pregnancypregnancy. moderate and heavier drinkers were significantly more likely to smoke before...
TRANSCRIPT
Journal of Epidemiology and Community Health, 1989, 43, 153-161
Confounding variables in studying the effects ofmaternal alcohol consumption before and duringpregnancy
IAN WALPOLE,' STEPHEN ZUBRICK2 AND JACQUELINE PONTRE3From 'the Department of Paediatrics, Princess Margaret Hospital for Children, Perth, Western Australia;2Neurosciences Unit, Health Department of Western Australia; and 3the Research and Evaluation Unit, HealthDepartment of Western Australia.
ABSTRACTStudy objective: to investigate the relationship between alcohol consumption and pregnancyoutcome.Design: prospective randomised cohort survey with follow up sample stratified on level of alcoholintake.Setting: antenatal clinic of large maternity hospital in Western Australia.Participants: 2002 randomly selected pregnant women recruited over 3 year period for questionnairesurvey (58% in 1st trimester, 33% in 2nd trimester, 8% in third trimester at recruitment). Only 19refused participation. Stratified subsample of 665 women followed up, ofwhom 60 had miscarriage,stillbirth or neonatal death. Subsample was selected on basis of prepregnancy alcohol consumption.Investigations and main results: All 2002 women completed a comprehensive questionnaire on
demographic, lifestyle, health (including diet) and obstetric factors. The stratified subsample was
followed through pregnancy and data were collected on obstetric course and infant outcome. Resultsshowed that beer, wine and spirits drinkers differed significantly in maternal characteristics, nutritionand other important variables such as smoking. Women with stillbirths or miscarriages drank morebeer than those with live births, though total levels ofalcohol intake did not differ. Beer drinkers wereless likely to reduce their consumption in pregnancy than other drinkers if they also smoked morethan 20 cigarettes per day.Conclusions: Studies of effects of maternal drinking must include extensive information on thevariables examined in this study or conclusions relating to maternal drinking in pregnancy are likelyto be invalid.
Maternal alcohol ingestion has been implicated as acause of multiple serious effects on the developingfetus. 1-5 Social or moderate maternal alcohol intake issaid to result in offspring with reduced growth andhead circumference, increased rates of neurologicalabnormalities including intellectual handicap andbehavioural disturbance, malformations, prematurityand miscarriages, suggesting there is no safe level ofalcohol intake.5-'7 The most severe end result ofheavy, usually chronic, maternal alcohol abuse is thefetal alcohol syndrome. Criteria for diagnosis of thiscondition include antenatal and postnatal growthfailure of proportional distribution, intellectualsubnormality, and recognisable facial dysmorphicfeatures such as short palpebral fissures, broad lownasal bridge and a long shallow philtrum. Associated
birth defects, particularly of the central nervous,cardiovascular and musculoskeletal systems alsooccur. 1-5
Because an alcohol dose threshold for thesereported effects is not apparent, several authorities,including the US Surgeon General and the RoyalCollege of Psychiatrists, have advised total avoidanceof alcohol by pregnant women.'4 18-24 Suchstatements, issued as a matter of prudence, are notbased on conclusive evidence, and are contrary to thefindings of some workers.2531Many of the earlier reports of fetal alcohol
syndrome were retrospective and described highlyselected populations. Often information was obtainedfrom studies retrospectively or from studies notspecifically designed to look at alcohol effects.
153
Protected by copyright.
on March 14, 2020 by guest.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.43.2.153 on 1 June 1989. D
ownloaded from
154
Consequently, alcohol quantification methods weresometimes poor, and usually the type of beverage wasnot specified, with very little information on diet andinsufficient consideration of confounding variablessuch as socio-economic status, smoking or othersubstance abuse.'-16 27 28
Several animal models for fetal alcohol syndromehave been developed. There is general agreement thathigh doses of ethanol given to pregnant animalsproduce toxic fetal effects. These are not found withlow alcohol doses, suggesting a threshold effect.32-36The aim of this paper, therefore, was to determine
those methodological factors that might bias any ofthe described effects of light to moderate maternaldrinking on pregnancy outcome. An added impetusfor this study was the significant public concern aboutthe increasing use of alcohol by young women ofchildbearing age in this country.37Methods
SUBJECTSSubjects for this study were 2002 pregnant womenattending the public antenatal clinic of the mainmaternity hospital in Western Australia. The womenwere selected randomly between January 1982 andDecember 1984 at their first antenatal visit for thatparticular pregnancy. The majority of women (58%)were in the first trimester of their pregnancy atrecruitment, 33% were in the second and 8% were intheir third trimester. We compared our sample with avariety of demographic population characteristicsprovided by the Australian Bureau of Statistics. Thesample contains a higher proportion of single mothersthan is typical of the Australian population butotherwise it is indistinguishable from the populationof child bearing women in Western Australia in1981.38
QUESTIONNAIREThe questionnaire was of broad scope and consistedof items assessing demographic characteristics,prepregnancy weight and height, and details ofprevious pregnancies, as well as levels of smoking,consumption of coffee, soft drinks, beer, wine andspirits. Questions on beverages took the formnecessary to derive scores on levels ofabsolute alcohol(AA) consumption per day39 and could also be used toderive Calahan's quantitative frequenc-volume(QFV) and volume variability (VV) scores. Womenwere asked how frequently they drank each categoryof beverage using forced choice questions withresponse categories ranging from "never" to "three ormore times per day". They were also asked how oftenthey drank each ofthe quantities "5 or more", "3 or 4"or "1 or 2" glasses. Daily levels of absolute alcohol
Ian Walpole, Stephen Zubrick, and Jacqueline Pontre
were derived according to the procedure of Jessor etal.39 Questions on smoking required the women toreport how many cigarettes per day they smoked andwhich brand they usually smoked. Daily intakes ofnicotine and tar were then calculated. There werefurther questions on dietary habits, appetite, numberof meals per day, main food items consumed, andfrequency and method of cooking. From thisinformation it was possible to derive scores measuringintake of folate and other nutrients.
Medication usage was assessed and medicationswere divided into major groups. These were: non-narcotic analgesics; hypnotics and sedatives;indigestion and constipation medications; antibiotics;iron, vitamins and tonics; and nausea controlmedications.
PROCEDUREThe questionnaire briefly introduced the aim andpurposes of the study without specifically callingattention to alcohol use, and informed the respondentsthat all answers given were confidential. No verbaldirection on how to complete the questionnaire wasgiven, but a study researcher was available to answerquestions if necessary and check that forms had beencompleted. The questionnaire took between twentyand thirty minutes to complete.The reliability of answers to the smoking and
drinking items was assessed by sampling 50 mothersand retesting them within 4-6 weeks of the originalquestionnaire. Test-retest reliability (repeatability)coefficients were 0-85 and 0-87 respectively ondrinking and smoking items and were deemedacceptable.
IDENTIFICATION OF GROUPSComplete clinical and behavioural follow up ofmother-baby pairs was intended but with availableresources this meant limiting the follow up samplewhile still ensuring a range of alcohol consumption.Thus from the initial sample of 2002, a subsample of665 pregnant women, stratified on level of alcoholintake, was drawn. Stratified sampling ensured thatthe sample included a wide spectrum of drinkers.Mothers were selected for follow up during
confinement and postpartum on the basis of alcoholintake prior to pregnancy rather than duringpregnancy or a combination of the two measures. Thisdeliberate decision was based on a number of factorsincluding the often reported decline in maternalalcohol intake during pregnancy,69 41 as was laterdemonstrated in this study.
In the cohort of 665 pregnant women selected forstudy, 60 had subsequent outcomes of miscarriage(n = 42), still birth (n= 12) or neonatal death (n= 6).
Protected by copyright.
on March 14, 2020 by guest.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.43.2.153 on 1 June 1989. D
ownloaded from
Confounding variables in pregnancy alcohol consumption
Based on alcohol intake, the 665 mother-infantpairs were divided into three groups. Group I (n= 308)consisted of women who reported drinking less than2 8 ml (0 1 oz) of absolute alcohol daily. This groupincluded those who reported no alcohol intake. GroupII (n= 265) consisted ofmothers whose alcohol intakewas recorded as between 2-8 and 27-9 ml of absolutealcohol daily (0- 1 -099 oz); and Group III (n = 92)consisted of those whose alcohol intake was recordedas 28 ml (1 oz) or more daily. Two drinks of spirits,two glasses of wine or two and a half cans of beercontain approximately 28 ml absolute alcohol.' Thethree groups were called abstainers/light drinkers,moderate drinkers and heavy drinkers respectively.
OBSTETRC DATA COLLECTION AND INFANT OUTCOMEApproximately 100 further obstetric factors were thensought for the women of the above groups fromhospital records and, when records were inadequate,from further maternal interview. Particular attentionwas paid to past and current obstetric problems suchas miscarriage or bleeding, medical illness such as
diabetes, heart disease or infections (18 items), and tointrapartum and postpartum factors. The use ofmedications such as analgesics, their dosages and theirtiming were recorded, plus other possible neonatalrisks.Necropsy records for miscarriages, stillbirths and
neonatal deaths were examined.Physical examination was performed by the same
paediatrician on all the infants of the cohort. Thepaediatrician was unaware of the maternal drinkingstatus.
Neurobehavioural assessment was conducted usinga slightly modified version of the Albert Einsteinneurobehavioural assessment schedule, which isreliable and has been shown to distinguish lowbirthweight and premature infants from those ofnormal birthweight and gestation.42
Both the physical examination and theneurobehavioural assessment were undertakenbetween 24 and 72 h after birth unless the infant waspreterm, in which case assessment took place at theappropriate postconceptional age. Infant outcomeswill be the focus of a subsequent paper and are notreported here.
Results
ADEQUACY OF FOLLOW UP SAMPLESeveral comparisons were made of the characteristicsof the 665 mothers selected into the follow up cohortcompared with those who were not selected.Significant.ly more of those followed up were marriedas opposed to single (X2 = 22-45; df = 3; p<0-001).Otherwise there were no significant differences in
maternal height, weight, age, educational level,number of previous pregnancies, rate of cigarettesmoking and ethnicity for those chosen for follow upand those not chosen. In addition there were nosignificant differences in the level of alcoholconsumption both before and during pregnancy forthe mothers of children followed versus those notfollowed.
Overall we were satisfied that our samplingprocedure yielded a follow up group that wasrepresentative of the population ofwomen presentingat a major metropolitan maternity hospital.
CHARACTERISTICS OF LIGHT, MODERATE, AND HEAVYDRINKING WOMENTable 1 shows the characteristics of women identifiedas light, moderate and heavy drinkers beforepregnancy. Categorical data were compared using x2tests. Analysis of variance (ANOVA) was used forinterval level data.
Demographic factors-Moderate and heavy drinkerswere significantly more likely to be single, divorced orseparated and out of the work force. They were morelikely to be living alone or with a boyfriend. Light tomoderate drinking was more prevalent in whiteAustralians, while women of European extractionwere more likely to be heavier drinkers. Moderate toheavy drinking was significantly associated withhigher educational levels. There were no significantdifferences in parity among the three groups.
Physical characteristics-Moderate and heavydrinkers were taller than light drinkers, but there wereno significant differences in mean weight among thethree groups. Moderate and heavy drinkers weresignificantly older than light drinkers.
Diet and smoking-Analysis of variance revealed nosignificant differences in mean folate scores among thethree drinking groups either before or duringpregnancy. Moderate and heavier drinkers weresignificantly more likely to smoke before pregnancy(50% and 65-2%) than were light drinkers (36-6%).All groups were more likely to reduce their smokingduring pregnancy, but as table I shows, the positiveassociation between smoking and alcoholconsumption remained.
Medication-We studied the frequency distributionsof reported medication by aggregating data under themajor group headings, as well as examining thefrequency distributions of the subgroups. Thesedistributions took into account the type ofmedicationtaken as well as the frequency of usage.
155
Protected by copyright.
on March 14, 2020 by guest.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.43.2.153 on 1 June 1989. D
ownloaded from

156 Ian Walpole, Stephen Zubrick, and Jacqueline PontreTable 1 Characteristics of light, moderate, and heavy drinking women (n = 665)
Maternal characteristic
I Height (cm)
2 Weight (kg)
3 Age (years)
<2020-2425-2930-34>34
4 Cigarettes per day(before pregnancy)None<1010-20>20
5 Cigarettes per day(during pregnancy)None<1010-20>20
6 Alcohol(during pregnancy)AA < 2-8 ml/dAA 2-8-27-9 ml/dAA > 28 mI/d
7 Folate score(before pregnancy)LowMediumHigh
8 Folate score(during pregnancy)LowMediumHigh
9 Employment statusIn work forceHome makerNot in work force
10 ParityPrimipMultip
11 Ethnic groupAustralian, AboriginalAustralian, whiteAsianEuropean
12 Marital statusMarriedSingleDe factoDivorced/separated
13 Education< 3 yrs high school3 yrs high school4-5 yrs high schoolTertiary
14 Household compositionAloneWith husbandWith boyfriendOther arrangements
15 Pregnancy outcomeLive birthMiscarriageStillbirthNeonatal death
AA = absolute alcohol
Alcohol consumption before pregnancy
Light abstinent Moderate( < 2-8 ml AA daily) (2 8-27 9 ml AA daily)(n = 308) (n = 265)
X = 1617 X = 1641SD = 7-4 SD = 6-8X = 56-7 X = 57 8SD = 10 2 SD = 85X = 25-3 X = 26-6SD = 5-5 SD = 5-4
13-0 10-933-8 24-931 5 33-2159 24558 6-4
63-311 01629-4
73-713610-42-3
98-41-303
159707134
17569-1134
34-761 63-7
32-667-4
3-754-26-8
35-3
76-01307-83-2
15037-922924-3
6-673-35.9
14-2
89-97-81-60-6
50210-223-016-6
66-41251624-9
65734004
12269-6183
12668-419-0
48-342-59-3
37-662-4
3-262 11-6
33-2
70-21709 13-8
9-328-732-229-8
7-769-07-3
16-1
92-53-8231 5
Heavy(>28ml AA daily)(n= 92)
X = 1637SD = 6-8X = 57-1SD = 99X = 26-9SD = 5-7
10929-3239250109
348163185304
47-822-817.4120
40-246-7130
11-7740143
20066213*7
49-440-410 1
42-957-1
1.15522-3
41-4
56-024-212-17-7
9034-8303258
11-156-714-4178
902871.100
Statistical significance
F = 7-84p < 0001F = 0-84NSF = 4-88p < 0-01
x2df -NS
15 158
x2 = 38-86df = 6p <0001
x2 = 3137df = 6p <0-001
x2 = 208-57df = 4p <00001
x2=df =NS
x2 =x2df =NS
x2=df =p
x2 =df=
3504
5-584
27-104
< 0-001
3-722
x2 = 1398df = 6p <0-05
x2 = 1461df = 6p < 0-05
x2 = 1419df = 6p <0-05
x2 = 1195df = 6p < 0-05
x2=df =NS
7-466
Protected by copyright.
on March 14, 2020 by guest.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.43.2.153 on 1 June 1989. D
ownloaded from

Confounding variables in pregnancy alcohol consumption
Whilst nearly 30% of women reported regularanalgesic use (paracetamol and/or salicylate), nosignificant associations between usage of analgesicsand alcohol intake or maternal, demographic andlifestyle factors were found.The remaining categories ofdrug usage provided us
with frequencies that were so small that we could notshow any significant associations between their usageand the numerous factors reported above.
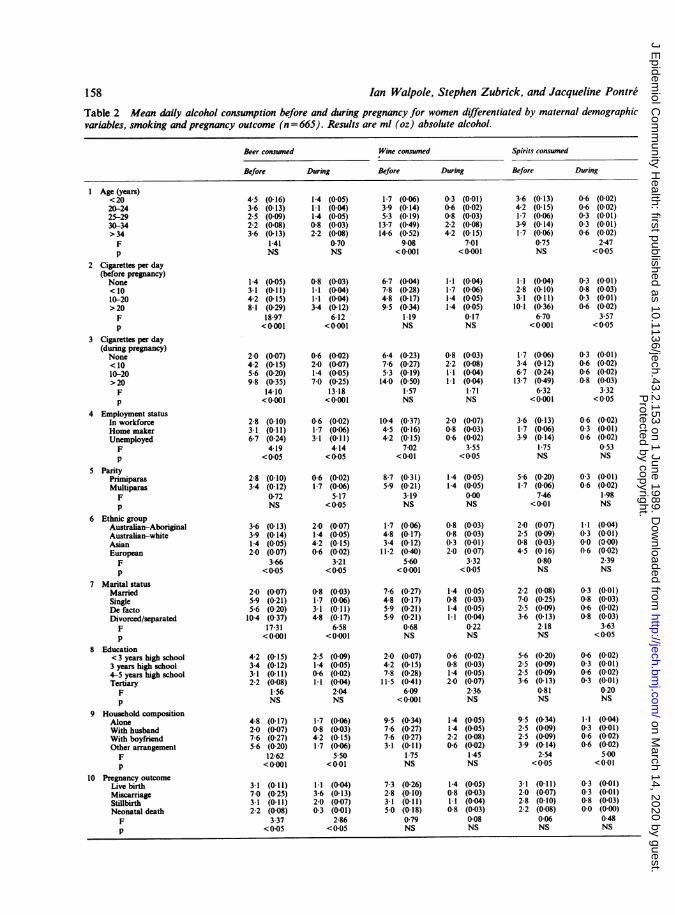
Beverages-Consumption of beer, wine and spiritswas studied as an independent factor. For eachbeverage mentioned above, ANOVAs were conductedon the mean absolute alcohol level for groupsdifferentiated by a variety of maternal, demographicand lifestyle characteristics. In this manner we couldstudy the covariation ofthe type of alcoholic beverageconsumed with a range of maternal and demographicvariables. Table 2 presents these data.
Beer was consumed more often by unemployedwhite Australian women either under the age of 25 or
over the age of 34. These women smoked more than 20cigarettes a day both before and during pregnancy,and were in de facto or divorced circumstances andliving with a boyfriend. Unlike wine or spiritsdrinkers, beer drinkers were less likely to reduce theirmean level of absolute alcohol consumption if theysmoked more than 20 cigarettes per day.Wine was consumed more often by women who
were characteristically over the age of 30, of Europeanbackground, who had had tertiary education, wereliving alone, and were in the workforce. There was no
significant difference in mean absolute alcohol levelwith level of smoking.Women who consumed spirits tended to live alone
and smoke more than 20 cigarettes a day, but were notdistinguished by other factors.The highest volumes of alcohol were consumed by
older women who drank wine, smoked more than 20cigarettes per day, had tertiary education and were ofEuropean background.
OUTCOMES INVOLVING STILLBIRTHS, SPONTANEOUSABORTIONS AND NEONATAL DEATHSSixty women (9%) had stillbirths, spontaneousabortions or neonatal deaths.We compared the 55 women who had spontaneous
abortions and stillbirths to those who had livebirths.There were no significant differences in their mean
age, height, weight, number of previous livebirths,educational level or ethnic group.Those women who had stillbirths or spontaneous
abortions had a significantly higher mean number ofpregnancies compared to women with livebirths(x = 2-7 vx = 2-2; t240 = -2 40, p < 0-01). They were
significantly more likely to be in single or de facto
relationships than women whose babies were bornalive (X2 = 18X4; df = 5, p<0-01).We studied the cigarette and alcohol use in both
groups of women for their reported consumptionbefore and during their pregnancy. There was nosignificant difference in mean cigarette and meanabsolute alcohol consumption before and duringpregnancy in women who had spontaneous abortionor stillbirths versus those with livebirths (t testcomparison). However, in terms of the pattern ofalcohol consumption, we showed in table 2 thatwomen who miscarried drank significantly highervolumes of beer (absolute alcohol intake frombeer= 7ml per day) than those with live births (3ml) orstillbirth (3ml).
Finally, of the six neonatal deaths, three were malesand three were females. Four of these deaths resultedfrom sequelae of extreme prematurity in infants bornat 20, 21, 23 and 26 weeks gestation. Of the remainingtwo deaths, one was due to a group B streptococcalinfection, and the other to hydranencephaly.
Discussion
Of the many epidemiological studies of the effects ofmaternal drinking on fetal outcome, most do notdescribe their population broadly or compare it withthe general population, so that selected cohorts may bebiased. The Seattle study of Streissguth et al43 iSperhaps an exception, being based on a "non-selected"hospital population (which nonetheless waspredominantly white, married and middle class). Itwas the aim of this present study to look at a cohortwhich was representative of the moderate socialdrinking group which comprises the majority of theobstetric population. The aim was achieved with theexception of slight overrepresentation of marriedmothers.
CHARACTERISTICS OF LIGHT, MODERATE AND HEAVYDRINKING WOMENDetailed analysis of the many possible confoundingfactors in the different alcohol groups is mandatory inattempting to assess a maternal alcohol effect on thefetus. These factors were considered in the studycohort in terms of maternal demographiccharacteristics, physical characteristics and nutrition,smoking and drug abuse, and type of beverageconsumed.
Demographic characteristics-Moderate and heavydrinkers in our sample were more likely to be single,divorced or separated than their lighter drinking peers.This finding is consistent with other studies which alsofound that alcohol abusing patients were more likelyto have been married in the past but less likely to bemarried during the index pregnancy.8 9 36
157
Protected by copyright.
on March 14, 2020 by guest.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.43.2.153 on 1 June 1989. D
ownloaded from
Ian Walpole, Stephen Zubrick, and Jacqueline Pontre
Table 2 Mean daily alcohol consumption before and during pregnancy for women differentiated by maternal demographicvariables, smoking and pregnancy outcome (n = 665). Results are ml (oz) absolute alcohol.
Beer consumed Wine consumed Spirits consumed
Before During Before During Before During
1 Age (years) ,,<2020-2425-2930-34>34Fp
2 Cigarettes per day(before pregnancy)None<1010-20>20Fp
3 Cigarettes per day(during pregnancy)None<1010-20>20Fp
4 Employment statusIn workforceHome makerUnemployedFp
5 ParityPrimiparasMultiparasFp
6 Ethnic groupAustralian-AboriginalAustralian-whiteAsianEuropeanFp
7 Marital statusMarriedSingleDe factoDivorced/separatedFp
8 Education< 3 years high school3 years high school4-5 years high schoolTertiaryFp
9 Household compositionAloneWith husbandWith boyfriendOther arrangementFp
10 Pregnancy outcomeLive birthMiscarriageStillbirthNeonatal deathFp
4-5 (0-16)3-6 (0-13)2-5 (0 09)2-2 (0-08)3-6 (0-13)
1-41NS
1-4 (0-05)3-1 (0-11)4-2 (0-15)8-1 (0-29)
18-97<0-001
2-0 (0-07)4-2 (0-15)5-6 (0-20)9-8 (0-35)
14-10<0-001
2-8 (0-10)3-1 (0-11)6-7 (0-24)
4-19< 0-05
2-8 (0- 10)3-4 (0-12)
0-72NS
3-6 (0-13)3-9 (0-14)1-4 (0-05)2-0 (0-07)
3-66< 0-05
2-0 (0-07)5-9 (0-21)5-6 (0-20)10-4 (0-37)
17-31<0-001
4-2 (0-15)3-4 (0-12)3-1 (0-1 1)2-2 (0-08)
1-56NS
4-8 (0-17)2-0 (0-07)7-6 (0-27)5-6 (0-20)
12-62<0-001
3-1 (0-11)7-0 (0-25)3-1 (0-11)2-2 (0-08)
3-37< 0-05
1-4 (0-05)1-1 (0 04)1-4 (0-05)0-8 (0-03)2-2 (0-08)
070NS
0-8 (0-03)1-1 (0-04)1-1 (0-04)3-4 (0-12)
6-12<0-00 1
0-6 (0-02)2-0 (0-07)1-4 (0-05)7-0 (0-25)
13-18<0-001
0-6 (0-02)1-7 (0-06)3-1 (0-1 1)
4-14< 0-05
0-6 (0-02)1-7 (0-06)
5-17<0-05
2-0 (0-07)1-4 (0-05)4-2 (0-15)0-6 (0-02)
3-21< 0-05
0-8 (0-03)1-7 (0-06)3-1 (0-11)4-8 (0-17)
6-58<0-001
2-5 (0-09)1-4 (0-05)0-6 (0-02)1-1 (0-04)
2-04NS
1-7 (0-06)0-8 (0-03)4-2 (0-15)1-7 (0-06)
5-50<0-0 1
1-1 (0-04)3-6 (0-13)2-0 (0-07)0-3 (0-01)
2-86<0-05
1-7 (0 06)3-9 (0-14)5-3 (0-19)
13-7 (0-49)14-6 (0-52)
9-08<0-001
6-7 (0-04)7-8 (0-28)4-8 (0-17)9-5 (0-34)
1-19NS
6-4 (0-23)7-6 (0-27)5-3 (0-19)
14-0 (0-50)1-57NS
10-4 (0-37)4-5 (0-16)4-2 (0-15)
7-02<0-01
8-7 (0-31)5-9 (0-21)
3-19NS
1-7 (0-06)4-8 (0-17)3-4 (0-12)
11-2 (0-40)5-60
<0-001
7-6 (0-27)4-8 (0-17)5-9 (0-21)5-9 (0-21)
0-68NS
2-0 (0-07)4-2 (0-15)7-8 (0-28)11-5 (0-41)
6-09<0-001
9-5 (0-34)7-6 (0-27)7-6 (0-27)3-1 (0-11)
1-75NS
7-3 (0-26)2-8 (0- 10)3-1 (0-11)5-0 (0-18)
0-79NS
0-3 (0-01)0-6 (0-02)0-8 (0-03)2-2 (0-08)4-2 (0 15)
7-01<0-001
3-6 (0-13)4-2 (0-15)1-7 (0-06)3-9 (0-14)1-7 (0-06)
0-75NS
1-1 (0-04) 1-1 (004)1-7 (0 06) 2-8 (0-10)1-4 (0 05) 3-1 (0- 1)1-4 (0-05) 10-1 (0-36)
017 6-70NS <00001
0-8 (0-03)2-2 (0-08)1-1 (0-04)1-1 (0-04)
1-71NS
2-0 (0-07)0-8 (0-03)0-6 (0-02)
3-55<0-05
1-4 (0-05)1-4 (0-05)
0-00NS
0-8 (0-03)0-8 (0-03)0-3 (0-01)2-0 (0-07)
3-32<0-05
1-4 (0-05)0-8 (0-03)1-4 (0-05)1-1 (0-04)
0-22NS
0-6 (0-02)0-8 (0-03)1-4 (0-05)2-0 (0-07)
2-36NS
1-4 (0-05)1-4 (0-05)2-2 (0-08)0-6 (0-02)
1-45NS
1-7 (0-06)3-4 (0-12)6-7 (0-24)
13-7 (0-49)6-32
<0-001
3-6 (0-13)1-7 (0-06)3-9 (0-14)
1-75NS
5-6 (0-20)1-7 (0-06)
7-46<0-01
2-0 (0-07)2-5 (0-09)0-8 (0-03)4-5 (0-16)
0-80NS
2-2 (0-08)7-0 (0-25)2-5 (0-09)3-6 (0-13)
2-18NS
5-6 (0-20)2-5 (0-09)2-5 (0-09)3-6 (0-13)
0-81NS
9-5 (0-34)2-5 (0-09)2-5 (0-09)3-9 (0-14)
2-54<0-05
1-4 (0-05) 3-1 (0-11)0-8 (0-03) 2-0 (0-07)1-1 (0-04) 2-8 (0-10)0-8 (0-03) 2-2 (0-08)
0-08 0-06NS NS
158
0-6 (0-02)0-6 (0-02)0-3 (0-01)0-3 (0-01)0-6 (0-02)
2-47< 0-05
0-3 (0-01)0-8 (0-03)0-3 (0-01)0-6 (0-02)
3.57<0-05
0-3 (0-01)0-6 (0-02)0-6 (0-02)0-8 (0-03)
3-32<0-05
0-6 (0-02)0-3 (0-01)0-6 (0-02)
0-53NS
0-3 (0-01)0-6 (0-02)
1-98NS
1-1 (0-04)0-3 (0-01)0-0 (0-00)0-6 (0-02)
2-39NS
0-3 (0-01)0-8 (0-03)0-6 (0-02)0-8 (0-03)
3-63<0-05
0-6 (0-02)0-3 (0-01)0-6 (0-02)0-3 (0-01)
0-20NS
II (0-04)0-3 (0-01)0-6 (0-02)0-6 (0-02)
5-00<0-01
0-3 (0-01)0-3 (0-01)0-8 (0-03)0-0 (0-00)
0-48NS
Protected by copyright.
on March 14, 2020 by guest.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.43.2.153 on 1 June 1989. D
ownloaded from

Confounding variables in pregnancy alcohol consumption
There was a significant trend for those individuals inthe regular workforce and with higher education alsoto be the heavier drinkers, which is contrary to thefindings of several other studies.8 2744 In a Frenchstudy of 18 275 pregnant mothers, those who drankmore than 400 ml of wine per day werecharacteristically of lower socio-economic status andnot in the work force.8 Conversely, in a British cohortof 1256 randomly selected pregnant women, it wasfound that those who drank most heavily were fromsocial classes I and II.28 Similarly in another Londonstudy, twice as many women in class I and 11 (28%)were relatively heavy drinkers as in classes III-V(14%).15 These differences probably reflect importantcultural and social characteristics which influencedrinking patterns within populations.
Physical characteristics and nutrition-In this studyconsiderable effort went to obtaining details of thematernal diet and its adequacy, and the generation ofthe folate intake score. It was therefore a veryimportant negative finding that, in general, diets werehighly satisfactory throughout the three alcoholgroups, and there was no significant difference inmean folate scores for these groups. Similarly, therewere no significant maternal weight differencesbetween the groups of mothers.
It is well known that maternal weight prior to andduring pregnancy is significantly related to fetaloutcome. Women who begin pregnancy with a weightwhich is equal to or less than 10% below the standardfor height are at greater risk for perinatal mortalityand, according to some studies, for intrauterinegrowth retardation.4546 Various studies have failed toshow a consistent correlation between maternalnutrition and subsequent psychomotordevelopment.47 Alcoholic malnutrition has beenassociated with maternal zinc deficiency, reported toproduce teratogenic effects and reduced birthweight.48 Furthermore, one study in mice hassuggested that zinc deficiency potentiates theteratogenic effect of alcohol.49 Poor nutrition in thealcoholic mother predisposes to higher blood alcohollevels. Weinberg has cautioned that in several animalstudies, lack of attention to nutritional status mayinvalidate the conclusions.32
Increased parity has been associated with heavieralcohol intake and increased risk of fetal alcoholsyndrome in a number of studies. Later born childrenof alcoholics are usually more seriously affected thantheir older siblings.36 No differences in parity wereobserved between the three alcohol groups in thisstudy.Smoking and drug abuse-That heavier drinkers
were significantly more likely to smoke is a findinguniformly consistent with all studies. Similarly, all
groups were significantly more likely to reduce theirsmoking during pregnancy.4 41 43
Both alcohol use and smoking have been shown tohave an effect on birth weight.6 8 9 15 Pregnant heavydrinkers are also more likely than other women to usemarihuana (42-9% versus 14%), sedatives,barbiturates, tranquillisers (13 9% versus 2%) andheroin (1 3% versus 0.4%).6 In one study alcoholicswere four times more likely to be narcotic usersalthough the percentage use among alcoholics wasrelatively low.
In our population, rates of drug taking, even ofprescribed medications (with the exception of theanalgesic and antinausea groups), were generally solow as to be of little statistical significance. In theanalgesic and antinausea groups there was nosignificant association with the alcohol intake groups.
STILLBIRTHS AND SPONTANEOUS ABORTIONSIn this study, the 55 women who had stillbirths orspontaneous abortions drank significantly higherquantities ofbeer, although their overall total absolutealcohol levels were not different from those withlivebirths. Moderate and heavy maternal drinkingbefore and during pregnancy has previously beenassociated with increased spontaneous abortionrates.9-ll A case-control study ofwomen who abortedspontaneously and women who delivered after at least28 weeks gestation showed that even moderateconsumption of alcohol during pregnancy is a riskfactor for spontaneous abortion."I However in thelight of our findings the reported differences inspontaneous abortion may not be due to beerconsumption but instead reflect other maternalcharacteristics or variables such as smoking.
BEVERAGEOf major interest in this study is the finding thatalcohol intake may well be better characterised byanalysis of the type of beverage consumed rather thansimple absolute alcohol intake. The heavy beer drinkerwas more likely to smoke more than one pack ofcigarettes a day than the wine drinker. Beer and winedrinkers were likely to be of different ethnic origins,marital status, and levels of education andemployment (and therefore social class). All thesefactors have important and different associations withalcohol related disease and fetal outcomes andtherefore the relative risks within beverage groupsmight be expected to be different.The above observation is important because there
have been previous reports, though scant, to suggestthat there are differences in perinatal outcomeaccording to preferred beverage. Kuzma et al,29 in astudy of 5093 maternal-infant pairs, showed that thefrequency of beer drinking, with wine drinking, spirits
159
Protected by copyright.
on March 14, 2020 by guest.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.43.2.153 on 1 June 1989. D
ownloaded from

160
drinking and other variables, contributedindependently to a reduction in intrauterine growth, asmeasured by birthweight adjusted for gestational age.The study also found that wine and spirits drinking,when considered separately, correlated positively withinfant birthweight, in contrast to the negativecorrelation found with beer drinking.A population based study of 952 Dundee
primigravidas indicated that, on analysis by beverage,mothers drinking beer heavily during the first 4months ofpregnancy had babies ofshorter gestationalage, lower Apgar scores at 5 minutes and reduced headcircumference. Consumption of wine and spirits didnot have the same adverse outcome. The authorsurged cautious interpretation of the results because ofthe small number ofmothers involved who were heavybeer drinkers.3'
In a French study of 9236 pregnancies followedthrough to delivery, birthweight was significantlyreduced and the proportion of small for gestationalage infants was significantly increased in a subgroupof 158 women who were heavy beer drinkers comparedto women who did not drink heavily. Heavy beerdrinkers also had an extremely high rate of stillbirths.8Kuzma et al 29 suggested that beer drinkers,
particularly those with chronic alcoholic problems,were more likely to have nutritional deficiencies (forexample of zinc) or to be subject to toxic componentsof beer. This study supports his hypothesis that beerdrinkers may have distinctly different demographic,socio-economic and/or medical/obstetric risks fromwomen who drink mainly spirits or wine.
CONCLUSIONSThis paper reports and comments on the methodologyused in a large prospective study of lifestyle variables(including alcohol intake) of a representative sampleof a population of pregnant women and details anumber of important characteristics related to level ofalcohol intake. The most important results were thatthere were consistent differences in lifestyle anddemographic variables for beer, wine and spiritsdrinkers and that beer drinking women had a poorerpregnancy outcome. A detailed assessment ofnutrition showed no significant differences betweenthe prepregnancy alcohol intake of the groups in thestudy. Our next step will be to analyse the birthoutcomes of this sample, allowing for these differencesto ensure unbiased interpretation.
We wish to acknowledge the work of Dr CarmenLawrence in providing this project with initialguidance and support. Our gratitude goes to Ms SallyMullighan who was instrumental in meticulouslygathering the data and assessing the infants. We wouldlike to thank the staff and administration of King
Ian Walpole, Stephen Zubrick, and Jacqueline Pontre
Edward Memorial Hospital for Women, Subiaco,Western Australia, for their full support. We thankDrs Robert Finlay-Jones, Alison Garton and FionaStanley for their valued comments.
This research was in part supported by grants fromTVW Telethon Foundation and the PrincessMargaret Hospital for Children Medical ResearchFoundation.
Correspondence to Dr Ian Walpole FRACP,Department of Paediatrics, Princess MargaretHospital for Children, Subiaco 6008, WesternAustralia.
References
I Hanson JW, Jones KL, Smith DW. Fetal alcoholsyndrome, experience with 41 patients. JAMA 1976; 235:1458-61.
2 Jones KL, Smith DW, Ulleland CN, Streissguth AP.Pattern ofmalformation in offspring ofchronic alcoholicmothers. Lancet 1973; i: 1267-71.
3Clarren SK, Smith DW. The fetal alcohol syndrome. NEngl J Med 1978; 298: 1063-7.
4 Ouelette EM, Rosett HL, Rosman NP, Weiner L. Adverseeffects on offspring of maternal alcohol abuse duringpregnancy. N Engi J Med 1977; 297: 528-30.
5Olegard R, Sabel KG, Aronson M, et al. Effects on thechild of alcohol abuse during pregnancy, retrospectiveand prospective studies. Acta Paediatr Scand Suppi 1979;279:- 112-21.
6 Little RE. Moderate alcohol use during pregnancy anddecreased infant birth weight. Am J Public Health 1977;67: 1154-6.
7 Streissguth AP. Fetal alcohol syndrome; anepidemiological perspective. Am J Epidemiol 1978; 107:467-78.
8Kaminski M, Rumeau C, Schwartz D. Alcoholconsumption in pregnant women and the outcome ofpregnancy. Alcoholism Clin Exp Res; 1978; 2: 155-63.
9Sokol RJ, Miller SI, Reed G. Alcohol abuse duringpregnancy: an epidemiologic study. Alcoholism Clin ExpRes 1980; 4: 135-45.
'0Harlap S, Shiono PH. Alcohol, smoking, and incidence ofspontaneous abortions in the first and second trimester.Lancet 1980; ii: 173-6.
1 Kline J, Shrout P, Stein Z, Susser M, Warburton D.Drinking during pregnancy and spontaneous abortion.Lancet 1980; i: 176-80.
2 Sokol RJ, Miller SI, Debanne S, et al. The ClevelandNIAAA prospective alcohol-in-pregnancy study: the firstyear. Neurobehav Toxicol Teratol 1981; 3: 203-9.
3 Kaminski M, Franc M, Lebouvier M, Du Mazaubrun C,Rumeau-Rouquette C. Moderate alcohol use andpregnancy outcome. Neurobehav Toxicol Teratol 1981; 3:173-81.
14 Davis PJM, Partridge JW, Storrs CN. Alcoholconsumption, pregnancy and low birthweight. Lancet1983; i: 664-5.
Wright JT, Waterson EJ, Barrison IG et al. Alcoholconsumption, pregnancy and low birth weight. Lancet1983; i: 663-5.
Hanson JW, Streissguth AP, Smith DW. The effects ofmoderate consumption during pregnancy on fetal growthand morphogenesis. J Pediatr 1978; 92: 457-60.
Protected by copyright.
on March 14, 2020 by guest.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.43.2.153 on 1 June 1989. D
ownloaded from

Confounding variables in pregnancy alcohol consumption17 Landesman-Dwyer S, Keller LS, Streissguth AP.
Naturalistic observations of newborns: effects ofmaternal alcohol intake. Alcoholism Clin Exp Res 1978; 2:171-7.
18 Kolata GB. Fetal alcohol advisory debate. Science 1981;214: 642-4.
19 Leading Article. Fetal alcohol syndrome. PublicAwareness Week Morbidity & Mortality Weekly Report1984; 33: 1.
20 US Surgeon General. Surgeon Generals advisory onalcohol and pregnancy. FDA Drug Bull 1981; 11: 9-10.
21 Royal College of Psychiatrists. Alcohol and alcoholism.Bull R Coll Psychiatr 1982; 6: 69.
22Leading Article. Alcohol and advice to the pregnant23 women. Br Med J 1983; 286: 247-8.
Annotation. Alcohol and the fetus. Arch Dis Child 1984;59: 1113-4.
24 Royal Australian College of Physicians. The positionpaper on alcohol abuse for the fellows of the College andcolleagues throughout the medical profession. Mod MedAust 1983; 26: 39-40.
2sMau G. Moderate alcohol consumption during pregnancyand child development. Eur J Pediatr 1980; 133: 233-7.
26 Hingson R, Alpert JJ, Day N, et al. Effects of maternaldrinking and marijuana use on fetal growth anddevelopment. Pediatrics 1982; 70: 539-46.
27Tennes K, Blackard C. Maternal alcohol consumption,birthweight and minor physical anomalies. Am J ObstetGynecol 1980; 138: 774-80.
28Grisso JA, Roman E, Inskip H, Beral V, Donovan J.Alcohol consumption and outcome of pregnancy. JEpidemiol Community Health 1984; 38: 232-5.
29Kuzma JW, Sokol RJ. Maternal drinking behaviour anddecreased intrauterine growth. Alcoholism Clin Exp Res1982; 6: 396-402.
30 Mills JL, Graubard BI. Is moderate drinking duringpregnancy associated with an increased risk formalformations? Pediatrics 1987; 80: 309-14.
3 Sulaiman ND, Florey CduV, Taylor DJ, Ogston SA.Alcohol consumption in Dundee primigravidas and itseffects on outcome of pregnancy. Br Med J 1988; 296:1500-3.
32 Weinberg J. Nutritional issues in perinatal alcoholesposure. Neurobehav Toxicol Teratol 1984; 6: 261-9.
33Sulik KK, Johnston MC, Webb MA. Fetal alcoholsyndrome: embryogenesis in a mouse model. Science1981; 214: 936-8.
3 Bartley HL, Coyle IR, Singer G. The effects of alcoholinduced malnutrition in pregnancy on offspring brain andbehavioural development. Pharmacol Biochem Behav1983; 19: 513-8.
3 Webster WS, Walsh DA, Lipson AH. Teratogenesis afteracute alcohol exposure in inbred and outbred mice.Neurobehav Toxicol Teratol 1980; 2: 227-34.
36 Abel EL. Fetal alcohol syndrome andfetal alcohol effects.New York: Plenum Press, 1984.
3 Drew LRH. Changes in Australian drinking patterns:1969-76. Australian Journal on Alcohol and DrugDependency 1977; 4: 78-80.
38Australian Bureau of Statistics Publication. Birth,Australia, Catalogue Number 3301.0, 1981.
39Jessor R, Graves RD, Hanson RC, Jessor SL. Societypersonality and deviant behaviour: A study of triethniccommunity. New York: Holt, Rinehart and Winston,1968.
40 Calahan D, Cisin I, Crossley H. American drinkingpractices: A natural study of drinking behaviour andattitudes. New Brunswick, NJ: Rutger Center of AlcoholStudies, 1969.
41 Little RE, Streissguth AP. Drinking during pregnancy inalcoholic women. Alcoholism Clin Exp Res 1980; 2:179-83.
42 Kutzberg D, Vaughan HG, Daum C, Grellong BA, AlbinS, Rotkin L. Neurobehavioural performance of low-birthweight infants at 40 weeks conceptional age:comparison with normal fullterm infants. Devel MedChild Neurol 1979; 21: 590-607.
43 Streissguth AP, Martin DC, Martin JC, Barr HM. TheSeattle longitudinal prospective study on alcohol andpregnancy. Neurobehav Toxicol Teratol 1981; 3: 223-33.
4Alpert JJ, Day N, Dooling E et al. Maternal alcoholconsumption and newborn assessment: methodology ofthe Boston City Hospital prospective study. NeurobehavToxicol Teratol 1981; 3: 195-202.
4 Edwards LE, Alton IR, Barrada MI, Hackanson EY.Pregnancy in the underweight woman: course, outcomeand growth patterns of the infant. Am J Obstet Gynecol1979; 135: 297-302.
46 Low JA, Galbraith RS, Muir D, Killen H, Karchmar J,Campbell D. Intrauterine growth retardation: apreliminary report of long term morbidity. Am J ObstetGynecol 1978; 130: 534.
47Naeye RL. Maternal nutrition and pregnancy outcome.In: Dobbing J, ed. Maternal nutrition inpregnancy, eatingfor two? (Nestle Nutrition Workshop. New York:Academic Press. 1981: 89-111.
48 Flynn A, Martier SS, Sokol RJ, Miller SI, Golden NL, DelVillano BC. Zinc status of pregnant women: adeterminant of fetal outcome. Lancet 1981; i: 572-4.
49 Keppen LD, Pysher T, Rennert OM. Zinc deficiency actsas a co-teratogen with alcohol in fetal alcohol syndrome.Pediatr Res 1985; 19: 944-7.
Acceptedfor publication December 1988
161
Protected by copyright.
on March 14, 2020 by guest.
http://jech.bmj.com
/J E
pidemiol C
omm
unity Health: first published as 10.1136/jech.43.2.153 on 1 June 1989. D
ownloaded from