predictors of pressure ulcers in adult critical care patients.pdf
TRANSCRIPT

http://ajcc.aacnjournals.org/cgi/external_ref?link_type=PERMISSIONDIRECTPersonal use only. For copyright permission information: Published online http://www.ajcconline.org© 2011 American Association of Critical-Care Nurses
doi: 10.4037/ajcc2011934 2011;20:364-375Am J Crit Care Jill CoxPredictors of Pressure Ulcers in Adult Critical Care Patients
http://ajcc.aacnjournals.org/subscriptions/Subscription Information
http://ajcc.aacnjournals.org/misc/ifora.shtmlInformation for authors
http://www.editorialmanager.com/ajccSubmit a manuscript
http://ajcc.aacnjournals.org/subscriptions/etoc.shtmlEmail alerts
by AACN. All rights reserved. © 2011 CopyrightTelephone: (800) 899-1712, (949) 362-2050, ext. 532. Fax: (949) 362-2049. bimonthly by The InnoVision Group, 101 Columbia, Aliso Viejo, CA 92656.journal of the American Association of Critical-Care Nurses (AACN), published AJCC, the American Journal of Critical Care, is the official peer-reviewed research
by guest on March 29, 2012ajcc.aacnjournals.orgDownloaded from

By Jill Cox, RN, PhD, APN, CWOCN
Background Pressure ulcers are one of the most underrated
conditions in critically ill patients. Despite the introduction of
clinical practice guidelines and advances in medical technol-
ogy, the prevalence of pressure ulcers in hospitalized patients
continues to escalate. Currently, consensus is lacking on the
most important risk factors for pressure ulcers in critically ill
patients, and no risk assessment scale exclusively for pres-
sure ulcers in these patients is available.
Objective To determine which risk factors are most predictive
of pressure ulcers in adult critical care patients. Risk factors
investigated included total score on the Braden Scale, mobility,
activity, sensory perception, moisture, friction/shear, nutrition,
age, blood pressure, length of stay in the intensive care unit,
score on the Acute Physiology and Chronic Health Evaluation
II, vasopressor administration, and comorbid conditions.
Methods A retrospective, correlational design was used to
examine 347 patients admitted to a medical-surgical intensive
care unit from October 2008 through May 2009.
Results According to direct logistic regression analyses, age,
length of stay, mobility, friction/shear, norepinephrine infusion,
and cardiovascular disease explained a major part of the vari-
ance in pressure ulcers.
Conclusion Current risk assessment scales for development
of pressure ulcers may not include risk factors common in
critically ill adults. Development of a risk assessment model
for pressure ulcers in these patients is warranted and could
be the foundation for development of a risk assessment tool.
(American Journal of Critical Care. 2011;20:364-375)
PREDICTORS OF
PRESSURE ULCERS IN
ADULT CRITICAL CARE
PATIENTS
C E 1.0 Hour
Notice to CE enrollees:A closed-book, multiple-choice examination following this article tests your under standing ofthe following objectives:
1. Identify the stages of pressure ulcers as definedby the National Pressure Ulcer Advisory Panel.
2. Describe the components of the Braden Scalefor assessing risk for pressure ulcers.
3. Discuss potential factors not included in theBraden Scale that can be predictors for pres-sure ulcers in critical care populations.
To read this article and take the CE test online,visit www.ajcconline.org and click “CE Articles in This Issue.” No CE test fee for AACN members.
364 AJCC�AMERICAN JOURNAL OF CRITICAL CARE, September 2011, Volume 20, No. 5 www.ajcconline.org
©2011 American Association of Critical-Care Nursesdoi: http://dx.doi.org/10.4037/ajcc2011934
Pressure Ulcer Management
This article is supplemented by an AJCC Patient CarePage on page 376.
by guest on March 29, 2012ajcc.aacnjournals.orgDownloaded from

In 2006, the Centers for Medicare and MedicaidServices6 declared that hospital-acquired stage III orstage IV pressure ulcers are adverse patient safetyevents, or “never events,” that could reasonably beprevented by implementing evidence-based preven-tion guidelines. As a result, beginning in 2008, reim-bursement limitations were enacted for acute carehospitals for care associated with stage III or stageIV pressure ulcers not documented as present whena patient was admitted.7 This change has sparked arenewed urgency and awareness related to preventingpressure ulcers. Although the implementation ofcomprehensive prevention programs can reduce theprevalence of hospital-acquired pressure ulcers,8,9
pressure ulcers do develop in hospitalized patients,despite quality care and best practice. Furthermore,the risk for pressure ulcers may be greater for ICUpatients than for other patients.10-12
The first step in preventing pressure ulcers is deter-mining what constitutes appropriate risk. Many riskfactors have been identified empirically; however, con-sensus on the most important risk factors is lacking.
Review of Relevant LiteratureThe lack of a risk assessment scale exclusively for
determining the risk for pressure ulcers is an imped-iment to accurately determining risk in critical carepatients.3,13 In the United States, the Braden Scale14 isthe most widely used risk assessment tool in mostcare settings, including the ICU, and current clinicalpractice guidelines15-17 recommend its use. With theBraden Scale, derived from the conceptual framework
of Braden and Bergstrom,18 6 subscales are used tomeasure risk for pressure ulcers: sensory perception,activity, mobility, nutrition, moisture, and friction/shear. Potential scores range from 6 to 23; lowerscores indicate greater risk. Scores of 15 to 18 indi-cate risk or mild risk; scores of 13 to 14, moderaterisk; scores of 10 to 12, high risk; and scores of 9 orless, very high risk.19 Stratification of risk for pressureulcers can be useful clinically for determining andimplementing the appropriate level of prevention.20
Although evidence4,21-23 supports the total scoreon the Braden Scale as a predictor of pressure ulcersin critical care patients, investigation of the contribu-tions of the subscale scores has been limited, and thefindings have been inconclusive. Although the sub-scales of sensory perception,22,24 moisture,21,24 mobil-ity,21 and friction/shear24 have been found to besignificant predictors of pressure ulcerdevelopment in ICU patients, the activ-ity and nutrition subscales have not.
Other factors not included inthe Braden Scale may also increase apatient’s level of risk for pressure ulcersand thus be important determinantsin adult critical care patients. Empiricalevidence suggests that the followingfactors can be predictive of pressureulcers in critical care patients:advanced age1,4,21,25,26; low arteriolar pressure27-29; pro-longed ICU stay1,21,26,30; severity of illness as indicatedby scores on the Acute Physiology and ChronicHealth Evaluation (APACHE) II1,31; comorbid condi-tions, including diabetes mellitus, sepsis, and vasculardisease21,25,27; and iatrogenic factors, such as the useof vasopressor agents.1,25,27 Although research hasindicated that many of these factors are significantlyrelated to the development of pressure ulcers in ICUpatients, the findings were not consistent in all ofthe studies in which these relationships were tested.
Development of pressure ulcers is complex and multifactorial. In critical carepatients, pressure ulcers are an additional comorbid threat in patients who arealready physiologically compromised. In fact, pressure ulcers are one of themost underrated medical problems in critical care patients.1 Despite advancesin medical technology and the use of formalized prevention programs based
on clinical practice guidelines, the prevalence of pressure ulcers during hospitalization contin-ues to increase. In 2008, Russo et al2 of the Health Care Cost and Utilization Project reportedan 80% increase in the occurrence of pressure ulcers from 1993 to 2006 in hospitalized adultpatients and estimated that total associated health care costs were $11 billion. Among all hos-pitalized patients, prevalence rates of acquired pressure ulcers are the highest in patients in theintensive care unit (ICU), from 14% to 42%.3-5
About the AuthorJill Cox is an advanced practice nurse and a wound,ostomy, continence nurse at Englewood Hospital andMedical Center, Englewood, New Jersey.
Corresponding author: Jill Cox, RN, PhD, APN, CWOCN,
Englewood Hospital and Medical Center, 350 Engle St,Englewood NJ, 07631 (e-mail: [email protected]).
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, September 2011, Volume 20, No. 5 365
Pressure ulcersare one of themost underratedmedical problemsin critical carepatients.
by guest on March 29, 2012ajcc.aacnjournals.orgDownloaded from

medical-surgical ICU (MSICU) in Englewood Hos-pital and Medical Center, a suburban Magnet teach-ing hospital in Englewood, New Jersey.
SampleAll adult patients admitted to the MSICU from
October 2008 through May 2009 who met theinclusion criteria were included in this conveniencesample. Patients were included if they were 18 yearsor older and had an MSICU stay of 24 hours or greater.Patients were excluded if they had an MSICU stayof less than 24 hours or had a pressure ulcer at thetime of admission to the MSICU. A power analysiswas conducted for regression analysis to determinean appropriate sample size.32 In order to achieve apower of 80%, a minimum sample size of 163 wasneeded for a moderate effect size, a significance levelof α= .05, and 22 predictor variables.
Data CollectionData were abstracted from the hospital’s exist-
ing computerized documentation systems andincluded the following study variables: pressureulcer (recorded as present or absent at dischargefrom the MSICU); score on Braden Scale at thetime of admission to the MSICU; scores onBraden subscales at admission to the unit; age;arteriolar pressure (defined as the total numberof hours in the first 48 hours that the patient hadmean arterial pressure <60 mm Hg, and/or sys-tolic blood pressure <90 mm Hg, and/or diastolicblood pressure <60 mm Hg); length of MSICUstay; total number of hours of administration ofany of the following vasopressor agents duringthe MSICU stay: norepinephrine, epinephrine,vasopressin, dopamine, and phenylephrine; sever-ity of illness according to the APACHE II score;and presence or absence of any of the followingcomorbid conditions: diabetes mellitus, cardio-vascular disease, peripheral vascular disease, andconcomitant infection/sepsis. During the studyperiod, routine protocols for prevention of pres-sure ulcers were in place in the MSICU. The pro-tocols were based on the clinical practiceguidelines33,34 current at that time.
Demographic data and patient characteristicsincluded ethnicity, sex, and admitting MSICUdiagnosis. In addition, for patients in whom apressure ulcer developed, the number of hoursinto the admission the pressure ulcer occurred andthe anatomical location and stage of the pressureulcer according to the 2007 National PressureUlcer Advisory Panel staging system35 (Table 1)were recorded.
The purpose of my study was to determine whichrisk factors derived from the Braden Scale and theempirical literature are the best predictors of pressureulcers in adult critical care patients. The followingrisk factors were examined: total Braden score, mobil-ity, activity, sensory perception, moisture, nutrition,
friction/shear, ICU length of stay,age, arteriolar pressure, vasopressoradministration, score on APACHEII, and comorbid conditions.
MethodsThis study received exempt
status from the hospital’s institu-tional review board. The studyposed no risk to the participantsbecause the variables abstracted
reflected care parameters implemented and recordedduring routine patient care. All patient informationrecorded was deidentified to ensure patient anonymity.
Study Design and SettingA retrospective descriptive, correlational design
was used. The setting was an intensivist-led, 12-bed
366 �AJCC�AMERICAN JOURNAL OF CRITICAL CARE, September 2011, Volume 20, No. 5 www.ajcconline.org
Table 1 Pressure ulcer staging system of theNational Pressure Ulcer Advisory Panela
Stage Description
a Based on data from the National Pressure Ulcer Advisory Panel.
Suspected deeptissue injury
I
II
III
IV
Unstageable
Purple or maroon localized area of discolored intact skinor blood-filled blister due to damage of underlyingsoft tissue from pressure and/or shear
The area may be preceded by tissue that is painful, firm,mushy, boggy, and warmer or cooler than adjacent tissue
Intact skin with nonblanchable redness of a localizedarea, usually over a bony prominence
Darkly pigmented skin may not have visible blanching;its color may differ from that of the surrounding area
Partial-thickness loss of dermis manifested as a shallow,open ulcer with a red-pink wound bed, without slough
May also be manifested as an intact or open/rupturedserum-filled blister
Full-thickness tissue lossSubcutaneous fat may be visible, but bone, tendon, or
muscle are not exposedSlough may be present but does not obscure the depth
of tissue loss
Full-thickness tissue loss with exposed bone, tendon, ormuscle
Slough or eschar may be present on some parts of thewound
Often includes undermining and tunneling
Full-thickness tissue loss in which the base of the ulcer iscovered by slough (yellow, tan, gray, green, or brown)or eschar (tan, brown, or black) in the wound bed
Braden subscalesof activity and nutri-
tion have not beenuseful as risk pre-
dictors in intensivecare patients.
by guest on March 29, 2012ajcc.aacnjournals.orgDownloaded from

Data AnalysisSPSS, version 16.0 for Windows, software (SPSS
Inc, Chicago Illinois) was used for data analysis.Descriptive statistics included frequency distribu-tions for study variables and demographic data. ThePearson product moment correlation was used forcorrelational analyses of the study variables. Directlogistic regression was used to create the best modelfor predicting the development of pressure ulcers inICU patients. For comparison of study variablesbetween patients with and without pressure ulcers,t tests and χ2 analysis were used.
ResultsDescription of the Sample
Of the 579 patients admitted to the MSICUduring the study period, 347 met the inclusion cri-teria and were included in the final sample. Thepatients were 20 to 97 years old (mean, 69; SD, 17).The top 3 admitting diagnoses were respiratory fail-ure or distress (20.7%), sepsis or septic shock (17.3%),and neurological problems (15%). Demographiccharacteristics of the sample are summarized inTable 2.
Descriptive Statistics of the Study VariablesDescriptive statistics of the study variables are
summarized in Table 3. Among the 347 patients inthe sample, a pressure ulcer developed in 65 (18.7%).Of these ulcers, most (35%) were stage II, and thesacrum was the most common anatomical location(58%). Mean time until development of a pressureulcer was 133.61 hours (median 90.0; range, 5-573;SD, 120.13). The distribution of pressure ulcers bystage and hours to development is summarized inTable 4.
Mean Braden Scale scores were 14.28 (SD, 2.68;range, 6-23) for the entire patient sample, 12.73(SD, 2.65) for patients in whom pressure ulcersdeveloped, and 14.63 (SD, 2.65) for patients whoremained ulcer-free. Of the 65 patients in whom apressure ulcer developed, 28% (n = 18) were classi-fied as at risk, 28% (n = 18) as at moderate risk,35% (n = 23) as at high risk, and 9% (n = 6) as atvery high risk. Predictive validity of the Braden Scalewas measured by using sensitivity and specificityvalues in addition to negative and positive predic-tive values36 (Table 5). At a cut-off score of 18, thesensitivity was 100%, specificity was 7%, positivepredictive value was 20%, and negative predictivevalue was 100%. According to the scores on theBraden Scale, 94% of the sample was predicted tobe at risk for pressure ulcers; the actual occurrencerate was 18.7%.
Logistic Regression AnalysesIndependent variables significantly associated
with the dependent variable development of a pres-sure ulcer were included in direct logistic regression(Table 6). The following risk factors were significantpredictors of pressure ulcers: mobility (B= -0.823;P= .04; odds ratio [OR] = 0.439; 95% confidenceinterval [CI], 0.21-0.95), age (B=0.033;P= .03; OR = 1.033; 95% CI, 1.003-1.064), length of ICU admission (B= 0.008; P< .001; OR = 1.008; 95%CI, 1.005-1.011), and cardiovasculardisease (B= 1.082; P= .007; OR = 2.952;95% CI, 1.3-6.4; Table 7).
In order to better understand therisk factors that lead to actual breaksin skin integrity, a second direct logisticregression was done for a subsample ofthe population (n = 327) that excluded all patients inwhom a stage I pressure ulcer developed. The fol-lowing risk factors were significantly predictive ofthe development of a stage II or greater pressureulcer: friction/shear (B= 1.743; P= .01; OR = 5.715;95% CI, 1.423-22.950), length of ICU stay (B= .008;P< .001; OR = 1.008; 95% CI, 1.004-1.012), norepi-nephrine administration (B= .017; P= .04; OR=1.017;95% CI, 1.001-1.033), and cardiovascular disease
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, September 2011, Volume 20, No. 5 367
A pressure ulcer developedin 18.7% of thesample; mostwere stage IIsacral ulcers.
Table 2 Demographic characteristicsof the study sample (n = 347)
Characteristic Valuea
a Values are number (%) unless otherwise indicated. Because of rounding, not allpercentages total 100.
Age, mean (SD), range, y
SexMaleFemale
RaceWhiteBlack/African AmericanAsian/Pacific IslanderHispanicOther
Intensive care unit admitting diagnosisRespiratory arrest/distressSepsis/septic shockNeuromedical problemGeneral medical problemGastrointestinal bleedingNeurosurgical problemGastrointestinal surgical problemVascular surgical problemOther surgical problemCardiac conditionCardiac arrest
69 (17.0), 20-97
171 (49.3)176 (50.7)
255 (73.5)48 (13.8)26 (7.5)17 (4.9)
1 (0.3)
72 (20.7)60 (17.3)52 (15.0)44 (12.7)24 (6.9)24 (6.9)23 (6.6)17 (4.9)13 (3.7)12 (3.5)
6 (1.7)
by guest on March 29, 2012ajcc.aacnjournals.orgDownloaded from
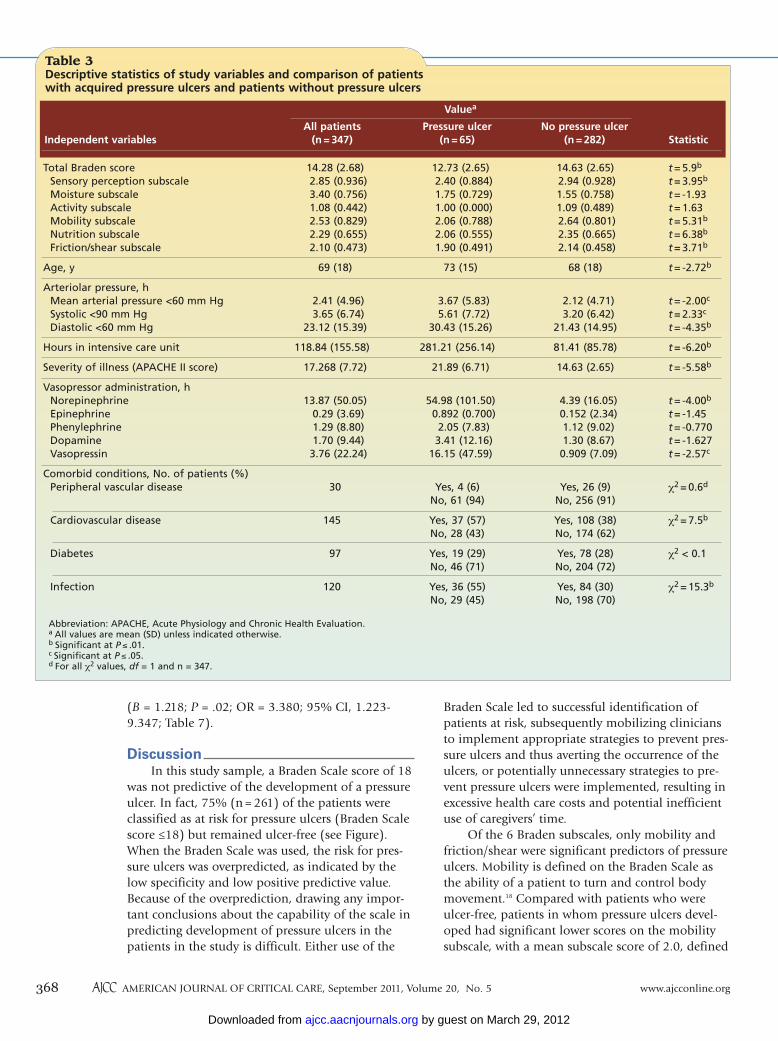
Braden Scale led to successful identification ofpatients at risk, subsequently mobilizing cliniciansto implement appropriate strategies to prevent pres-sure ulcers and thus averting the occurrence of theulcers, or potentially unnecessary strategies to pre-vent pressure ulcers were implemented, resulting inexcessive health care costs and potential inefficientuse of caregivers’ time.
Of the 6 Braden subscales, only mobility andfriction/shear were significant predictors of pressureulcers. Mobility is defined on the Braden Scale asthe ability of a patient to turn and control bodymovement.18 Compared with patients who wereulcer-free, patients in whom pressure ulcers devel-oped had significant lower scores on the mobilitysubscale, with a mean subscale score of 2.0, defined
(B = 1.218; P = .02; OR = 3.380; 95% CI, 1.223-9.347; Table 7).
DiscussionIn this study sample, a Braden Scale score of 18
was not predictive of the development of a pressureulcer. In fact, 75% (n = 261) of the patients wereclassified as at risk for pressure ulcers (Braden Scalescore ≤18) but remained ulcer-free (see Figure).When the Braden Scale was used, the risk for pres-sure ulcers was overpredicted, as indicated by thelow specificity and low positive predictive value.Because of the overprediction, drawing any impor-tant conclusions about the capability of the scale inpredicting development of pressure ulcers in thepatients in the study is difficult. Either use of the
368 �AJCC�AMERICAN JOURNAL OF CRITICAL CARE, September 2011, Volume 20, No. 5 www.ajcconline.org
Table 3 Descriptive statistics of study variables and comparison of patientswith acquired pressure ulcers and patients without pressure ulcers
Total Braden scoreSensory perception subscale Moisture subscaleActivity subscale Mobility subscaleNutrition subscaleFriction/shear subscale
Age, y
Arteriolar pressure, hMean arterial pressure <60 mm HgSystolic <90 mm HgDiastolic <60 mm Hg
Hours in intensive care unit
Severity of illness (APACHE II score)
Vasopressor administration, hNorepinephrineEpinephrinePhenylephrineDopamineVasopressin
Comorbid conditions, No. of patients (%)Peripheral vascular disease
Cardiovascular disease
Diabetes
Infection
14.28 (2.68)2.85 (0.936) 3.40 (0.756)1.08 (0.442)2.53 (0.829)2.29 (0.655) 2.10 (0.473)
69 (18)
2.41 (4.96) 3.65 (6.74)
23.12 (15.39)
118.84 (155.58)
17.268 (7.72)
13.87 (50.05)0.29 (3.69)1.29 (8.80)1.70 (9.44)3.76 (22.24)
30
145
97
120
12.73 (2.65)2.40 (0.884)1.75 (0.729)1.00 (0.000)2.06 (0.788)2.06 (0.555)1.90 (0.491)
73 (15)
3.67 (5.83)5.61 (7.72)
30.43 (15.26)
281.21 (256.14)
21.89 (6.71)
54.98 (101.50)0.892 (0.700)2.05 (7.83)3.41 (12.16)
16.15 (47.59)
Yes, 4 (6)No, 61 (94)
Yes, 37 (57)No, 28 (43)
Yes, 19 (29)No, 46 (71)
Yes, 36 (55)No, 29 (45)
14.63 (2.65)2.94 (0.928)1.55 (0.758)1.09 (0.489)2.64 (0.801)2.35 (0.665)2.14 (0.458)
68 (18)
2.12 (4.71)3.20 (6.42)
21.43 (14.95)
81.41 (85.78)
14.63 (2.65)
4.39 (16.05)0.152 (2.34)1.12 (9.02)1.30 (8.67)0.909 (7.09)
Yes, 26 (9)No, 256 (91)
Yes, 108 (38)No, 174 (62)
Yes, 78 (28)No, 204 (72)
Yes, 84 (30)No, 198 (70)
t = 5.9b
t = 3.95b
t = -1.93t = 1.63t = 5.31b
t = 6.38b
t = 3.71b
t = -2.72b
t = -2.00c
t = 2.33c
t = -4.35b
t = -6.20b
t = -5.58b
t = -4.00b
t = -1.45t = -0.770t = -1.627t = -2.57c
χ2 = 0.6d
χ2 = 7.5b
χ2 < 0.1
χ2 = 15.3b
Abbreviation: APACHE, Acute Physiology and Chronic Health Evaluation.a All values are mean (SD) unless indicated otherwise.b Significant at P ≤ .01.c Significant at P ≤ .05.d For all χ2 values, df = 1 and n = 347.
Independent variables StatisticNo pressure ulcer
(n = 282)Pressure ulcer
(n = 65)All patients
(n = 347)
Valuea
by guest on March 29, 2012ajcc.aacnjournals.orgDownloaded from

as very limited mobility. Turning and repositioningan immobile patient is a basic tenet of nursing careand is recommended in all current practice guide-lines as a strategy to prevent pressure ulcers. Althoughevidence for the optimal frequency for reposition-ing immobile patients is lacking,37 the guidelines16,17
indicate that regular repositioning is vital. Someevidence38 also supports the use of low air loss mat-tresses for pressure redistribution in ICU patients.The use of low air loss mattresses and regular turn-ing and repositioning of immobile patients may be2 essential strategies for preventing pressure ulcersin critical care patients. The effect of progressivemobility programs on reduction of pressure ulcersin ICU patients is an area ripe for empirical study.
Development of a stage II or greater pressureulcer was almost 6 times more likely in patients withhigher exposure to friction/shear than in patientswith low exposure. Previous studies in critical carepatients have yielded inconclusive evidence for thissubscale. Although Jiricka et al24 found a significancedifference in the mean Braden friction/shear sub-scale scores between patients in whom pressure ulcersdeveloped and patients who remained ulcer-free,other investigators21,22 found no relationship betweenthe subscale and development of pressure ulcers incritical care patients. In a recent study39 in a surgicaltrauma ICU, 41 patients at high risk for pressureulcers received an application of a silicone-bordered,nonadherent foam dressing to the sacral area tominimize the forces of friction, shear, and moisture.Application of this topical dressing significantlyreduced the occurrence of pressure ulcers to zero.The study is being replicated to validate the findings.
Immobile, critically ill patients are totallydependent on caregivers for both repositioning andtransfers, increasing the risk for exposure to theforces of friction/shear and subsequent develop-ment of pressure ulcers. Advocates of safe patienthandling procedures recommend the use of glidesheets and patient transfer devices to reduce thedeleterious effects of friction/shear on the skin andsimultaneously protect staff from musculoskeletalinjuries.40 Additional factors such as prolonged headelevation in critically ill, intubated patients to pre-vent ventilator-associated pneumonia or in enterallyfed patients to prevent aspiration also increase therisk for exposure to friction/shear. Continued researchinto the effects of prolonged head elevation on skinintegrity is warranted to better understand thesequelae of shear forces and to develop interventionsto counteract these forces.
In my study, patients in whom pressure ulcersdeveloped had lower mean scores on the Braden
sensory perception subscale than did patients whoremained ulcer-free. However, this subscale was nota significant predictor. Diminished levels of sensoryperception experienced by all patients in the samplemay have rendered this risk factor nonsignificant
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, September 2011, Volume 20, No. 5 369
Table 4 Analysis of patients with pressure ulcers
Characteristic
No. of pressure ulcers by stage and hours to detection
No. (%)a
Pressure ulcer
Pressure ulcer stageIIIIIIIVDeep tissue injury Unstageable
Pressure ulcer locationSacrumButtocks HeelsOther
Hours to pressure ulcer detection 1- 8
49-72 73-144≥145
Hours to detection
1-48
49-72
73-144
≥145
Stage I
8
2
3
7
Stage II
7
2
6
8
Stage III
0
0
1
0
Stage IV
0
0
0
1
Deep tissue injury
5
2
3
5
Unstage-able
1
1
2
1
Total
21
7
15
22
65 (18.7)
20 (31)23 (35)1 (2)1 (2)
15 (23)5 (7)
38 (58)22 (34) 3 (5)2 (3)
21 (32)7 (11)
15 (23)22 (34)
a Because of rounding, not all percentages total 100.
Criterion Description
Sensitivity
Specificity
Predictive value ofa positive test
Predictive value ofa negative test
What percentage of patients who actually had apressure ulcer develop were classified as at risk?
What percentage of patients who remained free of apressure ulcer were accurately classified as not at risk?
How accurate is the risk assessment scale as aprospective predictor of which patients will have apressure ulcer develop?
How accurate is the risk assessment scale as aprospective predictor of which patients will nothave a pressure ulcer develop?
a Based on data from Bolton.36
Table 5 Predictive validity criteria of a pressureulcer risk assessment scalea
by guest on March 29, 2012ajcc.aacnjournals.orgDownloaded from

when analyzed with other risk factors. In 2 previousstudies22,24 in critical care patients, however, scoreson the Braden sensory perception subscale werepredictive of pressure ulcers. Current pressure ulcerguidelines17 recommend that practitioners considerthe impact of the score on the Braden sensory per-ception subscale when determining a patient's riskfor pressure ulcers.
In my sample, the activity subscale was notrelated to development of pressure ulcers, a findingconsistent with the results of previous studies21,22,24
in critical care patients in which the Braden activitysubscale was used. Because most patients in theMSICU were bed bound, the patients in my samplehad little variation in activity levels.
A possible explanation for the finding that thescore on the Braden moisture subscale was not pre-dictive of pressure ulcers in my study is the frequentuse of indwelling devices that minimize skin expo-sure to moisture from 2 primary sources: urine(indwelling urinary catheters) and liquid stool(fecal containment devices). In 2 previous studies21,24
in ICU patients, scores on the Braden moisture sub-scale were predictive of pressure ulcers, and in anotherstudy,1 fecal incontinence was a significant risk fac-tor for pressure ulcers. Bowel management systems,also called fecal containment devices, were intro-duced to the clinical market in 2004, after theaforementioned studies were published. In a studyby Benoit and Watts,41 use of these devices in com-bination with strategies to prevent pressure ulcersdecreased the prevalence of pressure ulcers forpatients exposed to high levels of moisture fromliquid stool incontinence.
Although scores on the Braden nutrition subscalewere related to the development of pressure ulcersin my study, the scores were not a significant pre-dictor, consistent with the findings of previousstudies21,22,24 in ICU patients. The score on this sub-scale is a measure of the usual food intake of apatient, and most critically ill patients may havedifficulty articulating a diet history or be unable todo so, especially in the initial days of an ICU admis-sion, diminishing the value of the subscale in thesepatients. In a previous study26 in ICU patients, how-ever, nutrition, measured as the number of dayswithout nutrition, was a significant predictor of thedevelopment of pressure ulcers. Additionally, theresults of measurements of many biological mark-ers of nutrition, such as body weight, serum levelsof albumin, and, in some instances, serum levels ofprealbumin, may be erroneous because of fluid shiftsthat occur in critical illness, thus creating greaterchallenges in determining appropriate objective
370 �AJCC�AMERICAN JOURNAL OF CRITICAL CARE, September 2011, Volume 20, No. 5 www.ajcconline.org
Independent variable Independent variable rr
Total Braden scoreMobilityActivitySensory perceptionMoistureFriction/shearNutritionAgeMean arterial
pressure <60 mm HgSystolic pressure
<90 mm HgDiastolic pressure
<60 mm Hg
Hours in intensive care unit
Severity of illness (APACHE II score)
Vasopressor administrationNorepinephrinePhenylephrineEpinephrineDopamineVasopressin
Comorbid conditionsCardiovascular diseasePeripheral vascular diseaseDiabetes mellitusInfection
0.288a
0.395a
0.0410.0780.0870.268a
0.147a
-0.0430.0140.210a
-0.276a
-0.275a
-0.088-0.208a
0.1040.196a
-0.175a
0.130b
0.122b
0.140a
0.228a
0.502a
Abbreviation: APACHE, Acute Physiology and Chronic Health Evaluation.a Significant at P ≤ .01.b Significant at P ≤ .05.
Table 6 Bivariate correlations: independent variables anddependent variable (pressure ulcer development)
Variable
95% Confidence
intervalExp (B)B PWaldStandard
error
Age
Hours in intensive careunit
Cardiovasculardisease
Mobility
Constant
Logistic regression (n = 347)
1.003 to 1.064
1.005 to 1.011
1.3 to 6.4
0.210 to 0.95
1.033
1.008
2.952
0.439
0.001
.03
<.001
.007
.04
.01
4.725
21.996
7.288
4.262
6.087
0.015
0.002
0.401
0.398
2.857
0.033
0.008
1.082
-0.823
-7.049
Nagelkerke R2 = 0.512.Hosmer and Lemeshow test: χ2 = 6.993, df = 8, P = .54.
Table 7 Logistic regression analyses
Variable
95% Confidence
intervalExp (B)B PWaldStandard
error
Hours in inten-sive care unit
Cardiovasculardisease
Friction/shear
Norepinephrine
Constant
Logistic regression (n = 327), subsample of all patients excluding patientswith stage I pressure ulcers
1.004 to 1.012
1.223 to 9.347
1.423 to 22.95
1.001 to 1.033
1.008
3.380
5.715
1.017
0.000
<.001
.02
.01
.04
.005
18.063
5.510
6.039
4.223
7.737
0.002
0.519
0.709
0.008
3.779
0.008
1.218
1.743
0.017
-10.512
Nagelkerke R2 = 0.569.Hosmer and Lemeshow test: χ2 = 5.836, df = 8, P = .67.
by guest on March 29, 2012ajcc.aacnjournals.orgDownloaded from

nutritional markers. Currently, there is a lack ofconsensus among researchers and clinicians regard-ing the best metric of nutritional status.42
In my study, risk factors not included in theBraden Scale, that is, age, length of ICU stay, norepi-nephrine administration, and cardiovascular disease,were all significant predictors. The mean age of patientsin whom pressure ulcers developed was 73 years,whereas the mean age in patients who remainedulcer-free was 67 years. Strong empirical evidencesupports the relationship between advanced ageand development of pressure ulcers in critical carepatients, and perhaps this risk factor should begiven stronger consideration for inclusion in a riskassessment scale.1,4,21,25,26
In my study, development of pressure ulcerswas more likely in patients with longer ICU staysthan in patients with shorter stays. This result isconsistent with the findings of previous studies.1,21,26
In my study, the mean MSICU stay was 281 hours(11.7 days) for patients in whom a pressure ulcerdeveloped and 81 hours (3.3 days) for patients whoremained ulcer-free.
The most vulnerable time for development ofpressure ulcers during the MSICU stay was the firstweek; 66% of the sample had development of apressure ulcer in the first 6 days of their MSICUstay, a finding consistent with the results of otherstudies22,23,43 in critical care patients. On the basis ofthis finding, the first week of a patient’s ICU stayshould be a period of hypervigilance to assess therisk for pressure ulcers, and strategies to preventsuch ulcers should be aggressively implemented. Par-adoxically, the first week of an ICU stay may also bethe most likely period in which a patient experi-ences the greatest physiological instability, requiringnurses and other members of the health care teamto manage multiple life-saving technologies whilesimultaneously preventing pressure ulcers. Duringthis time, communication among all members ofthe health care team of the potential for pressureulcers is crucial. Moreover, a multidisciplinary forumcan underscore the premise that prevention of pres-sure ulcers is the responsibility of all members ofthe health care team, not just nurses.
In my study, norepinephrine was the only vaso-pressor that was a significant predictor for pressureulcers, a finding consistent with the results of previ-ous studies1,27 in ICU patients. Of note, 32 of the 65patients (49%) in my study who had a pressure ulcerdevelop received norepinephrine. Moreover, the meannumber of hours of norepinephrine infusions inpatients who had stage II or higher pressure ulcerswas significantly higher (55 hours) than in patients
who remained ulcer-free (4 hours). Evidence tosupport norepinephrine as a predictor of pressureulcers in critical care patients is increasing.1,27
Cardiovascular disease was the only comorbidcondition in my study that was a significant predic-tor of pressure ulcers. In my sample, 57% of patientsin whom pressure ulcers developed had cardiovas-cular disease. Although cardiovascular disease hasbeen associated with the development of pressureulcers in non-ICU patients and in cardiac surgerypatients,44-47 this comorbid condition has not beenstudied extensively as a risk factor ingeneral ICU patients. Further researchis needed to elucidate the importanceof this unmodifiable risk factor in thedevelopment of pressure ulcers ingeneral critical care patients.
In my study, patients in whom apressure ulcer developed had signifi-cantly lower mean diastolic bloodpressures, lower mean arterial pres-sure, and lower mean systolic bloodpressures than did patients whoremained free of pressure ulcers.However, none of these variables was a significantpredictor. In 3 previous studies27,28,43 in ICU patients,no significant relationships were found between anymeasure of blood pressure and development ofpressure ulcers. In another study,29 diastolic bloodpressure was lower in critical care patients in whompressure ulcers developed; however, this relationshipwas not statistically significant. The finding thatnone of the blood pressure variables was a predictorof pressure ulcers in my study and in other studiesis noteworthy and may be due to the frequent mon-itoring of blood pressure in critical care patients,resulting in quicker implementation of interventions
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, September 2011, Volume 20, No. 5 371
Figure Score on the Braden Scale and occurrence of pressureulcers (blue bars, present; red bars, absent).
No
. of
pat
ien
ts
Score on Braden Scale
019-23 15-18 13-14 10-12 6-9
75
100
125
50
25
The first week of stay in the intensive care unitshould be a periodof hypervigilancefor pressure ulcer risk.
by guest on March 29, 2012ajcc.aacnjournals.orgDownloaded from

to increase arterial pressure. In my study, the findingmay also represent a methodological limitation,because measurement of blood pressures was con-fined to the first 48 hours of the MSICU stay.
Although severity of illness was not predictiveof pressure ulcers in my sample, patients in whompressure ulcers developed had significantly highermean APACHE II scores (21.89; SD, 6.71) than didpatients who remained ulcer-free (mean, 14.63; SD,
2.65), suggesting that patientswith pressure ulcers had a greaterdisease burden. This finding isconsistent with the results of aprevious study31 in ICU patients.The APACHE II score (at ≥13)was predictive of pressure ulcersin only one study.1 A total of 36of the 347 patients in my sampledied, an overall mortality rate of
10%. Among the patients who died during theirMSICU stay, almost half (17) had a pressure ulcerat the time of death. Although APACHE II scores area valid measure of severity of illness and mortalityrisk, they may not be a reliable empirical indicatorfor severity of illness as a risk for development ofpressure ulcers.
LimitationsThe retrospective nature of this study is a limi-
tation. However, most of the data abstracted repre-sent objective clinical data that would not vary onthe basis of the study design. Using only the BradenScale measurements recorded in the first 24 hoursof the ICU stay may also be a limitation; however,
determining risk early during apatient’s stay is crucial becausethe determination may result inearlier implementation of pre-vention strategies. The inabilityto assess and stage developingpressure ulcers is also a limita-tion of a retrospective design.Pressure ulcers were staged andrecorded in the patients’ record
by staff nurses who are educated annually on assess-ment and staging of pressure ulcers and use of theBraden Scale. Use of a single study site also dimin-ishes the generalizability of the study findings.
ConclusionsCritical care patients are a unique subset of hos-
pitalized patients and are the sickest patients in thehealth care system. ICU patients are repeatedly con-fronted with multiple, concomitant risk factors for
372 �AJCC�AMERICAN JOURNAL OF CRITICAL CARE, September 2011, Volume 20, No. 5 www.ajcconline.org
development of pressure ulcers, and no consensusexists on how best to measure these factors.3,13
Although specific measures of risk for pressure ulcersare available for other populations of patients, includ-ing children, neonates, patients who receive care athome, patients who receive hospice and palliativecare, and patients with spinal cord injuries,17,18,48 nosuch tool exists for critical care patients, creating abarrier to accurate assessment of risk for pressureulcers in ICU patients.
Accurate identification of risk factors is a pre-requisite for determining appropriate strategies toprevent pressure ulcers. However, even with consis-tent and ongoing skin assessment, early identificationof skin changes, and the implementation of appro-priate prevention strategies to minimize damage,skin and tissue damage can occur in critically illpatients.49 Certain prevention strategies, such asturning of a patient whose hemodynamic status isunstable, may be medically contraindicated, andadequate prevention of pressure ulcers in patientswith multiple risk factors is difficult.50 Paradoxically,occurrence of pressure ulcers in hospitalized patients,including critical care patients, is considered anadverse event by the Centers for Medicare and Med-icaid Services, leaving caregivers in a challenging sit-uation of trying to prevent a pressure ulcer that maynot realistically be preventable. Continued researchon risk factors for pressure ulcers in critical carepatients is imperative, not only to ultimately decreasethe prevalence of pressure ulcers but also to helpcaregivers identify and implement risk appropriateevidence-based strategies to prevent the ulcers. Addi-tionally, research will validate the existence of riskfactors for pressure ulcers that cannot be controlledand thus are not preventable.
My results demonstrate the multifactorial causesof pressure ulcers in critical care patients. Althoughscores on 2 Braden subscale risk factors (mobility,friction/shear) were predictive of pressure ulcers,other risk factors not measured by the Braden Scale,including age, length of ICU stay, norepinephrineadministration, and cardiovascular disease, alsowere significant predictors in multivariate analysis.
My findings underscore the need for develop-ment and testing of model for assessing the risk forpressure ulcers in ICU patients, in order to providea basis for explaining the development of pressureulcers in these patients. This model could serve asthe foundation for development of a pressure ulcerrisk assessment scale for critical care patients. AlthoughPancorbo-Hildago et al51 have stated that use of arisk assessment scale increases the implementationof pressure ulcer initiatives, the ultimate test is the
Only mobility andfriction/shear
Braden subscaleswere predictors of
pressure ulcers.
A model for assessing pressure
ulcer risk in inten-sive care patients
is needed.
by guest on March 29, 2012ajcc.aacnjournals.orgDownloaded from

ability to translate the findings of such an assessmentinto a reduction in the occurrence of pressureulcers. Little evidence supports such a reductionwhen current risk assessment tools are used.16,17,51-53
Many opportunities exist for research on theeffects of various prevention strategies, such as sup-port surfaces, fecal containment devices, frequencyof repositioning, the use of topical dressings appliedto the sacrum to minimize friction/shear, progres-sive mobility programs, and the use of glide sheetsand patient transfer equipment, on the developmentof pressure ulcers in ICU patients. Ultimately, accu-rate identification of the risk factors for pressureulcers and testing and implementing evidence-basedprevention strategies can lead to reductions in boththe occurrence of pressure ulcers and health carecosts and can promote positive health outcomes incritical care patients.
ACKNOWLEDGMENTSThis research was done at Englewood Hospital andMedical Center.
FINANCIAL DISCLOSURESNone reported.
REFERENCES1. Theaker C, Mannan M, Ives N, Soni N. Risk factors for pres-
sure sores in the critically ill. Anaesthesia. 2000;55:221-224.2. Russo C, Steiner C, Spector W. Hospitalizations related to
pressure ulcers among adults 18 years and older, 2006.Healthcare Cost and Utilization Project, Statistical Brief 64.Agency for Healthcare Quality and Research Web site.http://www.hcup-us.ahrq.gov/reports/statbriefs/sb64.pdf.Published December 2008. Accessed June 3, 2011.
3. Keller P, Wille J, van Ramshorst B, van der Werken C. Pres-sure ulcers in intensive care patients: a review of risks andprevention. Intensive Care Med. 2002;28(10):1379-1388.
4. Shahin ES, Dassen T, Halfens RJ. Pressure ulcer prevalencein intensive care patients: a cross-sectional study. J EvalClin Prac. 2008;14:563-568.
5. VanGilder C, Amlung S, Harrison P, Meyer S. Results of the2008-2009 International Pressure Ulcer Prevalence Surveyand a 3-year acute care, unit-specific analysis. OstomyWound Manage. 2009;55(11):39-45.
6. Centers for Medicare and Medicaid Services. Eliminatingserious, preventable and costly medical errors–neverevents. Centers for Medicare and Medicaid Services Website. http://www.cms.hhs.gov/apps/media/press/release.asp?Counter=1863. Published May 18, 2006. AccessedJune 3, 2011.
7. Centers for Medicare and Medicaid Services. CMS proposesadditions to hospital-acquired conditions for fiscal year
2009. Centers for Medicare and Medicaid Services Website. http://www.cms.gov/apps/media/fact_sheets.asp. Pub-lished April 14, 2008. Accessed June 3, 2011.
8. Institute for Healthcare Improvement. Relieve the pressureand reduce harm. Institute for Healthcare ImprovementWeb site. http://www.ihi.org/IHI/Topics/PatientSafety/Safety-General/ImprovementStories/FSRelievethePressureandReduceHarm.htm. Published May 21, 2007. Accessed June4, 2011.
9. Agency for Health Care Research and Quality, InnovationsExchange. Comprehensive, interdisciplinary guidelines,combined with tools to increase adherence, significantlyreduce hospital-acquired pressure ulcers. Agency forHealth Care Research and Quality Web site. http://www.innovations.ahrq.gov/content.aspx?id=2589. PublishedMarch 3, 2010. Updated April 13, 2011. Accessed June 4,2011.
10. Baumgarten M, Margolis D, Berlin J, et al. Risk factors forpressure ulcers among elderly hip fracture patients. WoundRepair Regen. 2003;11(2):96-103.
11. Baumgarten M, Margolis DJ, Localio AR, et al. Extrinsic riskfactors for pressure ulcers early in the hospital stay: anested case-control study. J Gerontol A Biol Sci Med Sci.2008;63(4):408-413.
12. Krapfl L, Mackey D. Medicare changes to the hospital inpa-tient prospective payment systems: commentary on theimplications for the hospital-based wound care clinician. J Wound Ostomy Continence Nurs. 2008;35(1):61-62.
13. de Laat E, Schoonhoven L, Pickkers P, Verbeek A, vanAch -terberg T. Epidemiology, risk and prevention of pressureulcers in critically ill patients: a review of the literature. J Wound Care. 2006;15(6):269 275.
14. Bergstrom N, Braden B, Laguzza A, Holman V. The BradenScale for predicting pressure sore risk. Nurs Res. 1987;36(4):205-210.
15. Lyder CH, Ayello EA. Pressure ulcers: a patient safety issue.In: Hughes R, ed. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Rockville, MD: Agency forHealthcare Quality and Research; 2008. AHRQ publication08-0043.
16. Wound Ostomy and Continence Nurses Society. Guideline forthe Prevention and Management of Pressure Ulcers. Mt Laurel,NJ: Wound, Ostomy and Continence Nurses Society; 2010.
17. National Pressure Ulcer Advisory Panel and European Pres-sure Ulcer Advisory Panel. Prevention and Treatment ofPressure Ulcers: Clinical Practice Guideline. Washington,DC; National Pressure Ulcer Advisory Panel; 2009.
18. Braden B, Bergstrom N. A conceptual schema for the studyof the etiology of pressure sores. Rehabil Nurs. 1987;12(1):8-12,15.
19. Braden B. Protocols by level of risk. http://www.bradenscale.com/images/protocols_by_level_of_risk.pdf. Published2001. Accessed June 4, 2011.
20. Ayello EA, Braden B. How and why do pressure ulcer riskassessment? Adv Skin Wound Care. 2002;15(3):125-133.
21. Bours G, De Laat E, Halfens R, Lubbers M. Prevalence, riskfactors and prevention of pressure ulcers in Dutch inten-sive care units. Intensive Care Med. 2001;27:1599-1605.
22. Carlson E, Kemp M, Shott S. Predicting the risk of pressureulcers in critically ill patients. Am J Crit Care. 1999;8(4):262-269.
23. Fife C, Otto G, Capsuto E, et al. Incidence of pressure ulcersin a neurologic intensive care unit. Crit Care Med. 2001;29(2):273-290.
24. Jiricka M, Ryan P, Carvalho M, Bukvich J. Pressure ulcer riskfactors in an ICU population. Am J Crit Care. 1995;4(5):361-367.
25. Frankel H, Sperry J, Kaplan L. Risk factors for pressureulcer development in a best practice surgical intensive careunit. Am Surg. 2007;73:1215-1217.
26. Eachempati S, Hydo L, Barie P. Factors influencing thedevelopment of decubitus ulcers in critically ill surgicalpatients. Crit Care Med. 2001;29(9):1678-1682.
27. Batson S, Adam S, Hall G, Quirke S. The development of apressure area scoring system for critically ill patients: apilot study. Intensive Crit Care Nurs. 1993;9:146-151.
28. Pender L, Frazier S. The relationship between dermal ulcers,oxygenation and perfusion in mechanically ventilatedpatients. Intensive Crit Care Nurs. 2005;21:29-38.
29. Seturan L, Karabacak U, Ozdilek S, et al. The relationshipamong pressure ulcers, oxygenation, and perfusion inmechanically ventilated patients in an intensive care unit.
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, September 2011, Volume 20, No. 5 373
eLettersNow that you’ve read the article, create or contribute to anonline discussion on this topic. Visit www.ajcconline.organd click “Respond to This Article” in either the full-text orPDF view of the article.
SEE ALSOFor more about preventing pressure ulcers, visit theCritical Care Nurse Web site, www.ccnonline.org, andread the article by Jankowski, “Tips for ProtectingCritically Ill Patients From Pressure Ulcers” (April2010).
by guest on March 29, 2012ajcc.aacnjournals.orgDownloaded from
tors in ICU patients: nursing skin assessment versus objec-tive parameters. J Wound Care. 2008;17(10):417-420, 422-424.
44. Bergstrom N, Braden B, Kemp M, Champagne M, Ruby E.Multi-site study of incidence of pressure ulcers and therelationship between risk level, demographic characteristics,diagnoses and prescription of preventive interventions. J Am Geriatr Soc. 1996;44(1):22-30.
45. Lindgren M, Unosson M, Fredrickson M, Ek A. Immobility—a major risk factor for development of pressure ulcersamong adult hospitalized patients: a prospective study.Scand J Caring Sci. 2004;18(1):57-64.
46. Lewicki L, Mion L, Splane K, Samstag D, Secic M. Patientrisk factors for pressure ulcers during cardiac surgery.AORN J. 1997;65(5):933-942.
47. Pokorny M, Koldjeski D, Swanson M. Skin care interven-tions for patients having cardiac surgery. Am J Crit Care.2003;12(6):535-544.
48. Spinal Cord Injury Rehabilitation Evidence. Outcome Meas-ures. Spinal cord injury pressure ulcer risk scale. SpinalCord Injury Rehabilitation Evidence Web site. http://www.scireproject.com/outcome-measures. Published 2010.Accessed June 6, 2011.
49. Langemo D, Brown G. Skin fails too: acute, chronic and end-stage skin failure. Adv Skin Wound Care. 2006;19(4):206-211.
50. Wound, Ostomy and Continence Nurses Society. Wound,Ostomy and Continence Nurses Society position statementon avoidable versus unavoidable pressure ulcers. J WoundOstomy Continence Nurs. 2009;36(4):378-381.
51. Pancorbo Hildago T, Garcia Fernandez F, Lopez Madina I,Alvarez Nieto C. Risk assessment scales for pressure ulcer pre-vention: a systematic review. J Adv Nurs. 2006;54(1):94-110.
52. Anthony D, Papanikolaou P, Parboteeah S, Saleh M. Do riskassessment scales for pressure ulcers work? J Tissue Viability.2010;19(4):132-126. doi:10.1016/j.jtv.2009.11.006.
53. Stechmiller J, Cowan L, Whitney J, et al. Guidelines for theprevention of pressure ulcers. Wound Repair Regen. 2008;16(2):151-168.
J Wound Ostomy Continence Nurs. 2009;36(5):503-508.30. Sayar S, Turgut S, Dogan H, et al. Incidence of pressure
ulcers in intensive care unit patients at risk according tothe Waterlow scale and factors influencing the develop-ment of pressure ulcers. J Clin Nurs. 2008;18(5):765-774.
31. Shahin E, Dassen T, Halfens R. Incidence, prevention andtreatment of pressure ulcers in intensive care patients: alongitudinal study. Int J Nurs Stud. 2009;46:413-421.
32. Cohen J. Statistical Power Analysis for the Behavioral Sci-ences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Assoc; 1988.
33. Wound Ostomy and Continence Nurses Society. Guidelinefor the Prevention and Management of Pressure Ulcers.Glenview, IL: Wound, Ostomy and Continence Nurses Society;2003.
34. Agency for Health Care Policy and Research. Pressure Ulcersin Adults: Prediction and Prevention. Rockville, MD: Agencyfor Health Care Policy and Research; 1992. AHCPR publica-tion 92-0047.
35. National Pressure Ulcer Advisory Panel. Updated stagingsystem: pressure ulcer stages revised by NPUAP. NationalPressure Ulcer Advisory Panel Web site. http://www.npuap.org/pr2.htm. Published 2007. Accessed June 4, 2011.
36. Bolton L. Which pressure ulcer risk assessment scales arevalid for clinical use? J Wound Ostomy Continence Nurs.2007;34(4):368-381.
37. Krapfl L, Gray M. Does regular repositioning prevent pres-sure ulcers? J Wound Ostomy Continence Nurs. 2008;35(6):571-577.
38. McInnes E, Bell Syer SE, Dumville JC, Legood R, Cullum NA.Support surfaces for pressure ulcer prevention. CochraneDatabase Syst Rev. 2008;8(4):CD001735.
39. Brindle CT. Outliers to the Braden Scale: identifying highrisk ICU patients and the results of prophylactic dressinguse. WCET J. 2010;30(1):11-18.
40. Sibbald R, Norton L, Woo K. Optimized skin care can preventpressure ulcers. Adv Skin Wound Care. 2009;22(9):392.
41. Benoit R, Watts C. The effect of a pressure ulcer preventionprogram and the bowel management system in reducingpressure ulcer prevalence in an ICU setting. J WoundOstomy Continence Nurs. 2007;34(2):163-175.
42. Doughty DB. Prevention and early detection of pressureulcers in hospitalized patients. J Wound Ostomy ContinenceNurs. 2008;35(1):76-78.
43. Compton F, Hoffmann F, Hortig T, et al. Pressure ulcer predic-
374 �AJCC�AMERICAN JOURNAL OF CRITICAL CARE, September 2011, Volume 20, No. 5 www.ajcconline.org
To purchase electronic or print reprints, contact TheInnoVision Group, 101 Columbia, Aliso Viejo, CA 92656.Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax,(949) 362-2049; e-mail, [email protected].
by guest on March 29, 2012ajcc.aacnjournals.orgDownloaded from

Name Member #
Address
City State ZIP
Country Phone E-mail address
RN License #1 State
RN License #2 State
Payment by: ❑ Visa ❑ M/C ❑ AMEX ❑ Check
Card # Expiration Date
Signature
CE Test Test ID A112005: Predictors of Pressure Ulcers in Adult Critical Care Patients. Learning objectives: 1. Identify the stages of pressure ulcers asdefined by the National Pressure Ulcer Advisory Panel. 2. Describe the components of the Braden Scale for assessing risk for pressure ulcers. 3. Discuss poten-tial factors not included in the Braden Scale that can be predictors for pressure ulcers in critical care populations.
Program evaluationYes No
Objective 1 was met ❑ ❑Objective 2 was met ❑ ❑Objective 3 was met ❑ ❑Content was relevant to my
nursing practice ❑ ❑My expectations were met ❑ ❑This method of CE is effective
for this content ❑ ❑The level of difficulty of this test was: ❑ easy ❑ medium ❑ difficult
To complete this program, it took me hours/minutes.
Test ID: A112005 Contact hours: 1.0 Form expires: September 1, 2013. Test Answers: Mark only one box for your answer to each question. You may photocopy this form.
1. Which of the following is the estimated percentage of hospitalacquired pressure ulcers in intensive care patients? a. 13% to 35% c. 16% to 63%b. 14% to 42% d. 17% to 71%
2. Which of the following explains the reasoning for the Centersfor Medicare and Medicaid Services’ limited reimbursementfor “never events?”a. They can be prevented by implementing evidence-based preven-tive measuresb. They are grounds for malpractice against the nursing staffc. They are unavoidable consequences of properly organized cared. They are inexpensive to treat
3. Which of the following Braden scores belongs to the patientwith a high risk for developing a pressure ulcer?a. 16 c. 11b. 13 d. 8
4. Which of the following pressure ulcer risk factors was notincluded as part of the Braden Scale? a. Sensory perception c. Low arteriolar pressureb. Mobility d. Nutrition
5. Which of the following was included in the def inition oflow arteriolar pressure in the study? a. Number of hypotensive hours during intensive care unit (ICU) stayb. Mean arterial pressure <60c. Systolic blood pressure <100d. Diastolic blood pressure <70
6. In this study, which of the following were the most commonanatomical location and stage of pressure ulcers? a. Buttocks; stage IIb. Sacrum; stage Ic. Sacrum; stage IId. Buttocks; stage I
7. In this study, which of the following Braden Scale categorieswas signif icant for predicting pressure ulcers? a. Nutrition and mobilityb. Moisture and friction/shearc. Moisture and nutritiond. Mobility and friction/shear
8. Which of the following factors increases the risk of exposureto friction and shear?a. Using a glide sheetb. Applying a silicone bordered dressingsc. Elevating the head of the bed for a prolonged periodd. Using a low air loss mattress
9. Use of which of the following explains the lack of predictabilityof the moisture subscale in this study compared to previousstudies?a. Silicone bordered dressingsb. Less indwelling urinary cathetersc. Bowel management systemsd. Low air loss mattresses
10. Which of the following vasoactive drug infusions was a sta-tistically signif icant predictor for pressure ulcers in the study?a. Neosynephrine c. Vasopressinb. Norepinephrine d. Epinephrine
11. Which of the following comorbidities had statistical signif icance as a predictor for pressure ulcers in the study?a. Cardiovascular disease c. Infectionb. Diabetes d. Peripheral vascular disease
12. If a patient has a 5 cm shallow ulcer into the dermal layerthat has a pink wound bed but no sloughing, this would becategorized as which of the following?a. Stage I pressure ulcer c. Unstagableb. Stage II pressure ulcer d. Suspected deep tissue injury
For faster processing, takethis CE test online at
www.ajcconline.org (“CEArticles in This Issue”) ormail this entire page to:AACN, 101 Columbia, Aliso Viejo, CA 92656.
Fee: AACN members, $0; nonmembers, $10 Passing score: 10 correct (77%) Category: A, Synergy CERP A Test writer: Marylee Bressie, MSN, RN, CCRN, CCNS, CEN.
9. ❑a❑b❑c❑d
8. ❑a❑b❑c❑d
7. ❑a❑b❑c❑d
6. ❑a❑b❑c❑d
5. ❑a❑b❑c❑d
4. ❑a❑b❑c❑d
3. ❑a❑b❑c❑d
2. ❑a❑b❑c❑d
1. ❑a❑b❑c❑d
10. ❑a❑b❑c❑d
11. ❑a❑b❑c❑d
12. ❑a❑b❑c❑d
The American Association of Critical-Care Nurses is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
AACN has been approved as a provider of continuing education in nursing by the State Boards of Nursing of Alabama (#ABNP0062), California (#01036), and Louisiana (#ABN12). AACNprogramming meets the standards for most other states requiring mandatory continuing education credit for relicensure.
by guest on March 29, 2012ajcc.aacnjournals.orgDownloaded from