co-morbidities including the presence of sepsis and any clinical evidence of VOL were detailed. Echo parameters including the Mitral inflow, DTI, Left Ventricular Ejection Fraction (LVEF) and derived PCWP [(1.29 (E/E′) + 1.9], were obtained within 48 hours of BNP.Results: A total of 99 patients (61±14 years, 45 male/ 54 female) had a mean BNP (pg/ml) of 2727±1376 (SD). BNP values were higher if LVEF<40 (3001±1409, n=36, PCWP =19) versus LVEF>40 (2573±1354, n=60, PCWP=15). Univariate linear regression models for factors age, creatinine and hemoglobin and 2-D echocardiographic parameters including left atrial size and LV internal diastolic dimension along with Doppler parameters of left ventricular filling including E/A, E/E′ and PCWP, each independently explained very little variation of BNP values (maximum R2 = 0.03). There were 52 patients (53%) with sepsis, 47 had no evidence of VOL with mean BNP of 2797 ± 1311pg/ml (p=ns). Among these, 38 had DTI with a mean PCWP of 17mmHg and a LVEF>40. BNP values, although all elevated, were higher in VOL (3050±1521, n=28, PCWP of 18) versus No VOL (2572±1294, n=71, PCWP of 16) (p=ns).Conclusion: In patients admitted with cancer and multiple co-morbidities, markedly elevated BNP values do not correlate with non-invasive measurement of PCWP by Echo. Echo parameters and derived hemodynamics support clinical observations, and therefore therapeutic decisions may need to be guided more by them as opposed to BNP levels alone. Entities like sepsis and other inflammatory cytokines may be important in causing these non-specific elevations of BNP
�
Journal of the American Society of EchocardiographyVolume 19 Number 5 Abstracts 629

P3-43
Tissue Doppler Indices Detect Subclinical Cardiac Dysfunction in Sickle Cell Disease
Jai Nahar1, Yesoda Rao1, Inez Ernst1, Wynona Coles1, Jim Nichols1, Yukitaka Shizukuda1, Dotti Tripodi1, Craig Sable2, Mark Gladwin1, Vandana Sachdev1
1National Institutes of Health, National Heart, Lung and Blood Institute, Bethesda, MD;2Children‘s National Medical Center, Washington, DC
BACKGROUND: Cardiomegaly has been well-described in sickle cell disease (SCD) patients in relation to anemia, but ventricular dysfunction is uncommon. Pulmonary hypertension (PH) is seen in one-third of patients and is a strong predictor of mortality. Ventricular dysfunction has been proposed as a contributor to the PH and high morbidity and mortality. Conventional Tissue Doppler (TD) indices have been shown to be useful in the detection of abnormal systolic and diastolic ventricular function. Myocardial performance index (MPI) is a global index of combined systolic and diastolic function and can be measured from annular tissue Doppler data.METHODS: Thirty-five SCD patients (age 37±12) and 15 healthy volunteers (age 45±7) underwent a transthoracic echocardiogram with septal and lateral mitral annular TD measurements and tricuspid annular TD measurements. Peak E, A, and S velocities and MPI were measured from the TD data in a blinded manner.RESULTS: SCD patients had normal left ventricular systolic function with an ejection fraction of 61±6%. TD-derived peak S velocities were not significantly different between SCD patients and controls, but septal E/A ratio was higher in SCD patients (1.6 ± 0.5 SCD vs 1.3 ± 0.4 controls, p=0.02). MPI measurements from TD were significantly higher in SCD patients in the septal (0.5 ± 0.1 SCD vs 0.3 ± 0.04 controls, p<0.0001) and lateral mitral annulus (0.5 ± 0.1 SCD vs 0.4 ± 0.03 controls, p<0.0001).There was no significant difference in TD and TD-MPI parameters of the right ventricle in SCD patients vs. controls. In SCD patients with PH (tricuspid regurgitation jet velocity �3 m/s), TD-derived MPI index from the septal and lateral mitral annulus was similar compared with SCD patients without PH. However, tricuspid annular TDI-derived MPI was significantly higher (0.5 ± 0.1 TR�3 m/s vs 0.4 ± 0.1 TR<3, p<0.0001) suggesting subclinical RV dysfunction with higher pulmonary pressures.CONCLUSION: Tissue Doppler parameters suggest that SCD patients have subclinical left ventricular dysfunction when compared with healthy controls. In SCD patients with elevated pulmonary pressures, there is evidence of mild right ventricular dysfunction. Further studies of SCD patients with TD are necessary to distinguish systolic from diastolic dysfunction and to determine its clinical significance.
P3-44
Is Diasolic Heart Failure a Seperate Entity? Demonstration of a Strong Interrelationsship between Systolic and Diastolic Myocardial Function
Mohsen Gaballa, Sr.1, Lars-Ake Brodin, Sr.2, Jan Van der Linden, Sr.2, Ken O`Rielly, Sr.3, Lars Brudin, Sr.1
1Kalmar Hospital, Kalmar, Sweden; 2Karolinska Hospital, Stockholm, Sweden; 3Royal Alexandra Hospital, Edmonton, AB, Canada
Objectives: Isolated diastolic heart failure (i.e. clinical heart failure with preserved or normal ejection fraction (EF) has emerged over the last decade as a separate entity, having claimed to account for about 30% of patients with heart failure. On the contrary we believe that the systolic and diastolic myocardial function are coupled and inseparably linked with each other. Methods: A total of 2000 patients, either cardiovascular normal or with a background of hypertensive, ischemic or valvular heart failure were screened by conventional echocardiography and tissue Doppler examinations to assess the relationship between systolic and diastolic function. Multiple regression analysis was used to investigate the correlation between EF, systolic velocity S‘, early and late diastolic velocity E’ and A’ respectively to assess if either sysolic contraction or diastolic relaxation can function independently of each other. Left ventricular filling pressure was estimated by the E/E’-ratio, where E is Doppler E wave of the mitral valve and E’ the velocity of tissue doppler. A value more than >15 were considered abnormal.Results: There was a significant negative correlation between S’ and E/E‘ in patients with normal EF as well as in patients with restrictive filling of the left ventricle (Fig 1). A highly significant positive correlation was also found between S’ and E’ in patient with abnormal left ventricular relaxation and or increased filling pressure.Conclusion: Systolic and diastolic left ventricular function are coupled and inseparably linked processes. The concept that isolated diastolic failure do exist might be due to the fact that EF, though being a robust method, is not a quite sensitive technique to detect discrete changes in systolic myocardial function.
P3-45
Clinical Importance of Gender and Age Related Global Longitudinal Diastolic Function in Normal Population Quantified by Two-Dimensional Novel Speckle-Tracking Strain Rate Imaging
Kaoru Dohi, Katsuya Onishi, Yuko Sakurai, Takashi Tanigawa, Tetsuya Kitamura, Masaaki Ito, Naoki Isaka, Takeshi Nakano Mie University School of Medicine, Tsu, Japan
Background: Quantification of left ventricular (LV) diastolic function is clinically important. Longitudinal dynamics had been recognized as one of the major contributions for diastolic function. Two-dimensional novel speckle-tracking strain rate imaging is a new and promising technique to quantify global LV function. We hypothesized that speckle-tracking strain rate imaging can identify possible age- and gender-related differences in longitudinal diastolic function in normal population.Methods: Sixty subjects (30 female and 30 male, age of 14-87, 49±18 year old) who had normal finding by routine clinical echocardiographic evaluations and no medical history of hypertension, diabetes mellitus, or hyperlipidemia were recruited to the present study. Speckle tracking applied to routine apical 4-, 2-, long axis, and mid-ventricular short axis images calculated longitudinal and circumferential global strain rate from multiple points averaged to 6 standard segments (EchoPACK; GE Medical Systems).Results: All patients had normal ejection fraction (57-70%, mean 65±4%). Longitudinal global early diastolic strain rate averaged from apical 4-, 2-, and long axis images negatively correlated to age and the slope of the linear regression was much steeper in female than those in male (y=0.019x+2.5, r=0.83 in female and y=0.012x+1.7, r=0.73 in male, respectively). Circumferential global early diastolic strain rate had no relationship to age.Conclusion: Two-dimensional novel speckle-tracking strain rate imaging identified age-related decline of longitudinal diastolic function and its gender-difference in normal population.
P3-46
Usefulness of Tissue Doppler Imaging for Detection of Subclinical Left Ventricular Dysfunction in Hemodialysis Patients
Atsuko Muranaka, Satoshi Yuda, Hitomi Yamamoto, Sakiko Fujii, Jyunichi Kaide, Akiyoshi Hashimoto, Tomoaki Nakata, Kazufumi Tsuchihashi, Nobuyuki Ura, Hiroshi Natori, Kazuaki Shimamoto Sapporo Medical University School of Medicine, Sapporo, Japan
Background: In hemodialysis (HD) patients, cardiovascular disease is the common complication and subclinical left ventricular (LV) dysfunction may occur even in normal global systolic function. Our purpose was to evaluate myocardial function in HD patients with preserved systolic function using tissue Doppler imaging (TDI) and identify the determinants of myocardial function in HD patients.Methods: Forty HD patients (23 men, 56±12 years) and 30 age-matched controls (19 men, 53±11 years) underwent conventional echocardiography and TDI. HD patients underwent echocardiographic examinations after HD. Normal LV filling (N) pattern was defined according to Canadian consensus guideline using transmitral and pulmonary venous Doppler echocardiographic parameters. Mitral annulus velocity was obtained from each of 4 mitral annulus (inferior, anterior, septum and lateral) sites in the apical views. Mean peak systolic velocities (Sm) and mean early diastolic velocities (Em) were calculated by averaging at each site. Patients with history of coronary artery diseases and systolic dysfunction (ejection fraction (EF) <50%) were excluded.Results: Significant differences in systolic blood pressure, LV mass index, E/A ratio, and deceleration time of E (DcT) were found between the two groups, although EF was similar. Both Sm and Em in HD patients were significantly lower than those in controls (Table). N pattern was present in 17 controls and in 9 HD patients. Em in HD patients with N pattern was also significantly lower than that in controls with N pattern (8.8±2.0 vs. 11.0±2.5 cm/s, p<0.05). Both Sm and Em significantly correlated with age and LV mass index, but not duration of HD, intact PTH level, calcium phosphate product. In addition to age (P=0.007) for Em, LV mass index was the independent determinant of both Sm (P=0.01) and Em (P=0.03) in HD patients.Conclusions: In HD patients, TDI can detect the systolic and diastolic myocardial dysfunctions, which can not be detected by conventional echocardiography. These myocardial dysfunctions associate with LV hypertrophy and scarcely associate with HD and calcium-phosphate metabolism.
Comparison of echocardiorpahic parameters between HD patints and controlsHD patients Controls P value
(n=40) (n=30) Systolic BP (mmHg) 132±23 120±16 <0.05EF (%) 66±8 67±7 NSLV mass index (g/m2) 142±45 106±29 <0.001E/A ratio 0.9±0.3 1.1±0.4 <0.001DcT (ms) 244±55 204±47 <0.05Sm (cm/s) 8.2±2.9 9.0±1.8 <0.05Em (cm/s) 7.9±2.1 9.8±2.4 <0.001
Journal of the American Society of Echocardiography630 Abstracts May 2006

P3-47
Echocardiografical Analysis of the Systolic Function of Patients Submitted to Autologous Bone Marrow Mononuclear Cells Transplantation After Acute Myocardial Infarction
Fernanda B S Nogueira, Julio Cesar Tolentino, Luciano J Belem, Arnaldo Rabischoffsky, Antonio Carlos S Nogueira, Marcelo I Garcia, Jaqueline Leite, Christine Rutherford, Suzana A Silva, Andrea Haddad, Hans Fernando R Dohmann Hospital Pró-Cardíaco, Rio de Janeiro, Brazil
Background: Acute myocardial infarction (AMI) is a major cause of heart failure. Some trials have shown that Autologous Bone Marrow Mononuclear Cells Transplantation (ABMMNCT) has reduced AMI area. The main objective of this trial is to analyze systolic function of patients before and after ABMMNCT.Methods: Randomized, controlled trial with a 3 month follow-up of 23 pts after AMI who had undergone successful percutaneous angioplasty. Echocardiography analysis was done independently. Pts must have basal depressed myocardial contractility measured by echo and myocardial cintilography. Randomization was made at the third day after infarction. Vivid 7 was used to perform echo exams, which were done on both treated (TG) and control group (CG). The following parameters were measured: end-diastolic diameter (EDD), end-systolic diameter (ESD), end-diastolic volume (EDV), end-systolic volume (ESV), ejection fraction by Simpson (EF), wall motion index score (WMIS). Statiscal analysis was performed by using ANOVA.Results: The mean age at CG was 58,8±11y and TG was 58,7±11y (p=NS). EDD has moved from 53,45 ± 3,5 mm to 55,6±6,6mm in GC and from 51,6±5,8mm to 50,5±4,9mm in TG (p=NS); ESD has altered from 34,7±4,1mm to 38,4±7,2mm in CG and from 36,8±6,3mm to 33,8±5,3mm in TG (p=NS). In the CG, EF has changed from 55,7±8,7% to 54,3±8,3% while in TG it ranged from 49,1±4,4% to 57,6±8,3% (p=0,08). EDV has moved from 111,8±27,9ml to 103,5±13,5ml in CG and in TG from 85,4±21,1ml to 82,6±17,4ml (p=0,06). There was an alteration in ESV in CG, varying from 49,8±17,1ml to 47,6±12,2ml and in TG varying from 43,5±11,9ml to 34,7±8,5ml(p=NS). Relating to WMIS, in CG it ranged from 1,48±0,27 to 1,49±0,31 and in TG from 1,73±0,25 to 1,44±0,30(p=0,07).Conclusion: These preliminary data have shown a trend of improvement in the treated group in relation to control group. A greater number of patients will be necessary to confirm this statistical trend.
P3-48
Rapid Screening of Left Ventricular Systolic Dysfunction in a Pacemaker Clinic Using a Hand-Carried Ultrasound Device
James N Kirkpatrick, Syed N. Ghani, Kirk T. Spencer, Gwendolyn L. Smith, Martin C. Burke, Susan S. Kim, Aseem D. Desai, Bradley P. Knight University of Chicago, Chicago, IL
Background: Pacemaker recipients with left ventricular (LV) dysfunction are potential candidates for aggressive medical treatment and for an upgrade of the device to an implantable defibrillator or cardiac resynchronization pacing device. The purpose of this study was to determine if a portable hand-carried ultrasound device (HCU) could be used as a rapid, inexpensive method to identify patients with LV dysfunction in a busy pacemaker clinic.Methods: 80 consecutive patients undergoing routine pacemaker follow up were enrolled. Each patient underwent HCU in the sitting position during device interrogation, by a general internist who had 20 hours of didactic training and had performed 20 practice examinations. LV dysfunction was defined as an ejection fraction (EF) < 40%. Each patient also underwent a formal echocardiogram limited to assessment of EF by a sonographer using a full feature platform.Results: The mean age was 75±13 years and 53% were female. 71% had no known coronary artery disease and 82% were NYHA functional class I or II. Half of the subjects had a history of atrial fibrillation. HCU images were interpretable in 91% (73/80) and required 3.7±0.9 minutes to complete. Based on the full feature echo, the prevalence of LV dysfunction was 16/73 (22%); 25% of these patients were NYHA class I. HCU exam sensitivity for detecting LV dysfunction was 75%, specificity 91%, negative predictive value 93%, positive predictive value 71%, and accuracy 88%. One subject with a recent pacemaker implant had a large pericardial effusion diagnosed by HCU and underwent pericardiocentesis.Conclusions: HCU can be used in a pacemaker clinic by a non-cardiologist to rapidly and accurately identify pacemaker recipients with LV dysfunction who might be candidates for intensive medical therapy or a device upgrade.
P3-49
Starling Law and Left Atrium: Real Time Three Dimensional Echocardiographic Study
Ashraf M A Anwar, Osama I I Soliman, Marcel L Geleijnse, Folkert J ten Cate Thoraxcenter Erasmus mc, Rotterdam, The Netherlands
Background The relation between left ventricular volume and function is characterized by the Starling law. Little is known about the relation between left atrial volume (LAV) and function.Aim To study the relation between left atrial volume (LAV) and function.Methods Fifty consecutive stable patients in sinus rhythm were included (mean age 45.6 ± 9.3 years, 65% males). LAVs were calculated at end-systole (ES), end-diastole (ED) and pre-atrial (pre A) contraction with real time three-dimensional echocardiography using sonos 7500 philips echo machine and Q lab soft ware system for analysis.The active atrial emptying fraction (AAEF) was selected as a marker for active atrial function and calculated as (pre-A LAV - ED LAV) / pre-A LAV x 100. Depending on the ES LAV, patients were classified into three groups (G): G I included 22 patients with ES LAV <50 ml, G II included 11 patients with ES LAV 50-70 ml and G III included 17 patients with ES LAV >70 ml.Results As seen in the Table, AAEF significantly increased from G I to G II (30.5 ± 20.0% vs. 48.4 ± 18.6%, P = 0.02) but decreased from G II to G III (48.4 ± 18.6% vs. 26.5 ± 18.6%, P = 0.02).
Group I G II G III (ES LAV <50 ml) (ES LAV 50-70 ml) (ES LAV >70 ml)ES LAV 32.2 ± 11.9 67.4 ± 28.0 90.7 ± 23.0Pre-A LAV 23.0 ± 8.5 43.3 ± 12.4 62.0 ± 15.0AA EF (%) 30.5 ± 20.0 48.4 ± 18.6 26.5 ± 18.6
Conclusion It is concluded that larger ES LAV results in a better AAEF until a certain limit at which the relation between ES LAV and AAEF becomes inverse. This relation could be expressed in curve very similar to Starling curve described for the left ventricle and explain the clinical states where left atrial dilatation occurred on expense of its active function.
P3-50
Mitral Annular Velocities Differentiate Upper Septal Hypertrophy Due to Hypertension from Hypertrophic Obstructive Cardiomyopathy
Annabel A Chen, Michael A. Fifer, Michael H. Picard, Judy W. Hung Massachusetts General Hospital, Boston, MA
Background: Discrete upper septal hypertrophy (USH) without LVOT obstruction is often associated with older age and hypertension (HTN). It is unclear whether USH represents abnormal remodeling related to pressure load or is a subclinical manifestation of hypertrophic obstructive cardiomyopathy (HOCM). Tissue Doppler imaging (TDI) measures myocardial function and may differentiate USH from HOCM. We aimed to compare TDI patterns in patients with USH and HOCM.Methods: Clinical history and echos were analyzed for age- and sex-matched groups of normals, USH and HOCM. Patients with abnormal LVEF or atrial fibrillation were excluded. The normal group had no history of HTN and had structurally normal hearts. The USH group had normal echos except for USH, a focal area of IVS thickness � 13 mm and maximal IVS/posterior wall thickness � 1.4. The HOCM group had� 1 symptom (dyspnea, angina, or syncope) and echo with maximal IVS of � 15 mm, systolic anterior motion of the mitral valve and� mild mitral regurgitation, and a resting or provoked outflow tract gradient � 30 mm Hg. LVEF was calculated by biplane Simpson’s method.Results: Clinical and echo characteristics are presented in the Table as mean±SD. The resting outflow tract gradient in HOCM patients was 67±41 mm Hg. Compared to normals, USH patients had significantly lower lateral E′ (p = 0.01) and septal E′ (p = 0.02) and higher E/ lateral E′ (p = 0.02). Compared to HOCM patients, USH patients had significantly higher septal E′ (p = 0.01), A′ (p < 0.001) and S′ (p = 0.02) and lower E/lateral E′ (p = 0.003).Conclusions: Annular Doppler velocities can differentiate the septal hypertrophy of USH from HOCM. The abnormal annular velocities in USH patients suggest that further investigation is indicated to elucidate its clinical significance. Normal (13) USH (19) HOCM (13) p valueAge (yrs) 64±9 66±8 65±9 0.63% Women 62 58 46 0.71Body-surface area (m2) 1.8±0.3 1.9±0.2 1.9±0.2 0.56Heart rate 71±11 67±15 67±12 0.67Maximum IVS thickness (mm) 8.8±0.9 16.7±2.6 18.7±2.6 <0.001Posterior wall thickness (mm) 8.8±0.7 9.3±1.4 11.7±2.0 <0.001Left atrial volume index (ml/m2) 19±8 28±10 36±13 <0.001Left ventricular ejection fraction (%) 64±7 65±9 69±7 0.14E/A 1.0±0.3 0.9±0.4 1.1±0.5 0.58Lateral E’ (cm/s) 9.8±2.0 7.8±2.4 6.3±2.3 0.001Lateral A’ (cm/s) 11.0±2.6 11.0±3.0 8.8±3.0 0.09Lateral S’ (cm/s) 8.5±1.6 7.7±1.9 6.6±2.4 0.05E/lateral E’ 6.5±1.4 8.8±3.5 15.8±6.7 <0.001Septal E’ (cm/s) 8.1±2.6 5.9±1.3 4.6±1.2 0.001Septal A’ (cm/s) 10.6±2.7 10.3±2.1 7.5±1.8 0.002Septal S’ (cm/s) 7.7±1.6 7.0±1.4 5.7±1.3 0.006
Journal of the American Society of EchocardiographyVolume 19 Number 5 Abstracts 631

P3-51
Post-Systolic Peak Velocities Affect the Predictive Value of Dyssynchrony Analysis for Cardiac Resynchronization Therapy
Masaki Tanabe1, Maxime Cannesson1, Matthew S Suffoletto1, Randy Martin2, Angel Leon2, Samir Saba1, John Merlino2, John Gorcsan, III1
1University of Pittsburgh, Pittsburgh, PA;2Emory University, Atlanta, GA
Background: Dyssynchrony analysis by tissue Doppler has not been standardized; some investigators include post-systolic peak velocities and others limit analysis to left ventricular (LV) ejection. The impact of these different approaches to predict response to cardiac resynchronization therapy (CRT) is not known.Methods: To test the hypothesis that inclusion of post-systolic velocities affects the predictive value of dyssynchrony analysis, 86 patients (pts) undergoing CRT were studied. Mean age was 65±11, ejection fraction 25±8, QRS duration 164±31; 55 had ischemic and 31 had non-ischemic cardiomyopathy. Color-coded longitudinal velocity (GE Corp) was recorded in 4-chamber, 2-chamber, and apical long-axis views at basal and mid levels for each view (12-sites). Dyssynchrony analyses of time to peak velocities were approached 2 ways: 1) including post-systolic peaks after aortic valve closure and 2) limited to LV ejection. An opposing wall delay cut-off of >65ms (maximum per view) was used to define significant dyssynchrony.Results: Sixty-nine pts (80%) were CRT responders, defined as >15% increase in EF at 6±4 months, and 17 pts (20%) were non-responders. Forty-two pts (49%) had post-systolic peak velocities (35 responders, 7 non-responders). Dyssynchrony analysis including post-systolic velocities predicted EF response to CRT with high sensitivity (93%) but moderate specificity (59%). When analysis was limited to LV ejection, 10 pts (12%) were reclassified as having no dyssynchrony; 4 were non-responders (all ischemic cardiomyopathy) but 6 were responders (5 non-ischemic and 1 ischemic cardiomyopathy). When dyssynchrony analysis was limited to LV ejection, an opposing wall delay >65ms predicted response to CRT with 84% sensitivity and 82% specificity.
Conclusions: Dyssynchrony analysis including post-systolic peak velocities has superior sensitivity, but inferior specificity to predict response to CRT, compared with dyssynchrony analysis limited to LV ejection. These important findings may impact patient selection for CRT.
P3-52
Another Pathognomonic Sign in Arrhythmogenic Right Ventricular Dysplasia Visualized by Pulsed Wave Doppler in Septal Cusp of Tricuspid Valve
Ivana I Vranic Institute for Cardiovascular Diseases Clinical Center of Serbia, Belgrade, Serbia and Montenegro
Purpose: Recently „V sign“ was described on 2D echo confirming previously recognized apoptotic process mostly localized in the crista supraventricularis in ARVD patients. As intact crista supraventricularis is indispensable for normal function of tricuspid valve we wanted to examine its motion among affected patients.Methods: Study population consisted of 72 patients, age between 22 and 72, gender 38 male (52.78%) and 36 female (47.22%) fulfilling the WHF criteria for a positive diagnosis of ARVD. This series was compared to a control group including 150 individuals studied for routine physical examination, patients age between 18 and 65, gender 83 male (53.33%), 67 female (46.67%). 2D echo was performed in each patient in apical four chamber view and technique of pulsed Doppler tissue imaging was used. The pulsed wave Doppler sample volume (size 4) was placed on the right ventricular side at the basal part of septal cusp and special attention was paid to aligning the Doppler beam to the interventricular septum to optimize measurements which were obtained during end expiration. In a parallel direction we recorded transtricuspid flow profile and values of all echocardiographic parameters were averaged over five cardiac cycles to avoid respiratory changes. A Chi square test was performed and a value of p<0.05 was considered statistically significant.Results: Clinical results showed a previously unrecognized irregular pattern of septal cusp behavior in tricuspid valve motion during diastole in ARVD patients as compared to controls (p<0.05). This irregular pattern showed rhythmical changes over cycle of five consecutive beats during which an E wave in transtricuspid flow was flattened at least only once or twice as opposed to controls (p<0.05).Conclusion: Tricuspid valve is first affected nearby structure capable of supporting enough information that might point to ARVD diagnosis. These findings also encourage the significance of V sign in ARVD patients.
P3-53
Quantitative Echocardiographic Determination of Left Ventricular Recovery on Mechanical Circulatory Support
Karim Sallam, Donald Severyn, Robert L. Kormos, Dennis M McNamara, John Gorcsan, III University of Pittsburgh, Pittsburgh, PA
Background: The left ventricular (LV) assist device (AD) is lifesaving to patients with end-stage heart failure as a bridge to transplant. However, an important subset of patients can have LV recovery on LVAD and can be weaned to device explantation, but means to identify LV recovery on LVAD is clinically challenging.Methods: To test the hypothesis that patterns of LV function on LVAD support may be predictive of LV recovery, 30 patients, aged 45±19yrs on chronic LVAD support 234± 169 days were studied. Mid-LV short-axis echo views were recorded on-line using automated border detection to determine beat to beat changes. Stroke area (end-diastolic area - end-systolic area) and fractional area change (Stroke area/end-diastolic area) were calculated on full LVAD support and then during weaning trials of partial to no LVAD support.Results: Overall, LV recovery was identified in 10 patients who had successful LVAD removal, 20 remained LVAD dependent. On full LVAD flow, the average stroke area was higher in the LV recovery group than the LVAD dependent group: 8.0± 1.8cm2 vs. 6.1± 2.6cm2, respectively, p< 0.05. The fractional area change was also higher in the LV recovery group than the LVAD dependent group: 59±13% vs. 39±17%, respectively p< 0.005. A fractional area change cut off of 46% on full LVAD support predicted LV recovery with 89% sensitivity and 71% specificity. All but one patient with fractional area change >46% on full LVAD support had LV recovery, and all with fractional area change >38% on full LVAD support had LV recovery. During weaning trials of partial LVAD support, fractional area change was significantly higher in the LV recovery group than the LVAD dependent group: 52±13 vs. 24±9%, respectively p< 0.005. A fractional area change cut off of 34% improved the ability to predict LV recovery with 100% sensitivity and 89% specificity.Conclusions: Quantitative echocardiographic assessment of LV function on full LVAD support has promise as a screening method for LV recovery, but weaning trials are needed for optimal sensivitivity and specificity for determining LV recovery.
P3-54
Incidence of Systolic Asynchrony in LV Dysfunction, Aortic Regurgitation, and Diastolic Dysfunction: Prediction of Asynchrony by Isovolumic Contraction Time
Steven J Lavine University of Florida/Jacksonville, Jacksonville, FL
Background: Resynchronization therapy has used the QRS duration for patient selection with 20-30% failing to respond. Criteria for systolic asynchrony (Asyn) employing tissue Doppler have been proposed. However, Asyn has been noted in other cardiac diseases, but its incidence has not been assessed. As diastolic asynchrony was related to prolonged relaxation, we hypothesized that a prolonged isovolumic contraction time (ICT) may be associated with Asyn.Methods: We evaluated 2D, tissue and spectral Doppler in 152 patients: 47 with LV dysfunction (LVD), 31 with aortic regurgitation (AR), 33 normals, and 41 with diastolic dysfunction (Ddys). We employed 4 measures of Asyn: (1) Standard deviation of the R wave to peak systolic wall velocity interval of the proximal and mid segments from 3 apical views (asynSD), (2) Maximal difference (maxD) in timing among walls, (3) Septal to lateral and (4) Anteroseptal to posterior wall timing differences. The incidence of abnormal Asyn in each group as defined by a septal to lateral or anteroseptal to posterior timing difference >60 ms, maxD >100 ms, and SDasyn > 33 ms was assessed.Results: Comparable LV dilatation was noted in AR and LVD patients as compared to normals and Ddys patients (p< 0.05). LVD patients had a reduced ejection fraction (33+12%) as compared to the other groups: 63-66%, p<0.001. AsynSD was increased in AR (61+27 ms), Ddys (44+16 ms), and LVD (93+38 ms) as compared to normals (23+10 ms, all p<0.01). MaxD was prolonged in AR (204+99ms), LVD (291+146 ms), and Ddys (127+33 ms) patients as compared to normals (69+24 ms, all p<0.01). Abnormal Asyn as measured by any of the above indexes was present in 5 normals, 26 Ddys patients, 38 LVD patients, and 24 AR patients (all p<0.01 vs normal). For all patients with Asyn, a SDasyn >33 ms was present in all normals, 23/26 with Ddys, 36/38 with LVD, and 21/24 with AR. Both SDasyn and maxD were significantly correlated with ICT (r=0.63 and 0.71, p<0.001). Forward stepwise multiple regression revealed that end systolic volume (p=0.006), ICT (p=0.0009), and the QRS duration (p=0.0088) were independent predictors of SDasyn (r=0.792 p<0.0001). End systolic volume (p<0.0001) and ICT (p<0.0001) were independent predictors of maxD (r=0.8064, p<0.0001). End systolic volume and ICT were significant predictors of SDasyn and maxD for each subgroup.Conclusion: There is a substantial incidence of Asyn in AR and Ddys patients comparable to LVD patients. SDasyn is related to ICT in patients with and without LV dilatation or dysfunction and adds additional independent predictive value for identifying patients with Asyn.
Journal of the American Society of Echocardiography632 Abstracts May 2006

P3-55
Ultrasonic Tissue Characterization in Doxorrubicin Induced Myocardiopathy: An Animal Model Study
Minna M D Romano, João L O‘Connell, Antonio Pazin-Filho, Marcus V Simões, Benedito C Maciel Medical School of Ribeirão Preto, Ribeirão Preto, Brazil
In the clinical setting, the early detection of myocardial injury induced by doxorubicin (DXR) remains a challenge. To evaluate whether or not ultrasonic tissue characterization, as evaluated by integrated backscatter (IBS), could early identify DXR myocardial injury, we studied Wistar rats using two different intraperithoneal infusion drug protocols: a short term (group I: N=10) infusion of 15 mg/Kg during 2 weeks, and a long term (group II: N=11) infusion 18 mg/Kg through 9 weeks; a control group (III) included 17 rats. The quantification of IBS was performed by an acoustic densitometry software package incorporated in a commercially available ultrasound system. IBS images were obtained in parasternal short axis (papillary muscle level) view and analyzed in posterior left ventricle (LV) segment. The following IBS variables were evaluated: 1) the corrected coefficient (CC) of IBS, obtained by dividing IBS intensity by IBS intensity measured in a rubber phantom, using the same equipment adjustments, at the same depth; 2) magnitude of cardiac cyclic variation (MCV) of IBS, as measured by the peak-to-peak difference between maximal and minimal values of IBS in cardiac cycle. LV ejection fraction (EF) was also measured. Results: EF was significantly lower (p < 0.001) in group II (66±6%) than in I (83±6%) and control (84±5%) groups. MCV was significantly (p< 0.05) lower in group II (7.5±1.5) than in groups I (11.9±3.3) and control (9.7±3.6), while the CC was larger (p <0.0001) in group II (1.81±0.45) comparing to groups I (1.05±0.24) and control (1.12±0.27). There was a good correlation (r = -0.74, p<0.0001) between EF and CC. In conclusion: 1) a slight but significant reduction of EF was observed only after high dose infusion; 2) The CC of IBS and MCV were able to early differentiate cardiac injury due to DXR in the high dose infusion protocol ; 3) the increasing of the CC of IBS with worsening of LV EF suggests a relationship between the acoustic properties of myocardial tissue and grading of myocardial injury even considering the minor degree of LV systolic disfunction induced by DXR in this study.
P3-56
Phenotypic Spectrum and Clinical Characteristics of Apical Hypertrophic Cardiomyopathy (Multicenter Study)
Eui-Young Choi1, Jong-Won Ha1, Se-Joong Rim1, Yong-Jin Kim2, Duk-Hyun Kang3,Seung-Woo Park4, Jae-Kwan Song3, Dea-Won Sohn2, Namsik Chung1
1Yonsei University College of Medicine, Seoul, Republic of Korea; 2Seoul National University College of Medicine, Seoul, Republic of Korea;3Ulsan University College of Medicine, Seoul, Republic of Korea; 4Sungkyunkwan University College of Medicine, Seoul, Republic of Korea
Background: The aim of this study was to describe the phenotypic spectrum of apical hypertrophic cardiomyopathy (apHCM) and their clinical characteristics. Methods: In the 200 consecutive apHCM patients (58.9±11.2 years;156 men) with preserved LV systolic function (ejection fraction � 50%), patterns of left ventricular hypertrophy by measuring end-diastolic wall thickness of all 16 segments, echo-Doppler parameters, ECG findings, and clinical findings were analyzed. To help the accurate border definition, contrast echocardiography was performed in some patients (n=36). ApHCM was classified into 3 types according to patterns of hypertrophy. Pure focal type (n=84) was defined as hypertrophy confined to 2 or less apical segments, pure diffuse type (n=74) as more than 2 apical segments, and mixed type (n=42) as apical hypertrophy combined with asymmetrical septal hypertrophy but not extend to base and maximal thickness in the apical segment. Results : Lateral apical segment was the most predominant site of maximal hypertrophy. (122 patients, 61%, mean thickness:17.8 mm). Incidence of atrial fibrillation (6% vs. 11% vs. 22%, p<0.005), left atrial volume index (31.0±12.3 ml/m2 vs. 36.1±14.8 ml/m2 vs. 44.3±17.0, p<0.001), peak systolic mitral annular velocity (S’)(6.8±1.4 cm/s vs. 6.6±1.2 cm/s vs. 6.1±2.0 cm/s, p<0.05) were significantly different among subtypes. Total sum of total segmental thckness significantly correlated with sum of precordial (V3-6) negative T waves (r=0.261, p<0.001), S’(r=-0.275, p=0.020) and LAVi (r=0.245, p=0.004). Conclusions: ApHCM contains morphologically heterogenous phenotypes and this subtyping has value on determining the clinical characteristics.
P3-57
Decrease Left Ventricular Mass after Septal Reduction in Patients with Hypertrophic Cardiomyopathy, a Real-time Three-Dimensional Echocardiographic Study
Jian Xin Qin1, Harry M Lever2, Craig R Asher2, Richard D White2, Nicholas G Smedira2, E. Murat Tuzcu2, James D. Thomas2, Takahiro Shiota2
1St. Mary‘s Hospital, Waterbury, CT;2Heart Center, Cleveland Clinic, Cleveland, OH
Introduction: Real-time 3-dimensional echocardiography (RT3DE) can determine volumes in an asymmetric heart without geometric assumptions. The aim of the study was first to demonstrate the accuracy of left ventricular (LV) mass measured by RT3DE, and second to assess the LV mass changes after septal reduction intervention (SRI) in patients with hypertrophic cardiomyopathy (HCM).Methods: Twenty-three HCM patients were enrolled in this study. The first seven patients who underwent RT3DE, 2D echo and magnetic resonance imaging (MRI) within 1 to 2 days were used for the validation study. The remaining 16 patients who had SRI done (2 patients with septal myectomy surgery and 14 patients with percutaneous transluminal septal myocardial alcohol ablation), and had RT3DE and 2D echo performed before and at an average of 6-months after SRI were used to assess the LV mass changes. LV mass was measured using a series of short axis views with Simpson’s rule for both RT3DE and MRI, respectively, and by Penn’s method for M-mode echo. The maximal left atrial (LA) volume was determined by RT3DE. The peak pressure gradient of left ventricular outflow track was obtained from Doppler echo with the simplified Bernoulli equation.Results: For the validation study, the average LV mass measured by MRI was 255 ± 105 gram (130 to 388 gram). A good correlation and agreement for LV mass measurement was found between RT3DE and MRI (LV mass by RT3DE = 0.9 LV mass by MRI + 17, r = 0.99, ?D = -4 ± 7%, p< 0.0001), while M-mode significantly overestimated the LV mass measured by MRI (LV mass by M-mode = 1.0 LV mass by MRI +75, r = 0.71,DD = 42 ± 57%, p = 0.002). For patients with SRI, the peak pressure gradients through left ventricular outflow tract significantly reduced from 60 ± 43 mmHg to 16 ± 12 mmHg, p < 0.001. The LV mass and LA volume measured by RT3DE were significantly decreased from 250 ± 80 gram to 210 ± 62 gram (p < 0.001) and 87 ± 51 ml to 60 ± 20 ml (p = 0.007), respectively. LV mass by M-mode also significantly decreased from 459 ± 129 gram to 359 ± 83 gram (p < 0.0001), however, M-mode significantly overestimated LV mass measured by RT3DE in HCM patients (DD = 85 ± 62%, p < 0.0001).Conclusion: This study demonstrated that RT3DE is an accurate clinical tool for assessing LV remodeling in comparison with routine 2D/M-mode echo, and the LV mass reduced significantly after SRI, which may represent benefits from the relief of the obstruction of left ventricular outflow tract and improve symptoms in patients with HCM.
P3-58
Impact of Player Position on Left Ventricular Mass and Left Atrial Size in Retired National Football League Players
Lori B Croft1, Marc A Miller1, Adam R Belanger1, Arthur J Roberts2, Martin E Goldman1
1Mount Sinai Medical Center, New York, NY;2Living Heart Foundation, Monmouth, NJ
Background: Retired National Football League linemen have a three times greater risk of dying from heart disease compared to non-linemen players, from a report by the National Institute of Occupational Safety and Health. Excessive strength training, from high school through the professional ranks, can lead to persistent increased left ventricular mass (LVM) and left atrial area (LAA), both established risk factors for cardiovascular mortality. We hypothesized that a significantly higher percentage of retired linemen (strength-trained) would exhibit increased LVM and LAA, when compared to non-linemen (endurance-trained).Methods: We measured the LVM (corrected-American Society of Echocardiography cube formula indexed to height) and LAA (apical view) in 303 retired National Football League players who participated in a multi-city screening. Analysis was blinded to demographic, health and professional career information.Results: Retired linemen had greater septal (IVS) thickness, diastolic LV internal diameter (LVID), posterior wall thickness (PWT), LVM, and LAA compared to former non-linemen. A significantly greater percentage of linemen had an LVM/Height of �126 g/m, when compared to non-linemen. There was no difference in age, blood pressure, years in retirement or years played between the two groups.Conclusions: Former Pro Linemen exhibited significantly greater LVM and LAA compared to non-linemen, which may contribute to their higher cardiovascular mortality. Modification of strength-training regimens for high school, college, and professional athletes may need to be considered to minimize long-term cardiovascular consequences.
Non-Lineman Lineman (n=210) (n=93) Measurements Mean SD Mean SD p-valueIVS (cm) 1.08 0.21 1.13 0.20 0.043LVID (cm) 5.02 0.58 5.30 0.60 < 0.001PWT (cm) 1.02 0.17 1.07 0.16 0.008LAA/Height (cm2/m) 11.10 2.57 11.93 3.09 0.018LVM/Height �126 g/m 24.5% 36.9% 0.0275LVM/Height (g/m) 107.6 30.1 121.2 32.7 < 0.001
Journal of the American Society of EchocardiographyVolume 19 Number 5 Abstracts 633

P3-59
Extent of Regional Left and Right Ventricular Apical Wall Motion Abnormalities in Transient Apical Ballooning Syndrome Versus Apical Dysfunction from Coronary Artery Disease: The Importance of Right Ventricular Wall Motion
Robert S. Finkelhor, Mazen Hanna, W. Fredrick Shaw, Robert C. Bahler Case Western Reserve University at MetroHealth Medical Center, Cleveland, OH
Background: Differentiating the ventricular dysfunction due to apical ballooning syndrome (ABS) from that due to apical involvement from coronary artery disease currently requires coronary angiography. As little information exists about subtle differences in their echocardiographic appearance, we sought to determine if the extent of regional left and right ventricular dysfunction could differentiate these conditions. Methods and Results: The 2-D echocardiographic location of wall motion hinge points in both the right and left ventricle were blindly determined in 8 patients with ABS and in 16 patients with acute coronary syndromes producing isolated apical wall motion abnormalities. The extent of the wall motion abnormality was expressed as the percent of the wall that was akinetic from the apex to the annulus for the RV free wall, interventricular septum, anterior LV, inferior LV and lateral LV walls. The RV free wall was adequately visualized in all ABS patients and in 13 of the coronary syndrome patients. The percent of RV involvement was significantly greater in the ABS than with a coronary syndrome (48±20% versus 7.3±15%, p<0.0001). There was no significant difference in septal, inferior and anterior involvement, all around 50%, but the ABS had more involvement of the lateral LV wall (53±18% versus 34±11, p=0.005). An RV hinge point 40% from the apex was exceeded in 7/8 ABS patients but in only 1/13 of those with a coronary syndrome (p=0.0005). Conclusions: The alignment of the ventricular hinge points in the ABS almost linearly transected the apical and basal portions of both ventricles in striking contrast to their more staggered appearance in apical coronary syndromes. This pattern could allow for differentiation of ABS from a coronary syndrome involving the apex.
P3-60
Early Diagnosis of Cardiac Involvement in Primary Amyloidosis: A Potential Role For B-Natriuretic Peptide
Diego Bellavia1, Patricia A. Pellikka1, Ghormallah Al-Zahrani1, Chinami Miyazaki1,Jae K. Oh1, Theodore P. Abraham2, Fletcher A. Miller1
1Mayo Clinic, Rochester, MN;2Johns Hopkins, Baltimora, MD
Background: Brain Natriuretic Peptide (BNP) is a marker of ventricular dysfunction and can be used to identify patients with increased filling pressure. Echocardiography (Echo) is recognized as the best noninvasive imaging tool to diagnose cardiac amyloidosis. We hypothesized that BNP might serve as a screening tool to detect amyloid heart disease in patients with systemic amyloidosis.Methods : Of 103 patients with systemic amyloidosis, patients were divided into two groups based on left ventricular wall thickness. As expected, the group with increased wall thickness (cardiac amyloid) had larger left atria and larger mitral E/E’ ratio. BNP level was compared for the two groups. ROC analysis was performed to determine the BNP level which best discriminated the 2 groups. Clinical and echo characteristics and BNP levels for the two groups are detailed in the following table.Results:Variable (mean±SD) Group I Group II (LV wall � 12 mm) (LV wall > 12 mm)Patient number 73 30Symptoms 0 16 (53%)Age (yrs) 61 ± 10 64 ± 7.6Gender (M = MalesF =Females) M = 31 ; F = 42 M = 25, F= 5SBP (mmHg) 119 ± 10 114 ± 14DBP (mmHg) 70 ± 10 69 ± 10LV wall (mm) 10.1 ± 1.2† 15.5 ± 2.8LA Vol (cc) 33.9 ± 8.7* 43.8 ± 12.2Cardiac_index (l/m²/min) 3.20 ± 0.62 2.96 ± 0.96E/E’’ Ratio (septal E’) 11.4 ± 4.1† 20.1 ± 12.2BNP (Median ± SD) pg/ml 48.5 ± 95.5† 689.1 ± 763.4* p < 0.05 compared with group II; † p < 0.001 compared with group II; SBP: systolic blood pressure; DBP: diastolic blood pressure;LV wall.: half of the sum of the thickness of ventricular septum and posterior walls; LA vol= left atrial volumeBy ROC analysis, BNP level 127.5 pg/ml best discriminated patients with echo evidence of amyloid, AUC 0.908. Of the patients with echo evidence of amyloid, BNP levels were not significantly higher in the subgroup with symptoms (16 vs.14 p =0.27). BNP levels were abnormal (> 127.5 pg/ml) in 24% of patients without echo evidence of cardiac amyloidosis (creatinine 1.52 ± 0.81 mg/dl).Conclusions: BNP was sensitive for identifying patients with systemic amyloid who have definite cardiac amyloid. However, BNP was also elevated in 24% of systemic amyloid patients without echo evidence of cardiac amyloid. Follow-up of these patients is currently underway, to see if they develop cardiac amyloid.
P3-61
Left Atrial Volume Determined by Real-Time 3-Dimensional Echocardiography Predicts Clinical Outcome in Patients with Severe Left Ventricular Dysfunction
Jong-Min Song, Yong-Hyun Park, Eun-Young Lee, Sung-Hee Kang, Jae-Joong Kim, Duk-Hyun Kang, Jae-Kwan Song Asan Medical Center, Seoul, Republic of Korea
Background: Left atrial volume can be accurately measured by real-time 3-dimensional echocardiography (RT3DE) without any geometric assumption. However, clinical impact of left atrial volume determined by RT3DE in patients with left ventricular dysfunction has not been demonstrated.Methods: In 73 patients with severe left ventricular dysfunction (ejection fraction: 27±7%) and sinus rhythm, left ventricular end-systolic and end-diastolic volumes, and left atrial end-systolic (LAVs) and end-diastolic volumes (LAVd) were measured using RT3DE. At the same day, M-mode and 2D Doppler echocardiography were performed. Clinical observation was conducted during 5.1±6.0 months.Results: During the follow-up period, 12 patients admitted to hospital due to heart failure and no patient presented cardiac death. Those 12 patients (16%) showed larger initial LAVs (124±42 vs. 81±30 ml, p<0.001) and LAVd (96±41 vs. 58±28 ml, p<0.01), higher transmitral E wave velocity, lower late diastolic mitral annular velocity, more severe mitral and tricuspid regurgitation, and higher maximal velocity of tricuspid regurgitation than those without clinical events. There was no significant difference between the two groups in initial left atrial diameter on M-mode echocardiography, E/E’ ratio, left ventricular volumes and ejection fraction, and the proportion of ischemic cardiomyopathy. Among all variables, LAVs showed the largest area under the curve (0.80, 95% confidence interval: 0.66-0.94) in ROC curve analysis for predicting cardiac events. LAVs � 93 ml predicted the events with sensitivity 83% and specificity 67% (Figure).
Conclusion: LAVs determined by RT3DE is a strong predictor for heart failure in patients with severe left ventricular systolic dysfunction and sinus rhythm.
P3-62
Diastolic Septal Wall Motion in Constrictive Pericarditis: Color Doppler Tissue Velocity Imaging and Strain Rate Imaging Study
Seong-Mi Park, Grace C Casaclang-Verzosa, Bellavia Diego, Raul E Espinosa, Fletcher A Miller, Jae K Oh Mayo Clinic, Rochester, MN
Background Constrictive pericarditis (CP) has a limitation of diastolic filling of both ventricles and has a characteristic ventricular septal (VS) motion abnormality due to hemodynamic changes. We hypothesized that the diastolic VS wall motion in CP would have a strain rate imaging (SRI) pattern that would distinguish it from normal and from restrictive cardiomyopathy.Methods Color Doppler tissue imaging was performed in three groups (mean age; 58±12 years, 10 normal controls, 10 patients with CP and 10 patients with cardiac amyloidosis,CA). Tissue Doppler velocity imaging (TVI) and SRI values were obtained from the VS at the base, mid and apex, using apical 4-chamber view.
Results In patients with CP, TVI of the VS showed high early diastolic velocity (Em) with low systolic velocity (Sm) and these velocities decreased from base to apex. In six patients with CP, TVI showed an additional velocity wave (1.0~2.0 cm/s) in opposite direction, immediately after Em, that was not clearly observed in normal and CA (Fig. TVI, red arrow). This TVI pattern was similar in all segments. Patients with CP also showed increased early diastolic SR (SRe) but, systolic SR was well preserved. Eight patients with CP had a more prominent and abrupt wave (-0.6~-2.0 1/s) in the
opposite direction after SRe (Fig. SRI, red arrow). The other two patients with CP did not show this opposite wave with either TVI or SRI. In contrast to TVI, SRe of CP was not reduced in apical segment and the wave pattern of SRI during diastole was different for each segment. In CA, Em and Sm were decreased in all segments and were more decreased in the apical segment. SRe of CA was low at base and mid levels and relatively increased in the apical segment of VS. No patient with CA had a prominent extra-septal wall motion wave following Em and SRe.Conclusion The diastolic septal wall motion pattern in CP with TVI and SRI was different from normal and from CA. SRI showed biphasic septal wall motion during the diastolic period, representing a unique disturbance of ventricular diastolic filling in CP.
Color Doppler Tissue Velocity and Strain Rate of Ventricular Septum Normal Control Constrictive Pericarditis Cardiac Amyloidosis
Base Mid Apical Base Mid Apical Base Mid ApicalSm (cm/s) 6.0±1.1 4.0±1.3 2.8±1.2 4.1±1.2 2.6±1.2 1.5±0.9 4.6±1.3 3.4±1.1 2.8±0.9Em (cm/s) -6.6±1.8 -5.3±1.4 -4.1±1.3 -7.3±3.0 -6.1±2.1 -4.4±1.9 -4.2±1.4 -3.3±0.9 -2.7±0.7Am (cm/s) -5.3±1.3 -4.5±1.1 -3.2±1.1 -3.4±3.0 -2.4±1.9 -2.8±1.4 -6.6±1.2 -5.8±0.9 -4.5±1.1SRs (1/s) -1.2±0.1 -1.2±0.4 -1.1±0.3 -1.4±0.4 -1.4±0.5 -1.2±0.3 -0.7±0.3 -0.4±0.5 -0.8±0.1SRe (1/s) 1.7±0.5 1.3±0.4 1.4±0.6 2.1±0.8 1.7±0.8 2.0±1.1 0.6±0.3 0.5±0.3 0.9±0.3SRa (1/s) 0.9±0.4 0.8±0.4 0.8±0.4 0.9±1.1 1.4±1.3 1.2±1.0 0.9±0.7 1.1±0.9 1.1±0.7
Journal of the American Society of Echocardiography634 Abstracts May 2006

P3-63
Hyperhomocysteinemia-Induced Atrial Remodeling in Patients with Chronic Heart Failure
Prasad V Maddukuri1, Sunil Matiwala1, Timothy Fitzgibbons1, GVRK Sharma2,Jacob Joseph3
1Boston Medical Center, Boston, MA;2VA Boston Healthcare System and Harvard Medical School, West Roxbury, MA;3VA Boston Healthcare System and Boston University School of Medicine, West Roxbury, MA
Background: Preclinical studies indicate that hyperhomocysteinemia (Hhe) leads to myocardial fibrosis and cardiac dysfunction, and recent epidemiologic and clinical investigations suggest an association of Hhe with myocardial dysfunction and clinical heart failure (HF), both systolic and diastolic. Although Hhe-induced atrial remodeling has been reported in preclinical studies, prior human studies in subjects without HF have failed to show an association. Hence we examined the relation of Hhe to echocardiographic measures of LA and left ventricular (LV) structure in patients with HF and LV systolic dysfunction, which has not been previously studied.Methods: We performed a retrospective analysis of patients with LV systolic dysfunction followed in the HF clinic at VA Boston Healthcare, who had prior plasma homocysteine (Hcy) measurements, as well as transthoracic echocardiography within 4 weeks of Hcy measurement. A total of 126 patients (all male) met inclusion criteria. (mean LV Ejection fraction 28 ± 7; mean age 72 ± 10 yrs; and 30% non-ischemic HF). Echocardiographic measurements including LV mass by American Society of Echocardiography cube method were correlated with plasma Hcy values. Regression analysis (r) was performed to correct for confounding variables.Results: Univariate analysis showed that Hcy is significantly related to LA size (r = 0.33; p=0.0002), while there was no correlation with systolic blood pressure, LV end diastolic diameter, LV relative wall thickness, fractional shortening, LV EF and LV mass. Multivariate analysis showed Hcy is a strong independent predictor of LA size (r = 0.28, p = 0.009) even after correcting for age, severity of mitral regurgitation, and LV mass. Figure 1 demonstrates that mean LA size in patients with Hcy levels above the median for the group(13.78 µmol/L) was significantly elevated (48.23 ± 0.3) compared to patients below the median level ( 45.5 ± 0.4; p< 0.05).
Conclusions: Plasma Hcy values were significantly correlated with LA size in male patients with systolic HF independent of age, LV mass and severity of mitral regurgitation. The Hhe-induced remodeling of LA, not reported before in patients with systolic HF, may be secondary to a direct effect of Hcy on LA structure and function due to increased myocardial fibrosis, as reported in preclinical studies.
P3-64
Isolated Left Ventricular Noncompaction: A Normal 2D Echocardiographic Variant?
Usha Donthireddi, Andrew J. Najovits, Adam R. Belanger, Martin E. Goldman Mount Sinai School of Medicine, New York, NY
Background: Isolated left ventricular noncompaction/hypertrabeculation (LVNC) is a distinct cardiomyopathy associated with left ventricular (LV) dysfunction, thrombosis, arrhythmias, and neuromuscular disorders. Previous definitions of LVNC have applied strict echocardiographic criteria for diagnosis, including > 3 trabeculations, ratio of noncompacted/compacted myocardium width (N/C) > 2, and evidence of blood flow between trabeculae on color Doppler imaging. Prominent trabeculations in the apex of the LV may be more common than previously reported, especially with current high-resolution echo systems.Objective: To evaluate the prevalence and spectrum of noncompaction; to explore the relationship between LVNC and echocardiographic and clinical parameters of LV function in unselected echocardiograms.Methods: We reviewed 500 randomly selected transthoracic echocardiograms representing a wide range of ages and ethnicities, and including both inpatients and outpatients. Two reviewers assessed each echo for noncompaction of the LV apex, blinded to age, sex, indication, and global LV size and function. When present, the linear N/C ratio was measured and the total area of noncompaction (LVNC area) was digitally planimetered and graded 0-4 based on severity in the apical 4-chamber view. These findings were correlated with the corresponding patient’s echocardiographic and clinical features.Results: Of the 500 echocardiograms, 84 patients had at least one vessel coronary artery disease on cardiac catheterization, and were excluded. 74 of the remaining echoes (17.8%) had measurable areas of noncompaction at the LV apex. There was a correlation between the N/C ratio and the LVNC area (R = 0.420, p =0.0002). The N/C ratio underclassified the severity of LVNC in 7 of 10 cases (using LVNC area as the gold standard). Patients with severe LVNC by area (>4 cm2) had a lower ejection fraction when compared to patients with minimal (<1 cm2) LVNC by area (42% vs. 56%, respectively, p = 0.03). Otherwise, there was no significant correlation between LVNC severity - using the N/C ratio or the LVNC area - and age, gender, LV size, or LV systolic or diastolic function.Conclusions: Using high-resolution 2D echocardiography LVNC occurs more commonly than previously appreciated, and exists as a spectrum from mild to severe. Though prior studies have addressed implications of the severe variant of LVNC, the milder forms of LVNC may not adversely affect LV performance and may be considered a normal variant. The relative utility of measuring the total LVNC area rather than the linear N/C ratio needs to be further explored.
P3-65
Echocardiographic Features of the Cardiomyopathy Associated with Alstrom Syndrome: A Retrospective Review
Michael E. Zubrow1, Amgad Makaryus2, Jan D. Marshall3, Sheryl Horowitz1, Linda D. Gillam1, Judy R Mangion1
1Hartford Hospital, Hartford, CT;2Northshore University Hospital, Manhasset, NY;3Jackson Laboratory, Bar Harbor, ME
Background: Alstrom Syndrome is an extremely rare (369 clinically diagnosed cases in the world), autosomal recessive genetic disorder characterized by infantile onset dilated cardiomyopathy(CMP), blindness, hearing impairment/loss, and obesity. Prior reports have demonstrated an 81% incidence of dilated CMP with heart failure presenting between 2 weeks and 7 months of age. Many of these pts ultimately die of heart failure as infants and children, although some survive to adulthood. To date, there have been no prior reports examining the echo features of the CMP.Methods: 11 pts(7 female, 4 male) diagnosed with Alstrom Syndrome(age 1-14 yrs), who underwent 1 or more transthoracic echocardiograms (TTEs) from 1994-2003 were retrospectively evaluated. A total of 16 TTEs were reviewed by a level III trained echocardiographer with emphasis on chamber sizes, wall thickness, left and right ventricular systolic function (regional and global), valve disease, congenital disease, and pericardial disease.Results: 4/11pts (36%) had evidence of global LV systolic dysfunction (quantitative EF range 9-29%). 3 of these 4 pts also had severe generalized RV systolic dysfunction, while 1 had normal RV systolic function. LV and RV dilation was present in 3/4. 4/4 low EF pts had an apically tethered mitral valve closure pattern, however only 1/4 had moderate MR. 3/4 low EF pts had an apically tethered tricuspid valve closure pattern, however none had more than mild TR. There was no significant aortic or pulmonic valve pathology. LVH was present in 2/11 pts(18%) overall and 1/4 (25%) with low EF. LV and LA dilation was observed in 3/7(42.9%) of the pts with normal EF although RV and RA size were normal. Reduced EF was not associated with regional wall motion abnormalities, however 3/11 (27%) pts overall and 2/4 (50%) of the low EF pts had pericardial effusions. 2/4 of the low EF pts had a patent foramen ovale. No other congenital abnormality was identified. None of the pts with low EF had f/u echoes.Conclusions: The Alstrom CMP in this cohort of pts was typically dilated and non-segmental with predominantly biventricular involvement. It was not associated with myocardial hypertrophy. Apically tethered mitral and tricuspid valve closure patterns were visualized, although severe functional valvular insufficiency was not present. LV and LA dilatation was observed in a number of pts without reduced EF, and may be an early stage in the development of the CMP.
P3-66
Adding Cardiac Resynchronization Therapy Enhances the Efficacy of Left Ventriculoplasty for End-Stage Congestive Heart Failure
Takeshi Shimamoto, Takeshi Nishina, Keiichi Tambara, Akira Marui, Yoshiaki Saji, Masashi Komeda Kyoto University Hospital, Kyoto, Japan
[Background]Cardiac resynchronization therapy (CRT) utilizing biventricular (Bi-V) pacing has been shown to improve cardiac function in patients with severe congestive heart failure (CHF) and intraventricular conduction disturbance. Left ventriculoplasty (LVP) improves LV performance by excluding dyskinetic/akinetic region, adjusting LV size/shape and mitral regurgitation if any. Efficacy of each treatment and their combination needs to be interrogated. [Methods] Sixty three patients with end-stage CHF were treated with LVP. Among those, ratio of ischemic cardiomyopaty(ICM)/dilated cardiomyopathy(DCM) etiology is 46/17. LVP were performed on beating basis to protect myocardium. [Results]Parameters before and 1 week after the operation were as follows: EF 30 to 41#%, LVDd 70 to 55#mm(), MR grade 2.0 to 0.4†, Tenting length 8.2 to 4.0mm*, 9 preoperative IABP and 12 emergency operations in LVP group, respectively (*p<0.05, #p<0.01 and †p<0.0005 vs. preoperative). Seven patients with intraventricular dyssynchrony showed remarkable hemodynamic improvement with perioperative Bi-V (LVP+CRT group) and did well without any ventricular assisting device. There were 10 early death (1 with LVP+CRT, mostly emergency patients or preoperative MOF) and 5 late death (2 with LVP+CRT) among LVP group.[Conclusion]LVP treats mitral-LV complex simultaneously and effectively and is indicated for higher-risk patients who are otherwise abandoned. This study showed that LVP treat end-stage CHF efficaciously and CRT have a synergistic/additive effect to LVP.
Journal of the American Society of EchocardiographyVolume 19 Number 5 Abstracts 635

P3-67
Comparison of Computed Tomography to Echocardiography for Assessing Hemodynamic Significance of Pericardial Effusions
Brian C Kolski, William Kakimoto, David L Levin, Daniel G Blanchard University of California, San Diego, San Diego, CA
Purpose Rapid diagnosis of cardiac tamponade is critically important in patients with pericardial effusion (PE). Although Doppler echocardiography is the noninvasive test of choice for diagnosis of tamponade, pericardial effusions are often first detected by computed tomography (CT). Few data are available, however, regarding the accuracy of CT in detecting tamponade. In this study, we investigated the diagnostic accuracy of CT compared to echocardiography in correctly diagnosing hemodynamically significant pericardial effusions (HSPE).Methods We retrospectively identified 29 consecutive hospitalized patients with pericardial effusion who underwent both chest CT and cardiac echo within forty-eight hours between 2001 and 2005. CTs were analyzed by experienced radiologists without knowledge of the echo results. CT diagnosis of HSPE was based on the following findings: (1) right ventricular (RV) wall flattening; (2) PE size; and (3) presence of pericardial thickening. The findings were compared to Doppler echocardiography, using the presence of (1) right ventricular diastolic collapse and/or (2) >20% respiratory variation in transmitral peak Doppler flow velocity as the criteria of hemodynamic significance.Results Of the 29 patients, 16 had hemodynamically significant PE by echo criteria. RV wall flattening on CT correlated with HSPE with a positive predictive value of 71%. Pericardial thickening on CT correlated with HSPE with a positive predictive value of 66%. CT was most accurate in diagnosing HSPE when the effusions were large (n=6) and was 100% sensitive and specific in this group. Of the small to moderate sized effusions (n=23), the sensitivity and specificity were 80% and 75%, respectively.Conclusions Although not as accurate as echo, chest CT is nonetheless a useful method to detect HSPE. CT findings of RV wall flattening, pericardial thickening, and a large pericardial effusion significantly increase the likelihood of tamponade. In this study, the majority of patients diagnosed with HSPE by CT did indeed have tamponade by standard echo criteria. Thus, the diagnosis of HSPE by CT is usually correct and should prompt a rapid clinical evaluation of affected patients.
P3-68
Left Ventricular Global Performance and Diastolic Function in Indeterminate and Cardiac Forms of Chagas’ Disease
Minna M D Romano, Rogério G Furtado, Antônio Pazin-Filho, José A Marin-Neto, Benedito C Maciel Medical School of Ribeirão Preto, Ribeirão Preto, Brazil
The majority of patients with Chagas‘ disease (CD) remain for 10-30 or even more years in the indeterminate form (IF) of this disease.They have: no symptoms, serologic positivity, normal ECG and heart size and normal left ventricular global and segmental (LV) systolic function on 2D echo. To investigate if this group of patients have any impairment of LV global performance (Tei) and diastolic function, we have studied 47 individuals aged 49 ± 12 years, divided in three groups: 17 normal (N), 12 individuals with IF, and 18 with the cardiac form (CF) (4 with only ECG changes and 14 with exclusive LV segmental dysfunction). Echo measurements included: ejection fraction (EF), Tei index, left atrial volume (LAVol), transmitral (E, A, TD, A duration) and pulmonary ( S, D, Ar and Ar duration) flow velocities, and tissue Doppler (TD) velocities at lateral mitral annulus (Em, Am, S). Results: (* = p<0,05; # = p<0,001; & = p<0,0001; CF x N e IF).
Table 1. N IF CFEF 66 ± 7 63 ± 5 53± 10 *TEI 0,62 ± 0,11 0,64 ± 0,11 0,74 ± 0,2 (NS)S(TD) 9,42 ± 1,70 9,6 ± 3,00 6,43 ± 1,26 &LAVol 22,3 ± 5,7 21,3 ± 6,6 31,2 ± 15 *E 76 ± 16 66 ± 14 60 ± 15 *E/Em(TD) 5,2 ± 1,2 5,1 ± 1,5 7,8± 2,9 #Em(TD) 14,8 ± 3,2 13,8 ± 4 8,3 ± 2,8 &
In conclusion: 1) although EF and S(TD) velocity were lower in patients with CF of CD comparing to normals and IF, Tei index was not able to differentiate these patients from the other groups; 2) diastolic disfunction was documented in patients with CF of CD by LAVol,E velocity, E/Em(TD), Em(TD); 3) patients with the IF of CD did not show any abnormality of diastolic function.
P3-69
Actitvation Sequence & Dyssynchrony in Patients with LV Dysfunction: An Analysis Using Tissue Doppler Imaging
Vanita Arora, Simmi M Manocha, Ravi R Kasliwal, Pankaj Gupta, Aparna Jaswal, Nagendra Chauhan Escorts Heart Institute and Research Centre, New Delhi, India
Background: A vast majority of LV dysfunction patients present with LBBB & IVCD, while upto 20% of cardiac resynchronization therapy (CRT) candidates present with RBBB or narrow QRS complex morphology. CRT may provide additional benefit when applied to the most delayed site in all patients demonstrating dysynchrony, regardless of the EKG pattern. The goal of this study was to evaluate the patterns of dysynchrony in patients with LV dysfunction with or without BBB.Methods: Tissue doppler imaging (TDI) was used for assessment of atrio-ventricular dysynchrony (diastolic filling period DFP<40% of cardiac cycle), inter-ventricular dysynchrony (AEP-PEP= >40 msec and time delay between RV free wall & inter-ventricular septum= >40 msec), intra-ventricular dysynchrony (septal posterior wall delay SPWD and maximum delay between any two walls= >60 msec) and LV activation pattern in 70 consecutive patients of LV dysfunction (LVEF<30%). The result was then correlated with the QRS morphology.Results: The earliest & delayed activation sequence was quite similar in patients with LBBB & RBBB. However the SPWD was not seen in patients with RBBB. There was delayed opening of the pulmonary valve in patients with RBBB & with narrow QRS, hence equalizing AEP & PEP, a representation of dyssynchrony.Conclusion: Refinement of the selection criteria based solely on mechanical measures of resynchronization is promising, but premature. Analysis of both electrical and mechanical measures of dysynchrony will not only help us better select patients for the CRT, but will widen the benefits of the therapy in groups left out for the therapy.
LBBB + IVCD + PACED RBBB NARROW QRSNo of pts 39 + 7 + 2 11 11SPWD >130 msec 21 + 5 + 1 0 2Intraventricular Dysynchrony 32 + 5 + 1 8 6Interventricular delay >40 msec 19 + 5 + 1 5 5
Early(E) & Delayed(D) activation sequence (TDI result) LBBB + IVCD RBBB NORMAL QRSSeptal E31 E8 E0 D9 D2 D0Inferior Posterior Lateral wall E12 E3 E0 D34 D9 D11Anterior wall E5 E0 E11 D5 D0 D0
P3-70
N-Terminal Pro-Brain Natriuretic Peptide can Grade Left Ventricular Diastolic Dysfunction in Patients with Idiopathic Dilated Cardiomyopathy
Sung Uk Kwon, Seung Woo Park, Sang-Chol Lee, Eun-Seok Jeon Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
Background and study objective: Although the echocardiographic criteria of left ventricular (LV) diastolic dysfunction have been used clinically, N-terminal pro-brain natriuretic peptide (NT-proBNP) levels have not been correlated nor have not been compared with echocardiographic criteria to evaluate the degree of LV diastolic dysfunction in patients with idiopathic dilated cardiomyopathy who had already LV systolic dysfunction. Therefore, we wanted to evaluate whether NT-proBNP could estimate the degree of LV diastolic dysfunction and could be used as a powerful predictor of LV diastolic dysfunction in patients with dilated cardiomyopathy.Subjects and methods: Thirty consecutive patients at outpatient clinics with idiopathic cardiomyopathy enrolled. NT-proBNP levels, clinical assessment and comprehensive echocardiographic study have done simultaneously. In the presence of a left ventricular ejection fraction <50%, echocardiographic heart falure (eCHF) had been defined as 2 of 3 of the following diastolic dysfunction criteria: 1) mitral inflow (E/A >1 or deceleration time <160ms, or both), 2) left atrial volume >30 mL/m2 and 3) tissue Doppler-derived ratios (E/Ea >15).Results: There was no difference in NYHA class comparison between eCHF and Non-eCHF. However, there were differences in LVESD, EF, E/A, E/Ea ratio, LAVI and NT-proBNP levels between groups (p <0.05, respectively). In ROC curve, NT-proBNP > 300 pg/mL (AUC 0.949, p <0.001), E/Ea >10 (AUC 0.831, p=0.002), LAVI > 35 mL/m2 (AUC 0.866, p=0.001), and LVEF > 30 % (AUC 0.769, p=0.014) were predictive of eCHF.Conclusion: The levels of NT-proBNP (more than 300 pg/mL) could estimate the severity of LV diastolic dysfunction and eCHF in idiopathic dilated cardiomyopathy with LV systolic dysfunction.
Journal of the American Society of Echocardiography636 Abstracts May 2006

P3-71
The Role of N-Terminal Pro-B-Type Natriuretic Peptide for Assessment of Disease Severity in Patients with Pericardial Effusion
Shin-Jae Kim, Eun-Seok Shin, Sang-Gon Lee Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Republic of Korea
Background: N-terminal pro-B-type natriuretic peptide(NT-proBNP) has been introduced recently as an useful marker for the diagnosis in patients with dyspnea and for the prognosis in patients with heart failure and coronary artery disease. However, its role for assessment of disease severity in patients with pericardial effusion, especially cardiac tamponade in which diastolic pressures of both ventricles are increased despite of decreased intracardiac volumes, has not been defined. We tested the hypothesis that NT-proBNP levels correlate with the clinical and echocardiographic parameters in patients with pericardial effusion.Methods: 50 consecutive patients who showed moderate or more amounts of pericardial effusion with preserved left ventricular(LV) systolic function were enrolled. Patients with ejection fraction <40%, postoperative effusion, more than 1.5mg/dl of serum creatinine, known coronary or valvular heart diesease, or atrial fibrillation were excluded; 32 patients participated. We evaluated the etiology, clinical and echocardiographic parameters, and the serum NT-proBNP levels.Results: Patents(37.5% male, mean age 58±17 years) showed preserved LV systolic function(61.8±8.8%) and pericardial effusion(moderate 59.4%, large 40.6%); 30.3% of which had cardiac tamponades. The causes of pericardial effusion were tuberculosis(34.4%), idiopathic(28.1%), malignancy(21.9%), hypothyroidism(6.3%), and others(9.3%). The NT-proBNP levels ranged from 5 to 5289ng/L with a median of 861.4ng/L. Among a variety of clinical and echocardiograhic parameters used for the assessment of the severity of pericardial effusion the NT-proBNP levels were significantly higher in groups with findings of large pericardial effusion*, cardiac tamponade**, neck vein distension**, exaggerated respiratory variation of transmitral inflow* and plethora of inferior vena cava(IVC)* compared to patients without these findings(*p<0.05, **p<0.01). NT-proBNP showed significant negative correlations with LV end-diastolic dimension(r=-0.36 and p<0.05) but not deceleration time of early transmitral flow, ratio of transmitral peak E velocity/mitral annular E’ velocity, left atrial volume index, and diameter of IVC.Conclusion: NT pro-BNP may have a potential use as an additional, simple and relatively cheap, method as a marker for disease severity in patients with pericardial effusion. Large prospective randomized trials are needed to confirm utility.
P3-72
Variables Influencing the Accuracy of Right Ventricular Volume Assessment by Real-Time Three-Dimensional Echocardiography: An in vitro Tank Model Study
Martin Hoch, Nikolay Vasilyev, Brian Soriano, Kimberlee Gauvreau, Gerald R Marx Children‘s Hospital Boston, Boston, MA
Background: Our preliminary experience in matrix array real-time three-dimensional echocardiography (3DE) in pediatric patients has demonstrated a consistent underestimation of right ventricle volume (RVV) measurements, when compared to MRI. Our hypothesis was that variables in 3DE acquisition and off-line analysis, including offline gain settings, thickness, and orientation of discs could alter RVV measurements.Methods: Displacements of 7 different volumes of water from a latex model derived from an excised lamb heart were used for comparisons. Philips 7500 3DE system was used with X4 matrix array probe. RVVs were calculated offline by TomTec software using summation of 5mm discs oriented in the short axis, and optimal offline gain settings (median value 25%). Axis of cut planes was analyzed comparing long to short axis. Gain was compared at low value (decreased 50%), and high value, (increased 50%) of optimal settings. Cut planes were compared at 5, 10, and 15 mm disc thickness.Results: Mean RVV by 3DE was 28.5 ml +/- 9.1 (range 18.8-43.6). Mean RVV by displacement of water was 29.7 ml +/- 9.8 (range 19-44), (p=ns); y=1.01x-0.2, r= 0.99; mean difference was -0.49ml (limits - 4.5 to 3.5). Mean RVV by 3DE with high gain settings was 24.5ml +/- 1.8 (range 13.3-40.1); (p<0.01); y=1.03x+4.4, r=0.98; mean difference -5.2 ml (limits-8.7 to 1.7). Mean RVV with low gain settings was 23.7ml +/- 10.4 (range 16.9-40.1); (p<0.01); y=0.85+9.6, r=0.9; mean difference -6.1 ml (limits -14.8 to 2.7). Mean RVV traced in a long axis cut plane was 26.85 ml +/- 9.31 (range 16.3 - 42.2); p<0.01; y=1.04x+1.8, r=0.99; mean difference -2ml (limits -8.2 to 4.2). No significant difference was found for 3DE RVV measurements for 5 and 10 mm thickness, however 15 mm thickness cut planes were significantly different. To determine the maximum thickness of cut planes for accurate RVV determinations, comparison was done at 11 and 12 mm. A significant difference was noted at 11 mm slice thickness.Conclusions: Right ventricular volumes can be assessed accurately by matrix array three-dimensional echocardiography in combination with summation of discs method in an in-vitro model. Operator dependent changes in offline gain settings, number, and orientation of cut-planes underestimated right ventricular volumes. On going study now includes a pump model for systolic and diastolic comparisons. Considering operator dependent variables of off-line gain settings, and number and orientation of cut planes, should allow accurate three-dimensional echocardiographic right ventricular volume measurements in clinical studies.
P3-73
Mitral Annular Dilatation in Patients with Functional Mitral Regurgitation: A Novel Computerized 3D Echo Method
Masao Daimon, Giuseppe Saracino, Shota Fukuda, Deborah A Agler, A. Marc Gillinov, James D Thomas, Takahiro Shiota Cleveland Clinic Foundation, Cleveland, OH
Background: We assessed dynamic change of mitral annular area (MAA) during the cardiac cycle in patients with mitral regurgitation (MR) by idiopathic dilated cardiomyopathy (DCM-MR) using a novel computerized 3D echo method. Then, we examined 1) the relationship between minimum MAA and the MR severity, and 2) the relationship between minimum MAA and left ventricular (LV) geometries.Methods: Real-time 3D echo was performed in 12 normal controls and 15 patients with DCM-MR. Twelve points along the saddle-shaped annulus in 3D space were identified manually with customized visualization in every 3D volume/frame during a cardiac cycle. For each 3D volume/frame, we assessed mitral annular area (MAA) determined by the best-fit plane of curved 3D mitral annulus. LV volumes were calculated using 3D volume data. The sphericity of the LV chamber at end-systole was calculated as the ratio of the LV chamber width to the LV heights from the mitral annulus in both the antero-posterior and commissura-commissura planes, using 3D echo data. MR was quantified by regurgitant orifice area (ROA) using the PISA method.Results: DCM-MR had larger minimum and maximum MAA than controls (7.7 ± 2.1 vs 3.6 ± 0.8 cm2, 9.6 ± 2.3 vs 6.4 ± 1.2 cm2, p < 0.001 for both, respectively). Minimum MAA in DCM-MR had a significant correlation with MR severity by ROA (r = 0.73, p < 0.01). While neither LV end-systolic volume (r = 0.50, p = 0.06) and end-diastolic volume (r = 0.46, p = 0.08) nor LV ejection fraction (r = 0.11, p = 0.7) had significant correlations with minimum MAA, both LV sphericities at the antero-posterior and commissura-commissura planes had significant correlations with minimum MAA (r = 0.59, p < 0.03 and r = 0.70, p < 0.01). Conclusion: Our novel computerized 3D echo method disclosed dynamic change of MAA in DCM-MR. Mitral annular dilatation was an important pathogenesis in DCM-MR, and had a significant relationship with LV sphericity rather than LV volume.
P3-74
Objective Visualization and Quantification of Spatial and Temporal Extent of Wall Motion Asynchrony Using 3D echocardiographic Phase Imaging in Heart Failure
Arthur Filusch1, Alexander Hansen1, Stefan Hardt1, Grigorios Korosoglou1,Christian Galuschke2, Helen Houle3, Helmut Kuecherer1
1University of Heidelberg, Heidelberg, Germany; 2Tomtec Imaging Systems, Unterschleissheim, Germany; 3Siemens Medical Solutions, Ultrasound Division, Mountain View, CA
Background: Temporal and spatial extent of contraction asynchrony have been identified as risk factors for worsening heart failure and reduced clinical outcome. Assessment of mechanical asynchrony by echocardiography is an evolving method of predicting systolic function improvement with cardiac resynchronisation therapy (CRT) in patients with biventricular pacemakers. The aim of the study was to test whether 3D parametric echocardiographic phase imaging (EPI) of endocardial motion can be used to objectively quantify intraventricular contraction delays. Methods: 3D parametric echocardiographic phase images (EPI) were obtained in twentyfive patients with heart failure (mean age 65±5, EF 30±5%). Digital cine loops of apical four, three and two chamber views were mathematically transformed into a 3D myocardial map using a first harmonic Fourier algorithm displaying magnitude and temporal sequence of cyclic endocardial motion in a color-coded format. As a reference time to peak myocardial velocity was measured using pulsed wave TDI. Asynchrony was determined as the difference between the electromechanical coupling times in the basal myocardial segments and the basal septum. Contraction delays derived from TDI were compared to those derived from 3D EPI using linear regression and Bland-Altman statistics. Results: Motion asynchrony was easily identified from parametric 3D images. Spatial extent of mechanical asynchrony was clearly estimated by 3D EPI (53.6±5% of total LV). 3D EPI correlated very closely with TDI (r=0.7182 for lateral wall, r=0.9362 for inferior wall, r= 0.7407 for anterior wall, r=0.8243 for posterior wall; p=0.0002). The mean difference between TDI and EPI derived intersegmental delays was 4,6±10,6 ms with upper and lower limits of agreement of 25,5 and -21,3 ms. Conclusions: Echographic 3D phase imaging allows objective visualization and quantification of intraventricular asynchrony in patients with heart failure. This new method can be easily used for the analysis of the effects of resynchronisation therapy on left ventricular function.
Journal of the American Society of EchocardiographyVolume 19 Number 5 Abstracts 637

P3-75
Cardiac Resynchronization Therapy is Associated with Acute and Persistent Reduction in Left Atrial Volume in Patients with Advanced Heart Failure
Prasad V Maddukuri1, Alawi A Alsheikh-Ali2, Robert S Phang3, Marcelo L Vieira4,Ayan R Patel2, Natesa G Pandian2, N.A Mark Estes, III2, Mark S Link2
1Boston Medical Center, Boston, MA; 2Tufts New England Medical Center, Boston, MA; 3Albany Medical Associates, Albany, NY; 4Heart Institute (InCor), University of São Paulo Medical School, São Paulo, Brazil
Background: Left atrial (LA) enlargement is a marker of adverse clinical events and may predispose to atrial fibrillation. Cardiac resynchronization therapy (CRT) improves outcomes in patients with advanced heart failure (HF). While CRT reduces left ventricular (LV) volume, its impact on LA volume (LAV) is less defined.Methods: Patients with HF (n=24) underwent live 3D full volume echocardiograms (Philips 7500) at baseline and 48 hours post CRT. A subset of patients (n=13) also completed a 2 month post CRT study. Using off line analysis (Tomtec), LAV (at ventricular end-systole), LV end-systolic volume (LVESV), LV end-diastolic volume (LVEDV) and LV ejection fraction (LVEF) were measured.Results: Patient baseline characteristics were (mean ± SD): age 68 ± 9.7 years, EF 22.7 ± 7.3 %, 16 males, mean NYHA class 3, 83% with ischemic cardiomyopathy. There was a significant reduction in LAV at 48 hours post CRT (TABLE). The reduction in LAV persisted in the subset of patients assessed at 2 months of follow-up. CRT was also associated with an increase in LVEF and reduction in LVESV. There was a significant correlation between changes in LV volumes and the observed reduction in LAV, both at 48 hours (change in LAV vs LVESV r = 0.4, LAV vs LVEDV r = 0.5) and at 2 months (change in LAV vs LVESV r = 0.7, LAV vs LVEDV r = 0.6; P < 0.05 for all correlations).Conclusion: CRT in patients with advanced HF is associated with an acute and persistent reduction in LAV. Further studies are needed to assess the prognostic implications of this finding.
Mean values [% change from baseline] for 3D-echo parameters. * P < 0.05, † P < 0.001 vs baselineLAV (ml) LVEF (%) LVESV (ml) LVEDV (ml)
Baseline (n = 24) 86.7 22.9 122.8 15748 hrs [%change] (n = 24) 78.2 26.9 115.8 156.7 [-9.8%]† [+17.5%]† [-5.7%]* [-0.00%]2 months [% change](n = 13) 72.1 28.3 115.3 160.7 [-13.4%]† [+26.3%]† [-14.2%]* [+7.3%]
P3-76
The Regional Contraction Pattern of the Right Ventricle Differs between Dilated Cardiomyopathy and Tetralogy of Fallot
Florence Sheehan1, Wes Vick2, Shuping Ge2
1University of Washington, Seattle, WA;2Baylor College of Medicine, Houston, TX
Background: The right ventricle (RV)’s principle fiber direction is longitudinal. However we have previously reported significant differences in three dimensional (3D) shape between patients with cardiomyopathy vs. repaired tetralogy of Fallot (TOF) with wide open pulmonary regurgitation: increased roundness of the RV’s cross section in TOF vs. crescentic cross sections in cardiomyopathy similar to normal.Methods: We analyzed RV regional function from our patients‘ 3D reconstructions, which had been generated from echo or MRI data using the piecewise smooth subdivision surface method. We computed the stroke volume contributed by each of 20 slices spanning the RV’s length from apex to tricuspid annulus (TA). Each slice’s contribution to global stroke volume was computed as [ED slice area x ED RV length /20]- [ES slice area x ES RV length /20] .Results: RV ejection fraction was 49+/-8% in 20 normal subjects, 27+/-10 in 9 cardiomyopathy patients, and 38+/-10 in 16 TOF patients (p<0.0001 by ANOVA). The pattern of stroke volume contribution varied by slice location from apex to TA and between between diagnosis groups (Figure)(p=0.001 ANOVA for repeated measures). In cardiomyopathy most of the regional stroke volume was contributed by basal slices, whereas much more stroke volume was contributed by mid-RV and apical slices in TOF. The greatest difference between the cardiomyopathy and TOF groups was seen at slice 5 near the apex and slice 19 near the TA. When the ratio of these two slices was computed and correlated with the eccentricity of the slice cross sectional contour, we saw that the apical slice contributed more to stroke volume when its shape was rounder (less eccentric): r=0.51, p<0.005).
Conclusions: The greater stroke volume contributed by apical and mid-RV slices in TOF suggests that the greater roundness of the RV is an accommodation to the hemodynamic load to enhance cardiac output. Analysis of RV shape may thus provide a metric of compensation.
P3-77
3D Echo Provides a Common Language for LV Volume Measurement: An International Multicenter Study
Carly Jenkins1, Tsui-Lieh Hsu2, Jun Kwan3, Satoshi Nakatani4, Hao Wang5, Thomas H Marwick1
1University of Queensland, Woolloongabba, Australia; 2Veterans General hospital, Taipei, Taiwan Republic of China; 3University College of Medicine, Incheon, Republic of Korea; 4National Cardiovascular Center, Osaka, Japan; 5Beijing Fuwai Hospital, Beijing, China
Background: Standard two dimensional echo (2DE) has limited reproducibility for LV quantitation, so it is quite common for different laboratories to make different measurements without a change in a patient’s status. Recent single center studies have documented the reliability of realtime 3D (RT3D), which may be a solution to this problem. In a multicenter trial format we sought a) to validate RT3D against magnetic resonance imaging (MRI), b) to compare with 2D, and c) to examine the variability of LV measurements at multiple sites.Methods: Patients from 5 international sites (n=44) were studied with RT3D (Philips Sonos 7500). RT3D volumes and ejection fraction were measured in all studies at all sites (4D analysis, Tomtec Gmbh, Untersclessheim, Germany). In a subgroup (n=20), cardiac MRI images which were obtained using true FISP during breath-hold, and 3D volumes and EF were measured off-line.Results: MRI (EDV 155±62mls, ESV 84±42mls and EF 51±6%) correlated better with RT3D (EDV r=0.89*, ESV r=97*, EF r=0.91*) than 2DE(EDV r=0.69*, ESV r=0.86*, EF r=0.91*). The mean differences between MRI and 3D (EDV -17±39ml, ESV -37±54ml, EF -3±5%) were less than between MRI and 2DE (-53±52ml, ESV -31±41ml, EF -4±5%). There was high correlation between centers for all LV parameters (table).Conclusions: The validation of RT3D measurement of volumes and EF has been confirmed in this multicenter study. Semi-automated measurement of RT3D is a feasible approach to reduce variation of LV volume and EF measurements between centers.
Table 1. p<0.01*n=44 Mean ± SD Correlation ranges between sites Diff from Mean ± SDEDV (mls) 136±32 r=0.79*-0.96* -3±12ESV (mls) 73±27 r=0.83*-0.97* -1±5EF (%) 50±7 r=0.54*-0.98* -1±3
P3-78
Mitral Annulus Dynamic Tracking and Evaluation from Real Time 3D Echocardiographic Data
Federico Veronesi1, Cristiana Corsi1, Enrico G Caiani2, Roberto M Lang3, Claudio Lamberti1
1University of Bologna, Bologna, Italy; 2Polytechnic of Milan, Milan, Italy; 3University of Chicago Medical Center, Chicago, IL
Background: The analysis of the mitral annulus (MA) shape is an important determinant for the evaluation of several pathologies. In particular, mitral regurgitation caused by ischemia and idiopathic dilated cardiomyopathy could be evaluated assessing quantitative parameters such as mitral annulus area. Using 2D echocardiography, these parameters are usually evaluated by manual tracing from different views (apical 2- and 4-chambers views), and in case of the mitral valve area also by geometric modeling (by assuming an elliptic planar shape for the MA). Recently, real-time 3D echocardiographic (RT3DE) data have been utilized to quantify the MA shape; however, static measurements were manually obtained by multiple rotational 2D views, excluding dynamic analysis of shape changes. Our goal was to develop a semi-automated tool for MA reconstruction in the 3D space and tracking throughout the cardiac cycle, thus exploiting all the information contained in the dataset and allowing more accurate and less subjective 3D-derived measurements. Comparison of the obtained indices between normal (N) and dilated cardiomyopathy (DCM) patients was performed to evaluate clinical significance of the computed indices.Methods: RT3DE (Philips 7500, X4 probe, apical view) datasets acquired from 16 patients (10 N, 6 DCM) were analyzed using custom software. First, the MA is manually identified on the end-diastolic (ED) frame by selecting the points corresponding to its contour in 8-10 rotational planes. Then, an algorithm based on optical flow, which takes into account the presence of speckle noise in the data, is applied in order to perform an automated tracking of the MA position throughout the cardiac cycle. Finally, for each frame i, a 3D surface representing the MA shape is derived, from which MA surface area (MASA) is computed, and MASA change (MASAC) calculated as 100*(MASA(ED)-MASA(i))/MASA(ED).Results: Analysis of a single RT3DE data set required <3 min including MA initialization and tracking. In N, the ED MASA was found significantly (p<0.01, t-test) smaller than in DCM (6.48±3.18 cm2 and 9.29±3.47 cm2, respectively). The maximum value of MASAC resulted in correspondence of the mitral valve opening as expected and it was significantly greater in N than in DCM (58.5% and 22.6%, respectively) (p<0.01).Conclusion: This study shows that semi-automated dynamic tracking and analysis of MA shape on RT3DE datasets is feasible. Moreover, from the detected 3D MA surface, it is possible to extract classical as well as new parameters that could potentially discriminate between normal and pathological condition.
Journal of the American Society of Echocardiography638 Abstracts May 2006

P3-79
A Novel Quantitative Three-Dimensional Wall Motion Analysis of Contrast Enhanced Real-Time Three-Dimensional Dobutamine Stress Echocardiography
Susan L Herz, Todd C Pulerwitz, Yukio Abe, Kazue Okajima, Andrew F Laine, Marco R Di Tullio, Shunichi Homma, Jeffrey W Holmes Columbia University, NY, NY
Background: Qualitative left ventricular (LV) wall motion analysis is subject to large inter-observer variability. In this study, we developed a novel three-dimensional (3D) analysis technique to quantify wall motion in real-time 3D dobutamine stress echocardiography. We compared results from our quantitative automated computer analysis to standard 16-segment wall motion scores of two experienced cardiologists.Methods: 14 3D full volume echocardiograms (Philips Sonos 7500) were obtained from 7 patients at rest and at peak dobutamine infusion (PDI) with contrast enhancement. Cardiologists agreed on wall motion scores assigning a 1 for normal wall motion, 1.5 for mild, 2 for moderate, 2.5 for severe hypokinesis, 3 for akinesis and 4 for dyskinesis. The LV endocardial border was manually traced and regional 3D fractional shortening (3DFS) calculated as the fractional change in 3D radial coordinate from end-diastole to end-systole in each of the 16 standard LV segments. 3DFS >25% was defined as normal wall motion, 20% - 25% as mild hypokinesis, 10% - 20% as moderate hypokinesis, 5% - 10% as severe hypokinesis, 0% - 5% as akinesis, and < 0% as dyskinesis.
Results: Wall motion was successfully quantified for all 14 data sets. Time required per data set was 40 minutes for manual tracing plus 5 minutes for quantitative analysis. 96% of segments were considered adequate for assessment by the cardiologists. The cardiologists scored 86% of segments as normal, 13% as hypokinetic, and 1% as akinetic. By comparison, quantitative analysis resulted in 80% of the visible segments classified as normal, 14% hypokinetic, 4% akinetic, and 2% dyskinetic. The percentage of segments in which cardiologist and quantitative scores
agreed (0.5 or less difference in score) was 85%. 8 studies (3 rest, 5 PDI) had >85% agreement (2 or less segments disagreed), 4 studies (3 rest, 1 PDI) had 75% - 85% agreement, and 2 studies (1 rest, 1 PDI) had <75% of segments in agreement.Conclusions: Quantification of 3DFS by this novel 3D analysis technique is feasible. There was excellent concordance with cardiologists’ analysis. This method may provide a more objective, quantitative and rapid approach to evaluating segmental wall motion and function once integrated with an automated endocardial border detection algorithm.
P3-80
Left Ventricular Dyssynchrony Assessment: Comparison of 3D Real Time Echocardiography Using Semi-Automatic Quantification and Tissue Doppler Imaging in Four Groups of Patients
Eric Saloux1, Philippe Pon Gabrielsen1, Pascal Allain2, Olivier Gerard2, Arnaud Pellissier1, Fabien Labombarda1
1University Hospital, Caen, France; 2Philips Medical Systems Research, Suresnes, France
Background Left ventricular mechanical dyssynchrony (LVMD) is frequently observed in patients with non-ischemic dilated cardiomyopathy (NIDC) and complete left bundle branch block (LBBB). It is not well established if dyssynchrony is essentially secondary to systolic dysfunction or intraventricular conduction disturbances.Objective Impact of LVEF and LBBB on echocardiographic indexes of LVMD including tissue Doppler imaging (TDI), strain imaging (SI) and 3D real-time echocardiography (3DRTE).Methods 42 patients (12 controls, 8 patients with isolated LBBB, 12 patients with NIDC and narrow QRS complex, 10 patients with NIDC and LBBB) were included. All patients were in sinus rhythm. TDI, SI and 3DRTE were performed with Sonos 7500 and Ie33 (PHILIPS®). Acquisitions were performed in the apical 4, 2, and 3 chamber views. Philips QLab prototype was usedfor analysis of 3D data. The following parameters were measured off-line in each of the 12 nonapical segments: time to myocardial contraction onset (To), time to myocardial contraction peak (Tp), time to peak systolic strain (Tε) and time to minimal systolic 3DRT volume (3DTmsv). Dyssynchrony indexes were calculated from each of these parameters as the standard deviation (SD) and the maximal difference (Dif). LVEF was measured by 3DRT. ANOVA with repeated measures was used for comparisons of Doppler and 3D variables in # subgroups (LVEF, LBBB, segments). Correlations were performed with linear regression and Pearson’s coefficient.Results We found a significant effect of LVEF on To_Dif and To_SD (p=.0004), Tε_Dif (p=.0032) and Tε_SD (p=.004), Tmsv_Dif and Tmsv_SD (p<.0001), but not any significant effect of LBBB on these indexes. The number of segments for indexes calculation as a significant effect on the Dif values, Tε_SD and 3D_Tmsv_SD. A good correlation is found between Tε_SD and 3DTmsv_SD over 12 segments (R = 0.7), and a logarithmic correlation is found between LVEF and 3D Tmsv_SD (|R|=0.6).Conclusions In our study 3DRTE seems to be a new interesting tool to identify patients with LVMD independent of the QRS duration and 3DRTE dyssynchrony and Strain indexes have acceptable correlation.
P3-81
Relation between Left Ventricular Diastolic Function and Morphological Changes of the Left Atrial Volume During the Cardiac Cycle Using Real Time 3D Echocardiography
Yasuyoshi Takei, Nobihiro Tanaka, Saiko Kurohane, Nori Takahashi, Kenji Takazawa, Akira Yamashina Tokyo Medical University, Tokyo, Japan
Background: Although, it has been reported that the left atrial volume increases with the severity of left ventricular (LV) diastolic dysfunction, the relation between LV diastolic function and the morphologic changes of LA volume during the cardiac cycle is still unknown.Objective: To morphologically analyze the changes of LA volume evaluated by real time 3D echocardiography during the cardiac cycle in comparison with LV diastolic function.Subjects: Thirty-three patients with sinus rhythm, but without mitral valve disease, pericardial disease and history of cardiac surgery.Methods: The LA volume at each cardiac phase was measured by full volume acquisitions of the apex on the 4 chamber view and 2 chamber view. The LA volume index (LAVI) was calculated from the body surface area. Patients were evaluated for LV diastolic functions based on their trans-mitral flow patterns and divided into four groups; normal (N), impaired LV relaxation (A), pseudo-normal (P) and restrictive (R) for comparative analysis.
Results: The LAVI was maximum (LAVImax) at end-systole and minimum (LAVImin) at end-diastole in all groups. There was no significant difference in the LAVImax between groups N and A and between groups P and R. In contrast, the LAVImax was significantly higher in group P than that in group A (p=0.03). The LAVImin was similar in groups N and A. Group P had a significantly higher LAVImin than group A
(p=0.0002), while the LAVImin of group R was significantly higher than that of group P (p=0.003). The rate of change in LAVI (r-LAV) decreased with the reduction in diastolic function (p=0.003 for N vs. A, p=0.04 for A vs. P and p=0.02 for P vs. R).Conclusion: The LA volume increased with the increasing severity of LV diastolic dysfunction, and its morphological changes decreased with the cardiac cycle.
P3-82
Left Atrial Volumetry by Real-Time Triplane Three-Dimensional Echocardiography: Comparative study with Two-Dimensional Echocardiography
Hiroko Kobayakawa, Kazuaki Tanabe, Junichi Kawai, Kazuto Yamaguchi, Toshikazu Yagi, Tomoko Tani, Shigefumi Morioka, Yasuki Kihara Kobe General Hospital, Kobe, Japan
Background: Since the left atrial (LA) size has been recognized as a critical determinant in a variety of cardiac diseases that show the ventricular diastolic dysfunction, more accurate measurement of LA volume is required in the clinical settings. In this study we tested feasibility and reliability of a new, real-time triplane 3DE to measure LA volume and compared the measures to those from 2DE, which present the current standard.Methods: To test the volumetric reliability of 3DE (Vivid7 Dimension, GE Yokogawa Medical) in vitro, 11 water-filled (36 to 320ml) latex balloon phantoms with various shapes were used. For in vivo study, we studied 52 patients by 2DE and real-time triplane 3DE. LA volume by 3DE was calculated from the geometric method, using simultaneously collected equally spaced 3 tomograms (by increments of 60 degrees) from the apical window. LA volume by 2DE was calculated by the modified single-plane (4-chamber and 2-chamber) and bi-plane Simpson’s rule. In addition, LA antero-posterior dimension (LAD) was measured by 2DE.Results: In vitro study, there was a high correlation and good agreement (y=1.0x-3.3(ml), r=0.99, p<0.0001) between the true volume and the estimated volume by 3DE. In patients, LA volume by 3DE ranged from 36 to 199 mL (79±35 mL). These 3DE measures were tightly correlated to any types of LA measures by 2DE. However there were consistent underestimations by 2DE-derived data (biplane: y=0.72x + 13.0, r=0.88, bias=-13.7 mL, single-4 chamber: y=0.68x + 14.1, r=0.81, bias=-16.3 mL, single-2 chamber: y=0.77x + 13.2, r=0.85, bias=-14.3 mL). Besides, while LAD had a statistically significant correlation with 3DE-derived volume, the correlation was not satisfactory (y=0.016x+2.5, r=0.79).Conclusions: The 3DE-derived LA measures provide more accurate data of the actual LA volume. The current standard, LAD, is quite unreliable. In addition, LA volume by 2DE underestimates the volume by 23-32%.
Journal of the American Society of EchocardiographyVolume 19 Number 5 Abstracts 639