pre hospital management of sci - anzona
TRANSCRIPT

Acute to Rehab Spinal Cord
Injuries
Anna Brown CNC, Certificate SCI Nursing,
Grad Dip Rehabilitation Studies, La Trobe
Victorian Spinal Cord Service Austin Health

SCI – Acute to Rehab
Let the rollercoaster ride begin . . .

National Data Causes of SCI
• Land Transport 46 % – MV occupants 51%
– Unprotected road users 49%
• Falls 28 % – Low falls < 1 metre 64%
– High falls 1 metre or > 36%
• Diving & Water Related 9 %
• Struck by another person or object 9 %
• Miscellaneous causes 8 %
Lynda Norton, 2010 – Spinal cord injury, Australia 2007-08
Research Centre for Injury Studies, Flinders University
Australian Demographics Spinal Cord Injuries
• 237 new SCIs in Australia per year – VSCS admits 85 – 90 annually
– Paediatric incidence is not clear
• Segment of population at greatest risk adult men b/w 16 – 30 years
– Men > Women approx 4 : 1
– Paediatric incidence is > in boys than girls
• Most common age – 19 years
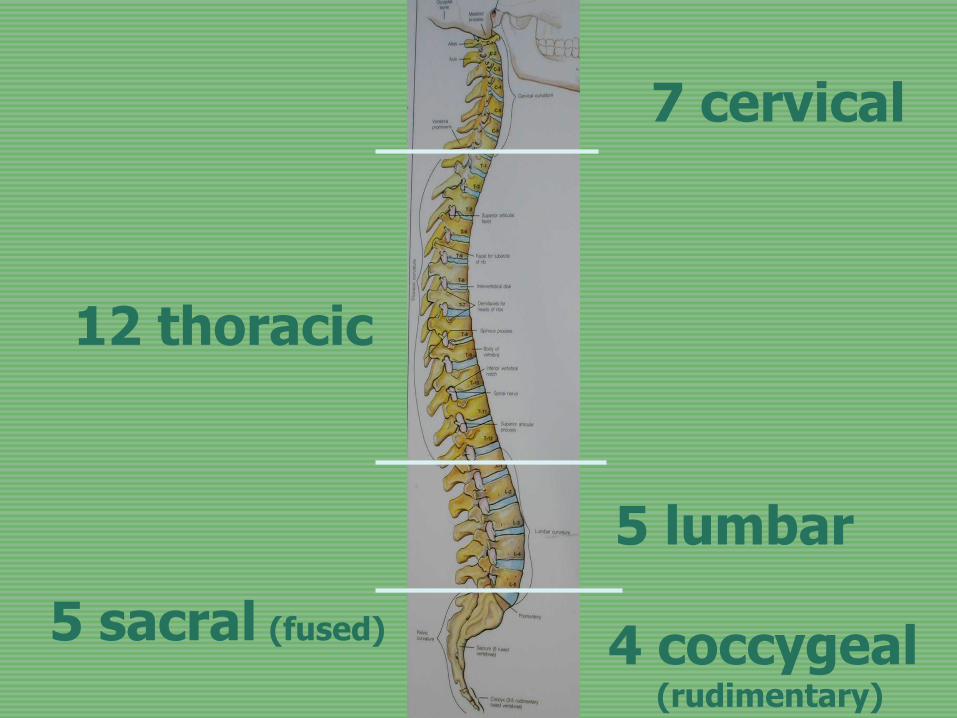
7 cervical
12 thoracic
5 lumbar
5 sacral (fused)
4 coccygeal
(rudimentary)
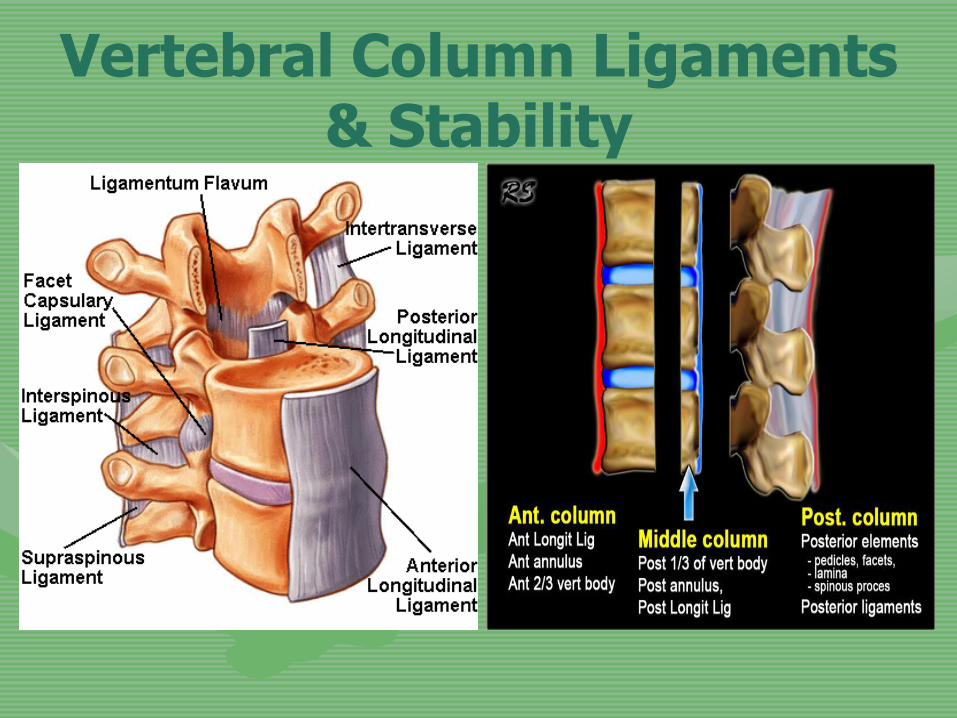
Vertebral Column Ligaments & Stability

The Spinal Cord – Approx. 45 cms in length
– Continuous with the brain
– Consists of millions of neurone bundles
– Extends from superior border of C 1
– The thickness of the little finger
– Consistency of toothpaste
– Encased & protected by the vertebrae
– Ends at vertebral level L 1 /2

The Spinal Nerves
31 pairs of nerves
– 8 cervical
– 12 thoracic
– 5 lumbar
– 5 sacral
– 1 coccygeal

A Spinal Cord Injury Results in
• Loss of movement
• Loss of sensation
• Interruption to ANS – sympathetic pathways
– Resulting in low BP
– Inability to control body temperature
• Altered respiratory function
• Loss of bladder & bowel control
• Altered sexual function
Classification of SCI
• Quadriplegia / Tetraplegia
– T 1 and above
• Paraplegia
– T 2 and below
• Complete / Incomplete
– Motor and / or sensory sparing

Neurological Examination
• Motor power - myotome / muscle innervation
• 0 - 5 grading
• Sensory function - dermatome level • 0 - 2 score
• Light touch / aesthesia
• Pin prick / analgesia
• Proprioception
• Reflex activity • 0 - +++ score

http://www.asia-spinalinjury.org/publications/2006_Classif_work
sheet.pdf

ASIA Standard Classification
American Spinal Injury Association
Scale of SCI Impairment
– A = Complete
– B = Motor complete / Sensory incomplete
– C = Incomplete - Below Grade 3
– D = Incomplete - Grade 3 or above
– E = Normal

Neurogenic Shock • Results from injury to the descending
sympathetic pathways
• SCI at T6 & above may have profound effects resulting in
Triad of Clinical Signs
– Bradycardia • unopposed vagal tone on heart
– Hypotension • vasodilatation & loss of sympathetic tone; expect
BP 90/60
– Hypothermia • sympathetic loss – resulting in poilkilothermia
Initial Management
• Position & alignment
– Immobilise spine board, cervical collar
– Neutral whole vertebral column
– Avoid repeating mechanism of injury
• Skin & pressure
– Pressure relief - essential
– Awareness of potential problems
– Assistive devices / equipment

Head Holding Techniques
From the Top
From the Side
Pistol grip

Spinal Immobilisation in Paediatrics
Position / alignment • Disproportionate head size in
children under 3yrs
• With toddler & infant use Occian pad / Papoose to position correctly
Papoose
Occian Pad

Management Prior to Transport
• Clinical examination – Neurological assessment
– Bradycardia & hypotension
• Oxygen /respiratory support
• Monitor temperature - Poikilothermia
– combination of hypotension & hypothermia
– appropriate environmental temperatures
• Adequate x-rays

Management Prior to Transport
• Naso-gastric tube – open drainage, monitor pH
• Urethral catheter – correct size, balloon volume
– expect 30 mls/hr output
• IV therapy
– avoid overload – expect hypotension

Radiological Examination
Full vertebral column views
AP views Lateral views
CT scan MRI SCIWORA MRI essential
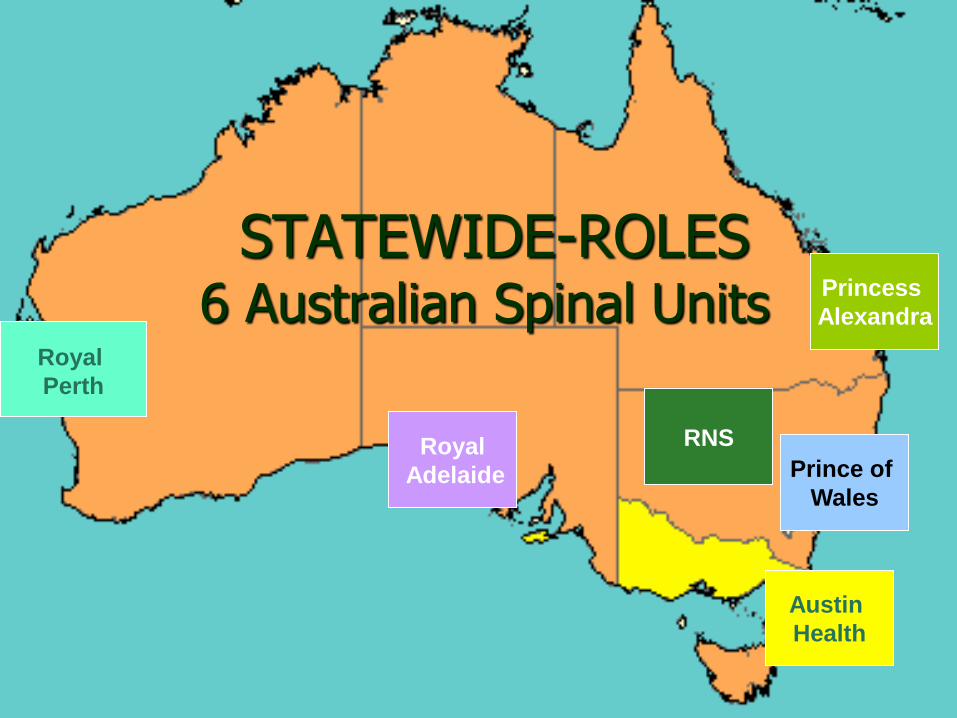
STATEWIDE-ROLES 6 Australian Spinal Units
Princess
Alexandra
Royal
Adelaide
Royal
Perth
Prince of
Wales
RNS
Austin
Health
Acute Management
• Cardiovascular
• Respiratory
• Vertebral column stabilisation
• Skin integrity & pressure management
• Gastro intestinal, including establishing bowel routine
• Nutrition
• Bladder management
• Prevention of complications – VTE, respiratory, pressure injuries
• Psychosocial . . .

Acute Management
• Psychosocial – Consistent, objective information
– Psych review & support through grieving & immobility
– Relative / family support
– Prepare for the transition to rehab.
– Team approach
REHABILITATION STARTS
ON DAY 1
The next stop . . . rehabilitation
Continuing on the rollercoaster ride . . . onto rehabilitation & community

Functional / Neurological Level of SCI
– Level of spinal cord injury – ASIA scale grading
– Associated injuries / complications
– Age & aging factors
– Gender - body proportions
– Cultural factors / family support
– Motivation / emotional status
– Carer factors

Activities of Daily Living (ADLs)
• OT, Nursing, Physio
– Showering, hygiene & grooming
– Dressing - upper / lower limb
– Feeding, meal preparation
– Domestic skills
– Communication skills
– Home modifications
– Community access
Mobility / Transfers
• Physio, Nursing, OT
– Muscle strengthening & endurance
– Balance / stretches
– Transfers – hoist, slide-board or lift
• bed to chair
• bed to commode / toilet / shower seat
• car / transport

Mobility / Transfers
• Physio, Nursing, OT
– Bed mobility
– Wheelchair mobility
– Gait training
– Posture / pressure management

Posture, Pressure & Skin Care
– Know sensory level / deficits
– Assess all potential sites of pressure
– Nutritional status if ‘at risk’
– Suitable bedding → mattress, protective &
assistive devices
– Wheelchair & suitable cushion
– Transfer skills

Bladder & Bowel Management
Nursing with input from physio & OT
– Bladder training
• Intermittent catheters – hand function necessary
• SPC / IDC
• Regular surveillance
– Bowel training
• Establish a routine – time of day, suitable to lifestyle, prevents unplanned bowel actions
• 5 ‘Rs’ - right time, place, consistency, amount & reliable trigger

Patient Education
• Information / empowerment
• Readiness for learning / rehabilitation
• Teaching techniques
• Modules of relevant information
• Balance of theory & practice
• Problem solving skills
• Written information - later reference

Community Integration
– Home modifications
• bathroom, access
– ‘Role’ in family & community
– Vocational options
– Transport options
• driving, maxi taxis, public transport
– Leisure & socialisation

Leisure Options
• Snow skiing
• Water-skiing
• Wheelchair rugby
• Basketball
• Netball
• Pistol shooting
• Darts
• Bowling – lawn & 10pin
• Sailing
• Driving a car
• Computer / internet
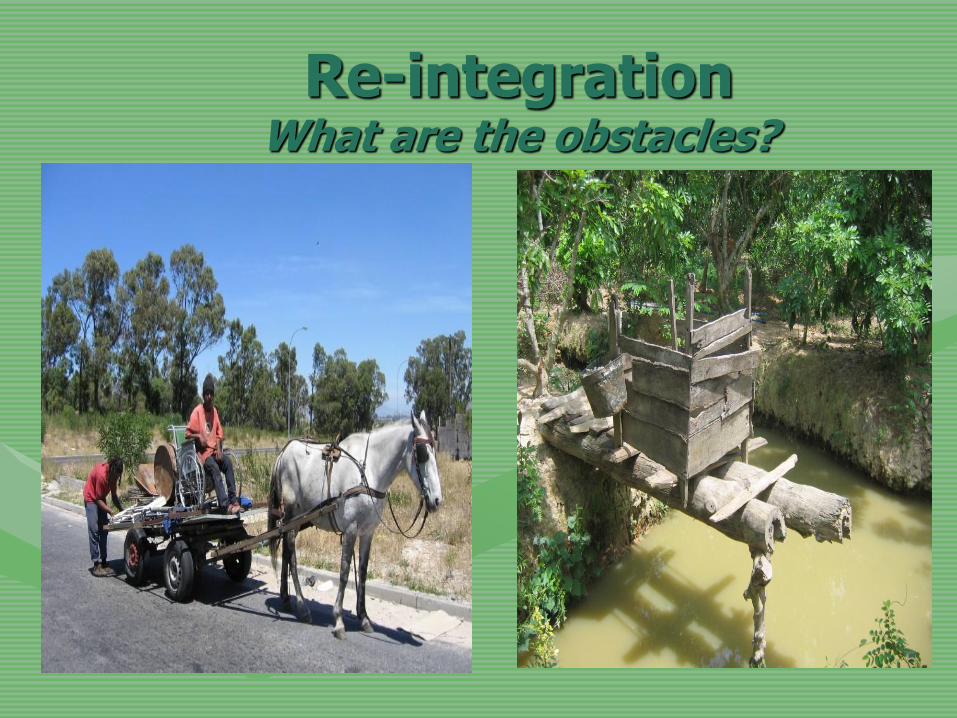
Re-integration What are the obstacles?

Rehabilitation of the SCI Person
• Successful rehab dependent on – Team approach
– Patient education → theory & practice
– Discharge planning
– Appropriate equipment
– Housing → suitable modifications
– Community reintegration & resources
– Support & follow up
• Community spinal nurses
• Annual review – Country & Metro Clinics
Spinal Cord Injury
• ‘Life for most of us is a matter of adjusting to change. Yet few of us are prepared to adjust to all the changes in life caused by a spinal cord injury (SCI). Even under the best of circumstances successful adaptation to the results of SCI requires courage, perseverance, faith, support from family & friends, & quality rehabilitation.’
Lex Frieden
Foreword in Zejdlik C.P., (1992) Management of Spinal Cord Injury