powerpoint presentation · insulin 35 inhaled insulin •inhaled insulin—afrezza® regular...
TRANSCRIPT

4/1/2016
1
1
What’s New in Diabetes Medications
Jena Torpin, PharmD
2
• Discuss new medications in the management of diabetes
• Understand the mechanism of the medications discussed
• Understand the side effects of the medications discussed
Objectives
Acknowledgement: Some slides adapted/used with permission from
Dr. Heather Blue’s Presentation, Diabetes Medication Update, 3/5/2015
3
•Types of Diabeteso Type 1: complete insulin deficiencyo Type 2: decreased insulin secretion & insulin resistance
Review of Diabetes
Cefalu, Diabetes Care, 2016; Khardori R, www.Medscape.org, 2015
Hepatic Glucose Production
Peripheral Glucose Uptake
Pancreatic Insulin secretion
Blood
Glucose

4/1/2016
2
4
Review of Diabetes- Diagnosis
Test Dx Criteria
Fasting Plasma Glucose (FPG) ≥ 126 mg/dL
2 Hour Plasma Glucose ≥ 200 mg/dL
A1C ≥ 6.5%
Random Glucose ≥ 200 mg/dL + symptoms of
hyperglycemia/crisis
Cefalu, Diabetes Care, 2016; Khardori R, www.Medscape.org, 2015
5
Review of Diabetes-Goals
Patient population A1C Goal (%)
Most adults (non-pregnant) ≤ 7
Select patients (low risk for hypoglycemic events) ≤ 6.5
Select patients (high risk for hypoglycemic events,
advanced age, vascular complications)
≤ 8
Cefalu, Diabetes Care, 2016
6
Review of Diabetes- Treatment of Type 2 Diabetes
2nd Line1st Line
Metformin
Oral Agent
GLP-1 Analog
Insulin
• Sulfonylurea
• Thiazolidinedione
• DPP-4 Inhibitor
• SGLT2 Inhibitor
Cefalu, Diabetes Care, 2016

4/1/2016
3
7
•Metformin•Sulfonylureas•Thiazolidinediones•Insulin•Meglitinides•Alpha-glucosidase inhibitors
7
Previous Toolbox
8
•Effectiveness: Decreases A1C by 1-1.5%
•Dosing: titrate to goal 1000mg BID or 2000mg qday if ER
•Adverse Drug Events: GI Side (need to titrate/take with food), Vitamin B12 deficiency, lactic acidosis (rare)
•Cost: $4 list
8
Previous Toolbox- Biguanide (Metformin)
Hepatic Glucose
Production
Insulin Sensitivity•Mechanism:
Cefalu, Diabetes Care, 2016; UpToDate; Bahal O’Mara, Pharmacist’s Letter, 2015
9
•Mechanism of Action: pancreatic release of insulin
•Effectiveness: Decreases A1C by 1-1.5%
•Dosing: Start low and go slow in elderly patients and those with hepatic or renal disease
•Adverse Drug Events: hypoglycemia
•Cost: $4 list
9
Previous Toolbox- Sulfonylureas (Glyburide, Glipizide, Glimepiride)
Cefalu, Diabetes Care, 2016; Bahal O’Mara, Pharmacist’s Letter, 2015

4/1/2016
4
10
•Mechanism of Action: Increased insulin sensitivity
•Effectiveness: Decreases A1C by 1-1.5%
•Dosing: titrate cautiously- monitor for signs of heart failure
•Adverse Drug Events: Edema, heart failure, fractures, increased LDL (rosiglitazone)
•Cost: Low
10
Previous Toolbox- Thiazolidinediones (TZDS- Pioglitazone, Rosiglitazone)
Cefalu, Diabetes Care, 2016; Bahal O’Mara, Pharmacist’s Letter, 2015; UpToDate
1111
Previous Toolbox-Insulin
Micromedex, Lexicomp, UpToDate
1212
Previous Toolbox-Insulin Profiles
Micromedex, Lexicomp, UpToDate

4/1/2016
5
1313
Previous Toolbox
Metformin Sulfonylurea TZD Insulin
Efficacy/A1C
reduction
High: 1-1.5% High: 1-1.5% High: 1-1.5% Highest: 1.5-
3.5%
Hypoglycemia
Risk
Low Moderate Low High
Weight Neutral Gain Gain Gain
Side Effects GI, lactic
acidosis (rare)
Hypoglycemia Edema, Heart
failure,
fractures
Hypoglycemia
Costs Low- $4 list Low- $4 list Low Variable
Cefalu, Diabetes Care, 2016; Bahal O’Mara, Pharmacist’s Letter, 2015
14
• Sodium-glucose cotransporter 2 (SGLT2) Inhibitors
• Dipeptidyl pepidase-4 (DPP-4) Inhibitors (gliptins)
• Injectable glucagon-like peptide 1 (GLP-1) receptor agonists
• New insulin formulations-Inhaled insulin-New concentrations
New Diabetes Medications
Sodium Glucose
Co-Transporter 2
Inhibitors
15

4/1/2016
6
16
•Drugs:o canagliflozin (Invokana®)o dapagliflozin (Farxiga®)o empagliflozin (Jardiance®)
•Mechanism: Prevents glucose from being reabsorbed by kidneys, resulting in glucose loss into urine
16
Sodium-glucose transporter 2
inhibitors
Cefalu, Diabetes Care, 2016; Bahal O’Mara, Pharmacist’s Letter, 2015; UpToDate
17
•Reduced A1c by 0.5-1% points
•Weight loss seen in trials (up to 4.5 kg)
•Reduction of blood pressure (up to 7 mmHg)
•No hypoglycemia
•Decreased CVD events/mortality in pt’s with CVD
17
Effectiveness of SGLT2 Inhibitors
Cefalu, Diabetes Care, 2016; Bahal O’Mara, Pharmacist’s Letter, 2015; Nauck, Drug Des Devel
Ther, 2014
1818
Dosing of SGLT2 Inhibitors
canagliflozin dapagliflozin empagliflozin
Usual adult dose
GFR >60
mL/min/1.73 m(2)
100mg
300mg daily
5mg 10mg
daily
10mg 25mg
daily
GFR 45-60
mL/min/1.73 m(2)
Limit dose at
100mg daily
Do not use 10mg 25mg
daily
GFR <45
mL/min/1.73 m(2)
Do not use Do not use Do not use
Micromedex
4/1/2016
7
19
•Urinary tract infections (~5%)•Genital infections (up to ~11%)•Renal impairment•Polyuria (~5%)•Hypovolemia•Increased LDL•Bladder cancer?
19
Adverse Effects of SGLT2 Inhibitors
Cefalu, Diabetes Care, 2016; Bahal O’Mara, Pharmacist’s Letter, 2015; Micromedex, UpToDate
Dipeptidyl
Peptidase-4
Inhibitors
20
21
Dipeptidyl Peptidase-4 Inhibitors
•Drugs:o sitagliptin (Januvia®)o saxagliptin (Onglyza®)o linagliptin (Tradjenta®)o alogliptan (Nesina®)
•Mechanism: Inhibit dipeptidyl peptidase-4 which is an enzyme which breaks down endogenous incretins o e.g. glucagon like peptide 1 (GLP-1)
Cefalu, Diabetes Care, 2016; Bahal O’Mara, Pharmacist’s Letter, 2015

4/1/2016
8
22
Insulin Secretion/Synthesis
Glucagon secretion
Henry RR, www.medscape.org, 2009
Endogenous Incretin Mechanism of Action
23Image: Adapted from Henry RR, www.medscape.org, 2009
24
•Reduced A1C by 0.5-1%; some believe to more around ≤ 0.7%
•No hypoglycemia (monotherapy)
•Weight neutral
24
Effectiveness of DPP-4 Inhibitors
Cefalu, Diabetes Care, 2016; Bahal O’Mara, Pharmacist’s Letter, 2015

4/1/2016
9
2525
Dosing of DPP-4 Inhibitors
sitagliptin saxagliptin linagliptin alogliptin
Usual dose 100 mg daily 2.5-5 mg daily 5 mg daily 25 mg daily
Renal CrCl 30-50
50 mg daily
CrCl <30 25
mg daily
CrCl
<50ml/min
2.5 mg daily
No
adjustments
needed
30-60
12.5 mg daily
<306.25 mg
daily
UpToDate
26
•Potential for pancreatitis
•May increase risk of hospitalizations due to heart failure
•Immune –mediated dermatological/angioedema side effects
26
Adverse Effects of DPP4-Inhbitors
Cefalu, Diabetes Care, 2016; Bahal O’Mara, Pharmacist’s Letter, 2015
27
Glucagon-Like
Peptide-1 (GLP-1)
Agonist
4/1/2016
10
28
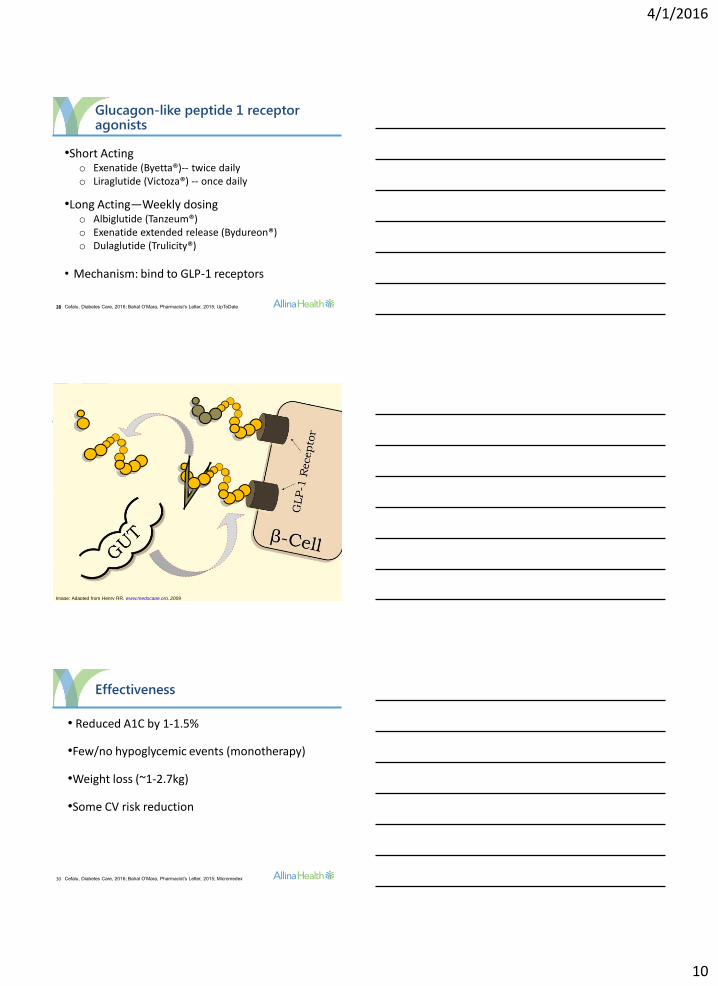
•Short Actingo Exenatide (Byetta®)-- twice dailyo Liraglutide (Victoza®) -- once daily
•Long Acting—Weekly dosingo Albiglutide (Tanzeum®) o Exenatide extended release (Bydureon®) o Dulaglutide (Trulicity®)
• Mechanism: bind to GLP-1 receptors
28
Glucagon-like peptide 1 receptor agonists
Cefalu, Diabetes Care, 2016; Bahal O’Mara, Pharmacist’s Letter, 2015; UpToDate
29Image: Adapted from Henry RR, www.medscape.org, 2009
30
Effectiveness
• Reduced A1C by 1-1.5%
•Few/no hypoglycemic events (monotherapy)
•Weight loss (~1-2.7kg)
•Some CV risk reduction
Cefalu, Diabetes Care, 2016; Bahal O’Mara, Pharmacist’s Letter, 2015; Micromedex

4/1/2016
11
31
Dosing
Exenatide Liraglutide
Usual dose 5 mcg 10 mcg SubQ BID 0.6 mg 1.2-1.8mg SubQ
qday
Renal CrCl 30-50 mL/min: use caution
CrCl <30 mL/min: not recommended
No adjustment needed
Exenatide (extended
release)
Albiglutide Dulaglutide
Usual
dose
2mg SubQ qWeek 30 mg 50 mg SubQ
qWeek
0.75mg 1.5mg
SubQ qWeek
Renal CrCl 30-50 mL/min: use
caution
CrCl <30 mL/min: not
recommended
No adjustments needed No adjustment
needed (use with
caution)
UpToDate,
32
•Boxed warning: thyroid C-cell tumors
•GI Side Effects: Nausea/vomiting/diarrhea: 10-50%
•Potential for pancreatitis
•Renal dysfunction
•Injection site reactions
32
Adverse effects of Glucagon-like peptide 1 receptor agonists
Cefalu, Diabetes Care, 2016; Bahal O’Mara, Pharmacist’s Letter, 2015; Micromedex
33
New Diabetes Medications
DPP-4 Inhibitor SGLT2 Inhibitor GLP-1 Receptor Agonist
Efficacy/A1C
reduction
Intermediate: 0.5-
1%
Intermediate: 0.5-
1%
High: 1-1.5%
Hypoglycemia
Risk
Low Low Low
Weight Neutral Loss Loss
Side Effects Rare Genitourinary,
dehydration
GI
Costs High High High
Cefalu, Diabetes Care, 2016; Bahal O’Mara, Pharmacist’s Letter, 2015

4/1/2016
12
34
Insulin
35
Inhaled Insulin
•Inhaled insulin—Afrezza® regular insulin•4 unit, 8 unit, and 12 unit cartridges
•Dosing:
•Side Effects: hypoglycemia, cough, throat pain
Afrezza®, Prescribing Information, 2014
Injected Prandial Insulin Afrezza Dose
Up to 4 units 4 units
5-8 units 8 units
9-12 units 12 units
13-16 units 16 units
17-20 units 20 units
21-24 units 24 units
36
•Lispro (Humalog KwikPen): 200 units/mL
•Glargine (Toujeo SoloStar): 300 units/mL
•Degludec (Tresiba FlexTouch): 100 units/mL &
200 units/mL
•Degludec/aspart 70/30 (Ryzodeg 70/30): 100
units/mL
36
Other/New Insulin Formulations
UpToDate

4/1/2016
13
37
Take Away Points
•Many new medications with novel mechanisms
•Mainstay of therapy while patients are in the hospital still remains insulin therapy
thank you!