preoperative assessment of coronary artery bypass graft patients
TRANSCRIPT

PREOPERATIVE ASSESSMENT
OF CABG PATIENTS
G.D.A. Samaranayaka
Purpose
• Evaluation of the patient’s current medical status
• Recommendations regarding the management and risk of cardiac problems during the perioperative period
• Provide a clinical risk profile to assist with treatment decisions, that affect short and long term outcomes
• Quick reference for decision making
• Lower the risk of surgery

Pre operative assessment
Risk Stratification

PREOPERATIVE ASSESSMENT

Assessment
• History
• Examination
• Investigations
• Cardiovascular, Respiratory, Renal, GIT, CNS,
Endocrine

Cardiovascular
History
• Angina (stable or unstable)
• Dyspnoea (systolic or diastolic dysfunction)
• Recent myocardial infarction (has it occurred since the decision to operate)
• Episodes of cardiac failure
• Flash pulmonary oedema.
Examination
• SOB, Ankle oedema, Pulse, BP, JVP, Murmurs

Cardiovascular
Investigations
• CXR – Cardiomegaly, Effusions, PHT
• ECG
• Regular ECG – “Basis for comparison” Territory of infarcts, Recent infarctions, conduction abnormalities
• Stress ECG – Ischemic threshold
• 2D echo – LV function, areas of hypo/akinesia, evidence of PHT
• Coronary Angiogram – Number site and severity of the disease sp LMCA or LMCA equivalent
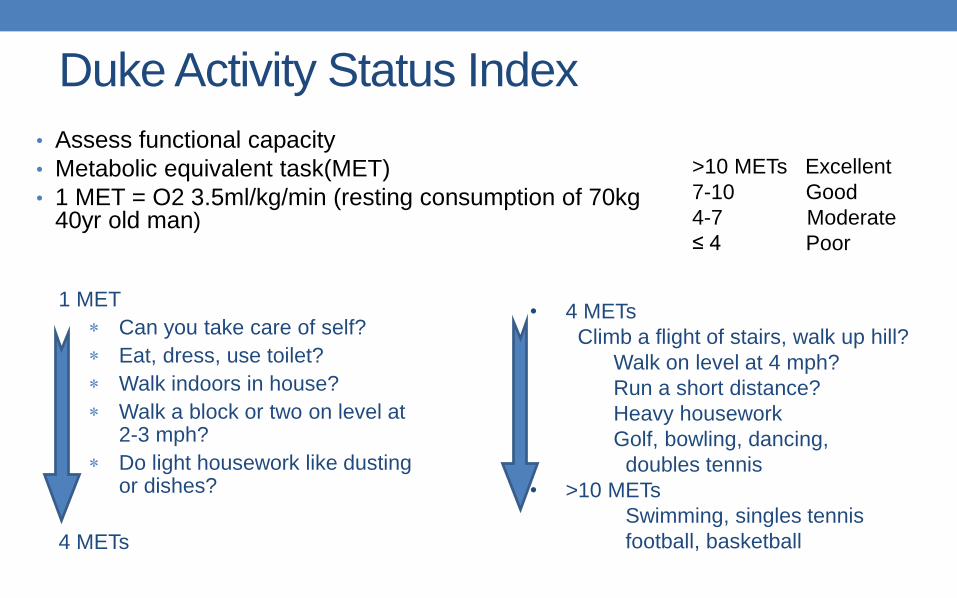
Duke Activity Status Index
• Assess functional capacity
• Metabolic equivalent task(MET)
• 1 MET = O2 3.5ml/kg/min (resting consumption of 70kg 40yr old man)
1 MET
Can you take care of self?
Eat, dress, use toilet?
Walk indoors in house?
Walk a block or two on level at 2-3 mph?
Do light housework like dusting or dishes?
4 METs
• 4 METs
Climb a flight of stairs, walk up hill?
Walk on level at 4 mph?
Run a short distance?
Heavy housework
Golf, bowling, dancing,
doubles tennis
• >10 METs
Swimming, singles tennis
football, basketball
>10 METs Excellent
7-10 Good
4-7 Moderate
≤ 4 Poor

Canadian Cardiovascular Society grading of
angina
• Class I – Angina only during strenuous or prolonged physical activity
• Class II – Slight limitation, with angina only during vigorous physical activity
• Ex: Walking or climbing stairs rapidly, Walking uphill, Walking or stair-climbing after meals, Emotional stress
• Class III – Symptoms with everyday living activities• Ex:- walking one or two level blocks and climbing one flight of stairs in normal
conditions and at a normal pace
• Class IV – Inability to perform any activity without angina or angina at rest
Classification of severity of
angina
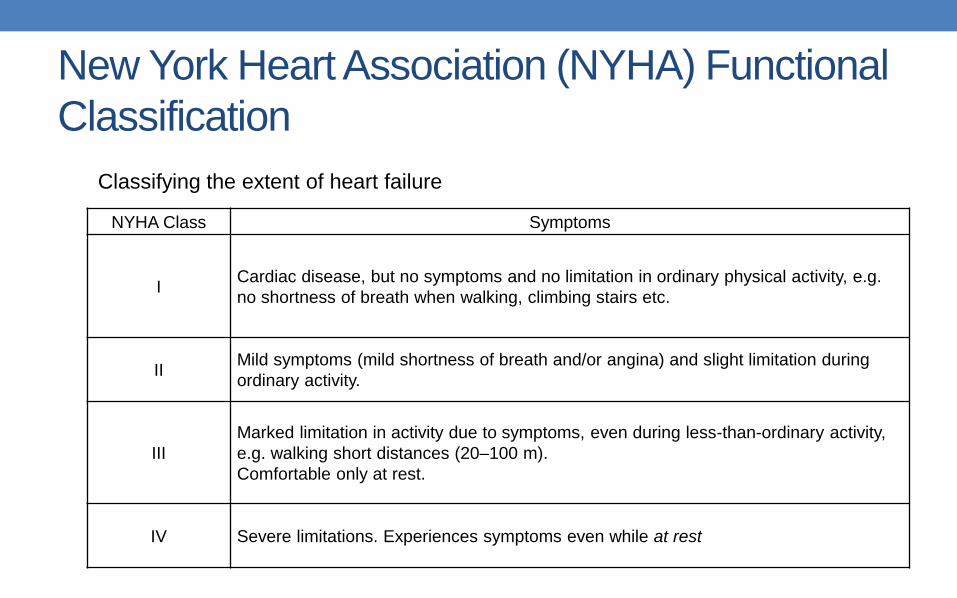
New York Heart Association (NYHA) Functional
Classification
NYHA Class Symptoms
ICardiac disease, but no symptoms and no limitation in ordinary physical activity, e.g.
no shortness of breath when walking, climbing stairs etc.
IIMild symptoms (mild shortness of breath and/or angina) and slight limitation during
ordinary activity.
III
Marked limitation in activity due to symptoms, even during less-than-ordinary activity,
e.g. walking short distances (20–100 m).
Comfortable only at rest.
IV Severe limitations. Experiences symptoms even while at rest
Classifying the extent of heart failure
Respiratory
History
• Recent RTI, Smoking, Bronchial asthma, COAD
Examination
• SOB at rest, Crepts, rhonchi
Investigations
• CXR
• ABG – Smokers, COAD
• Lung function test – Obstructive/restrictive lung diseases
Renal
History
• Uncontrolled or prolong history of DM & HT
• Renal toxic drugs
• Renal surgery
• Dialysis
Investigations
• BU, S Cr, estimated GFR, USS abdomen

Gastrointestinal system
• To reduce the risk of regurgitation and pulmonary aspiration
• GORD and Peptic ulcer disease
• Past hx of Hiatus hernia, oesophageal strictures, mediastinal irradiation -> TOE
Investigations
• Hepatic status – Liver enzymes, Clotting profile, Serum proteins

CNS
History
• CVA, syncopal attacks
• Peripheral or autonomic neuropathy
Examination
Residual weaknesses, sensory loss, carotid bruit
Investigations
Carotid dopplar, CT/MRI

Endocrine
Diabetes
• Duration, current treatment and control
• Microvascular Complications – Neuropathy, nephropathy and retinopathy
Thyroid
• Thyroid status, previous thyroid surgery
• Current treatment
• TSH/FT4

Others
• Allergies – Heparin, Seafood (Protamine)
• Current medications – Anti anginals, Anti hypertensives,
Anti arythmics, Hypoglycaemic agents, ect.
• Patient cooperation – For inserting lines
• Airway assessment

RISK STRATIFICATION

Risk stratification
• To assess the morbidity and mortality following the surgery
Postoperative morbidity
• Includes acute MI and reversible events such as congestive HF and need for inotropic support
• Prolongs ICU/hospital stay -> Financial Cost
Postoperative mortality
• Reported as either in-hospital or 30-day
• Cardiac or noncardiac
• If cardiac, may be ischemic or non ischemic.

Scoring systems• Several number of risk stratification scoring system
• Multiple variables
• Common Variables Associated with Increased Risk of Cardiac Surgery • Age
• Female gender
• Left ventricular function
• Body habitus
• Reoperation
• Type of surgery
• Urgency of surgery
• Commonly used systems - EuroSCORE II and Parsonnetscore

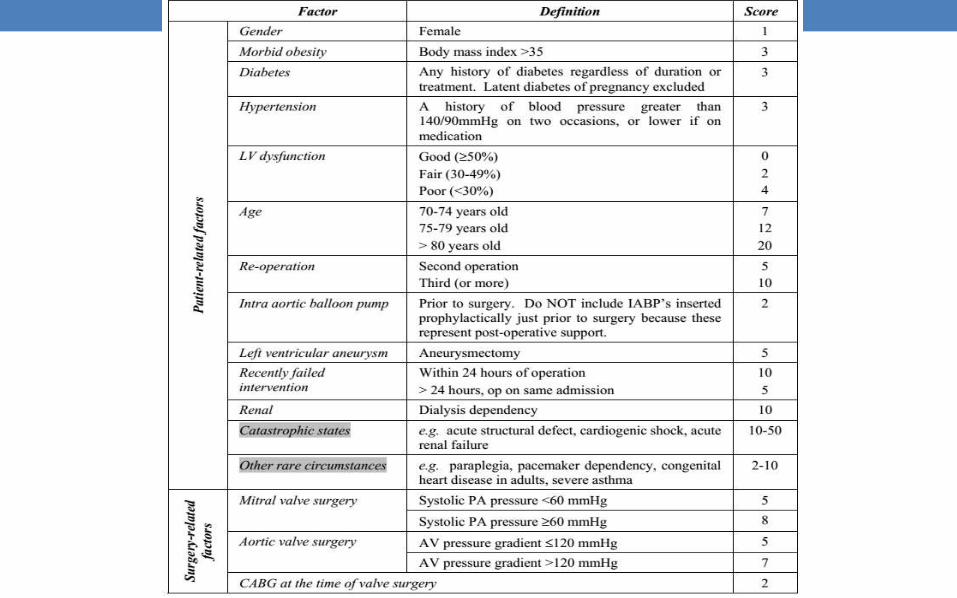
Parsonnet Score
• Developed by Victor Parsonnet and colleagues
• Additive system to calculate mortality rate
• Tendency to over predict surgical risks
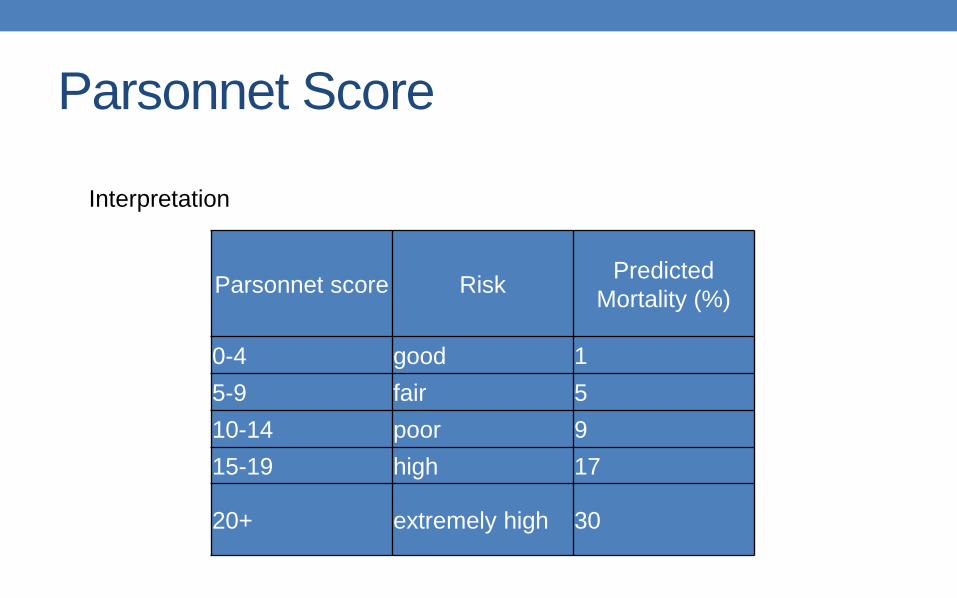
Parsonnet Score
Parsonnet score RiskPredicted
Mortality (%)
0-4 good 1
5-9 fair 5
10-14 poor 9
15-19 high 17
20+ extremely high 30
Interpretation

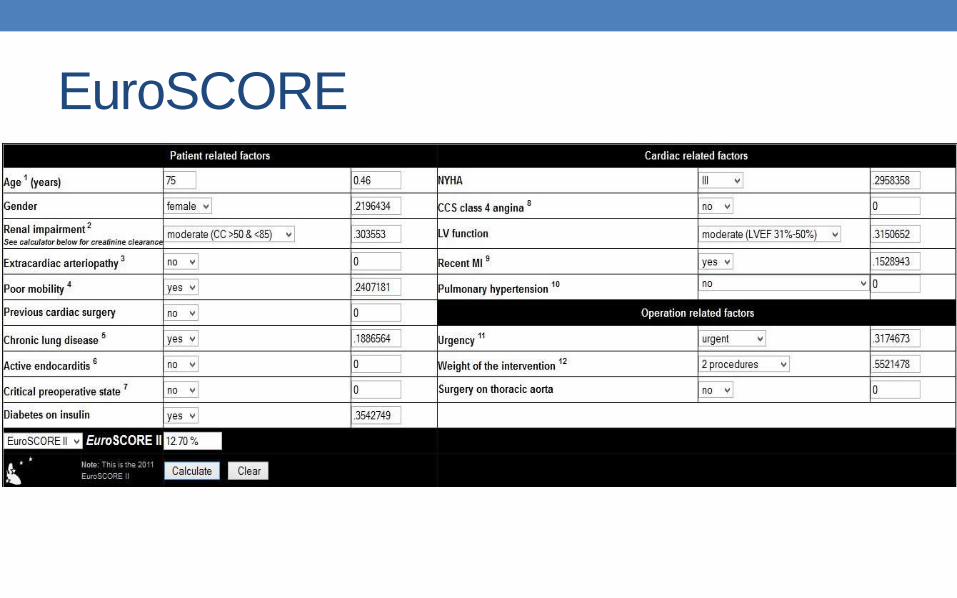
EuroSCORE
• European System for Cardiac Operative Risk
Evaluation

Patient-related factors Score
Age (per 5 years or part thereof over 60 years) 1
Sex female 1
Chronic pulmonary disease longterm use of bronchodilators or steroids for lung disease 1
Extracardiac arteriopathy any one or more of the following: claudication, carotid occlusion or >50% stenosis, previous or
planned intervention on the abdominal aorta,limb arteries or carotids
2
Neurological dysfunction disease severely affecting ambulation or day-to-day functioning 2
Previous cardiac surgery requiring opening of the pericardium 3
Serum creatinine >200m micromol/L preoperatively 2
Active endocarditis patient still under antibiotic treatment for endocarditis at the time of surgery 3
Critical preoperative state any one or more of the following: ventricular tachycardia or fibrillation or aborted sudden death,
preoperative cardiac massage, preoperative ventilation before arrival in the anaesthetic
room,preoperative inotropic support, intraaortic balloon counterpulsation or preoperative acute renal
failure (anuria or oliguria<10 ml/hour)
3
Cardiac-related factors Score
Unstable angina rest angina requiring iv nitrates until arrival in the anaesthetic room 2
LV dysfunction moderate or LVEF30-50% 1
poor or LVEF <30 3
Recent myocardial infarct (<90 days) 2
Pulmonary hypertension Systolic PA pressure>60 mmHg 2
Operation-related factors Score
Emergency carried out on referral before the beginning of the next working day 2
Other than isolated CABG major cardiac procedure other than or in addition to CABG 2
Surgery on thoracic aorta for disorder of ascending, arch or descending aorta 3
Postinfarct septal rupture 4
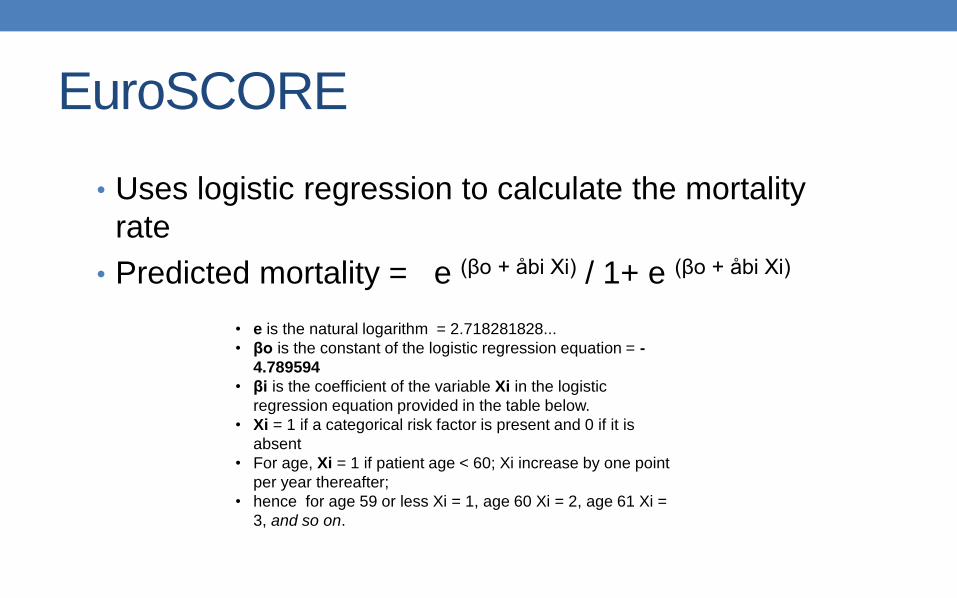
EuroSCORE
• Uses logistic regression to calculate the mortality
rate
• Predicted mortality = e (βo + åbi Xi) / 1+ e (βo + åbi Xi)
• e is the natural logarithm = 2.718281828...
• βo is the constant of the logistic regression equation = -
4.789594
• βi is the coefficient of the variable Xi in the logistic
regression equation provided in the table below.
• Xi = 1 if a categorical risk factor is present and 0 if it is
absent
• For age, Xi = 1 if patient age < 60; Xi increase by one point
per year thereafter;
• hence for age 59 or less Xi = 1, age 60 Xi = 2, age 61 Xi =
3, and so on.
EuroSCORE
THANK YOU