practicing safety steve kairys, md, mph, faap diane abatemarco, phd, msw practicing safety learning...
TRANSCRIPT
Practicing Safety
Steve Kairys, MD, MPH, FAAPDiane Abatemarco, PhD, MSW
Practicing Safety Learning SessionMay 30, 2009

Disclosures
Steven Kairys: I have no relevant financial relationships with the manufacturers of any commercial products and/or provider of commercial services discussed in this CME activity. I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation.
Diane Abatemarco: I have no relevant financial relationships with the manufacturers of any commercial products and/or provider of commercial services discussed in this CME activity. I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation.

The Importance of Prevention
10-15% of young children are victims of serious physical trauma (Finkelhor and Straus)
Neglect is the leading cause of substantiated cases of abuse (over 60%)
Children < age 3 account for nearly 30 percent of victims.
Estimates of treatment costs are 24 billion dollars a year. Long term sequelae are enormous in terms of psycho-
logical and functional damage, substance abuse, delinquency, learned aggressiveness and abuse potential when a parent.
The Relationship of Adverse ChildhoodExperiences to Adult Health Status
A collaborative effort of Kaiser Permanente and
The Centers for Disease Control and Prevention
Vincent J. Felitti, M.D.Robert F. Anda, M.D.

The Adverse Childhood Experiences (ACE) Study
• The largest study of its kind ever done to examine the health and social effects of adverse childhood experiences over the lifespan (18,000 participants)
What do we mean by Adverse Childhood Experiences?
• Experiences that represent medical and social problems of national importance. - Childhood abuse and neglect- Growing up with domestic violence,
substance abuse or mental illness in the home
- Parental loss - Crime

ACE Study Design
Survey Wave 1 -- complete71% response (9,508/13,454) n=15,000 71% response
Survey Wave II n=15,000
All medical evaluationsabstracted
PresentHealth Status
Mortality National Death Index
Morbidity Hospital Discharge Outpatient Visits Emergency Room Visits Pharmacy Utilization
All medical evaluationsabstracted
vs. &

The Adverse Childhood Experiences (ACE) Study
Summary of Findings:• Adverse Childhood Experiences (ACEs)
are very common • ACEs are strong predictors of later
health risks and disease• This combination makes ACEs the leading determinant
of the health and social well-being of our nation

Categories of Adverse Childhood Experiences
CategoryPrevalence (%)
Abuse, by Category Psychological (by parents) 11% Physical (by parents) 11% Sexual (anyone) 22%
Household Dysfunction, by Category Substance Abuse 26% Mental Illness 19% Mother Treated Violently 13% Imprisoned Household Member 3%
What is conventionallyviewed as a problem
is actually a solution to an unrecognized prior
adversity.
Adverse Childhood Experiences determine the likelihood of the ten most common causes of death in the United States.
Top 10 Risk Factors: smoking, severe obesity, physical inactivity, depression, suicide attempt, alcoholism, illicit drug use, injected drug use, 50+ sexual partners, h/o STD.

Evidence from ACE Study Suggests:
Adverse childhood experiences are the most basic cause of health risk
behaviors, morbidity, disability, mortality, and healthcare costs.

Adverse Childhood ExperiencesAdverse Childhood Experiences
Social, Emotional, & Cognitive Impairment
Adoption ofHealth-risk Behaviors
Disease, Disability
EarlyEarlyDeathDeath
The Influence of AdverseChildhood Experiences Throughout
Life
Death
Birth
The Role Primary Care Practice in Preventing Child Abuse and
Neglect
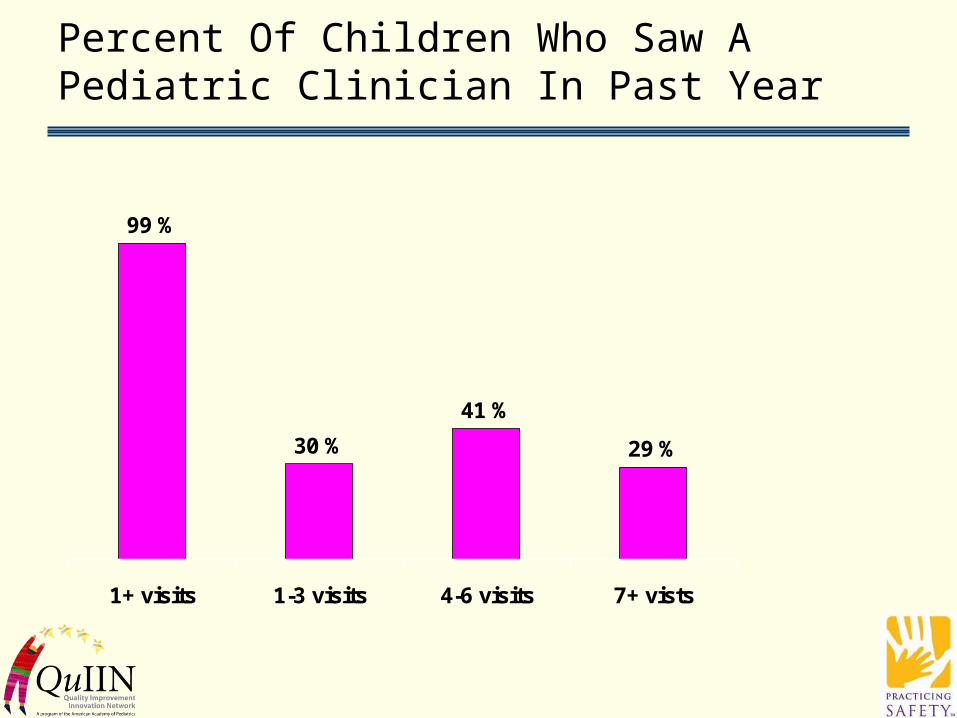
Percent Of Children Who Saw A Pediatric Clinician In Past Year
99 %
30 %
41 %
29 %
1+ visits 1-3 visits 4-6 visits 7+ vists

Periodic Survey of Fellows of the American Academy of Pediatrics
Periodic Survey: National, random sample, mailed survey of 1600 US members of AAP
Fielded: March 2000 - August 2000
Return rate = 67%
Data reported on 811 pediatricians who provide health supervision to children under 36 months of age
Most pediatricians say they discuss traditional topics with less than 75% of parents of patients 0-9 months:
Immunizations (94%), nutrition (93%), sleeping positions (82%), breastfeeding (70%)
Less frequently discussed are topics related to cognitive development:
Reading to child (48%) & how child communicates (42%)
Least discussed are topics related to family & community needs:
Social support (28%), financial needs (16%), violence in the community (13%)
Pediatrician Perspectives on Content of Health Supervision
Common topics not discussed over 50% even though 86% of pediatricians think those topics are important:
discipline
child development
behavior
Only 33% discuss guidance/discipline with parents of toddlers
What Doctors Talk About With Their Families
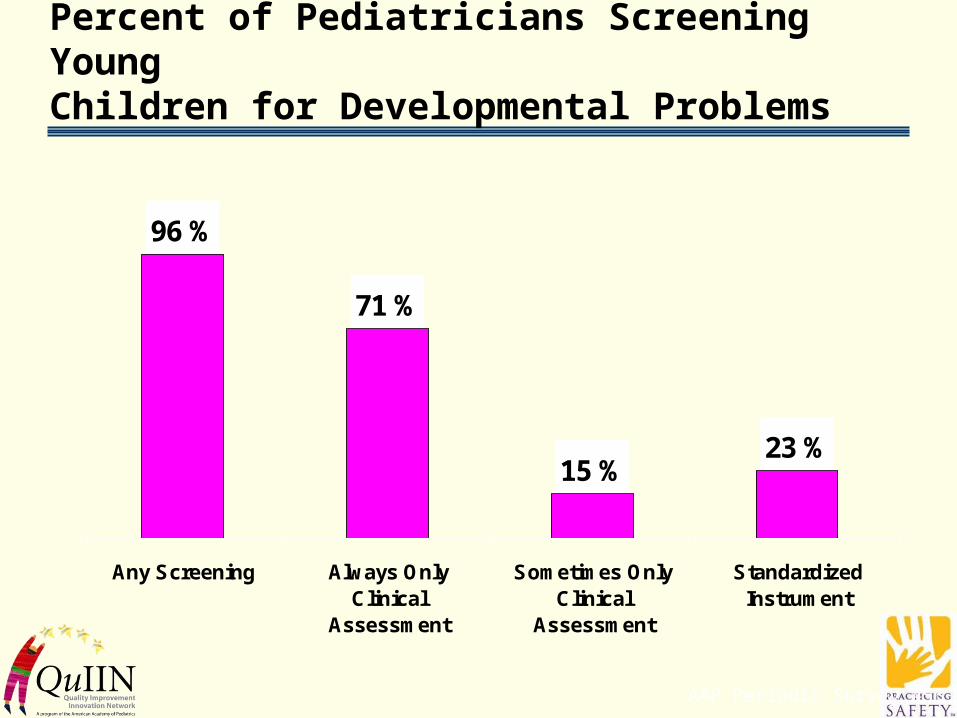
Percent of Pediatricians Screening Young Children for Developmental Problems
96 %
71 %
15 %23 %
Any Screening Always OnlyClinical
Assessment
Sometimes OnlyClinical
Assessment
StandardizedInstrument
AAP Periodic Survey #53, 2002

Parents With Concerns About Their Children Ages 4-35 Months
48 %45 %
42 % 41 %38 %
Behavior Communication Emotional well-being
Getting alongwith others
Learningpreschool skills
National Survey of Early Childhood Health, 2000

Parents’ Misconceptions
Parents of young children…
57% believe a baby younger than 6 months can
be spoiled
Almost 40% believe a 12-month-old’s behavior
can be based on revenge
51% expect a 15-month-old to share
What Grown-Ups Understand About Child Development, Civitas, 2000

Missed Opportunities
Parents concerns are often not elicited or addressed
44-79% of parents report not discussing important child development topics with their pediatricians
About 57% of parents report receiving a developmental assessment of any kind
Only half of “exemplary” practices refer children to developmental programs
What Child Health Professionals Should Do
Screening: Identify risk factors that could lead to a problem, and initiate treatment to reduce or remove the risk
Educate: Anticipate potential problems, and initiate treatment to promote resilience in the child and family
Treat and Refer: Newly identify a problem, diagnose, initiate treatment or referral and provide care coordination

PRACTICING SAFETYPHASE I

Overall Goal: Decrease child abuse and neglect by
increasing screening and improving anticipatory guidance provided by pediatric practices to parents of children ages 0-3.
TOOLKIT7 Color coded Modules:
Red: Coping with Crying/SBS Prevention
Purple: Parenting
Pink: Safety in Others’ Care
Blue: Family & The Environment
Orange: Effective Discipline
Green: Sleeping/Eating Issues
Aqua: Toilet Training
Practice Guides with:
Background information about each topic
Assessment Questions
Anticipatory Guidance
Parent Educational Materials
Office Marketing Tools
Staff tools
Moderate Interactives/Tangibles
Issues Management
Practicing Safety Modules include…Practicing Safety Modules include…
Practice GuideA tool for the clinician
Explanation of topic
Stages to introduce and reinforce information
Assessment Questions
Anticipatory Guidance
Materials for the office, parents, and staff
Issues Management
Practice Guide - Utilization A tool for the clinician
Assessment Questions
Anticipatory Guidance
Incorporate the materials into your routine patterns of practice
Create and use a Community Resource Guide

Data Analysis: Phase 1
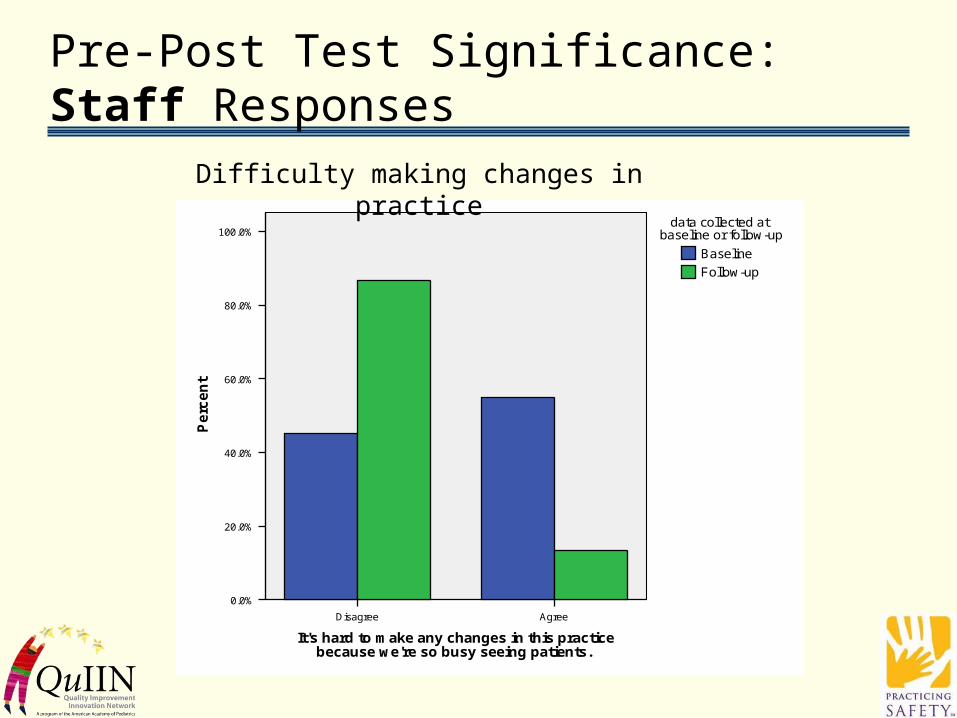
AgreeDisagree
It's hard to make any changes in this practice because we're so busy seeing patients.
100.0%
80.0%
60.0%
40.0%
20.0%
0.0%
Pe
rce
nt
Follow-up
Baseline
data collected at baseline or follow-up
Pre-Post Test Significance: Staff Responses
Difficulty making changes in practice

Pre-Post Test Significance: Staff Responses
At least occasionallyNever or rarely
How often do you use a health risk assessment (HRA) protocol or questionnaire to identify parents or
patients who may benefit from counseling or other interventions for the following - Maternal depression
80.0%
60.0%
40.0%
20.0%
0.0%
Perc
ent
Follow-up
Baseline
Data collected at baseline or follow-up
At least occasionallyNever or rarely
How often do you use nurses or health educators, within your practice, for individual counseling to your
patients with - Maternal depression
80.0%
60.0%
40.0%
20.0%
0.0%
Per
cent
Follow-up
Baseline
Data collected at baseline or follow-up
Use of screening tool for depression Counseling for maternal depression

No Yes
In the last 12 months, have your child’s doctors or office providers in this practice asked you: If you ever feel depressed, sad, or have crying spells
80.0%
60.0%
40.0%
20.0%
0.0%
Pe
rce
nt
Follow up
Baseline
data collected at baseline or follow up
Pre-Post Test Significance: Parent Responses
Asked about depression
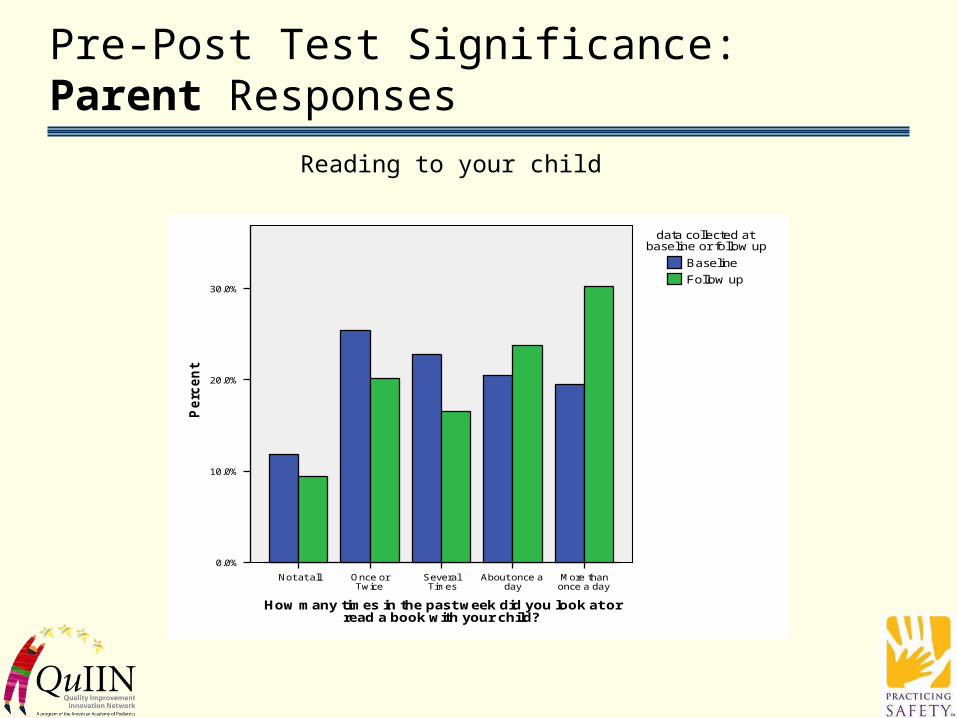
More than once a day
About once a day
Several Times
Once or Twice
Not at all
How many times in the past week did you look at or read a book with your child?
30.0%
20.0%
10.0%
0.0%
Pe
rce
nt
Follow up
Baseline
data collected at baseline or follow up
Pre-Post Test Significance: Parent Responses
Reading to your child

Tool Evaluation Summary
0
10
20
30
40
50
60
70
80
90
Overall usefulness of modules (Percentage of respondents
who rated module as 3 or 4)Module 1: Coping with Crying Module 2: Parenting Module 3: Safety in Others’ Care Module 4: Family & the Environment Module 5: Effective Discipline Module 6: Sleeping and Feeding Module 7: Toilet Training

Tool Evaluation by Module Tools Rated most useful
Coping with Crying Module “Coping with Crying” posters (95% rated 3
or 4) “World of Parenting” brochure (83% rated 3
or 4)
Parenting Module “Post-partum Depression” brochure (89%
rated 3 or 4) “Bonding With Your Child” booklet (88%
rated 3 or 4)
Safety in Others’ Care ModuleSupport telephone numbers magnet (82% rated
3 or 4) “Choosing Child Care: What’s Best for
Your Family” (59% rated 3 or 4)
Family and the Environment ModuleSupport phone #s magnet (88% rated 3-4) Domestic violence shoe card (74% rated 3-
4)
Effective Discipline Module “Teaching Good Behavior—Tips on
Discipline” brochure (88% rated 3 or 4) “Temper Tantrums: A Normal Part of
Growing Up” brochure (87% rated 3 or 4)
Sleeping and Feeding Module “Sleep Problems in Children” brochure
(75% rated 3 or 4) “Feeding Kids Isn’t Always Easy” brochure
(75% rated 3 or 4)
Toilet Training Module “Toilet Training” brochure (95% rated 3 or 4) “Bed-wetting” brochure (89% rated 3 or 4)
Further Assessment
Focus group discussion sessions were conducted with 5-8 members of the practice staff, including members and non-members of the Reflective Adaptive Process (RAP) team.
In-depth telephone interviews were conducted with a physician in each of the practices.
Qualitative data collected were reflexively coded by 3 members of the research team separately. Inter-rater reliability was checked.
Changes in practice Raised awareness about child abuse and neglect. Maternal depression screening was adopted by 4
of the 5 pediatric practices. The practice that did not adopt screening identified lack of a referral source for depressed mothers within the community.
Infant crying, discipline and toilet training modules were also implemented by the practices.
Maternal drug and alcohol issues were generally difficult for practices to address although those with established referral systems to social workers fared better.
Most practices noted that the intervention program contained too much information.
Strengths of Practicing Safety
Staff focus groups Raised staff and MD awareness of issues and
approach to patients/parents. Helped institute depression screening and discussion
of toilet training. Provided opportunity for practice to reflect Materials and helping identify parents at risk
Physician interviews Increased awareness of problems leading to child
abuse & neglect Developed more systematic ways of sharing
information

WeaknessesFocus Groups Too much information (and cost of materials) Not targeted to varied audience Lack of feedback loop – from docs back to staff and
from parents back to staff – staff discontent with not knowing impact of PS materials/efforts
No change in roles; staff wanted to play a bigger role
Physician Interviews Too many meetings Materials too wordy, language barriers Staff complained of too much work
Revisions
5 Points to Practicing Safety1. Reflective Practice Change
2. Infant
3. Mother
4. Toddler
5. Community
Toolkit Revision
Infant Mother Toddler
BUNDLES

Team Expectations
Submit 20 Monthly Chart Documentation Forms on 30th of every month (June-November)
Submit Monthly Progress Report on 30th of every month Share lessons learned and problem-solve with other participating
practices through monthly conference calls and e-mail. Complete a post-Inventory survey in November Complete a Tool Evaluation survey in November A selected number of practices will be asked to participate in
telephone interviews at the conclusion of the project Work with other members of your practice’s clinical team to improve
care processes related to maternal depression screening, counseling about crying, counseling about toilet training, and counseling about effective discipline.
Test innovations in care delivery to prevent child abuse and neglect.

Agenda For Day
Baseline Data ResultsToolkit Bundles (Infant,
Mother/Caregiver, Toddler)Model for ImprovementData Collection and
MeasurementTeam Planning TimeTeam SharingWrap Up and Next Steps
Ask Questions!
Share Experiences!
Plan for Testing!