practical aspects of assessing tumors using clinical
TRANSCRIPT

211
*Corresponding author, Phone: +44-208-661-3340, E-mail:dowmukoh@icr.ac.uk
211
Magn Reson Med Sci, Vol. 6, No. 4, pp. 211–224, 2007
REVIEW
Practical Aspects of Assessing Tumors Using Clinical DiŠusion-weighted Imaging in the Body
Dow-Mu KOH1*, Taro TAKAHARA2,3, Yutaka IMAI2, and David J COLLINS1
1CR UK Clinical Magnetic Resonance Research Group, Institute of Cancer Research andAcademic Department of Radiology, Royal Marsden Hospital
Downs Road, Sutton SM2 5PT, UK2Department of Radiology, Tokai University Hospital, Japan3Division of Radiology, Radiotherapy and Nuclear Medicine,
University Medical Centre, Utrecht, Netherlands(Received July 23, 2007; Accepted September 5, 2007)
DiŠusion-weighted magnetic resonance (MR) imaging (DWI) is increasingly applied toevaluate tumors in the abdomen and pelvis. However, DWI is susceptible to a variety of ar-tifacts that arise from motion, use of strong gradient pulses, and echo-planar imaging tech-nique. We discuss practical issues to help radiologists optimize the use of DWI to evaluatetumors in the body, including breath-hold DWI, multiple-acquisition non-breath-holdDWI, and diŠusion-weighted whole-body imaging with background body signal suppres-sion (DWIBS). Considerations of meticulous technique, sequence optimization, and quali-ty assurance are emphasized for consistent acquisition of high quality images. We illustratethe potential use of these techniques to detect and characterize tumors and to monitortreatment eŠects.
Keywords: magnetic resonance imaging, diŠusion, technique
Introduction
DiŠusion-weighted magnetic resonance imaging(DWI) probes the diŠusion of water in the body.The motion of water molecules in the extra- and in-tracellular spaces and intravascular space contrib-utes to the net water displacement measured byDWI. The technique yields qualitative and quan-titative information that re‰ects tissue cellularityand cell membrane integrity and thus complementsmorphological information obtained by conven-tional MR imaging.
Performing DWI in the body is challenging be-cause the inhomogeneity of the magnetic ˆeld overa large imaging area and motion arising fromdiŠerent organs conspire to degrade image quality.In the past decade, a series of technological ad-vancements in MR imaging, including higher am-plitude gradients, echo-planar imaging (EPI),parallel imaging techniques, and the use of respira-tory gating and cardiac triggering for motion com-pensation, has helped overcome many of these is-
sues. Of these, the development of parallel imaginghas been critical because its enables use of veryshort echo time and reduced echo-train length forvery quick acquisition of images with good signal-to-noise that are relatively undegraded by motionand local ˆeld gradients.
High quality DWI images can be routinely ob-tained using modern 1.5T MR imaging systemsfrom the major manufacturers (e.g., General Elec-tric, Milwaukee, USA; Siemens, Erlangen, Germa-ny; Philips, Eindhoven, The Netherlands). How-ever, implementation of DWI sequences diŠersamong manufacturers, and the reader should befamiliar with the strengths and limitations of theirown imaging systems to optimize imaging perform-ance. In this regard, the radiologist should workclosely with the physicist and technologist in estab-lishing scanning protocols to ensure acquisition ofimages of consistently high quality.
We discuss the advantages and disadvantages ofcommonly applied DWI strategies in the body andimportant considerations for image optimization toensure high quality images for qualitative visual as-sessment or quantitative analysis, and we illustratethe potential use of these techniques to detect and

212
Table. DiŠusion-weighted MR imaging sequences for evaluating tumors in the body*
TechniqueBreath-hold single-shot
echo-planar (EPI) diŠusion-weighted imaging (DWI)
Free-breathing multipleaveraging single-shot
EPI DWI
Whole-body DWI withbackground suppression
Field of view 340–400 cm 340–400 cm 380–400 cmMatrix size 112×256 112×256 160×256Repetition time 2500 3900 À3500 msEcho time 56–68 ms 78 72 msFat suppression SPAIR SPAIR/STIR STIREPI factor 65 59 47Parallel imaging factor 2 2 2NSA Single-shot 5 6Section thickness 7 mm contiguous 5 mm 4 mm/1 mm overlapDirections of motion-probing gradients
Phase, frequency, and slice Phase, frequency, and slice Phase, frequency, and slice
b-factors (s/mm2) usually3 b-values (e.g., 0, 100, 500s/mm2)
allows multiple b-values(e.g., 0, 50, 100, 250, 500,750 s/mm2)
0 and 1000 s/mm2
* Imaging protocols as implemented on a Philip's 1.5T magnetic resonance imaging systemSTIR=Short-tau inversion recoverySPAIR=Spectral selected attenuated inversion recovery
212 D-M. Koh et al.
Magnetic Resonance in Medical Sciences
characterize tumors and to demonstrate treatmentresponse. We assume knowledge of and will notdiscuss the basic principles of DWI.1
DWI Imaging Strategies in the Body
DWI imaging in the body is frequently per-formed using modiˆed single and dual spin-echo se-quences with the application of motion-probinggradients placed on either side of the 1809refocus-ing pulses. This is combined with echo-planar imag-ing (EPI) readout and parallel acquisition tech-niques (e.g. SENSE, GRAPPA) to minimize imag-ing time, thus preserving image signal-to-noise andreducing motion-related artifacts, without sig-niˆcantly impacting apparent diŠusion coe‹cient(ADC) calculations.2
Current widely used imaging strategies for DWIin the body include: (1) breath-hold single-shotDWI, (2) non-breath-hold multiple averagingDWI, and (3) non-breath-hold multiple averagingDWI performed at multiple body stations (diŠu-sion-weighted whole-body imaging with back-ground body signal suppression [DWIBS]). Al-though each of these strategies is suitable for gener-al imaging of the abdomen and pelvis, the selectionof imaging sequence may be in‰uenced by the ana-tomical region being investigated, whether the im-ages are to be analyzed qualitatively or quantita-tively, and the size and heterogeneity of lesionsevaluated. Table summarizes typical examples of
these imaging approaches.Breath-hold single-shot DWI. The key advantage
of using breath-hold single-shot DWI is the shortimage acquisition time. For example, the entireliver can be evaluated over 2 breath-holds, eachlasting only 20 s. Combining parallel imaging andsingle-shot EPI measurements allows very shortecho times (e.g., 45 to 75 ms), thereby preservingsignal-to-noise.3,4 Furthermore, breath-hold single-shot DWI would be theoretically more eŠective incharacterizing lesion heterogeneity (e.g., on a pixel-by-pixel basis) and in quantifying the ADC ofsmaller lesions because such information is lesslikely to be degraded by the volume averaging thatoccurs with free-breathing techniques.
However, single-shot measurements are inher-ently noisy because of the low signal-to-noise of thesource data. Although artifacts arising frombreathing motion are reduced, pulsatile motionfrom the heart and the aorta can still induce ar-tifacts. Therefore, some advocate combining thistechnique with cardiac pulse triggering to improveimage quality and ADC calculation.5 However, theuse of pulse triggering increases image acquisitiontime and may render the images more prone to bulkmotion. Cardiac pulsation artifacts have beenshown to increase ADC measurement in the leftlobe of the normal liver compared with the rightlobe.6 The need for good signal-to-noise also meansthat breath-hold imaging may require thicker slicepartitions (6 to 8 mm). Another potential disadvan-

213213Clinical DWI in the Body to Assess Tumors
Vol. 6 No. 4, 2007
tage of this technique is the number of b-values thatcan be accommodated within a single breath-hold,which may have bearing on the accuracy of ADCdetermination.
Free-breathing multiple-averaging DWI. Theprinciple advantages of free-breathing multiple-averaging DWI are that signal averaging allows useof multiple b-values and thin slice partitions (e.g. 4to 5 mm) and the technique yields images with highsignal-to-noise. These images can be qualitativelyassessed using multi-planar reconstruction (MPR)or maximum intensity projection (MIP) (Fig. 1).7
In addition, DWI or ADC maps may be eŠectivelylaid over morphological information to produce fu-sion images that combine diŠusion-weighted func-tional information with anatomical details (Fig. 1).Using multiple b-values also enables evaluation ofthe ADC of lesions. Thus, free-breathing multipleaveraging DWI appears to be a versatile techniquethat allows good use of DWI images for bothqualitative and quantitative analysis.
However, ADC calculation using this techniquemay be less optimal in characterizing smaller le-sions or in reporting lesion heterogeneity becauseof volume averaging. So, there is considerable in-terest in combining such sequences with respirato-ry8,9 and cardiac triggering techniques to improveimage registration and ADC assessment. Not sur-prisingly, it has been shown that compared withfree-breathing acquisition, the use of respiratorytriggering in the liver lead to better contrast-to-noise ratio and a decrease in the scattering of ADCvalues.8 However, implementing such a scheme inclinical imaging is challenging because it may fur-ther increase the already noticeable scan time of 4to 6 min for each acquisition. Novel techniques thatenable more e‹cient gains in signal acquisition dur-ing respiratory gating are being investigated and de-veloped.
DiŠusion-weighted whole-body imaging withbackground body signal suppression (DWIBS).DWIBS was conceived primarily as a method tovisualize tumors in the body by their restrictedwater mobility. Because these images are usuallyevaluated qualitatively, only b-values of 0 and 1000s/mm2 are employed. Fat suppression and high b-value are used to maximize background suppres-sion. Free-breathing multiple averaging DWI isrepeated at contiguous imaging stations. The im-ages are processed by MIP, composed together anddisplayed using an inverted gray scale.7 The datasetcan also be visualized in 3D using MPR and volumerendered (VR) displays (Fig. 2).
Signals from normal tissue, such as blood ves-sels, fat, muscle and bowel are usually suppressed,
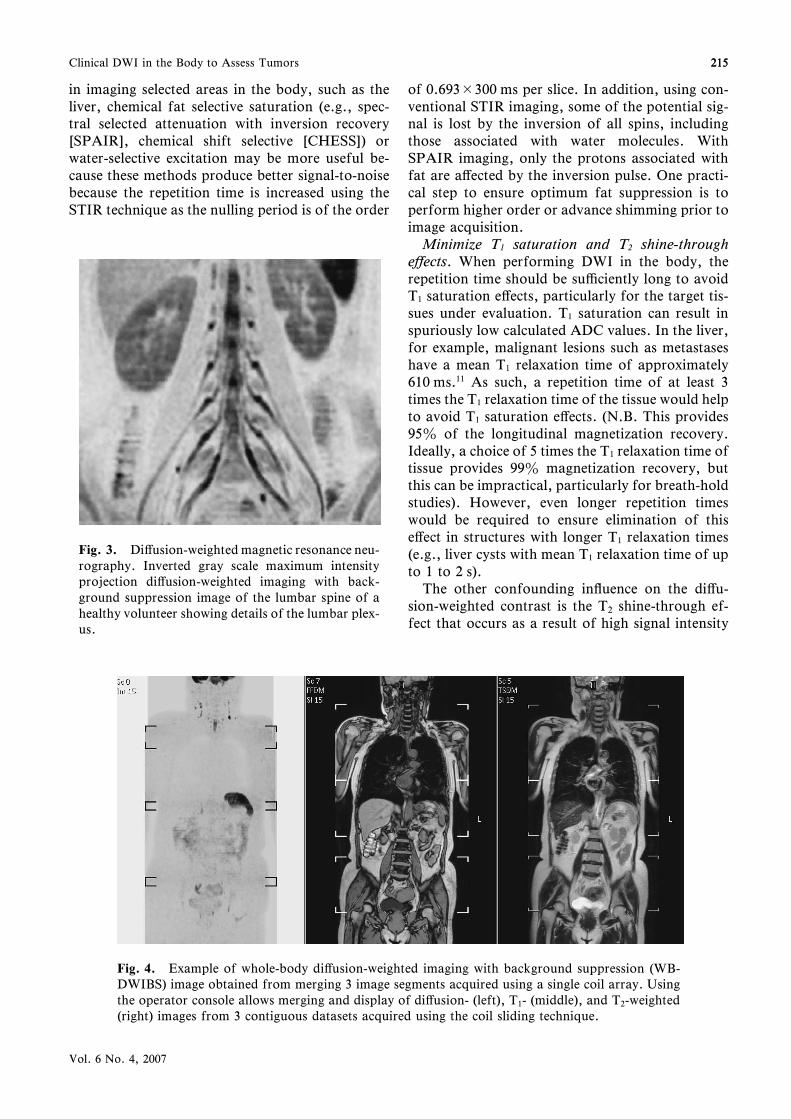
whereas other normal structures, such as thespleen, prostate, testes, ovaries, endometrium, andspinal cord, remain visible.7 DWIBS detects notonly tumor (i.e., restricted diŠusion) but alsohyperviscous ‰uids (i.e., nonrestricted diŠusionwith hyperviscosity), such as abscesses. The tech-nique appears promising for detecting tumors ofsmall volume in the lymph nodes, peritoneum, andother sites of occult disease.7 It can also be used tovisualize peripheral nerves as diŠusion-weightedMR neurography (Fig. 3).10
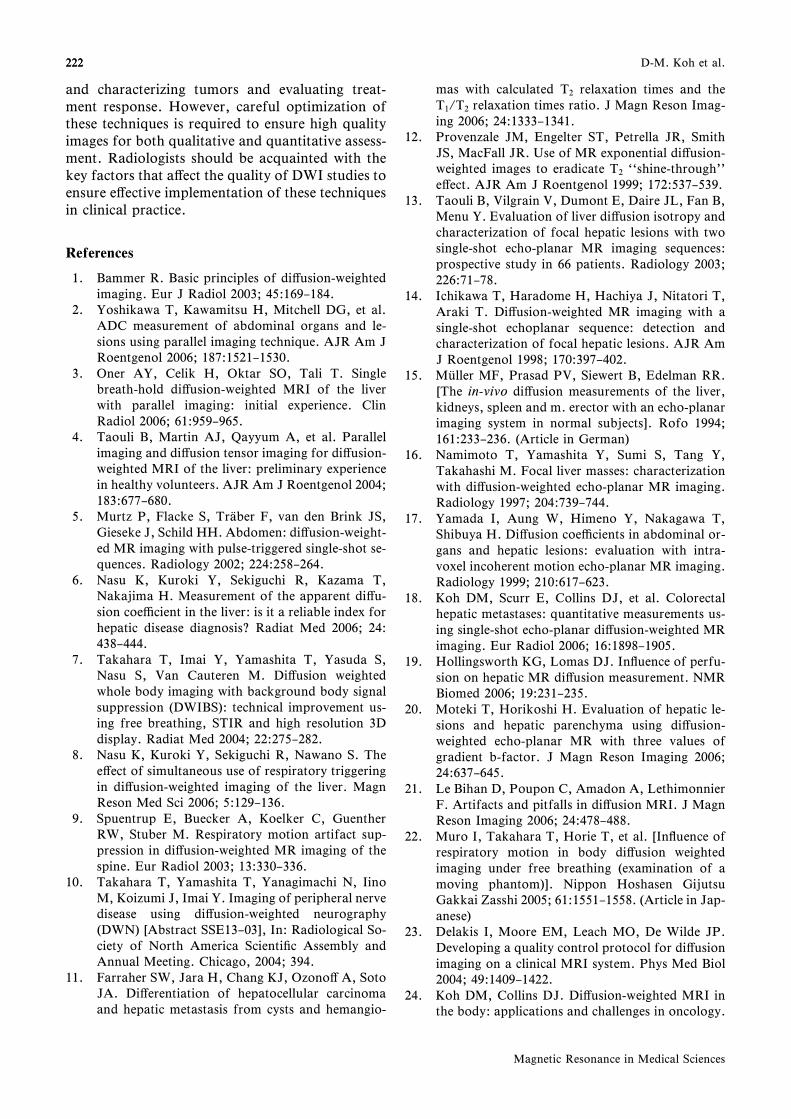
DWIBS can be obtained using a sophisticatedwhole-body coil array system, like the total imagingmatrix system (TIM, Siemens Medical Solutions,Malvern, Pennsylvania) or other commerciallyavailable long coil arrays. However, such imagingcan also be achieved using just a single coil array.To do this, the patient lies on a table extensionelevated from the MR table-top at the 2 ends byspacers. A 4-cm gap between the table extensionand the MR table-top allows the posterior coil ele-ments to be placed under the patient. Placing theposterior coil in this gap enables movement of itselement freely to another imaging station withoutmoving the patient or altering the referenced scanposition. In this way, images acquired at diŠerentimaging stations can be composed to yield a whole-body image (Fig. 4).
DWIBS shares many of the advantages of free-breathing multiple averaging DWI, such as thin im-age partitions and good signal-to-noise. Its maindisadvantage is the relatively long image acquisi-tion time required to evaluate the entire body.
Optimization of DWI in the Body
The image contrast at DWI relies on intrinsicdiŠerences in the water diŠusion between tissues.To maximize this contrast to detect and character-ize lesions, scanning parameters must be chosenthat optimize signal and contrast-to-noise betweenthe tumor and surrounding tissues and thatminimize artifacts and other eŠects that may modi-fy or confound the native diŠusion-weighted con-trast. Appreciation of these factors will help theradiologist make informed decisions at clinicalscanning.
Fat suppression. Fat suppression is routinely em-ployed to increase the dynamic range of the DWIimages and reduce the chemical shift-inducedghosting that is prevalent in EPI. When performingDWI over a large area of the body, an inversion-recovery (e.g., STIR) approach is preferred becauseit is likely to produce more uniform fat suppressionand is the method adopted for DWIBS. However,

214
Fig. 1. Free-breathing multiple averaging diŠusion-weighted imaging. Study in a 54-year-old woman shows alarge mass within the rectouterine pouch that demonstrates restricted diŠusion on the b=750 s/mm2 image dis-played using an inverted gray scale. Thin image partitions produce images of good signal-to-noise that allow mul-ti-planar reformats. Note the corresponding T2-weighted image and the apparent diŠusion coe‹cient map. ThediŠusion-weighted axial image could also be displayed using a color scale (tumor colored red and orange) andfused with the T2-weighted image to provide combination of functional and anatomical information.
Fig. 2. Three-dimensional displays of diŠusion-weighted images with background suppression (DWIBS) tech-nique. A 66-year-old woman with bladder cancer. (a) Axial T2-weighted image shows large bladder cancer in theposterior wall and small daughter nodule anteriorly. (b) T2-weighted magnetic resonance urography showsbilateral hydronephrosis from obstruction of the ureterovesicle junctions. (c) Maximum intensity projection ofDWIBS image showing main tumor and metastatic left common iliac nodes. (d) Axial reformat (8-mm slice thick-ness, obtained from 4-mm source image) demonstrates metastatic left iliac nodes. (e) Sagittal reformat showsmain posterior tumor and small anterosuperior daughter nodule. (f) Volume rendering image shows 3D shape ofthe tumor. Images (c) to (f) are derived from one thin section data set.
214 D-M. Koh et al.
Magnetic Resonance in Medical Sciences
215
Fig. 4. Example of whole-body diŠusion-weighted imaging with background suppression (WB-DWIBS) image obtained from merging 3 image segments acquired using a single coil array. Usingthe operator console allows merging and display of diŠusion- (left), T1- (middle), and T2-weighted(right) images from 3 contiguous datasets acquired using the coil sliding technique.
Fig. 3. DiŠusion-weighted magnetic resonance neu-rography. Inverted gray scale maximum intensityprojection diŠusion-weighted imaging with back-ground suppression image of the lumbar spine of ahealthy volunteer showing details of the lumbar plex-us.
215Clinical DWI in the Body to Assess Tumors
Vol. 6 No. 4, 2007
in imaging selected areas in the body, such as theliver, chemical fat selective saturation (e.g., spec-tral selected attenuation with inversion recovery[SPAIR], chemical shift selective [CHESS]) orwater-selective excitation may be more useful be-cause these methods produce better signal-to-noisebecause the repetition time is increased using theSTIR technique as the nulling period is of the order
of 0.693×300 ms per slice. In addition, using con-ventional STIR imaging, some of the potential sig-nal is lost by the inversion of all spins, includingthose associated with water molecules. WithSPAIR imaging, only the protons associated withfat are aŠected by the inversion pulse. One practi-cal step to ensure optimum fat suppression is toperform higher order or advance shimming prior toimage acquisition.
Minimize T1 saturation and T2 shine-througheŠects. When performing DWI in the body, therepetition time should be su‹ciently long to avoidT1 saturation eŠects, particularly for the target tis-sues under evaluation. T1 saturation can result inspuriously low calculated ADC values. In the liver,for example, malignant lesions such as metastaseshave a mean T1 relaxation time of approximately610 ms.11 As such, a repetition time of at least 3times the T1 relaxation time of the tissue would helpto avoid T1 saturation eŠects. (N.B. This provides95z of the longitudinal magnetization recovery.Ideally, a choice of 5 times the T1 relaxation time oftissue provides 99z magnetization recovery, butthis can be impractical, particularly for breath-holdstudies). However, even longer repetition timeswould be required to ensure elimination of thiseŠect in structures with longer T1 relaxation times(e.g., liver cysts with mean T1 relaxation time of upto 1 to 2 s).
The other confounding in‰uence on the diŠu-sion-weighted contrast is the T2 shine-through ef-fect that occurs as a result of high signal intensity

216
Fig. 5. Overcoming T2 shine-through using apparent diŠusion coe‹cient (ADC) maps. (a) T1-weighted axial image of the liver showing a small cyst (arrow) and larger metastases (arrowhead).(b) At diŠusion-weighted imaging, both cyst and metastasis return high signal on b=500 s/mm2
image. (c) The ADC map conˆrms the cyst as showing high ADC (bright) compared with themetastases, which return a low ADC value.
Fig. 6. Signal attenuation in intra-abdominal or-gans. Graph showing biexponential signal attenua-tion in major intra-abdominal organs with increasingdiŠusion weighting. Note the initial rapid signal at-tenuation with a small increase in b-value, followedby a more gradual slope of signal attenuation beyondapproximately b=100 s/mm2.
216 D-M. Koh et al.
Magnetic Resonance in Medical Sciences
returned from tissues with long intrinsic T2 relaxa-tion times contributing to the overall measureddiŠusion-weighted signal. Visual assessment alonemay falsely ascribe the high signal intensity ob-served to restriction in water diŠusion. This phe-nomenon is more di‹cult to avoid but may beovercome by using an exponential image12 or cal-culating the ADC (Fig. 5).
Choice of b-values. When choosing the magni-tude and number of b-values to be applied forDWI, considerations should include the DWI tech-nique used, the anticipated image signal-to-noise,the target organ being evaluated, and whether DWIis primarily used for qualitative or quantitativeanalysis.
When DWI is performed with increasing b-values, the attenuation of the signal intensity in ab-dominal organs has been shown to be biexponentialfor the range used for clinical imaging in the body(e.g., b=0 to 1000 s/mm2). An initial rapid de-crease in signal intensity with a small increase inb-value is followed by a more gradual slope of sig-nal attenuation as the b-value increases further. Asummary plot derived from published literaturevalues and our own experiments suggests that theinitial rapid signal attenuation extends to a b-valueof about 100 s/mm2 (Fig. 6).
With this in mind, the use of only 2 b-values atDWI13 will not adequately characterize this biex-ponential behavior, but it would be possible to der-ive ADC calculations to re‰ect this phenomenonusing at least 3 b-values. An ADC calculated usingonly low b-values (Ã100 s/mm2; sometimes re-ferred to as ADCfast or ADClow) will be sensi-tive to intravoxel capillary perfusion. By contrast,
ADC calculations derived from images of b-valuesgreater than 100 s/mm2 (sometimes referred to asADCslow or ADChigh) will be relatively perfusioninsensitive and theoretically more re‰ective of tis-sue cellularity and the integrity of cellular mem-branes. Of course, ADC can still be calculated overan entire range of b-values, and such an approachhas been established in clinical practice for many

217
Fig. 7. Evaluating treatment response. Assessment of response made using free-breathing multipleaveraging diŠusion-weighted imaging, (a) apparent diŠusion coe‹cient (ADC)fast and (b) T2-weighted image showing an irregular 3-cm left inguinal node (arrow) in a 54-year-old woman withmetastatic ovarian cancer. (c) Box and Whisker plots of the pixel values of ADCfast and ADCslowwithin a region of interest drawn over the lymph node before and at one week after treatment with anovel antivascular drug. Lines through boxes indicate median ADC value, and the whiskers indicatethe 5th and 95th percentile values. Rounded circles deˆne the 95z conˆdence interval. After treat-ment, there was a signiˆcant decrease in the ADCfast with a contemporaneous signiˆcant increase inthe ADCslow (Pº0.001, Wilcoxon signed rank test).
217Clinical DWI in the Body to Assess Tumors
Vol. 6 No. 4, 2007
years. Indeed, the intravoxel incoherent motion(IVIM) equation has been applied to characterizethe biexponential behavior. However, fractionatingthe ADC calculations into ADCfast and ADCslowmay potentially be more informative, especially forevaluating treatment response, because drug treat-ment (e.g., antiangiogenic drug) may reduce blood‰ow (decrease ADCfast) and tissue cellularity (in-crease ADCslow) with little change in overall ADCvalue. (Fig. 7)
The in‰uence of the choice of b-value on ADCcalculations can be observed in the literature.For example, in liver metastases, ADC values cal-culated using relatively low b-values (e.g.,º100s/mm2)14 are higher than ADC calculationsobtained using larger b-values (e.g.,À100 s/mm2).13,15–17 It has also been shown that the meanADC of colorectal liver metastases calculated overa range of b-values (0, 150, and 500 s/mm2) ishigher than that calculated using higher b-valuesonly (150 and 500 s/mm2).18 Similarly, ADCfastcalculated using low b-values are usually higherthan ADCslow derived from higher b-values (Fig.8). More recently, it was shown in normal volun-teers that portal perfusion exerted a signiˆcanteŠect when a b-value of 200 s/mm2 was used, andthe ADC measurement of the liver was morereproducible when only higher b-values (b=500and 750 s/mm2) were employed.19
Although it may seem prescriptive to recommendb-values for tumor imaging in the body, DWI for
quantifying tumor ADC should include a range ofb-values that enables calculation of the ADCfastand ADCslow. When using non-breath-hold multi-ple averaging DWI imaging, multiple b-values canbe employed to achieve this (e.g., b=0, 50 100,250, 500, 750 s/mm2). However, when breath-holdimaging is used, there is a limit to the number of b-values that can be accommodated within eachbreath-hold without increasing the echo or acquisi-tion time. Thus, the choice of 3 appropriate b-values (e.g., b=0, 100, 500 s/mm2) is practicalwhen using breath-hold imaging and still enablesthe fractionating of the ADCs.
Some authors have employed very low b-values(e.g., b=3 s/mm2) for DWI study.20 However, en-suring the validity of these small b-values requiresproper account of the diŠusion weighting intro-duced by the imaging sequence read-out gradients.Furthermore, some MR systems do not permit theuse of very low b-value. Hence, to facilitate mean-ingful data comparison between centers, it wouldbe useful to ensure that the smallest diŠusionweight-ing applied for imaging can be eŠectively achievedon other MR systems.
When performing DWIBS, a higher b-value(1000 s/mm2) is typically used to maximize back-ground signal attenuation and suppression.7 How-ever, it has to be remembered that the greater sig-nal attenuation at higher b-values usually requiresa larger number of signal averages (e.g., n=4 to6) to maintain good signal and contrast-to-noise.

218
Fig. 8. Apparent diŠusion coe‹cient (ADC)fast and ADCslow. (a) T2-weighted magnetic resonance imaging showing a 4-cm left external iliac lymphnode (arrow). A similar region of interest was drawn encompassing the node(arrows) on the (b) ADCfast (from b=0 and 150 s/mm2 images) and (c)ADCslow (from b=150 and 500 s/mm2 images) maps. (d) The mean ADCfastwas higher than the mean ADCslow (gray bars). Individual pixel values withinthe region of interest are plotted as black dots.
218 D-M. Koh et al.
Magnetic Resonance in Medical Sciences
Motion-probing gradients. Because water diŠu-sion in tumors and major abdominal organs (exceptthe kidneys) is typically isotropic, it has been sug-gested that the motion-probing gradient can be ap-plied in just a single direction in abdominal organsshowing isotropic diŠusion.13 However, it may stillbe useful to perform DWI using 3 orthogonalmotion-probing gradients in the body to yield bothdirectional and trace DWI images. One clear ad-vantage of calculating the trace image is an im-provement in the signal-to-noise ratio by squareroot of 3 in isotropic regions. In nonisotropicregions (e.g., the kidneys), the trace provides adirection-independent estimate of diŠusivity. Rev-iew of the directional DWI images can also be help-ful when random susceptibility, motion, or EPI ar-tifacts that are present in images of one directionpropagate to degrade the trace image.
The use of tetrahedral encoding allows 3 or-thogonal motion-probing gradients to be appliedsimultaneously. Tetrahedral encoding provides the
ability to reduce echo-time by combining gradientsto obtain high b-values with shorter lengths ofMPGs. The reduced echo-time can substantiallyimprove image quality and signal-to-noise and canbe used as a strategy to improve the quality of DWIimages, but the individual directional images areusually not available for review. Nevertheless, sucha technique has been successfully implemented forimaging in the body, including multiple-averagingnon-breath-hold DWI.
Reducing artifacts. DiŠusion-weighted MR imag-ing is susceptible to a range of artifacts related tomotion, EPI, and susceptibility eŠects. A detailedaccount of these is beyond the scope of this article,and the reader is referred to an excellent recentreview.21
Perhaps, it is worth re‰ecting upon the nature ofmotion to which DWI is susceptible. Motion in thebody can be thought of as either incoherent or co-herent. The former leads to phase dispersion by themotion-probing gradient and results in signal de-

219
Fig. 9. EŠect of motion on apparent diŠusion coe‹cient (ADC) measure-ments. ADC map of phantoms containing water (W; left), fat (F; middle), anddetergent (A; right) embedded in agar. The phantom was scanned moving alongthe axis of the magnetic resonance scanner simulating respiration. Graphs showthe calculated ADC values measured when the phantom was moving at speed of10 mm/s (lower left) and 20 mm/s (lower right) in the diŠerent directions ofmotion-probing gradients and b-values compared with measurements takenwhen stationary. Note that the errors for ADC measurement were less than 0.1.This suggests that coherent motion may not aŠect the ADC measurements.(Permission for reprint obtained by Dr. Takahara from the Nippon HoshasenGijutsu Gakkai Zasshi 2005; 61:1551–1558).
219Clinical DWI in the Body to Assess Tumors
Vol. 6 No. 4, 2007
crease at DWI. However, the latter leads only tophase shift and so does not result in signiˆcant sig-nal attenuation.
Interestingly, respiratory movement can beviewed as analogous to coherent motion. Muro andcolleagues22 demonstrated this eŠect in an experi-ment using ‰uid-ˆlled phantoms that movedperiodically in their long axes along the z-directionof the MR system to simulate respiratory motion.They found that such motion resulted in less than10z error in ADC measurements of the ‰uid in thephantom (Fig. 9), and their results suggested thatuniform respiratory motion may not lead to sig-niˆcant decrease in DWI signal or substantial er-rors in ADC measurements, especially over a largenearly uniform structure (e.g., liver). However,respiratory motion can still result in ADC errors insmall focal lesions, caused by contamination of sig-nal from adjacent tissues. In addition, movementof the diaphragm at higher speed (or wider excur-sion) can still lead to blurring of small objects andADC errors. Bowel peristalsis can also be consid-ered coherent motion (Fig. 10). By contrast, cardi-
ac motion appears to be largely incoherent andcan result in severe signal loss in the mediastinumor over the left lobe of the liver (Fig. 11). One tech-nique to minimize such errors and artifacts is tosynchronize image acquisition with the source ofmotion, such as by using cardiac gating and naviga-tor echoes for respiratory triggered acquisitions.
The use of periodically rotated overlapping par-allel lines with enhanced reconstruction (PRO-PELLER) can also help minimize motion eŠects.PROPELLER is a radial fast spin-echo sequenceused with multi-shot imaging. The data is acquiredusing a series of concentric blades, each of whichrotates through the center of the k-space, whichreduces any rotation and translation artifacts thatoccur between the acquisitions of the blades anddistributes artifacts uniformly throughout the im-age.
A major source of artifacts is the eddy currentsinduced by the rapid switching on and oŠ of themotion-probing gradients, which can lead to geo-metric distortion as well as image-shearing artifactsthat may become more pronounced with increasing

220
Fig. 10. Small bowel peristalsis. A 52-year-old woman with suspected bowelobstruction. Cine magnetic resonance imaging (not shown) shows good move-ment in a dilated jejunal loop. Coronal single-shot echo-planar images (a) at b=0 s/mm2 and (b) at b=50 s/mm2 shows that the signal from the jejunal wall(white arrows) is maintained when diŠusion weighting is applied in (b).However, there is signal attenuation of the luminal contents. This suggests thatperistaltic intestinal wall motion is relatively coherent compared with the inco-herent motion of luminal turbulence.
Fig. 11. Signal loss in the left lobe of the liverresulting from cardiac motion. Coronal reformat im-age of diŠusion-weighted imaging (b=50 s/mm2)shows signiˆcant signal attenuation (arrow) over theleft lobe of the liver, especially just adjacent to theheart.
220 D-M. Koh et al.
Magnetic Resonance in Medical Sciences
b-values. When EPI is employed, there can also besigniˆcant magnetization phase shifts that cause``ghosting'' artifacts, which are usually worst in thephase-encoding direction. Several adjustments atimaging can help improve image quality, such aschanging the band-width, which alters the echo-spacing; and reducing the ˆeld of view in the phaseencoding direction to a minimum. Increasing theband-width reduces geometric artifacts but can leadto reduction in signal-to-noise and increased ghost-ing. Because these issues can be complex, it is valu-able to engage the expertise of an MR physicist to
ˆnely tune the system for optimal performance.DiŠusion-weighted imaging is highly sensitive to
susceptibility artifacts. In the abdomen, air in thegastrointestinal tract can cause susceptibility ar-tifacts that obscure visualization of adjacent struc-tures. Intriguingly, it was recently reported that theadministration of intravenous Buscopan prior toimaging can worsen the degree of artifacts encoun-tered over the left lobe of the liver.6
Quality assurance. To ensure that the MR systemis optimized, it is important to develop quality as-surance testing as part of the imaging program.One method23 uses diŠusion phantoms made ofcopper sulphate and sucrose solutions. This allowsthe precision and accuracy of the ADC measure-ment to be determined in relation to the noise of theMR imaging system, signal reproducibility, anddiŠerences between nominal and eŠective b-values.23 In addition, use of these phantoms will al-low early recognition of geometric distortion andother eddy current-induced artifacts, thereby ena-bling their rectiˆcation or minimization prior toclinical scanning.
Applications of DWI Techniques for TumorAssessment
The range of DWI imaging methods describedhas been employed to assess tumors in the body.24
DiŠusion-weighted imaging has been used to de-tect25–28 and characterize16,29,30 tumors, assess treat-

221
Fig. 12. Lesion detection in the liver using free-breathing diŠusion-weighted imaging (DWI). A45-year-old woman with breast cancer. In this example, metastases were di‹cult to visualize on the(a) unenhanced axial T1- and (b) T2-weighted images However, at DWI, (c) the high signal from in-trahepatic vessels is suppressed by application of diŠusion gradient on the b=100 s/mm2 image,enabling the metastases (arrows) to be clearly identiˆed. Note also the incidental ˆnding of ahemangioma within the vertebral body (arrowhead).
221Clinical DWI in the Body to Assess Tumors
Vol. 6 No. 4, 2007
ment response,31,32 and provide prognostic informa-tion.33–35 Although not exhaustive, the following ac-count of the clinical applications of DWI illustratesthe potential of these techniques.
Breath-hold single shot DWI. Breath-hold single-shot echo planar DWI has been used successfully toevaluate target areas within the abdomen and pel-vis. DWI has been applied to detect and character-ize tumors in the liver,18,27,36–40 pancreas,41 kid-neys,41–45 colon,46 and prostate.47,48
For example, in the liver, breath-hold DWI imag-ing alone could accurately detect the presence ofcolorectal hepatic metastases with high sensitivityand speciˆcity27 (Fig. 12). Application of low diŠu-sion weighting at image acquisition nulls the highsignal within intrahepatic blood vessels, therebyfacilitating the detection of small metastases lyingadjacent to blood vessels. Quantitative ADC mea-surements can also be calculated using breath-holdDWI, which may aid lesion characterization. It hasbeen shown that malignant hepatic lesions returnlower ADC values than do benign lesions, but thereis signiˆcant overlap.13 More recently, it was foundthat high pretreatment ADC values in colorectalhepatic metastases predicted for poor response tochemotherapy.49 ADC values have also been shownto increase in colorectal hepatic metastases, thusshowing at least a partial response to chemother-apy, but not in the nonresponders.49
Free-breathing multiple averaging DWI. Free-breathing multiple averaging DWI is a versatileimaging technique that can be applied to virtuallyany area in the body (Fig. 11). It has been used to e-valuate tumors in diverse areas, such as the headand neck,50,51 pancreas,25 kidneys,45,52 and prostate.53
ADCs can be calculated from the multiple-b-value
DWI images acquired, which may help in assessingtreatment response.
DiŠusion-weighted whole-body imaging withbackground body signal suppression (DWIBS). Be-cause DWIBS images are usually evaluated quali-tatively, the use of just two b-values is usuallysu‹cient (b=0 and 1000 s/mm2). The choice of ahigher b-value in combination with fat suppressionresults in good background suppression. However,more b-values may be accommodated within themeasurement to facilitate the calculation of ADCs.
Initial experience in applying the technique toclinical studies has shown substantial promise.However, DWIBS should be interpreted with otherimaging sequences because benign lesions mayresult in false positives, and certain malignant le-sions, such as sclerotic bone metastases, can leadto false negative results. Furthermore, becauseDWIBS discriminates tissues on the basis of cel-lularity rather than malignancy, its ability to distin-guish between benign and malignant lymph nodesremains uncertain. Its implementation in the evalu-ation of lymphoma appears promising, but furtherstudies evaluating the clinical applications of thetechnique are being undertaken. There is also con-siderable interest in establishing the diagnostic ac-curacy of the technique in tumor detection com-pared with whole-body STIR imaging and 18-‰urodeoxyglucose positron emission tomography.
Conclusions
DiŠusion-weighted MR imaging is useful for as-sessing tumors. In the body, 3 main DWI strategiesare currently applied for tumor imaging. Thesetechniques show considerable promise for detecting
222222 D-M. Koh et al.
Magnetic Resonance in Medical Sciences
and characterizing tumors and evaluating treat-ment response. However, careful optimization ofthese techniques is required to ensure high qualityimages for both qualitative and quantitative assess-ment. Radiologists should be acquainted with thekey factors that aŠect the quality of DWI studies toensure eŠective implementation of these techniquesin clinical practice.
References
1. Bammer R. Basic principles of diŠusion-weightedimaging. Eur J Radiol 2003; 45:169–184.
2. Yoshikawa T, Kawamitsu H, Mitchell DG, et al.ADC measurement of abdominal organs and le-sions using parallel imaging technique. AJR Am JRoentgenol 2006; 187:1521–1530.
3. Oner AY, Celik H, Oktar SO, Tali T. Singlebreath-hold diŠusion-weighted MRI of the liverwith parallel imaging: initial experience. ClinRadiol 2006; 61:959–965.
4. Taouli B, Martin AJ, Qayyum A, et al. Parallelimaging and diŠusion tensor imaging for diŠusion-weighted MRI of the liver: preliminary experiencein healthy volunteers. AJR Am J Roentgenol 2004;183:677–680.
5. Murtz P, Flacke S, Tr äaber F, van den Brink JS,Gieseke J, Schild HH. Abdomen: diŠusion-weight-ed MR imaging with pulse-triggered single-shot se-quences. Radiology 2002; 224:258–264.
6. Nasu K, Kuroki Y, Sekiguchi R, Kazama T,Nakajima H. Measurement of the apparent diŠu-sion coe‹cient in the liver: is it a reliable index forhepatic disease diagnosis? Radiat Med 2006; 24:438–444.
7. Takahara T, Imai Y, Yamashita T, Yasuda S,Nasu S, Van Cauteren M. DiŠusion weightedwhole body imaging with background body signalsuppression (DWIBS): technical improvement us-ing free breathing, STIR and high resolution 3Ddisplay. Radiat Med 2004; 22:275–282.
8. Nasu K, Kuroki Y, Sekiguchi R, Nawano S. TheeŠect of simultaneous use of respiratory triggeringin diŠusion-weighted imaging of the liver. MagnReson Med Sci 2006; 5:129–136.
9. Spuentrup E, Buecker A, Koelker C, GuentherRW, Stuber M. Respiratory motion artifact sup-pression in diŠusion-weighted MR imaging of thespine. Eur Radiol 2003; 13:330–336.
10. Takahara T, Yamashita T, Yanagimachi N, IinoM, Koizumi J, Imai Y. Imaging of peripheral nervedisease using diŠusion-weighted neurography(DWN) [Abstract SSE13–03], In: Radiological So-ciety of North America Scientiˆc Assembly andAnnual Meeting. Chicago, 2004; 394.
11. Farraher SW, Jara H, Chang KJ, OzonoŠ A, SotoJA. DiŠerentiation of hepatocellular carcinomaand hepatic metastasis from cysts and hemangio-
mas with calculated T2 relaxation times and theT1/T2 relaxation times ratio. J Magn Reson Imag-ing 2006; 24:1333–1341.
12. Provenzale JM, Engelter ST, Petrella JR, SmithJS, MacFall JR. Use of MR exponential diŠusion-weighted images to eradicate T2 ``shine-through''eŠect. AJR Am J Roentgenol 1999; 172:537–539.
13. Taouli B, Vilgrain V, Dumont E, Daire JL, Fan B,Menu Y. Evaluation of liver diŠusion isotropy andcharacterization of focal hepatic lesions with twosingle-shot echo-planar MR imaging sequences:prospective study in 66 patients. Radiology 2003;226:71–78.
14. Ichikawa T, Haradome H, Hachiya J, Nitatori T,Araki T. DiŠusion-weighted MR imaging with asingle-shot echoplanar sequence: detection andcharacterization of focal hepatic lesions. AJR AmJ Roentgenol 1998; 170:397–402.
15. M äuller MF, Prasad PV, Siewert B, Edelman RR.[The in-vivo diŠusion measurements of the liver,kidneys, spleen and m. erector with an echo-planarimaging system in normal subjects]. Rofo 1994;161:233–236. (Article in German)
16. Namimoto T, Yamashita Y, Sumi S, Tang Y,Takahashi M. Focal liver masses: characterizationwith diŠusion-weighted echo-planar MR imaging.Radiology 1997; 204:739–744.
17. Yamada I, Aung W, Himeno Y, Nakagawa T,Shibuya H. DiŠusion coe‹cients in abdominal or-gans and hepatic lesions: evaluation with intra-voxel incoherent motion echo-planar MR imaging.Radiology 1999; 210:617–623.
18. Koh DM, Scurr E, Collins DJ, et al. Colorectalhepatic metastases: quantitative measurements us-ing single-shot echo-planar diŠusion-weighted MRimaging. Eur Radiol 2006; 16:1898–1905.
19. Hollingsworth KG, Lomas DJ. In‰uence of perfu-sion on hepatic MR diŠusion measurement. NMRBiomed 2006; 19:231–235.
20. Moteki T, Horikoshi H. Evaluation of hepatic le-sions and hepatic parenchyma using diŠusion-weighted echo-planar MR with three values ofgradient b-factor. J Magn Reson Imaging 2006;24:637–645.
21. Le Bihan D, Poupon C, Amadon A, LethimonnierF. Artifacts and pitfalls in diŠusion MRI. J MagnReson Imaging 2006; 24:478–488.
22. Muro I, Takahara T, Horie T, et al. [In‰uence ofrespiratory motion in body diŠusion weightedimaging under free breathing (examination of amoving phantom)]. Nippon Hoshasen GijutsuGakkai Zasshi 2005; 61:1551–1558. (Article in Jap-anese)
23. Delakis I, Moore EM, Leach MO, De Wilde JP.Developing a quality control protocol for diŠusionimaging on a clinical MRI system. Phys Med Biol2004; 49:1409–1422.
24. Koh DM, Collins DJ. DiŠusion-weighted MRI inthe body: applications and challenges in oncology.

223223Clinical DWI in the Body to Assess Tumors
Vol. 6 No. 4, 2007
AJR Am J Roentgenol 2007; 188:1622–1635.25. Ichikawa T, Erturk SM, Motosugi U, et al. High-b
value diŠusion-weighted MRI for detecting pan-creatic adenocarcinoma: preliminary results. AJRAm J Roentgenol 2007; 188:409–414.
26. Ichikawa T, Erturk SM, Motosugi U, et al. High-B-value diŠusion-weighted MRI in colorectal can-cer. AJR Am J Roentgenol 2006; 187:181–184.
27. Nasu K, Kuroki Y, Nawano S, et al. Hepaticmetastases: diŠusion-weighted sensitivity-encodingversus SPIO-enhanced MR imaging. Radiology2006; 239:122–130.
28. Naganawa S, Sato C, Nakamura T, et al. DiŠu-sion-weighted images of the liver: comparison oftumor detection before and after contrast enhance-ment with superparamagnetic iron oxide. J MagnReson Imaging 2005; 21:836–840.
29. Chan JH, Tsui EY, Luk SH, et al. DiŠusion-weighted MR imaging of the liver: distinguishinghepatic abscess from cystic or necrotic tumor.Abdom Imaging 2001; 26:161–165.
30. Kim T, Murakami T, Takahashi S, Hori M, TsudaK, Nakamura H. DiŠusion-weighted single-shotechoplanar MR imaging for liver disease. AJR AmJ Roentgenol 1999; 173:393–398.
31. Byun WM, Shin SO, Chang Y, Lee SJ, Finster-busch J, Frahm J. DiŠusion-weighted MR imagingof metastatic disease of the spine: assessment ofresponse to therapy. AJNR Am J Neuroradiol2002; 23:906–912.
32. Chen CY, Li CW, Kuo YT, et al. Early response ofhepatocellular carcinoma to transcatheter arterialchemoembolization: choline levels and MR diŠu-sion constants–initial experience. Radiology 2006;239:448–456.
33. Mardor Y, Roth Y, Ochershvilli A, et al. Pretreat-ment prediction of brain tumors' response to radi-ation therapy using high b-value diŠusion-weight-ed MRI. Neoplasia 2004; 6:136–142.
34. Dzik-Jurasz A, Domenig C, George M, et al.DiŠusion MRI for prediction of response of rectalcancer to chemoradiation. Lancet 2002; 360:307–308.
35. Provenzale JM, Mukundan S, Barboriak DP.DiŠusion-weighted and perfusion MR imaging forbrain tumor characterization and assessment oftreatment response. Radiology 2006; 239:632–649.
36. Okada Y, Ohtomo K, Kiryu S, Sasaki Y. Breath-hold T2-weighted MRI of hepatic tumors: value ofecho planar imaging with diŠusion-sensitizinggradient. J Comput Assist Tomogr 1998; 22:364–371.
37. Abe Y, Yamashita Y, Tang Y, Namimoto T,Takahashi M. Calculation of T2 relaxation timefrom ultrafast single shot sequences for diŠerentia-tion of liver tumors: comparison of echo-planar,HASTE, and spin-echo sequences. Radiat Med2000; 18:7–14.
38. Yamashita Y, Tang Y, Takahashi M. Ultrafast MR
imaging of the abdomen: echo planar imaging anddiŠusion-weighted imaging. J Magn Reson Imag-ing 1998; 8:367–374.
39. Ito K, Mitchell DG, Matsunaga N. MR imaging ofthe liver: techniques and clinical applications. EurJ Radiol 1999; 32:2–14.
40. Quan XY, Sun XJ, Yu ZJ, Tang M. Evaluation ofdiŠusion weighted imaging of magnetic resonanceimaging in small focal hepatic lesions: a quantita-tive study in 56 cases. Hepatobiliary Pancreat DisInt 2005; 4:406–409.
41. Chow LC, Bammer R, Moseley ME, Sommer FG.Single breath-hold diŠusion-weighted imaging ofthe abdomen. J Magn Reson Imaging 2003; 18:377–382.
42. Squillaci E, Manenti G, Di Stefano F, Miano R,Strigari L, Simonetti G. DiŠusion-weighted MRimaging in the evaluation of renal tumours. J ExpClin Cancer Res 2004; 23:39–45.
43. Squillaci E, Manenti G, Cova M, et al. Correlationof diŠusion-weighted MR imaging with cellularityof renal tumours. Anticancer Res 2004; 24:4175–4179.
44. Cova M, Squillaci E, Stacul F, et al. DiŠusion-weighted MRI in the evaluation of renal lesions:preliminary results. Br J Radiol 2004; 77:851–857.
45. Pozzi-Mucelli R. Can diŠusion-weighted MRI with-out breath-holding be used to evaluate renal abnor-malities? Nat Clin Pract Nephrol 2006; 2:126–127.
46. Nasu K, Kuroki Y, Kuroki S, Murakami K,Nawano S, Moriyama N. DiŠusion-weighted singleshot echo planar imaging of colorectal cancer usinga sensitivity-encoding technique. Jpn J Clin Oncol2004; 34:620–626.
47. Hosseinzadeh K, Schwarz SD. Endorectal diŠu-sion-weighted imaging in prostate cancer to diŠer-entiate malignant and benign peripheral zone tis-sue. J Magn Reson Imaging 2004; 20:654–661.
48. Reinsberg SA, Payne GS, Riches SF, et al. Com-bined use of diŠusion-weighted MRI and 1H MRspectroscopy to increase accuracy in prostate can-cer detection. AJR Am J Roentgenol 2007; 188:91–98.
49. Koh DM, Scurr E, Collins DJ, et al. Predictingresponse of colorectal hepatic metastases: value ofpre-treatment apparent diŠusion coe‹cients. AJRAm J Roentgenol 2007; 188:1001–1008
50. Koç O, Paksoy Y, Erayman I, Kivrak AS, ArbagH. Role of diŠusion weighted MR in the discrimi-nation diagnosis of the cystic and/or necrotic headand neck lesions. Eur J Radiol 2007; 62:205–213.
51. Vandecaveye V, De Keyzer F, Nuyts S, et al. De-tection of head and neck squamous cell carcinomawith diŠusion weighted mri after (chemo) radio-therapy: Correlation between radiologic and his-topathologic ˆndings. Int J Radiat Oncol BiolPhys 2007; 67:960–971.
52. Thoeny HC, De Keyzer F, Oyen RH, Peeters RR.

224224 D-M. Koh et al.
Magnetic Resonance in Medical Sciences
DiŠusion-weighted MR imaging of kidneys inhealthy volunteers and patients with parenchymaldiseases: initial experience. Radiology 2005; 235:911–917.
53. Kurhanewicz J, Vigneron DB, Males RG, SwansonMG, Yu KK, Hricak H. The prostate: MR imagingand spectroscopy. Present and future. Radiol ClinNorth Am 2000; 38:115–138, viii-ix.