powerpoint presentation · –clinical practice improvement activities 15% ... asthma outcomes when...
TRANSCRIPT

10/24/2016
1
An Asthma Telehealth Program to Improve Adherence to Inhaled
Corticosteroid Therapy
11th Annual Nemacolin Asthma Conference
October 29, 2016
Andrew G Weinstein MD President, Asthma Management Systems
Disclosures
• National Institute Health
• Merck
• President Asthma Management Systems
Overview of Presentation
• The Importance of Adherence and Outcomes
• Asthma Adherence Management Model
• Application of Model: Case Example Steroid Phobia

10/24/2016
2
Asthma Treatment Mantra
Correct Diagnosis
Correct Treatment
Adherence to Treatment
Morbidity, Cost
QOL
Medical Reimbursement
ADHERENCE OUTCOMES
• Fee for service - - Prior to 2017
• Value / At Risk + + 2017 on
Merit-based Incentive Payment System
Four categories of clinician performance derive
Composite Performance Score (CPS)
– Quality 50%
– Advancing Care Information (formerly Meaningful Use) 25%
– Clinical Practice Improvement Activities 15%
– Resource Use 10%
10/24/2016
3
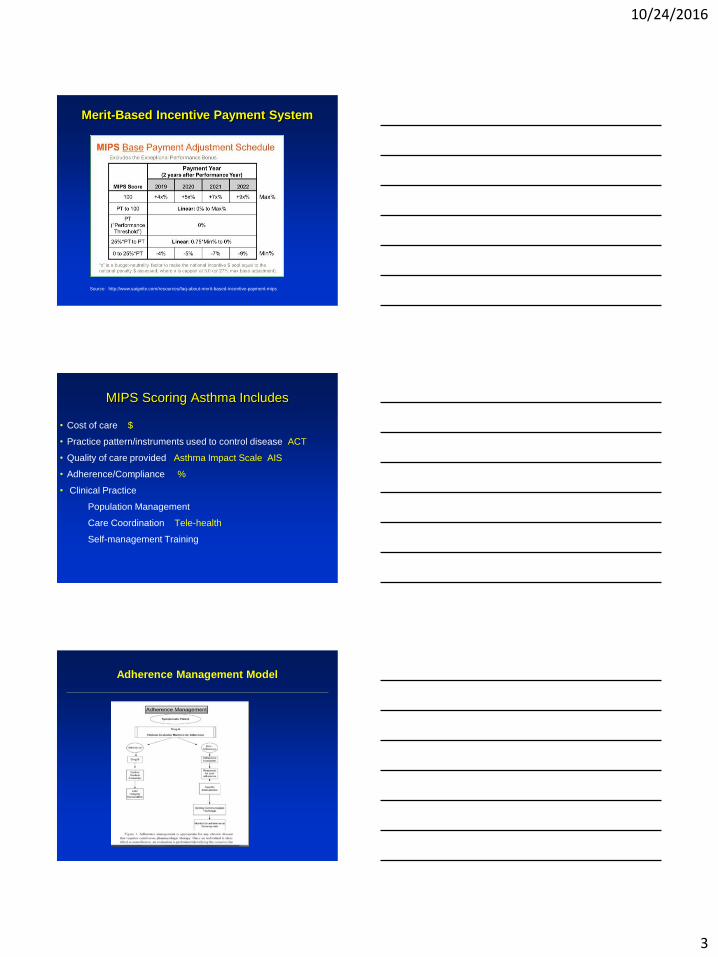
Merit-Based Incentive Payment System
Source: http://www.saignite.com/resources/faq-about-merit-based-incentive-payment-mips
MIPS Scoring Asthma Includes
• Cost of care $
• Practice pattern/instruments used to control disease ACT
• Quality of care provided Asthma Impact Scale AIS
• Adherence/Compliance %
• Clinical Practice
Population Management
Care Coordination Tele-health
Self-management Training
Adherence Management Model
10/24/2016
4
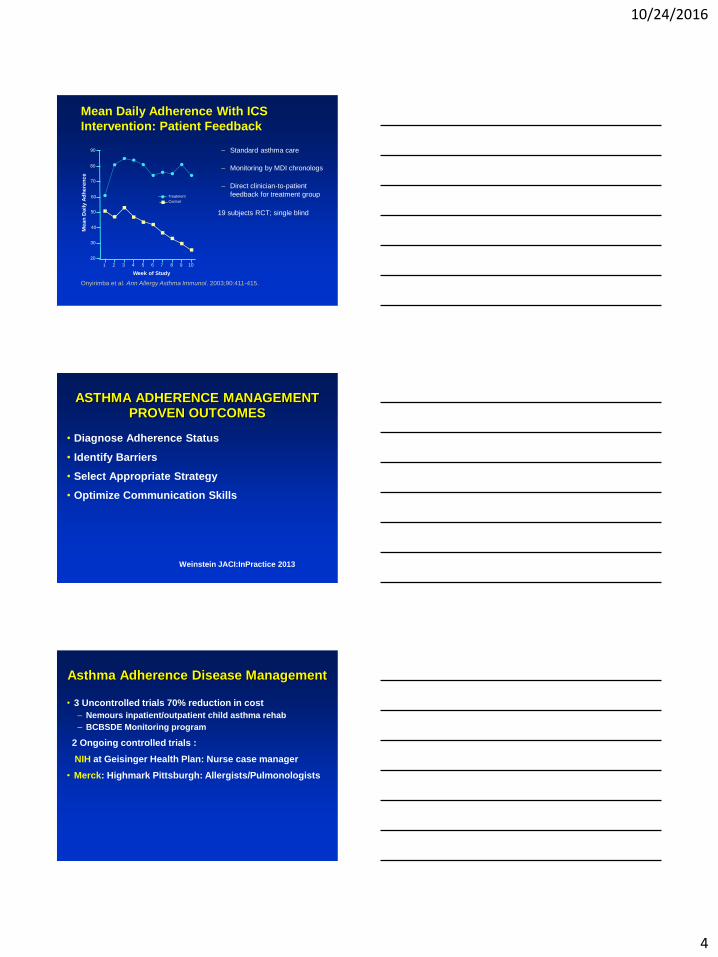
Mean Daily Adherence With ICS
Intervention: Patient Feedback
– Standard asthma care
– Monitoring by MDI chronologs
– Direct clinician-to-patient
feedback for treatment group
19 subjects RCT; single blind
Onyirimba et al. Ann Allergy Asthma Immunol. 2003;90:411-415.
1 2 3 4 5 6 7 8 9 10
20
30
40
50
60
70
80
90
Treatment
Control
Me
an
Da
ily
Ad
he
ren
ce
Week of Study
ASTHMA ADHERENCE MANAGEMENT PROVEN OUTCOMES
• Diagnose Adherence Status
• Identify Barriers
• Select Appropriate Strategy
• Optimize Communication Skills
Weinstein JACI:InPractice 2013
Asthma Adherence Disease Management
• 3 Uncontrolled trials 70% reduction in cost
– Nemours inpatient/outpatient child asthma rehab
– BCBSDE Monitoring program
2 Ongoing controlled trials :
NIH at Geisinger Health Plan: Nurse case manager
• Merck: Highmark Pittsburgh: Allergists/Pulmonologists
10/24/2016
5
Dulera Adherence Ongoing Study
• 40 persistent adult asthma 20 control/ 20 intervention
• Asthma Control Questionaire > 1.0
• 15 completed Intervention Asthma Adherence Pathway
– Identify barriers to adherence
– Clinical Decision Intervention/Motivational Interviewing
– Monitored Dulera Adherence at time of visit
• Mean Adherence Intervention group
• ACQ Initial 3 month Follow up
Control
Intervention
Solution: Asthma Adherence Pathway web-app(AAP™)
PATIENT PORTAL PROVIDER PORTAL
Patient login
Step 2: Patients self-identify barriers to Rx with validated survey
Provider login
Step 3: Clinicians identify hi-risk patients and respond with clinical decision support strategies
Survey data
• Extensive library of digital and video educational resources addresses barriers to adherence identified in survey
• Adherence strategies supported with robust guidelines and literature links
Provides analysis and objective monitoring: why patients don’t adhere to Rx
Step 1: Real time objective adherence monitoring (preventative/rescue)
Step 4: In-person and remote communications training: Shared- Decision-Making and Motivational interviewing
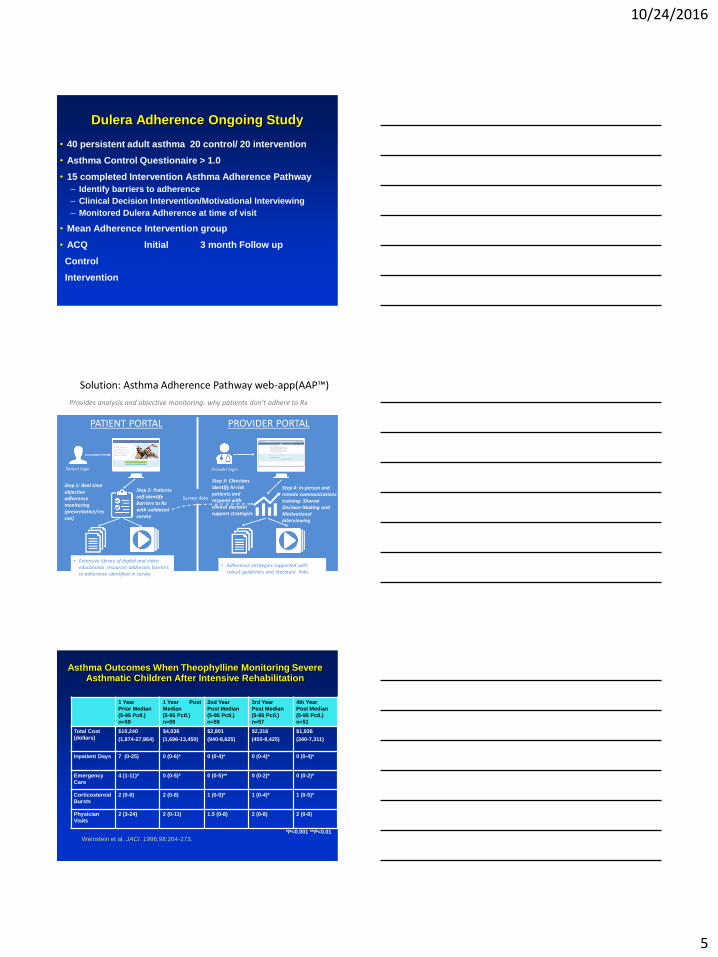
Asthma Outcomes When Theophylline Monitoring Severe Asthmatic Children After Intensive Rehabilitation
1 Year
Prior Median
(5-95 Pctl.)
n=59
1 Year Post
Median
(5-95 Pctl.)
n=59
2nd Year
Post Median
(5-95 Pctl.)
n=59
3rd Year
Post Median
(5-95 Pctl.)
n=57
4th Year
Post Median
(5-95 Pctl.)
n=51
Total Cost
(dollars)
$10,240
(1,874-27,964)
$4,036
(1,696-13,450)
$2,801
(940-8,625)
$2,316
(450-8,425)
$1,936
(340-7,311)
Inpatient Days 7 (0-25) 0 (0-6)* 0 (0-4)*
0 (0-4)*
0 (0-4)*
Emergency
Care
4 (1-11)*
0 (0-5)*
0 (0-5)**
0 (0-2)*
0 (0-2)*
Corticosteroid
Bursts
2 (0-9)
2 (0-8) 1 (0-5)* 1 (0-4)*
1 (0-5)*
Physician
Visits
2 (3-24) 2 (0-11) 1.5 (0-8) 2 (0-8) 2 (0-8)
*P<0.001 **P<0.01
Weinstein et al. JACI. 1996;98:264-273.
10/24/2016
6
ASTHMA ADHERENCE MANAGEMENT PROVEN OUTCOMES
• Diagnose Adherence Status
• Identify Barriers
• Select Appropriate Strategy
• Optimize Communication Skills
Weinstein JACI:IP 2013
Assessing Adherence Status
Methods
– Question the patient
– Evaluate patient diaries for completeness
– Ask patient to complete questionnaire
– Assess adherence based on response to treatment
– Conduct pill counts
– Use electronic monitors
– Determine prescriptions filled at pharmacy
– Blood/Urine
– Observation
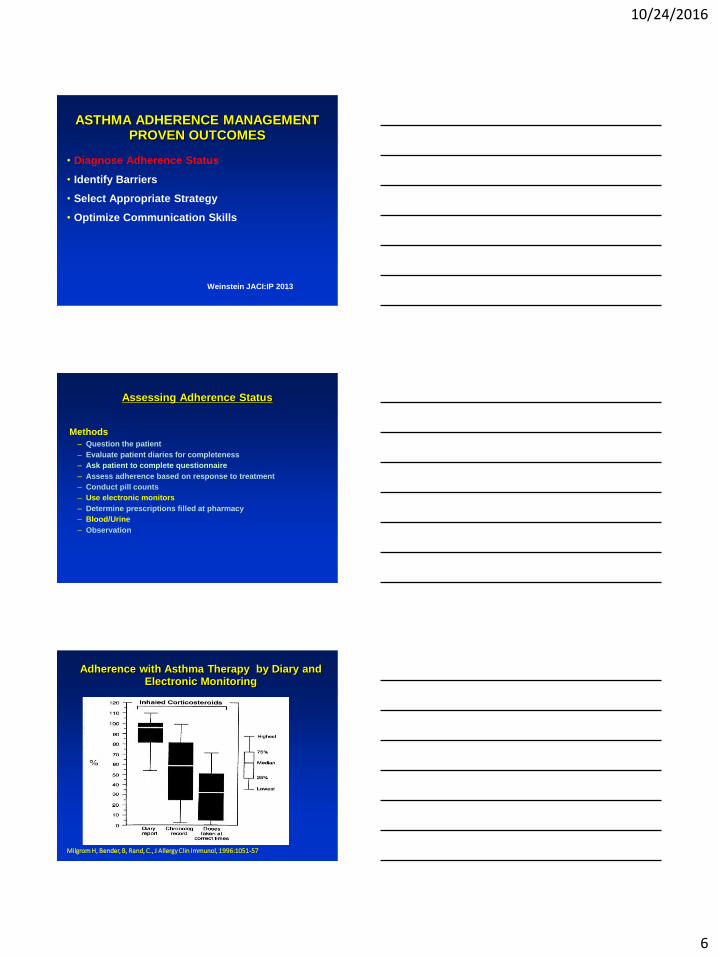
Adherence with Asthma Therapy by Diary and Electronic Monitoring
Milgrom H, Bender, B, Rand, C., J Allergy Clin Immunol, 1996:1051-57

10/24/2016
7
Nonadherence is associated with increased
risk of disease exacerbations
Milgrom H, Bender, B, Rand, C., J Allergy Clin Immunol, 1996:1051-57
ASTHMA ADHERENCE MANAGEMENT PROVEN OUTCOMES
• Diagnose Adherence Status
• Identify Barriers
• Select Appropriate Strategy
• Optimize Communication Skills
Weinstein JACI:IP 2013
10/24/2016
8

10/24/2016
9
Factors (Barriers) Involved in Non-Adherence GINA 2008
Drug Factors
• Difficulties with inhaler devices
• Awkward regimes
(e.g.,four times daily or multiple drugs)
• Side effects
• Cost of medication
• Dislike of medication
• Distant pharmacies
• ASTHMA MANAGEMENT AND PREVENTION 53
Non-Drug Factors
• Misunderstanding or lack of instruction
• Fears about side-effects
• Dissatisfaction with health care professionals
• Unexpressed/undisclosed fears or concerns
• Inappropriate expectations
• Poor supervision, training, or follow-up
• Anger about condition or its treatment
• Underestimation of severity
• Cultural issues
• Stigmatization
• Forgetfulness or complacency
• Attitudes toward ill health
• Religious issues
Factors Involved in Non-Adherence
Asthma Adherence Pathway
Drug Factors
• Difficulties with inhaler devices
• Awkward regimes
(e.g.,four times daily or multiple drugs)
• Side effects
• Cost of medication
• Dislike of medication
• Distant pharmacies
• ASTHMA MANAGEMENT AND PREVENTION 53
Non-Drug Factors
• Misunderstanding or lack of instruction
• Fears about side-effects
• Dissatisfaction with health care professionals
• Unexpressed/undisclosed fears or concerns
• Inappropriate expectations
• Poor supervision, training, or follow-up
• Anger about condition or its treatment
• Underestimation of severity
• Cultural issues
• Stigmatization
• Forgetfulness or complacency
• Attitudes toward ill health
• Religious issues
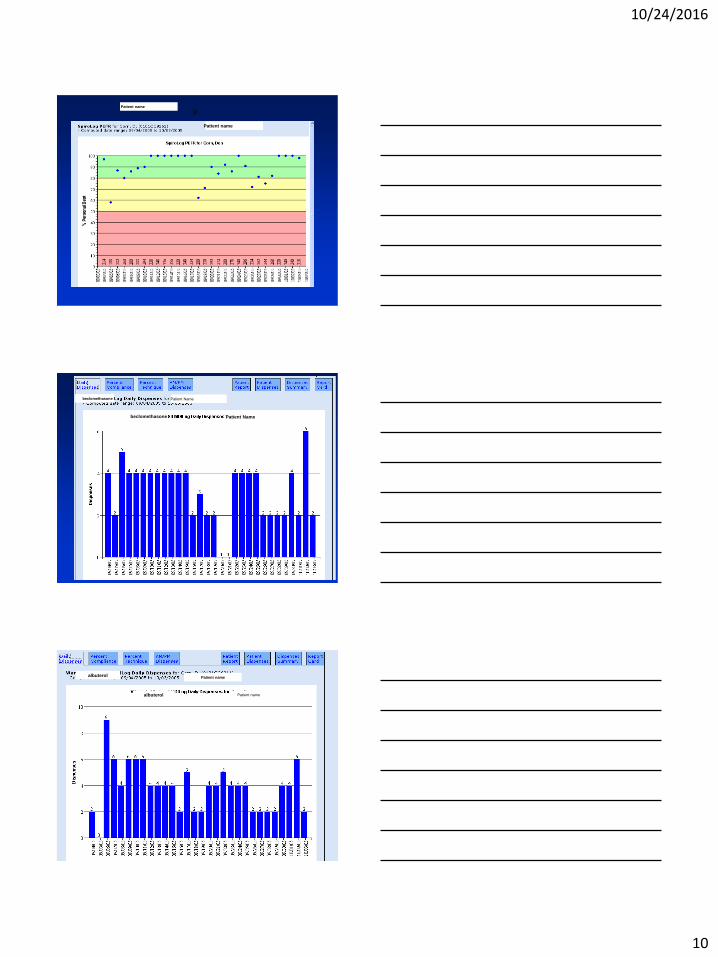
Blue Cross Blue Shield DE Asthma Monitoring Program
“I start treatment without delay: Never”
10/24/2016
10
Patient name
Patient name
p
Patient Name
Patient Name beclomethasone
beclomethasone
albuterol
albuterol Patient name
Patient name
10/24/2016
11
ASTHMA ADHERENCE MANAGEMENT PROVEN OUTCOMES
• Diagnose Adherence Status
• Identify Barriers
• Select Appropriate Strategy:
• Steroid Phobia
• Optimize Communication Skills
Weinstein JACI:IP 2013
ASTHMA ADHERENCE MANAGEMENT PROVEN OUTCOMES
• Diagnose Adherence Status
• Identify Barriers
• Select Appropriate Strategy
• Optimize Communication Skills
Motivational Interviewing
Weinstein JACI:IP 2013
What is Motivational Interviewing
• Patient –Centerd
• Focuses patient ambivalence
• Explores reasons for and against change
• Designed to enhance intrinsic motivation

10/24/2016
12
Paradigm Shift
Patient Must
Change
Move patient along
continuum of change
Help patient
to resolve
ambivalence
Build motivation and
confidence
Ambivalence
• Normal and understandable
• Any decision to change can have competing motivations, each of which has costs and benefits
• Strategy to help individuals examine, understand and resolve ambivalence to change
• Strategy to enhance a individual’s motivation to change
Exploring Ambivalence
Weigh the pros and cons of change
“What are some of the good things
about taking your medication?”
“What are some of the less good
things about taking your medication?”
10/24/2016
13
Initial Visit
ADHERENCE MANAGEMENT MODEL: Steroid Phobia
INITIAL VISIT
• History / PE
• Make recommendation
• Provide further rationale if recommendation not accepted
• Prescribe reasonable alternative if available
• Provide close supervision
MI Communications Strategies
• Reflections
• Cost-Benefit Analysis
10/24/2016
14
Reflective Listening
Statement, not a question
Let’s the patient know you are listening and trying to understand.
Ends with a down turn
Hypothesis testing
(If I understand you correctly, it sounds like..)
Take a guess at what the person means.
Affirms and validates
Keeps the client thinking and talking
Used strategically to elicit self-
motivational statements & diffuse
resistance
Reflective Listening
The words the
speaker says The words the
listener hears
What the listener
THINKS the speaker
means
What the speaker
means
Levels of Reflective Listening
Simple (Repeating) Reflection
– The simplest level. Merely repeat what the patient has said.
– . Mother: I am worried and frightened.
– Dr: So you’re worried and frightened.
End as a statement, not as a question
10/24/2016
15
Levels of Listening
Early/Small Jump
Restating Rephrasing Paraphrasing Deduction
Later/Big Jump
Levels of Reflective Listening
Simple (Repeating) Reflection
– The simplest level. Merely repeat what the patient has said.
– . Mother: I am worried and frightened.
– Dr: So you’re worried and frightened.
End as a statement, not as a question
Follow-up Visit
10/24/2016
16
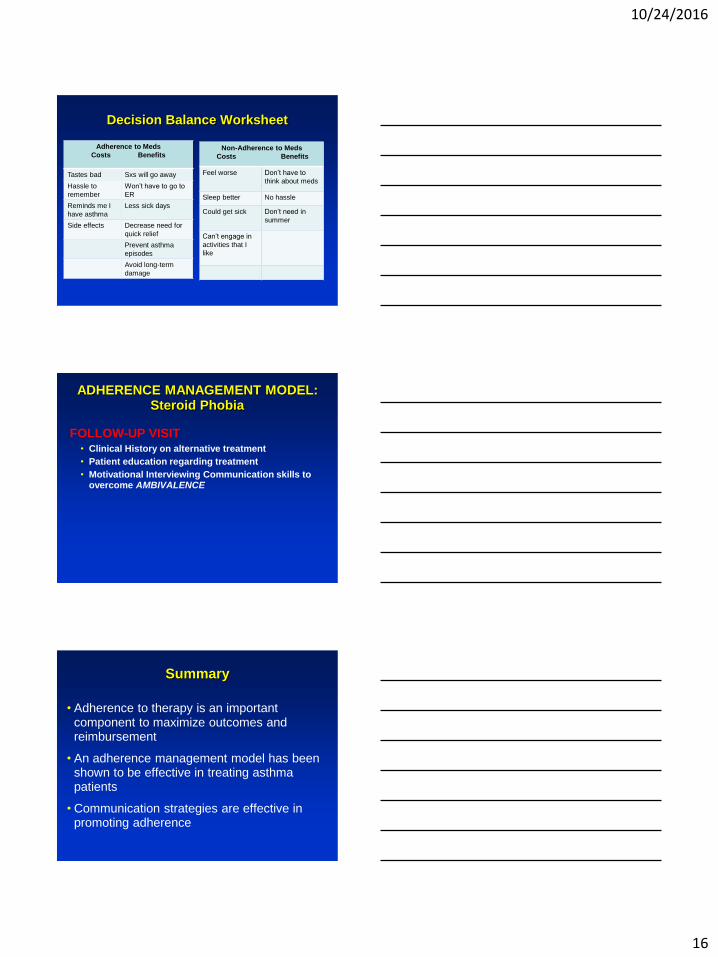
Decision Balance Worksheet
Adherence to Meds
Costs Benefits
Tastes bad Sxs will go away
Hassle to
remember
Won’t have to go to
ER
Reminds me I
have asthma
Less sick days
Side effects Decrease need for
quick relief
Prevent asthma
episodes
Avoid long-term
damage
Non-Adherence to Meds
Costs Benefits
Feel worse Don’t have to
think about meds
Sleep better No hassle
Could get sick Don’t need in
summer
Can’t engage in
activities that I
like
ADHERENCE MANAGEMENT MODEL: Steroid Phobia
FOLLOW-UP VISIT • Clinical History on alternative treatment
• Patient education regarding treatment
• Motivational Interviewing Communication skills to overcome AMBIVALENCE
Summary
• Adherence to therapy is an important component to maximize outcomes and reimbursement
• An adherence management model has been shown to be effective in treating asthma patients
• Communication strategies are effective in promoting adherence

10/24/2016
17
Comparing Outpatient to Inpatient Asthma Rehabilitation*
11 Outpatient 22 Inpatient
ONE YEAR PRIOR **
Total Asthma Charges $6,374 ($6,319) $7,053 ( $5,640)
Hospital 3.91 (0 – 18) 5.09 (0 - 18)
ER 2.55 (0 – 6) 3.0 (2 - 12)
Corticosteroid Bursts 4.09 (2 – 10) 3.77 (2 - 12)
Length of Rehab (days) 4.82 (4 – 5) 14.05 (10 - 26)
ONE YEAR POST **
Hospital 0.09 (0 - 1) 0.64 (0 - 6)
ER 0.18 (0 - 1) 1.4 (2 - 6)
Corticosteroid Bursts 1.64 (0 - 4) 2.36 (0 - 10)
Rehab Physician Visits 0.5 (0 - 1) 9.45 (0 - 12)
P < 0.004
* Matched for 1-year prior morbidity
** Mean ( Median) Weinstein JACI 1998
Available Adherence Monitors
SmartInhaler
Source: http://www.smartinhaler.com/platform.html
10/24/2016
18
Propeller
Source: http://propellerhealth.com/solutions/
Gecko
Source: http://www.caretrx.com/#!/