preparation for week 22 cardiology …emodules.med.utoronto.ca/ume/22/devcv.pdf · preparation for...
TRANSCRIPT
Foundations year 1, Faculty of Medicine, University of Toronto 1
PREPARATION FOR WEEK 22 CARDIOLOGY DEVELOPMENT OF THE CARDIOVASCULAR SYSTEM LEARNING OBJECTIVES By completing this pre-week preparation and further learning during the week, the learner should be able to: 1. Describe the formation and changing position of the primitive heart tube. 2. Describe the parts of the primitive heart tube and their contributions to the development of the
adult heart. 3. Describe the formation of the interatrial, interventricular, and aorticopulmonary septae. 4. Understand the contributions of sinus venosus and pulmonary veins in the development of the
atria. 5. Describe the flow of blood through the fetal heart. 6. Understand the changes in blood flow through the heart that take place in the newborn. INTRODUCTION The primordial heart and the vascular system appear in the 3rd week of embryonic development. By the early 4th week, the cardiovascular system begins to function and it is the first system of the embryo to become fully functional. This becomes necessary as simple diffusion of nutrients and oxygen from the surrounding milieu is not sufficient to meet the needs of the rapidly growing embryo. There is a need for an efficient method of acquiring oxygen and nutrients from maternal blood and distributing it to embryonic tissues and for disposal of wastes from embryonic blood.
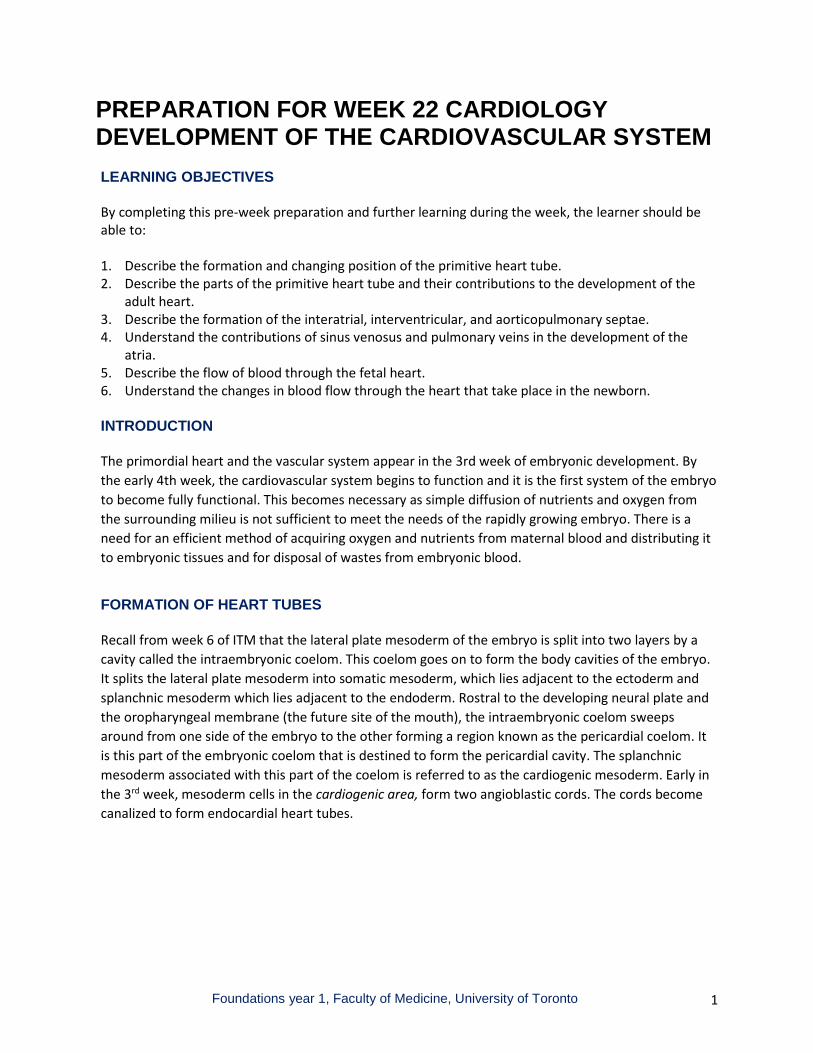
FORMATION OF HEART TUBES Recall from week 6 of ITM that the lateral plate mesoderm of the embryo is split into two layers by a cavity called the intraembryonic coelom. This coelom goes on to form the body cavities of the embryo. It splits the lateral plate mesoderm into somatic mesoderm, which lies adjacent to the ectoderm and splanchnic mesoderm which lies adjacent to the endoderm. Rostral to the developing neural plate and the oropharyngeal membrane (the future site of the mouth), the intraembryonic coelom sweeps around from one side of the embryo to the other forming a region known as the pericardial coelom. It is this part of the embryonic coelom that is destined to form the pericardial cavity. The splanchnic mesoderm associated with this part of the coelom is referred to as the cardiogenic mesoderm. Early in the 3rd week, mesoderm cells in the cardiogenic area, form two angioblastic cords. The cords become canalized to form endocardial heart tubes.
Foundations year 1, Faculty of Medicine, University of Toronto 2
A) Dorsal view of embryo showing the heart primordium developing in the cardiogenic area in relation to the position of the neural plate.
B) Transverse section taken through the cardiogenic area showing the angioblastic cords in the splanchnic mesoderm
C) Sagittal section showing an angioblastic cord in the splanchnic mesoderm ventral to the pericardial coelom.
When the angioblastic cords first appear, the pericardial coelom lies dorsal to the developing heart tubes. During the folding movements of the embryo, which are responsible for the formation of the primitive embryonic gut, the heart and pericardial coelom are brought ventral to the foregut part of the primitive gut tube with the heart now lying dorsal to the developing pericardial cavity.
Sagittal views of the change in position of the pericardial coelom and angioblastic cords as the embryo folds.
Late in the third week, the tubes approach each other and they become fused to form a single heart tube. As the heart tubes fuse, the endothelium of the tubes forms the endocardium of the heart and the surrounding splanchnic mesoderm becomes the primitive myocardium.

Foundations year 1, Faculty of Medicine, University of Toronto 3
Ventral views of the endothelial heart tubes as they fuse into a single tube.
FORMATION OF HEART LOOP
The tubular heart begins to elongate and push into the pericardial cavity, and a series of dilatations and constrictions appear along the length of the tube.
T - Truncus arteriosus: This is continuous cranially with developing arterial system. It will contribute to the aorta and pulmonary trunk.
B - Bulbus cordis: Located between truncus arteriosus and the primitive ventricle. It will contribute to the formation of the trabeculated part of the right ventricle and to the smooth parts of the right and left ventricles (the conus and vestibule).
PV - Primitive ventricle: Contributes to the formation of the trabeculated part of the left ventricle.
PA - Primitive atrium: The primitive atrium forms the trabeculated parts of the right and left atria (the auricular appendages). The connection between the primitive atrium and the primitive ventricle is known as the atrioventricular (AV) canal. This is where the atrioventricular valves will develop.
SV. - Sinus venosus (SV): Receives blood from veins and will contribute to the formation of the smooth part of the right atrium and to the coronary sinus.
By the time the single heart tube has formed, a primitive circulation begins, as peristaltic waves move blood through the tube from sinus venosus to truncus arteriosus.
The heart tube begins to elongate, but the bulboventricular portion grows faster than the rest of the heart causing the tube to begin to bend or loop within the confines of the pericardial cavity.
Foundations year 1, Faculty of Medicine, University of Toronto 4
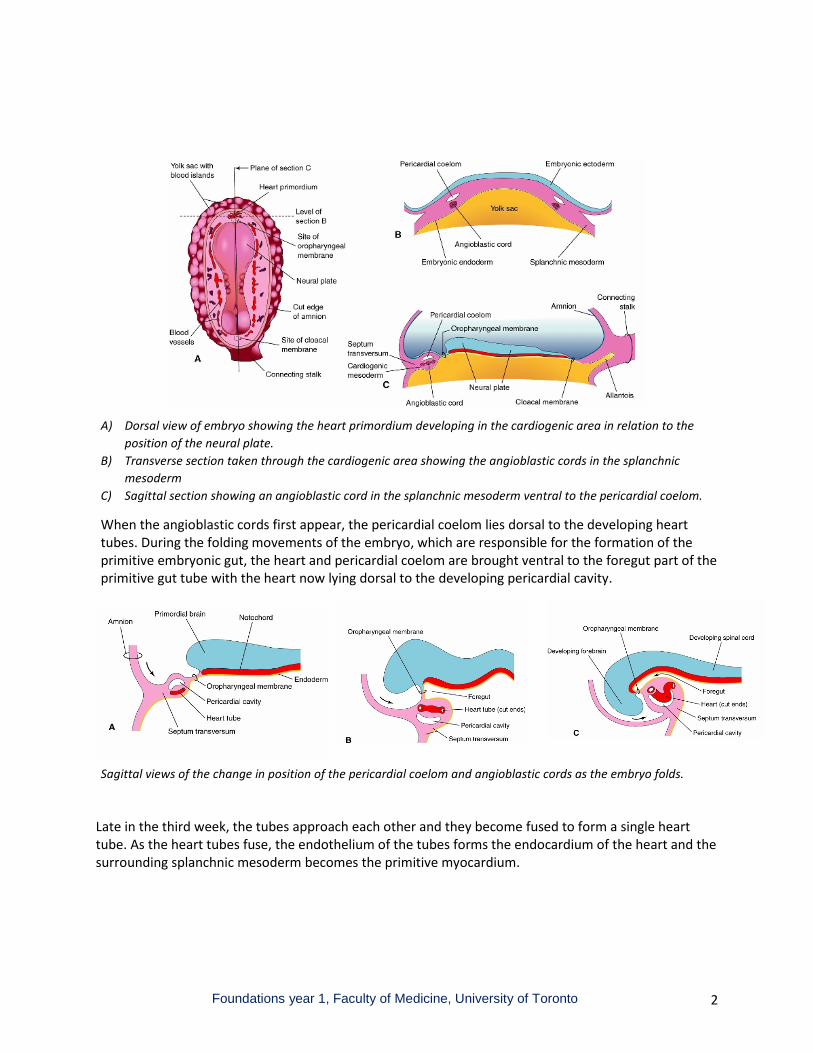
Lateral view of the heart tube as the heart loop develops, viewed from the left. The area of the pericardial coelom is indicated by the dotted line.
The bulboventricular portion bends in a ventral and caudal direction and slightly to the right. The atrium and sinus venosus shift in a dorsocranial direction and slightly to the left. The end result is that the primitive atrium and sinus venosus come to lie posterior to the developing ventricles.
Anterior views of the heart tube as looping begins (D), and nearing completion (E). Note that the primitive atrium and the sinus venosus now lie posterior to the developing ventricles. The trabeculated part of the right ventricle develops from the lower part of the bulbus cordis and the trabeculated part of the left ventricle develops from the primitive ventricle. The smooth walled parts of the right and left ventricles both develop from the upper part of the bulbus cordis.

Foundations year 1, Faculty of Medicine, University of Toronto 5
FORMATION OF THE ATRIA
The sinus venosus part of the heart tube receives two sinus horns, each of which receives venous blood from a vitelline vein (VIT), umbilical vein (UV), and common cardinal vein (CCV) formed by the union of anterior and posterior cardinal veins (ACV and PCV).
Posterior view of the sinus venosus at the site of the sinuatrial junction with the primitive atrium.
During the development of the atria, the opening of the sinus venosus shifts to the side of the developing right atrium. The shift is due in part to the regression of the tributaries of the left sinus horn and the development of the tributaries of the right sinus horn into the superior and inferior venae cavae.
Posterior views of the developing heart showing the incorporation of the sinus venosus and right sinus horn into the right atrium (light grey) and the fate of the left sinus horn as the coronary sinus (dark grey)

Foundations year 1, Faculty of Medicine, University of Toronto 6
As the right atrium expands, the sinus venosus and right sinus horn are incorporated into its wall as the smooth-walled part of the right atrium (the sinus venarum) and the remains of the primitive atrium then form the right auricular appendage. The remains of the left sinus horn becomes the coronary sinus. A number of pulmonary veins develop in association with the lung. They drain into a single common channel that opens into the left side of the primitive atrium. As the left atrium expands, the common pulmonary vein is incorporated into its wall as the smooth-walled portion of the left atrium. Tissue of the primitive embryonic atrium is reduced to the left auricular appendage. The branches of the common pulmonary vein then come to open independently into the left atrium as the pulmonary veins of the adult heart.
Anterior view into the developing left atrium to show how the common pulmonary vein is incorporated into the developing chamber with the result that its branches come to open independently into the atrium as the pulmonary veins of the adult heart.
FORMATION OF ATRIAL SEPTUM By the end of 4th week, projections of tissue called the endocardial cushions begin to appear on the dorsal and ventral walls of the atrioventricular canal. Eventually, these endocardial cushions will fuse with each other to form the atrioventricular septum, dividing the atrioventricular canal into right and left atrioventricular canals. The atrioventricular valves will develop at the site of these atrioventricular canals. In addition, a sickle shaped crest known as septum primum begins to grow from the roof of the primitive atrium towards these endocardial cushions. The transient opening between the septum primum and the endocardial cushions is known as the foramen primum.

Foundations year 1, Faculty of Medicine, University of Toronto 7
A. Sagittal view of the primitive atrium from the right side, showing the appearance of the endocardial cushions in the dorsal and ventral walls of the atrioventricular canal, and the beginnings of the septum primum from the dorsal atrial wall.
A1. Coronal view of the atrium showing the endocardial cushions beginning to divide the single atrioventricular canal into right and left atrioventricular canals.
As the septum primum continues to grow towards the endocardial cushions, perforations appear in the upper part of it. These perforations coalesce into an opening called the foramen secundum.
C. Sagittal view of the atrium from the right side showing the appearance of the foramen secundum in the septum primum.
C1. Coronal view of the atrium showing foramen primum and foramen secundum in the septum primum.
The septum primum begins to merge with the now fused-together endocardial cushions, thus obliteratiing the foramen primum. As this happens, a second septum (the septum secundum) begins to grow toward the endocardial cushions from the atrial wall, on the right atrial side of the septum primum.
Foundations year 1, Faculty of Medicine, University of Toronto 8
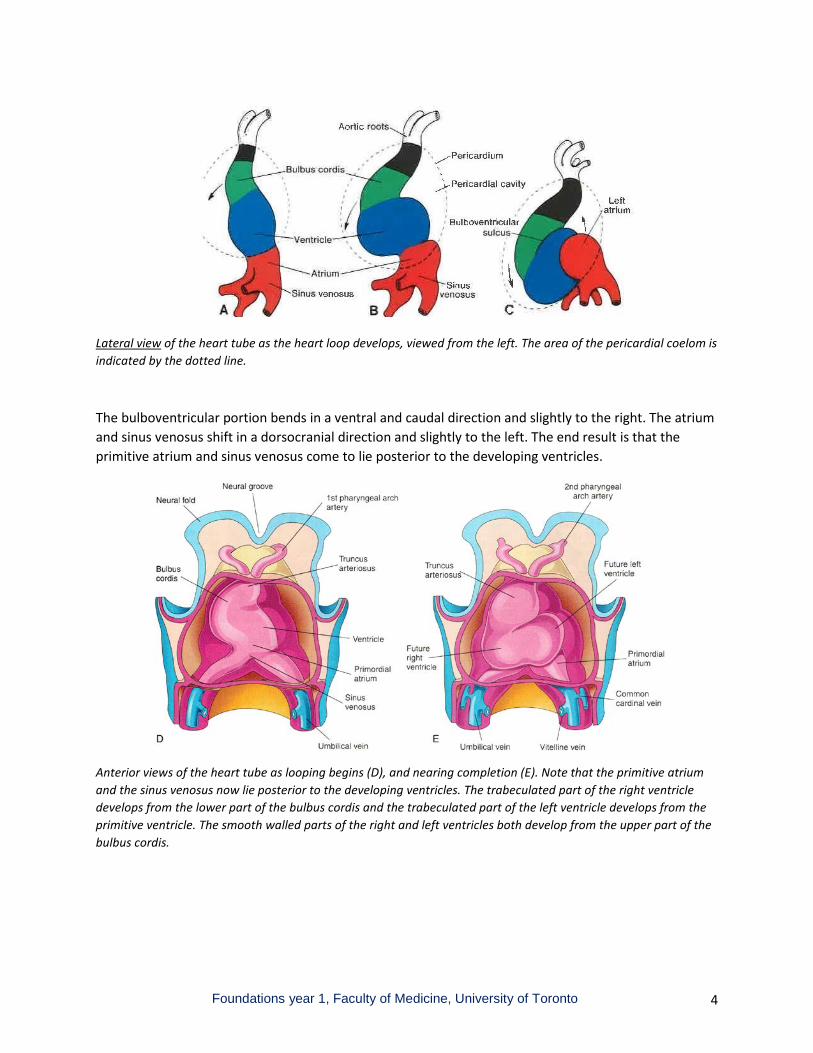
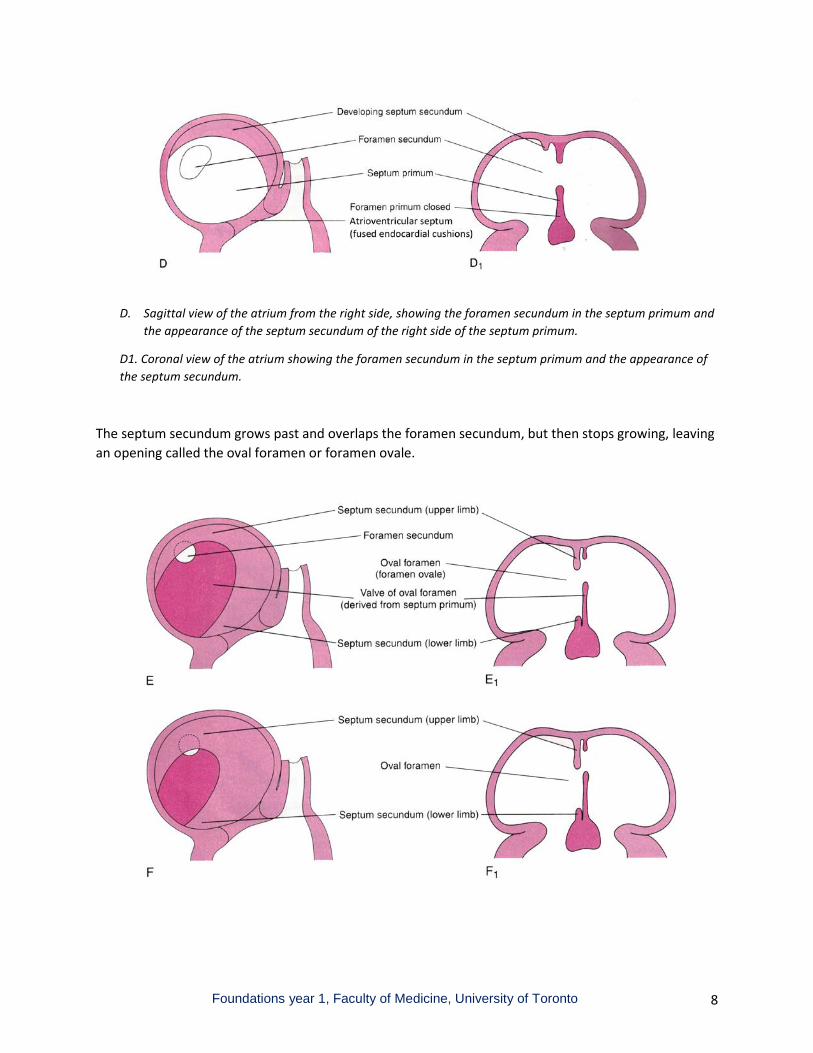
D. Sagittal view of the atrium from the right side, showing the foramen secundum in the septum primum and the appearance of the septum secundum of the right side of the septum primum.
D1. Coronal view of the atrium showing the foramen secundum in the septum primum and the appearance of the septum secundum.
The septum secundum grows past and overlaps the foramen secundum, but then stops growing, leaving an opening called the oval foramen or foramen ovale.

Foundations year 1, Faculty of Medicine, University of Toronto 9
The upper part of septum primum eventually disappears leaving the lower part to act as a valve on the oval foramen.
Before birth, because the lungs are not fully developed, vascular resistance is high in the pulmonary circulation. Consequently, blood pressure is higher on the right side of the heart than the left. As a result, blood entering the right atrium will push open the valve of the foramen ovale and enter directly into the left atrium. The oval foramen then acts a shunt for much of the blood entering the right atrium to pass directly into the left atrium, thereby bypassing the circulation to the lungs (which are not functional yet anyway).
After birth, as the lungs expand and pulmonary resistance falls, more blood passes to the lungs from the right side of the heart, and the pressure falls in the right atrium. With more blood flowing to the lungs, more blood is returned to the left atrium. The pressure in the left atrium then exceeds that in the right atrium and this forces the valve of the oval foramen (the septum primum) to close against the septum secundum. This results in functional separation of the right and left atria. Over time there is fusion between the margin of the oval foramen and the septum primum creating the depression on the right side of the interatrial septum that can be identified in the postnatal heart as the fossa ovalis. In some hearts complete fusion does not occur, but as long as the pressure in the left atrium exceeds that in the right, the valve will remain functionally closed. In such cases, in the dissection room, it is possible to slip the tip of a probe under the edge of the fossa ovale into the left atrium. This is referred to as a ‘probe patent foramen ovale’.
Foundations year 1, Faculty of Medicine, University of Toronto 10
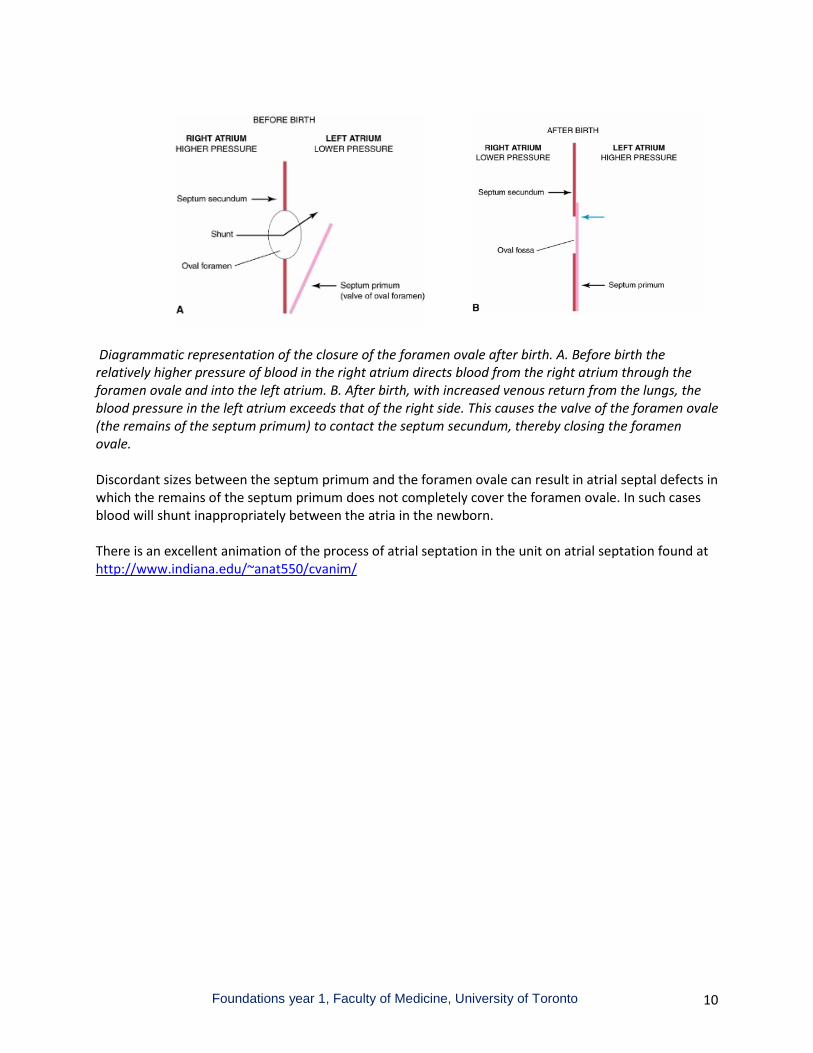
Diagrammatic representation of the closure of the foramen ovale after birth. A. Before birth the relatively higher pressure of blood in the right atrium directs blood from the right atrium through the foramen ovale and into the left atrium. B. After birth, with increased venous return from the lungs, the blood pressure in the left atrium exceeds that of the right side. This causes the valve of the foramen ovale (the remains of the septum primum) to contact the septum secundum, thereby closing the foramen ovale. Discordant sizes between the septum primum and the foramen ovale can result in atrial septal defects in which the remains of the septum primum does not completely cover the foramen ovale. In such cases blood will shunt inappropriately between the atria in the newborn. There is an excellent animation of the process of atrial septation in the unit on atrial septation found at http://www.indiana.edu/~anat550/cvanim/

Foundations year 1, Faculty of Medicine, University of Toronto 11
FORMATION OF INTERVENTRICULAR SEPTUM The atrioventricular canal initially connects the primitive atrium and primitive ventricle of the heart tube. Following the looping and rotation movements of the heart tube, the primitive atrium comes to lie posterior to the primitive ventricle and the bulbus cordis. Shifting of the opening of the atrioventricular canal to the right (indicated by the blue arrows in the following diagrams) then brings the primitive atrium into direct communication with both the primitive ventricle and the bulbus cordis.
A and B. Coronal sections through the heart loop showing the shift in the position of the atrioventricular (AV) canal, indicated by the blue arrow. The shift in the position of the AV canal brings the atrium into direct communication with both the primitive ventricle and the bulbus cordis. When the endocardial cushions merge with each other to form the atrioventricular septum, they divide the atrioventricular canal into a left AV canal connecting the developing left atrium with the primitive ventricle (destined to contribute to the trabeculated part of the left ventricle) and a right AV canal connecting the developing the right atrium with the inferior part of the bulbus cordis (destined to contribute to the trabeculated part of the right ventricle). Dilatation of the chambers in the developing right and left ventricles results in the appearance of a muscular interventricular septum between the two, which begins to extend toward the merged endocardial cushions. For a time, the two ventricles remain connected by a gap, called the interventricular foramen, which lies between the upper margin of the muscular ventricular septum and the atrioventricular septum (formed by the merger of the endocardial cushions). The interventricular

Foundations year 1, Faculty of Medicine, University of Toronto 12
foramen closes thus completing separation of the two ventricles as part of the process that creates the aorta and pulmonary trunk from the truncus arteriosus. SEPTUM FORMATION IN TRUNCUS ARTERIOSUS Separation of the truncus arteriosus into the aorta and pulmonary trunk is accomplished through the growth of ridges of tissue that develop on opposite sides of the truncus arteriosus. These conotruncal ridges, shown in yellow and green in the accompanying diagram, spiral through the trunus arteriosus and extend into the upper part of the remains of the bulbus cordis.

Foundations year 1, Faculty of Medicine, University of Toronto 13
The conotruncal ridges grow towards each other and fuse across the truncus arteriosus and the upper part of the bulbus cordis. The ridges divide the truncus arteriosus into the ascending aorta and the pulmonary trunk and they divide the upper part of the bulbus cordis into the non-trabeculated parts of the ventricles (the conus part of the right ventricle and the aortic vestibule of the left ventricle). The spiral course of the conotruncal ridges explains why the aorta and pulmonary trunk twist around each other as they leave the heart.
Faulty development or misalignment of the conotruncal ridges leads to inappropriate connections between the ventricles and their proper outflow vessels.
As the conotruncal ridges extend into the bulbus cordis, another extension of tissue from the atrioventricular septum (the fused endocardial cushions – shown in orange in the previous illustration) fuses with the ridges and with the upper part of the muscular interventricular septum to close the interventricular foramen and complete the separation of the ventricles. This tissue from the atrioventricular septum and conotruncal ridges that closes the interventricular foramen forms the membranous part of the interventricular septum in the adult heart. This is a common site for interventricular septal defects.
Growth of the conotruncal ridges depends on the proper development of a population of neural crest cells that migrate into the ridges from the cranial part of the neural tube. Recall from week 6 of ITM that cranial neural crest cells play a key role in the development of craniofacial structures. The role played by the cranial neural crest cells in the development of both the craniofacial skeleton and the heart is reflected in the frequent association between congenital craniofacial defects and heart malformations.
FETAL CIRCULATION
During fetal life, oxygen and nutrients from blood in the maternal circulation cross the placenta to enter the umbilical vein of the fetus. The umbilical vein connects with the fetal inferior vena cava which enters the right atrium. Since there is relatively little blood flow to the lungs of the fetus, pressure on the right side of the fetal heart is higher than the left. As a result, much of the blood entering the right atrium passes through the foramen ovale and enters directly into the left atrium. The blood which does pass from the right atrium to the right ventricle flows into the pulmonary trunk. The branches of the pulmonary trunk are comparatively small in the fetus and so most of this blood passes directly to the aorta via the ductus arteriosus a fetal vessel which connects the pulmonary artery with the arch of the aorta. Thus, during fetal life, there are 2 vascular shunts (the foramen ovale and the ductus arteriosus) that bypass the lungs and which direct most of the blood entering the right atrium into the systemic circulation rather than to the lungs.

Foundations year 1, Faculty of Medicine, University of Toronto 14
Schematic representation of the circulation through the fetal heart. The oval foramen allows much of the blood entering the right atrium to flow directly into the left atrium. Of the blood that does reach the right ventricle, most will be directed by the ductus arteriosus from the pulmonary trunk into the aorta. Only a relatively small amount will reach the lungs.
NEONATAL CIRCULATION
At birth, oxygen is no longer available through the placenta; the lungs begin to fill with air and expand; and the vascular resistance in the pulmonary circulation begins to drop and more blood from the right ventricle reaches the lungs. In addition, the ductus arteriosus begins to constrict (eventually forming the ligamentum arteriosum of the adult heart) and as a result, the blood entering into the ductus arteriosus is diverted to the lungs through the pulmonary arteries. With more blood now entering the lungs, more blood is returned to the left atrium. As the pressure in the left atrium rises, the valve of the foramen ovale closes against the interatrial septum, thereby completing the separation of the right and left atria.

Foundations year 1, Faculty of Medicine, University of Toronto 15
Schematic representation of the changes which take place in blood flow through the hearts after birth.
The animation of heart development by the late Dr. Robert Acland is an excellent summary of heart development.
SUMMARY OF HEART DEVELOPMENT
• The heart develops from the cardiogenic mesoderm, an area of splanchnic mesoderm that initially lies rostal to the neural plate of the week 3 embryo.
• A pair of primitive heart tubes develop in the cardiogenic mesoderm • During the folding movements of the embryo, which create the primitive gut, the heart tubes are
carried ventrally into the future thoracic region of the embryo where they fuse together into a single primitive heart tube.
• The heart tube lengthens and develops a series of expansions and shallow constrictions that divide the tube into primordial heart chambers: the sinus venosus, primitive atrium, primitive ventricle, bulbus cordis, and truncus arteriosus.
• As the heart tube lengthens it forms a looping structure, which bends to the right. The looping and turning movements establish the positions in which the atria and ventricles will develop from the chambers of the primitive heart tube.
• Between weeks 4 and 8 through a process of remodeling, realignment and septation the looping single lumen of the primitive heart tube is transformed into the 4 chambers of the definitive heart tube and the ventricles are aligned with the ascending aorta and pulmonary trunk.
• Formation and fusion of a pair of endocardial cushions at the connection of the primitive atrium with the primitive ventricle divides the single passage into right and left atrioventricular openings.
• The primitive atrium contributes to the formation of the right and left auricular appendages. The smooth walled part of the right atrium develops through incorporation of the sinus venosus into this chamber. The smooth walled part of the left atrium develops through incorporation of a common pulmonary vein. The branches of this vein then come to open independently into the left atrium as the pulmonary veins of the adult heart.
• A pair of septae, the septum primum and septum secundum grow to separate the right and left atria. Each of these septae has an opening in it (foramen secundum in the septum primum and foramen ovale in the septum secundum) that are staggered with respect to each other. The arrangement allows right to left shunting of blood during fetal life.
• The trabeculated parts of the ventricles develop from the primitive ventricle and the inferior part of the bulbus cordis. Initially the two ventricles are connected to each other by an interventricular foramen, which lies above the muscular part of the interventricular septum.
• A pair of spiraling ridges develops opposite each other extending though the truncus arteriosus and upper part of the bulbus cordis. These ridges fuse together dividing the truncus arteriosus into the ascending aorta and pulmonary trunk and dividing the upper part of the bulbus cordis into the conus and vestibule. Extensions for the ridges in the bulbus cordis, together with tissue from the endocardial cushions seals the interventricular foramen and forms the membranous part of the interventricular septum.

Foundations year 1, Faculty of Medicine, University of Toronto 16
REFERENCES
Moore, K.L and T.V.N. Persaud. The Developing Human. Clinically Oriented Embryology. 8th edition. Saunders Elsevier. 2008.
Sadler, T.W. Langman’s Medical Embryology. 10th edition. Lippincott Williams & Wilkins. 2006.
Carlson, B.M. Human Embryology and Developmental Biology. 5th edition. Elsevier Saunders. 2014.
Schoenwolf, G., S. Bleyl, P. Brauer and P. Francis-West. Larsen’s Human Embryology. Elsevier Churchill Livingston. 2009.
Developed by: Mike Wiley Last updated: January 23, 2017