powerpoint presentation s049 - marathe... · •rarely hirschsprung disease •rarely deafness ....
TRANSCRIPT

3/21/2019
1
Boards Blitz Pediatric Dermatology
Kalyani Marathe, MD MPH Assistant Professor of Dermatology and
Pediatrics, GWU SOM
What most likely triggered this eruption?
A. Trimethoprim-Sulfamethoxazole
B. Compositae
C. Methylisothiazolinone
D. Crisaborole
E. Asthma inhaler
Periorificial dermatitis is usually triggered by steroids contacting the skin and some say it is a precursor to rosacea.
• Treatment:
– Topical calcineurin inhibitors
– Metronidazole cream/gel
– Oral antibiotics (erythromycin/azithromycin)
Hurwitz, 5th ed
Granulomatous periorificial dermatitis is a more inflammatory version and can resemble sarcoidosis or Blau.
Hurwitz, 5th ed
This child should be screened with which of the following tests?
A) Spinal Ultrasound
B) Genitourinary Ultrasound
C) Skin biopsy
D) A and B
E) All of the above
3/21/2019
2
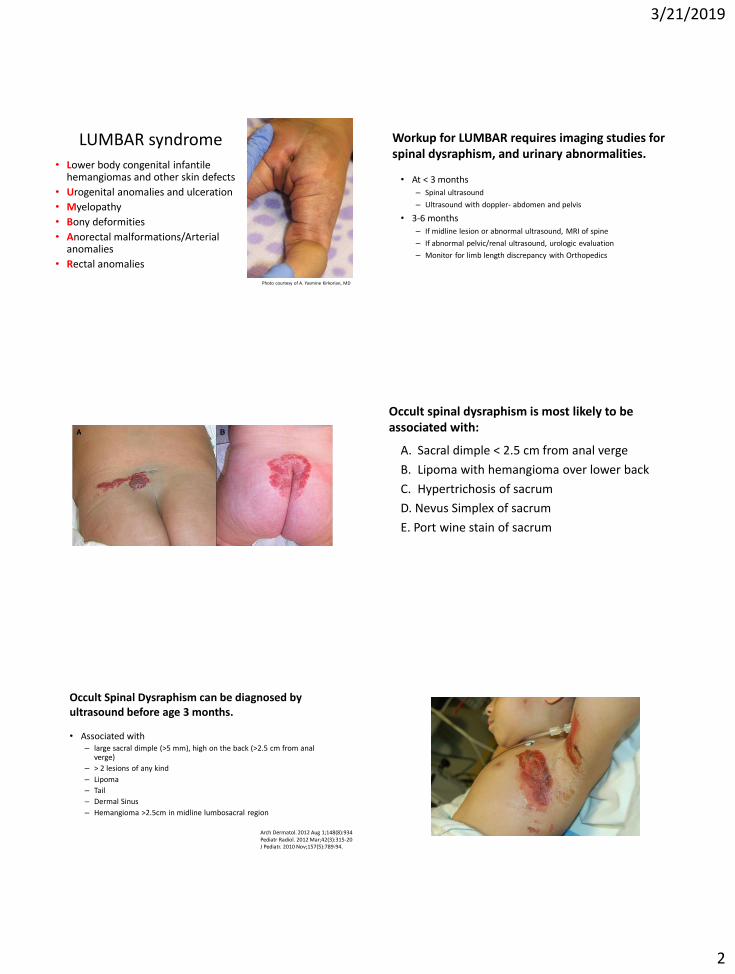
LUMBAR syndrome
• Lower body congenital infantile hemangiomas and other skin defects
• Urogenital anomalies and ulceration
• Myelopathy
• Bony deformities
• Anorectal malformations/Arterial anomalies
• Rectal anomalies
Photo courtesy of A. Yasmine Kirkorian, MD
Workup for LUMBAR requires imaging studies for spinal dysraphism, and urinary abnormalities.
• At < 3 months – Spinal ultrasound
– Ultrasound with doppler- abdomen and pelvis
• 3-6 months – If midline lesion or abnormal ultrasound, MRI of spine
– If abnormal pelvic/renal ultrasound, urologic evaluation
– Monitor for limb length discrepancy with Orthopedics
Occult spinal dysraphism is most likely to be associated with:
A. Sacral dimple < 2.5 cm from anal verge
B. Lipoma with hemangioma over lower back
C. Hypertrichosis of sacrum
D. Nevus Simplex of sacrum
E. Port wine stain of sacrum
Occult Spinal Dysraphism can be diagnosed by ultrasound before age 3 months.
• Associated with – large sacral dimple (>5 mm), high on the back (>2.5 cm from anal
verge)
– > 2 lesions of any kind
– Lipoma
– Tail
– Dermal Sinus
– Hemangioma >2.5cm in midline lumbosacral region
Arch Dermatol. 2012 Aug 1;148(8):934. Pediatr Radiol. 2012 Mar;42(3):315-20. J Pediatr. 2010 Nov;157(5):789-94.

3/21/2019
3
This child’s skin reaction is from an attack on the same protein as which disease?
A. Pemphigus Vulgaris
B. Pemphigus Foliaceus
C. Pemphigoid Gestationis
D. Linear IgA Bullous Disease
E. Bullous Pemphigoid
Bullous Impetigo is usually localized but can be diffuse.
• Infection with staph > strep
• Systemic treatment in special populations or if very diffuse
• Mupirocin ointment and dilute bleach baths if localized
Staphylococcal exotoxin-A Phage group II
Attacks Desmoglein-1
Blisters, pustules, superficial erosions
FLI-1412-2DC-3N
Bullous impetigo usually affects face and intertriginous areas and does not cause systemic symtoms.
Exfoliative exotoxins are made by 5% of S. aureus strains.
• Toxins ETA and ETB
• Likely act as proteases that target desmoglein-1
• All phage groups are able to produce exfoliative toxin
Name that Target!!!!!
A. Epidermolysis Bullosa Acquisita
B. Pemphigus Foliaceus
C. Pemphigoid Gestationis
D. Linear IgA Bullous Disease
E. Bullous Pemphigoid
Name that Target!!!!!
A. Epidermolysis Bullosa Acquisita- Collagen VII
B. Pemphigus Foliaceus- Desmoglein 1
C. Pemphigoid Gestationis- BPAG2
D. Linear IgA Bullous Disease- LABD97 (97 kD NC domain of BPAG2)
E. Bullous Pemphigoid- BPAG2 > BPAG1

3/21/2019
4
What test should be checked on this child?
A. Calcium
B. TSH
C. Lipids
D. CBC with differential
E. Abdominal ultrasound
Subcutaneous Fat Necrosis of the Newborn more common in babies that have had cooling.
Monitor for elevated calcium, especially if the disease is extensive
Should monitor up to 6 months
No guidelines
What is the first test to order in this child?atal Lupus
A. CBC
B. EKG
C. Abdominal ultrasound
D.A. and B.
E. A, B, and C

3/21/2019
5
Neonatal Lupus
Neonatal Lupus • Ultraviolet light may exacerbate or initiate cutaneous lesions
• *Do bilirubin lights cause exacerbation? • No • Bilirubin lights = 420-470 nm (visible spectrum) • Ultraviolet light = 200-400 nm
• To mothers with SLE, or other CTD, HLA-DR3 • 50% mothers asymptomatic at delivery • Lesions usually resolve by 6 months without scarring • Dyspigmentation and telangiectasias can remain • “Ro makes the heart go slow”
50% of Neonatal lupus patients can have heart block
• Third degree most common- which is permanent
• Can also manifest with thrombocytopenia and liver disease
• Risk of second child with LE approx 25%
• Occasional U1RNP antibodies, which is not associated with heart block
What is the most appropriate treatment?
A. Ketoconazole shampoo
B. Ketoconazole cream
C. Griseofulvin 10mg/kg/day
D. Griseofulvin 20mg/kg/day
E. Terbinafine 250 mg daily
Feel for occipital and posterior cervical lymph nodes if you suspect tinea capitis.

3/21/2019
6
Tinea Capitis requires systemic treatment for 6-8 weeks.
• Griseofulvin Solution (microsize) 20-25mg/kg x 8 weeks OR at least 2 weeks past symptom resolution – Gris-Peg (ultramicrosize) is better absorbed but often not covered
• Terbinafine: FDA approved as sprinkles but these are typically not covered by insurance. Prescribe generic tablet with weight-based dosing and parents can crush: – <20kg: 62.5mg daily x 6 weeks – 20-40kg: 125mg daily x 6 weeks – 40kg: 250mg daily x 6 weeks
What neoplasm is this child most likely to develop in adulthood?
A. SCC
B. BCC
C. Trichoblastoma
D. Poroma
E. Trichoepithelioma
Nevus Sebaceus is a benign growth present at birth and experiences hormonal changes.
• Long term:
– Previously thought to develop basal cell carcinoma
– Now thought to be benign growths
– Trichoblastoma and Syringocystadenoma papilliferum both reported as most common
• Do not routinely need to be removed
J Am Acad Dermatol. 2014 Feb;70(2):332-7. J Dermatol. 2016 Feb;43(2):175-80.
Can you name the functions of these proteins?
Desmosome
Adherens Junction
Gap Junction
Tight Junction
Bind Actin Filaments
Intercellular Communication
“Barrier and Fence”
Keratinocyte Adhesion
A 4 year old child comes in for persistently scaly feet and palms You notice these findings. Upon closer examination, the mother’s feet look like this:
3/21/2019
7
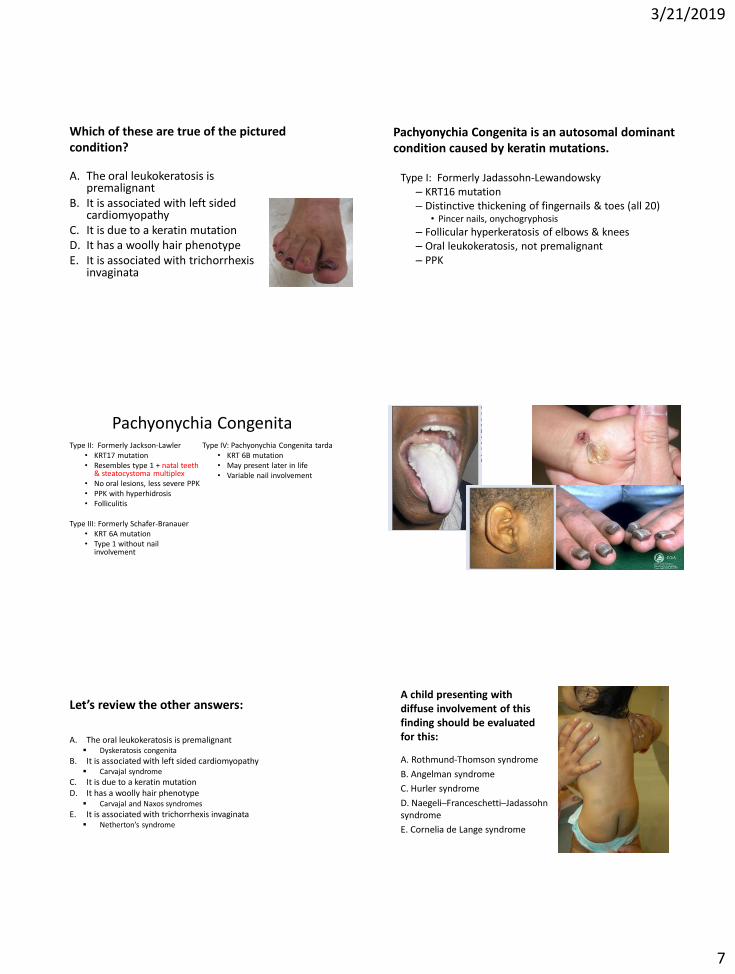
Which of these are true of the pictured condition?
A. The oral leukokeratosis is premalignant
B. It is associated with left sided cardiomyopathy
C. It is due to a keratin mutation D. It has a woolly hair phenotype E. It is associated with trichorrhexis
invaginata
Pachyonychia Congenita is an autosomal dominant condition caused by keratin mutations.
Type I: Formerly Jadassohn-Lewandowsky – KRT16 mutation – Distinctive thickening of fingernails & toes (all 20)
• Pincer nails, onychogryphosis
– Follicular hyperkeratosis of elbows & knees – Oral leukokeratosis, not premalignant – PPK
Pachyonychia Congenita Type II: Formerly Jackson-Lawler
• KRT17 mutation • Resembles type 1 + natal teeth
& steatocystoma multiplex • No oral lesions, less severe PPK • PPK with hyperhidrosis • Folliculitis
Type III: Formerly Schafer-Branauer
• KRT 6A mutation • Type 1 without nail
involvement
Type IV: Pachyonychia Congenita tarda • KRT 6B mutation • May present later in life • Variable nail involvement
Let’s review the other answers:
A. The oral leukokeratosis is premalignant Dyskeratosis congenita
B. It is associated with left sided cardiomyopathy Carvajal syndrome
C. It is due to a keratin mutation D. It has a woolly hair phenotype
Carvajal and Naxos syndromes
E. It is associated with trichorrhexis invaginata Netherton’s syndrome
A child presenting with diffuse involvement of this finding should be evaluated for this:
A. Rothmund-Thomson syndrome
B. Angelman syndrome
C. Hurler syndrome
D. Naegeli–Franceschetti–Jadassohn syndrome
E. Cornelia de Lange syndrome
3/21/2019
8
Diffuse Dermal Melanocytosis can be a marker of metabolic diseases/mucopolysaccharidoses.
Associated with lysosomal storage disorders and mucopolysaccharidoses
Hurler>Hunter
Look for other cutaneous stigmata
• Coarse facies
• Thickened skin
• Excessive hair growth
• Pebbled skin on upper back
• Atherosclerotic changes of hands
Gupta D, Thappa DM. Mongolian spots. Indian J Dermatol Venereol Leprol 2013;79:469-78 Pediatr Dermatol. 2016 Nov;33(6):594-601.
X-linked dominant diseases: The CHICAGO Bulls Dominated because they had the MIDAS touch • Conradi Hunerman
• Incontinentia Pigmenti
• CHILD
• Albright’s hereditary osteodystrophy
• Goltz
• Oro-facial-digital Syndrome
• Bazex
• MIDAS
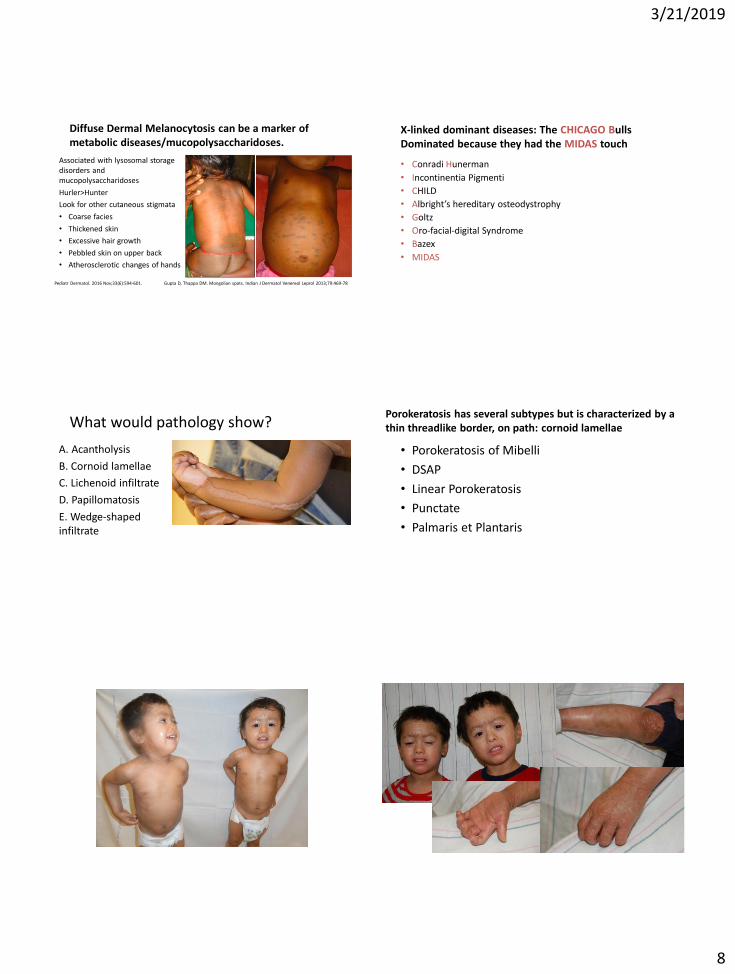
What would pathology show?
A. Acantholysis
B. Cornoid lamellae
C. Lichenoid infiltrate
D. Papillomatosis
E. Wedge-shaped infiltrate
Porokeratosis has several subtypes but is characterized by a thin threadlike border, on path: cornoid lamellae
• Porokeratosis of Mibelli
• DSAP
• Linear Porokeratosis
• Punctate
• Palmaris et Plantaris

3/21/2019
9
What is the most likely mutation in these patients?
A. ABCA12
B. LIPN
C. ALOXE3
D. TGM1
E. STI4
Lamellar Ichthyosis is caused by an AR mutation in TGM-1
• Transglutaminase 1
• Scarring alopecia, nail dystrophy
• Collodion baby at birth
• Ectropion is almost always present, eclabium
• Moderate hyperkeratosis of the palms and soles is usually present, hypohidrosis, heat intolerance
Which of the following is INCORRECT about the pictured condition?
A. There is a reduced number of disulfide bonds in hair shafts
B. Trichorrhexis nodosa is found
C. Serum IgE is markedly elevated
D. Intermittent aminoaciduria is uncommon
E. The gene encodes for LEKTI
Netherton Syndrome is an autosomal recessive condition with notable atopic features.
• SPINK5 gene encoding LEK1, serine protease inhibitor
• Ichthyosis linearis circumflexa
• Atopic dermatitis
• Trichorrhexis invaginata
• Pili torti, trichorrhexis nodosa
• Food allergies
The classic triad
3/21/2019
10
What test should be performed?
A. MRI brain and spine
B. Skin biopsy
C. Liver ultrasound
D. GU ultrasound
E. Limb length testing
Neurocutaneous melanosis is a potentially deadly condition when symptomatic
Risk factors:
• A large CMN, especially if >40 cm predicted final size and in a posterior axial location
• Multiple satellite nevi
• More than two medium-sized CMN (especially if numerous)
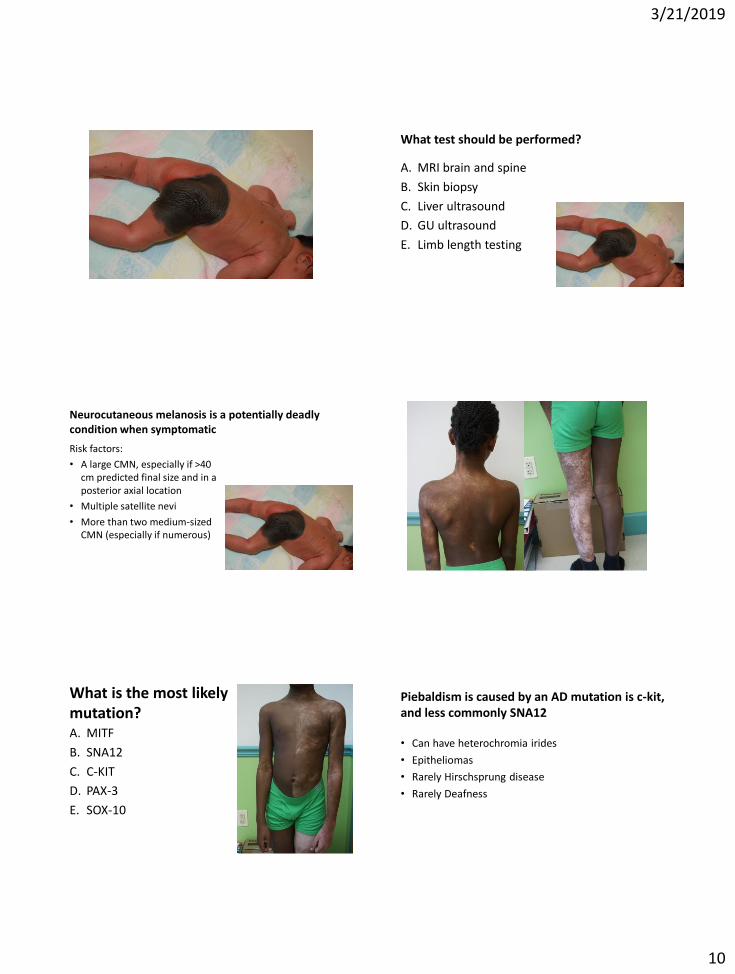
What is the most likely mutation? A. MITF
B. SNA12
C. C-KIT
D. PAX-3
E. SOX-10
Piebaldism is caused by an AD mutation is c-kit, and less commonly SNA12
• Can have heterochromia irides
• Epitheliomas
• Rarely Hirschsprung disease
• Rarely Deafness

3/21/2019
11
A previously healthy 5 year old boy presents with cough, crusted and fissured lips, and injected conjunctiva. You also note rare blisters on his trunk. He also has a cough. What is the treatment?
A. Oral Acyclovir B. Azithromycin C. VZV D. Supportive Care E. TPN
Mycoplasma-Induced Rash and Mucositis (MIRM)
Mycoplasma Induced Rash and Mucositis (MIRM) is a new term for an old condition
• Patients age on average 12
• Majority male
• Features of SJS
J Am Acad Dermatol. 2015 Feb;72(2):239-45.
Mycoplasma Induced Rash and Mucositis (MIRM) presents with primarily mucous membrane involvement
• Oral (94%), Ocular (82%), Urogenital (63%)
• Treatment:
• Antibiotics, systemic steroids, IVIG, supportive care
• Nutritional support
• 8% recurrence rate, 3% mortality
J Am Acad Dermatol. 2015 Feb;72(2):239-45.

3/21/2019
12
When this child reaches her 20’s, what is most likely to be her cause of death?
A. Sepsis
B. Esophageal rupture
C. Failure to thrive
D. SCC
E. Suicide
Recessive Dystrophic EB is caused by an autosomal recessive mutation in Col VII.
When fatal in first year, sepsis
Mitten deformity
Wound care
Nutrition/GI
UpToDate
3/21/2019
13
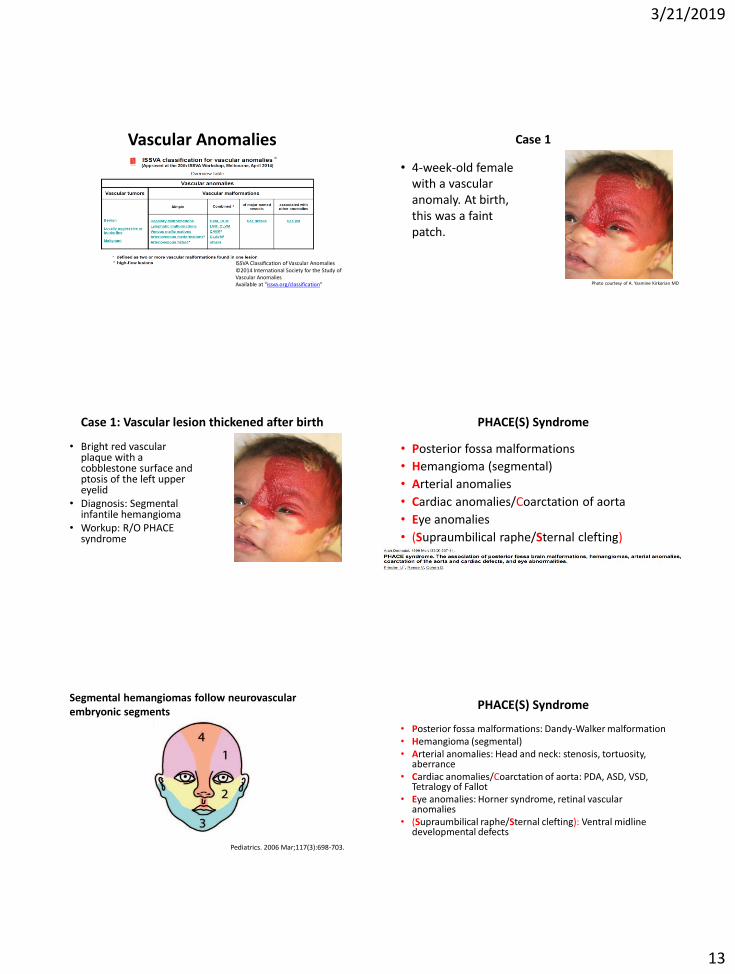
Vascular Anomalies
ISSVA Classification of Vascular Anomalies ©2014 International Society for the Study of Vascular Anomalies Available at "issva.org/classification"
Case 1
• 4-week-old female with a vascular anomaly. At birth, this was a faint patch.
Photo courtesy of A. Yasmine Kirkorian MD
Case 1: Vascular lesion thickened after birth
• Bright red vascular plaque with a cobblestone surface and ptosis of the left upper eyelid
• Diagnosis: Segmental infantile hemangioma
• Workup: R/O PHACE syndrome
PHACE(S) Syndrome
• Posterior fossa malformations
• Hemangioma (segmental)
• Arterial anomalies
• Cardiac anomalies/Coarctation of aorta
• Eye anomalies
• (Supraumbilical raphe/Sternal clefting)
Segmental hemangiomas follow neurovascular embryonic segments
Pediatrics. 2006 Mar;117(3):698-703.
PHACE(S) Syndrome
• Posterior fossa malformations: Dandy-Walker malformation • Hemangioma (segmental) • Arterial anomalies: Head and neck: stenosis, tortuosity,
aberrance • Cardiac anomalies/Coarctation of aorta: PDA, ASD, VSD,
Tetralogy of Fallot • Eye anomalies: Horner syndrome, retinal vascular
anomalies • (Supraumbilical raphe/Sternal clefting): Ventral midline
developmental defects

3/21/2019
14
Many thanks to neuroradiologist Dr. Jonathon Murnick
Photo courtesy of A. Yasmine Kirkorian, MD and Johnathan Murnick, MD
Photo courtesy of A. Yasmine Kirkorian, MD and Johnathan Murnick, MD
Workup for PHACE
• Neuroimaging
– MRI/MRA
• Echocardiogram
• Ophthalmologic evaluation
Hemangioma Treatment
Hemangioma Treatment Oral Propranolol is the only FDA approved treatment for infantile hemangiomas
• Infants > 5 weeks
• Uptitrate to 3.4 mg/kg/day in BID dosing
• Monitor for bradycardia, hypotension, hypoglycemia
3/21/2019
15
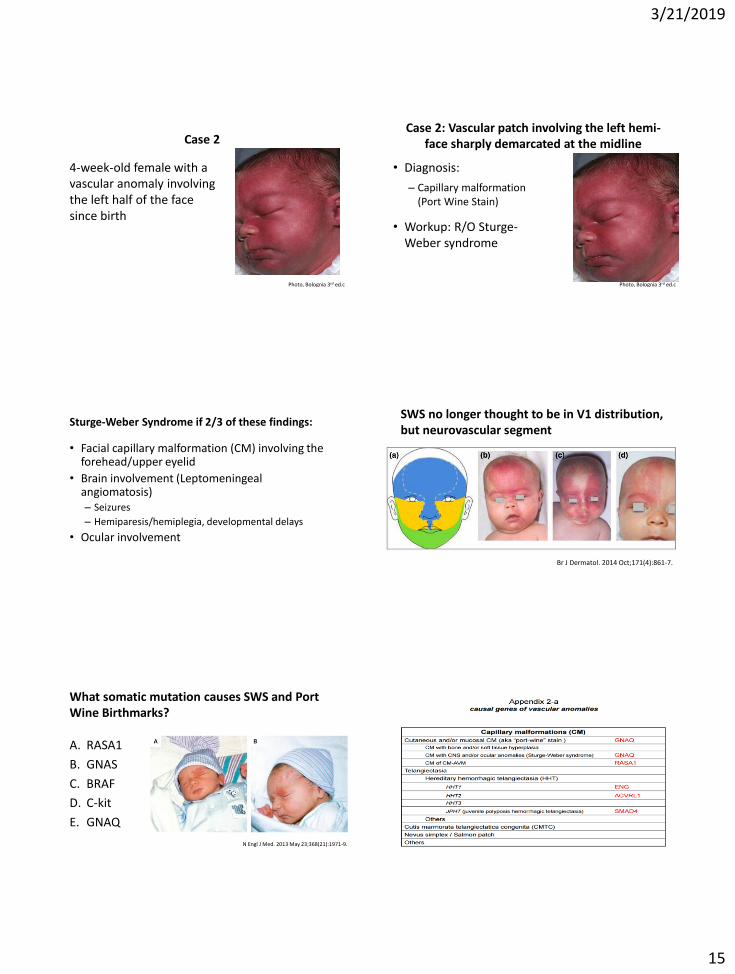
Case 2
4-week-old female with a vascular anomaly involving the left half of the face since birth
Photo, Bolognia 3rd ed.c
Case 2: Vascular patch involving the left hemi-face sharply demarcated at the midline
• Diagnosis:
– Capillary malformation (Port Wine Stain)
• Workup: R/O Sturge-Weber syndrome
Photo, Bolognia 3rd ed.c
Sturge-Weber Syndrome if 2/3 of these findings:
• Facial capillary malformation (CM) involving the forehead/upper eyelid
• Brain involvement (Leptomeningeal angiomatosis) – Seizures
– Hemiparesis/hemiplegia, developmental delays
• Ocular involvement
SWS no longer thought to be in V1 distribution, but neurovascular segment
Br J Dermatol. 2014 Oct;171(4):861-7.
What somatic mutation causes SWS and Port Wine Birthmarks?
A. RASA1
B. GNAS
C. BRAF
D. C-kit
E. GNAQ
N Engl J Med. 2013 May 23;368(21):1971-9.
3/21/2019
16
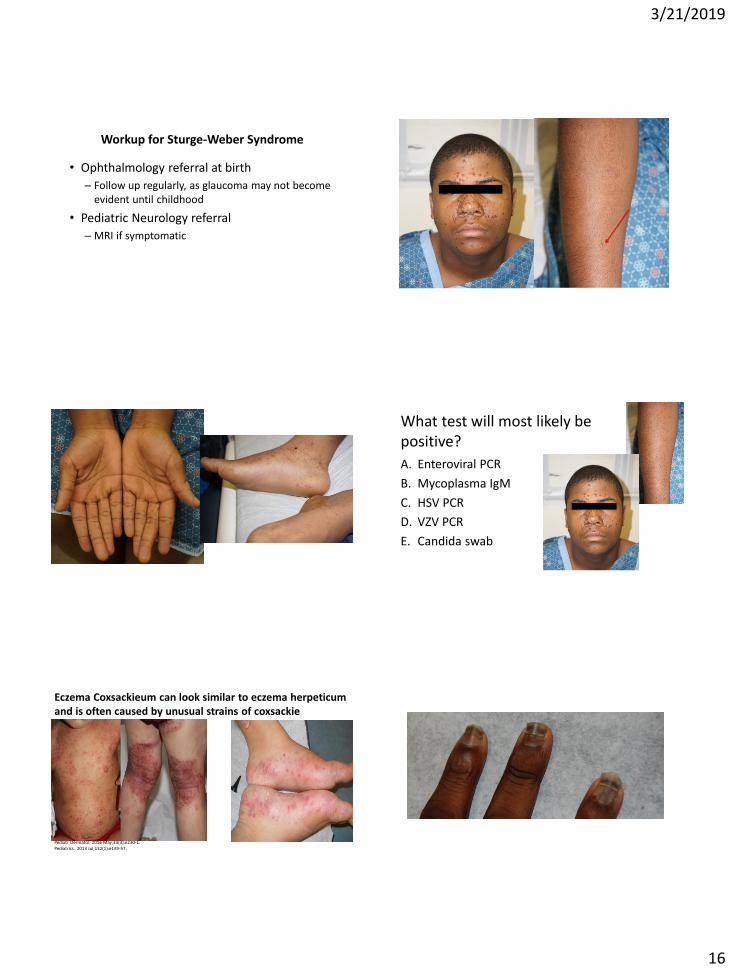
Workup for Sturge-Weber Syndrome
• Ophthalmology referral at birth
– Follow up regularly, as glaucoma may not become evident until childhood
• Pediatric Neurology referral
– MRI if symptomatic
What test will most likely be positive?
A. Enteroviral PCR
B. Mycoplasma IgM
C. HSV PCR
D. VZV PCR
E. Candida swab
Eczema Coxsackieum can look similar to eczema herpeticum and is often caused by unusual strains of coxsackie
Pediatr Dermatol. 2016 May;33(3):e230-1. Pediatrics. 2013 Jul;132(1):e149-57.
