ppt slide - jeffrey bryan - treatment modalities drug ... · treatment modalities: drug therapy,...
TRANSCRIPT

1
PowerPoint Slides English Text Spanish Translation
Treatment Modalities: Drug Therapy, Part 2 Video Transcript
Modalidades de Tratamiento: Terapia de Medicamentos, Parte 2
Transcripción del video
Professional Oncology Education Treatment Modalities: Drug Therapy, Part 2 Time: 18:16
Educación Oncológica Profesional Modalidades de Tratamiento: Terapia de Medicamentos, Parte 2 Duración: 18:16
Jeffrey Bryan, Pharm.D. Clinical Pharmacy Specialist Pharmacy Clinical Programs The University of Texas MD Anderson Cancer Center
Dr. Jeffrey Bryan, Doctor en Farmacia
Especialista en Farmacia Clínica
Programas Clínicos de Farmacia
MD Anderson Cancer Center, Universidad de Texas
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Treatment Modalities: Treatment Modalities:
Drug Therapy Drug Therapy –– Part II Part II
Jeffrey Bryan, Pharm.D.
Clinical Pharmacy Specialist
Pharmacy Clinical Programs
Hello, my name is Jeffrey Bryan. I am a Clinical Pharmacy Specialist with The University of Texas MD Anderson Cancer Center. I would like to welcome you to the second part of Treatment Modalities: Drug Therapy.
Hola. Me llamo Jeffrey Bryan. Soy Especialista en Farmacia Clínica en el MD Anderson Center de la Universidad de Texas y le doy a usted la bienvenida a la segunda parte de la sección Modalidades de Tratamiento: Terapia de Medicamentos.

2
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
ObjectivesObjectivesObjectivesObjectives
Upon completion of this lesson, participants will
be able to:
• Discuss the goals and roles of drug therapy
• Identify classifications of chemotherapy
• Differentiate between chemotherapy, hormone,
immune-based, and targeted therapy
• Identify common toxicities of drug treatment
Upon completion of this lesson, participants should be able to discuss the goals and roles of drug therapy; identify classifications of chemotherapy; differentiate between chemotherapy, hormone therapy, immune-based therapy, and targeted therapy; and identify some common toxicities associated with chemotherapeutic agents.
Una vez finalizada esta lección los participantes podrán hablar sobre los objetivos y roles de la terapia de medicamentos; identificar las clasificaciones de la quimioterapia; diferenciar entre la quimioterapia, la terapia hormonal, la terapia inmunológica y la terapia dirigida; e identificar las toxicidades comunes asociadas a los agentes quimioterapéuticos.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Immune-based Therapy and
Targeted Therapy
At first, we will start off with immune-based therapy, then discuss targeted therapy.
Comenzaremos con la terapia inmunológica y seguiremos con la terapia dirigida.

3
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
ImmuneImmuneImmuneImmune----based Therapybased Therapybased Therapybased Therapy
• Treatment with agents from biologic sources
and/or agents able to affect biologic responses
• Stimulates host’s immune system to fight
against cancer
• A means to deliver systemic anticancer therapy
The idea of stimulating or augmenting the body’s own immune system to fight or prevent cancer led to the development of immune-based therapies. This is now referred to by many as the fourth cancer treatment modality. The idea is to use various cytokines and other biologic response modifiers, such as interferon, monoclonal antibodies, and vaccines, to stimulate the host immune system to attack the tumors.
La idea de estimular o reforzar el propio sistema inmunológico para combatir o prevenir el cáncer dio lugar al desarrollo de las terapias inmunológicas, que ahora muchos consideran la cuarta modalidad de tratamiento contra el cáncer. La idea es usar varias citocinas y otros modificadores de respuesta biológica, como el interferón, anticuerpos monoclonales y vacunas, para promover que el sistema inmunológico huésped ataque a los tumores.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIImmuneImmuneImmuneImmune----based Therapy based Therapy based Therapy based Therapy ----Interferons/InterleukinsInterferons/InterleukinsInterferons/InterleukinsInterferons/Interleukins
• Cytokines - proteins that are normally produced in
the body in response to stress
• Act as chemical signals to:
– Directly slow tumor growth
– Slow angiogenesis (formation of new blood vessels)
– Stimulate cancer cells to produce antigens
– Stimulate immune system cells to attack cancer cells
• Interferon-alfa: CML, melanoma, lymphoma
• Interleukin-2 (IL-2): melanoma, renal cell
Interferons, interleukins are part of a family of cytokines and proteins that are normally produced in the body in response to stress or inflammation. Genetically-engineered interferon and interleukin have been shown to have anti-tumor effects in several malignancies. Although their toxicities differ from conventional chemotherapy, they are associated with a constellation of symptoms, such as fever, chills, myalgias, depression, and sometimes myelosuppression.
Los inteferones y las interleucinas forman parte de una familia de citocinas y proteínas que normalmente produce el cuerpo en respuesta al estrés o la inflamación. Se ha demostrado que los interferones genéticamente modificados y las interleucinas tienen efectos antitumorales en varias neoplasias. Si bien sus toxicidades difieren de la quimioterapia convencional, están asociadas a un sinnúmero de síntomas como fiebre, escalofríos, mialgia, depresión y, a veces, mielosupresión.
4
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIImmuneImmuneImmuneImmune----based Therapy based Therapy based Therapy based Therapy ----Monoclonal Antibodies (MoAb)Monoclonal Antibodies (MoAb)Monoclonal Antibodies (MoAb)Monoclonal Antibodies (MoAb)
• Developed to target specific proteins/antigens
involved in the development and progression
of cancer
• High specificity to tumor-specific targets
• Different toxicity profile from conventional
cytotoxic agents
• Synergy with chemotherapy agents
In recent years, a number of monoclonal antibodies have been developed for the treatment of patients with a variety of cancers. These agents target specific proteins or antigens that are expressed on tumor cells. Additionally, these agents can be given as a single agent or in combination with conventional chemotherapy without overlapping or increasing toxicity.
En los últimos años se han desarrollado varios anticuerpos monoclonales para tratar distintos cánceres. Estos agentes están dirigidos a proteínas o antígenos específicos con expresión en células tumorales. Asimismo, pueden administrarse como un único agente o en combinación con la quimioterapia convencional sin superponerse o aumentar la toxicidad.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
• Four Types of MoAbs
Murine (100% Murine)
Chimeric (30% Murine, 70% human)
Humanized (5% Murine, 95% human)
Human (100% human)
Monoclonal Antibodies (MoAbs)Monoclonal Antibodies (MoAbs)Monoclonal Antibodies (MoAbs)Monoclonal Antibodies (MoAbs)
Mouse
Human
(Murine = Mouse)
Monoclonal antibodies are synthesized from different sources. The majority of monoclonal antibodies are chimeric, meaning that they have a murine variable region fused to a human constant region or humanized, meaning they are predominantly of human origin.
Los anticuerpos monoclonales se sintetizan de distintas fuentes. La mayor parte de los anticuerpos monoclonales son quiméricos, es decir, tienen una región variable murina fusionada con una región constante humana o humanizada, lo cual implica que son predominantemente de origen humano.
5
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIMonoclonal Antibodies Monoclonal Antibodies Monoclonal Antibodies Monoclonal Antibodies ----Conjugated vs. UnconjugatedConjugated vs. UnconjugatedConjugated vs. UnconjugatedConjugated vs. Unconjugated
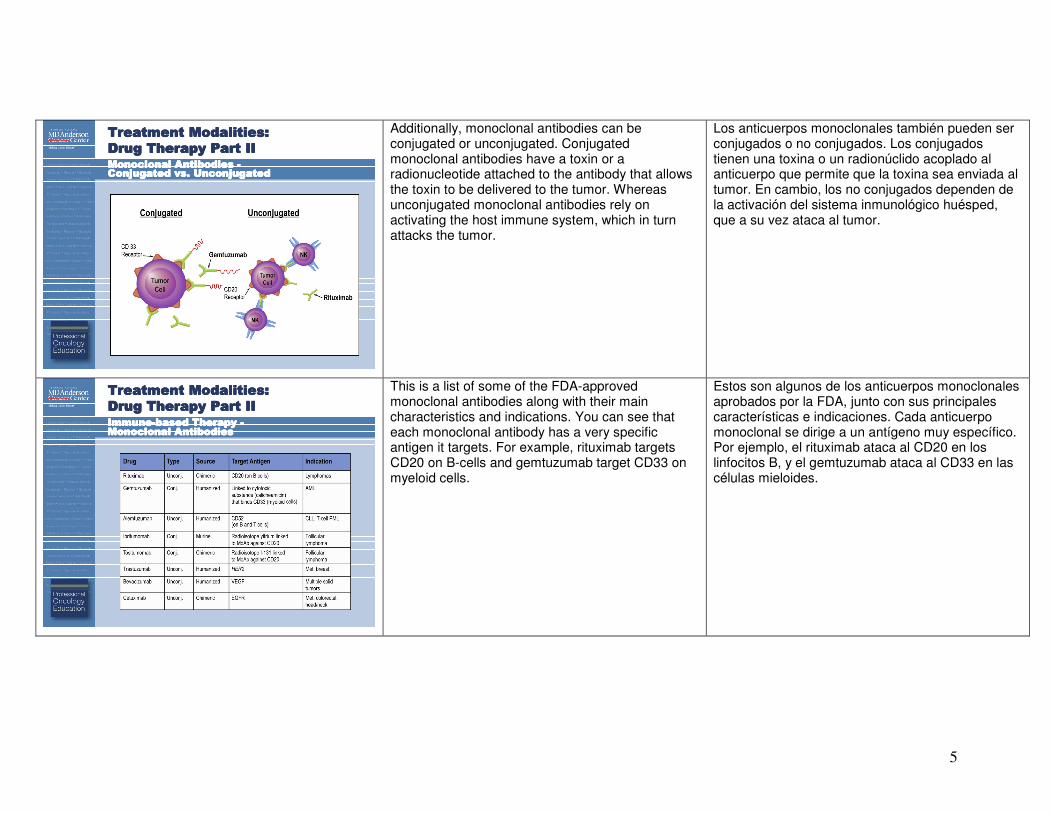
Additionally, monoclonal antibodies can be conjugated or unconjugated. Conjugated monoclonal antibodies have a toxin or a radionucleotide attached to the antibody that allows the toxin to be delivered to the tumor. Whereas unconjugated monoclonal antibodies rely on activating the host immune system, which in turn attacks the tumor.
Los anticuerpos monoclonales también pueden ser conjugados o no conjugados. Los conjugados tienen una toxina o un radionúclido acoplado al anticuerpo que permite que la toxina sea enviada al tumor. En cambio, los no conjugados dependen de la activación del sistema inmunológico huésped, que a su vez ataca al tumor.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIImmuneImmuneImmuneImmune----based Therapy based Therapy based Therapy based Therapy ----Monoclonal AntibodiesMonoclonal AntibodiesMonoclonal AntibodiesMonoclonal Antibodies
This is a list of some of the FDA-approved monoclonal antibodies along with their main characteristics and indications. You can see that each monoclonal antibody has a very specific antigen it targets. For example, rituximab targets CD20 on B-cells and gemtuzumab target CD33 on myeloid cells.
Estos son algunos de los anticuerpos monoclonales aprobados por la FDA, junto con sus principales características e indicaciones. Cada anticuerpo monoclonal se dirige a un antígeno muy específico. Por ejemplo, el rituximab ataca al CD20 en los linfocitos B, y el gemtuzumab ataca al CD33 en las células mieloides.

6
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Targeted TherapyTargeted TherapyTargeted TherapyTargeted Therapy
• Agents that specifically target cell processes that
are aberrant or more abundant in malignant cells
than normal cells
• Target cellular processes and signaling pathways
that affect:
– Cell growth and differentiation
– Angiogenesis (new blood vessel formation)
– Apoptosis (programmed cell death)
– Cell motility
We have discussed conventional chemotherapy, hormone therapy, and immune-based therapy. Now, I will spend some time discussing what is called targeted therapy and the implications on the treatment of cancer. A major limitation of current cytotoxic therapy is the lack of sensitivity on malignant cells. Chemotherapy can affect any cell that is rapidly dividing whether it be normal or malignant. As our knowledge of tumor biology increases, novel therapeutic strategies, such as targeted therapy have evolved. What is unique about targeted therapy [is] that it targets processes. Targeted therapy blocks growth of cancer cells by interfering with specific molecules, a process very different from conventional chemotherapy, hormone therapy, and immune-based therapy.
Ya hemos hablado de la quimioterapia convencional, la terapia hormonal y la terapia inmunológica. Ahora me referiré brevemente a la terapia dirigida y a sus implicancias en el tratamiento del cáncer. Una limitación importante de la terapia citotóxica actual es la falta de sensibilidad de las células malignas. La quimioterapia puede afectar toda célula que se divida rápidamente, sea normal o maligna. A medida que crece nuestro conocimiento de la biología tumoral, evolucionan nuevas estrategias terapéuticas, como la terapia dirigida. El aspecto singular de la terapia dirigida es que está orientada a procesos. La terapia dirigida obstruye el crecimiento de las células cancerosas interfiriendo en moléculas específicas, un proceso muy distinto de la quimioterapia convencional, la terapia hormonal y la terapia inmunológica.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Targeted Therapy (continued)Targeted Therapy (continued)Targeted Therapy (continued)Targeted Therapy (continued)
• Systemic-like chemotherapy designed to target
cancer cells
• Optimal targets vary widely between cancers
• Effectiveness depends on the expression of
target antigen, receptor, or other molecules
• Different toxicity profile from conventional
cytotoxic agents
• Intravenous and oral formulations
Similar to conventional chemotherapy, targeted therapy is considered systemic therapy, but designed to affect predominantly cancer cells. For this reason, these drugs are associated with very different and sometimes less side effects. The effectiveness of these drugs often depends on the expression of the target antigen receptor and other molecules on the cancer cells. A benefit of targeted therapy is that they often come in oral formulations.
De manera similar a la quimioterapia convencional, la terapia dirigida es considerada una terapia sistémica, aunque concebida para afectar más que nada las células cancerosas. Por ese motivo, estos medicamentos se asocian a efectos secundarios muy distintos, y a veces a menos efectos. La efectividad de estos medicamentos suele depender de la expresión del receptor antígeno diana y otras moléculas de las células cancerosas. Un beneficio de la terapia dirigida es que suele venir en formulaciones orales.

7
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Targeted Therapy Targeted Therapy Targeted Therapy Targeted Therapy ---- Mechanism of ActionMechanism of ActionMechanism of ActionMechanism of Action
This diagram shows the different targets for drug therapy. You can see that outside of the cell, or on the cell surface, there are growth factors that bind to the receptors. The binding triggers a cascade of intracellular events involving many tyrosine kinases. This results in increasing cell growth, proliferation, and differentiation along with angiogenesis. By inhibiting one of these proteins, you can prevent the downstream effects.
Este diagrama muestra los distintos blancos de la terapia de medicamentos. Puede observarse que afuera de la célula, o sobre su superficie, hay factores de crecimiento que se unen a los receptores. Dicha unión desencadena varios eventos intracelulares que involucran diversas tirosinas quinasas. Esto aumenta el crecimiento, la proliferación y la diferenciación de la célula, junto con la angiogénesis. Al inhibir una de estas proteínas, es posible impedir los efectos corriente abajo.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Targeted Therapy Targeted Therapy Targeted Therapy Targeted Therapy ---- Mechanism of ActionMechanism of ActionMechanism of ActionMechanism of Action
This is another depiction of the targets for some of our monoclonal antibodies and/or tyrosine kinase inhibitors. For instance, gemtuzumab targets the CD33. Gemtuzumab is complexed with a toxin called calicheamicin. Upon binding the CD33, the calicheamicin is engulfed by the cell, which causes ultimate cell death. On the bottom half of this picture, a lot of these monoclonal antibodies are used for solid tumors. But these target cell processes. And internally a lot of the tyrosine kinases such as imatinib and dasatinib target pathways that are responsible for cell differentiation and cell survival.
Aquí tenemos otra representación de los blancos de algunos de nuestros anticuerpos monoclonales e inhibidores de la tirosina quinasa. Por ejemplo, el gemtuzumab ataca al CD33. El gemtuzumab forma un complejo con una toxina llamada caliqueamicina. Luego de unirse al CD33, la caliqueamicina es engullida por la célula, lo cual finalmente provoca la muerte celular. En la mitad inferior de esta figura muchos de estos anticuerpos monoclonales son utilizados para tumores sólidos, aunque estos atacan procesos celulares. Internamente, muchas de las tirosinas quinasas como imatinib y dasatinib se dirigen a las vías responsables de la diferenciación y la supervivencia celular.

8
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Targeted Therapy Targeted Therapy Targeted Therapy Targeted Therapy ---- Summary of AgentsSummary of AgentsSummary of AgentsSummary of Agents
Vascular endothelial growth factor = VEGF
Epidermal growth factor receptor = EGFRTyrosine kinase inhibitor = TKI
Platelet-derived growth factor receptor = PDGFR
This list lists --- this table lists many FDA-approved targeted therapies and summarizes their mechanisms of action, targets, and indications. For example, bevacizumab targets VGEF, which is the vascular endothelial growth factor. And cetuximab covers --- cetuximab binds to the epidermal growth factor receptor. And we get a whole list of tyrosine kinase inhibitors, which target the cell processes within the cell, for instance, imatinib, dasatinib and erlotinib.
Aquí se enumeran varias terapias dirigidas aprobadas por la FDA y se resumen sus mecanismos de acción, blancos e indicaciones. Por ejemplo, el bevacizumab ataca al factor de crecimiento endotelial vascular (VEGF). El cetuximab se une al receptor del factor de crecimiento epidérmico. Hay una larga lista de inhibidores de la tirosina quinasa que atacan a los procesos celulares, por ejemplo, imatinib, dasatinib y erlotinib.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIImmuneImmuneImmuneImmune----based and Targeted Therapy based and Targeted Therapy based and Targeted Therapy based and Targeted Therapy ----SummarySummarySummarySummary
• Blocks the growth of cancer cells by interfering with
specific targeted molecules needed for tumor growth
• Important role as monotherapy or in combination with
chemotherapy for the treatment of cancers
• Future of cancer drug development
In summary, immune-based therapy and targeted therapy blocks the growth of cancer cells by interfering with specific targeted molecules needed for tumor growth. These play an important role for monotherapy and in combination in chemotherapy for the treatment of cancers. And this is the future of cancer drug development.
En resumen, la terapia inmunológica y la terapia dirigida obstruyen el crecimiento de las células cancerosas interfiriendo en las moléculas específicas que necesita el tumor para crecer. Ambas desempeñan un rol importante en la monoterapia y combinadas con la quimioterapia para el tratamiento del cáncer. Este es el futuro del desarrollo de medicamentos contra el cáncer.

9
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Dosing and Toxicity
Now we are going to switch gears a little bit and talk about dosing and toxicity.
Ahora cambiaremos un poco de tema para hablar de dosificación y toxicidad.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Dosing StrategiesDosing StrategiesDosing StrategiesDosing Strategies
• Body Surface Area (BSA)
– BSA(m2) =
• Single Agent Chemotherapy
– Less toxicity to normal tissue BUT
less toxicity to cancer cells
– Palliative role
• Combination Chemotherapy
– Different mechanisms of action
– Greater cell kill
– Fewer resistant cell lines
height (cm) x weight (kg)
3600√
Conventional chemotherapy is generally dosed off of BSA, which is calculated off the height and weight of the patient. For instance, a dose of 20 mg/m
2 in
the BSA of a patient is 2, the dose will be 40 mg. Oftentimes, single-agent chemotherapy is used in the palliative role, but it is generally less toxic and less toxic to cancer cells, whereas chemotherapy given in combination capitalizes on different mechanisms of action of the chemotherapy for achieving greater cell kill and preventing resistant cell lines.
La quimioterapia convencional por lo general se dosifica según el área de superficie corporal (BSA), que se calcula con la altura y el peso del paciente. Por ejemplo, si una dosis de 20mg/m
2 de la BSA de
un paciente es 2, la dosis será de 40 mg. Con mucha frecuencia, la quimioterapia de agente único tiene un rol paliativo, pero generalmente es menos tóxica para las células cancerosas, en tanto que la quimioterapia combinada aprovecha los distintos mecanismos de acción de la quimioterapia para matar más células y prevenir las líneas celulares resistentes.
10
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Dosing Strategies (continued)Dosing Strategies (continued)Dosing Strategies (continued)Dosing Strategies (continued)
• Dose Intensity - dose delivered over a specified
period of time (mg/m2/week)
– ⇑ dose intensity = ⇑ response rate
– Leukemias, lymphomas, breast, ovarian
• Dose Density - shortening the usual interval between
doses; designed to maximize the drug’s effects on
tumor growth kinetics
– May require growth factor support
Now that we are familiar with dosing chemotherapy, effecting --- effective dosing can be a factor limiting the ability of chemotherapy to achieve a cure. There are generally two types of dosing strategies: dose intensity and dose density. Dose intensity is the total amount of drug administered at one time or over a week, every 28 days for instance. There can be a positive relationship between dose intensity and response rate. However, there is also a correlation with increased toxicity with dose intense regimens. Dose density, on the other hand - you give the drug, give smaller doses of the drug more often, for instance, once a week or every two weeks.
Ahora que conocemos la dosificación de la quimioterapia, una dosificación efectiva puede ser un factor que limite la capacidad de la quimioterapia para lograr una cura. Generalmente hay dos tipos de estrategias de dosificación: intensidad y densidad de la dosis. La intensidad de la dosis es la cantidad total del medicamento administrado una vez o durante una semana, por ejemplo, cada 28 días. Puede haber una relación positiva entre la intensidad de la dosis y la tasa de respuesta. También existe una correlación entre la toxicidad y los regímenes intensos de dosificación. En cuanto a la densidad de la dosis, pueden administrarse menores dosis del medicamento más a menudo, como una vez por semana o cada dos semanas.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Common Drug Therapy ToxicitiesCommon Drug Therapy ToxicitiesCommon Drug Therapy ToxicitiesCommon Drug Therapy Toxicities
• Gastrointestinal toxicity
• Cardiotoxicity
• Neurotoxicity
• Hepatotoxicity
• Nephrotoxicity
• Dermatologic toxicity
• Myelotoxicity
The ideal chemotherapeutic medication will kill tumor cells and spare normal cells. Unfortunately, this is not the case when it comes to most --- most chemotherapy. Toxicities from chemotherapy can potentially affect any organ in the body and result in affecting both the patient’s quality of life and treatment outcomes. I will spend some time going over some of the toxicities of chemotherapy.
La medicación quimioterapéutica ideal mata las células tumorales y deja ilesas a las células normales. Desafortunadamente, esto no sucede en la mayor parte de las quimioterapias. Las toxicidades de la quimioterapia pueden afectar un órgano del cuerpo y perjudicar tanto la calidad de vida como los resultados del tratamiento del paciente. Hablaremos sobre algunas de las toxicidades de la quimioterapia,

11
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Drug Therapy ToxicityDrug Therapy ToxicityDrug Therapy ToxicityDrug Therapy Toxicity
• Factors that may influence treatment toxicity
– Dose of chemotherapy
• High dose vs. low dose
– Treatment schedule
• Weekly vs. biweekly vs. monthly
– Combination therapy
• Anthracycline with antimetabolite
– Patient specific factors
• Age, BSA, organ function, comorbidities,
response to prior therapies
– Method of administration
• Continuous vs. bolus
– Drug-drug and drug-herbal interactions
But, before we do this, there are many factors that influence treatment toxicity, for instance the dose of chemotherapy, the treatment schedule, whether the chemotherapy is given in combination or as a single agent, and patient-specific factors, such as age. Elderly patients have less --- are less tolerable of chemotherapy, oftentimes because they might have poor organ function or other comorbidities. Additionally, the method of administration, whether it is given continuous versus bolus, can affect the toxicity of the drug. And you have to consider other drugs and herbal products when giving chemotherapy as well.
pero, antes de eso, mencionemos que hay varios factores que inciden en la toxicidad del tratamiento, por ejemplo, la dosis de la quimioterapia, el programa de tratamiento, si la quimioterapia es combinada o de agente único, y los factores particulares del paciente, como la edad. Los pacientes mayores tienen menos tolerancia a la quimioterapia, a menudo por sus pobres funciones orgánicas y otras comorbilidades. El método de administración, sea continua o en bolos, también puede afectar la toxicidad del medicamento. Cuando se administra quimioterapia, es preciso considerar otros medicamentos y productos herbales.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Gastrointestinal ToxicityGastrointestinal ToxicityGastrointestinal ToxicityGastrointestinal Toxicity
• Nausea and vomiting
– Most common early manifestation of toxicity
– Mechanisms
• Stimulation of chemoreceptor zones
• Damage to gastrointestinal mucosa
• Alterations in taste and smell
• Five distinct clinical syndromes
– Acute: < 24 hours after chemotherapy
– Delayed: ≥ 24 hours after chemotherapy
– Breakthrough: Symptoms despite prophylaxis
– Refractory: Ineffective treatment
– Anticipatory: Symptoms prior to therapy
Nausea and vomiting are common side effects of chemotherapy and are feared by most patients. In the setting of chemotherapy, nausea and vomiting is medically known as chemotherapy-induced nausea and vomiting. It is often the first side effect of patients that --- it is often the first side effect patients experience. Nausea and vomiting can be characterized as acute, occurring within the first 24 hours of starting chemotherapy, or delayed nausea and vomiting occurs within 24 hours after chemotherapy. Breakthrough nausea and vomiting is that which occurs despite being on medication to preventive it. Refractory nausea and vomiting is that that does not respond at all to treatment. Finally, anticipatory nausea and vomiting is when a patient experiences symptoms prior to starting their next cycle of chemotherapy.
Las náuseas y los vómitos son efectos secundarios comunes de la quimioterapia, y casi todos los pacientes les temen. En la quimioterapia, a las náuseas y los vómitos se los denomina náuseas y vómitos inducidos por la quimioterapia. Suelen ser el primer efecto secundario que sufren los pacientes. Las náuseas y los vómitos pueden caracterizarse como agudos, cuando ocurren dentro de las primeras 24 horas de la quimioterapia, o demorados, si ocurren después de esas 24 horas. Las náuseas y los vómitos intensificados suceden pese a la medicación que los previene. Las náuseas y los vómitos resistentes ocurren en quienes el tratamiento no responde para nada. Finalmente, las náuseas y los vómitos anticipados se dan cuando un paciente experimenta síntomas antes de comenzar su siguiente ciclo de la quimioterapia.

12
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIEmetogenic Potential of Commonly Emetogenic Potential of Commonly Emetogenic Potential of Commonly Emetogenic Potential of Commonly used Agents used Agents used Agents used Agents
NCCN v.1.2010 Antiemesis Practice Guidelineshttp://www.nccn.org/professionals/physician_gls/PDF/antiemesis.pdf
Interestingly, not all chemotherapeutic agents cause the same degree of nausea or vomiting. There are several classification systems that define emetogenicity of chemotherapy. And this helps us choose what kind of antiemesis regimen we will use. Although this table is not all inclusive, it shows examples of chemotherapeutic agents that are thought to be of high emetogenic risk and associated with minimal emetogenic risk. As you may have noticed, the emetogenic potential - some chemotherapy is dose --- dose-dependent.
Lo interesante es que no todos los agentes quimioterapéuticos causan el mismo nivel de náuseas o vómitos. Hay varios sistemas de clasificación que definen la emetogenicidad de la quimioterapia. Esto nos ayuda a elegir la clase de régimen de antiemesis que usaremos. Si bien esta tabla no es taxativa, muestra ejemplos de agentes quimioterapéuticos que se consideran de alto riesgo emetogénico y los asociados a un mínimo riesgo. Habrán notado que el potencial emetogénico de algunas quimioterapias depende de la dosis.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Gastrointestinal ToxicityGastrointestinal ToxicityGastrointestinal ToxicityGastrointestinal Toxicity
• Mucositis
– Inflammatory reaction and ulcerative lesions
of mucosal surfaces
– Most commonly caused by methotrexate,
5-fluorouracil, vinca alkaloids
• Diarrhea
– Common adverse effect of irinotecan
• Constipation
– Common adverse effect of vincristine
And, if nausea and vomiting is not enough, certain agents also destroy the mucosal lining throughout the gastrointestinal tract. Tissue lining this gastrointestinal tract is usually rapidly dividing cells. Hence, these cells are susceptible to the actions of chemotherapy. Agents, such as methotrexate and 5-fluorouracil, can cause mucositis and inflammatory reactions of the mucosal lining. Irinotecan, used for the treatment of colon cancer, almost always causes diarrhea, whereas vincristine does the opposite, causes constipation.
Como si las náuseas y los vómitos no bastaran, ciertos agentes también destruyen el revestimiento mucoso de todo el tubo digestivo. En el tejido que reviste este tubo, las células suelen dividirse rápidamente. Por ende, son susceptibles a la acción de la quimioterapia. Agentes como el metotrexato y el 5-fluorouracilo pueden provocar mucositis y reacciones inflamatorias del revestimiento mucoso. El irinotecán, usado para tratar el cáncer de colon, casi siempre provoca diarrea, en tanto la vincristina produce el efecto opuesto: estreñimiento.

13
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
CardiotoxicityCardiotoxicityCardiotoxicityCardiotoxicity
• Rare but serious complication of cancer therapy
• Incidence and severity depends on agent, dose,
schedule, patient factors, and other treatments
• Cardiomyopathy
– Anthracyclines, interferon
• Ischemia
– Fluorouracil, sorafenib
• Arryhthmias
– Anthracyclines, arsenic, taxanes
• Hypertension
– Bevacizumab, sorafenib
A rare, but serious, complication with some chemotherapy agents is cardiotoxicity. Cardiotox --- Cardiotoxicity can manifest as cardiomyopathy, congestive heart failure, ischemia, arrhythmias, or hypertension. Anthracyclines are well recognized as the agents that cause cardiomyopathies and congestive heart failure when certain cumulative doses of the anthracycline have been reached.
Una complicación poco frecuente, pero grave, con algunos agentes de quimioterapia es la cardiotoxicidad, que puede manifestarse como cardiomiopatía, insuficiencia cardíaca congestiva, isquemia, arritmia o hipertensión. Las antraciclinas son bien reconocidas como los agentes que provocan cardiomiopatía e insuficiencia cardíaca congestiva cuando se han alcanzado ciertas dosis acumulativas.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
NeurotoxicityNeurotoxicityNeurotoxicityNeurotoxicity
• Cerebellar toxicity
– Ataxia, nystagmus, gait and coordination abnormalities
– High dose cytarabine (> 1 gm/m2)
• Encephalopathy
– Confusion, aphasia, headache
– Methotrexate, ifosfamide
• Arachnoiditis
– Headache, nausea/vomiting, fever, photophobia
– Intrathecal methotrexate and cytarabine
• Seizures
– Nelarabine
Neurotoxic effects of chemotherapy occur fairly frequently and are often reasons to limit the dose or delay therapy. Some agents cause both central and peripheral neurotoxicity. For example, high-dose cytarabine, ifosfamide, and nelarabine are commonly known for their central neurotoxic side effects.
Los efectos neurotóxicos de la quimioterapia ocurren con bastante frecuencia y suelen constituir motivos para limitar la dosis o demorar la terapia. Algunos agentes provocan neurotoxicidad tanto central como periférica. Por ejemplo, las altas dosis de citarabina, ifosfamida y nelarabina son conocidas por sus efectos secundarios neurotóxicos centrales.

14
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Neurotoxicity (continued)Neurotoxicity (continued)Neurotoxicity (continued)Neurotoxicity (continued)
• Peripheral neuropathy
– Manifest as stocking-glove like distribution,
pain, tingling
– Vinca Alkaloids
• Vincristine
– Platinum Analogs
• Cisplatin and oxaliplatin
– Taxanes
• Paclitaxel > Docetaxel
Chemotherapy can also induce peripheral neuropathy that is related to the cumulative dose and the type of drug used. The vinca alkaloids, the platinum analogs, and the taxanes are notorious for inducing peripheral neuropathy. The early signs and symptoms are pain or tingling in the hands and feet and sometimes loss of reflexes. And this is usually a reason for delaying or reducing the dose of the next cycle.
La quimioterapia también puede inducir la neuropatía periférica relacionada con la dosificación acumulativa y el tipo de medicamento usado. Los alcaloides de la vinca, los análogos de platino y los taxanos son conocidos por inducir la neuropatía periférica. Los primeros signos y síntomas son dolor o cosquilleo en las manos y los pies, y a veces pérdida de reflejos. Esta suele ser la razón para demorar o reducir la dosis del siguiente ciclo.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Neurotoxicity (continued)Neurotoxicity (continued)Neurotoxicity (continued)Neurotoxicity (continued)
• Constipation, Bowel obstructions
– Vinca alkaloids, cisplatin
• Ocular Toxicity
– Chemical conjuctivitis
– High dose cytarabine
• Ototoxicity
– Loss of high frequency ranges,
acute tinnitus, chronic hearing loss
– Cisplatin
And some --- additional neurotoxic effects can involve the bowel system, the eyes, and the ears.
Ciertos efectos neurotóxicos adicionales pueden involucrar el sistema intestinal, los ojos y los oídos.

15
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
HepatotoxicityHepatotoxicityHepatotoxicityHepatotoxicity
• Hepatotoxicity manifests in a variety of patterns
– Hepatocellular necrosis - acute toxicity
– Cholestasis - impaired flow of bile from liver to duodenum
– Steatosis - fatty liver
– Veno-occlusive disease (VOD) - injury to hepatic venous
endothelium
• Hepatocellular injury is generally reversible and nonfatal
• Many drugs require dose reduction or avoidance in the
setting of hepatic insufficiency
• Hepatotoxic agents include: vinca alkaloids, cytarabine,
methotrexate, clofarabine, gemtuzumab, imatinib,
L-asparaginase
Chemotherapy can also cause hepatotoxicity that can manifest as elevated liver function tests, cholestasis, and veno-occlusive disease, which is injury to the hepatic venous endothelium. Many of these drugs are cleared through the liver, hence, will require dose adjustment in the setting of hepatocellular injury or reduced liver function. I’ve provided a list of drugs that are typically hepatotoxic or hepatically-cleared agents. Some of them include vinca alkaloids, cytarabine, methotrexate, clofarabine, imatinib, and L-asparaginase.
La quimioterapia también puede provocar hepatotoxicidad, que se manifiesta como resultados elevados en pruebas de la función hepática, colestasis y enfermedad venooclusiva, una lesión del endotelio venoso hepático. Muchos de estos medicamentos son eliminados por el hígado, por lo que requieren un ajuste de dosis en el contexto de una lesión hepatocelular o de función hepática reducida. Esta es una lista de medicamentos normalmente hepatotóxicos y agentes eliminados hepáticamente. Algunos de ellos son los alcaloides de la vinca, la citarabina, el metotrexato, la clofarabina, el imatinib y la L-asparaginasa.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
NephrotoxicityNephrotoxicityNephrotoxicityNephrotoxicity
• Chemotherapy can impair kidney function
• Impairment can range from asymptomatic elevations
of serum creatinine to renal failure requiring dialysis
– Methotrexate and cisplatin are well-known nephrotoxins
• Impaired renal function can increase systemic
toxicities
• Many drugs require dose reduction or avoidance in
the setting of renal insufficiency
– Cytarabine, methotrexate, cisplatin, carboplatin, etoposide
And you cannot forget about nephrotoxicity. Many of the chemotherapy agents are renally cleared through the kidneys. Two common agents are methotrexate and cisplatin. They are both renally eliminated and cause --- can cause renal insufficiency or renal failure. Impaired renal function can increase systemic toxicities. Hence many drugs require dose reduction or avoidance in the setting of renal insufficiency.
No olvidemos la nefrotoxicidad. Muchos de los agentes de la quimioterapia se eliminan a través de los riñones. Dos agentes comunes son el metotrexato y el cisplatino. Ambos son eliminados renalmente y pueden provocar insuficiencia renal. Las dificultades en la función renal pueden aumentar las toxicidades sistémicas. Por lo tanto, varios medicamentos requieren que se reduzca la dosis o se los evite en caso de insuficiencia renal.