preparing for the health future for filipino obstetrician-gynecologists jose y. cueto jr., md, mhped...
TRANSCRIPT

Preparing for the Health Preparing for the Health Future for Filipino Future for Filipino
Obstetrician-Obstetrician-Gynecologists Gynecologists
Jose Y. Cueto Jr., MD, MHPEdJose Y. Cueto Jr., MD, MHPEd
Member, Board of MedicineMember, Board of Medicine

Confluence of EventsConfluence of Events
PRC Planning Workshop (Feb. 10-11)PRC Planning Workshop (Feb. 10-11)
1. Medical manpower survey1. Medical manpower survey
2. Predicting medical manpower 2. Predicting medical manpower needs forneeds for
the next 10-15 yearsthe next 10-15 years

Confluence of EventsConfluence of Events
MRA Meeting in Thailand (Feb. 21-23)MRA Meeting in Thailand (Feb. 21-23)
1. Draft of core competencies1. Draft of core competencies
2. Template for data-gathering 2. Template for data-gathering (ASEAN)(ASEAN)

The Future?The Future?
Looking at the presentLooking at the present
Identifying the trendsIdentifying the trends
Predicting the possible developmentsPredicting the possible developments
Developing a planDeveloping a plan

Questions to AnswerQuestions to Answer
What are the key areas to consider in What are the key areas to consider in predicting the future?predicting the future?
What is the present situation now?What is the present situation now? Can we identify a “trend”?Can we identify a “trend”? What are the most possible future What are the most possible future
change or scenario?change or scenario? What do we need to improve on?What do we need to improve on?

I. Population Trends I. Population Trends (Bureau of Census, US Dept. of (Bureau of Census, US Dept. of
Commerce, 1996)Commerce, 1996)

Population TrendsPopulation Trends
YEARYEAR POPULATIONPOPULATIONGROWTH GROWTH RATE RATE PER YEARPER YEAR
19961996 73 MILLION73 MILLION 2.3%2.3%
20102010 99 MILLION99 MILLION 1.8%1.8%
20202020 113 MILLION113 MILLION 1.8%1.8%
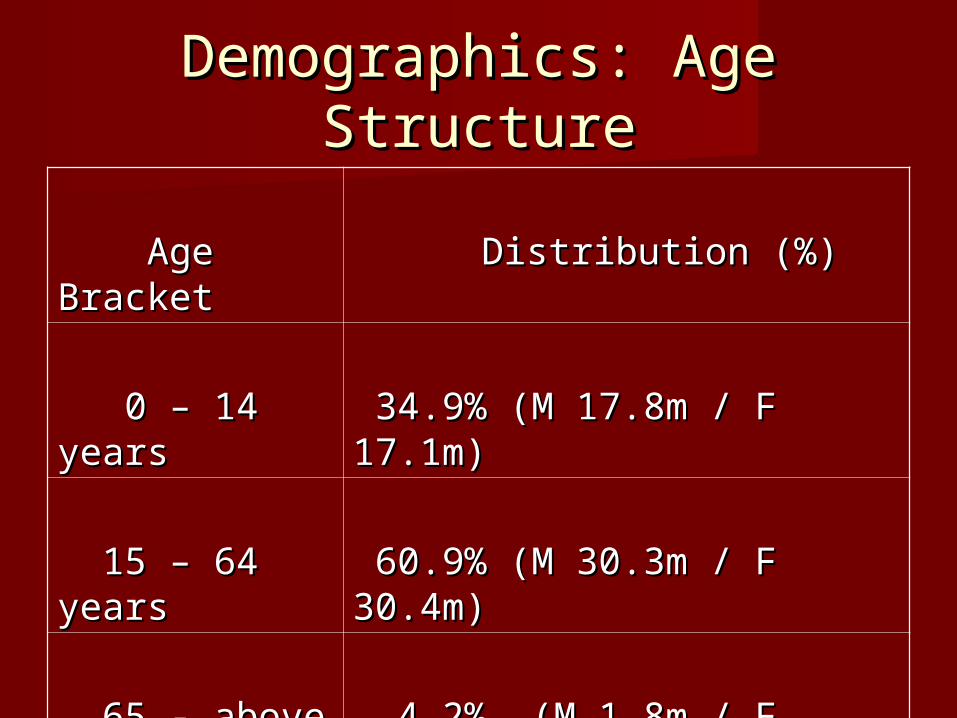
Demographics: Age Demographics: Age StructureStructure
Age BracketAge Bracket Distribution (%)Distribution (%)
0 – 14 years0 – 14 years 34.9% (M 17.8m / F 17.1m)34.9% (M 17.8m / F 17.1m)
15 – 64 years15 – 64 years 60.9% (M 30.3m / F 30.4m)60.9% (M 30.3m / F 30.4m)
65 - above65 - above 4.2% (M 1.8m / F 2.3m)4.2% (M 1.8m / F 2.3m)

DemographicsDemographics
Birth RateBirth Rate 25.68 per 1000 women25.68 per 1000 women
Fertility RateFertility Rate 3.23 children per 3.23 children per womanwoman
Death RateDeath Rate 5.06 deaths per 1000 5.06 deaths per 1000 citizenscitizens

Trend and ProjectionTrend and Projection
High growth rateHigh growth rate High fertility rateHigh fertility rate High number of childbearing ageHigh number of childbearing age High birth rateHigh birth rate
very busy OB practicevery busy OB practice

II. Health StatisticsII. Health Statistics
Infant Mortality Rate Infant Mortality Rate 29/100,000 live 29/100,000 live birthsbirths
Maternal Mortality RateMaternal Mortality Rate 138/100,000 live 138/100,000 live birthsbirths
% of birth attended by % of birth attended by health professionalhealth professional 65.3%65.3%
% of maternal deaths % of maternal deaths attended by health attended by health professionalprofessional
62%62%

Trend / What to doTrend / What to do
High IMRHigh IMR High MMRHigh MMR Wide discrepancy among regionsWide discrepancy among regions Many factors involvedMany factors involved
Analysis of root causesAnalysis of root causes
Failure of present Failure of present measuresmeasures

The FutureThe Future
Increase in population, increase in Increase in population, increase in number of poor citizensnumber of poor citizens
Budget for health may remain the Budget for health may remain the samesame
Deterioration in medical servicesDeterioration in medical services Increase in mortality ratesIncrease in mortality rates
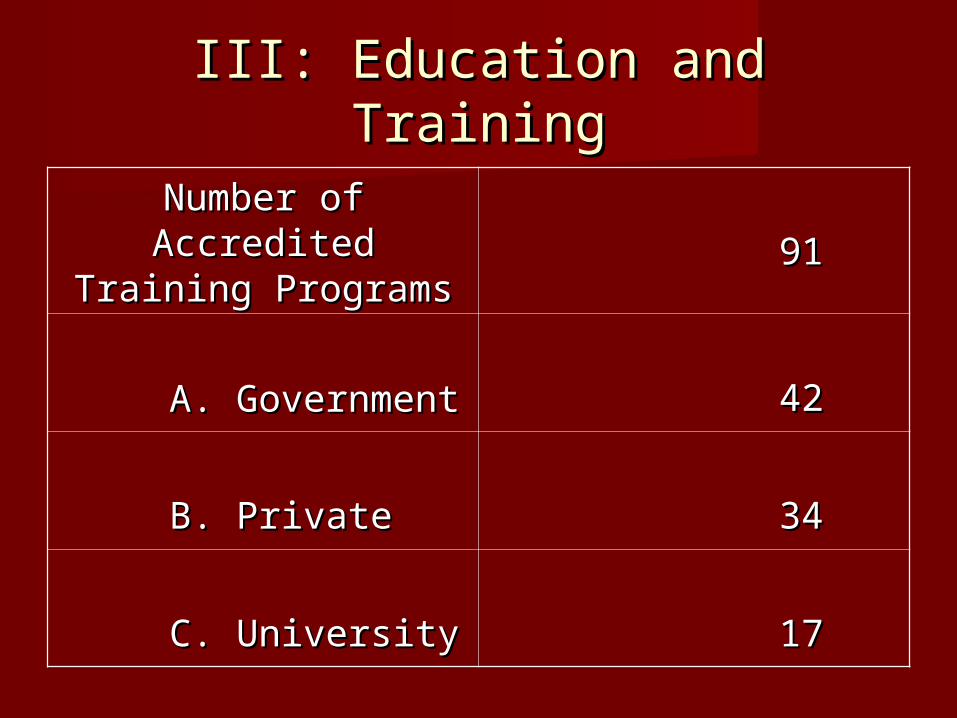
III: Education and TrainingIII: Education and Training
Number of Accredited Number of Accredited Training ProgramsTraining Programs 9191
A. GovernmentA. Government 4242
B. PrivateB. Private 3434
C. UniversityC. University 1717

Education and TrainingEducation and Training
Core CurriculumCore Curriculum Duration: 4 yearsDuration: 4 years Modular: 6 yearsModular: 6 years ConsortiumConsortium Accreditation RequirementsAccreditation Requirements Residents In-service ExaminationsResidents In-service Examinations Subspecialty TrainingSubspecialty Training
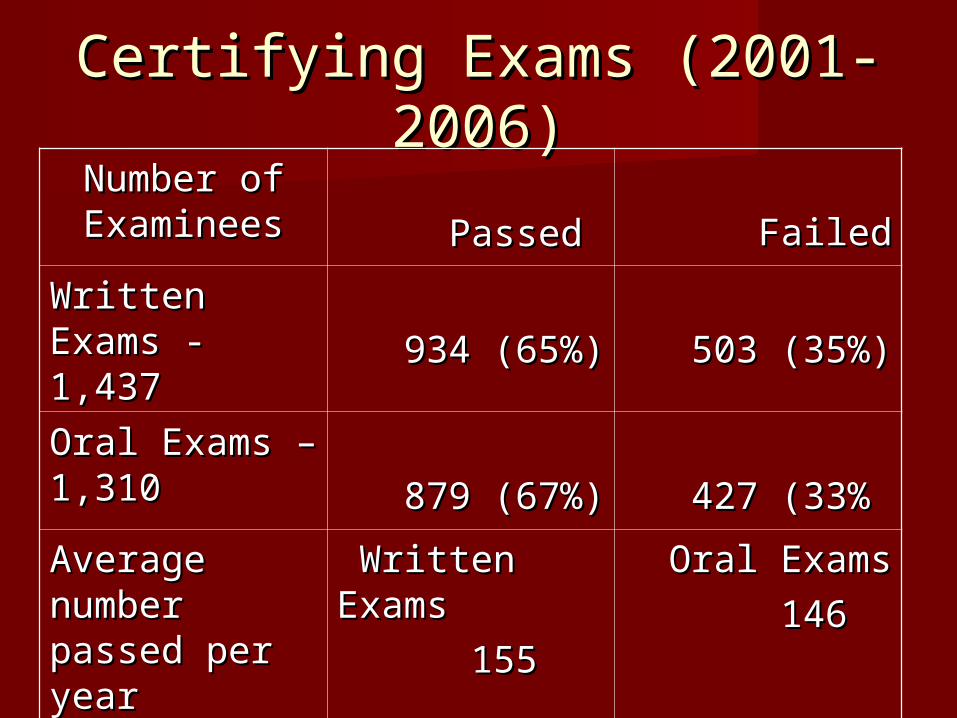
Certifying Exams (2001-Certifying Exams (2001-2006)2006)
Number of Number of ExamineesExaminees
PassedPassed FailedFailed
Written Written Exams - 1,437Exams - 1,437 934 (65%)934 (65%) 503 (35%)503 (35%)
Oral Exams – Oral Exams – 1,3101,310 879 (67%)879 (67%) 427 (33%427 (33%
Average Average number number passed per passed per yearyear
Written Written ExamsExams
155155
Oral ExamsOral Exams
146146

TrendTrend
Total No. of Residents: 878 per yearTotal No. of Residents: 878 per year
Ave. No. of examinees (WE): Ave. No. of examinees (WE): 239.5/year239.5/year
No. passed (WE): 155/yearNo. passed (WE): 155/year Backlog: 84.5 examineesBacklog: 84.5 examinees

TrendTrend
Ave. No. of examinees (OE): 218/yearAve. No. of examinees (OE): 218/year No. passed (OE): 146/year No. passed (OE): 146/year Backlog: 72.3 examineesBacklog: 72.3 examinees

Deeper StudyDeeper Study
What happened to those who failed?What happened to those who failed? Did they eventually pass the exams?Did they eventually pass the exams? Did they go into practice?Did they go into practice? Did they join another organization?Did they join another organization? Are they now classified as “GP with Are they now classified as “GP with
training” by Philhealth?training” by Philhealth?
IV: The Practice of OB-GYNIV: The Practice of OB-GYN
POGS Fellows: 2,029POGS Fellows: 2,029 Diplomates: 224Diplomates: 224
Distribution and place of practice: Distribution and place of practice: data not availabledata not available

Philhealth DataPhilhealth Data
• Data on CS claims from July 2008 to Data on CS claims from July 2008 to June 2009June 2009
• Performed by Fellows/diplomates: Performed by Fellows/diplomates: 59.86%59.86%
• GP’s with training, PAMS, DOH-GP’s with training, PAMS, DOH-certified: 29.5%certified: 29.5%
• MD’s with no training: 7.4%MD’s with no training: 7.4%

Profile Data NeededProfile Data Needed
1.1. Type of PracticeType of Practice SoloSolo Group, single specialtyGroup, single specialty Group, multi-specialtyGroup, multi-specialty SalariedSalaried Salaried / Private practiceSalaried / Private practice OthersOthers

ProfileProfile
2. Scope of Practice2. Scope of Practice General OB-GYNGeneral OB-GYN OB onlyOB only Gynecology onlyGynecology only PerinatologyPerinatology Infectious DiseaseInfectious Disease Gynecologic OncologyGynecologic Oncology Endocrine/InfertilityEndocrine/Infertility Uro-gynecologyUro-gynecology UltrasonographyUltrasonography
ProfileProfile
3. Setting or place3. Setting or place Metro areasMetro areas Non-metro areasNon-metro areas Area without diplomates and FellowsArea without diplomates and Fellows

ProfileProfile
4. Experience4. Experience Less than 5 yearsLess than 5 years 5-10 years5-10 years 11-20 years11-20 years More than 20 yearsMore than 20 years
QuestionsQuestions
At any given time, what is the At any given time, what is the predominant profile?predominant profile?
How do we make projections for the How do we make projections for the future?future?
How many training programs do we How many training programs do we need?need?
How many graduates do we need to How many graduates do we need to produce?produce?
QuestionsQuestions
How do we address maldistribution?How do we address maldistribution? What is our stand on those performing What is our stand on those performing
operations without credentials?operations without credentials? What do we recommend about the What do we recommend about the
GP’s with training? (products of GP’s with training? (products of accredited, non-accredited TP’s)accredited, non-accredited TP’s)
What will the picture be in 2020-2030?What will the picture be in 2020-2030?
V. Hospitals / Levels of CareV. Hospitals / Levels of Care
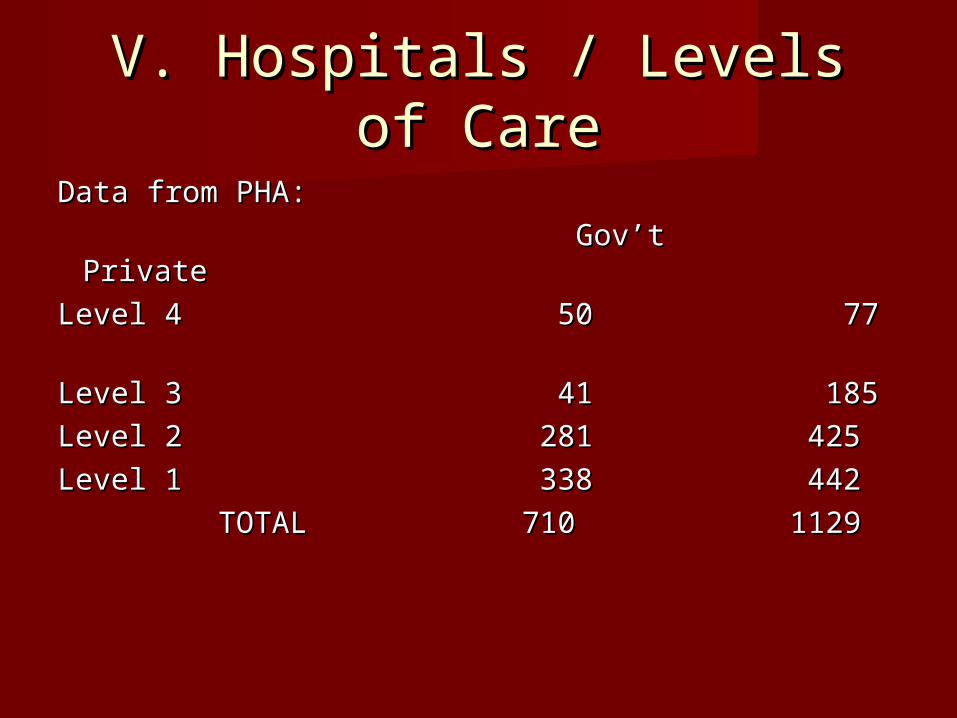
Data from PHA:Data from PHA:
Gov’t PrivateGov’t Private
Level 4 50 77 Level 4 50 77
Level 3 41 185Level 3 41 185
Level 2 281 425Level 2 281 425
Level 1 338 442Level 1 338 442
TOTAL 710 1129TOTAL 710 1129

Hospitals / Levels of CareHospitals / Levels of Care
Different needs (competence and Different needs (competence and expertise)expertise)
Different capabilities (equipment, Different capabilities (equipment, facilities)facilities)
Varying profiles of patientsVarying profiles of patients
Senate HearingSenate Hearing
President of PAMSPresident of PAMS Publicly complained against specialty Publicly complained against specialty
organizations which he described as organizations which he described as “elitist”“elitist”
Claimed that specialty exam questions Claimed that specialty exam questions are geared to practice in big medical are geared to practice in big medical centerscenters
Pointed out that diplomates and Fellows Pointed out that diplomates and Fellows could not be found practicing in could not be found practicing in provincial, district and local hospitalsprovincial, district and local hospitals

Training CurriculumTraining Curriculum
Primary care: 1Primary care: 1stst year year Secondary care: 2Secondary care: 2ndnd year year Tertiary care: 3Tertiary care: 3rdrd/4/4thth years years

Trend and QuestionsTrend and Questions
• Levels 3 and 4 constitute 29.4%Levels 3 and 4 constitute 29.4%• Majority belong to Levels 1 and 2Majority belong to Levels 1 and 2• How should training programs How should training programs
respond?respond?• Are there enough diplomates and Are there enough diplomates and
Fellows?Fellows?

ProblemProblem
Standards for accreditation of Standards for accreditation of programs and certification of programs and certification of graduatesgraduates
Rule being implemented: Rule being implemented:
only one standardonly one standard
only one examining board for only one examining board for specialtyspecialty
Need to respond to national needsNeed to respond to national needs

VI. The Regulatory BodyVI. The Regulatory Body
The Professional Regulation The Professional Regulation Commission-Board of MedicineCommission-Board of Medicine
RA 2382 as legal basisRA 2382 as legal basis Art. I. Sec. 1 “the supervision, Art. I. Sec. 1 “the supervision,
control and regulation of the control and regulation of the practice of medicine”practice of medicine”
Quasi-legislative and quasi-judicial Quasi-legislative and quasi-judicial functionsfunctions

Board of MedicineBoard of Medicine
Drafted resolutions:Drafted resolutions:
1. Practice of medicine1. Practice of medicine
2. Classification of physicians 2. Classification of physicians (GP/specialist)(GP/specialist)
3. Declaring residency training as practice 3. Declaring residency training as practice of medicineof medicine
4. Deputizing PMA to oversee residency 4. Deputizing PMA to oversee residency trainingtraining
5. Mediation of cases5. Mediation of cases

Philhealth WorkshopPhilhealth Workshop
Topic: Credentialing and PrivilegingTopic: Credentialing and Privileging BOM: GP and SpecialistBOM: GP and Specialist No “GP with training” classificationNo “GP with training” classification If cases are filed in regular courts or PRC, If cases are filed in regular courts or PRC,
the practitioner will only be classified as the practitioner will only be classified as GPGP
Solution: give 5 years to pass certifying Solution: give 5 years to pass certifying when practicing in Metro areaswhen practicing in Metro areas
In areas w/o diplomates and Fellows, give In areas w/o diplomates and Fellows, give incentives for them to practiceincentives for them to practice

Pending Bills amending RA Pending Bills amending RA 23822382
List of Sanctions List of Sanctions Art. V. Sec. 28 (k)Art. V. Sec. 28 (k) Performing….an area of medical Performing….an area of medical
specialization without fulfilling specialization without fulfilling specialization requirements specialization requirements prescribed by the IPMA and the prescribed by the IPMA and the BoardBoard

Control of Residency Control of Residency TrainingTraining
Three InstitutionsThree Institutions
1.1. PRC - PMAPRC - PMA
2.2. DOH - PMACDOH - PMAC
3.3. CHED - TPMECHED - TPME

The FutureThe Future
What would be the best arrangement What would be the best arrangement or relationship between medical or relationship between medical specialty organizations and the specialty organizations and the regulatory body?regulatory body?
What amendments should we What amendments should we recommend?recommend?

VII: Continuing Professional VII: Continuing Professional EducationEducation
In many countries, initial certification In many countries, initial certification after residency trainingafter residency training
After a period of time (7-10 years), After a period of time (7-10 years), require re-certification examsrequire re-certification exams
Traditional: attendance in conventionsTraditional: attendance in conventions Expensive, difficult to evaluateExpensive, difficult to evaluate Distance from place of practiceDistance from place of practice Sponsorship from drug companiesSponsorship from drug companies

CPECPE
Non-traditional Activities / Sources of DataNon-traditional Activities / Sources of Data 1. Practice evaluation1. Practice evaluation 2. Outcomes assessment2. Outcomes assessment 3. Self-assessment programs3. Self-assessment programs 4. Distance learning modules4. Distance learning modules 5. Submission of list of cases, procedures5. Submission of list of cases, procedures 6. CME Committee bulletins, advisories, 6. CME Committee bulletins, advisories,
updates, CPG’supdates, CPG’s 7. Feedback from PRC, PMA, Philhealth, 7. Feedback from PRC, PMA, Philhealth,
othersothers

PRCPRC
Longitudinal tracking of physiciansLongitudinal tracking of physicians Done every 3 years on renewal of Done every 3 years on renewal of
PRC ID’sPRC ID’s After licensureAfter licensure After residency trainingAfter residency training Additional trainingAdditional training

FutureFuture
With improvement of IT technology, With improvement of IT technology, there will be less need to gather all there will be less need to gather all members in large-scale conventionsmembers in large-scale conventions
What will be the most effective What will be the most effective method of disseminating new method of disseminating new knowledge / information?knowledge / information?
Or learning skills?Or learning skills?

VIII: The ASEAN Mutual VIII: The ASEAN Mutual Recognition Agreement (MRA)Recognition Agreement (MRA)
Exchange of professionalsExchange of professionals Licensed in home countryLicensed in home country Main problem: regulatory law limits Main problem: regulatory law limits
practice of medicine to Filipino practice of medicine to Filipino citizenscitizens
Exception: reciprocity arrangementException: reciprocity arrangement

Determining EquivalenceDetermining Equivalence
Data-gathering on:Data-gathering on:
1. MD degree program1. MD degree program
2. Residency training: curriculum2. Residency training: curriculum
competenciescompetencies
certificationcertification
3. Subspecialty training3. Subspecialty training
4. Competencies (GP, etc.)4. Competencies (GP, etc.)

MRAMRA
Main concern: competence, ability to Main concern: competence, ability to compete with graduates from other compete with graduates from other countriescountries
Communication skillsCommunication skills Regulatory laws and policiesRegulatory laws and policies CultureCulture Direction of transferDirection of transfer

FutureFuture
Completion of data from member Completion of data from member countriescountries
Implementing guidelinesImplementing guidelines Solving problems like legislationSolving problems like legislation Orientation and dissemination to Orientation and dissemination to
practicing physicianspracticing physicians Continuing communicationContinuing communication

IX: Scientific and Technological IX: Scientific and Technological DevelopmentsDevelopments
1. Genomics1. Genomics
2. Stem Cell2. Stem Cell
3. Vaccines 3. Vaccines
4. Drugs4. Drugs

Scientific and Technological Scientific and Technological DevelopmentsDevelopments
5. Advances in operative procedures (lap, 5. Advances in operative procedures (lap, robotics, etc.)robotics, etc.)
6. Imaging techniques6. Imaging techniques
7. Information technology7. Information technology
8. Changes in management (operative to 8. Changes in management (operative to non-operative) non-operative)

Scientific and Technological Scientific and Technological AdvancesAdvances
9. Tumor markers / screening methods9. Tumor markers / screening methods
10. Transplantation10. Transplantation

TrendTrend
Numerous advancesNumerous advances Different stages of developmentDifferent stages of development Offer cures or treatment for various Offer cures or treatment for various
disordersdisorders Definite impact on the training of Definite impact on the training of
physicians and on the practice of physicians and on the practice of medicinemedicine

ConclusionConclusion
1.1. There will be a lot of factors that There will be a lot of factors that will impact on the future of will impact on the future of Obstetrician-GynecologistsObstetrician-Gynecologists
2. The future is bright with the 2. The future is bright with the increase in number of potential increase in number of potential patients and the sustained interest patients and the sustained interest of medical graduates in the of medical graduates in the specialtyspecialty

ConclusionConclusion
3. Trends in education, training and 3. Trends in education, training and eventual practice in the specialty can eventual practice in the specialty can be identifiedbe identified
4. The impact of regulatory laws and 4. The impact of regulatory laws and international agreements should be international agreements should be studiedstudied
ConclusionConclusion
5. There are scientific and technological 5. There are scientific and technological advances that will become part of the advances that will become part of the practice of medicine. practice of medicine.
6. Our main problem as members of 6. Our main problem as members of academic, certifying and regulatory academic, certifying and regulatory bodies is to determine what to retain bodies is to determine what to retain and what to changeand what to change

ConclusionConclusion
7. There is a need to conduct 7. There is a need to conduct researches on various educational researches on various educational and practice-related topics and and practice-related topics and issuesissues
8. There is a need for a national 8. There is a need for a national comprehensive plan for developing comprehensive plan for developing the medical manpower of our countrythe medical manpower of our country

THANK YOU!THANK YOU!

GUIDELINES FOR GUIDELINES FOR CURRICULUM CURRICULUM PLANNING PLANNING
Jose Y. Cueto Jr., MD, MHPEdJose Y. Cueto Jr., MD, MHPEd
MemberMember
Board of MedicineBoard of Medicine

Overall Plan Overall Plan
CURRICULUMCURRICULUM INSTRUCTIONINSTRUCTION

Curriculum: Basic ElementsCurriculum: Basic Elements
Hilda Taba: “Curriculum Development: Hilda Taba: “Curriculum Development: Theory and Practice”Theory and Practice”
1. Objectives1. Objectives
2. Content2. Content
3. Teaching-learning activities3. Teaching-learning activities
4. Evaluation4. Evaluation

Planning a CurriculumPlanning a Curriculum
GOALGOAL
GENERAL/SPECIFIC OBJECTIVESGENERAL/SPECIFIC OBJECTIVES
COMPETENCIES OR ABILITIESCOMPETENCIES OR ABILITIES
CONTENT OR SUBJECT MATTERCONTENT OR SUBJECT MATTER

Planning a CurriculumPlanning a Curriculum
TEACHING-LEARNING ACTIVITIES TEACHING-LEARNING ACTIVITIES
ORGANIZATION OF ROTATIONS ORGANIZATION OF ROTATIONS
EVALUATION OF RESIDENTS EVALUATION OF RESIDENTS
RESOURCES RESOURCES
Planning a CurriculumPlanning a Curriculum
Instructional Design for Rotations Instructional Design for Rotations (Oncology, Infectious diseases, etc)(Oncology, Infectious diseases, etc)
1.1. ObjectivesObjectives
2.2. ContentContent
3.3. Teaching-learning activitiesTeaching-learning activities
4.4. ResourcesResources
5.5. EvaluationEvaluation

Planning a CurriculumPlanning a Curriculum
Evaluation of Program (by Evaluation of Program (by accrediting body)accrediting body)
Evaluation of Graduates (by Evaluation of Graduates (by certifying body)certifying body)

The GoalThe Goal
Sets the overall target for the whole Sets the overall target for the whole training programtraining program
May be worded “To train residents to May be worded “To train residents to assume the following roles….”assume the following roles….”

The General ObjectiveThe General Objective
What should be accomplished at the What should be accomplished at the end of the whole programend of the whole program
Emphasis on the role as clinician, in Emphasis on the role as clinician, in the diagnosis and management of the diagnosis and management of diseasesdiseases
The Specific ObjectivesThe Specific Objectives
The objectives at the end of each The objectives at the end of each year of trainingyear of training
Different domains: CognitiveDifferent domains: Cognitive
PsychomotorPsychomotor
AffectiveAffective

The CompetenciesThe Competencies
The abilities that should be acquired The abilities that should be acquired by the traineeby the trainee
The competencies include:The competencies include: CognitiveCognitive PsychomotorPsychomotor AffectiveAffective Interpersonal SkillsInterpersonal Skills Communication SkillsCommunication Skills

The ContentThe Content
This specifies all the subject matter This specifies all the subject matter that the trainee needs to learn in the that the trainee needs to learn in the different domains different domains
Cognitive, Psychomotor, AffectiveCognitive, Psychomotor, Affective

The Teaching-Learning The Teaching-Learning ActivitiesActivities
The wide range of learning The wide range of learning experiences of the trainees coupled experiences of the trainees coupled with the activities utilized by the with the activities utilized by the trainors to “teach, train, trainors to “teach, train, demonstrate”demonstrate”
Include actual patient management Include actual patient management in different settings, rounds, in different settings, rounds, presentations, discussions, presentations, discussions, conferencesconferences

Acquisition of Psychomotor Acquisition of Psychomotor SkillsSkills
Fitts and Posner (1976)Fitts and Posner (1976)
1.1. Cognitive PhaseCognitive Phase
2.2. Associative PhaseAssociative Phase
3.3. Autonomous or Fixation PhaseAutonomous or Fixation Phase

Psychomotor SkillsPsychomotor Skills
Documentation of progressionDocumentation of progression AssistsAssists Supervised operationsSupervised operations Operations independently Operations independently
performedperformed

OperationOperation 11stst AssistAssist
SupervisSuperviseded
IndependentIndependently performedly performed
1.Hysterecto1.Hysterectomymy
2. Cesarian 2. Cesarian sectionsection
3. Adnexal 3. Adnexal surgerysurgery

AdvantageAdvantage
Credentialing and privilegingCredentialing and privileging Complete documentationComplete documentation Use for determining hospital Use for determining hospital
privileges to be grantedprivileges to be granted Physician will only be allowed to Physician will only be allowed to
perform procedures based on what perform procedures based on what he was able to do during traininghe was able to do during training

The Organization of The Organization of RotationsRotations
Sequence and structure, durationSequence and structure, duration Covered by the Instructional Design Covered by the Instructional Design
for the particular rotationfor the particular rotation Short periods (1-4 months)Short periods (1-4 months)

The Evaluation of ResidentsThe Evaluation of Residents
The knowledge, skills and attitudes The knowledge, skills and attitudes acquired by the residents during acquired by the residents during rotations, at end of rotations, at the rotations, at end of rotations, at the end of the year, and at the end of the end of the year, and at the end of the training program need to be assessedtraining program need to be assessed
Utilize different methodsUtilize different methods Feedback should be given after the Feedback should be given after the
evaluationevaluation Internal and externalInternal and external
The ResourcesThe Resources
Sufficient number of trainorsSufficient number of trainors Adequate facilities, equipment, and Adequate facilities, equipment, and
clinical materialclinical material Support services Support services

Evaluation of ProgramEvaluation of Program
To assess the overall qualityTo assess the overall quality Different componentsDifferent components Conducted by appropriate bodyConducted by appropriate body Structured systemStructured system
Evaluation of GraduatesEvaluation of Graduates
For certificationFor certification Written, oral and practical examsWritten, oral and practical exams Feedback to institutionsFeedback to institutions
Instructional Design for Instructional Design for RotationRotation
DetailedDetailed Covers each rotationCovers each rotation Communicates what should be Communicates what should be
learned during the rotationlearned during the rotation

SummarySummary
The basic elements of a curriculum The basic elements of a curriculum were identifiedwere identified
For planning a residency training For planning a residency training curriculum, additional elements were curriculum, additional elements were incorporatedincorporated
The guidelines can be modified as The guidelines can be modified as the need arisesthe need arises
Ownership of the curriculum should Ownership of the curriculum should be developed to ensure its be developed to ensure its implementationimplementation
THANK YOU!THANK YOU!