powerpoint presentation - amazon web...
TRANSCRIPT

3/28/2016
1
Peter Hollmann MD
Past CPT Panel Chair
Evaluation and Management – Emerging Trends
© 2016 American Medical Association. All rights reserved.
Disclosures
• Ambassador for AMA CPT
• Member RBRVS Update Committee
2
Evaluation and
Management
3 © 2016 American Medical Association. All rights reserved.
Evaluation and Management – The History
• Created for CPT 1992
– CPT E/M Guidelines, Preventive Medicine Codes also 1992
• 1995 HCFA Documentation Guidelines
• 1997 HCFA Documentation Guidelines
• E/M Workgroup 2002-2004
• Rise of Electronic Records
• Recognition Non Face to Face and Team Care
• Care Management and PCMH
• Medical Decision Making 2014
4
© 2016 American Medical Association. All rights reserved.
E/M - The reality
• 2010 total Part B spend $110B
• 2010 Part B on E/M $33.5B
• A substantial portion of “surgical” procedures is unreported E/M
– Actual post op visits or similar services in pre/post time
• Used by all specialties (almost) and non physician professionals
• Due to budget neutrality any change in E/M will be paid for from E/M
• Intra-specialty consistency vs. inter-specialty consistency
• Fundamental structure is single problem focused H+P – the Medical Student Approach to Coding
5 © 2016 American Medical Association. All rights reserved.
2012 PFS Proposed Rule (July 2011)
6
3/28/2016
2
© 2016 American Medical Association. All rights reserved.
Professional Response
• Meet with CMS to better understand request and educate
• Recognize established codes (e.g., warfarin management)
• Recognize monthly fee for PCMH
• CPT/RUC will create/value codes that address non F2F time and care
management
• Discussed only and not proposed – Revise E/M
– Acute care
– Chronic care
– Post op global care
7 © 2016 American Medical Association. All rights reserved.
Goals of New Services
• Recognize work and practice expense of chronic care management
– Non F2F
– Electronic Records
– Advanced Primary Care
– Team care and efficient practice at the top of the license
– Patient/caregiver involvement
• Stimulate transformation of the delivery system
• Primary Care orientation without creating specialty specific codes
8
© 2016 American Medical Association. All rights reserved.
B Status
• 99339-99340 CPO (other than homecare, hospice, NF) – 2006
• 99358-99359 Prolonged Services Non F2F – 1999
• 99363-99364 Anticoagulant Management – 2007
• 99336-99368 Medical Team Conferences – 2008
• 99379-99380 CPO Nursing Facility – 1999
• 99441-99443 Telephone – 2008
• 99444 On-line – 2008
• 99446-99449 Interprofessional Consultation – 2014
• 99487-99489 Complex Chronic Care Management - 2013
9 © 2016 American Medical Association. All rights reserved.
Medicare Statutory Benefit and Other E/M like Codes
• Welcome to Medicare Physical (G0402)
• Annual Wellness Visit (G0438-G0439)
• Preventive Services Screening/counseling (many G codes)
• CPO Home Care and Hospice (G0181-G0182)
• Certification/recertification of home care (G0179-G0180)
10
© 2016 American Medical Association. All rights reserved.
New Paid Services Since Proposed PFS 2012 Rule
• 99495-99496 Transitional Care Management – 2013
• 99490 Chronic Care Management – 2015
• 99497-99498 Advance Care Planning – 2016
• 99415-99416 Prolonged Professional Staff Services - 2016
11
Evolving Concepts
12
3/28/2016
3
© 2016 American Medical Association. All rights reserved.
2016 PFS Proposed Rule
13 © 2016 American Medical Association. All rights reserved.
2016 PFS Proposed Rule
14
© 2016 American Medical Association. All rights reserved.
2016 PFS Proposed Rule
15 © 2016 American Medical Association. All rights reserved.
Under Consideration
• Dementia Assessment
– Guideline driven, quality measure, E/M does not describe service adequately
• CCM based on Professional Time
– CPO when not HH or Hospice (or CCM is N/A or less favorable)
• Non F2F Acute Care Episodes
– NF and home/dom/ALF
• Principle Care CCM
– CCM without two or more conditions, not PCP
• MTM in a physician/QHCP office
– Using pharmacists outside of Part D
• Behavioral Health Co-Management/Assistance
– Community Based Consult Services applied to PCMH embedded MH clinicians
• Unusual Complexity E/M add-on
16
Putting Newer
Codes into Practice
17 © 2016 American Medical Association. All rights reserved.
Newer Services – Coding and Tips
• TCM
• CCM
• Advance Care Planning
• Prolonged Clinical Staff Services
18
3/28/2016
4
Transitional Care
Management
19 © 2016 American Medical Association. All rights reserved.
TCM - New in Final Rule 2016
20
© 2016 American Medical Association. All rights reserved.
TCM – The Patient
• DISCHARGE FROM
– IP Acute Care Hospital
– IP Psychiatric Hospital
– LTC Hospital
– SNF
– IP Rehab Facility
– Hospital Outpatient OBS or
Partial Hospital
– Partial Hospital at CMHC
• DISCHARGE TO
– Home
– Domiciliary
– Rest Home
– Assisted Living Facility
21 © 2016 American Medical Association. All rights reserved.
Required Services
• Interactive Contact
– Within 2 business days: F2F, phone, e-mail
– Must make 2 attempt within 2 business days
• Certain Non Face to Face Services
– Necessary services for transition (eg record review, care coordination)
• A face to face visit
– Within 14 days
– Medication Reconciliation required by required F2F date
22
© 2016 American Medical Association. All rights reserved.
TCM Rules
• 30 days (Date of Discharge is Day#1)
• First F2F visit is not reported separately; additional E/M may be
reported
• Only one professional may report
• Not to be reported by professional who is providing services within a
global period
• The discharge day services may not constitute the initial F2F visit
• May not report Certification (G0179-G0180), CPO (G0181-G0182), or
ESRD (90951-90970)
23 © 2016 American Medical Association. All rights reserved.
TCM – Code Selection
24
3/28/2016
5
© 2016 American Medical Association. All rights reserved.
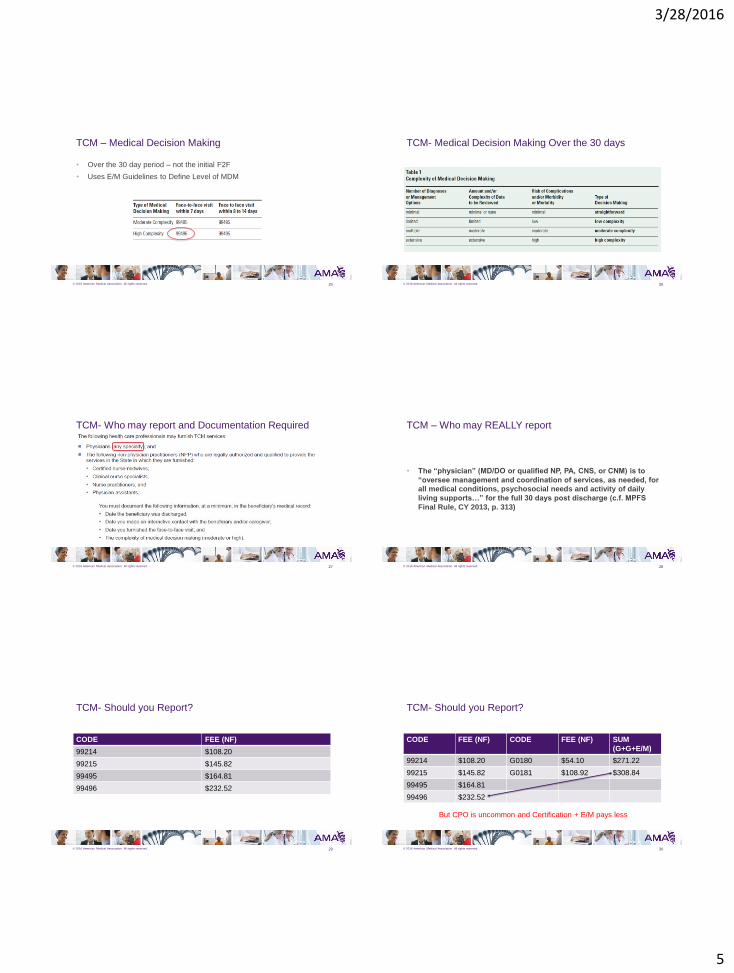
TCM – Medical Decision Making
• Over the 30 day period – not the initial F2F
• Uses E/M Guidelines to Define Level of MDM
25 © 2016 American Medical Association. All rights reserved.
TCM- Medical Decision Making Over the 30 days
26
© 2016 American Medical Association. All rights reserved.
TCM- Who may report and Documentation Required
27 © 2016 American Medical Association. All rights reserved.
TCM – Who may REALLY report
• The “physician” (MD/DO or qualified NP, PA, CNS, or CNM) is to
“oversee management and coordination of services, as needed, for
all medical conditions, psychosocial needs and activity of daily
living supports…” for the full 30 days post discharge (c.f. MPFS
Final Rule, CY 2013, p. 313)
28
© 2016 American Medical Association. All rights reserved.
TCM- Should you Report?
CODE FEE (NF)
99214 $108.20
99215 $145.82
99495 $164.81
99496 $232.52
29 © 2016 American Medical Association. All rights reserved.
TCM- Should you Report?
CODE FEE (NF) CODE FEE (NF) SUM
(G+G+E/M)
99214 $108.20 G0180 $54.10 $271.22
99215 $145.82 G0181 $108.92 $308.84
99495 $164.81
99496 $232.52
30
But CPO is uncommon and Certification + E/M pays less
3/28/2016
6
© 2016 American Medical Association. All rights reserved.
TCM Resource (ICN 908628 - June 2013)
31
This publication notes
billing on Day 30
Chronic Care
Management
32
© 2016 American Medical Association. All rights reserved.
Chronic Care Management
• TCM and CCM codes created by CPT for 2013
• Medicare accepts TCM and CCM is “B” status
• 2014 Fee Schedule CMS proposes paying a single G code for CCM of 20 minutes or more in a 30 days period, for persons with 2 or more chronic conditions
• Lots of other issues included, eg PCMH and EMR certification and no link to a face to face service
• Apparent goal was high volume, low dollar payments for a large proportion of beneficiaries
• CPT responds with “Medicare code” 99490
• Value $42
33 © 2016 American Medical Association. All rights reserved.
Chronic Care Management
34
© 2016 American Medical Association. All rights reserved.
CCM and Complex CCM
CODE 99490 99487
# Chronic Conditions >2 >2
Duration of Conditions 12 months or until death 12 months or until death
Clinical Staff Time > 20 minutes > 60 minutes
Period of service Calendar Month Calendar Month
Comprehensive Care
Plan
Established, implemented,
revised or monitored
Established or substantial
revision
MDM No requirement Moderate or High
Medicare Payment $40.84 B Status
35 © 2016 American Medical Association. All rights reserved.
CCM- Who Qualifies
36
3/28/2016
7
© 2016 American Medical Association. All rights reserved.
Role of Physician or QHCP
• Oversees the management and/or coordination of services, as needed, for:
• All medical conditions,
• Psychosocial needs and
• Activities of daily living
• Incident to
• By appropriately qualified clinical staff
• Or personally by provider
37 © 2016 American Medical Association. All rights reserved.
CCM Services
38
© 2016 American Medical Association. All rights reserved.
CCM Services
39 © 2016 American Medical Association. All rights reserved.
CCM – Care Plan
40
© 2016 American Medical Association. All rights reserved.
CCM- Practice Requirements
41 © 2016 American Medical Association. All rights reserved.
CCM – Initiation and Consent
42
3/28/2016
8
© 2016 American Medical Association. All rights reserved.
CCM- EMR Requirements
43 © 2016 American Medical Association. All rights reserved.
CCM- EMR Requirements
44
© 2016 American Medical Association. All rights reserved.
CCM- EMR Requirements
45 © 2016 American Medical Association. All rights reserved.
CCM - Restrictions
• Not in an Advanced Primary Care Demonstration Project – the Specific
Patient
• Not with other Care Management Service Codes for same time period
46
© 2016 American Medical Association. All rights reserved.
CCM Resource (ICN 909188 - May 2015)
47
Advance Care
Planning
48
3/28/2016
9
© 2016 American Medical Association. All rights reserved.
Advance Care Planning (99497-99498)
49 © 2016 American Medical Association. All rights reserved. 50
Advance Care Planning
• For CY 2016, CMS has changed assignment of CPT
codes 99497 and 99498 PFS status to indicator “A,”
(defined as: Active code).
• The presence of an “A” indicator does not mean that
Medicare has made a national coverage determination
regarding the service. Contractors remain responsible
for local coverage decisions in the absence of a
national Medicare policy.
• Medicare allowance is $85.99 and $74.88 for 99497
and 99498 respectively.
© 2016 American Medical Association. All rights reserved. 51
Advance Care Plan 2016 Final Rule
• Separately payable with AWV; use modifier -33 so
beneficiary has no cost sharing
• If done with AWV can also be a team service
• Also separately payable with E/M; use modifier -25 on
E/M (does not include Critical Care)
• CMS allows that the service be “incident to” with some
significant direct supervision
© 2016 American Medical Association. All rights reserved.
2016 Final Rule
52
© 2016 American Medical Association. All rights reserved.
ACP - additional points
• Standard CPT Time Rules (more than ½ way to midpoint)
• Do not count any time that was part of determining level of E/M as ACP
time
• Does not require execution of a legally recognized advance directive
• No predetermined frequency limits
• No specific special training/specialty restrictions
53
Prolonged Clinical
Staff Services
54

3/28/2016
10
© 2016 American Medical Association. All rights reserved. 55
Prolonged Services: New Codes 99415-99416
Prolonged Service Clinical Staff Services With Physician or
Other Qualified Health Care Professional Supervision
• New title and subsection guidelines
• New timed codes to identify prolonged clinical staff
time of one hour (99415) and each additional half hour
(99416).
• Reported for prolonged clinical staff services service
(beyond the typical E/M service time) during an
evaluation and management service
© 2016 American Medical Association. All rights reserved. 56
What has changed for Prolonged Services?
Prior to 2016, codes 99354 and 99355 were
the only codes that could be reported for prolonged services
provided face-to-face with the patient.
These services state that the physician or qualified health care
professional was providing the service.
The development of the new codes allows a method for reporting face-to-face services
that are not provided by the physician/QHP for things that only require
face-to-face observation by clinical staff under the supervision of a
physician /QHP.
Development of the new codes allow for
such reporting under specifically
noted circumstances.
© 2016 American Medical Association. All rights reserved. 57
Reporting 99415 and 99416
• The typical face-to-face time of the primary (ie physician/QHCP) service is used in defining when prolonged services time begins
• Less than 45 minutes of prolonged service is not reported separately
• When face-to-face time is noncontiguous, use only the face-to-face time provided to the patient by the clinical staff. Do not count time of CS providing other reported services (except the E/M).
• No more than 2 simultaneous patients
• Physician/QHCP must be present
• Do not report with physician/QHCP prolonged services codes
© 2016 American Medical Association. All rights reserved. 58
Prolonged Services: Example
99214 Office or other outpatient visit for the evaluation and management of an established patient, which
requires at least 2 of these 3 key components:
A detailed history;
A detailed examination;
Medical decision making of moderate complexity.
Counseling and/or coordination of care with other physicians, other qualified health care professionals, or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs.
Usually, the presenting problem(s) are of moderate to high severity. Typically, 25 minutes are spent face-to-face with the patient and/or family.
© 2016 American Medical Association. All rights reserved. 59
Prolonged Services: Example
• Prolonged services begins AFTER 25 minutes (typical time listed in 99214)
99214
• Code 99415 is not reported until at least 70 minutes total face-to-face clinical staff time has been performed
99415• Because 45
minutes of prolonged services must be performed beginning AFTER the typical time
• 25 + 45 = 70
Why?
© 2016 American Medical Association. All rights reserved. 60
Total Duration of Prolonged Services Table
Total Duration ofProlonged Services
Code(s)
less than 45 minutes Not reported separately
45-74 minutes(45 minutes - 1 hr. 14 min.)
99415 X 1
75-104 minutes(1 hr. 15 min. - 1 hr. 44 min.)
99415 X 1 AND 99416 X 1
105 or more(1 hr. 45 min. or more) 99415 X 1 AND 99416 X 2 or more
for each additional 30 minutes.
3/28/2016
11
© 2016 American Medical Association. All rights reserved. 61
Prolonged Services: Revised Codes and
Guidelines
Prolonged Services codes and guidelines have been revised and updated for consistency with instructions in the Psychotherapy guidelines and following code 90837.
These changes:
• Further define that codes 99354 and 99355 are prolonged evaluation and management and psychotherapy service(s) rather than just the generic prolonged “services”
• Refer to new codes 99415 and 99416 when reporting prolonged clinical staff services
© 2016 American Medical Association. All rights reserved.
Medicare Fee
CODE FEE
99415 $8.96
99416 $0.72
62
© 2016 American Medical Association. All rights reserved. 63