prescribing outlook - welcome to ukmi national medicines ... · prescribing outlook new medicines...
TRANSCRIPT
Prescribing Outlook
New Medicines
September 2013
A resource for the NHS to help with budget setting,
prescribing planning and medicines management.

Contents
Foreword ..............................................................................................................................1
Abbreviations .......................................................................................................................3
Key ........................................................................................................................................4
Summary of predicted launch dates ..................................................................................5
Highlights .............................................................................................................................8
Table 1. Pipeline drugs ..................................................................................................... 11
BNF 1. Gastrointestinal system ................................................................................................................... 11
BNF 2. Cardiovascular system .................................................................................................................... 13
BNF 3. Respiratory system .......................................................................................................................... 18
BNF 4. Central nervous system ................................................................................................................... 20
BNF 5. Infections .......................................................................................................................................... 22
BNF 6. Endocrine system ............................................................................................................................ 26
BNF 7. Obstetrics, gynaecology, and urinary-tract disorders ...................................................................... 29
BNF 8. Malignant disease and immunosuppression ................................................................................... 30
BNF 9. Nutrition and blood ........................................................................................................................... 51
BNF 10. Musculoskeletal and joint diseases ............................................................................................... 53
BNF 11. Eye ................................................................................................................................................. 56
BNF 13. Skin ................................................................................................................................................ 57
BNF 14. Vaccines ........................................................................................................................................ 59
Table 2. Drugs in Prescribing Outlook 2012 - development delayed .......................... 60
Table 3. Recent UK drug launches or licence extensions ............................................ 61
BNF 1. Gastrointestinal system .................................................................................................................... 61
BNF 2. Cardiovascular system ..................................................................................................................... 61
BNF 3. Respiratory system ........................................................................................................................... 61
BNF 4. Central nervous system .................................................................................................................... 62
BNF 5. Infections ........................................................................................................................................... 62
BNF 6. Endocrine system ............................................................................................................................. 63
BNF 7. Obstetrics, gynaecology, and urinary-tract disorders ....................................................................... 63
BNF 8. Malignant disease and immunosuppression .................................................................................... 64
BNF 9. Nutrition and blood ............................................................................................................................ 66
BNF 10. Musculoskeletal and joint diseases ................................................................................................ 66
BNF 11. Eye .................................................................................................................................................. 66
BNF 12. Ear, nose and oropharynx .............................................................................................................. 67
BNF 13. Skin ................................................................................................................................................. 67
Patent expiries 2013 - 2015 ............................................................................................... 68
Biosimilar developments .................................................................................................. 69
Index ................................................................................................................................... 71
Acknowledgements ........................................................................................................... 73

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 1 No responsibility is accepted for the content of documents derived from this original publication.
Foreword
Managing new medicines
Underpinning the strategic direction for managing new
medicines is the Department of Health's report Innovation
Health and Wealth, Accelerating Adoption and Diffusion in
the NHS document (2011, updated 2012) . It sets out the
Government’s support for the NHS to embrace innovation
to meet current and future healthcare challenges and
outlines the importance of early adoption and diffusion of
clinically and cost effective innovative practices, including
medicines. Horizon scanning is essential at many
organisational levels so that new medicines that improve
patient outcomes can be planned for and adopted.
Since April 2013, NHS England Area Teams have a
strategic medicines management role and are responsible
for commissioning the majority of high cost drugs as well
as all cancer chemotherapy. The detail of the operational
mechanisms underpinning these responsibilities is yet to
be fully outlined although a number of interim
commissioning documents relevant to medicines have
been published including:
Individual funding requests (IFRs) – for when drugs are
not routinely commissioned.
Implementation and funding of NICE guidance
Experimental and unproven treatments
On-going treatment following a NHS England funded
trial
On-going treatment following non-commercially funded
clinical trials
On-going access to treatment following a trial of
treatment
On-going access to treatment following industry
sponsored clinical trials or funding
Specialised Services Commissioning Innovation Fund
(SSCIF)
The cancer drug fund (CDF), set up to facilitate patient
access to cancer treatments that fail to get NICE approval,
is being managed by NHS England until the end of 2013.
The most recent list of drugs funded by the CDF can be
accessed via the NHS England website. The intention is
that the CDF will cease as value based pricing (VBP) is
implemented in January 2014. Under VBP, different pricing
strategies will apply to different indications for drugs based
on the assessed ‘value’ for each indication. The
mechanism for VBP is still to be decided but NICE will have
a central role in the process and be responsible for the full
value assessment of medicines (see terms of reference).
There are already situations where the same medicine has
a different price for different indications. This is especially
true for medicines that have an orphan designation. In this
case, the medicine will have a different brand name for
non-orphan and orphan indications.
The majority of new medicines highlighted in this document
are due to be launched in 2014 or beyond. Their launch will
be affected by VBP reimbursement negotiations, but exactly
how is currently uncertain. For high cost new medicines
that are in the NICE work programme manufacturers have
the option to submit a proposal for a Patient Access
Schemes (PAS). This allows NICE to recommend
treatments that it might otherwise not have been found to be
cost effective. PAS are either cost (discounts, free stock
etc) or outcome (price variation linked to patient outcomes)
based. A list of NICE technologies with an approved PAS
can be viewed on the NICE website. In Prescribing Outlook
current PAS schemes are highlighted if they are relevant to
a new medicine in the same therapeutic area, and, although
this will not give an indication of the likely cost of the new
medicine, it suggests that subsequent treatment options will
have to be competitive.
The role of NICE is expanding to include support for
implementation of NICE guidance. Where relevant, links
are provided in Prescribing Outlook to NICE pathways,
commissioning guidance and quality standards. Quality
standards are designed to drive and measure quality
improvements within a particular area of care and be
reflected in commissioning frameworks. NICE
implementation tools for launched drugs include costing
templates and these may provide relevant information for
drugs yet to be launched. The NICE Medicines and
Prescribing Centre (MPC) has produced good practice
guidance on developing and updating local formularies in
response to Innovation Health and Wealth, Accelerating
Adoption and Diffusion in the NHS. It advises that local
systems and processes for accessing medicines support
innovation where appropriate and recommends horizon
scanning is included as a standing agenda item in local
formulary decision-making meetings.
It is estimated more than 70% of the secondary care drugs
bill can be accounted for by ‘high cost’ drugs excluded from
the Payment by Results (PbR) tariff, the national system for
paying trusts for activity. Standard tariff prices do not
always allow fair reimbursement of some interventions so a
list of drugs and services excluded from the tariff has been
developed. The majority of drugs appearing on this list
(previously known as ‘PbR exclusions’, now referred to as
‘Specified high cost drugs’) are likely to be commissioned
by NHS England via specialised commissioning systems
but the detail of exactly which drugs and how the funding
streams operate is awaited. The Manual outlining which
services (and treatments) are commissioned by NHS
England has been published but will be updated shortly.
As of April 2013 the Department of Health is no longer
responsible for managing PbR; Monitor has been charged
with this and is currently consulting on the future direction
of the Tariff. There are few changes for the 2013/14 PbR
tariff (see tab 19 for high cost drugs detailed list) but
payment mechanisms for high cost drugs in 2014/15 could
be influenced by the outcome of the consultation. In
previous editions of Prescribing Outlook an ‘educated
guess’ as to the potential tariff positioning of each new
medicine has been made. Current uncertainty now makes
this difficult. In the absence of additional guidance for
2014/15, estimates of tariff positioning in this document are
based on historical assumptions. An ‘educated guess’ is
also made on the likely commissioning route for individual

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 2 No responsibility is accepted for the content of documents derived from this original publication.
medicines to take into account new commissioning
arrangements outlined above.
For the pharmaceutical industry, the cost of bringing a new
drug to the market is high. It is inevitable that more effort is
being put into looking for new uses for, or new formulations
of, currently licensed products. Applications for licence
extensions are processed through licensing systems faster
than those for new drugs as less safety and technical data
are required. Data collection of pipeline licence extensions
and new formulations has also improved over recent years.
As a result an increased number of potential licence
extensions appear in this document. This year, to manage
this, there are two types of monograph; a full monograph
with all the information previously included and an
abbreviated entry (highlighted in blue) containing basic
information for those drugs with an anticipated launch date
in 2015 or beyond. This enables us to highlight drugs near
and slightly further away from launch in the same
therapeutic area.
As in previous editions of Prescribing Outlook, drugs with
patents due to expire in the near future are highlighted as
they are then open to generic competition. It is important
that the possibility of generic options is considered as part
of the wider medicines management agenda, hence their
inclusion in this document together with an ‘educated
guess’ as to which have the potential for generic
competition and an indication whether generic product
licence applications are currently in progress in the EU.
For the first time we have included a separate section on
biosimilar drugs. Although there are a small number of
biosimilar drugs already on the market there are many
more in the pipeline that could have a potentially cost
saving impact on medicines budgets. It is estimated about
50% of the current UK market for biological medicines
spend may be subject to biosimilar competition by 2019.1
There are a number of regulatory schemes that impact on
the availability of new medicines. Those that allow earlier
access to medicines in the EU and UK include ‘individual
patient supply’ and ‘conditional approval’. Where relevant,
and if known, details of these are included in this
document. Details of a scheme which would allow patients
access to new medicines prior to licensing were put out for
consultation by the Medicines and Healthcare products
Regulatory Agency (MHRA) in July 2012. The intention of
the scheme is to widen access to "promising new
medicines that will treat, diagnose or prevent life
threatening, chronic or seriously debilitating conditions
without adequate treatment options". The outcome of the
consultation is awaited.
1. Anon. What are biosimilars and are they important? Drug and
Therapeutics Bulletin 2013; 51(5): 57-60.
About Prescribing Outlook
The aim of the annually published Prescribing Outlook
series produced by UK Medicines Information (UKMi) is to
assist NHS organisations in planning, implementing and
budgeting for new medicines or licence extensions and
national guidance. It provides support to commissioners
and providers by highlighting new medicines and service
developments that may require dialogue about financial
and operational resource implications. The Prescribing
Outlook series is produced for primary and secondary care
NHS organisations and has a national perspective. This
document is the first in the series that comprises
Prescribing Outlook - New Medicines and Prescribing
Outlook - National Developments, and is supported by an
electronic Cost Calculator. These are all available at
www.ukmi.nhs.uk. The component documents of the
Prescribing Outlook series are published each autumn in
line with annual budget planning timeframes and key
outputs from NICE. Updates on the progress of individual
medicines at other times throughout the year can be found
on the UKMi New Drugs Online database.
The content and presentation of the Prescribing Outlook
series has evolved following consultation with users. These
documents they are all now only published electronically
but are formatted to make them suitable for printing.
Further specialist medicines information not included in the
series can also be obtained from local and regional
medicines information centres. See www.ukmi.nhs.uk.
Prescribing Outlook – New Medicines. It aims to provide
advance information about new medicines (and new
licensed indications or formulations) with anticipated
market launches in the next 18 to 24 months. In addition,
brief details of drugs launched in the last 12 months are
included as this is often useful for local planning purposes.
The content is not comprehensive but focuses on
medicines with the potential for significant clinical or
financial impact on the NHS. Estimates of potential uptake,
patient, service and financial implications are included
where possible. Reference is made to relevant national
guidance and links to in-depth independent reviews are
included, where available.
How is the content decided?
Various criteria are applied to prioritise those medicines in
the pipeline likely to have the largest impact. These
include considering whether:
the medicine is expected to provide a significant
improvement in disease management,
the medicine is first-in-class or has a major new
indication,
there are limited alternatives,
the medicine cost will be high,
the target population is large,
there is likely to be a significant effect on service
implications e.g. route/ formulation/ method of delivery,
the medicine or disease area is an NHS priority,
the medicine has significant additional indications in the
advanced pipeline stage,
the medicine is in the EU licensing process,
there is likely to be significant media interest.
UKMi September 2013 Solely for use within the NHS and not for commercial use. page 3 No responsibility is accepted for the content of documents derived from this original publication.
There will be additional, unquantifiable, factors that have
implications for the NHS such as local demographics and
prescribing preferences which cannot be accommodated in
a national document.
More detailed information on the medicines listed can be
obtained from the UKMi New Drugs Online (NDO)
database which can be accessed directly from the generic
name hyperlink in this document.
Please direct comments on Prescribing Outlook – New
Medicines to the editor: Helen Davis, North West
Medicines Information Centre, Pharmacy Practice Unit.
Other UKMi horizon scanning resources
Prescribing Outlook – National Developments estimates
the impact on clinical practice and prescribing budgets of
national guidance, mainly that issued by NICE. It is
intended to inform discussions between commissioners
and providers, and highlight issues around implementation
of guidance. Access is via www.ukmi.nhs.uk.
Prescribing Outlook – Cost Calculator is an Excel
spreadsheet tool to facilitate estimates of potential
prescribing changes for a local population. Access is via
www.ukmi.nhs.uk.
Please direct comments on Prescribing Outlook – National
Developments and the Cost Calculator to: Devika Sennik
or David Erskine, London and South East Medicines
Information Centre, Guy’s and St. Thomas’ NHS
Foundation Trust. [email protected],
New Drugs Online (NDO) database includes information
on medicines in clinical development from phase II trials to
product launch and includes links to evaluated information
on medicines up to one year post launch. This database is
maintained by UKMi and forms the basis of the content of
Prescribing Outlook – New Medicines. This dynamic
horizon scanning tool is updated daily and can be used to
produce reports based on a number of criteria including
possible launch date, stage of clinical development or
pharmaceutical company. Access is free to all with an NHS
email address via www.ukmi.nhs.uk but requires individual
registration. Access is. Limited access is also freely
available to non-NHS users via Evidence search
(www.evidence.nhs.uk).
Please direct comments and enquiries on New Drugs
Online to: Alexandra Denby, London Medicines Information
Service-Northwick Park, Northwick Park & St Mark's
Hospitals. [email protected]
Horizon scanning and new medicines support materials are available via www.ukmi.nhs.uk
The information in these resources is the best available at the time of publication but is subject to significant change with time.
Abbreviations
AWMSG All Wales Medicines Strategy Group
BNF British National Formulary
CCG Clinical Commissioning Group
DH Department of Health
EMA European Medicines Agency
EU European Union
HR Hazard ratio
HRG Healthcare Resource Group (definition)
i.m. Intramuscular
i.v. Intravenous
L(C)NDG London (Cancer) New Drugs Group
MHRA Medicines and Healthcare products Regulatory agency
MTRAC Midland Therapeutics Review & Advisory Committee
NDO New Drugs Online
NETAG North East Treatment Advisory Group
NHSE NHS England
NIHR-HSC National Institute for Health Research Horizon Scanning Centre
NICE National Institute for Health and Care Excellence
NICE-MPC NICE Medicines and Prescribing Centre
NNH Number needed to harm
NNT Number needed to treat
NPC National Prescribing Centre (now the NICE Medicines and Prescribing Centre – MPC)
ns Not significant
PAS Patient Access Scheme
PbR Payment by Results
RDTC Regional Drug & Therapeutics Centre, Newcastle
s.c. Subcutaneous
SIGN Scottish Intercollegiate Guidelines Network.
SMC Scottish Medicines Consortium
SmPC Summary of Product Characteristics
TBC To be confirmed
UKMi United Kingdom Medicines Information
US United States

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 4 No responsibility is accepted for the content of documents derived from this original publication.
Key
Generic name and formulation
Brand name
Company
Medicines
are listed by BNF category and linked to relevant publicly available pages of the NDO database.
The company that holds the marketing rights in the EU is listed together with a co-promoter company if relevant.
Included in abbreviated entries.
Indication
The indication
for the product.
The closer the drug is to launch the more specific this can be.
Included in abbreviated entries.
Current status
PII/III – in phase two/three trials.
Filed – licence application has
been submitted.
Recommended for approval – opinion of the advisory committee of the licensing authority suggests the medicine should be licensed. In the EU a full licence is likely within three months. Relevant links are included.
Licensed – the product has been
granted a marketing licence. The company determines launch date.
Launched – the medicine is
marketed in the EU. If launched elsewhere in the world, but not the UK, there are links to prescribing data.
Orphan status – If a medicine has a designated orphan status this is indicated (see definition page 7).
The following apply to US expediated programmes for serious or life-threatening conditions and suggest the drug will pass through licensing systems faster:
Breakthough therapy status –preliminary evidence indicates substantial improvement over existing therapies on clinically significant outcomes.
Fast-track status –potential to address unmet needs.
Priority review – provides significant improvement in safety or effectiveness.
Included in abbreviated entries.
Predicted UK launch or licence extension
An informed estimate based on knowledge of processes and timescales involved in licensing systems.
It is easier to predict when a product will be available once it is has entered the licensing process as known time frames apply. However, once a licence has been granted the company decides when and where to launch the product.
Included in abbreviated entries.
National guidance: Relevant publications (funding source).
NICE - National Institute for Health and
Care Excellence: www.nice.org.uk (DH).
SIGN - Scottish Intercollegiate Guidelines
Network. www.sign.ac.uk (NHS
Scotland).
SMC - Scottish Medicines Consortium.
www.scottishmedicines.org.uk (NHS
Scotland).
AWMSG - All Wales Medicines Strategy
Group. www.wales.nhs.uk/awmsg (NHS).
Reviews: Independent reviews and regional guidance that is accessible to all NHS sectors published between 2011 and 2013. Included in abbreviated entries.
NICE-MPC: NICE Medicines and
Prescribing centre (DH).
NIHR-HSC - NIHR Horizon Scanning
Centre. www.nhsc-healthhorizons.org.uk.
(NIHR).
NPC - National Prescribing Centre (now
the NICE-MPC. www.npc.co.uk. (Legacy
site for reviews prior to May 2012).
UKMi - United Kingdom Medicines
Information. www.ukmi.nhs.uk (NHS).
L(C)NDG - London (Cancer) New Drugs
Group (NHS organisations in Greater
London).
MTRAC - Midlands Therapeutics Review
& Advisory Committee. www.mtrac.co.uk.
(Primary Care NHS organisations in the
Midlands).
NETAG - North East Treatment Advisory
Group. www.netag.nhs.uk (legacy site of
sub-group of North East Specialised
Commissioning Group).
RDTC - Regional Drug & Therapeutics
Centre. rdtc.nhs.uk. (NHS organisations
in the North East of England).
Target population: Data
on prevalence (number with the disease) and incidence (number of new cases each year) are reported for a 100,000 population, if possible.
Sector: An indication of which sector in the NHS the medicine is likely to impact, at least initially, in terms of service provision.
Implications: Factors highlighted include patient options, monitoring or testing requirements
and service implications related to medicine delivery.
Financial implications: Cost implications are assessed based on a number of assumptions such as whether the medicine is added to existing therapy or is a competitor in areas where budgets are established. Factors that are difficult to quantify include likely uptake of the medicine within the target population. For launched products, costs are taken from the latest published NHS costs, or, for generic prices, from the Drug Tariff. Where a patient access scheme (PAS) may apply this is indicated. Unless stated, costs do not include VAT.
Likely commissioning route: An estimate of the potential commissioning route based on NHS structures implemented since Apr 2013 i.e. CCG or NHS England (NHSE). Included in abbreviated entries.
Payment by Results (PbR): The actual or anticipated tariff position based on historical
assumptions. For drugs not yet launched this becomes an educated guess. Drugs previously referred to as ‘PbR exclusions’ are now known as ‘Specified high cost drugs’. If a drug is not likely to be a specified high cost drug it is therefore, by default, likely to be included within tariff and will be listed as ‘HRG included’. Included in abbreviated entries.
Pharmacology: Therapeutic class and/or mode of action and administration details. Included in abbreviated entries.
Efficacy: Key studies with a link to trial details, especially when relevant for licence application. Primary outcome data and patient, rather than disease, orientated outcomes are preferentially included where available.
Safety: For medicines already marketed for other indications a link to the product information is included. For new
medicines, information is included where it is thought adverse effects reported to date may influence licensing requirements e.g. increased monitoring or where they differ significantly from those associated with current treatments.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 5 No responsibility is accepted for the content of documents derived from this original publication.
Summary of predicted launch dates
This list summarises the earliest predicted UK launch date for pipeline drugs listed in Table 1 – Pipeline drugs.
Refer to the index for a full list of generic and proprietary names. *Indicates which drugs have been assigned
orphan status in the EU (see page 7 for more details).
BNF Drug Indication Page
Late 2013
1 Golimumab Ulcerative colitis 11
2 Lomitapide Hypercholesterolaemia- familial
16
2 Defibrotide* Hepatic veno-occlusive disease
17
3 Indacaterol/ glycopyrronium
Chronic obstructive pulmonary disease
18
3 Nalfurafine* Dialysis-related pruritus 19
4 Lurasidone Schizophrenia 20
5 Tobramycin* Cystic fibrosis 22
5 Bedaquiline Tuberculosis 22
5 Cobicistat HIV infection (booster) 23
5 Dolutegravir HIV infection 23
6 Alogliptin Type 2 diabetes mellitus 26
6 Canagliflozin Type 2 diabetes mellitus 26
6 Dapagliflozin/ metformin
Type 2 diabetes mellitus
27
6 Follitropin alfa Biosimilar 70
7 Botulinum A toxin
Overactive bladder 29
8 Cabozantinib* Thyroid cancer 31
8 Afatinib Non-small cell lung cancer
31
8 Trastuzumab emtansine
Breast cancer 33
8 Trastuzumab/ hyaluronidase
Breast cancer 34
8 Masitinib* Pancreatic cancer 36
8 Regorafenib Colorectal cancer 37
8 Sipuleucel-T Prostate cancer 39
8 Radium-223 chloride
Prostate cancer 40
8 Dabrafenib Malignant melanoma 43
8 Bendamustine Non-Hodgkin’s lymphoma
45
8 Rituximab Non-Hodgkin’s lymphoma
45
8 Bortezomib Multiple myeloma 46
8 Alemtuzumab Multiple sclerosis 48
8 Laquinimod Multiple sclerosis 49
8 Dimethyl fumarate
Multiple sclerosis 50
8 Teriflunomide Multiple sclerosis 50
9 Eltrombopag Thrombocytopenia 51
9 Sodium phenylbutyrate
Urea cycle disorders 52
BNF Drug Indication Page
9 Alipogene tiparvovec*
Lipoprotein lipase deficiancy
52
10 Canakinumab* Juvenile idiopathic arthritis
53
10 Ustekinumab Psoriatic arthritis 54
10 Ataluren* Duchenne muscular dystrophy
55
10 Pegloticase Gout prophylaxis 55
11 Aflibercept Macular oedema 56
13 Afamelanotide* Erythropoietic protoporphyria
58
14 Meningococcal group-B vaccine
Meninitis B 59
2014
1 Vedolizumab Ulcerative colitis 11
1 Teduglutide* Short bowel syndrome 12
1 Vedolizumab Crohn's disease 12
2 Apixaban Venous thromboembolism treatment
13
2 Dabigatran Venous thromboembolism treatment and secondary prevention
13
2 Rivaroxaban Secondary prevention of atherothrombotic events in acute coronary syndrome
14
2 Rivaroxaban Acute coronary syndrome- prevention of stent thrombosis
14
2 Cangrelor Acute coronary syndrome – thrombosis prevention
15
2 Vorapaxar Secondary prevention of cardiovascular events
15
2 Riociguat Pulmonary arterial hypertension
16
2 Clevidipine Hypertension, perioperative
17
3 Umeclidinium Chronic obstructive pulmonary disease
18
3 Umeclidinium /vilanterol
Chronic obstructive pulmonary disease
18
3 Budesonide/ formoterol (Bufomix)
Asthma 19
3 Omalizumab Urticaria 19
4 Loxapine Agitation associated with schizophrenia and bipolar disorder
20

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 6 No responsibility is accepted for the content of documents derived from this original publication.
BNF Drug Indication Page
4 Dextrometh-orphan/quinidine
Pseudobulbar affect 21
4 Liraglutide Obesity 21
5 Simeprevir Hepatitis C 24
5 Sofosbuvir Hepatitis C 24
6 Bazedoxifene/ conjugated estrogens
Postmenopausal osteoporosis and menopausal symptoms
28
6 Insulin degludec /insulin aspart
Type 1 and 2 diabetes mellitus
27
6 Pasireotide* Acromegaly 28
6 Tolvaptan Polycystic kidney disease
29
6 Follitropin alfa Biosimilar 70
7 Collagenase clostridium histolyticum
Peyronie's disease 30
8 Sorafenib Thyroid cancer 30
8 Lenvatinib* Thyroid cancer 31
8 Enobosarm Non-small cell lung cancer
33
8 Trastuzumab emtansine
Breast cancer 34
8 Bevacizumab Breast cancer 34
8 Everolimus Breast cancer 35
8 Regorafenib Gastrointestinal stromal tumours
36
8 Doxorubicin heat-sensitive*
Hepatocellular carcinoma
37
8 Sorafenib Renal cell carcinoma 38
8 Apaziquone Bladder cancer 38
8 Ipilimumab Prostate cancer - treatment
39
8 Pazopanib Ovarian cancer 40
8 Bevacizumab Ovarian cancer 41
8 Vintafolide* Ovarian cancer 41
8 Paclitaxel* Ovarian cancer 41
8 Ipilimumab Malignant melanoma 42
8 Ipilimumab Malignant melanoma 43
8 Trametinib Malignant melanoma 44
8 Dasiprotimut-T* Non Hodgkin’s lymphoma
45
8 Carfilzomib* Multiple myeloma 46
8 Obinutuzumab* Chronic lymphocytic leukaemia
47
8 Ofatumumab* Chronic lymphocytic leukaemia
47
8 Chlormethine* Cutaneous T cell lymphoma
48
8 Peginterferon beta 1a
Multiple sclerosis 49
8 Teriflunomide Multiple sclerosis 51
8 Trastuzumab Biosimilar 70
BNF Drug Indication Page
9 Elosulfase alfa* Mucopolysaccharidosis IVA
51
10 Golimumab Juvenile idiopathic arthritis
53
10 Apremilast Psoriatic arthritis 54
10 Idebenone* Duchenne muscular dystrophy
56
11 Aflibercept Diabetic macular oedema
56
13 Apremilast Psoriasis 57
13 Tofacitinib Psoriasis 57
13 Secukinumab Psoriasis 58
13 Propranolol Infantile haemangioma 58
2015 or 2016
1 Obeticholic acid Cirrhosis 12
1 Infliximab Biosimilar 70
2 Desmoteplase Stroke 15
2 Evolcumab Hyperlipidaemia 16
2 Alirocumab Hypercholesterolaemia 16
3 Masitinib Asthma 19
3 Ataluren* Cystic fibrosis 20
3 Lumacaftor Cystic fibrosis 20
5 ABT450/ ritonavir / ABT-267/ ABT333
Hepatitis C 25
5 Asunaprevir/ daclatasvir
Hepatitis C 25
5 Sofosbuvir/ ledipasvir
Hepatitis C 25
5 Actoxumab/ bezlotoxumab
Clostridium difficile infection
25
6 Insulin inhaled Type 1 and 2 diabetes mellitus
27
6 Exenatide implant
Type 2 diabetes mellitus
27
6 Insulin glargine Biosimilar 70
8 Brain cancer vaccine*
Glioblastoma 30
8 Afatinib Head and neck cancer 30
8 Afatinib Non-small cell lung cancer
32
8 Belagen-pumatucel-L
Non-small cell lung cancer
32
8 LDK378 Non-small cell lung cancer
32
8 Eribulin Non- small cell lung cancer
32
8 Dacomitinib Non-small cell lung cancer
32
8 Ganetespib Non-small cell lung cancer
32
8 Anamorelin Cancer cachexia 33
8 Sorafenib Breast cancer 35
8 Palbociclib Breast cancer 35

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 7 No responsibility is accepted for the content of documents derived from this original publication.
BNF Drug Indication Page
8 Ramucirumab* Hepatocellular carcinoma
37
8 Sorafenib* Hepatocellular carcinoma
37
8 Custirsen Prostate cancer 39
8 Cabozantinib Prostate cancer 40
8 Trebananib Ovarian cancer etc. 42
8 Olaparib* Ovarian cancer 42
8 Eribulin* Sarcoma 42
8 Talimogene laherparepvec
Malignant melanoma 44
8 Cobimetanib Malignant melanoma 44
8 Erismodegib Basal cell carcinoma 44
8 Daratumumab Multiple myeloma 46
8 Ibrutinib* Mantle cell lymphoma 47
8 Idelalisib Chronic lymphocytic leukaemia
47
8 Vosaroxin* Acute myeloid leukaemia
47
8 Ibrutinib Chronic lymphocytic leukaemia
48
BNF Drug Indication Page
8 Rigosertib* Myelodysplastic syndromes
48
8 Daclizumab Multiple sclerosis 50
8 Fingolimod Multiple sclerosis 50
9 Sebelipase alfa* Liposomal acid lipase deficiency
52
10 Masitinib Rheumatoid arthritis 53
10 Secukinumab Rheumatoid arthritis 53
10 Secukinumab Ankylosing spondylitis 54
10 Secukinumab Psoriatic arthritis 54
10 Lesinurad Gout 55
10 Odanacatib Osteoporosis in men 55
10 Infliximab Biosimilar 70
11 Aflibercept Macular oedema 57
Uncertain
2 Serelaxin Heart failure 17
8 Omacetaxine* meppesuccinate
Chronic myelogenous leukaemia
46
*Indicates which drugs have been assigned orphan status in the EU. To qualify for orphan designation, a medicine must meet one of these criteria:
It is intended for a life-threatening or chronically debilitating condition affecting no more than 5 in 10,000 (50 in 100,000)
people in the EU;
It is intended for a life-threatening, seriously debilitating or serious and chronic condition and without incentives it is
unlikely that the revenue after marketing would cover the investment in its development.
In both cases, there must also be either no satisfactory method of diagnosis, prevention or treatment of the condition concerned
authorised, or, if such a method exists, the medicine must be of significant benefit to those affected by the condition.
Manufacturers of drugs that have received orphan designation benefit from incentives to support development of medicines to
treat rare diseases.
The US definition of an orphan drug is different. It is defined as a rare disease occurring in less than 200,000 individuals.
Assuming a US population of about 311 million this translates to a prevalence of about 65 in 100,000. The definition of an ultra
orphan condition used by NICE is a UK prevalence of less than 1 in 50,000.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 8 No responsibility is accepted for the content of documents derived from this original publication.
Highlights
The drugs listed below have been selected from table 1 (drugs not yet marketed) as warranting special
consideration due to their expected overall NHS impact taking account of financial implications, service provisions,
place in therapy and target population. Such data are limited so the list is for guidance only and will not take
account of local factors or perspective which will vary by sector, geography and speciality. You may also want to
refer to table 3 (recently launched drugs) to identify those requiring active management locally.
Drug Indication Reasons for highlighting
Defibrotide
page 17
Hepatic
veno-
occlusive
disease
(VOD).
In haematopoietic stem-cell transplant VOD is a leading cause of morbidity and mortality.
Supportive care is the current treatment option. Defibrotide will be the first specific therapy
for VOD. It is likely to be expensive; based on a dose of 25mg/kg/day, current named
patient cost is around £40,000 for 21 days treatment.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Rivaroxaban
page 14
Acute
coronary
syndrome
(ACS).
Rivaroxaban 2.5mg twice daily will be used for prevention of atherosclerotic events in
patients with elevated cardiac biomarkers in combination with one or more antiplatelets.
However, bleeding risks may be a concern, especially in older patients. Cost will be in
addition to existing therapy; price is currently uncertain.
Likely commissioning route: CCG. PbR: HRG included.
Dextro-
methorphan/
quinidine
page 21
Pseudo-
bulbar
affect
(PBA).
PBA can develop in several neurological diseases such as multiple sclerosis, or following
brain injury. The estimated prevalence of PBA is up to 500 per 100,000 people. This is the
first drug licensed for PBA. Diagnosis needs confirmation before treatment and may
increase referrals to specialist neurosciences. It is likely to be considerably more expensive
than unlicensed alternatives.
Likely commissioning route: NHSE. PbR: Likely HRG included.
Insulin
degludec/
insulin aspart
page 27
Type 1 and
type 2
diabetes
mellitus.
Estimated UK prevalence of diagnosed diabetes was 2.9 million people in 2011and a
further 850,000 are undiagnosed. Prevalence is projected to increase to 5 million by 2025.
Spending on analogue insulin is increasing and combination use of analogues is likely to
increase.
Likely commissioning route: CCG. PbR: HRG included.
Tolvaptan
page 29
Autosomal-
dominant
polycystic
kidney
disease
(ADPKD)
ADPKD has a prevalence of 100-1,300 per 100,000 people. In 2007 polycystic kidney
disease accounted for 12.7% of patients receiving renal transplants. There are currently no
therapies that modify disease course and slow decline in renal function. Current options
include anti-hypertensives, dialysis and renal transplant. Tolvaptan 60mg/day costs over
£4,100/month.
Likely commissioning route: Uncertain -depending on statge of renal failure.
PbR: Specified high cost drug.
Everolimus
Trastuzumab
emtansine
pages 34,35
Breast
cancer
(BC),
advanced
HER2-
positive –
first-,
second- or
third-line.
The incidence of metastatic BC in the UK is about 32 per 100,000 people. 25% are HER2-
positive with a worse prognosis. About 70% of patients do not respond to first-line
trastuzumab and the rest develop resistance within the first year.
Adding everolimus first-line may improve response rates and delay need for second-line
chemotherapy; it will compete with i.v. pertuzumab and costs will be additive. Used second
or third-line everolimus is an alternative to lapatinib for overcoming trastuzumab resistance.
Current monthly cost of everolimus is £2,250 to £2,970.
First-in-class trastuzumab emtansine is an antibody conjugate of trastuzumab and an anti-
mitotic agent, maytansinoid DM1. Used first-line in combination with pertuzumab it would
prevent the need for first-line chemotherapy and could result in a delay in disease
progression and improved quality of life. Cost is unknown but it would displace
trastuzumab plus taxane therapy. US cost is $9,800 a month. When used second or third-
line trastuzumab emtansine will compete with other second-line options including biological
therapies, chemotherapies and hormonal therapies.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 9 No responsibility is accepted for the content of documents derived from this original publication.
Trastuzumab/
hyaluronidase
page 34
Breast
cancer - s.c.
formulation.
Trastuzumab is co-formulated with recombinant human hyaluronidase to facilitate
absorption of trastuzumab through subcutaneous tissue. Compared to the i.v. formulation
which is given as a 30 minute infusion, s.c. trastuzumab will reduce preparation and
administration time. Cost is currently unknown.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Masitinib
page 36
Pancreatic
cancer,
advanced –
first-line.
UK incidence of pancreatic cancer is 13 per 100,000 people; 90% have advanced disease
at diagnosis and 3% survive 5 years. Masitinib may extend life in patients with few options.
It will be given in addition to gemcitabine, which is recommended by NICE for patients with
a Karnofsky score of ≥50. A test for the prognostic genetic biomarker is being developed.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Regorafenib
page 37
Colorectal
cancer
(CRC),
metastatic –
third- or
fourth-line.
UK incidence of CRC is 67 per 100,000 people; 20-55% of patients present with metastatic
disease. Management is mainly palliative with surgery and chemo/radiotherapy. For
patients with no further treatment options, regorafenib may delay disease progression and
improve quality of life. Regorafenib will be additive to other therapies. UK cost is unknown
but US cost is $9,350 per month.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pazopanib
Bevacizumab
Vintafolide
pages 40, 41
Ovarian
cancer
(OC).
UK incidence of OC is 21 per 100,000 people. 75% receive first-line platinum
chemotherapy; between 70 and 80% respond. Of these 55-75% relapse within 2 years and
most receive platinum chemotherapy a second or third time before developing resistance.
Pazopanib will be used as maintenance after first-line chemotherapy in addition to current
therapies, and may delay need for second-line chemotherapy. Monthly cost of 800mg daily
is £2,200.
Bevacizumab will be used in addition to chemotherapy in advanced platinum-resistant
disease. Current cost of 10 doses (15mg/kg) for a 65kg woman is £23,000.
Vintafolide will be used in advanced platinum-resistant, folate receptor (FR)-positive
disease and a radiopharmaceutical diagnostic test is needed to identify FR-positive
tumours (90% of patients). Vintafolide will be used in addition to doxorubicin.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Ipilimumab
Trametinib
Dabrafenib
pages 42, 43,
44
Malignant
melanoma.
UK incidence of malignant melanoma is about 21 per 100,000 people, and is doubling
every 10-20 years. 7% of 15-64 year olds present with advanced (III/IV) disease compared
with 20% aged ≥65 years. Median survival is 6-9 months, with 40-50% of stage III patients
surviving 5 years.
Ipilimumab will be used in resected high-risk stage III disease (first-line adjuvant therapy) to
delay or prevent recurrence, and in unresectable or metastatic disease (first-line with
dacarbazine). There is currently no standard adjuvant therapy. In combination with first-line
standard of care dacarbazine, ipilimumab will be an option for patients whose tumours do
not have BRAF mutations. Ipilimumab costs £52,500 per dose for a 70kg person.
Oral trametinib will be used in unresectable or metastatic BRAF-positive disease (first-or
second-line monotherapy and first-line in combination with dabrafenib). Trametinib, like
dabrafenib and vemurafenib, are alternatives to i.v. dacarbazine. A test is needed to
identify BRAF-positive patients. Combination therapy offers the possibility of improved
survival and better tolerability. US cost of trametinib is $8,700 for a 30-day supply.
Dabrafenib, used alone for first-line therapy, is likely to be similarly priced to vemurafenib
(£7,000 per month).
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Rituximab
page 45
Non-
Hodgkin's
lymphoma
(NHL) - s.c.
formulation.
Rituximab s.c. will be an option for all patients with NHL for whom i.v. rituximab is currently
indicated. Those with poor venous access may be initial candidates. It could reduce
outpatient preparation and administration time. Rituximab s.c. is likely to cost the same as
the current i.v. formulation but future availability of biosimilar i.v. formulations may affect
pricing strategy.
Likely commissioning route: NHSE. PbR: Specified high cost drug.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 10 No responsibility is accepted for the content of documents derived from this original publication.
Obinutuzu-
mab
Ofatumumab
page 47
Chronic
lymphocytic
leukaemia
(CLL).
UK annual incidence of CLL is 4.2 per 100,000 people, increasing to over 30 per 100,000
in those over 80 years of age.
Obinutuzumab and ofatumumab are humanised anti-CD20 monoclonal antibodies and
alternatives for patients with co-morbidities who cannot have FCR (fludarabine,
cyclophosphamide, rituximab). Current options for these patients include chlorambucil or
bendamustine (both with/ without rituximab) or reduced dose FCR. Ofatumumab 100mg
costs £1,820 per month. Alternative costs are chlorambucil £56, bendamustine £966,
rituximab £1,572.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Alemtuzumab
Laquinimod
Dimethyl
fumarate
Teriflunomide
pages 48, 49,
50
Multiple
sclerosis -
relapsing-
remitting
(RRMS).
In a population of 100,000, 39 will have relapsing-remitting disease (RRMS). 31% of these
receive, disease modifying agents; 74% interferons and 26% glatiramer. The availability of
more convenient and acceptable oral preparations could increase the proportion of patients
treated. NICE estimated that fingolimod, the first licensed oral preparation for RRMS, could
take up to 15% of the interferon market share. There may be price competition as more
oral agents become available.
Alemtuzumab will be for active RRMS defined by clinical or imaging features. As a single
annual i.v. treatment it may be attractive. Use is likely to be in the second-line setting.
Acquisition cost may be similar to other options but there may be additional monitoring
costs. Oral laquinimoddimethyl fumarate and teriflunomide will compete with fingolimod
which costs about £19,500/year although there is a PAS in place.
Likely commissioning route: NHSE. PbR: Specified high cost drugs.
Eltrombopag
page 51
Thrombo-
cytopenia
(TCP)
associated
with
hepatitis C
(HepC).
About 216,000 people in the UK are infected with hepatitis C (340 per 100,000); estimates
of the prevalence of HepC-associated TCP ranges from 0.16 - 45.4%. TCP may interfere
with diagnostic procedures, such as liver biopsy, and may exclude patients from antiviral
treatment. Eltrombopag will be used where TCP prevents starting, or limits the ability to
maintain, optimal interferon-based therapy. Eltrombopag costs between £770 and £3,080
for 28 days treatment.
Likely commissioning route: Uncertain – depending on complexity of patient.
PbR: Specified high cost drug.
Elosulfase
alfa
page 51
Mucopoly-
saccharid-
osis IVA.
Mucopolysaccharidosis type IVA affects less than 15 in 100,000 people in the EU and there
are currently no licensed treatments. Elosulfase is likely to be expensive and similar to
other treatments for mucopolysaccharidosis diseases (galsulfase, idursulfase, laronidase).
Likely commissioning route: NHSE. PbR: Likely specified high cost drug.
Apremilast
page 54
Plaque
psoriasis,
moderate to
severe.
Estimated prevalence of psoriasis in England is 1.63%; about 20 per 100,000 people have
moderate to severe disease. Plaque psoriasis is the most common form, affecting 80-90%
of people; about 1.1% are eligible for biological treatment. Apremilast is likely to be
licensed for use after conventional systemic therapies, but as an oral preparation may be
considered preferable to parenteral biological therapies. Acquisition and administration cost
may be lower than for biologicals.
Likely commissioning route: CCG. PbR: Likely specified high cost drug.
Ataluren
page 55
Duchenne
muscular
dystrophy,
nonsense-
mutation
(nmDMD).
DMD affects 1 in 3,600 to 6,000 male births in the UK; about 100 boys are diagnosed
annually and prevalence is about 1,500. 10-15% have a nonsense mutation (150-195
patients in the UK). Current options (corticosteroids) can delay but not prevent loss of
walking ability. Ataluren is the first therapy to target the underlying defect in nmDMD. It is
likely to be additional to current therapy in ambulant patients but could prolong
independence and delay complications. Likely to be expensive.
Likely commissioning route: NHSE. PbR: Likely specified high cost drug.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 11 No responsibility is accepted for the content of documents derived from this original publication.
Table 1. Pipeline drugs
BNF 1. Gastrointestinal system
Golimumab injection
Simponi
MSD
Indication: Ulcerative colitis (UC), moderate to severe – second-line if inadequate response/ intolerance/ contra-indication to conventional therapy.
Current status: Recommended for approval in EU Jul 2013.
Licensed in US - see prescribing information.
Predicted UK licence extension:
2013
National guidance:
NICE: UC - management, infliximab - UC
subacute manifestations, acute exacerbations. Biologic drugs commissioning guide.
Reviews: NIHR HSC Sep 2011.
Target population: The incidence and prevalence of UC in the UK is about 10 and 240 per 100,000 people, respectively. 30–60% of people will have at least one relapse per year. About 80% of these are mild to moderate and about 20% are severe.
Sector: Secondary care.
Implications: Golimumab will be a second-line option with the advantage of s.c. administration vs. i.v. administration for infliximab. However, monthly administration is required vs. every 6-8 weeks for infliximab.
Financial: As a further treatment option it will be additional to current costs.
Likely commissioning route: CCG. PbR: Specified high cost drug.
Pharmacology: Anti-TNF monoclonal antibody given by monthly s.c. injection.
Efficacy: The published PURSUIT-SC study (n=774) compared induction treatment with golimumab (either 200mg or 400mg at week 0 and 100mg or 200mg at week 2) with placebo. The primary outcome of clinical response (defined as Mayo score of ≥30% and 3 points vs. baseline score, with a decrease in rectal bleeding subscore of ≥1 or a rectal bleeding subscore of 0 or 1) at week 6 was met by 52%, 55% and 30% of patients, respectively (p<0.01, NNT=4). In the published PURSUIT-M study 464 patients who had responded to induction therapy in PURSUIT-SC were randomised to golimumab 50mg, 100mg or placebo every 4 weeks to week 52. Clinical response was maintained through to week 54 in 47% (p=0.01, NNT=6), 50.6% (p<0.001, NNT=5) vs. 31.4%, respectively.
Safety: See medicines.org.uk.
Vedolizumab injection
Takeda
Indication:
Ulcerative colitis (UC), moderate to severe - second-line when resistant/ intolerant to conventional therapy and to TNF-alpha antagonists.
Current status:
Filed in EU Mar 2013.
Predicted UK launch:
2014
National guidance:
As for golimumab above.
Reviews: NIHR HSC Mar 2013.
Target population: As for golimumab above.
Sector: Secondary care.
Implications: As first in a new class this could be an attractive option for patients with limited alternatives. It could compete with golimumab above as a second-line option but has the disadvantage of being an i.v. infusion.
Financial: As a further treatment option it will be additional to current costs.
Likely commissioning route: CCG. PbR: Likely specified high cost drug.
Pharmacology: Monoclonal-antibody, alpha4-beta7 integrin antagonist (first-in-class), given as a 30 minute i.v. infusion.
Efficacy: In the published PIII GEMINI I study, patients were randomised to vedolizumab or placebo at weeks 0, 2, 6 and then at 4- or 8-week intervals for up to one year. The primary outcome was the proportion of patients with clinical response at week 6 (induction period) and clinical remission at week 52. At week 6, response rates were 47.1% with vedolizumab vs. 25.5% with placebo (p<0.01, NNT=5). Among initial responders re-randomised at 6 weeks, 52-week remission rates were 44.8% with 4 weekly vs. 41.8% with 8 weekly vedolizumab vs. 15.9% for placebo (p<0.001 for both, NNT=3 and 4).
Safety: Frequency of adverse events in trials was comparable to placebo.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 12 No responsibility is accepted for the content of documents derived from this original publication.
Vedolizumab injection
Takeda
Indication:
Crohn’s disease, moderate
to severe - second-line when resistant/ intolerant to conventional therapy and to TNF-alpha antagonists.
Current status:
Filed in EU Mar 2013.
Predicted UK launch:
2014
National guidance:
NICE: Crohn’s disease: pathway, clinical
guideline; infliximab and adalimumab; Biologic drugs commissioning guide.
Reviews: NIHR HSC Mar 2013.
Target population: Estimates of UK
prevalence of Crohn’s disease range from 50 to 150 per 100,000 people; 20% may have severe active disease and up to 50% may be resistant to, or intolerant of, existing therapy, including TNF inhibitors.
Sector: Secondary care.
Implications: As first in a new class vedolizumab could be an attractive
option for patients with limited alternatives.
Financial: As a further treatment option it will be additional to current costs.
Likely commissioning route: CCG. PbR: Likely specified high cost drug.
Pharmacology: Monoclonal-antibody, alpha4-beta7 integrin antagonist (first-in-class), given as a 30 minute i.v. infusion.
Efficacy: In the published PIII GEMINI II study, patients were randomised to vedolizumab or placebo at weeks 0, 2, 6 and then at 4- or 8-week intervals for up to one year. The primary outcome was the proportion of patients in clinical remission at week 6 (induction period) and week 52. At week 6, remission rates were 14.5% with vedolizumab vs. 6.8% with placebo (p<0.03, NNT=13). Among initial responders re-randomised at 6 weeks, remission rates at 52 weeks were 36.4% with vedolizumab every 4 weeks vs. 39.0% for vedolizumab every 8 weeks vs. 21.6% for placebo (p<0.01 for both, NNT=7 and 6). In GEMINI III in 315 patients who failed anti-TNF therapy remission rates at week 6 were 15.2% vs. 12.1% for vedolizumab and placebo, respectively (p=ns).
Safety: Frequency of adverse events in trials was comparable to placebo.
Teduglutide injection
Revestive
NPS Pharma-ceuticals
Indication:
Short bowel syndrome (SBS).
Current status:
Licensed in EU Sep 2012 with orphan status – see prescribing information.
Predicted UK launch:
2014
National guidance:
NICE: Nutrition support in adults: clinical
guideline.
Reviews: No recent reviews.
Target population: The UK estimated
incidence of short bowel syndrome is 2 to 5 cases per million people.
Sector: Severe intestinal failure treatment is a specialised service.
Implications: Teduglutide would be the first drug specifically licensed for
SBS, the most common indication for home parenteral nutrition (PN). It may reduce PN volume requirements.
Financial: Likely to be expensive and additive to current options. The cost of teduglutide in the US is $295,000 a year. EU launch has been delayed by returning rights from Takeda to NPS Pharmaceuticals who recently established an office in Dublin in preparation for EU pricing negotiations. Teduglutide may initially be available on a named patient basis.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: Glucagon-like peptide-2 (GLP-2) analogue given by daily s.c injection.
Efficacy: In a published PIII study (n=86) teduglutide 0.05mg/kg was compared with placebo. Reduction in PN of ≥20% at weeks 20 to 24 was achieved by 63% vs. 30%, respectively (p=0.002, NNT=3). Patients completing this study were eligible to enter a 2-year follow-up study where all received teduglutide 0.05mg/kg. At a 6-month interim review, continued reductions in PN had been achieved and 3 patients no longer required PN. Another published PIII study (n=83) compared teduglutide to placebo. Teduglutide 0.10mg/kg did not meet the primary outcome of reduction of ≥20% in PN in weeks 16-24 (25% vs. 6%, p=ns). However, a post-hoc analysis of patients on teduglutide 0.05mg/kg did meet the primary outcome (46% vs. 6%, p<0.01, NNT=3). In a continuation study, of those who achieved ≥20% reduction of PN at week 20 and 24 in the initial study, 75% sustained this response after up to one year of continuous treatment.
Obeticholic acid oral
Intercept
Indication:
Cirrhosis, primary biliary - second line.
Pharmacology:
Modified bile acid; farnesoid X receptor agonist - first-in-class.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Likely HRG included.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 13 No responsibility is accepted for the content of documents derived from this original publication.
BNF 2. Cardiovascular system
Dabigatran oral
Pradaxa
Boehringer Ingelheim
Indication:
Venous thromboembolism (VTE) - treatment and secondary prevention (long-term).
Current status:
Filed in EU Jun 2013.
Predicted UK licence extension:
2014
National guidance:
NICE: VTE pathway, quality standard,
anticoagulation commissioning guide, guideline - thromboembolic diseases; VTE treatment and prevention: dabigatran due Oct 2014, rivaroxaban.
SIGN: VTE.
Reviews: No recent reviews.
Target population: Annual incidence of pulmonary embolism (PE) and deep vein thrombosis (DVT) is about 40 and 100 per 100,000 people, respectively.
Sector: Initiated in secondary care.
Implications: Dabigatran will compete with rivaroxaban currently licensed for treatment and prevention of recurrent DVT and PE and with apixaban currently in PIII studies for this indication (see below). Differences in dosing frequency may be important for compliance.
Financial: Competition will continue to influence pricing strategies.
Likely commissioning route: CCG. PbR: HRG included.
Pharmacology: Direct thrombin inhibitor.
Efficacy: Treatment. The published RE-COVER non-inferiority study (n=2,539) compared dabigatran (150mg twice daily) to warfarin (INR 2.0-3.0) for acute symptomatic VTE. The primary outcome was a composite of recurrent symptomatic VTE and deaths related to VTE, which was confirmed in 2.4% of patients on dabigatran and 2.1% of patients on warfarin (p<0.001 for non-inferiority). Major bleeding did not differ between the groups at 1.6% vs. 1.9%, respectively.
Secondary prevention. Two published PIII trials have compared dabigatran (150 mg twice daily) with warfarin (RE-MEDY, n=2,866) or placebo (RE-SONATE, n=1,353) in patients who had completed at least 3 months of treatment for VTE. In RE-MEDY, after a mean of 68 weeks treatment dabigatran was found to be non-inferior to warfarin for prevention of the primary outcome of recurrent symptomatic VTE or death associated with VTE (1.8% vs. 1.3%, p=0.01 for non-inferiority). Major bleeding was less common with dabigatran than warfarin (0.9% vs. 1.8%, p=0.06). In RE-SONATE, after a mean of 24 weeks treatment, recurrent VTE occurred in 0.4% vs. 5.6% of patients, respectively (p<0.001). Major or clinically relevant non-major bleeding was more common with dabigatran than placebo (5.3% vs. 1.8%, p=0.001, NNH=29).
Safety: See medicines.org.uk.
Apixaban oral
Eliquis
Pfizer
Indication:
Venous thromboembolism (VTE) treatment - extended use.
Current status:
PIII.
Predicted UK licence extension:
2014
National guidance:
As for dabigatran above.
Reviews: None.
Target population: Annual incidence of pulmonary embolism (PE) and deep vein thrombosis (DVT) is about 40 and 100 per 100,000 people, respectively.
Sector: Initiated in secondary care.
Implications: Rivaroxaban is now licensed for treatment and prevention of recurrent DVT and PE and dabigatran could have a similar licence soon (see above). Apixaban will be a competitor; differences in dosing frequency may be important for compliance.
Financial: Competition will influence pricing strategies.
Likely commissioning route: CCG. PbR: HRG included.
Pharmacology: Factor Xa inhibitor.
Efficacy: The published PIII AMPLIFY trial (n=5,395) compared apixaban (10mg twice daily for 7 days, then 5mg twice daily for 6 months) with standard care (enoxaparin and warfarin). Apixaban was non-inferior to standard care for the primary outcome recurrent symptomatic VTE or death related to VTE (2.3% vs. 2.7%, p<0.001 for non-inferiority). In the published PIII AMPLIFY-EXT trial (n=2,486) apixaban was compared with placebo for 12 months. Recurrent VTE or death was more common with placebo (8.8%) than apixaban 2.5mg twice daily (1.7%) or apixaban 5.0mg twice daily (1.7%, p<0.001, NNT=14 for both comparisons).
Safety: See medicines.org.uk.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 14 No responsibility is accepted for the content of documents derived from this original publication.
Rivaroxaban oral
Xarelto
Bayer
Indication:
Acute coronary syndrome (ACS) - prevention of atherothrombotic events in patients with elevated cardiac biomarkers (combination with antiplatelet drugs).
Current status:
Licensed in the EU May 2013 – see prescribing information.
Predicted UK launch:
2014
National guidance:
NICE: ACS: Ticagrelor , unstable angina
and NSTEMI, secondary prevention post MI, prasugrel with percutaneous coronary intervention, rivaroxaban due Mar 2015.
SIGN: ACS
Reviews: NPC Mar 2012, NIHR HSC Apr 2011.
Target population: ACS refers to a group of conditions including ST segment elevation myocardial infarction (STEMI), non-STEMI and unstable angina. In England during 2011/12, there were 72,400 hospital admissions for angina and 50,708 for myocardial infarction.
Sector: Initiated in secondary care.
Implications: Long term management of ACS includes the use of aspirin and another antiplatelet agent (clopidogrel, prasugrel or ticagrelor). Rivaroxaban 2.5mg twice daily is licensed for use in combination with aspirin alone or with aspirin plus clopidogrel or ticlopidine. Few patients over 75 years of age were included in the ATLAS study.
Financial: Cost will be in addition to existing therapy; price of 2.5mg tablets is currently uncertain.
Likely commissioning route: CCG. PbR: HRG included.
Pharmacology: Factor Xa inhibitor.
Efficacy: The published PIII ATLAS ACS 2 TIMI 51 trial (n=15,526) compared rivaroxaban with placebo in patients
hospitalised with ACS, who were also receiving aspirin and a thienopyridine (clopidogrel or ticlodipine). The 2-year event rate for the primary outcome, a composite of death from cardiovascular (CV) causes, myocardial infarction or stroke, was reduced in patients on rivaroxaban 2.5mg or 5mg twice daily vs. placebo (8.9% vs.10.7%, HR 0.84, p=0.008). Rivaroxaban 2.5mg reduced CV death rate (p=0.002) and death from any cause (p=0.002); a survival benefit was not seen with 5mg.
Safety: See prescribing information. The rate of major bleeding unrelated to CABG was increased with rivaroxaban
compared to placebo in the above trial (2.1% vs. 0.6%, p<0.001), but the risk of fatal bleeding was similar.
Rivaroxaban oral
Xarelto
Bayer
Indication:
Prevention of stent thrombosis in acute
coronary syndrome (ACS).
Current status:
PIII in EU.
Not approved in US Jun 2013.
Predicted UK licence extension:
2014
National guidance:
NICE: ACS pathway, unstable angina &
NSTEMI, myocardial infarction with ST-segment elevation.
SIGN: ACS.
Reviews: None.
Target population: In 2011-12 there were 53,567 admissions in England for balloon angioplasty and insertion of stent into a coronary artery.
Sector: Initiated in secondary care.
Implications: First of the new oral anticoagulants to seek a licence for this indication. Familiarity with the drug may increase willingness to use.
Financial: Rivaroxaban is added to standard therapy for ACS, so cost will also be additive.
Likely commissioning route: CCG. PbR: HRG included.
Pharmacology: Factor Xa inhibitor.
Efficacy: A published, pre-specified sub-group analysis of a PIII trial (sub-group n=9,631) compared twice daily rivaroxaban (2.5mg or 5.0mg) with standard care (aspirin with or without a thienopyridine) in patients with ACS who had at least one stent inserted. There was no difference in the rate of definite stent thrombosis (1.0% vs.1.3%, p=ns). The pooled rate of definite or probable stent thrombosis was lower with rivaroxaban (1.5% vs. 1.9%, p=0.017).
Safety: See medicines.org.uk.
UKMi September 2013 Solely for use within the NHS and not for commercial use. page 15 No responsibility is accepted for the content of documents derived from this original publication.
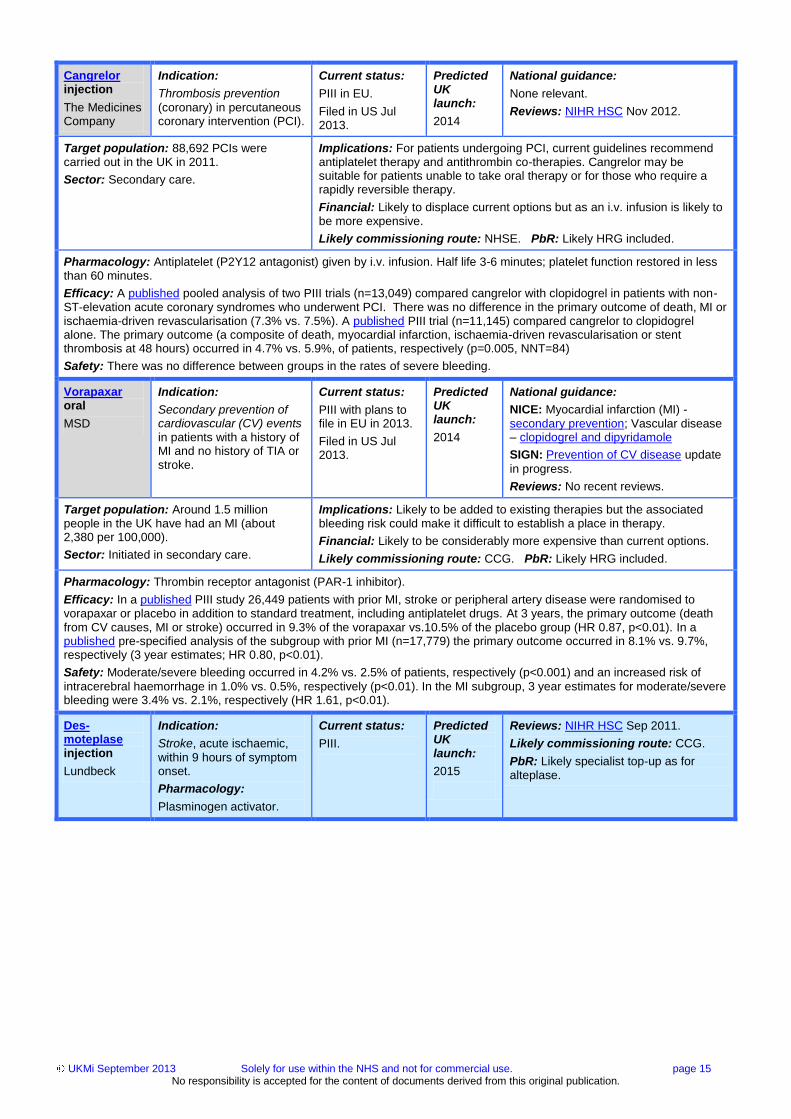
Cangrelor injection
The Medicines Company
Indication:
Thrombosis prevention
(coronary) in percutaneous coronary intervention (PCI).
Current status:
PIII in EU.
Filed in US Jul 2013.
Predicted UK launch:
2014
National guidance:
None relevant.
Reviews: NIHR HSC Nov 2012.
Target population: 88,692 PCIs were carried out in the UK in 2011.
Sector: Secondary care.
Implications: For patients undergoing PCI, current guidelines recommend antiplatelet therapy and antithrombin co-therapies. Cangrelor may be suitable for patients unable to take oral therapy or for those who require a rapidly reversible therapy.
Financial: Likely to displace current options but as an i.v. infusion is likely to be more expensive.
Likely commissioning route: NHSE. PbR: Likely HRG included.
Pharmacology: Antiplatelet (P2Y12 antagonist) given by i.v. infusion. Half life 3-6 minutes; platelet function restored in less than 60 minutes.
Efficacy: A published pooled analysis of two PIII trials (n=13,049) compared cangrelor with clopidogrel in patients with non-ST-elevation acute coronary syndromes who underwent PCI. There was no difference in the primary outcome of death, MI or ischaemia-driven revascularisation (7.3% vs. 7.5%). A published PIII trial (n=11,145) compared cangrelor to clopidogrel alone. The primary outcome (a composite of death, myocardial infarction, ischaemia-driven revascularisation or stent thrombosis at 48 hours) occurred in 4.7% vs. 5.9%, of patients, respectively (p=0.005, NNT=84)
Safety: There was no difference between groups in the rates of severe bleeding.
Vorapaxar oral
MSD
Indication:
Secondary prevention of cardiovascular (CV) events in patients with a history of MI and no history of TIA or stroke.
Current status:
PIII with plans to file in EU in 2013.
Filed in US Jul 2013.
Predicted UK launch:
2014
National guidance:
NICE: Myocardial infarction (MI) -
secondary prevention; Vascular disease – clopidogrel and dipyridamole
SIGN: Prevention of CV disease update
in progress.
Reviews: No recent reviews.
Target population: Around 1.5 million people in the UK have had an MI (about 2,380 per 100,000).
Sector: Initiated in secondary care.
Implications: Likely to be added to existing therapies but the associated bleeding risk could make it difficult to establish a place in therapy.
Financial: Likely to be considerably more expensive than current options.
Likely commissioning route: CCG. PbR: Likely HRG included.
Pharmacology: Thrombin receptor antagonist (PAR-1 inhibitor).
Efficacy: In a published PIII study 26,449 patients with prior MI, stroke or peripheral artery disease were randomised to vorapaxar or placebo in addition to standard treatment, including antiplatelet drugs. At 3 years, the primary outcome (death from CV causes, MI or stroke) occurred in 9.3% of the vorapaxar vs.10.5% of the placebo group (HR 0.87, p<0.01). In a published pre-specified analysis of the subgroup with prior MI (n=17,779) the primary outcome occurred in 8.1% vs. 9.7%, respectively (3 year estimates; HR 0.80, p<0.01).
Safety: Moderate/severe bleeding occurred in 4.2% vs. 2.5% of patients, respectively (p<0.001) and an increased risk of
intracerebral haemorrhage in 1.0% vs. 0.5%, respectively (p<0.01). In the MI subgroup, 3 year estimates for moderate/severe bleeding were 3.4% vs. 2.1%, respectively (HR 1.61, p<0.01).
Des-moteplase injection
Lundbeck
Indication:
Stroke, acute ischaemic,
within 9 hours of symptom onset.
Pharmacology:
Plasminogen activator.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: NIHR HSC Sep 2011.
Likely commissioning route: CCG.
PbR: Likely specialist top-up as for alteplase.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 16 No responsibility is accepted for the content of documents derived from this original publication.
Lomitapide oral
Lojuxta
Aegerion Pharma-ceuticals
Indication:
Hypercholesterolaemia,
homozygous familial (HoFH).
Current status:
Licensed in EU Aug 2013.
Predicted UK launch:
2013
National guidance:
NICE: Familial hypercholesterolaemia:
guideline; Cardiovascular disease prevention: commissioning guide.
SIGN: Prevention of cardiovascular
disease - update in progress.
Reviews: No recent reviews.
Target population: HoFH is rare, with an
incidence of about one case per million people.
Sector: Secondary care.
Implications: Lomitapide may be an option for patients with HoFH with an
inadequate response to current therapy. Genetic confirmation of HoFH should be obtained prior to starting therapy. Treatment may reduce the requirement for LDL apheresis in some patients.
Financial: Likely to be very expensive, but may reduce need for LDL apheresis. US price is around $25,000/month.
Likely commissioning route: CCG. PbR: Likely specified high cost drug.
Pharmacology: Microsomal triglyceride transfer protein inhibitor (first-in-class) given orally once daily.
Efficacy: In a published PIII open-label study (n=29) lomitapide combined with a low-fat diet was added to standard therapy, with or without apheresis. The mean reduction in LDL cholesterol (LDL-C) from baseline was 50% at 26 weeks (primary outcome), 44% at 56-weeks and 38% at 78-weeks (p<0.01 for all comparisons vs. baseline). Some patients were able to reduce or discontinue LDL apheresis.
Safety: Hepatotoxicity has been reported and regular liver function testing is advised. Gastrointestinal adverse effects are common.
Evolcumab injection
Amgen
Indication:
Hyperlipidaemia.
Pharmacology:
Monoclonal antibody -PCSK9 inhibitor.
Current status:
PIII.
Predicted launch:
2015
Reviews: NIHR HSC Mar 2013.
Likely commissioning route: CCG.
PbR: Likely specified high cost drug.
Alirocumab injection
Sanofi
Indication:
Hypercholesterolaemia –
third line.
Pharmacology:
Monoclonal antibody - PCSK9 inhibitor.
Current status:
PIII.
Predicted UK launch:
2016
Reviews: NIHR HSC Dec 2012.
Likely commissioning route: CCG.
PbR: Likely specified high cost drug.
Riociguat oral
Adempas
Bayer
Indication:
Pulmonary arterial hypertension (PAH) and chronic thromboembolic pulmonary hypertension (CTEPH)
Current status:
Filed in EU Feb 2013.
Recommended for approval in the US Aug 2013.
Predicted UK launch:
2014
National guidance:
None relevant.
Reviews: No recent reviews.
Target population: 7,000 patients attended
specialist PH centres in the UK in 2012, of whom 88% had a final diagnosis. Among those with a diagnosis 47% had PAH and 19% CTEPH, equating to 2,895 and 1,170 patients, respectively.
Sector: National Pulmonary Hypertension Service (see commissioning policy statement).
Implications: Riociguat will be an additional option for PAH and CTEPH.
Current options include prostacyclins, endothelin antagonists and phosphodiesterase inhibitors. Riociguat will be the first treatment specifically licensed for CTEPH.
Financial: Likely to be expensive and as a further treatment option will be
additive to current costs.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: Guanylate cyclase stimulant (first-in-class).
Efficacy: PAH. The published 12-week, PIII PATENT-1 study compared individually titrated riociguat with placebo in 443 patients with symptomatic PAH. Riociguat improved the primary outcome of 6-minute walking distance (6-MWD) by 36 meters (p<0.01) vs. placebo. In patients that reached one year of treatment in the long-term extension trial PATENT-2 the improvement in 6-MWD was 48 meters.
CTEPH. The 16-week, published PIII CHEST-1 study compared individually titrated riociguat with placebo in 261 patients with CTEPH or persistent/recurrent PH after surgery. Riociguat improved the primary outcome of 6-minute walking distance by 46 meters (p<0.01) vs. placebo. After one year of treatment in the CHEST-2 extension trial the improvement in 6-MWD was 48 meters.
Safety: To date no serious adverse effects have been reported.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 17 No responsibility is accepted for the content of documents derived from this original publication.
Serelaxin injection
Novartis
Indication:
Acute heart failure (AHF) –
decompensated.
Pharmacology:
Recombinant human relaxin-2, a peptide hormone.
Current status:
Filed in EU Dec 2012.
Predicted launch:
Uncertain.
Reviews: NIHR HSC Jul 2012.
Likely commissioning route: CCG.
PbR: Likely HRG included.
Defibrotide injection
Defitelio
Gentium
Indication:
Hepatic veno-occlusive disease (VOD) - treatment
in haematopoietic stem-cell transplant (HSCT).
Current status:
Recommended for approval in EU Jul 2013 with orphan status.
Predicted UK launch:
2013
National guidance:
None relevant.
Reviews: NIHR HSC Aug 2011, LNDG
due TBC.
Target population: VOD is a leading cause
of morbidity and mortality after HSCT. Without treatment 85% of those with severe VOD die within 100 days of HSCT.
Sector: Secondary or tertiary care.
Implications: Supportive care is the current treatment option. Defibrotide will
be the first specific therapy for VOD.
Financial: Likely to be expensive. Based on a dose of 25mg/kg/day, current named patient cost is around £40,000 for 21 days treatment.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: Cytokine modulator given every 6 hours for at least 21 days.
Efficacy: In a PIII trial (n=134) in patients with severe VOD and multi-organ failure, 24% in the defibrotide group achieved a
complete response at 100 days (primary outcome) vs. 9% in the historical control group (p<0.02, NNT=7). Mortality rate at day 100 (secondary outcome) was 62% vs. 75%, respectively, (p>0.05). An EMA analysis of US patient registry data showed that patients with severe VOD who received defibrotide plus standard care had better outcomes, including a higher survival rate after 100 days following transplantation, than those given standard care alone.
Safety: No safety concerns have been reported to date, with the frequency of adverse events comparable to control.
Clevidipine oral
Cleviprex
The Medicines Company
Indication:
Hypertension, perioperative.
Current status:
Licensed in UK Nov 2011 – see prescribing information.
Predicted UK launch:
2014
National guidance:
None relevant.
Reviews: No recent reviews.
Target population: Perioperative
hypertension may affect 25% of hypertensive patients undergoing surgery.
Sector: Secondary care.
Implications: Clevidipine is one of only two drugs (the other being esmolol)
specifically licensed for the management of perioperative hypertension.
Financial: Likely to be more expensive than available generic options.
Likely commissioning route: CCG. PbR: Likely HRG included.
Pharmacology: Ultra short-acting dihydropyridine calcium channel antagonist given by i.v. infusion.
Efficacy: Pooled results from three open-label PIII studies (ECLIPSE 1, 2 & 3) are published. Among patients undergoing cardiac surgery randomised to clevidipine, glyceryl trinitrate, sodium nitroprusside or nicardipine (n=1,512), there was no difference in primary outcome events (death, MI, stroke or renal dysfunction at 30 days) between the clevidipine group and the pooled comparator group.
Safety: See medicines.org.uk.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 18 No responsibility is accepted for the content of documents derived from this original publication.
BNF 3. Respiratory system
Indacaterol/ glycopyrron-ium inhaler
Ultibro Breezhaler
Novartis
Indication:
Chronic obstructive pulmonary disease (COPD).
Current status:
Recommended for approval in EU Jul 2013.
Predicted UK launch:
2013
National guidance:
NICE: COPD – clinical guideline,
commissioning guide, quality standard.
Reviews: NIHR HSC Aug 2011.
Target population: An estimated 3 million people in the UK are affected by COPD. The rate of COPD in the population is estimated at between 2% and 4%; the diagnosed prevalence is 1.5%.
Sector: Secondary and primary care.
Implications: The first combination inhaler to contain a long-acting muscarinic antagonist (LAMA) for use when maintenance long-acting beta agonist (LABA) is insufficient and an inhaled corticosteroid is not suitable.
Financial: Likely to be similar to other combination products.
Likely commissioning route: CCG. PbR: Likely HRG included.
Pharmacology: Once daily LABA and LAMA combination as a capsule for inhalation.
Efficacy: In the published PIII SHINE trial 2,144 patients were randomised to indacaterol/glycopyrronium, indacaterol, glycopyrronium, tiotropium or placebo. For the primary outcome of trough FEV1 at week 26, the difference between the combination and indacaterol alone was 0.07L, (p<0.01) and 0.09L vs. glycopyrronium (p<0.01). In the published PIII ILLUMINATE trial (n=523) indacaterol/ glycopyrronium was compared to salmeterol/fluticasone combination. At week 26, FEV1 (area under curve) at 12 hours was higher with indacaterol/glycopyrronium (difference 0.138L, p<0.0001).
Safety: In a 52-week safety study, ENLIGHTEN (n=339) the most frequent adverse event was COPD exacerbation (28.0%
vs. 25.7% in placebo group).
Umeclidinium inhaler
Espanda
GlaxoSmith-Kline
Indication:
Chronic obstructive pulmonary disease (COPD).
Current status:
Filed in EU Apr 2013.
Predicted UK launch:
2014
National guidance:
NICE: As for indacaterol/
glycopyronnium above.
Reviews: None.
Target population: As for Indacaterol/
glycopyronnium above.
Sector: Secondary and primary care.
Implications: Umeclidinium will complete with aclidinium, glycopyrronium
and tiotropium. The place of long-acting muscarinic antagonists (LAMAs) is described in the NICE COPD guideline.
Financial: Likely to be similar to other long-acting bronchodilators.
Likely commissioning route: CCG. PbR: Likely HRG included.
Pharmacology: A once-daily LAMA formulated as a dry powder inhaler administered once daily.
Efficacy: Two on-going PIII trials of 600 patients each (one and two) involve the addition of once daily umeclidinium (62.5mcg or 125mcg) or placebo to twice daily fluticasone/salmeterol (250/50mcg) over 12 weeks. The primary outcome is change from baseline in trough FEV1 at day 85. A 12-week PIII trial with the same outcome has compared umeclidinium 62.5mcg or 125mcg to placebo in 206 patients. Significant improvements were shown in mean change from baseline in trough FEV1 for 62.5mcg (127ml) and 125mcg (152ml) vs. placebo.
Safety: A PIII 52-week study is evaluating safety and tolerability.
Umeclidinium/vilanterol inhaler
GlaxoSmith-Kline
Indication:
Chronic obstructive pulmonary disease (COPD).
Current status:
Filed in EU Jan 2013.
Predicted UK launch:
2014
National guidance:
As for indacaterol/ glycopyronnium above.
Reviews: NIHR HSC Feb 2012.
Target population: As for indacaterol/ glycopyronnium above.
Sector: Secondary and primary care.
Implications: A long-acting muscarinic antagonist (LAMA) and long-acting beta agonist (LABA) combination is not yet available in a single inhaler.
Financial: Likely to be similar to other combination products.
Likely commissioning route: CCG. PbR: Likely HRG included.
Pharmacology: A once-daily dry powder inhaler containing a LAMA and a LABA.
Efficacy: In four 24-week studies the primary outcome was trough FEV1 at day 169. In a PIII study (n=871) the difference between tiotropium and umeclidinium/vilanterol (UMEC/VI) 125/25mcg was 74ml (p<0.01) and 60ml vs. UMEC/VI 62.5/25mcg (p=0.02). In another PIII study (n=846), both doses of UMEC/VI were more effective than tiotropium by 88 to 90ml (p<0.01). In a third PIII study (n=1,537) UMEC/VI 62.5/25mcg was more effective than placebo by 167ml (p<0.01) and in a fourth PIII study (n=1,493) UMEC/VI 125/25mcg was better than placebo by 238ml (p<0.01).
Safety: In the above studies, cardiovascular adverse events were seen in 6 to 11% of patients on UMEC/VI.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 19 No responsibility is accepted for the content of documents derived from this original publication.
Budesonide/ formoterol inhaler
Bufomix Easyhaler
Orion Pharma
Indication:
Asthma.
Current status:
Filed in the EU Apr 2013.
Predicted UK launch:
2014
National guidance:
NICE: Quality standard.
SIGN: British guideline on the
management of asthma.
Reviews: None.
Target population: At least 1 in 10 children and 1 in 12 adults have asthma in the UK.
Sector: Secondary and primary care.
Implications: Bufomix will compete with Seretide and Symbicort.
Financial: Likely to be similar to other dry powder inhalers (DPIs).
Likely commissioning route: CCG. PbR: Likely HRG included.
Pharmacology: Dry powder inhaler (DPI) containing a corticosteroid and long-acting beta agonist (LABA).
Efficacy: A PI/II study (n=87), has evaluated the bioequivalence of the Easyhaler to Symbicort Turbohaler.
Safety: For adverse effects of budesonide/formoterol DPI, see medicines.org.uk.
Masitinib oral
AB Science
Indication:
Asthma, severe persistent.
Pharmacology:
Tyrosine kinase inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: NIHR HSC Sep 2012.
Likely commissioning route: NHSE.
PbR: Likely specified high cost drug.
Nalfurafine injection
Winfuran
Fresenius Medical Care
Indication:
Pruritus, uraemic dialysis-related.
Current status:
Filed in EU Aug 2012 with orphan status.
Predicted UK launch:
2013
National guidance:
None relevant.
Reviews: None.
Target population: In the EU uraemic
pruritus affects about 3.5 per million people. Data from 2003-2004 indicates about 50% of patients on haemodialysis in the UK have moderate to extreme pruritus.
Sector: Renal services are a specialised service.
Implications: No other treatments are specifically licensed for uraemic
pruritus. Options include gabapentin and UVB phototherapy.
Financial: Likely to be more expensive than off-label use of oral agents.
Likely commissioning route: NHSE. PbR: Likely HRG included.
Pharmacology: Kappa opioid agonist.
Efficacy: A published meta-analysis reviewed data from 144 patients on haemodialysis with severe, uncontrolled pruritus. Patients received nalfurafine or placebo by i.v. infusion 3 times a week after haemodialysis. A 100-mm visual analogue scale was used to measure the “worst itching” during the previous 12 hours. At week 2, a mean difference of 9.53mm was found between nalfurafine and placebo (p<0.03). 36% on nalfurafine achieved ≥50% decrease from baseline in worst itching vs. 14% on placebo (p<0.03). Safety: The meta-analysis found adverse events to be similar to placebo.
Omalizumab injection
Xolair
Novartis
Indication:
Urticaria, chronic idiopathic
or spontaneous (CIU/CSU) - second line.
Current status:
PIII.
Predicted UK licence extension:
2014
National guidance:
None relevant.
Reviews: NIHR HSC Sep 2012.
Target population: In the UK, the point
prevalence of chronic urticaria is 0.1-0.51%, of which up to 50% of cases are idiopathic (50-250 per 100,000 people). First-line therapy is effective in <50% of patients.
Sector: Secondary care.
Implications: Omalizumab will be a second-line option for CIU/CSU
refractory to H1-antihistamines. It will provide an alternative option to off-label leukotriene receptor- and H2-receptor antagonists.
Financial: Current cost of omalizumab is £256 for 150mg; there will be additional administration costs.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: Monoclonal antibody – IgE receptor antagonist given by s.c injection every four weeks.
Efficacy: A published PIII trial (n=323) compared omalizumab 75mg, 150mg, or 300mg (every 4 weeks for 12 weeks) with
placebo in symptomatic patients with CIU despite H1-antihistamine therapy. The primary outcome was change from baseline to week 12 in a weekly itch-severity score (ranging from 0 to 21). At week 12, the mean reduction from baseline was 5.9 in the 75mg group (p=0.46), 8.1 for 150mg (p=0.01) and 9.8 for 300mg (p<0.01) vs. 5.1 for placebo. In a published PIII trial in 336 patients with CIU/CSU the mean reduction in itch-severity score from baseline at week 12 was 8.6 in the 300mg group vs. 4.0 for placebo (p<0.01).
Safety: See medicines.org.uk.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 20 No responsibility is accepted for the content of documents derived from this original publication.
Ataluren oral
Genzyme
Indication:
Cystic fibrosis (CF),
patients with nonsense mutation (nmCF).
Pharmacology:
CF transmembrane conductance regulator stimulant.
Current status:
PIII in EU with orphan status.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Likely specified high cost drug.
Lumacaftor oral
Vertex
Indication:
Cystic fibrosis, in
combination with ivacaftor in homozygous F508del patients.
Pharmacology:
CF transmembrane conductance regulator stimulant.
Current status:
PIII in EU, fixed dose combination product also in PIII trials.
Breakthrough therapy and orphan drug status in US.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Likely specified high cost drug.
BNF 4. Central nervous system
Loxapine inhalation
Adasuve
Grupo Ferrer
Indication:
Acute agitation associated with schizophrenia or bipolar disorder.
Current status:
Licensed in EU Feb 2013 – see prescribing information.
Predicted UK launch:
2014
National guidance:
NICE: Clinical guidelines: schizophrenia,
bipolar disorder. Commissioning guide: schizophrenia.
SIGN: Schizophrenia, bipolar disorder.
Reviews: RDTC Jun 2013, LNDG Feb 2013.
Target population: In England there are
about 755 people with schizophrenia and 865 with bipolar disorder per 100,000 people. More than 90% of people with either condition will experience agitation in their lifetime, with an average of 11 to 12 episodes of acute agitation each year.
Sector: Secondary care.
Implications: Inhaled administration is less invasive than i.m. injection and
may be preferred by some patients.
Financial: Likely to be more expensive than oral and i.m. alternatives.
Likely commissioning route: CCG. PbR: Likely HRG included.
Pharmacology: Dopamine D2 and serotonin 5-HT2A antagonist given by single-dose inhaler.
Efficacy: Schizophrenia. A published PIII trial (n=344) compared up to 3 doses of loxapine 4.5 or 9.1mg with placebo in agitated in-patients with schizophrenia. At 2-hours post first dose the change from baseline in Positive and Negative Syndrome Scale–Excited Component (PANSS-EC) was -8.1, -8.6 and -5.5, respectively (both p<0.01 vs. placebo).
Bipolar. In a published PIII trial in in-patients with bipolar I associated agitation (n=314), change from baseline in PANSS-EC score 2 hours after the first dose was -8.1 with 4.5mg, -9.0 with 9.1mg and -4.9 with placebo (both p<0.01 vs. placebo).
Safety: See prescribing information. Severe respiratory effects (bronchospasm) are possible.
Lurasidone oral
Latuda
Takeda
Indication:
Schizophrenia.
Current status:
Filed in the EU Oct 2012.
Launched in US see prescribing information.
Predicted UK launch:
2013
National guidance:
NICE: Schizophrenia - Clinical guideline,
commissioning guide.
SIGN: Schizophrenia.
Reviews: NICE Evidence summary Apr
2013.
Target population: In England there are about 800 per 100,000 people with schizophrenia.
Sector: Initiated in secondary care.
Implications: Lurasidone will be an additional treatment option alongside existing antipsychotics. A lower incidence of weight gain may be attractive.
Financial: Likely to be more costly than existing atypical antipsychotics.
Likely commissioning route: CCG. PbR: Likely HRG included.
Pharmacology: Dopamine and serotonin receptor antagonist.
Efficacy: In a published PIII trial, 478 hospitalised patients received lurasidone (40mg or 120mg), olanzapine or placebo. Improvement in the primary outcome of change from baseline to week 6 in the Positive and Negative Syndrome Scale (PANSS) total score was greater with lurasidone 40mg (-25.7, p=0.002), lurasidone 120mg (-23.6, p=0.022) and olanzapine (-28.7, p<0.001) vs. placebo (-16.0). Lurasidone and olanzapine were not directly compared.
Safety: In a published safety trial (n=621) the frequency of adverse events with lurasidone was similar to risperidone, but fewer patients experienced increased weight (9.3% vs. 19.8%).

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 21 No responsibility is accepted for the content of documents derived from this original publication.
Liraglutide injection
Victoza
Novo Nordisk
Indication:
Obesity.
Current status:
PIII.
Predicted UK licence extension:
2014
National guidance:
NICE: Obesity guidelines.
SIGN: Obesity.
Reviews: No recent reviews.
Target population: In 2011, 24% of men and 26% of women (>16 years) were classed obese (BMI ≥30kg/m
2); 41% of men and 33%
of women were overweight (BMI 25 to <30kg/m
2).
Sector: Initiated in secondary care with continued use in primary care.
Implications: It is likely liraglutide injection will be preferentially used in overweight patients with diabetes. It will have the advantage over exenatide which, although causes weight loss, is not specifically licensed for obesity. The liraglutide dose for obesity is much higher than for diabetes.
Financial: Based on a 3mg daily dose current cost of liraglutide is about £183/month vs. £32/month for orlistat 120mg 3 times a day.
Likely commissioning route: CCG. PbR: HRG included.
Pharmacology: Glucagon-like peptide analogue given by daily s.c. injection.
Efficacy: A published PIII study (n=422) compared liraglutide 3mg with placebo over 56 weeks following a 12-week low-calorie dietary run-in. Mean reduction in body weight was -6.2% for liraglutide vs. -0.2% for placebo (p<0.01). A ≥5% reduction in body weight was achieved by 50.5% vs. 21.8% of patients, respectively (p<0.01). A 20-week published PII study (n=564) compared liraglutide 1.2, 1.8, 2.4 or 3mg with placebo and orlistat 360mg/day. Mean weight loss with liraglutide ranged from 4.8 - 7.2kg vs. 2.8kg with placebo and 4.1kg with orlistat (p=0.003 for liraglutide 2.4 mg vs. orlistat and p<0.0001 for liraglutide 3.0 mg vs. orlistat). In a published extension of this study, patients receiving liraglutide (2.4mg or 3mg pooled) for two years lost 3.0kg more than those on orlistat (p<0.01).
Safety: See medicines.org.uk.
Dextro-methorphan/ quinidine oral
Nuedexta
Jenson
Indication:
Pseudobulbar affect (PBA).
Current status:
Licensed in EU Jun 2013 – see prescribing information.
Predicted UK launch:
2014
National guidance:
NICE: Pathways: stroke, dementia;
Clinical guidelines: multiple sclerosis, stroke rehabilitation, dementia, Parkinson’s disease; Quality standard: dementia
Reviews: None.
Target population: PBA can develop in several neurological diseases or following brain injury. The estimated prevalence of PBA is up to 500 per 100,000 people, of whom about 14 per 100,000 will have amyotrophic lateral sclerosis (ALS) or multiple sclerosis (MS).
Sector: Adult specialist neurosciences are a
specialised service.
Implications: First drug licensed for this indication. Confirmation of diagnosis is required before treatment as use in other emotional lability conditions would be off-label. This may increase referrals to specialist neurosciences. Although the indication is for treatment of PBA due to any cause efficacy has only been studied in those with ALS or MS.
Financial: Likely to be considerably more expensive than unlicensed alternatives (SSRIs, TCAs, levodopa, amantadine and thyrotropin-releasing hormone).
Likely commissioning route: NHSE. PbR: Likely HRG included.
Pharmacology: Dextromethorphan is a sigma-1 receptor agonist and NMDA antagonist. Quinidine is a CYP2D6 inhibitor,
which increases plasma levels of dextromethorphan.
Efficacy: A published 12-week PIII trial (n=326) compared dextromethorphan plus quinidine (30/10mg (DMq-30) or 20/10mg (DMq-20) twice daily) with placebo in ALS and MS patients with clinically significant PBA. The primary outcome of PBA-episode daily rate was 46.9% lower for DMq-30 and 49.0% lower for DMq-20 vs. placebo (p<0.01 for both).
Safety: No safety concerns are reported to date, but patients with cardiovascular disorders were excluded from studies.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 22 No responsibility is accepted for the content of documents derived from this original publication.
BNF 5. Infections
Tobramycin solution for inhalation
Vantobra
Pari Pharma
Indication:
Cystic fibrosis (CF)
associated respiratory tract infections.
Current status:
Filed in EU Nov 2012 with orphan status.
Predicted UK launch:
2013
National guidance:
NICE: CF (pseudomonas lung infection).
Reviews: None.
Target population: CF affects over 8,500 people in the UK. In 2008, 39.4% were found to be chronically infected with P. aeruginosa;
19.6% of these used nebulised tobramycin.
Sector: Secondary care, adult and paediatric specialist service.
Implications: The eFlow nebuliser system allows delivery of high concentration/low volume with shorter nebulisation time.
Financial: The current cost of 28-days therapy with Bramitob or TOBI nebuliser solutions is £1,187. Vantobra is likely to be competitive.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: Aminoglycoside antibiotic administered via the eFlow nebuliser delivery system.
Efficacy: A 28-day, PII study (n=78), compared Vantobra 100 (150mg/1.5mL) administered twice daily via an investigational eFlow nebuliser system with TOBI (tobramycin 300mg/5mL) delivered via the PARI LC PLUS nebuliser. The primary outcome was tobramycin serum level as a surrogate safety measure. However, inhalation time was also assessed with the average inhalation time being 4-4.5 minutes for Vantobra vs. 16-17 minutes for TOBI.
Safety: Maximum tobramycin serum levels were lower than recommended safety thresholds.
Bedaquiline oral
Situro
Janssen-Cilag
Indication:
Tuberculosis (TB), multi-
drug resistant (MDR).
Current status:
Filed in EU Aug 2012.
Licensed in US - see prescribing information.
Predicted UK launch:
2013
National guidance:
NICE: Tuberculosis pathway.
WHO interim guidance on the use of bedaquiline Jun 2013.
Reviews: None.
Target population: Around 9,000 cases of TB are reported each year in the UK. Most occur in major cities, particularly London. In 2011, there were 431 reports of MDR-TB, a 26% increase from 2010.
Sector: Secondary care.
Implications: Bedaquiline will be used in addition to second-line options. In the US it is only indicated when other options are not available. WHO recommend it should only be used when an effective regimen with four second-line drugs plus pyrazinamide is not possible or when there is evidence of resistance to any fluoroquinolone in addition to MDR-TB.
Financial: As add on therapy cost will be additional and is likely to be expensive. WHO conclude it would be cost effective in most settings.
Likely commissioning route: NHSE. PbR: Likely HRG included.
Pharmacology: Oral diarylquinoline ATPase inhibitor, first-in-class. Administered by directly observed therapy for 24 weeks.
Efficacy: In a published PII study (n=47), bedaquiline (400mg daily for 2 weeks then 200mg 3 times a week for 6 weeks)
added to background second-line therapy reduced the time to conversion to a negative sputum culture (primary outcome) vs. placebo (p=0.003), and increased the number of patients with conversion (secondary outcome) at week 8 (48% vs. 9%, respectively, NNT=3). In a subsequent PII study (n=160) bedaquiline (24 weeks treatment) decreased time to culture conversion vs. placebo (83 vs. 125 days, respectively, HR 2.44, p<0.0001) and improved culture conversion rates at week 24 vs. placebo (79% vs. 58%, respectively, p=0.008, NNT=5). Using WHO-recommended treatment outcome definitions applied to final 120-week data, 58% vs. 32%, respectively, were defined as cured (p=0.003, NNT=4).
Safety: In the US there are warnings that an increased risk of death (NNH=11) was seen in one study. WHO recommend testing and monitoring for QT prolongation as well as strict conditions for use pending further data to assess risk vs. benefit.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 23 No responsibility is accepted for the content of documents derived from this original publication.
Cobicistat oral
Tybost
Gilead
Indication:
HIV infection, enhancer of
the protease inhibitors atazanavir and darunavir.
Current status:
Recommended for approval in EU Jul 2013.
Predicted UK launch:
2013
National guidance:
British HIV Association (BHIVA) 2012.
Reviews: None.
Target population: In 2012, about 6,000 patients were diagnosed with HIV and about 96,000 were living with HIV with around 25% being undiagnosed.
Sector: Secondary care.
Implications: Cobicistat will be the second enhancer available in the UK, ritonavir being the first. However, unlike ritonavir, cobicistat has no inherent antiretroviral activity.
Financial: Ritonavir cost ranges from about £20 to £78/month. Cost of
cobicistat is likely to be competitive.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: Specific inhibitor of CYP3A without antiretroviral activity.
Efficacy: In a published PII study, 79 patients received cobicistat or ritonavir as enhancers for atazanavir in combination with emtricitabine plus tenofovir. The primary outcome of HIV-1 RNA <50 copies/mL at week 24 was achieved by 84% on atazanavir/cobicistat vs. 86% on atazanavir/ritonavir, and was sustained to week 48 (82% vs. 86%, respectively). Pharmacokinetic analyses showed comparable cobicistat- and ritonavir-boosted atazanavir exposures. An ongoing non-inferiority PIII study (n=692) is assessing cobicistat vs. ritonavir in combination with atazanavir plus tenofovir plus emtricitabine. The primary outcome was achieved in 85% on atazanavir/cobicistat vs. 87% on atazanavir/ritonavir.
Safety: In patents on cobicistat, changes in e-GFR occurred, remained stable through to week 48 and were similar to that seen in patients receiving ritonavir.
Dolutegravir oral
ViiV healthcare UK
Indication:
HIV infection, in combination with other antiretroviral agents.
Current status:
Filed in the EU Dec 2012 and in US with priority review status.
Predicted UK launch:
2013
National guidance:
As for cobicistat above.
Reviews: None.
Target population: As for cobicistat above.
Sector: Secondary care.
Implications: BHIVA guidelines suggest therapy-naïve patients start with two nucleoside reverse transcriptase inhibitors (NRTIs) plus one of the following: a ritonavir-boosted protease inhibitor (PI/r), an NNRTI (non-NRTI) or an integrase inhibitor. BHIVA do not recommend switching to an integrase inhibitor in patients with previous NRTI resistance mutations, historical/ existing mutations associated with NRTI resistance or past virological failure on NRTIs. Once daily dosing with dolutegravir may be an advantage over raltegravir twice daily.
Financial: Cost of raltegravir is £616/month. Elvitegravir is only available in a combination tablet (Stribald). Dolutegravir is likely to be competitive.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: Integrase inhibitor taken once daily.
Efficacy: The primary outcome in various PIII non-inferiority studies assessing dolutegravir plus optimised background
regimen (OBR) was the proportion of patients achieving HIV-1 RNA <50 copies/mL (virological suppression). In the published SPRING-2 study, 822 treatment-naïve patients received daily dolutegravir or twice daily raltegravir, plus OBR. At 48 weeks, 88% vs. 85%, respectively, achieved virological suppression, demonstrating non-inferiority. In the SINGLE study, 833 treatment-naïve patients received dolutegravir plus Kivexa, or Atripla. At 48 weeks, virological suppression was
achieved by 88% vs. 81%, respectively (p=0.003). In the SAILING study in 715 treatment-experienced, integrase-inhibitor naive patients interim 24-week data show virological suppression was achieved in 79% on dolutegravir vs. 70% on raltegravir (p=0.003). Virologic non-response was seen in 15% and 24%, respectively. In the open-label VIKING-3 study in183 treatment-experienced patients with resistance to raltegravir and/or elvitegravir, dolutegravir plus OBR led to a fall in mean HIV-RNA levels by 1.4 log10 copies/mL after 7 days and 63% of patients had virological suppression at 24 weeks.
Safety: Dolutegravir has a similar safety profile to raltegravir.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 24 No responsibility is accepted for the content of documents derived from this original publication.
Sofosbuvir oral
Gilead
Indication:
Hepatitis C viral infection (HCV), genotype 1 to 6 infection.
Current status:
Filed in EU Apr 2013 and in US with accelerated approval and priority review status.
Predicted UK launch:
2014
National guidance:
NICE: HCV- PEG/RBV, HCV genotype 1
- telapravir, boceprevir.
SIGN: Hepatitis C.
Reviews: NIHR HSC Sep 2012.
Target population: There are an estimated
173,000 chronically infected HCV patients in England and Wales; only 91,000 of these are diagnosed. Chronic HCV was the primary cause of 2,967 hospital admissions in England in 2010/11, with 2,688 bed days.
Sector: Secondary care.
Implications: HCV is a major cause of liver transplantation. Patients with
genotype 1 are treated with triple therapy. Sofosbuvir is another option with efficacy shown in HCV genotypes 1-6. It could reduce treatment duration with the advantage of reduced dosing frequency vs. available options.
Financial: Monthly cost of boceprevir is £2,800 and telaprevir is £7,466. Sofosbuvir is likely to be competitive.
Likely commissioning route: NHSE. PbR: Likely specified high cost drug.
Pharmacology: Once daily nucleotide NS5B inhibitor.
Efficacy: The primary outcome of all PIII studies is the proportion of patients achieving a sustained virologic response at 12 weeks (SVR12) after the end of therapy. In the published open-label NEUTRINO study, 90% of 327 treatment-naïve patients with HCV genotypes 1, 4, 5 or 6 treated with sofosbuvir plus peginterferon alfa 2a plus ribavirin (PEG/RBV) achieved a SVR12. In the published FISSION non-inferiority study, 499 patients with genotype 2 or 3 were treated with either sofosbuvir/RBV given for 12 weeks or PEG/RBV given for 24 weeks. SVR12 was 67% in both groups. In the sofosbuvir/RBV group, response rates in patients with genotype 3 were lower than in those with genotype 2 (56% vs. 97%, respectively). In the published PIII POSITRON study in 278 patients with genotypes 2 or 3 for whom treatment with peginterferon was not an option, the SVR12 was 78% in the sofosbuvir/RBV group vs. 0% for placebo (p<0.001). In the published PIII FUSION study in 201 patients who had not had a response to prior interferon treatment, patients received sofosbuvir/RBV for 12 or 16 weeks. The SVR12 was 50% and 73% (p<0.001), respectively. In both studies, response rates were lower in patients with genotype 3 than genotype 2. Sofosbuvir is also in PIII trials in patients co-infected with HIV.
Safety: Adverse events were less frequent with sofosbuvir than with peginterferon. Common adverse effects include headache, fatigue, nausea, and insomnia.
Simeprevir oral
Janssen-Cilag
Indication:
Hepatitis C virus infection (HCV), genotype 1 or 4 in adults with compensated liver disease who are treatment naïve or have failed interferon.
Current status:
Filed in EU Apr 2013.
Predicted UK launch:
2014
National guidance:
As for sofosbuvir above.
Reviews: NIHR HSC - treatment naïve Sep 2012, failed interferon Sep 2012.
Target population: As for sofosbuvir above.
Sector: Secondary care initiated.
Implications: Other oral protease inhibitors for genotype 1 infection are taken twice or three times a day.
Financial: As for sofosbuvir above.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: Once daily NS3/4A protease inhibitor.
Efficacy: The primary outcome of all the following PIII studies is the number of patients achieving a sustained virologic
response at 12 weeks (SVR12) after the end of therapy.
Treatment naïve: In CONCERTO-1, 183 patients received peginterferon alfa-2a plus ribavirin (PEG/RBV) for up to 24 or 48 weeks plus simeprevir or placebo for 12 weeks. SVR12 was achieved by 89% vs. 62%, respectively. In CONCERTO-4, 79 patients received PEG/RBV plus simeprevir for 12 weeks followed by response-guided treatment. SVR12 was 92%. In QUEST-1 (n=394) and QUEST-2 (n=391) patients received simeprevir or placebo for 12 weeks plus interferon-based therapy for 24 or 48 weeks. 80% and 81% of those on simeprevir achieved SVR12, respectively.
Failed interferon: In CONCERTO-2,106 previous non-responders received simeprevir plus PEG/RBV for 12 or 24 weeks, followed by response-guided treatment. SVR12 was achieved by 53 vs. 36% of patients after 12 or 24 weeks. In CONCERTO-3, 49 relapsed patients received simeprevir plus PEG/RBV for 12 weeks, plus PEG/RBV for up to 36 weeks. SVR12 was achieved by 96% of patients. In CONCERTO-4, 79 patients received simeprevir plus PEG/RBV for 12 weeks followed by response-guided treatment. SVR12 in patients who had previously relapsed on interferon-based treatment was 100% and 39% in prior non-responders. In PROMISE, 393 previously relapsed patients received simeprevir or placebo with PEG/RBV for 12 weeks then PEG or RBV for 12 or 36 weeks. 79% of the simeprevir group achieved SVR12. On-going trials include a PIII trial in patients with concomitant HIV-1 infection and the RESTORE trial in those with genotype 4 infection.
Safety: In the PROMISE study, simeprevir was associated with influenza-like illness, rash and itching.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 25 No responsibility is accepted for the content of documents derived from this original publication.
Sofosbuvir/ ledipasvir oral
Gilead
Indication:
Hepatitis C viral infection,
genotype 1.
Pharmacology:
Ledipasvir is a NS5A protein inhibitor and sofosbuvir is a nucleotide NS5B inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Likely specified high cost drug.
Asunaprevir/ daclatasvir oral
Bristol Myers Squibb
Indication:
Hepatitis C virus infection,
genotype 1.
Pharmacology:
Asunaprevir is a NS3 protease inhibitor and daclatasvir is a NS5A inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Likely specified high cost drug.
ABT450/ ritonavir/ ABT267/ ABT333 oral
AbbVie Ltd
Indication:
Hepatitis C virus infection,
genotype 1.
Pharmacology:
ABT 450 is a NS3/4A inhibitor, ABT 267 is a NS5A inhibitor, ABT 333 is a non-nucleoside inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Likely specified high cost drug.
Actoxumab/ bezlo- toxumab injection
MSD
Indication:
Clostridium difficile
infections, prevention of recurrence.
Pharmacology:
Monoclonal antibodies against C difficile-producing toxin A (actoxumab) and toxin B (bezlotoxumab).
Current status:
PIII.
Predicted UK launch:
2016
Reviews: None.
Likely commissioning route: NHSE.
(children and young people) or CCG (adults).
PbR: Likely HRG included.
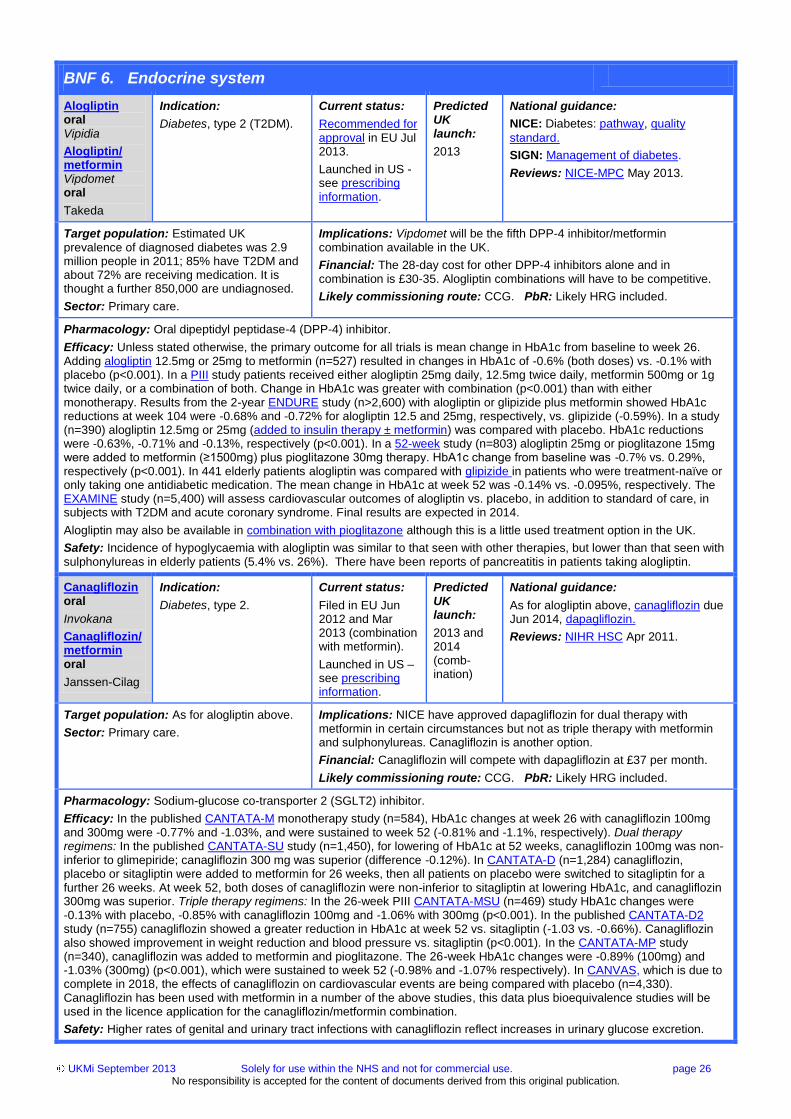
UKMi September 2013 Solely for use within the NHS and not for commercial use. page 26 No responsibility is accepted for the content of documents derived from this original publication.
BNF 6. Endocrine system
Alogliptin oral
Vipidia
Alogliptin/ metformin Vipdomet oral
Takeda
Indication:
Diabetes, type 2 (T2DM).
Current status:
Recommended for approval in EU Jul 2013.
Launched in US - see prescribing information.
Predicted UK launch:
2013
National guidance:
NICE: Diabetes: pathway, quality
standard.
SIGN: Management of diabetes.
Reviews: NICE-MPC May 2013.
Target population: Estimated UK prevalence of diagnosed diabetes was 2.9 million people in 2011; 85% have T2DM and about 72% are receiving medication. It is thought a further 850,000 are undiagnosed.
Sector: Primary care.
Implications: Vipdomet will be the fifth DPP-4 inhibitor/metformin combination available in the UK.
Financial: The 28-day cost for other DPP-4 inhibitors alone and in combination is £30-35. Alogliptin combinations will have to be competitive.
Likely commissioning route: CCG. PbR: Likely HRG included.
Pharmacology: Oral dipeptidyl peptidase-4 (DPP-4) inhibitor.
Efficacy: Unless stated otherwise, the primary outcome for all trials is mean change in HbA1c from baseline to week 26. Adding alogliptin 12.5mg or 25mg to metformin (n=527) resulted in changes in HbA1c of -0.6% (both doses) vs. -0.1% with placebo (p<0.001). In a PIII study patients received either alogliptin 25mg daily, 12.5mg twice daily, metformin 500mg or 1g twice daily, or a combination of both. Change in HbA1c was greater with combination (p<0.001) than with either monotherapy. Results from the 2-year ENDURE study (n>2,600) with alogliptin or glipizide plus metformin showed HbA1c reductions at week 104 were -0.68% and -0.72% for alogliptin 12.5 and 25mg, respectively, vs. glipizide (-0.59%). In a study (n=390) alogliptin 12.5mg or 25mg (added to insulin therapy ± metformin) was compared with placebo. HbA1c reductions were -0.63%, -0.71% and -0.13%, respectively (p<0.001). In a 52-week study (n=803) alogliptin 25mg or pioglitazone 15mg were added to metformin (≥1500mg) plus pioglitazone 30mg therapy. HbA1c change from baseline was -0.7% vs. 0.29%, respectively (p<0.001). In 441 elderly patients alogliptin was compared with glipizide in patients who were treatment-naïve or only taking one antidiabetic medication. The mean change in HbA1c at week 52 was -0.14% vs. -0.095%, respectively. The EXAMINE study (n=5,400) will assess cardiovascular outcomes of alogliptin vs. placebo, in addition to standard of care, in subjects with T2DM and acute coronary syndrome. Final results are expected in 2014.
Alogliptin may also be available in combination with pioglitazone although this is a little used treatment option in the UK.
Safety: Incidence of hypoglycaemia with alogliptin was similar to that seen with other therapies, but lower than that seen with sulphonylureas in elderly patients (5.4% vs. 26%). There have been reports of pancreatitis in patients taking alogliptin.
Canagliflozin oral
Invokana
Canagliflozin/metformin oral
Janssen-Cilag
Indication:
Diabetes, type 2.
Current status:
Filed in EU Jun 2012 and Mar 2013 (combination with metformin).
Launched in US –see prescribing information.
Predicted UK launch:
2013 and 2014 (comb-ination)
National guidance:
As for alogliptin above, canagliflozin due Jun 2014, dapagliflozin.
Reviews: NIHR HSC Apr 2011.
Target population: As for alogliptin above.
Sector: Primary care.
Implications: NICE have approved dapagliflozin for dual therapy with metformin in certain circumstances but not as triple therapy with metformin and sulphonylureas. Canagliflozin is another option.
Financial: Canagliflozin will compete with dapagliflozin at £37 per month.
Likely commissioning route: CCG. PbR: Likely HRG included.
Pharmacology: Sodium-glucose co-transporter 2 (SGLT2) inhibitor.
Efficacy: In the published CANTATA-M monotherapy study (n=584), HbA1c changes at week 26 with canagliflozin 100mg and 300mg were -0.77% and -1.03%, and were sustained to week 52 (-0.81% and -1.1%, respectively). Dual therapy regimens: In the published CANTATA-SU study (n=1,450), for lowering of HbA1c at 52 weeks, canagliflozin 100mg was non-inferior to glimepiride; canagliflozin 300 mg was superior (difference -0.12%). In CANTATA-D (n=1,284) canagliflozin, placebo or sitagliptin were added to metformin for 26 weeks, then all patients on placebo were switched to sitagliptin for a further 26 weeks. At week 52, both doses of canagliflozin were non-inferior to sitagliptin at lowering HbA1c, and canagliflozin 300mg was superior. Triple therapy regimens: In the 26-week PIII CANTATA-MSU (n=469) study HbA1c changes were -0.13% with placebo, -0.85% with canagliflozin 100mg and -1.06% with 300mg (p<0.001). In the published CANTATA-D2 study (n=755) canagliflozin showed a greater reduction in HbA1c at week 52 vs. sitagliptin (-1.03 vs. -0.66%). Canagliflozin also showed improvement in weight reduction and blood pressure vs. sitagliptin (p<0.001). In the CANTATA-MP study (n=340), canagliflozin was added to metformin and pioglitazone. The 26-week HbA1c changes were -0.89% (100mg) and -1.03% (300mg) (p<0.001), which were sustained to week 52 (-0.98% and -1.07% respectively). In CANVAS, which is due to complete in 2018, the effects of canagliflozin on cardiovascular events are being compared with placebo (n=4,330). Canagliflozin has been used with metformin in a number of the above studies, this data plus bioequivalence studies will be used in the licence application for the canagliflozin/metformin combination.
Safety: Higher rates of genital and urinary tract infections with canagliflozin reflect increases in urinary glucose excretion.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 27 No responsibility is accepted for the content of documents derived from this original publication.
Dapagliflozin/metformin oral
AstraZeneca/ Bristol Myers Squibb
Indication:
Diabetes, type 2.
Current status:
Filed in EU Dec 2012.
Predicted UK launch:
2013
National guidance:
NICE: As for alogliptin above,
dapagliflozin.
Reviews: NIHR HSC May 2011.
Target population: As for alogliptin above.
Sector: Primary care.
Implications: NICE has approved use of dapagliflozin as dual therapy with metformin in certain circumstances. The combination product may be more convenient for patients stabilised on the two drugs taken separately.
Financial: Currently UK cost for 28 days treatment with various metformin formulations ranges from around £1.50 to £12; dapagliflozin costs about £37/month. The combination product will have to compete with this.
Likely commissioning route: CCG. PbR: HRG included.
Pharmacology: SGLT2-inhibitor with a biguanide in a once daily formulation.
Efficacy: Dapagliflozin is licensed for use in combination with other glucose-lowering medicines, such as metformin, when
these, together with diet and exercise, do not provide adequate glycaemic control. Bioequivalence studies comparing fixed-dose combination products with individual components have been undertaken.
Safety: See medicines.org.uk.
Exenatide implant
Intarcia therapeutics
Indication:
Diabetes, type 2.
Pharmacology:
Long-acting analogue of glucagon-like peptide 1 (GLP-1) delivered via DUROS device over 3-12 months.
Current status:
PIII trials in EU and US.
Predicted UK launch:
2016
Reviews: None.
Likely commissioning route: CCG.
PbR: HRG included.
Insulin degludec/ insulin aspart injection
Ryzodeg
Novo Nordisk
Indication:
Diabetes, type 1 (T1DM)
and type 2 (T2DM).
Current status:
Licensed in EU Jan 2013. Company plan to launch early 2014.
Predicted UK launch:
2014
National guidance:
As for alogliptin above.
Reviews: NIHR HSC - T1DM, T2DM, Jan 2011.
Target population: As for alogliptin above. About 15% of adults and children with diabetes have T1DM.
Sector: Primary and secondary care.
Implications: In T2DM NICE recommends insulin (starting with human NPH insulin or a long-acting insulin analogue) for patients with HbA1c not controlled with metformin plus sulfonylurea. Ryzodeg will be another option
for those not controlled on oral therapy or basal insulin regimens.
Financial: Cost of 1,500 units of NovoMix 30 is about £30 and of Humulin M3 £15-22. Cost of 1,500 units insulin degludec is £72. Ryzodeg is likely to be more expensive than currently available insulin combinations.
Likely commissioning route: CCG. PbR: HRG included.
Pharmacology: Long-acting basal insulin [degludec, 70%] plus short-acting bolus insulin [aspart, 30%] (IDegAsp).
Efficacy: Unless stated otherwise, in all studies, the primary outcome was HBA1c change at 26 weeks.
T1DM. In the published BOOST-T1 study (n=548) IDegAsp given once-daily with any meal with insulin aspart (IAsp) at remaining meals was non-inferior to once-daily insulin detemir with IAsp at all meals.
T2DM. In BOOST-START 1 (n=530) and BOOST-INTESIFY-BASAL (n=465) IDegAsp demonstrated non-inferiority vs. insulin glargine (IGlar). In the published BOOST: Intensify All trial (n=296), at 26 weeks, mean HbA1c was 7% with IDegAsp vs. 7.3% with IGlar (difference -0.28%, p<0.01).
Safety: See medicines.org.uk. This has not been approved in the US pending further cardiovascular outcomes data.
Insulin inhalation
Afrezza
MannKind Corporation
Indication:
Diabetes, types 1 and 2.
Pharmacology:
Dry-powder formulation of insulin, rapid acting.
Current status:
PIII trials in EU and US.
Predicted UK launch:
2015
Reviews: No recent reviews.
Likely commissioning route: CCG.
PbR: Likely HRG Included.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 28 No responsibility is accepted for the content of documents derived from this original publication.
Bazedoxifene/conjugated estrogens oral
Duavive
Pfizer
Indication:
Postmenopausal osteoporosis and menopausal symptoms.
Current status:
Filed in EU Jul 2012.
Predicted UK launch:
2014
National guidance:
NICE: Osteoporosis pathway.
SIGN: Management of osteoporosis.
Reviews: None.
Target population: It is estimated that more than 2 million women have osteoporosis in England and Wales. After the menopause, the prevalence of osteoporosis increases markedly with age, from about 2% at 50 years of age rising to more than 25% at 80 years.
Sector: Primary care.
Implications: NICE suggests first-line treatment for primary prevention of postmenopausal osteoporosis is a bisphosphonate. Raloxifene (a SERM) is not recommended for primary prevention of osteoporotic fractures but can be used for secondary prevention. Many preparations are available for menopausal symptoms. Bazedoxifene plus conjugated oestrogens (BZA/CE) is another option and, as a single tablet, could be attractive.
Financial: Current 28-day treatment costs range from £1.10 (alendronate
70mg/week) to £17.06 (raloxifene 60mg/day) and £25.60 (strontium ranelate 2g/day). Conjugated oestrogens for HRT cost around £3-6 for 3 months treatment. BZA/CE is likely to be competitive.
Likely commissioning route: CCG. PbR: Likely HRG included.
Pharmacology: Selective oestrogen receptor modulators (SERM) plus oestrogen receptor agonist.
Efficacy: Five PIII Selective Estrogen Menopause and Response to Therapy (SMART) studies have been undertaken, the
results of four are fully published. Endometrial safety and changes in bone mineral density (BMD) are assessed in SMART-1 (n=3,397), SMART-4 (n=1,061) and SMART-5 (n=1,843). In SMART-1, over 24 months, BZA/CE was associated with low rates (<1%) of endometrial hyperplasia and endometrial thicknesses that were similar to placebo. BMD increases seen in all three studies were significantly greater with BZA/CE vs. placebo and in SMART-1, were greater with most doses of BZA/CE vs. raloxifene. In SMART-1 and SMART-2 (n=332) studies, the incidence of hot flushes by week 12 was reduced by 50-85% with BZE/CE vs. 17-50% with placebo (p<0.01). BZA/CE was used in SMART 3 (n=664) to treat vulvar/vaginal atrophy. BZA/CE increased superficial, and decreased parabasal, cells vs. placebo (p<0.01). Vaginal pH and dryness improved with BZA/CE vs. placebo (p≤0.05).
Safety: BZA/CE is associated with low rates (<1%) of endometrial hyperplasia and endometrial thicknesses.
Pasireotide LAR injection
Signifor
Novartis
Indication:
Acromegaly.
Current status:
PIII in EU with orphan status.
Predicted UK launch:
2014
National guidance: None.
Reviews: No recent reviews.
Target population: The UK incidence of acromegaly is about 3 per million; about 3,000 have the condition.
Sector: Secondary care.
Implications: Pasireotide will compete with other somatostatin analogues, pegvisomant and dopamine agonists.
Financial: Current depot therapy includes lanreotide 30mg (£645/month) or octreotide 20mg (£776/ month) for initial therapy, dose and/or frequency adjusted according to response.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: Somatostatin analogue in a long-acting release (LAR) i.m. injection given every 4 weeks.
Efficacy: In the PIII PASPORT-ACROMEGALY study (n=358), pasireotide LAR was compared with octreotide LAR both
given by monthly i.m. injection. At 12 months, 31.3% on pasireotide LAR vs. 19.2% on octreotide LAR (p=0.007) achieved a biochemical response (growth hormone level <2.5mcg/L and normal insulin like growth factor-1). Those who did not initially achieve biochemical control could switch to the other treatment in a 6-month extension phase; 81 switched to pasireotide LAR and 38 to octreotide LAR. A biochemical response was achieved by 21.0% and 2.6%, respectively. A PIII study assessing pasireotide vs. octreotide or lanreotide is ongoing.
Safety: See medicines.org.uk for short-acting formulation. Hyperglycaemia is more common with pasireotide than octreotide.
UKMi September 2013 Solely for use within the NHS and not for commercial use. page 29 No responsibility is accepted for the content of documents derived from this original publication.
Tolvaptan oral
Samsca
Otsuka Pharma-ceuticals
Indication:
Autosomal-dominant polycystic kidney disease (ADPKD)
Current status:
PIII in EU.
Not recommended for approval in US Aug 2013.
Predicted UK licence extension:
2014
National guidance:
NICE: Chronic kidney disease pathway.
SIGN: Diagnosis and management of
chronic kidney disease.
Reviews: NIHR HSC Apr 2012.
Target population: ADPKD has a prevalence of 100-1,300 per 100,000 people (at least 60,000 in the UK). In 2007 polycystic kidney disease accounted for 12.7% of patients receiving renal transplants.
Sector: Secondary care initiated.
Implications: There are currently no therapies that modify the disease course and slow the rate of decline in renal function. Current management options include anti-hypertensives, dialysis and renal transplantation.
Financial: Based on current prices, tolvaptan 60mg/day will cost over £4,100/month.
Likely commissioning route: Uncertain -depending on statge of renal failure. PbR: Specified high cost drug.
Pharmacology: Selective vasopressin V2-receptor antagonist.
Efficacy: In the published PIII TEMPO 3:4 trial (n=1,445) patients received tolvaptan at the highest of three dose regimens
tolerated or placebo. At 3 years, the increase in total kidney volume in the tolvaptan group was 2.8% per year vs. 5.5% per year for placebo (p<0.001). Secondary outcome measures including a composite of time to clinical progression (defined as worsening kidney function, kidney pain, hypertension, and albuminuria) and rate of kidney-function decline favoured tolvaptan (p=0.01 and p<0.001, respectively).
Safety: See medicines.org.uk. In the TEMPO 3:4 trial more patients on tolvaptan had raised liver enzymes. The MHRA has issued a safety warning.
BNF 7. Obstetrics, gynaecology, and urinary-tract disorders
Botulinum A toxin (onabotulinum-toxin A) injection
Botox
Allergan
Indication:
Overactive bladder (OAB), idiopathic in adults who have an inadequate response/are intolerant of antimuscarinic medication.
Current status:
Filed in UK, date uncertain. Recommended for approval in EU (but not UK) Dec 2012.
Launched in US - see prescribing information.
Predicted UK licence extension:
2013
National guidance:
NICE: Lower urinary tract symptoms in
men - pathway, quality standard due Sep 2013; Urinary incontinence in women – guideline, update due Sep 2013, commissioning guide.
SIGN: Urinary incontinence.
Reviews: NICE-MPC Sep 2012.
Target population: The estimated population with OAB for whom antimuscarinic treatment does not give an adequate response is around 0.265%, equating to around 106,000 adults in England.
Sector: Secondary care.
Implications: NICE guidance suggests that botulinum toxin is an option in patients able and willing to self-catheterise, for whom standard therapy with lifestyle changes, bladder retraining and anticholinergic drugs has failed and who might otherwise have been considered for surgical intervention or neuromodulation.
Financial: The current NHS cost of Botox is £138.20 for a 100-unit vial; the cost per patient will be £276.40/year if given twice. This does not include the cost of the procedure.
Likely commissioning route: CCG. PbR: Specified high cost drug.
Pharmacology: Purified neurotoxin complex presented as a single 1,000 unit injection administered as 20 individual 5 unit
injections into the detrusor muscle. The effects of a single injection can last for between 3-10 months.
Efficacy: In a published 12-week PIII trial (n=557) in the EMBARK programme, botulinum A toxin 100 units reduced the primary outcome of daily urinary incontinence episodes vs. placebo (-2.65 vs. -0.87, p<0.001) and 22.9% vs. 6.5% of patients became completely continent (NNT=6). More patients on botulinum A toxin reported a positive response on the treatment benefit scale (primary outcome) vs. placebo (60.8% vs. 29.2%, respectively, p<0.001). Similar results have been noted in another PIII study (n=548) in the EMBARK programme. An on-going, long-term follow-up study (n=750) has completed enrolment. The published UK RELAX study (n=240) reported that 31% of women were continent at 6 months after one botulinum 200 unit injection vs. 12% on placebo (NNT= 5).
Safety: In the PIII trials, 18% of patients had urinary tract infections, 9% had dysuria and 6.5% had urinary retention. NNH
(urinary tract infection/ requirement for self catheterisation) was 5 for botulinum and 8 for placebo.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 30 No responsibility is accepted for the content of documents derived from this original publication.
Collagenase clostridium histolyticum injection
Xiapex
Auxilium
Indication:
Peyronie’s disease (PsD).
Current status:
PIII in EU.
Filed in US in Nov 2012.
Predicted UK licence extension:
2014
National guidance:
NICE: Extracorporeal shock waves for
PsD.
EAU Guidelines on Penile Curvature 2012.
Reviews: None.
Target population: PsD affects around 1% of men; it will improve or resolve spontaneously in about 13%. The average age of onset is in the fifth decade with many cases undiagnosed.
Sector: Secondary care.
Implications: Current therapy incudes oral potassium para-aminobenzoate, intralesional interferon-alpha or verapamil, and surgery.
Financial: Xiapex 900 microgram currently costs £650; much more than interferon-alpha.
Likely commissioning route: CCG. PbR: Specified high cost drug.
Pharmacology: Collagenase stimulant injected into penile plaque twice weekly every 6 weeks for up to 4 treatment cycles, each injection accompanied by penile modelling.
Efficacy: A post-hoc meta-analysis of two identical 52-week PIII studies IMPRESS I and II has been published, each
enrolling over 400 men. Those treated with collagenase had a 34% mean improvement in penile curvature vs. 18% in those on placebo (representing a mean change -17.0 vs. -9.3 degrees, respectively). The mean change in Peyronie’s disease symptom bother score was improved with collagenase treatment (-2.8 vs. -1.8, p=0.004).
Safety: Local treatment site reactions are common and include injection site haematoma, pain and swelling. Across
IMPRESS I and II, 3 cases of corporal rupture and 3 serious penile haematomas occurred.
BNF 8. Malignant disease and immunosuppression
Brain cancer vaccine injection
DCVax-L
Northwest Bio-therapeutics
Indication:
Glioblastoma multiforme, first-line adjuvant therapy.
Pharmacology:
Immunostimulant vaccine manufactured using the patient’s dendritic cells and resected tumour tissue.
Current status:
PIII with orphan status.
Predicted UK launch:
2015
Reviews: No recent reviews.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Afatinib oral
Giotrif
Boehringer Ingelheim
Indication:
Head and neck cancer, squamous cell – locally advanced, recurrent or metastatic - second-line.
Pharmacology:
Tyrosine kinase inhibitor blocking EGFR and HER2.
Current status:
PIII.
Predicted UK licence extension:
2015
Reviews: NIHR HSC Mar 2013.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Sorafenib oral
Nexavar
Bayer
Indication:
Thyroid cancer, differentiated (DTC) – advanced, radioactive-iodine refractory.
Current status:
Filed in EU and US Jul 2013 with priority review in the US.
Predicted UK licence extension:
2014
National guidance:
None relevant.
Reviews: No recent reviews.
Target population: UK incidence of thyroid cancer is 3.5 per 100,000; DTC (papillary and follicular) accounts for 80%. 5-20% of patients develop local or regional recurrences and 10-15% have distant metastases.
Sector: Secondary or tertiary care.
Implications: Options for recurrent or metastatic disease include surgery, radioactive iodine and radiotherapy. Sorafenib will be the first drug licensed for progressive disease.
Financial: This is additional therapy that currently costs £2,980 a month. Median treatment duration in a PII trial was 16.5 months.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally
negotiated.
Pharmacology: Blocks Raf and tyrosine kinases, vascular endothelial and platelet derived growth factor receptors.
Efficacy: In the published PIII DECISION study (n=417), median PFS was 10.8 months with sorafenib vs. 5.8 months with
placebo (HR 0.58, p<0.0001). Median overall survival (OS) had not been reached in either arm. A partial response (PR) was seen in 12.2% and 0.5% of sorafenib and placebo patients, respectively (p<0.0001); 42% and 33% had stable disease (SD) lasting at least 6 months, respectively. In a published PII study (n=31), 59% had a clinical response (25% a PR and 34% SD); 22% had progressive disease. In published long-term results, median PFS was 18 months and median OS was 34.5 months. In a published PII study (n=19), the radiological response rate was 18% and OS 79% at 12 months.
Safety: See medicines.org.uk.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 31 No responsibility is accepted for the content of documents derived from this original publication.
Lenvatinib oral
Eisai
Indication:
Thyroid cancer,
differentiated (DTC) – advanced, radioactive-iodine refractory.
Current status:
PIII with orphan status.
Predicted UK launch:
2014
National guidance:
As for sorafenib above.
Reviews: None.
Target population: As for sorafenib above.
Sector: Secondary or tertiary care.
Implications: Options for recurrent or metastatic disease include surgery, radioactive iodine and radiotherapy. A competitor to twice-daily sorafenib.
Financial: Likely to be similarly priced to sorafenib (£2,980/month).
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: A once-daily, multi-targeted kinase inhibitor of VEGFR1-3, FGFR1-4 and RET tyrosine kinases.
Efficacy: Data from a PII trial (n=58) show an objective clinical response rate of 50%; the rate in patients who received prior VEGFR-directed treatment (n=17) was 41%, in those with no prior VEGFR-directed treatment it was 54%. Median PFS was 12.6 months after a minimum follow-up of 8 months. Results from the placebo-controlled PIII SELECT trial (n=360) are expected in 2013. A PII trial enrolling 104 patients with DTC and medullary TC is expected to complete in Oct 2013.
Safety: In a PII trial, 10% of patients experienced grade 3 diarrhoea, hypertension and proteinuria. Toxicities were manageable by dose reduction in 35% of patients. 23% withdrew from the study due to adverse events.
Cabozantinib oral
Cometriq
Exelixis
Indication:
Thyroid cancer, medullary
(MTC).
Current status:
Filed in EU Dec 2012 with orphan status.
Launched in US - see prescribing information.
Predicted UK launch:
2013
National guidance:
None relevant.
Reviews: NIHR HSC Feb 2012.
Target population: MTC is rare, accounting for 5-8% of all thyroid cancers (about 0.2 per 100,000 people).
Sector: Secondary or tertiary care.
Implications: First-line therapy is thyroidectomy. Cabozantinib may slow disease progression in patients who cannot be managed by surgery alone and will be an alternative to vandetanib.
Financial: Likely to be expensive but may offset other treatment costs. An alternative to vandetanib which costs £5,000 per month.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally
negotiated.
Pharmacology: Tyrosine kinase inhibitor that blocks RET, MET, VEGFR-1, -2 and -3, KIT, TRKB, FLT-3, AXL and TIE-2.
Efficacy: In the published PIII EXAM trial (n=330) progression-free survival (PFS) was 11.2 months with cabozantinib vs. 4.0
months with placebo (HR 0.28, p<0.0001). One-year PFS was 47.3% and 7.2%, respectively; overall response rates were 28% and 0%, respectively (p<0.0001). In a published PI study (n=35), 29% had a partial response to cabozantinib, and 49% had tumour shrinkage of 30% or more. At two years, 30% were progression-free.
Safety: Cabozantinib has been associated with perforations, fistulas, haemoptysis and gastrointestinal haemorrhage.
Afatinib oral
Giotrif
Boehringer Ingelheim
Indication:
Non-small cell lung cancer (NSCLC), advanced with EGFR mutation.
Current status:
Recommended for approval in EU Jul 2013.
Licensed in US - see prescribing information.
Predicted UK launch:
2013
National guidance:
NICE: Lung cancer - pathway, quality
standard; NSCLC - afatinib due May 2014.
SIGN: Lung cancer, update due 2013.
Reviews: No recent reviews.
Target population: UK incidence of advanced NSCLC is 45 per 100,000 people; 25% are able to have first-line therapy. Epidermal growth factor receptor (EGFR) is overexpressed in 10-15% of tumours.
Sector: Secondary care.
Implications: Afatinib will compete with first generation EGFR inhibitors, erlotinib and gefitinib. It is a less complicated and less toxic alternative to i.v. chemotherapy in selected patients.
Financial: PASs are in place for erlotinib and gefitinib for NSCLC. Monthly
list price is £1,600 and £2,000, respectively.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: Tyrosine kinase inhibitor irreversibly blocking epidermal growth factor receptors, including HER2.
Efficacy: In the published global PIII LUX-Lung 3 trial (n=345) comparing first-line afatinib with cisplatin and pemetrexed, median progression-free survival (PFS) was 11.1 vs. 6.9 months, respectively (HR 0.58, p=0.001). In 308 patients with EGFR mutation, median PFS was 13.6 months for afatinib vs. 6.9 months for chemotherapy (0.47, p=0.001). The objective response rate was 56% for afatinib vs. 23% in the control group (p<0.0001). Afatinib also delayed time to deterioration of cancer-related symptoms of cough (0.6, p=0.007) and dyspnoea (0.68, p<0.01). The PIII LUX-Lung 6 trial compared afatinib with cisplatin and gemcitabine in 364 Asian patients; median PFS was 11.0 vs. 5.6 months, respectively (0.28, p<0.0001).
Safety: Common adverse effects are diarrhoea, rash, mucositis and paronychia.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 32 No responsibility is accepted for the content of documents derived from this original publication.
Belagenpu-matucel-L injection
Lucanix
NovaRx Corporation
Indication:
Non-small cell lung cancer
– second-line.
Pharmacology:
Antisense-DNA vaccine.
Current status:
PIII.
Granted fast track status in US.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Afatinib oral
Giotrif
Boehringer Ingelheim
Indication:
Non-small cell lung cancer – second-line plus.
Pharmacology:
Tyrosine kinase inhibitor blocking EGFR and HER2.
Current status:
PIII.
Predicted UK licence extension:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Dacomitinib oral
Pfizer
Indication:
Non-small cell lung cancer, advanced – second-line plus.
Pharmacology:
Pan-HER tyrosine kinase inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: NIHR HSC Nov 2012.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Ganetespib injection
Synta
Indication:
Non-small cell lung cancer (NSCLC), advanced – second-line plus.
Pharmacology:
A second-generation heat shock protein-90 inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Eribulin injection
Halaven
Eisai
Indication:
Non-small cell lung cancer,
advanced – third-line.
Pharmacology:
Synthetic analogue of halichondrin B, with tubulin-based antimitotic activity.
Current status:
PIII.
Predicted UK licence extension:
2015
Reviews: NIHR HSC May 2013.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
LDK378 oral
Novartis
Indication:
Non-small cell lung cancer, ALK-positive, locally advanced or metastatic – second-line.
Pharmacology:
ALK inhibitor.
Current status:
PII.
Granted breakthrough therapy status in US.
Predicted UK launch:
2015
Reviews: NIHR HSC Mar 2013.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally
negotiated.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 33 No responsibility is accepted for the content of documents derived from this original publication.
Enobosarm oral
Ostarine
GTXi
Indication:
Non-small cell lung cancer (NSCLC), advanced – prevention and treatment of cachexia.
Current status:
PIII in EU.
PIII in US with fast track status.
Predicted UK launch:
2014
National guidance:
NICE: Lung cancer pathway, quality
standard.
SIGN: Lung cancer, update due 2013.
Reviews: NIHR HSC Nov 2012.
Target population: Cancer-related cachexia (loss of skeletal muscle mass and progressive functional impairment) occurs in 50% of cancer patients and causes at least 20% of deaths. The UK incidence of advanced NSCLC is 45 per 100,000 people; 25% receive first-line chemotherapy.
Sector: Secondary care.
Implications: Therapeutic options are limited for patients with cachexia, but include nutritional support, short-term corticosteroids and progestogens. Enobosarm is intended to be given to patients receiving first-line chemotherapy and may improve quality of life.
Financial: Costs will be additive to current therapy.
Likely commissioning route: NHSE. PbR: Likely HRG included.
Pharmacology: A first-in-class, non-steroidal selective androgen receptor modulator (SARM).
Efficacy: In a published PII trial (n=100; 31 with NSCLC), median total lean body mass (LBM) at 4 months increased from
baseline with enobosarm 1mg and 3mg (1.5kg and 1.0kg, respectively; both p<0.05) but not with placebo (0.02kg; p=0.88). Absolute changes from baseline in mean stair climb power (SCP) with enobosarm 1mg, 3mg and placebo were 18.0%, 21.7% and 4.8%, respectively. Although not designed to assess survival, the survival hazard ratios for patients on enobosarm 1mg or 3mg vs. placebo were 0.80 and 0.70, respectively. Initial data from two PIII trials (both n=325) show enobosarm failed to meet criteria for the co-primary outcome of LBM and SCP; POWER1 involves patients on first-line platinum plus taxane chemotherapy, and POWER2 involves patients on first-line platinum plus non-taxane chemotherapy. Although the effect of enobosarm vs. placebo on SCP was inconsistent, LBM was significantly increased at all assessment times (p=0.0003 and p=0.0227 at day 84 for POWER1 and POWER2, respectively). Survival and quality of life results are awaited.
Safety: Transient changes in liver function tests have been reported.
Anamorelin oral
Helsinn
Indication:
Anorexia/cachexia associated with non-small cell lung cancer.
Pharmacology:
Ghrelin receptor agonist.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Likely HRG included.
Trastuzumab emtansine injection
Kadcyla
Roche
Indication:
Breast cancer (BC),
advanced, HER2-positive – second/ third-line.
Current status:
Filed in EU Sep 2012.
Launched in US - see prescribing information.
Predicted UK launch:
2013
National guidance:
NICE: BC pathways - early/locally
advanced, advanced and familial, BC quality standard; trastuzumab emtansine due Aug 2014.
SIGN: Breast cancer.
Reviews: NIHR HSC Jan 2011.
Target population: The incidence of BC in the UK is about 80 per 100,000 people. About 40% develop metastatic disease; 25% of these are HER2-positive which has a worse prognosis. About 70% of patients do not respond to first-line trastuzumab and the rest develop resistance within the first year.
Sector: Secondary care.
Implications: This will compete with other second-line options including biological therapies, chemotherapies and hormonal therapies.
Financial: Cost unknown but will displace other expensive treatments. US cost is $9,800 a month.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: First-in-class trastuzumab emtasine (T-DM1) is an antibody conjugate of trastuzumab and an anti-mitotic
agent, maytansinoid DM1. Given by 3-weekly i.v. infusion.
Efficacy: The published EMILIA study enrolled 991 patients with BC that progressed after first-line trastuzumab and a taxane. Median progression-free survival (PFS) was 9.6 months for T-DM1 vs. 6.4 months for lapatinib and capecitabine (LC) (HR 0.65, p<0.001). Median overall survival at the second interim analysis was 30.9 months vs. 25.1 months, respectively (0.68, p<0.001). Objective response rates were 43.6% for T-DM1 and 30.8% for LC. 1-year and 2-year survival rates with T-DM1 were 85% and 65%; with LC they were 78% and 52%, respectively. The PIII TH3RESA study is comparing T-DM1 with treatment of choice in 606 women who have received at least 2 prior HER2 regimens. Results are due in 2015.
Safety: Compared with LC, T-DM1 more commonly causes thrombocytopenia and raised liver enzymes, but less often
causes diarrhoea, vomiting and hand-foot syndrome. Liver function and left ventricular ejection fraction require monitoring.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 34 No responsibility is accepted for the content of documents derived from this original publication.
Trastuzumab emtansine injection
Kadcyla
Roche
Indication:
Breast cancer (BC),
advanced, HER2-positive – first-line in combination with pertuzumab.
Current status:
PIII.
Predicted UK licence extension:
2014
National guidance:
As for trastuzumab emtansine above.
Reviews: NIHR HSC Jun 2012.
Target population: As for trastuzumab emtansine above.
Sector: Secondary care.
Implications: This could prevent the need for first-line chemotherapy and could result in a delay in disease progression and improved quality of life.
Financial: Cost unknown but would displace trastuzumab plus taxane
therapy. US cost is $9,800 a month.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: As above.
Efficacy: The PIII MARIANNE study is assessing progression-free survival (PFS) in 1,092 patients given first-line trastuzumab emtansine, either alone or in combination with pertuzumab vs. trastuzumab plus taxane. Results are expected in 2014. In a published PII trial (n=137), the objective response rate with T-DM1 was 64.2% vs. 58.0% with trastuzumab plus docetaxel. Compared with the control group, there was a 41% reduction in risk of disease progression or death with T-DM1, with median PFS of 9.2 months vs.14.2 months, respectively (HR 0.59).
Safety: T-DM1 caused fewer grade ≥3 adverse effects (46% vs. 91%) and adverse effects leading to discontinuations (7% vs. 41%) than trastuzumab plus taxane. Liver function and left ventricular ejection fraction require monitoring.
Trastuzumab/ hyaluronidaseinjection
Herceptin SC
Roche
Indication:
Breast cancer (BC), early and metastatic HER2-positive (all BC indications for which trastuzumab is currently indicated).
Current status:
Licensed in EU Sep 2013.
Predicted UK launch:
2013
National guidance:
As for trastuzumab emtansine above.
Reviews: NIHR HSC Jan 2011, NICE-MPC Mar 2013.
Target population: As for trastuzumab
emtansine above.
Sector: Secondary care.
Implications: Compared to the i.v. formulation, s.c. trastuzumab will reduce
preparation and administration time and would facilitate homecare delivery. This s.c. formulation is presented as a fixed dose formulation unlike the i.v. formulation that is dosed according to body weight. Biosimilar formulations of i.v. trastuzumab are in development (see page 70).
Financial: Cost unknown but may reduce overall costs and clinic time.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: Anti-HER2 monoclonal antibody co-formulated with recombinant human hyaluronidase to facilitate absorption of trastuzumab through subcutaneous tissue. Given by s.c. injection every 3 weeks.
Efficacy: The published PIII HannaH study compared the pharmacokinetics and efficacy of s.c and i.v. trastuzumab in 596 women with early HER2-postive BC. The s.c. formulation was non-inferior to the i.v. formulation; serum trough plasma concentrations before surgery were at least as high (69.0 and 51.8 microgram/mL, respectively) and efficacy as determined by pathological complete response was similar in both groups (45.4% and 40.7%, respectively).
Safety: Adverse effects are consistent with those of i.v. trastuzumab. See medicines.org.uk.
Bevacizumab injection
Avastin
Roche
Indication:
Breast cancer (BC), early HER2-positive – adjuvant therapy.
Current status:
PIII.
Predicted UK licence extension:
2014
National guidance:
As for trastuzumab emtansine above.
Reviews: NIHR HSC Apr 2012.
Target population: As for trastuzumab emtansine above. Around 95% of patients present with localised disease and are eligible for surgery. 15-20% are HER2-positive and have a worse prognosis; nearly all require adjuvant treatment with trastuzumab, which lowers risk of recurrence by 25-50% and risk of death by 17-33%.
Sector: Secondary care.
Implications: Despite treatment with trastuzumab, many women develop recurrent or metastatic disease. The addition of bevacizumab may improve response rates and delay progression.
Financial: Costs will be additive to chemotherapy and trastuzumab. Current
cost of one year’s treatment with bevacizumab for a 65kg woman is about £40,000.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: Vascular endothelial growth factor antagonist, given by i.v. infusion every 3 weeks.
Efficacy: The PIII BETH study is investigating whether giving bevacizumab for one year in addition to chemotherapy
(docetaxel/carboplatin or 5-fluorouracil, epirubicin and cyclophosphamide) plus trastuzumab improves invasive disease-free survival in 3,509 women who have undergone surgery. Interim results are expected in 2013.
Safety: See medicines.org.uk.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 35 No responsibility is accepted for the content of documents derived from this original publication.
Everolimus oral
Afinitor
Novartis
Indication:
Breast cancer (BC),
advanced HER2-positive – first-line.
Current status:
PIII.
Predicted UK licence extension:
2014/2015
National guidance:
As for trastuzumab emtansine above.
Reviews: NIHR HSC Apr 2012.
Target population: As for trastuzumab emtansine above.
Sector: Secondary care.
Implications: About 70% of patients are resistant to trastuzumab. Adding everolimus may improve response rates and delay need for second-line chemotherapy. Oral everolimus will compete with i.v. pertuzumab.
Financial: Costs will be additive to trastuzumab and chemotherapy. Current
cost of everolimus 10mg daily is £2,970 per month, and the costs of a 420mg dose of pertuzumab given three-weekly is £2,400 (excluding loading dose and administration costs).
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: mTOR inhibitor.
Efficacy: The PIII BOLERO-1 trial (n=717) is assessing addition of first-line everolimus to trastuzumab and paclitaxel.
Results are imminent. This study was initiated following published PI trial results. Disease was controlled for more than 6 months in 74% of 27 women with prior resistance to trastuzumab given everolimus in addition to paclitaxel and trastuzumab. Overall response rate was 44% and progression-free survival (PFS) was 8.5 months. A pooled analysis of PII data from 47 women with trastuzumab resistance showed adding everolimus to trastuzumab produced partial responses in 7 patients and persistent stable disease (lasting 6 months or longer) in 9 patients. Median PFS was 4.1 months.
Safety: See medicines.org.uk.
Everolimus oral
Afinitor
Novartis
Indication:
Breast cancer (BC), advanced HER2-positive – second- or third-line with trastuzumab.
Current status:
PIII.
Predicted UK licence extension:
2014
National guidance:
As for trastuzumab emtansine above.
Reviews: NIHR HSC Feb 2012.
Target population: As for trastuzumab emtansine above.
Sector: Secondary care.
Implications: Current options for patients resistant to trastuzumab produce low response rates and short durations of response. Everolimus is an alternative to lapatinib for overcoming trastuzumab resistance.
Financial: Costs will be additive to trastuzumab and chemotherapy. Current
cost of everolimus 5mg daily is £2,250/month, and lapatinib1g daily is £1,300/ month.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: mTOR inhibitor.
Efficacy: Final results of the placebo-controlled PIII BOLERO-3 trial (n=569) showed that adding everolimus 5mg daily to trastuzumab and vinorelbine reduced risk of disease progression by 22% (HR 0.78, p<0.01). Median time to progression was 7.0 months in the everolimus group and 5.8 months in the placebo group. All patients were resistant to trastuzumab-containing regimens and 27% were pre-treated with a lapatinib-containing regimen. Overall survival data are not yet mature.
Safety: See medicines.org.uk.
Sorafenib oral
Nexavar
Bayer
Indication:
Breast cancer, locally advanced metastatic HER2 negative, with capecitabine – second-line.
Pharmacology:
VEGFR, PDGFR and RAF inhibitor.
Current status:
PIII.
Predicted UK licence extension:
2015
Reviews: NIHR HSC Aug 2011.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Palbociclib oral
Pfizer
Indication:
Breast cancer, advanced or metastatic – first-line.
Pharmacology:
Cyclin-dependent kinase inhibitor.
Current status:
PII.
Granted breakthrough therapy status in US.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 36 No responsibility is accepted for the content of documents derived from this original publication.
Regorafenib oral
Stivarga
Bayer
Indication:
Gastrointestinal stromal tumours (GIST), metastatic – third-line.
Current status:
PIII.
Launched in US -see prescribing information.
Predicted UK launch:
2014
National guidance:
NICE: GIST - imatinib, sunitinib; not
recommended – higher-dose imatinib (after imatinib 400mg failure).
Reviews: None.
Target population: The incidence of metastatic GIST is 4 per million people. About two thirds of patients do not respond, or develop resistance, to first-line imatinib. Sunitinib is a second-line option.
Sector: Secondary care.
Implications: Regorafenib will provide another option for patients who have failed imatinib and sunitinib.
Financial: It will be additive to other therapies. UK cost unknown but is
$9,350/month in the US. A PAS is in place in the UK for sunitinib in GIST.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: Multi-targeted inhibitor of angiogenic, stromal and oncogenic kinase receptors, taken once daily for 3 weeks of every 4-week cycle.
Efficacy: In the published PIII GRID study 199 patients whose disease progressed despite at least 2 prior treatments received regorafenib or placebo, in addition to best supportive care. Median progression-free survival (PFS) was 4.8 months for regorafenib vs. 0.9 months for placebo (HR 0.27, p<0.0001). PFS rates at 3 and 6 months were 60% and 38% with regorafenib vs. 11% and 0% with placebo. The disease control rate (defined as the rate of partial response (PR) plus stable disease (SD) lasting for ≥12 weeks) was 53% vs. 9%, respectively (p<0.0001). In a published PII study (n=33), the clinical benefit rate (defined as complete or PR, and SD ≥16 weeks) was 79%. Four patients achieved PR, and 22 exhibited SD ≥16 weeks. Median PFS was 10.0 months.
Safety: Severe and sometimes fatal hepatotoxicity has been reported.
Masitinib oral
Kinaction
AB Science
Indication:
Pancreatic cancer, advanced – first-line in combination with chemotherapy.
Current status:
Filed in EU Oct 2012 with orphan status.
Predicted UK licence extension:
2013
National guidance:
NICE: Pancreatic cancer – gemcitabine;
masitinib due TBC.
Reviews: NIHR HSC Dec 2011.
Target population: UK incidence of pancreatic cancer is 13 per 100,000 people; 90% have advanced disease at diagnosis and 3% survive 5 years.
Sector: Secondary care.
Implications: Masitinib may extend life in patients with a bleak prognosis and few therapeutic options. It will be given in addition to gemcitabine, which is recommended by NICE for patients with a Karnofsky score of ≥50.
Financial: Cost of masitinib will be additive to current therapies. A test for
the prognostic genetic biomarker is being developed.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: Tyrosine kinase inhibitor which targets c-kit, platelet-derived growth factor receptors and fibroblast growth factor receptor 3.
Efficacy: In a PIII trial (n=348), the primary outcome of improved overall survival (OS) was not met in patients given masitinib vs. placebo, both in combination with gemcitabine (p=ns). However, masitinib increased median OS in two subgroups. In patients with a genetic biomarker (GBM) indicative of aggressive disease, median OS was 11.0 with masitinib vs. 5.0 months with placebo (0.29, p=0.00004); OS rates at 12 and 18 months were respectively, 41.4% and 18.5% for masitinib vs. 11.1% and 4.2% for placebo. In patients without the GBM, median OS in the placebo arm was 14.3 months. In patients with pain at baseline (VAS score >20mm on a 100mm scale) median OS was 8.1 months with masitinib vs. 5.4 months with placebo (0.61, p=0.01); OS rates at 12 and 18 months were respectively, 32.2% and 18.2% for masitinib vs. 17.8% and 7.8% for placebo. In patients without pain, median OS was 15.4 months for placebo.
Safety: Common adverse events in a published trial include nausea, vomiting, rash, oedema, and haematological effects.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 37 No responsibility is accepted for the content of documents derived from this original publication.
Doxorubicin heat-sensitive liposomes injection
ThermoDox
Celsion
Indication:
Hepatocellular carcinoma (HCC), inoperable – first-line.
Current status:
PIII in EU with orphan status.
PIII in US with orphan and fast track status.
Predicted UK launch:
2014
National guidance:
NICE: HCC - radiofrequency ablation,
microwave ablation, sorafenib not recommended.
Reviews: NIHR HSC Dec 2011.
Target population: UK incidence of HCC is 6 per 100,000 people. Potentially curative options are surgery (suitable for <25%) and microwave or radiofrequency ablation (RFA). 90% present with unresectable disease and 2-year survival rates are 8-50%; chemo-embolisation (chemotherapy delivered via the hepatic artery) is an option for some but systemic chemotherapy has limited benefits.
Sector: Secondary care.
Implications: For patients with limited treatment options, ThermoDox offers the possibility of greater efficacy and fewer systemic adverse effects than standard chemotherapy because of the combined effects of targeted cytotoxicity and ablation. Sorafenib is licensed for advanced HCC but not recommended by NICE. Mitozantrone is also used in the palliation of non-resectable primary hepatocellular carcinoma.
Financial: Likely to be more expensive than standard options.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: A heat-activated liposomal formulation of doxorubicin, which is released when the tumour site is heated by microwave or radiofrequency ablation (RFA) to 39-42
oC. Given by 30 minute infusion, started 15 minutes prior to ablation.
Efficacy: In the PIII HEAT trial (n=700), ThermoDox in combination with RFA vs. RFA alone did not improve progression-free survival (PFS). However, post-hoc analysis showed ThermoDox improved PFS and overall survival in 300 patients who had optimal RFA lasting ≥45 minutes, regardless of HCC lesion size.
Safety: Pre-medication is required to minimise infusion-related reactions.
Ramucirumab injection
Eli Lilly
Indication:
Hepatocellular carcinoma (HCC), advanced – second-line.
Pharmacology: Vascular endothelial growth factor receptor-2 antagonist.
Current status:
PIII in EU with orphan status.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Sorafenib oral
Nexavar
Bayer
Indication:
Hepatocellular carcinoma - adjuvant therapy.
Pharmacology:
VEGFR, PDGFR and RAF inhibitor.
Current status:
PIII with orphan status in EU and US and fast track in US.
Predicted UK licence extension:
2015
Reviews: NIHR HSC Aug 2011.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally
negotiated.
Regorafenib oral
Stivarga
Bayer
Indication:
Colorectal cancer (CRC), metastatic disease – third- or fourth-line.
Current status:
Recommended for approval in EU Jun 2013.
Launched in US -see prescribing information.
Predicted UK launch:
2013
National guidance:
NICE: CRC: pathway, quality standard;
regorafenib (suspended); not recommended - bevacizumab, cetuximab, panitumumab.
SIGN: CRC.
Reviews: NIHR HSC Aug 2011.
Target population: UK incidence of CRC is
67 per 100,000 people. 20-55% of patients present with metastatic disease. Management is mainly palliative with surgery and chemo/radiotherapy for symptom control.
Sector: Secondary care.
Implications: For patients with no further treatment options, regorafenib may
delay disease progression and improve quality of life.
Financial: Regorafenib will be additive to other therapies. UK cost is unknown but US cost is $9,350/month. A PAS is in place for cetuximab as first-line therapy for CRC in the UK.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: Multi-targeted inhibitor of angiogenic, stromal and oncogenic kinase receptors, taken once daily for 3 weeks
of every 4-week cycle.
Efficacy: The published PIII CORRECT study, in 753 adults with metastatic CRC that had progressed after receiving all approved drugs for CRC, was stopped early after meeting its primary outcome. Median overall survival was 6.4 months in patients randomised to regorafenib plus best supportive care (BSC) vs. 5.0 months for placebo plus BSC (HR 0.77, p=0.0052). Median progression-free survival was 1.9 vs. 1.7 months, respectively (0.49, p<0.0001). The on-going expanded-access PIII CONSIGN study is designed to collect safety data.
Safety: Severe and sometimes fatal hepatotoxicity has been reported.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 38 No responsibility is accepted for the content of documents derived from this original publication.
Sorafenib oral
Nexavar
Bayer
Indication:
Renal cell carcinoma (RCC) - adjuvant therapy.
Current status:
PIII with orphan status.
Predicted UK licence extension:
2014/2015
National guidance:
NICE: Urological cancer; pazopanib,
sunitinib (first-line advanced); not recommended – bevacizumab, sorafenib, sunitinib (second-line) and temsirolimus.
Reviews: None.
Target population: UK incidence of RCC is
12 per 100,000 people. Patients with stage 1 (39%) and 2 (16%) RCC, and some with stage 3 (26%), are candidates for surgery. Five-year survival ranges from 40-90% in stage 1-3 disease, and 10% in stage 4.
Sector: Secondary care.
Implications: RCC recurs in 30% of patients undergoing nephrectomy for
localised disease. Sorafenib may delay development of metastatic disease, which responds to targeted therapies, such as sorafenib and sunitinib, but not to chemotherapy.
Financial: Cost of sorafenib 400mg twice daily is £2,980/month.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally
negotiated.
Pharmacology: Blocks Raf and tyrosine kinases, vascular endothelial and platelet derived growth factor receptors.
Efficacy: Adjuvant sorafenib in patients who have undergone partial or radical nephrectomy, at high or intermediate risk of relapse, is being studied in two PIII trials. SORCE is a placebo-controlled trial in 1,656 patients treated for 1 or 3 years; ASSURE (n=1,923) will compare sorafenib with sunitinib or placebo for 1 year. Results are expected in 2013 and 2016, respectively. In a published trial, overall recurrence rate was 15.0% in patients receiving sorafenib (n=20), 17.4% in patients given sunitinib (n=23) and 38.7% in those receiving no adjuvant therapy (n=388, p<0.05 vs. treatment groups). Disease-free survival was 18.9 months, 16.9 months and 13.3 months, respectively (p<0.05 vs. treatment groups).
Safety: See medicines.org.uk.
Apaziquone intravesical
Neoquin
Spectrum
Indication:
Bladder cancer, non-
muscle invasive (NMIBC), in patients at low or intermediate risk of progression.
Current status:
PIII in EU.
PIII in the US with fast track status.
Predicted UK launch:
2014/2015
National guidance:
NICE: Urological cancer, bladder cancer
due 2014.
SIGN: Bladder cancer.
Reviews: None.
Target population: UK incidence of NMIBC is about 13 per 100,000 people. After surgery, intravesical chemotherapy reduces risk of recurrence at 1 year by up to 44% (depending on the number of doses).
Sector: Secondary care.
Implications: Apaziquone will be an alternative to intravesical mitomycin, epirubin and doxorubicin in patients at low or intermediate risk of progression. BCG vaccine is used in high-risk patients.
Financial: Apaziquone may displace current options.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: An indoloquinone mitomycin analogue prodrug metabolised to an alkylating agent by the DT-diaphorase enzyme, which is over-expressed by bladder cancer cells.
Efficacy: Two PIII trials (SPI-611 and SPI-612) each recruiting 800 patients have investigated use of a single dose of
apaziquone following transurethral resection of bladder tumours. Individually they did not meet their primary outcomes but pooled analysis showed apaziquone reduced the rate of tumour recurrence at 2 years (p=0.017). In a published PII study of 46 patients who underwent surgical excision of all but one superficial lesion, 67% had complete histological disappearance of the remaining lesion 2-4 weeks after 6 once-weekly instillations of apaziquone. After 24 months, 50% of responders were recurrence-free, with a median response duration of 18 months. Overall recurrence-free survival was 39%. Two ongoing placebo-controlled PIII studies (SPI-1011 and SPI-1012) are investigating 6-weekly instillations.
Safety: Adverse effects include cystitis, dysuria, haematuria and abdominal pain.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 39 No responsibility is accepted for the content of documents derived from this original publication.
Sipuleucel-T injection
Provenge
Dendreon
Indication:
Prostate cancer (PC),
metastatic castration-resistant – first-line.
Current status:
Recommended for approval in EU Jun 2013.
Launched in US – see prescribing information.
Predicted UK launch:
2013
National guidance:
NICE: PC pathway; docetaxel,
sipuleucel-T due Feb 2014.
Reviews: NIHR HSC Apr 2011.
Target population: In the UK, the incidence
of PC is 134 per 100,000 men. 55-65% develop metastatic disease and over 90% become resistant to standard hormonal therapy (castration-resistant).
Sector: Secondary care.
Implications: Sipuleucel-T will compete with docetaxel and first-line
abiraterone acetate. It may prolong survival and have improved tolerability over existing therapies.
Financial: Cost in the US is $93,000 for 3 doses.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: First personalised therapeutic vaccine that stimulates a T-cell response against prostatic acid phosphatase, an antigen expressed in most PCs but not in non-prostate tissue. Given by i.v. infusion every 2 weeks for 3 doses.
Efficacy: In published PIII trials, patients had leukapheresis followed 3 days later by infusion of sipuleucel-T or control (autologous peripheral blood mononuclear cells that had not been activated). In the IMPACT study (n=512), median overall survival (OS) was 25.8 months for sipuleucel-T vs. 21.7 months for control (HR 0.78, p=0.03). Median time to objective disease progression (TTP) was 14.6 weeks vs. 14.4 weeks, respectively (p=ns). In the D9901 study (n=127), median TTP for sipuleucel-T was 11.7 weeks vs. 10.0 weeks for placebo (1.45, p=0.052) and median OS was 25.9 months and 21.4 months, respectively (1.7, p=0.01). In a meta-analysis of 3 trials (n=737), median OS of patients who received sipuleucel-T vs. the control group was longer (0.73, p=0.001) but median TTP was not (p=ns).
Safety: Pre-medication is required to prevent acute infusion reactions (commonly chills, fever and fatigue).
Ipilimumab injection
Yervoy
Bristol Myers Squibb
Indication:
Prostate cancer (PC), metastatic castration-resistant – second-line.
Current status:
PIII.
Predicted UK licence extension:
2014
National guidance:
NICE: PC pathway; abiraterone,
docetaxel, enzalutamide due Feb 14; not recommended – cabazitaxel.
Reviews: NIHR HSC Dec 2011.
Target population: UK incidence of PC is 134 per 100,000 men. 55-65% develop metastases and >90% become resistant to hormonal therapy (castration-resistant). About 40% of these men receive first-line therapy (NICE recommends docetaxel), and of these about 75% may receive second-line therapy (24 per 100,000 men).
Sector: Secondary care.
Implications: Second-line treatments include abiraterone, cabazitaxel and enzalutamide. Ipilimumab may provide an additional treatment option for patients with a poor prognosis.
Financial: Ipilimumab costs £52,500 per dose for a 70kg person. A PAS is in place for second-line abiraterone.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: Anti-CTLA-4 monoclonal antibody given by i.v. infusion every 3 weeks for 4 doses, then 3-monthly.
Efficacy: A placebo-controlled PIII trial is assessing the effect of ipilimumab monotherapy following radiotherapy on overall survival in 800 men previously treated with docetaxel. Data are due soon. In a PII trial (n=24), decreases in serum prostate-specific antigen (PSA) levels of >50% were seen in 12.5% of patients treated with ipilimumab. One patient had a confirmed response lasting 246 days, one had a response of ≥79 days, and a third had an unconfirmed response.
Safety: See medicines.org.uk.
Custirsen injection
OncoGenex
Indication:
Prostate cancer, metastatic castration-resistant, first/second-line.
Pharmacology:
Clusterin inhibitor.
Current status:
PIII in EU.
PIII in US with fast track status.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally
negotiated.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 40 No responsibility is accepted for the content of documents derived from this original publication.
Cabozantinib oral
Cometriq
Exelixis
Indication:
Prostate cancer,
castration-resistant – third-line.
Pharmacology:
MET, RET and VEGFR2 inhibitor.
Current status:
PIII.
Predicted UK licence extension:
2015
Reviews: None
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Radium-223 chloride injection
Alpharadin
Bayer
Indication:
Prostate cancer (PC), castration-resistant (patients with bone metastases).
Current status:
Filed in EU Dec 2012.
Licensed in US after priority review. See US prescribing information.
Predicted UK launch:
2013
National guidance:
NICE: PC pathway, denosumab
(metastases in PC) due TBC, radium-223 due Feb 2014, denosumab (in solid tumours other than prostate).
Reviews: No recent reviews.
Target population: UK incidence of PC is 134 per 100,000 men. 55-65% develop metastases and >90% become resistant to standard hormonal therapy (castration-resistant). Over 90% with advanced disease develop bone metastases which can lead to fractures, uncontrollable bone pain and spinal cord compression.
Sector: Secondary care.
Implications: Radium-233 could improve quality of life and delay disease progression. It is potentially an alternative/additive option to palliative therapies.
Financial: Cost is unknown but may displace other therapies.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: A first-in-class radiopharmaceutical that targets bone metastases. Given i.v. monthly for up to 6 cycles.
Efficacy: The published PIII ALSYMPCA study (n=921) was stopped early after meeting its primary outcome. Median overall survival (OS) was 14.9 months in the radium-223 group vs. 11.3 months for placebo (HR 0.7, p<0.0001). Radium-223 delayed median time to first skeletal-related event vs. placebo (15.6 vs. 9.8 months, respectively, HR 0.66, p<0.001). In a published PII study (n=64), median change in alkaline phosphatase was -65.6% in the radium-223 group vs. 9.3% in the placebo group (p<0.001); median OS was 16.3 months vs. 11.6 months (p=0.066). In a published PII study (n=100), pain was significantly reduced at 8 weeks in 56% of men given a single dose of radium-223.
Safety: Most common adverse effects are nausea, diarrhoea, vomiting, peripheral oedema and anaemia.
Pazopanib oral
Votrient
GlaxoSmith-Kline
Indication:
Ovarian cancer (OC) – maintenance after first-line chemotherapy.
Current status:
Filed in EU Aug 2013.
Predicted UK licence extension:
2014
National guidance:
NICE: OC pathway, quality standard;
first-line – paclitaxel; not recommended – bevacizumab.
SIGN: Ovarian cancer.
Reviews: NIHR HSC Apr 2011.
Target population: UK incidence of OC is
21 per 100,000 people. Most women have advanced disease and 75% receive first-line platinum chemotherapy; between 70 and 80% respond (11-13 per 100,000). Of these 55-75% relapse within 2 years.
Sector: Secondary care.
Implications: Pazopanib will be used in addition to current therapies but
may delay need for second-line chemotherapy.
Financial: Cost of pazopanib 800mg daily is £2,200/month.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: Multi-targeted tyrosine kinase receptor inhibitor.
Efficacy: In a PIII trial (n=940) assessing the effect of pazopanib monotherapy for 2 years in OC (91% advanced disease), that has not progressed after first-line chemotherapy, median progression-free survival (PFS) was 17.9 months with pazopanib vs. 12.3 months with placebo (HR 0.77, p=0.0021). Overall survival data are immature. In a published PII trial (n=36) with pazopanib monotherapy, 31% of patients achieved the primary outcome of ≥50% decrease in cancer antigen-125 levels. Stable disease was seen in 56% of patients, with median duration of 80 days. At 6 months, 17% remained progression-free.
Safety: See medicines.org.uk.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 41 No responsibility is accepted for the content of documents derived from this original publication.
Paclitaxel injection
Paclical
Oasmia
Indication:
Ovarian cancer (OC),
platinum-sensitive or partially platinum-sensitive – second- or third-line.
Current status:
PIII with orphan status.
Predicted UK launch:
2014
National guidance:
NICE: As for pazopanib above plus OC
recurrent, advanced – paclitaxel, pegylated liposomal doxorubicin and topotecan; not recommended – bevacizumab, trabectedin.
SIGN: Ovarian cancer.
Reviews: NIHR HSC Dec 2011.
Target population: As for pazopanib above.
Sector: Secondary care.
Implications: Compared to current formulations, Paclical may cause fewer adverse effects, requires no pre-medication and may allow higher doses.
Financial: Cost unknown but will displace other taxanes. Cost of currently available paclitaxel is £3,600 for six cycles (body surface area of 1.7m
2).
Likely commissioning route: NHSE. PbR: Chemotherapy is locally
negotiated.
Pharmacology: A new formulation of paclitaxel encapsulated to increase its water solubility, removing the need for solvents
which can cause hypersensitivity reactions. Given by i.v infusion every 3 weeks for 6 cycles.
Efficacy: The PIII OAS-07OVA trial is comparing Paclical (250mg/m2) with Taxol (175mg/m
2), both in combination with
carboplatin, in 790 women with OC who have relapsed more than 6 months after first- or second-line chemotherapy. The final patient was treated in early 2013. Interim analysis indicates Paclical reduces levels of the biomarker, cancer antigen-125 (CA-125), to similar levels as Taxol.
Safety: Requires no pre-medication.
Vintafolide injection
Vynfinit
MSD
Indication:
Ovarian cancer (OC), advanced platinum-resistant, folate receptor (FR)-positive – second-line.
Current status:
Filed in EU Nov 2012 with orphan status.
Predicted UK launch:
2014
National guidance:
NICE: As for paclitaxel above plus
vintafolide due Jul 2014.
SIGN: Ovarian cancer.
Reviews: NIHR HSC Dec 2011.
Target population: As for pazopanib above. Between 90 and 100% of tumours are FR-positive.
Sector: Secondary care.
Implications: Vintafolide added to doxorubicin will provide a more targeted treatment for patients whose disease recurs within 6 months of chemotherapy. They are unlikely to respond to further platinum therapy and have few options, with 10-40% responding to non-platinum agents.
Financial: Likely to be expensive. Cost of the radiopharmaceutical diagnostic test technetium Tc99m etarfolatide is unknown.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: Vinca alkaloid conjugated to a folate molecule. It enters tumour cells via the folate receptor, which is over-expressed by most OC tumour cells. Given as an i.v. infusion in combination with pegylated liposomal doxorubicin (PLD).
Efficacy: The PII PRECEDENT study involved 162 women who had relapsed within 6 months of platinum chemotherapy. Progression-free survival (PFS) was 21.7 weeks in those on vintafolide plus PLD and 11.7 weeks in those on PLD alone (HR 0.63, p=0.03). PFS in patients with at least one FR-positive tumour site was 24.6 weeks in the vintafolide plus PLD group vs. 7.6 weeks in the PLD only group (0.6, p=0.04); in patients in whom all tumour sites were FR-positive it was 24.0 vs. 6.6 weeks, respectively (0.4, p<0.02). The PIII PROCEED trial (n=640) is similar in design with results due in 2014.
Safety: Adverse effects include neutropenia, anaemia, fatigue and hand/foot syndrome.
Bevacizumab injection
Avastin
Roche
Indication:
Ovarian cancer (OC), advanced platinum-resistant – second-line in combination.
Current status:
PIII.
Predicted UK licence extension:
2014
National guidance:
NICE: As for vintafolide above.
SIGN: Ovarian cancer.
Reviews: NIHR HSC Jan 2013.
Target population: As for pazopanib above. Most patients receive platinum chemotherapy a second or third time before developing resistance.
Sector: Secondary care.
Implications: Bevacizumab will be used in addition to current chemotherapies and may delay disease progression.
Financial: Current cost of 10 doses (15mg/kg) for a 65kg woman is £23,000.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally
negotiated.
Pharmacology: Vascular endothelial growth factor antagonist given by i.v. infusion every 3 weeks.
Efficacy: In the PIII AURELIA trial, 361 women were randomised to chemotherapy (liposomal doxorubicin, paclitaxel or
topotecan) alone or with bevacizumab (10mg/kg every 2 weeks or 15mg/kg every 3 weeks) until progression. Median progression-free survival (PFS) was 6.7 months in the bevacizumab group and 3.4 months in the control group (HR 0.48, p<0.001). The objective response rate was 30.9% vs. 12.6%, respectively (p=0.001).
Safety: See medicines.org.uk. Gastrointestinal perforations and fistulas occurred in 2% of women receiving bevacizumab
plus chemotherapy and in none of the control group.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 42 No responsibility is accepted for the content of documents derived from this original publication.
Olaparib oral
AstraZeneca
Indication:
Ovarian cancer, relapsed,
platinum-sensitive, gBRCAm positive.
Pharmacology:
PARP enzyme inhibitor.
Current status:
PII with orphan status in EU.
Predicted UK launch:
2015
Reviews: NIHR HSC May 2013.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Trebananib injection
Amgen
Indication:
Epithelial ovarian, fallopian tube or primary peritoneal cancer, recurrent disease.
Pharmacology:
Angiopoietin-1 and 2 inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: NIHR HSC Jan 2013.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Eribulin injection
Halaven
Eisai
Indication:
Soft tissue sarcoma, advanced – third-line.
Pharmacology:
Synthetic analogue of halichondrin B, with tubulin-based antimitotic activity.
Current status:
PIII with orphan status in US.
Predicted UK licence extension:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Ipilimumab injection
Yervoy
Bristol Myers Squibb
Indication:
Malignant melanoma, resected high-risk stage III – first-line adjuvant therapy.
Current status:
PIII.
Predicted UK licence extension:
2014
National guidance:
NICE: Skin tumours, melanoma due Apr
2015.
SIGN: Cutaneous melanoma.
Reviews: NIHR HSC Jun 2012.
Target population: UK incidence of malignant melanoma is about 21 per 100,000 people, and is doubling every 10-20 years. 7% of 15-64 year olds present with advanced (III/IV) disease compared with 20% aged ≥65.
Sector: Secondary care.
Implications: There is currently no standard adjuvant therapy. Interferon is of uncertain benefit and causes significant toxicity. Ipilimumab given after surgery may prevent melanoma recurrence.
Financial: Ipilimumab costs £52,500 per dose for a 70kg person.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: Anti-CTLA-4 monoclonal antibody given by i.v. infusion every 3 weeks for 4 doses, then 3-monthly.
Efficacy: A placebo-controlled PIII study is investigating the efficacy of ipilimumab in 950 adults with confirmed lymph node metastases, who have undergone complete resection of stage III melanoma. The primary outcome is recurrence-free survival and initial results are expected in 2013 or 2014. In a published PII trial (n=75), 56% of patients with stage III or IV melanoma given adjuvant ipilimumab were relapse-free and 86% alive at 2 years. An on-going PIII study is comparing adjuvant ipilimumab with high-dose interferon alfa-2b.
Safety: See medicines.org.uk.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 43 No responsibility is accepted for the content of documents derived from this original publication.
Dabrafenib oral
Tafinlar
GlaxoSmith-Kline
Indication:
Malignant melanoma,
unresectable or metastatic BRAF
V600E-positive – first-
line.
Current status:
Licensed in EU Sep 2013.
Licensed in US -see prescribing information.
Predicted UK licence extension:
2013
National guidance:
NICE: As for ipilimumab above plus
dabrafenib due TBC, vemurafenib, ipilimumab (first-line) due Jun 2014.
SIGN: Cutaneous melanoma.
Reviews: NIHR HSC Aug 2011.
Target population: As for ipilimumab above. About 50% are BRAF
V600-positive (80-90%
V600E and 10-20% V600K) which is associated with increased tumour aggressiveness.
Sector: Secondary care.
Implications: Dabrafenib will compete with vemurafenib, providing an alternative to i.v. dacarbazine which has a low response rate. A test is needed to identify BRAF
V600E-positive patients.
Financial: Likely to be similarly priced to vemurafenib (£7,000 per month).
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: BRAFV600E
kinase inhibitor taken twice daily.
Efficacy: In the published BREAK-3 trial, 250 adults with previously untreated, stage IV or unresectable stage III BRAFV600E
-positive melanoma were randomised to dabrafenib or 3-weekly cycles of i.v. dacarbazine. Median PFS was 5.1 months for dabrafenib vs. 2.7 months for dacarbazine; dabrafenib reduced risk of disease progression or death by 70% (HR 0.30, p<0.0001). There was no difference in overall survival (HR 0.61) but data are immature. 50% of patients on dabrafenib had a confirmed objective response vs. 6% on dacarbazine.
Safety: Photosensitivity, which is common with vemurafenib, occurs rarely with dabrafenib.
Ipilimumab injection
Yervoy
Bristol Myers Squibb
Indication:
Malignant melanoma, unresectable or metastatic – first-line with dacarbazine.
Current status:
PIII in EU.
Launched in US -see prescribing information.
Predicted UK licence extension:
2014/2015
National guidance:
NICE: As for ipilimumab above plus
vemurafenib, ipilimumab (first-line) due Jun 2014, dabrafenib due TBC.
SIGN: Cutaneous melanoma.
Reviews: No recent reviews.
Target population: As for ipilimumab above.
Sector: Secondary care.
Implications: A therapeutic option for patients whose tumours do not have
BRAF mutations, which may improve response rates and survival when added to current first-line standard of care (dacarbazine).
Financial: Ipilimumab costs £52,500 per dose for a 70kg person.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally
negotiated.
Pharmacology: Anti-CTLA-4 monoclonal antibody given by i.v. infusion every 3 weeks for 4 doses, then 3-monthly.
Efficacy: In the published 024 study, 502 patients were randomised to receive dacarbazine with or without ipilimumab.
Median overall survival (OS) in the ipilimumab plus dacarbazine group was 11.2 months vs. 9.1 months in the dacarbazine alone group (HR 0.72, p<0.001). OS rates at 1 year were 47.3% vs. 36.3%, at 2 years were 28.5% vs. 17.9%, and at 3 years were 20.8% vs. 12.2%, respectively (0.72, p<0.001). There was a 24% reduction in risk of progression in the ipilimumab plus dacarbazine group vs. the dacarbazine group (0.76, p=0.006).
Safety: See medicines.org.uk.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 44 No responsibility is accepted for the content of documents derived from this original publication.
Trametinib oral
Mekinist
GlaxoSmith-Kline
Indication:
Malignant melanoma,
unresectable or metastatic BRAF
V600-positive – first-or
second-line monotherapy and first-line in combination with dabrafenib.
Current status:
Filed in EU Feb 2013. Monotherapy is licensed in US -see prescribing information. Combination therapy filed in US Jul 2013.
Predicted UK launch:
2014
National guidance:
NICE: As for ipilimumab above plus
ipilimumab (second-line), vemurafenib, dabrafenib due TBC, ipilimumab (first-line) due Jun 2014.
SIGN: Cutaneous melanoma.
Reviews: NIHR HSC (monotherapy) Aug 2011, NIHR HSC (combination therapy) Sep 2012.
Target population: As for dabrafenib above. About 50% of patients progress within about 6 months of starting a BRAF or MEK inhibitor.
Sector: Secondary care.
Implications: Trametinib, like dabrafenib and vemurafenib, are alternatives to i.v. dacarbazine which has a response rate of 5-15% and improves progression-free survival (PFS) by only a few months. A test is needed to identify BRAF
V600-positive patients. Combination therapy offers the possibility
of improved survival and better tolerability.
Financial: US cost of trametinib is $8,700/month.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally
negotiated.
Pharmacology: A mitogen-activated extracellular signal regulated kinase-1 (MEK) inhibitor taken once daily. Use in
combination with twice-daily dabrafenib overcomes resistance to BRAF inhibition associated with reactivation of MEK.
Efficacy: Results from the published PIII METRIC study (n=322) show trametinib monotherapy increased PFS and overall survival (OS) at 6 months vs. chemotherapy (dacarbazine or paclitaxel). Median PFS was 4.8 months vs. 1.5 months, respectively (HR 0.45, p<0.001); respective OS rates were 81% and 67% (0.54, p=0.01, NNT 7). A published PII study showed patients previously treated with a BRAF inhibitor (n=40) were unresponsive to trametinib monotherapy, unlike BRAF inhibitor-naïve patients (n=57); median PFS was 1.8 months and 4.0 months, respectively. In a published PII trial (n=162) of dabrafenib-trametinib combination therapy, median PFS was 9.4 months vs. 5.8 months in patients given dabrafenib alone (0.39, p<0.001); objective response rates were 76% and 54%, respectively (p=0.03). 41% of patients were alive and progression-free at 1 year vs. 9% (p<0.001, NNT 3). PIII trials are comparing trametinib plus dabrafenib with vemurafenib (COMBI-v; n=694) or dabrafenib (COMBI-d; n=340) alone; initial results are expected in 2014.
Safety: Dose-limiting skin adverse effects occur less frequently with combination therapy, but the rate of pyrexia is higher.
Talimogene laherparepvec injection
Amgen
Indication:
Malignant melanoma,
unresectable or metastatic.
Pharmacology:
Oncolytic virus immunostimulant.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: No recent reviews.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Cobimetinib
oral
Roche
Indication:
Malignant melanoma, metastatic, BRAF positive, with vemurafenib – first-line.
Pharmacology:
MEK inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE
PbR: Chemotherapy is locally negotiated.
Erismodegib oral
Novartis
Indication:
Basal cell carcinoma, locally advanced or metastatic.
Pharmacology:
Smoothened (Smo) inhibitor.
Current status:
PII.
Predicted UK launch:
2015
Reviews: NIHR HSC Jan 2013.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 45 No responsibility is accepted for the content of documents derived from this original publication.
Rituximab injection
MabThera
Roche
Indication:
Non-Hodgkin's lymphoma (NHL) - s.c. formulation.
Current status:
Filed in EU Dec 2012.
Predicted UK launch:
2013
National guidance:
NICE: NHL - rituximab (follicular, first-
line), rituximab (follicular maintenance). Reviews: None.
Target population: All patients with NHL for whom i.v. rituximab is currently indicated. Those with poor venous access may be initial candidates.
Sector: Secondary care.
Implications: Availability of s.c. formulation could reduce outpatient preparation and administration time and may facilitate homecare delivery. Biosimilar i.v. formulations of rituximab are likely to be available in 2015.
Financial: Likely to be the same cost as the current i.v. formulation but future
availability of biosimilar i.v. formulations may affect pricing strategy.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: Anti-CD20 monoclonal antibody plus recombinant human hyaluronidase for s.c. administration.
Efficacy: The PIII SABRINA open-label study assessed s.c. vs. i.v. administration of rituximab in 530 patients with follicular NHL receiving induction and maintenance therapy. The stage 1 primary outcome of non-inferiority of the Ctrough,SC:Ctrough,IV ratio at cycle 7 of induction was met and analysis showed similar investigator-assessed overall response rates (84.4% for i.v. vs. 90.5% for s.c.). Stage 2 of the trial is on-going and will assess overall survival.
Safety: See medicines.org.uk. Injection site reactions are possible.
Benda-mustine injection
Levact
Napp
Indication:
Non-Hodgkin’s lymphoma (NHL), advanced low-
grade - first-line with rituximab.
Current status:
Filed in EU.
Filed in US Dec 2011 but additional data requested in Oct 2012.
Predicted UK licence extension:
2013
National guidance:
NICE: As for rituximab above plus NHL-
bendamustine first-line due Jul 2014.
Reviews: LCNDG Apr 2013.
Target population: The UK incidence of NHL is about 20 per 100,000 people and about 40% present with indolent (low-grade) disease, usually advanced (stage III or IV).
Sector: Secondary care.
Implications: Bendamustine could be used instead of standard chemotherapy regimens which have more adverse effects.
Financial: Bendamustine is currently licensed for second-line use in NHL.
Cost of a 12-dose course is about £6,500.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: An alkylating agent with antimetabolite activity, given by i.v. infusion for up to six cycles.
Efficacy: In the published PIII non-inferiority StiL trial, 549 patients newly diagnosed with stage III or IV indolent or mantle-cell lymphoma were randomised to bendamustine or standard therapy. At median follow-up of 45 months, median PFS was 69.5 months for bendamustine vs. 31.2 months for standard therapy (HR 0.58, p<0.0001). In the ongoing PIII BRIGHT study (n=477) bendamustine was non-inferior to standard therapy for complete response rate (31% vs. 25%, p<0.03).
Safety: See medicines.org.uk. In the StiL trial bendamustine resulted in lower rates of alopecia, haematological toxicity, infections, peripheral neuropathy and stomatitis than standard therapy (all p<0.003) but skin reactions were more common.
Dasiprotimut-T injection
BiovaxID
Biovest International
Indication:
Non-Hodgkin’s lymphoma (NHL), low-grade follicular disease.
Current status:
PIII with orphan status and plans to file in EU in 2013. Available on compassionate use basis. Fast track status in US.
Predicted UK launch:
2014
National guidance:
As for rituximab above.
Reviews: No recent reviews.
Target population: The UK incidence of follicular NHL is 5-7 per 100,000 and most present with stage III or IV disease. These patients are considered for chemotherapy and will be eligible for this vaccine if they have prolonged remission.
Sector: Secondary care.
Implications: The company believes dasiprotimut-T may eliminate the risk of rituximab resistance and increase utility of other therapies. A subgroup of patients with the IgM isotype may be more responsive to treatment; US authorities have requested additional data to confirm this.
Financial: Additive to current options after first-line treatment but may delay need for other therapies.
Likely commissioning route: NHSE. PbR: Uncertain.
Pharmacology: An autologous vaccine consisting of a conjugated lymphoma-associated antigen given about 6 months after chemotherapy. Five s.c. injections are given over a 6 month period. Booster vaccination may be required after 3 years.
Efficacy: In the prematurely closed PIII BV301 trial 117 patients who maintained a complete response to initial chemotherapy were given dasiprotimut-T or control vaccine. Median disease-free survival was 30.6 vs. 17 months, respectively (p<0.05). At 36 months, 61% of patients on dasiprotimut-T were disease-free vs. 37% of control patients (NNT=4). These data, together with data from two long-term PII trials will be used in the EU licence application. In another PIII study, in 35 IgM-positive patients given dasiprotimut-T made with IgM isotype, 5-year tumour-free rates were 42% vs.11% in patients receiving control vaccine (NNT=3). Median time to relapse was 52.9 vs. 28.7 months, respectively (HR 0.34, p=0.002).
Safety: To date no serious adverse effects have been reported.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 46 No responsibility is accepted for the content of documents derived from this original publication.
Bortezomib injection
Velcade
Janssen-Cilag
Indication:
Multiple myeloma (MM),
relapsed or progressive disease - combined with dexamethasone or pegylated doxorubicin.
Current status:
Filed in EU Oct 2012.
Predicted UK licence extension:
2013
National guidance:
NICE: MM - bortezomib (monotherapy,
relapsed), lenalidomide (after at least one prior therapy).
Reviews: NIHR HSC Sep 2012.
Target population: The UK incidence of MM is about 8 per 100,000 and prevalence is about 16 per 100,000 people. Of these, 39% have relapsed MM and of these 65% will have received 2 or more prior therapies. Patients typically relapse 3 or 4 times before developing treatment resistance.
Sector: Secondary care.
Implications: Current options in this setting include bortezomib monotherapy and lenalidomide plus dexamethasone. This licence extension will provide further options with the possibility of delaying disease progression further.
Financial: Cost of 32 doses (8 cycles) is about £24,000.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: A proteasome inhibitor given by i.v. injection.
Efficacy: In a published PIII study bortezomib plus pegylated liposomal doxorubicin (PLD) was compared with bortezomib monotherapy in 646 patients. Interim data show the primary outcome of median time to progression was 6.5 months for bortezomib vs. 9.3 months with PLD plus bortezomib (HR 1.82, p<0.001). The 15-month survival rate was 65% vs. 76%, respectively (p=0.03) and overall response rate was 41% vs. 44%, respectively (p=ns).
Safety: See medicines.org.uk.
Carfilzomib injection
Kyprolis
Onyx
Indication:
Multiple myeloma (MM), relapsed and refractory – third-line.
Current status:
PIII in EU with orphan status and plans to file 2013.
Launched in US - see prescribing information.
Predicted UK launch:
2014
National guidance:
NICE: As for bortezomib above.
Reviews: NIHR HSC Sep 2012.
Target population: As for pomalidomide above. The majority of patients are expected to receive third-line therapy.
Sector: Secondary care.
Implications: US indication is monotherapy use in relapsed MM after at least 2 prior therapies; this is likely to be the initial indication in the EU. There is currently no standard third-line option in the UK.
Financial: US cost is $10,000 per cycle for an average patient, making it the most expensive drug in the US for MM.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: Second generation selective and irreversible proteasome inhibitor, first-in-class.
Efficacy: The US licence is based on a published PII single-arm study in 266 patients with a median of 5 prior therapies, including bortezomib, lenalidomide, and thalidomide. The overall response rate was 23.7%. Median overall survival, a secondary outcome, was 15.6 months. The ongoing PIII FOCUS study compares carfilzomib with best supportive care after treatment with at least 3 prior therapies. The primary outcome is overall survival. Comparative studies with bortezomib (ENDEAVOR) and in combination with lenalidomide and dexamethasone (ASPIRE) are ongoing.
Safety: Adverse effects are similar to other proteasome inhibitors but low rates of peripheral neuropathy have been reported.
Daratumumab injection
Janssen-Cilag
Indication:
Multiple myeloma, recurrent/ refractory – second-line.
Pharmacology:
Humanised anti-CD38 monoclonal antibody.
Current status:
PII.
Granted fast track and breakthrough therapy status in US.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Omacetaxine meppe-succinate injection
Synribo
Teva
Indication:
Chronic myelogenous leukaemia (CML), after failure of two tyrosine kinase inhibitors.
Pharmacology:
Protein synthesis inhibitor.
Current status:
PIII in EU with orphan status. Launched in US– see prescribing information.
Predicted UK launch:
Uncertain.
Reviews: None.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
UKMi September 2013 Solely for use within the NHS and not for commercial use. page 47 No responsibility is accepted for the content of documents derived from this original publication.
Vosaroxin injection
Sunesis
Indication:
Acute myeloid leukaemia,
first relapse or refractory, with cytarabine.
Pharmacology:
Anticancer quinolone derivative.
Current status:
PIII with orphan status in EU and US.
Predicted UK launch:
2016
Reviews: NIHR HSC Jun 2013.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Obinutuzu-mab injection
Gazyva
Roche
Indication:
Chronic lymphocytic leukaemia (CLL), first-line
in patients with co-morbidities unable to have standard therapy.
Current status:
Filed in EU Apr 2013 with orphan status.
Filed in US with breakthrough therapy status.
Predicted UK launch:
2014
National guidance:
NICE: CLL - Bendamustine, fludarabine,
rituximab.
Reviews: NIHR HSC Jun 2012.
Target population: UK annual incidence of CLL is 4.2 per 100,000 people, increasing to over 30 per 100,000 in those over 80 years of age.
Sector: Secondary care.
Implications: An alternative for patients with co-morbidities who cannot have FCR (fludarabine, cyclophosphamide, rituximab). Current options include chlorambucil or bendamustine (both with/without rituximab) or reduced dose FCR. It will compete with ofatumumab below.
Financial: Alternative monthly treatment costs: chlorambucil £56, bendamustine £966, rituximab £1,572.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally
negotiated.
Pharmacology: Humanised anti-CD20 monoclonal antibody given by i.v. infusion.
Efficacy: In an interim analysis (n=589) of the on-going PIII CLL11 trial investigating obinutuzumab plus chlorambucil vs.
rituximab plus chlorambucil vs. chlorambucil alone in 781 patients, median progression-free survival (PFS) was 23 months for obinutuzumab and chlorambucil vs. 10.9 months for chlorambucil alone (p<0.01). The primary outcome of improved PFS with obinutuzumab plus chlorambucil vs. rituximab plus chlorambucil has been met; data will be released in Dec 2013.
Safety: Adverse events are similar to other anti-CD20 monoclonal antibodies.
Ofatumumab injection
Arzerra
GlaxoSmith-Kline
Indication:
Chronic lymphocytic leukaemia (CLL), first-line in patient with co-morbidities unable to have standard therapy.
Current status:
PIII in EU with orphan status.
Predicted UK licence extension:
2014
National guidance:
As for obintuzumab above.
Reviews: NIHR HSC Feb 2012.
Target population: As for obintuzumab
above.
Sector: Secondary care.
Implications: As for obinutuzumab above with which it will compete.
Financial: As for obinutuzumab above and cost for ofatumumab 100mg is £1,820/month.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally negotiated.
Pharmacology: Humanised anti-CD20 monoclonal antibody given by i.v. infusion.
Efficacy: In the on-going PIII COMPLEMENT-1 trial (n=447) median progression-free survival was 22.4 months for
ofatumumab and chlorambucil vs. 13.1 months for chlorambucil alone (HR 0.57, p<0.01). More data are due to be released in Sept 2013.
Safety: See medicines.org.uk.
Idelalisib oral
Gilead Sciences
Indication:
Chronic lymphocytic leukaemia - second-line.
Pharmacology:
Phosphatidylinositol 3-kinase delta (PI3K-delta) inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Ibrutinib oral
Janssen-Cilag
Indication:
Mantle cell lymphoma, refractory/relapsed – second-line.
Pharmacology:
Bruton’s tyrosine kinase inhibitor - first-in-class.
Current status:
PIII with orphan status in EU.
Filed in US Jul 2013 with orphan and breakthrough therapy status.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally
negotiated.
UKMi September 2013 Solely for use within the NHS and not for commercial use. page 48 No responsibility is accepted for the content of documents derived from this original publication.
Ibrutinib oral
Janssen-Cilag
Indication:
Chronic lymphocytic leukaemia (CLL), relapsed/ refractory - second line.
Pharmacology:
Bruton’s tyrosine kinase inhibitor – first-in-class.
Current status:
PIII in EU.
Filed in US Jul 2013.
Predicted UK launch:
2015
Reviews: NIHR HSC Jul 2013.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Chlormethine topical
Valchlor
Ceptaris Therapeutics
Indication:
Cutaneous T-cell lymphoma (CTCL),
mycosis fungoides (MF).
Current status:
PII with orphan status in EU. Licensed in US with orphan and fast track status.
Predicted UK launch:
2014
National guidance:
NICE: Skin tumours
Reviews: None.
Target population: The UK incidence of CTCL is 4 per million people. MF accounts for about 72% of CTCL. 71% of patients present with early stage disease; disease progression occurs in 34%.
Sector: Secondary care.
Implications: First-line options for early stage MF include topical therapy, radiotherapy and phototherapy. Unlicensed topical formulations of chlormethine have been used for many years but are cumbersome to prepare and use and global supply shortages have limited availability of raw ingredient. A solution licensed in France was discontinued in 2012.
Financial: As the first licensed topical formulation of chlormethine it is likely to be expensive.
Likely commissioning route: NHSE. PbR: Chemotherapy is locally
negotiated.
Pharmacology: Nitrogen mustard, an alkylating agent, formulated as a 0.02% gel applied daily.
Efficacy: In a published PII study (n=260) chlormethine 0.02% gel was compared with a 0.02% ointment formulation applied
daily for up to 12 months. The primary outcome (response rate based on composite assessment of index lesion severity) was achieved by 59% and 48% of patients, respectively, demonstrating non-inferiority.
Safety: In the above study, 20% of patients on gel and 17% on ointment withdrew due to drug-related skin irritation.
Rigosertib injection
Estybon
Baxter
Indication: Myelodysplastic syndromes, refractory/relapsed.
Pharmacology:
Phosphatidylinositol 3-kinase (PI3K) and polo-like kinase (PLK) inhibitor.
Current status:
PIII with orphan status in EU and US.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Chemotherapy is locally negotiated.
Alemtuzumab injection
Lemtrada
Genzyme
Indication:
Multiple sclerosis (MS, relapsing-remitting (RRMS) active disease defined by clinical or imaging features.
Current status:
Recommended for approval in EU Jun 2013.
Predicted UK launch:
2013
National guidance:
NICE: Multiple sclerosis (update due
Oct 2014), fingolimod, natalizumab, beta interferon and glatiramer, alemtuzumab due Apr 2014, dimethyl fumarate due Jan 2014, laquinimod due Feb 2014, teriflunomide due Jan 2014.
Reviews: No recent reviews.
Target population: In a population of 100,000, 110 people will have MS and 39 will have RRMS. 31% of these are on, or will have received, disease modifying agents. In 2011-12, there were 33,566 hospital admissions due to MS in England.
Sector: Secondary care.
Implications: This is a new class of drug for MS and as a single annual treatment may be attractive. Use is likely to be in the second-line setting.
Financial: Cost of Lemtrada may be similar to other options; beta-interferon costs up to £10,500 per year and fingolimod is around £19,500/year (PAS in place). There may be additional monitoring costs.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: Monoclonal CD52 antibody given by i.v. infusion daily for 5 days as a first annual treatment course, and as a 3 day course in the second year. An on-going extension study will help define a subsequent treatment regimen.
Efficacy: Two published PIII studies, CARE-MS 1 in 581 patients with early, active RRMS who had received no prior therapy, and CARE_MS II in 840 patients who had relapsed on prior therapy, compared alemtuzumab to high dose s.c. interferon beta-1a. Both studies met the primary outcome of relapse rate at 2 years (a 55% and 49% reduction vs. interferon, respectively, p<0.0001). CARE-MS II also met the co-primary outcome of time to 6-month sustained accumulation of disability (42% reduction vs. interferon, p=0.008), but CARE-MS I did not. Interim results from the first year of the PIII extension to the CARE-MS I & II studies suggest less than 20% of patients received a third course of alemtuzumab and 67% and 55% in the studies, respectively, remained relapse-free through to year 3.
Safety: Over 3 years, 30% of patients in the CARE studies on alemtuzumab developed autoimmune thyroid disease, 1% immune thrombocytopenia and 0.3% nephropathy. Regular monitoring for autoimmune disease may be required.
UKMi September 2013 Solely for use within the NHS and not for commercial use. page 49 No responsibility is accepted for the content of documents derived from this original publication.
Peginterferon beta-1a injection
Plegridy
Biogen Idec
Indication:
Multiple sclerosis (MS),
relapsing-remitting disease (RRMS).
Current status:
Filed in the EU Jul 2013.
Predicted UK launch:
2014
National guidance:
As for alemtuzumab above.
Reviews: NIHR HSC Sep 2012.
Target population: As for alemtuzumab above.
Sector: Initiated in secondary care.
Implications: Interferon is currently the most frequently used disease modifying agent to treat RRMS. Interferon beta-1a (Rebif) is given by s.c. injection 3 times a week. A less frequent administration schedule will be attractive to users, but it will have to complete with oral options.
Financial: Likely to be more expensive than non-pegylated interferon.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: A PEGylated form of recombinant human interferon-beta-1a given s.c. every 2 or 4 weeks.
Efficacy: The PIII ADVANCE study (n=1,516) reported a reduction in annual relapse rate at 1 year of 36% and 28% with peginterferon beta-1a given every 2 or 4 weeks, respectively (p<0.001 and p<0.02 vs. placebo). Secondary outcomes including 12-week confirmed disability progression were also met. After 1 year, patients on placebo were re-randomised to one of the peginterferon beta-1a arms for a further year. Patients then have the option of enrolling in an open-label extension study ATTAIN and followed for up to 4 years.
Safety: No unexpected safety issues reported.
Laquinimod oral
Teva
Indication:
Multiple sclerosis (MS), relapsing remitting (RRMS), first or second-line therapy.
Current status:
Filed in EU Jul 2012.
More data needed for US licensing.
Predicted UK launch:
2013
National guidance:
As for alemtuzumab above.
Reviews: NIHR HSC Aug 2011.
Target population: As for alemtuzumab above.
Sector: Secondary care.
Implications: Around 30% of patients with RRMS are on, or have received, disease modifying agents; 74% on interferons and 26% on glatiramer. NICE estimated that fingolimod, the first licensed oral preparation for RRMS, could take up to 15% of the interferon share of the market.
Financial: Beta-interferon costs up to £10,500/year and fingolimod costs about £19,500/year based on list price (PAS in place). There may be price competition as more oral agents become available.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: SAIK compound, an immune defence regulator.
Efficacy: In the published 2-year PIII ALLEGRO study (n=1,106), laquinimod 0.6mg daily reduced the mean annualised
relapse rate (ARR) vs. placebo (0.3 vs. 0.39, p=0.002) and reduced the risk of disability progression (11.1% vs. 15.7%, HR 0.64, p=0.01). The mean cumulative numbers of lesions on MRI scan were lower in the laquinimod group. In the PIII BRAVO study, laquinimod did not reduce the ARR vs. placebo whereas beta-interferon did. The on-going PIII CONCERTO study (n=1,800) is evaluating effect of laquinimod 0.6mg and 1.2mg daily on confirmed disability progression at 24 months.
Safety: Adverse events include headaches, nasopharyngitis and back pain. Increases in liver enzymes are reported.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 50 No responsibility is accepted for the content of documents derived from this original publication.
Teriflunomideoral
Aubagio
Sanofi
Indication:
Multiple sclerosis (MS),
relapsing remitting disease (RRMS) – monotherapy.
Current status:
Licensed in EU Sep 2013.
Launched in US - see prescribing information.
Predicted UK launch:
2013
National guidance:
As for alemtuzumab above.
Reviews: NIHR HSC Aug 2011.
Target population: As for alemtuzumab above.
Sector: Secondary care initiated.
Implications: Another oral option for the treatment of RRMS, at a cost likely to be lower than oral fingolimod.
Financial: In the US, teriflunomide costs slightly less than interferon beta-1a and about 30% less than fingolimod. There is a UK PAS for fingolimod.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: The active metabolite of leflunomide, teriflunomide is a dehydrogenase inhibitor.
Efficacy: In the published 2-year PIII TEMSO study (n=1,088), the annualised relapse rate (ARR) was 0.37 for patients on either 7mg or 14mg terflunomide daily vs. 0.54 for placebo (p<0.001). In the TOWER study (n=1,169), the ARR was 0.32 for teriflunomide 14mg vs. 0.50 for placebo (p<0.0001) and there was a 31.5% reduction (p=0.04 vs. placebo) in the risk of 12-week sustained accumulation of disability (SAD). Although the reduction in ARR in the 7mg group (0.39) was statistically significance vs. placebo, the 12-week SAD was not. In the PIII TENERE trial, the risk of treatment failure (primary outcome, defined as a confirmed relapse, or discontinuation of treatment for any reason) was similar among the 324 patients randomised to teriflunomide 7mg or 14mg or to beta-interferon (48.6%, 37.8% and 42.3%, respectively).
Safety: As an active metabolite of leflunomide adverse effects of teriflunomide are anticipated to be similar. See medicines.org.uk.
Dimethyl fumarate oral
Tecfidera
Biogen Idec
Indication:
Multiple sclerosis (MS), relapsing-remitting disease (RRMS) – monotherapy.
Current status:
Recommended for approval in EU Mar 2013.
Launched in US - see prescribing information.
Predicted UK launch:
2013
National guidance:
As for alemtuzumab above.
Reviews: NIHR HSC Dec 2011.
Target population: As for alemtuzumab above.
Sector: Initiated in secondary care.
Implications: The majority of patients on disease modifying agents are treated with beta-interferon which is not tolerated by many. Effective oral preparations may make treatment more convenient and acceptable, increasing the proportion of patients treated.
Financial: In the US the price for Tecfidera is between that for teriflunomide and fingolimod. There is a UK PAS in place for fingolimod.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: A derivative of fumaric acid with dual immunosuppressive and cytoprotective actions.
Efficacy: Two PIII studies, DEFINE (n=1,237) and CONFIRM (n=1,417) have been published. In DEFINE, 27% and 26% of
patients on dimethyl fumarate 240mg 2 and 3 times a day, respectively, relapsed over 2 years vs. 46% on placebo (p<0.001). The annualised relapse rates (ARR) were 0.17, 0.19 and 0.36, respectively. In CONFIRM, the ARRs for the corresponding groups were 0.22, 0.20 and 0.40 (p<0.001 vs. placebo), and in the glatiramer arm, 0.29 (p<0.01 vs. placebo). In a post-hoc analysis, 3- times daily dimethyl fumarate was more effective than glatiramer in reducing the ARR (p<0.05). Active treatment was associated with a reduction in disability progression vs. placebo (34-38% p=0.01) in DEFINE but not CONFIRM. There were fewer new gadolinium enhancing lesions with active treatment in both studies.
Safety: Flushing and gastrointestinal effects are the most frequent adverse events.
Daclizumab injection
Zenapax
Biogen
Indication:
Multiple sclerosis,
relapsing-remitting.
Pharmacology:
Interleukin 2 receptor antagonist, humanised monoclonal antibody that binds to CD25.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: NHSE.
PbR: Specified high cost drug.
Fingolimod oral
Gilenya
Novartis
Indication:
Multiple sclerosis, primary
progressive.
Pharmacology:
Oral sphingosine-1 phosphate receptor modulator.
Current status:
PIII.
Predicted UK licence extension:
2015
Reviews: No recent reviews.
Likely commissioning route: NHSE.
PbR: Specified high cost drug.
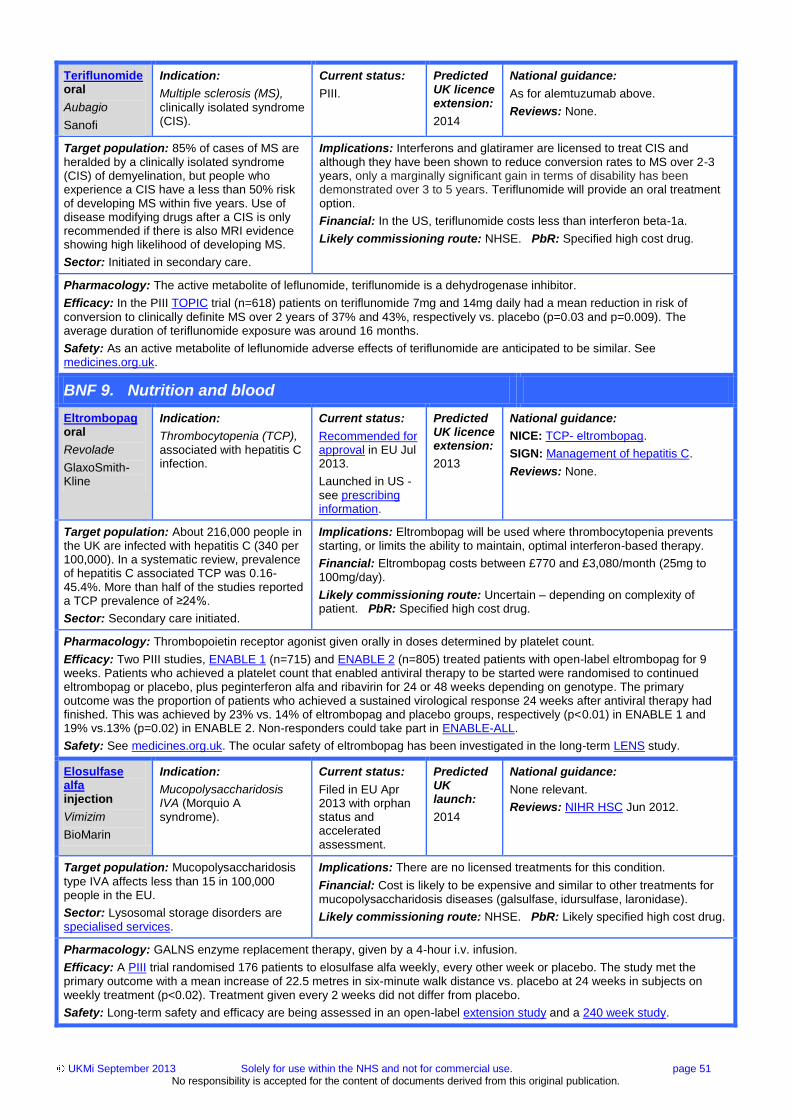
UKMi September 2013 Solely for use within the NHS and not for commercial use. page 51 No responsibility is accepted for the content of documents derived from this original publication.
Teriflunomide oral
Aubagio
Sanofi
Indication:
Multiple sclerosis (MS),
clinically isolated syndrome (CIS).
Current status:
PIII.
Predicted UK licence extension:
2014
National guidance:
As for alemtuzumab above.
Reviews: None.
Target population: 85% of cases of MS are heralded by a clinically isolated syndrome (CIS) of demyelination, but people who experience a CIS have a less than 50% risk of developing MS within five years. Use of disease modifying drugs after a CIS is only recommended if there is also MRI evidence showing high likelihood of developing MS.
Sector: Initiated in secondary care.
Implications: Interferons and glatiramer are licensed to treat CIS and although they have been shown to reduce conversion rates to MS over 2-3 years, only a marginally significant gain in terms of disability has been demonstrated over 3 to 5 years. Teriflunomide will provide an oral treatment option.
Financial: In the US, teriflunomide costs less than interferon beta-1a.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: The active metabolite of leflunomide, teriflunomide is a dehydrogenase inhibitor.
Efficacy: In the PIII TOPIC trial (n=618) patients on teriflunomide 7mg and 14mg daily had a mean reduction in risk of
conversion to clinically definite MS over 2 years of 37% and 43%, respectively vs. placebo (p=0.03 and p=0.009). The average duration of teriflunomide exposure was around 16 months.
Safety: As an active metabolite of leflunomide adverse effects of teriflunomide are anticipated to be similar. See medicines.org.uk.
BNF 9. Nutrition and blood
Eltrombopag oral
Revolade
GlaxoSmith-Kline
Indication:
Thrombocytopenia (TCP), associated with hepatitis C infection.
Current status:
Recommended for approval in EU Jul 2013.
Launched in US - see prescribing information.
Predicted UK licence extension:
2013
National guidance:
NICE: TCP- eltrombopag.
SIGN: Management of hepatitis C.
Reviews: None.
Target population: About 216,000 people in the UK are infected with hepatitis C (340 per 100,000). In a systematic review, prevalence of hepatitis C associated TCP was 0.16- 45.4%. More than half of the studies reported a TCP prevalence of ≥24%.
Sector: Secondary care initiated.
Implications: Eltrombopag will be used where thrombocytopenia prevents starting, or limits the ability to maintain, optimal interferon-based therapy.
Financial: Eltrombopag costs between £770 and £3,080/month (25mg to 100mg/day).
Likely commissioning route: Uncertain – depending on complexity of patient. PbR: Specified high cost drug.
Pharmacology: Thrombopoietin receptor agonist given orally in doses determined by platelet count.
Efficacy: Two PIII studies, ENABLE 1 (n=715) and ENABLE 2 (n=805) treated patients with open-label eltrombopag for 9 weeks. Patients who achieved a platelet count that enabled antiviral therapy to be started were randomised to continued eltrombopag or placebo, plus peginterferon alfa and ribavirin for 24 or 48 weeks depending on genotype. The primary outcome was the proportion of patients who achieved a sustained virological response 24 weeks after antiviral therapy had finished. This was achieved by 23% vs. 14% of eltrombopag and placebo groups, respectively (p<0.01) in ENABLE 1 and 19% vs.13% (p=0.02) in ENABLE 2. Non-responders could take part in ENABLE-ALL.
Safety: See medicines.org.uk. The ocular safety of eltrombopag has been investigated in the long-term LENS study.
Elosulfase alfa injection
Vimizim
BioMarin
Indication:
Mucopolysaccharidosis IVA (Morquio A syndrome).
Current status:
Filed in EU Apr 2013 with orphan status and accelerated assessment.
Predicted UK launch:
2014
National guidance:
None relevant.
Reviews: NIHR HSC Jun 2012.
Target population: Mucopolysaccharidosis
type IVA affects less than 15 in 100,000 people in the EU.
Sector: Lysosomal storage disorders are specialised services.
Implications: There are no licensed treatments for this condition.
Financial: Cost is likely to be expensive and similar to other treatments for mucopolysaccharidosis diseases (galsulfase, idursulfase, laronidase).
Likely commissioning route: NHSE. PbR: Likely specified high cost drug.
Pharmacology: GALNS enzyme replacement therapy, given by a 4-hour i.v. infusion.
Efficacy: A PIII trial randomised 176 patients to elosulfase alfa weekly, every other week or placebo. The study met the primary outcome with a mean increase of 22.5 metres in six-minute walk distance vs. placebo at 24 weeks in subjects on weekly treatment (p<0.02). Treatment given every 2 weeks did not differ from placebo.
Safety: Long-term safety and efficacy are being assessed in an open-label extension study and a 240 week study.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 52 No responsibility is accepted for the content of documents derived from this original publication.
Alipogene tiparvovec injection
Glybera
Chiesi
Indication:
Lipoprotein lipase deficiency, familial, in adults with pancreatitis despite dietary restrictions.
Current status:
Licensed in EU Oct 2012 with orphan status –see prescribing information.
Predicted UK launch:
2013 via a restricted access programme
National guidance:
None relevant.
Reviews: No recent reviews.
Target population: An estimated 30 - 50
people in the UK may be eligible for treatment in the next 5 years.
Sector: Secondary care.
Implications: Dietary restriction is currently the only management option.
Diagnosis has to be confirmed by genetic testing. Patients must adhere to a lipid-restricted diet and need short-term (12 weeks) immunosuppression with ciclosporin and mycophenolate mofetil. The product contains genetically-modified organisms requiring use of biosafety procedures.
Financial: Likely to be expensive.
Likely commissioning route: NHSE. PbR: Likely specified high cost drug.
Pharmacology: Single treatment gene therapy given by i.m. injection at multiple-sites in a single session. It is delivered
frozen in a patient-specific pack containing the correct amount of vials per patient, calculated according to weight.
Efficacy: In a published PII/III study (n=14), alipogene was administered as multiple injections into leg muscles on a single occasion under spinal anaesthesia. All patients maintained a low fat diet. 50% achieved the primary outcome of at least 40% reduction in triglycerides vs. baseline 3 to 12 weeks after dosing. In a published PII/III study, 5 patients received 1 x 10
12
gc/kg. 14 weeks after injection, mean total plasma triglyceride levels fell by about 60% (p<0.01 vs. controls). All patients in the above trials have entered continuation studies lasting several years.
Safety: In the PII/III study of 14 patients, 12 (86%) had injection site events.
Sodium phenyl-butyrate oral granules
Pheburane
Lucane Pharma
Indication:
Urea cycle disorders.
Current status:
Licensed in EU Aug 2013 - see prescribing information.
Predicted UK launch:
2013
National guidance:
None relevant.
Reviews: SMC due Nov 2013.
Target population: In the EU less than 2 per
million people are affected.
Sector: Urea cycle disorders are a specialised service.
Implications: Sodium phenylbutyrate Ammonaps (940mg/g) granules are already available. Pheburane contains less sodium phenylbutyrate per gram (483mg/g) due to a coating used to mask the unpleasant taste. This tasteless formulation is designed to improve compliance.
Financial: Cost of Ammonaps is £860 for 250g sodium phenylbutyrate. Likelihood for better compliance may increase the price of Pheburane.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: A conjugated metabolite is excreted in the urine, leading to reduced nitrogen and ammonia levels.
Efficacy: A bioequivalence study between Pheburane 483 mg/g granules and Ammonaps 940mg/g granules was submitted in the licence application. As Ammonaps is the reference product, no new clinical studies are needed.
Safety: See medicines.org.uk for Ammonaps, and prescribing information for Phenburane.
Sebelipase alfa injection
Synageva BioPharma
Indication:
Lysosomal acid lipase deficiency.
Pharmacology:
Recombinant human lysosomal acid lipase.
Current status:
PIII with orphan status in EU and US and breakthrough therapy status in US.
Predicted UK launch:
2015
Reviews: NIHR HSC Jun 2012.
Likely commissioning route: NHSE.
PbR: Likely specified high cost drug.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 53 No responsibility is accepted for the content of documents derived from this original publication.
BNF 10. Musculoskeletal and joint diseases
Canakinumab injection
Ilaris
Novartis
Indication:
Juvenile idiopathic arthritis (JIA), systemic disease in patients aged ≥ 2 years with inadequate response to NSAIDs and systemic corticosteroids.
Current status:
Recommended for approval in EU Jul 2013 with orphan status. Launched in US - see prescribing information.
Predicted UK licence extension:
2013
National guidance:
NICE: JIA - etanercept, tocilizumab
Reviews: No recent reviews.
Target population: NICE estimate the target population for tocilizumab in JIA is around 372 individuals in England.
Sector: Secondary care.
Implications: Likely to be a competitor to tocilizumab, with more convenient administration (s.c. vs. i.v.) but much higher price.
Financial: Monthly cost for 30kg child of canakinumab is nearly £10,000 (single dose of 4mg/kg) assuming no vial sharing vs. about £700 for tocilizumab (two doses of 8mg/kg); a PAS is in place for tocilizumab for JIA.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: Interleukin-1 beta inhibitor, given by s.c. injection. In the US it is given every 4 weeks.
Efficacy: Two PIII trials published together (β-SPECIFIC 1 and 2) examined single dose (β-SPECIFIC 1, n=84) and longer-term (β-SPECIFIC 2, n=177) efficacy in patients aged 2 to 19 years. In β-SPECIFIC 1, the primary outcome (an adapted JIA ACR 30 response) was achieved by 84% patients on canakinumab, vs. 10% on placebo (p<0.001) by day 15. The β-SPECIFIC 2 study started with an open-label phase; those who responded and achieved steroid tapering by 32 weeks (n=100) were randomised to a placebo-controlled withdrawal phase. Risk of flare was lower for those on canakinumab vs. those switched to placebo; 74% on canakinumab had no flare vs. 25% in the placebo group (HR 0.36, p=0.003, NNT=2).
Safety: See medicines.org.uk. In clinical trials, there were 7 cases of macrophage activation syndrome.
Golimumab injection
Simponi
MSD
Indication:
Juvenile idiopathic arthritis (JIA), polyarticular, poor response to methotrexate.
Current status:
PIII.
Predicted UK licence extension:
2014
National guidance:
As for canakinumab above.
Reviews: None.
Target population: NICE estimate around 600 children with polyarticular JIA would be eligible for etanercept, of whom over 300 would be maintained on it long-term.
Sector: Secondary care.
Implications: A competitor to etanercept with the advantage of once-monthly dosing vs. twice-monthly dosing for etanercept.
Financial: Golimumab is currently more expensive than etanercept and the etanercept patent expires in 2015; biosimilar formulations are in development. A PAS is in place for golimumab use in adults with arthritis and for tocilizumab for systemic JIA.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: A monoclonal TNF-alpha inhibitor, given by monthly s.c. injection.
Efficacy: In the PIII GO-KIDS study, 173 patients with JIA aged under 16 at diagnosis, at least 5 involved joints, and poor response to methotrexate were randomised to monthly golimumab 30mg/m
2 or placebo after a 16-week open-label run-in to
identify those showing at least 30% response to golimumab. Primary outcome is disease flare between weeks 16 to 48 with results due in 2013.
Safety: See medicines.org.uk.
Masitinib oral
AB Science
Indication:
Rheumatoid arthritis not
responding to standard therapy.
Pharmacology:
Protein kinase inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: None.
Likely commissioning route: CCG.
PbR: Likely specified high cost drug.
Secukinumab injection
Novartis
Indication:
Rheumatoid arthritis, when TNF-alpha inhibitors are ineffective or not tolerated.
Pharmacology:
Monoclonal interleukin IL-17A inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: NIHR HSC Sep 2012.
Likely commissioning route: CCG.
PbR: Likely specified high cost drug.
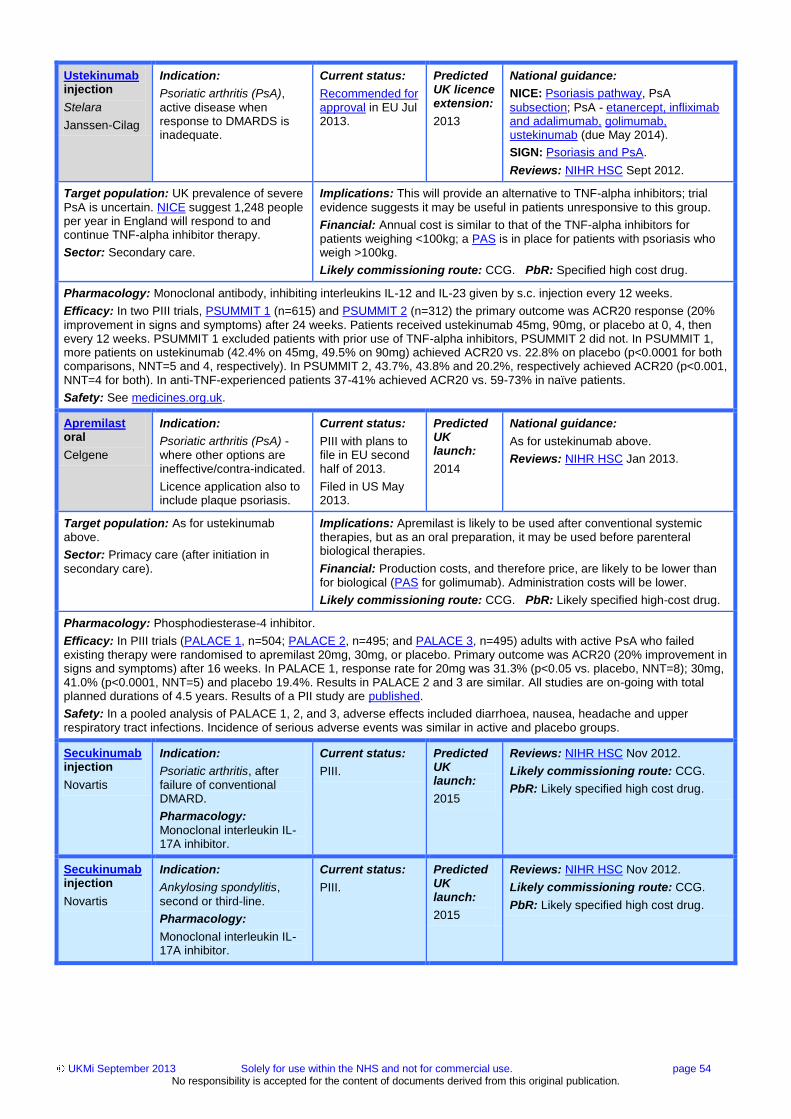
UKMi September 2013 Solely for use within the NHS and not for commercial use. page 54 No responsibility is accepted for the content of documents derived from this original publication.
Ustekinumab injection
Stelara
Janssen-Cilag
Indication:
Psoriatic arthritis (PsA),
active disease when response to DMARDS is inadequate.
Current status:
Recommended for approval in EU Jul 2013.
Predicted UK licence extension:
2013
National guidance:
NICE: Psoriasis pathway, PsA
subsection; PsA - etanercept, infliximab and adalimumab, golimumab, ustekinumab (due May 2014).
SIGN: Psoriasis and PsA.
Reviews: NIHR HSC Sept 2012.
Target population: UK prevalence of severe
PsA is uncertain. NICE suggest 1,248 people per year in England will respond to and continue TNF-alpha inhibitor therapy.
Sector: Secondary care.
Implications: This will provide an alternative to TNF-alpha inhibitors; trial
evidence suggests it may be useful in patients unresponsive to this group.
Financial: Annual cost is similar to that of the TNF-alpha inhibitors for patients weighing <100kg; a PAS is in place for patients with psoriasis who weigh >100kg.
Likely commissioning route: CCG. PbR: Specified high cost drug.
Pharmacology: Monoclonal antibody, inhibiting interleukins IL-12 and IL-23 given by s.c. injection every 12 weeks.
Efficacy: In two PIII trials, PSUMMIT 1 (n=615) and PSUMMIT 2 (n=312) the primary outcome was ACR20 response (20%
improvement in signs and symptoms) after 24 weeks. Patients received ustekinumab 45mg, 90mg, or placebo at 0, 4, then every 12 weeks. PSUMMIT 1 excluded patients with prior use of TNF-alpha inhibitors, PSUMMIT 2 did not. In PSUMMIT 1, more patients on ustekinumab (42.4% on 45mg, 49.5% on 90mg) achieved ACR20 vs. 22.8% on placebo (p<0.0001 for both comparisons, NNT=5 and 4, respectively). In PSUMMIT 2, 43.7%, 43.8% and 20.2%, respectively achieved ACR20 (p<0.001, NNT=4 for both). In anti-TNF-experienced patients 37-41% achieved ACR20 vs. 59-73% in naïve patients.
Safety: See medicines.org.uk.
Apremilast oral
Celgene
Indication:
Psoriatic arthritis (PsA) - where other options are ineffective/contra-indicated.
Licence application also to include plaque psoriasis.
Current status:
PIII with plans to file in EU second half of 2013.
Filed in US May 2013.
Predicted UK launch:
2014
National guidance:
As for ustekinumab above.
Reviews: NIHR HSC Jan 2013.
Target population: As for ustekinumab above.
Sector: Primacy care (after initiation in
secondary care).
Implications: Apremilast is likely to be used after conventional systemic therapies, but as an oral preparation, it may be used before parenteral biological therapies.
Financial: Production costs, and therefore price, are likely to be lower than for biological (PAS for golimumab). Administration costs will be lower.
Likely commissioning route: CCG. PbR: Likely specified high-cost drug.
Pharmacology: Phosphodiesterase-4 inhibitor.
Efficacy: In PIII trials (PALACE 1, n=504; PALACE 2, n=495; and PALACE 3, n=495) adults with active PsA who failed existing therapy were randomised to apremilast 20mg, 30mg, or placebo. Primary outcome was ACR20 (20% improvement in signs and symptoms) after 16 weeks. In PALACE 1, response rate for 20mg was 31.3% (p<0.05 vs. placebo, NNT=8); 30mg, 41.0% (p<0.0001, NNT=5) and placebo 19.4%. Results in PALACE 2 and 3 are similar. All studies are on-going with total planned durations of 4.5 years. Results of a PII study are published.
Safety: In a pooled analysis of PALACE 1, 2, and 3, adverse effects included diarrhoea, nausea, headache and upper respiratory tract infections. Incidence of serious adverse events was similar in active and placebo groups.
Secukinumab injection
Novartis
Indication:
Psoriatic arthritis, after failure of conventional DMARD.
Pharmacology:
Monoclonal interleukin IL-17A inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: NIHR HSC Nov 2012.
Likely commissioning route: CCG.
PbR: Likely specified high cost drug.
Secukinumab injection
Novartis
Indication:
Ankylosing spondylitis,
second or third-line.
Pharmacology:
Monoclonal interleukin IL-17A inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: NIHR HSC Nov 2012.
Likely commissioning route: CCG.
PbR: Likely specified high cost drug.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 55 No responsibility is accepted for the content of documents derived from this original publication.
Pegloticase injection
Krystexxa
Savient
Indication:
Gout prophylaxis, where
xanthine oxidase inhibitors have failed or are contra-indicated.
Current status:
Licensed in EU Jan 2013 – see prescribing information.
Predicted UK launch:
2013
National guidance:
NICE: Pegloticase Jun 2013.
Reviews: No recent reviews.
Target population: The manufacturer estimates about 2,700 people in England and Wales may be eligible; NICE estimates that the guidance would affect about 8 people per 100,000 in England.
Sector: Secondary care.
Implications: NICE does not currently recommend pegloticase as, although effective at lowering urate levels, it is not cost-effective at the £30,000 per QALY threshold and can cause serious adverse reactions. It would be a competitor to canakinumab (also not recommended by NICE).
Financial: Pegloticase cost is £1,770 per vial (about £23,000 for 6 months therapy) and would require fortnightly day case admission as infusion plus minimum observation period for severe allergic reactions is 3.5 hours. Canakinumab cost is about £1,000 per dose (max. 2 doses in 6 months).
Likely commissioning route: CCG. PbR: Specified high cost drug.
Pharmacology: A polyethylene glycol conjugate of recombinant uricase given by a 2-hour i.v. infusion every 2 weeks.
Efficacy: The published PIII GOUT1 and 2 studies randomised 225 patients to pegloticase bi-weekly or monthly, or placebo, for 6 months. The primary outcome, plasma uric acid <6.0mg/dL 80% of the time at 3 and 6 months, was met in GOUT1 by 47% of patients (bi- weekly, p<0.001) and 20% (monthly, p<0.05) and in GOUT2 by 38% (p=0.001) and 49% (p<0.001), respectively.
Safety: Anaphylaxis (including anaphylactic shock) in about 6.5% of patients and infusion reactions (26%) are reported; premedication with antihistamines and corticosteroids is mandated in prescribing information.
Lesinurad oral
AstraZeneca
Indication:
Gout, second-line.
Pharmacology:
Selective urate transporter-1 inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: NIHR HSC Jan 2013.
Likely commissioning route: CCG.
PbR: Likely HRG included.
Odanacatib oral
MSD
Indication:
Osteoporosis in men when
bisphosphonates contra-indicated or not successful.
Pharmacology:
Selective cathepsin-K inhibitor.
Current status:
PIII.
Predicted UK launch:
2015
Reviews: NIHR HSC Jun 2013.
Likely commissioning route: CCG.
PbR: Likely HRG included.
Ataluren oral
Translarna
PTC Therapeutics
Indication:
Duchenne muscular dystrophy, nonsense-
mutation (nmDMD).
Current status:
Filed in EU Dec 2012 with orphan status.
Predicted UK launch:
2013
National guidance:
None relevant.
Reviews: No recent reviews.
Target population: DMD affects 1 in 3,600
to 6,000 male births in the UK; about 100 boys are diagnosed annually and UK prevalence is about 1,500. Around 10-15% have a nonsense mutation (nm), corresponding to 150-195 patients in the UK who may be eligible.
Sector: Secondary care.
Implications: Current options (corticosteroids) can delay but not prevent
loss of walking ability. Ataluren is the first therapy to target the underlying defect in nmDMD, but will benefit only a small proportion of all DMD patients. It is likely to be additional to current therapy in ambulant patients but could prolong independence and delay complications.
Financial: Likely to be expensive.
Likely commissioning route: NHSE. PbR: Likely specified high cost drug.
Pharmacology: Dystrophin synthesis stimulant, mechanism of action is uncertain.
Efficacy: Licence application is based on a PII trial in boys (n=174) with nm Duchenne or Becker MD, aged ≥5 years treated with 40mg/kg or 80mg/kg ataluren daily or placebo. At week 48, mean change from baseline in the primary outcome of 6-minute walk distance failed to reach statistical significance for both doses. However, post-hoc secondary analyses suggest there may be a benefit with the lower dose. A larger PIII study (n=220 target) is in progress.
Safety: Ataluren was well tolerated in trials.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 56 No responsibility is accepted for the content of documents derived from this original publication.
Idebenone oral
Sovrima
Takeda
Indication:
Duchenne muscular dystrophy (DMD).
Current status:
PIII with orphan status.
Predicted UK launch:
2014
National guidance:
None relevant.
Reviews: None.
Target population: As for ataluren above. Patients are living longer due to intensive symptomatic respiratory and cardiac support.
Sector: Secondary care.
Implications: Unlike ataluren above, if licensed, idebenone would potentially be suitable for all affected patients with DMD.
Financial: Likely to be expensive.
Likely commissioning route: NHSE. PbR: Likely specified high cost drug.
Pharmacology: Coenzyme Q10 analogue that enhances mitochondrial respiratory chain function.
Efficacy: The on-going PIII DELOS study compares idebenone 900mg daily with placebo in 260 boys aged 10 to 18 years.
The primary outcome is percentage change in predicted peak expiratory flow as a measure of respiratory function, over 52 weeks. Trial completion is expected late 2013. The PII DELPHI trial (n=21) results have been published. Idebenone 450mg daily did not show a significant difference from placebo at 12 months in the primary outcome of effect on peak systolic radial strain in the left ventricular inferolateral wall, the region of the heart that is earliest and most severely affected in DMD. Patients completing DELPHI entered the open-label DELPHI-extension study and received 450mg or 900mg (based on weight) for 24 months. This study completed in 2011 but results have yet to be published.
Safety: Idebenone has been well tolerated in trials.
BNF 11. Eye
Aflibercept intravitreal injection
Eylea
Bayer
Indication:
Macular oedema, secondary to central retinal vein occlusion (CRVO).
Current status:
Recommended for approval in EU Jul 2013.
Launched in US - see prescribing information.
Predicted UK licence extension:
2013
National guidance:
NICE: Aflibercept due Apr 2014,
ranibizumab, costing template, dexamethasone.
Reviews: NIHR HSC May 2011.
Target population: RVO affects 1–2% of
people aged over 40 years. In England and Wales about 17 per 100,000 people will require treatment for macular oedema following CRVO annually.
Sector: Secondary care.
Implications: A new treatment option that will compete with ranibizumab
injection and dexamethasone implant.
Financial: Based on current prices, aflibercept cost is £816/month and dexamethasone implant cost is £870. PASs are in place for ranibizumab for wet age-related macular degeneration and diabetic macular oedema.
Likely commissioning route: CCG. PbR: Specified high cost drug.
Pharmacology: Vascular endothelial growth factor inhibitor (VEGF) and placental growth factor inhibitor given monthly.
Efficacy: In the published PIII GALILEO study (n=177), at 6-months, 60.2% on aflibercept 2mg monthly and 22.1% on
control treatment, gained ≥15 letters of vision from baseline (p<0.01). The mean number of letters gained was 18 vs. 3.3, respectively (p<0.01). In the published PIII COPERNICUS (n=189), at 6 months, ≥15 letters were gained by 56.1% on aflibercept vs. 12.3% on placebo (p<0.01). Those on aflibercept gained a mean of 17.3 letters vs. a mean loss of 4 letters with placebo, p<0.01. From week 24 to week 52, all patients received aflibercept as needed. At 12 months, ≥15 letters were gained by 55.3% on aflibercept vs. 30.1% on placebo (p<0.01). Those on aflibercept gained a mean of 16.2 letters vs. a mean of 3.8 letters with placebo, p<0.01.
Safety: See medicines.org.uk.
Aflibercept intravitreal injection
Eylea
Bayer
Indication:
Diabetic macular oedema (DMO).
Current status:
PIII.
Predicted UK licence extension:
2014.
National guidance:
NICE: Diabetes pathway, quality
standard, fluocinolone implant (rapid review due Nov 2013) ranibizumab, costing template.
Reviews: NIHR HSC Jun 2013, LNDG
Feb 2011.
Target population: About 322 patients with
diabetes have DMO per 100,000 people. 39% of these have clinically significant macular oedema, which can lead to blindness.
Sector: Secondary care.
Implications: A new treatment option that will compete with ranibizumab.
Financial: As for aflibercept above.
Likely commissioning route: CCG. PbR: Specified high cost drug.
Pharmacology: Vascular endothelial growth factor inhibitor (VEGF) and placental growth factor inhibitor given monthly.
Efficacy: The 12-month results of the PIII VIVID-DME and VISTA-DME trials of aflibercept 2mg monthly vs. aflibercept every
2 months vs. laser photocoagulation are available. In VIVID-DME mean change from baseline in best corrected visual acuity was 10.5 letters, 10.7 letters and 1.2 letters in the three groups, respectively. The results for VISTA-DME were 12.5, 10.7 and 0.2 letters, respectively (p<0.01 for both trials, both aflibercept groups vs. laser).
Safety: See medicines.org.uk.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 57 No responsibility is accepted for the content of documents derived from this original publication.
Aflibercept intravitreal injection
Eylea
Bayer
Indication:
Macular oedema,
secondary to branch retinal vein occlusion (BRVO).
Pharmacology:
As for aflibercept above.
Current status:
PIII.
Predicted UK licence extension:
2015
Reviews: None.
Likely commissioning route: CCG.
PbR: Specified high cost drug.
BNF 13. Skin
Apremilast oral
Celgene
Indication:
Psoriasis, plaque, moderate to severe.
Current status:
PIII.
Predicted UK launch:
2014
National guidance:
NICE: Psoriasis pathway, assessment
and management, commissioning guide, costing report, quality standards; ustekinumab , adalimumab, infliximab, efalizumab and etanercept.
SIGN: Psoriasis.
Reviews: NIHR HSC Jan 2013.
Target population: Estimated prevalence of psoriasis in England is 1.63%; about 20% of people have moderate to severe disease (20 per 100,000). Plaque psoriasis is the most common form, affecting 80-90% of people. It is estimated 1.1% of people with psoriasis are eligible for biological treatment (7,100).
Sector: Primary and secondary care.
Implications: Likely to be licensed for use after conventional systemic therapies, but as an oral preparation may be considered for use before parenteral biological therapies. However, unlike established therapies, long -term efficacy and safety data are lacking.
Financial: Production costs, and therefore drug price, are likely to be lower than for biologicals (which cost £8,000-£11,000/year). Administration costs will also be lower.
Likely commissioning route: CCG. PbR: Likely specified high cost drug.
Pharmacology: Inhibitor of type-4 cyclic nucleotide phosphodiesterase (PDE-4).
Efficacy: On-going studies of apremilast vs. placebo include PIII ESTEEM 1 and 2 (n=1,257 combined) and a PIIIb study
(n=240) vs. etanercept and placebo. The PIIIb study has enrolled only biological-naïve patients. In a published PIIb study (n=352) the primary outcome, 75% reduction in Psoriasis Area and Severity Index (PASI 75) at week 16, was achieved in 41% of patients on apremilast vs. 6% on placebo (p<0.0001). In ESTEEM 1, PASI 75 at 16 weeks was achieved by 33.1% of patients on apremilast vs. 5.3% on placebo (p<0.0001). Higher scores were seen in systemic- and biologic-naïve subjects vs. placebo (38.7% vs. 7.6%; p<0.0001 and 35.8% vs. 5.9%; p<0.0001, respectively).
Safety: No major safety issues have been reported.
Tofacitinib oral
Xeljanz
Pfizer
Indication:
Psoriasis, plaque,
moderate to severe.
Current status:
PIII.
Predicted UK launch:
2014
National guidance:
As for apremilast above.
Reviews: NIHR HSC Nov 2012.
Target population: As for apremilast above.
Sector: Primary and secondary care.
Implications: Tofacitinib will compete with other second line treatments in
adults who are candidates for systemic therapy. It has the advantage of oral administration but safety concerns may be an issue. This may limit its use to patients who have failed on an established biological.
Financial: In the US, it has been priced about 7% cheaper ($24,666 a year)
compared to etanercept and adalimumab.
Likely commissioning route: CCG. PbR: Specified high cost drug.
Pharmacology: An immunosuppressant, janus kinase (JAK) 3 inhibitor (5 or 10mg twice daily).
Efficacy: Completed PIII studies include two 1-year placebo controlled trials (1 & 2 both n=825) with Physician´s Global Assessment (PGA) and PASI 75 response at week 16 as the co-primary outcomes, a 12-week trial (n=1,100) vs. etanercept with a primary outcome of PGA, and a withdrawal and re-treatment study (n=684). An open-label long-term safety study (n=3,200) is on-going. In a published PIIb dose-ranging study (2, 5 and 15mg twice daily), PASI 75 at week 12, was reported in 25%, 41% and 67% of patients, respectively, vs. 2% in patients on placebo.
Safety: Major concerns about its overall safety profile including serious infections, certain cancers, gastro-intestinal perforations, liver damage and hyperlipidaemia were among the reasons the CHMP recommended against approval in the EU for rheumatoid arthritis in April 13.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 58 No responsibility is accepted for the content of documents derived from this original publication.
Secukinumab injection
Novartis
Indication:
Psoriasis, plaque,
moderate to severe.
Current status:
PIII.
Predicted UK launch:
2014
National guidance:
As for apremilast above.
Reviews: NIHR HSC Apr 2012.
Target population: As for apremilast above.
Sector: Secondary care.
Implications: Secukinumab targets a different immunological mediator to
currently available biological therapies and is likely to be used as an alternative to existing biologicals in patients who have failure, contraindication or intolerance to standard systemic treatments.
Financial: Likely to be around the same price as other biologicals (£8,000-
£11,000/year).
Likely commissioning route: CCG. PbR: Likely specified high cost drug.
Pharmacology: First-in-class fully human monoclonal interleukin-17A (IL-17A) antibody given by s.c .injection as 5, weekly loading doses then monthly maintenance doses (150 or 300mg).
Efficacy: There are a number of on-going PIII studies, including four 1-year studies, FIXTURE (n=1,264), ERASURE (n=720), FEATURE (n=171) and JUNCTURE (n=171). The latter two use autoinjectors; only one study, FIXTURE, has an active control arm (etanercept). The primary outcomes are PASI scores and Investigators´ Global Assessment (IGA) at week 12. Two on-going PIII extension studies (n=1,220 and n=740) are collecting 2 additional years of data from either continuous or interrupted treatment regimens. Three PII dose-ranging studies have been published (one, two, three) showing effectiveness in induction and maintenance, but did not employ the regimen adopted in PIII studies.
Safety: Neutropenia has been reported.
Propranolol oral
Pierre Fabre
Indication:
Infantile haemangioma (IH), proliferating, requiring systemic therapy.
Current status:
Filed in EU Apr 2013.
Predicted UK launch:
2014
National guidance:
None relevant.
Reviews: None.
Target population: Around 3-5% of infants may be affected by IH and about 10% of these may require treatment during the proliferative stage, equating to about 6 cases per 100,000 people per year.
Sector: Secondary care.
Implications: This will be the first drug licensed for this indication which may lead to more affected infants being considered for treatment.
Financial: Likely to cost considerably more than currently used unlicensed
alternatives such as corticosteroids and propranolol products.
Likely commissioning route: CCG. PbR: Likely HRG included.
Pharmacology: Beta-blocker.
Efficacy: A published PII trial compared propranolol or placebo for 6 months in 40 children aged between 9 weeks and 5 years with facial IH or IH at sites with potential for disfigurement. At week 24 the reduction in IH volume was 60% vs.14%, respectively (p=0.01). A PIII trial (n=460) has been completed but has yet to be published. A systematic review of uncontrolled trials reported a response rate over 90%.
Safety: See medicines.org.uk. Cardiac monitoring may be required.
Afamelanotide implant
Scenesse
Clinuvel
Indication:
Erythropoietic protoporphyria (EPP).
Current status:
Filed in EU Feb 2012 with orphan status. Launched in Italy (2010) and Switzerland (2012).
Predicted UK launch:
2013
National guidance:
None relevant.
Reviews: No recent reviews.
Target population: EPP affects <2 per 100,000 people in the EU. Protoporphyrin accumulates in the skin and causes severe photosensitivity with sun exposure leading to burning, erythema and pain.
Sector: Secondary or tertiary care.
Implications: There are no other specific EPP treatments. Options include staying indoors, sun-blocking clothes and sunscreen.
Financial: Likely to be expensive.
Likely commissioning route: NHSE. PbR: Specified high cost drug.
Pharmacology: Synthetic analogue of alpha-melanocyte-stimulating hormone which induces the synthesis of melanin. Given as a controlled release dissolvable s.c implant.
Efficacy: In the PIII CUV029 study 74 patients received afamelanotide or placebo once every 60 days, over 9 months. Afamelanotide was associated with fewer phototoxic reactions measured by visual analogue scale (primary outcome; p=0.044) and a lower total median pain score (secondary outcome; 6.0 vs. 17.5, p=0.035). In the 12-month PIII CUV017 crossover trial 91 patients received afamelanotide or placebo implants every 2 months. Afamelanotide reduced the total number of days on which patients experienced pain (p<0.003) and all individual daily pain scores were lower vs. placebo (p<0.002). The US PIII CUV039 study (n=93) completed in April 2013 but results have not yet been made public. The EMA has delayed its decision on approval, possibly waiting for the results of this study.
Safety: No specific concerns have been identified.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 59 No responsibility is accepted for the content of documents derived from this original publication.
BNF 14. Vaccines
Meningo-coccal group-B vaccine injection
Bexsero
Novartis
Indication:
Meningococcal B disease (MenB) immunisation, invasive disease caused by Neisseria meningitidis group B in subjects >2 months old.
Current status:
Licensed in the EU Jan 2013 - see prescribing information.
Predicted UK launch:
2013/2014
National guidance:
DH routine vaccination schedule 2013/14.
JCVI recommendation Jun 2013.
Reviews: None.
Target population: In the UK, the number of
cases of meningitis has halved over the last decade to around 25 per 100,000 in children <1 year of age and to <2 per 100,000 in all ages. Around 80% were caused by MenB. In 2011/12, there were 613 lab-confirmed cases of MenB and 33 deaths. Around 1 in 10 who survive will suffer major disabilities.
Sector: Primary care.
Implications: Surveys suggest the vaccine may cover around 73% of MenB
strains circulating in the UK. Although the vaccine has been shown to induce an immune response, effectiveness against invasive MenB disease has not been established.
Financial: The Joint Committee on Vaccination and Immunisation (JCVI) has recommended against including this in the routine immunisation programme as they do not consider it likely to be cost effective.
Likely commissioning route: CCG. PbR: Not applicable.
Pharmacology: Quadrivalent vaccine (4CMenB) given as a 2 or 3 dose course, possibly followed by a booster dose.
Efficacy: Results of a primary and booster PIII study have been published. In the primary study, 3,630 infants received routine vaccinations at 2, 4 and 6 months of age, either alone or with MenB vaccine. One month after the final dose, 84-100% of infants had a serological response to 4 reference MenB strains, without a clinically significant effect on the immunogenicity of routine vaccines. In the booster phase, 1,555 subjects aged 12 months received MenB vaccine either with or 1 month prior to MMR varicella-zoster virus vaccine. Over 95% showed a protective response to all four MenB vaccine components. A further PII/III study in infants which met all primary outcomes has been published. On-going studies are assessing persistence of antibody levels 5 years post-vaccination, and efficacy in children, adolescents and young adults.
Safety: See prescribing information.
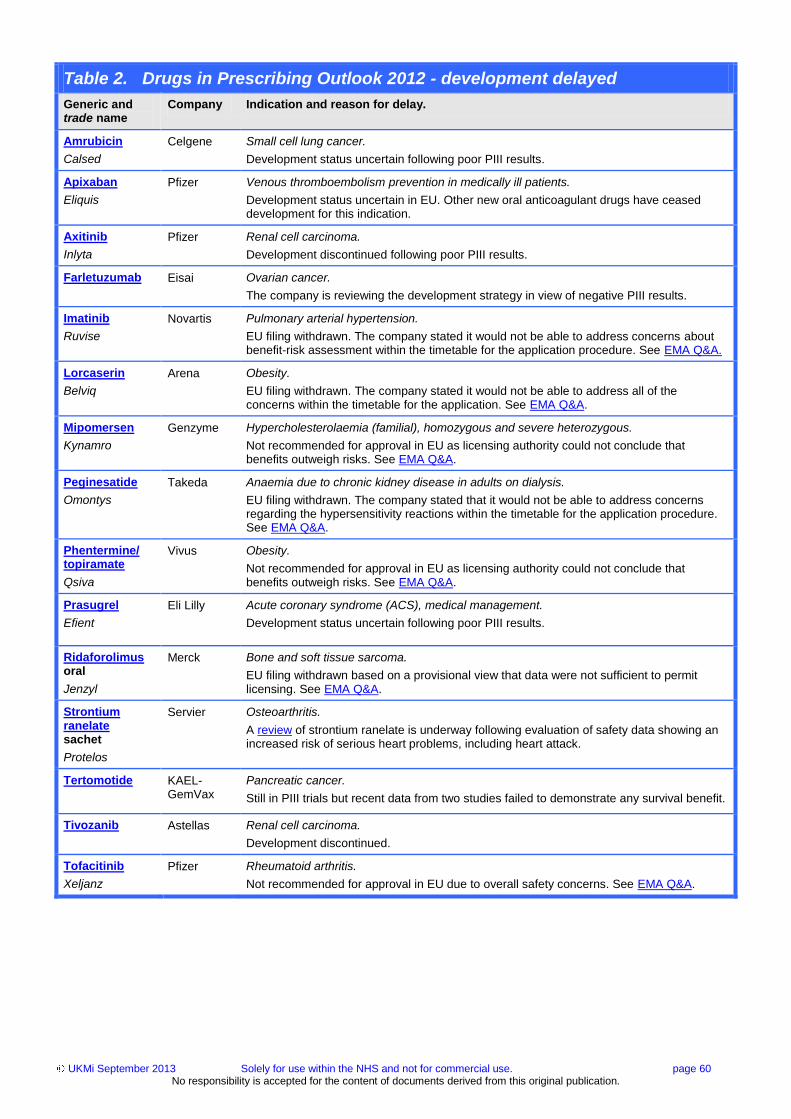
UKMi September 2013 Solely for use within the NHS and not for commercial use. page 60 No responsibility is accepted for the content of documents derived from this original publication.
Table 2. Drugs in Prescribing Outlook 2012 - development delayed
Generic and trade name
Company Indication and reason for delay.
Amrubicin
Calsed
Celgene Small cell lung cancer.
Development status uncertain following poor PIII results.
Apixaban
Eliquis
Pfizer Venous thromboembolism prevention in medically ill patients.
Development status uncertain in EU. Other new oral anticoagulant drugs have ceased development for this indication.
Axitinib
Inlyta
Pfizer Renal cell carcinoma.
Development discontinued following poor PIII results.
Farletuzumab Eisai Ovarian cancer.
The company is reviewing the development strategy in view of negative PIII results.
Imatinib
Ruvise
Novartis Pulmonary arterial hypertension.
EU filing withdrawn. The company stated it would not be able to address concerns about benefit-risk assessment within the timetable for the application procedure. See EMA Q&A.
Lorcaserin
Belviq
Arena Obesity.
EU filing withdrawn. The company stated it would not be able to address all of the concerns within the timetable for the application. See EMA Q&A.
Mipomersen
Kynamro
Genzyme
Hypercholesterolaemia (familial), homozygous and severe heterozygous.
Not recommended for approval in EU as licensing authority could not conclude that benefits outweigh risks. See EMA Q&A.
Peginesatide
Omontys
Takeda Anaemia due to chronic kidney disease in adults on dialysis.
EU filing withdrawn. The company stated that it would not be able to address concerns regarding the hypersensitivity reactions within the timetable for the application procedure. See EMA Q&A.
Phentermine/ topiramate
Qsiva
Vivus Obesity.
Not recommended for approval in EU as licensing authority could not conclude that benefits outweigh risks. See EMA Q&A.
Prasugrel
Efient
Eli Lilly Acute coronary syndrome (ACS), medical management.
Development status uncertain following poor PIII results.
Ridaforolimus oral
Jenzyl
Merck Bone and soft tissue sarcoma.
EU filing withdrawn based on a provisional view that data were not sufficient to permit licensing. See EMA Q&A.
Strontium ranelate sachet
Protelos
Servier Osteoarthritis.
A review of strontium ranelate is underway following evaluation of safety data showing an increased risk of serious heart problems, including heart attack.
Tertomotide
KAEL-GemVax
Pancreatic cancer.
Still in PIII trials but recent data from two studies failed to demonstrate any survival benefit.
Tivozanib Astellas Renal cell carcinoma.
Development discontinued.
Tofacitinib
Xeljanz
Pfizer Rheumatoid arthritis.
Not recommended for approval in EU due to overall safety concerns. See EMA Q&A.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 61 No responsibility is accepted for the content of documents derived from this original publication.
Table 3. Recent UK drug launches or licence extensions (Sep 2012 to Aug 2013)
Generic and brand name.
Company. Indication and relevant guidance. Full prescribing information can be found on the electronic medicines compendium at medicines.org.uk via brand name link.
BNF 1. Gastrointestinal system
Adalimumab
Humira - SmPC
AbbVie
Licence extension: Treatment of severe active Crohn's disease in patients aged 6 to 17 years – second-line.
Guidance: NICE: Crohn’s disease pathway. SMC: Restricted use. AWMSG: Recommended.
Reviews: No recent reviews.
Linaclotide
Constella - SmPC
Almirall
Licensed indication: Treatment of moderate to severe irritable bowel syndrome (IBS) with constipation in adults.
Guidance: NICE: IBS pathway. SMC: restricted use. AWMSG: Not endorsed.
Reviews: MTRAC Jun 2013, NICE-MPC Apr 2013, RDTC Mar 2013.
Racecadotril
Hidrasec - SmPC
Abbott
Licensed indication: Treatment of acute diarrhoea in infants (older than 3 months), children
and adults when causal treatment is not possible.
Guidance: SMC: Not approved adults/children. AWMSG: Not endorsed adults/ not
recommended children.
Reviews: NICE-MPC adults/children Mar 2013, RDTC children Nov 2012.
BNF 2. Cardiovascular system
Apixaban
Eliquis - SmPC
Bristol Myers Squibb Pfizer
Licence extension: Prevention of stroke and systemic embolism in adults with non-valvular atrial fibrillation.
Guidance: NICE: Stroke pathway, apixaban, atrial fibrillation. SMC: Approved.
Reviews: RDTC Dec 2012, NPC Nov 2011.
Rivaroxaban
Xarelto - SmPC
Bayer
Licence extension: Pulmonary embolism (PE) – treatment, and prevention of recurrent PE and deep vein thrombosis.
Guidance: NICE: VTE pathway, rivaroxaban. SIGN: Venous thromboembolism. SMC: Approved.
Reviews: RDTC Mar 2013.
BNF 3. Respiratory system
Aclidinium
Eklira Genuair - SmPC
Almirall
Licensed indication: Symptom relief in chronic obstructive pulmonary disease (COPD).
Guidance: NICE: COPD pathway. SMC: Approved. AWMSG: Recommended.
Reviews: NICE-MPC Jan 2013, MTRAC Nov 2012, RDTC Oct 2012, NPC/UKMi Nov 2011.
Beclometasone/ formoterol
Fostair - SmPC
Chiesi
Licence extension: Regular maintenance treatment and ‘as needed’ for adults with asthma.
Guidance: NICE: Asthma. SIGN: Asthma.
Review: NICE-MPC Jun 2013.
C1-esterase inhibitor (human)
Berinert - SmPC
CSL Behring
Licence extension: Hereditary angioedema – pre-procedure prevention of acute attacks in adults and children.
Guidance: AWMSG: Recommended.
Reviews: None.
Colistimethate sodium
Colobreathe - SmPC
Forest Laboratories
Licensed indication: Cystic fibrosis – chronic lung infection with Pseudomonas aeruginosa in
patients aged six years and older.
Guidance: NICE: Colistimethate sodium.
Reviews: None.
Fluticasone propionate/ formoterol fumarate
Flutiform - SmPC
Napp
Licensed indication: Regular maintenance treatment for asthma.
Guidance: NICE: Asthma. SIGN: Asthma. SMC: Approved.
Reviews: NICE-MPC Oct 2012, MTRAC Sep 2012.
Glycopyrronium bromide
Seebri Breezhaler-SmPC
Novartis
Licensed indication: Symptom relief in adults with chronic obstructive pulmonary disease.
Guidance: NICE: COPD pathway. SMC: Approved. AWMSG: Recommended.
Reviews: NICE-MPC Jan 2013, RDTC Nov 2012, MTRAC Nov 2012.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 62 No responsibility is accepted for the content of documents derived from this original publication.
Table 3. Recent UK drug launches or licence extensions (Sep 2012 to Aug 2013)
Generic and brand name.
Company. Indication and relevant guidance. Full prescribing information can be found on the electronic medicines compendium at medicines.org.uk via brand name link.
Ivacaftor
Kalydeco - SmPC
Vertex
Licensed indication: Cystic fibrosis in patients aged six years and older who have a G551D mutation in the CFTR gene.
Guidance: SMC: Not approved. AWMSG: Terminated, available for use in Wales.
Reviews: No recent reviews.
Pirfenidone
Esbriet - SmPC
InterMune
Licensed indication: Idiopathic pulmonary fibrosis.
Guidance: NICE: IPF pathway, pirfenidone. SMC: Restricted use.
Reviews: LNDG Dec 2011.
BNF 4. Central nervous system
Aripiprazole
Abilify - SmPC
Otsuka
Licence extension: Moderate to severe manic episodes in bipolar I disorder in adolescents
aged 13 years and older.
Guidance: NICE: Aripiprazole. SMC: Due Sep 2013.
Reviews: None.
Atomoxetine
Strattera - SmPC
Eli Lilly
Licence extension: Attention deficit/hyperactivity disorder in adults, but only when pre-existing symptoms during childhood can be confirmed by a third-party.
Guidance: NICE: ADHD pathway. SIGN: Attention deficit and hyperkinetic disorders.
Reviews: None.
Etoricoxib
Arcoxia - SmPC
MSD
Licence extension: Pain associated with dental surgery.
Guidance: SMC: Not approved. AWMSG: Not endorsed.
Reviews: None.
Lisdexamfetamine dimesylate
Elvanse - SmPC
Shire
Licensed indication: Attention deficit/hyperactivity disorder in children aged six years and over – second-line.
Guidance: NICE: ADHD pathway. SIGN: Attention deficit and hyperkinetic disorders. SMC: Approved. AWMSG: In progress.
Reviews: NICE-MPC May 2013.
Nalmefene
Selincro - SmPC
Lundbeck
Licensed indication: Reduction of alcohol consumption in adults with alcohol dependence.
Guidance: NICE: Alcohol use: pathway. SIGN: Alcohol dependence. SMC: Due Oct 13. AWMSG: In progress.
Reviews: NIHR HSC Sep 2012, RDTC due TBC.
Naloxone
Prenoxad - SmPC
Martindale
Licensed indication: Reversal of opioid-induced respiratory depression, emergency use in the home or other non-medical setting.
Guidance: None.
Reviews: None.
Perampanel
Fycompa - SmPC
Eisai
Licensed indication: Epilepsy in patients aged 12 years and older – adjunctive therapy of partial seizures.
Guidance: NICE: Epilepsy pathway. SMC: Restricted use. AWMSG: Restricted use.
Reviews: NICE-MPC Dec 2012, NETAG Oct 2012, NIHR HSC Apr 2011.
Tafamidis
Vyndaqel - SmPC
Pfizer
Licensed indication: Transthyretin amyloidosis.
Guidance: SMC: Not approved. AWMSG: Not endorsed.
Reviews: No recent reviews.
BNF 5. Infections
Ceftaroline
Zinforo - SmPC
AstraZeneca
Licensed indication: Complicated skin and soft tissue infections (cSSTI) or community acquired pneumonia (CAP).
Guidance: NICE: Pneumonia due TBC. SMC: Restricted use in cSSTI; not approved for CAP. AWMSG: Restricted use in cSSTI; not recommended for CAP.
Reviews: LNDG Sep 2012.
Elvitegravir/ cobicistat/ emtricitabine/ tenofovir
Stribild - SmPC
Gilead
Licensed indication: HIV-1 infection.
Guidance: SMC: Approved. AWMSG: In progress.
Reviews: LNDG Jan 2013.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 63 No responsibility is accepted for the content of documents derived from this original publication.
Table 3. Recent UK drug launches or licence extensions (Sep 2012 to Aug 2013)
Generic and brand name.
Company. Indication and relevant guidance. Full prescribing information can be found on the electronic medicines compendium at medicines.org.uk via brand name link.
Rifaximin
Targaxan - SmPC
Norgine
Licensed indication: Hepatic encephalopathy.
Guidance: SMC: Due Sep 2013.
Reviews: No recent reviews.
BNF 6. Endocrine system
Dapagliflozin
Forxiga - SmPC
AstraZeneca
Licensed indication: Type 2 diabetes mellitus – monotherapy and add-on.
Guidance: NICE: Diabetes: pathway, dapagliflozin. SIGN: Diabetes. SMC: Restricted use.
Reviews: MTRAC Feb 2013, RDTC Dec 2012, LNDG Nov 2012, NPC/UKMI Mar 2011.
Hydrocortisone MR
Plenadren - SmPC
ViroPharma
Licensed indication: Adrenal insufficiency.
Guidance: SMC: Not approved. AWMSG: Not endorsed.
Reviews: UKMi Oct 2012.
Insulin degludec
Tresiba - SmPC
Novo Nordisk
Licensed indication: Diabetes mellitus.
Guidance: NICE: Diabetes: pathway. SMC: Not approved. AWMSG: Not endorsed. SIGN: Diabetes.
Reviews: MTRAC Feb 2013, NICE-MPC - T1DM and T2DM Nov 2012, RDTC Aug 2012, NPC/UKMi - T2DM Mar 2012, NIHR HSC - T1DM and T2DM Jan 2011.
Insulin glargine
Lantus - SmPC
Sanofi
Licence extension: Diabetes mellitus in children aged two to less than six years.
Guidance: NICE: Diabetes: pathway. SMC: Restricted use. AWMSG: Recommended. SIGN: Diabetes.
Reviews: None.
Linagliptin
Trajenta - SmPC
Boehringer Ingelheim
Licence extension: Type 2 diabetes mellitus– with insulin.
Guidance: NICE: Diabetes: pathway. SIGN: Diabetes. SMC: Restricted use. AWMSG: Recommended.
Reviews: RDTC Mar 2012.
Linagliptin/metformin
Jentadueto - SmPC
Boehringer Ingelheim
Licensed indication: Type 2 diabetes mellitus.
Guidance: NICE: Diabetes: pathway. SIGN: Diabetes. SMC: Restricted use. AWMSG: Recommended.
Reviews: None.
Lixisenatide
Lyxumia - SmPC
Sanofi
Licensed indication: Type 2 diabetes mellitus.
Guidance: NICE: Diabetes: pathway. SIGN: Diabetes. SMC: Due Sep 2013. AWMSG: In progress.
Reviews: NICE-MPC Jan 2013.
Pasireotide
Signifor - SmPC
Novartis
Licensed indication: Cushing's disease.
Guidance: SMC: Not approved. AWMSG: Not endorsed.
Reviews: NETAG Jul 2012, LNDG Feb 2012.
Saxagliptin/metformin
Komboglyze - SmPC
Bristol Myers Squibb-AstraZeneca EEIG
Licensed indication: Type 2 diabetes mellitus.
Guidance: NICE: Diabetes: pathway. SIGN: Diabetes. SMC: Restricted use.
Reviews: None.
BNF 7. Obstetrics, gynaecology, and urinary-tract disorders
Botulinum A toxin
Botox - SmPC
Allergan
Licensed extension: Urinary incontinence (UI) in adults with detrusor overactivity in a neurologic condition in patients unresponsive to/intolerant of antimuscarinic medication.
Guidance: NICE: UI in neurological disease pathway. SMC: Due Oct 2013. SIGN: UI. AWMSG: In progress.
Reviews: NICE-MPC Sep 2012.
Medroxyprogesterone acetate
Sayana - SmPC
Pfizer
Licensed indication: Contraception, three-monthly subcutaneous injection.
Guidance: None.
Reviews: None.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 64 No responsibility is accepted for the content of documents derived from this original publication.
Table 3. Recent UK drug launches or licence extensions (Sep 2012 to Aug 2013)
Generic and brand name.
Company. Indication and relevant guidance. Full prescribing information can be found on the electronic medicines compendium at medicines.org.uk via brand name link.
Mirabegron
Betmiga - SmPC
Astellas
Licensed indication: Overactive bladder – with symptoms of urge urinary incontinence (UI),
urgency and urinary frequency.
Guidance: NICE: Mirabegron. SIGN: UI. SMC: Approved.
Reviews: MTRAC Aug 2013, LNDG Mar 2013, RDTC Feb 2013.
Nomegestrol acetate/ estradiol
Zoely - SmPC
MSD
Licensed indication: Contraception, oral.
Guidance: SMC: Not approved. AWMSG: Not endorsed.
Reviews: NICE-MPC due Oct 2013.
Tadalafil
Cialis - SmPC
Eli Lilly
Licence extension: Benign prostatic hyperplasia.
Guidance: SMC: Not approved. AWMSG: Not endorsed.
Reviews: NICE-MPC May 2013, RDTC Apr 2013.
BNF 8. Malignant disease and immunosuppression
Abiraterone acetate
Zytiga - SmPC
Janssen-Cilag
Licence extension: Metastatic, castration-resistant, prostate cancer after failure of androgen deprivation therapy and when chemotherapy is not yet clinically indicated.
Guidance: NICE: PC pathway, Abiraterone. SMC: Not approved.
Reviews: LCNDG Jan 2013.
Aflibercept
Zaltrap - SmPC
Sanofi
Licensed indication: Colorectal cancer (CRC), metastatic – second-line.
Guidance: NICE: CRC pathway, aflibercept due Oct 2013. SIGN: CRC.SMC: Not approved.
Reviews: None.
Axitinib
Inlyta - SmPC
Pfizer
Licensed indication: Advanced renal cell carcinoma – second-line.
Guidance: NICE: Overdue. SMC: Not approved.
Reviews: LCNDG Jan 2013.
Bevacizumab
Avastin - SmPC
Roche
Licence extension: Platinum-sensitive epithelian ovarian (OC), fallopian tube or primary peritoneal cancer.
Guidance: NICE: OC pathway, bevacizumab. SIGN: OC. SMC: Not approved.
Reviews: No recent reviews.
Bevacizumab
Avastin - SmPC
Roche
Licence extension: Metastatic colorectal cancer (CRC) in adults who have already been
treated with bevacizumab and chemotherapy.
Guidance: NICE: CRC pathway. SIGN: CRC.
Reviews: None.
Bortezomib
Velcade - SmPC
Janssen-Cilag
Licence extension: Multiple myeloma – subcutaneous administration.
Guidance: NICE: Bortezomib. SMC: Approved. AWMSG: Recommended.
Reviews: None.
Bortezomib
Velcade - SmPC
Janssen-Cilag
Licence extension: Multiple myeloma – re-treatment with bortezomib.
Guidance: NICE: Bortezomib.
Reviews: None.
Bortezomib
Velcade - SmPC
Janssen-Cilag
Licence extension: Multiple myeloma – first-line induction treatment of adults eligible for high-dose chemotherapy and stem cell transplantation.
Guidance: NICE: Bortezomib due Jan 2014.
Reviews: NIHR HSC Apr 2011.
Bosutinib
Bosulif - SmPC
Pfizer
Licensed indication: Chronic myeloid leukaemia, Philadelphia chromosome-positive – second-line.
Guidance: NICE: Haemato-oncology. SMC: Due Nov 2013.
Reviews: No recent reviews.
Brentuximab
Adcetris - SmPC
Takeda
Licensed indication: Hodgkin’s lymphoma – relapsed/refractory post autologous stem cell transplant (ASCT) or when ASCT unsuitable.
Guidance: NICE: Haemato-oncology. SMC: Not approved. AWMSG: Not endorsed.
Reviews: NIHR HSC Jan 2011.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 65 No responsibility is accepted for the content of documents derived from this original publication.
Table 3. Recent UK drug launches or licence extensions (Sep 2012 to Aug 2013)
Generic and brand name.
Company. Indication and relevant guidance. Full prescribing information can be found on the electronic medicines compendium at medicines.org.uk via brand name link.
Brentuximab
Adcetris - SmPC
Takeda
Licensed indication: Relapsed/refractory systemic anaplastic large cell lymphoma.
Guidance: SMC: Not approved. AWMSG: Not endorsed.
Reviews: LCNDG Mar 2013, NIHR HSC Jan 2011.
Crizotinib
Xalkori - SmPC
Pfizer
Licensed indication: ALK-positive non-small cell lung cancer, advanced – second line.
Guidance: NICE: Lung cancer: pathway, crizotinib due Sep 2013. SIGN: Lung cancer. SMC: Not approved, resubmission due Oct 2013.
Reviews: LCNDG Nov 2012.
Decitabine
Dacogen- SmPC
Janssen-Cilag
Licensed indication: Acute myeloid leukaemia (AML) in patients aged at least 65 years who are unsuitable for standard chemotherapy.
Guidance: NICE: Decitabine. SMC: Not approved. AWMSG: Not endorsed.
Reviews: No recent reviews.
Enzalutamide
Xtandi - SmPC
Astellas
Licensed indication: Prostate cancer, metastatic, castration-resistant – second-line.
Guidance: NICE: PC pathway. SMC: Due Nov 2013.
Reviews: NIHR HSC Feb 2012.
Lapatinib
Tyverb - SmPC
GlaxoSmithKline
Licence extension: HER2-positive, hormone receptor-negative metastatic breast cancer (BC) that has progressed on prior trastuzumab – in combination with trastuzumab and chemotherapy.
Guidance: NICE: Advanced BC pathway. AWMSG: Restricted use.
Reviews: NIHR HSC Feb 2012.
Lenalidomide
Revlimid - SmPC
Celgene
Licence extension: Myelodysplastic syndromes associated with a 5q chromosomal deletion in
patients with transfusion-dependent anaemia.
Guidance: NICE: Lenalidomide due Dec 2013.
Reviews: LCNDG Jan 2013.
Pertuzumab
Perjeta - SmPC
Roche
Licensed indication: Breast cancer (BC), metastatic HER2-positive disease – first-line with trastuzumab and docetaxel.
Guidance: NICE: Advanced BC pathway, pertuzumab due Nov 2013. SMC: Due Oct 2013.
Reviews: LCNDG Mar 2013.
Pomalidomide
Imnovid - SmPC Celgene
Licensed indication: Multiple myeloma, relapsed or refractory – in combination with dexamethasone, third-line.
Guidance: None.
Reviews: NIHR HSC Nov 2012.
Ponatinib
Iclusig - SmPC
Ariad
Licensed indication: Chronic myeloid leukaemia and acute lymphoblastic leukaemia.
Guidance: CML- bosutinib draft guidance, imatinib resistant/ intolerant patients
Reviews: NIHR HSC Sep 2012.
Rituximab
MabThera - SmPC
Roche
Licence extension: Vasculitis, anti-neutrophil cytoplasmic antibody (ANCA)-associated.
Guidance: NICE: Rituximab due Nov 2013.
Reviews: NIHR HSC Dec 2011.
Ruxolitinib
Jakavi - SmPC
Novartis
Licensed indication: Disease-related splenomegaly or symptoms in adults with chronic idiopathic myelofibrosis, post polycythaemia vera myelofibrosis or post essential thrombocythaemia myelofibrosis.
Guidance: NICE: Ruxolitinib. SMC: Not approved.
Reviews: RDTC Jan 2013, LCNDG Jun 2012.
Triptorelin SR
Decapeptyl SR - SmPC
Ipsen
New formulation: Prostate cancer, six-monthly preparation.
Guidance: NICE: PC pathway.
Reviews: NICE-MPC due Nov 2013.
Vismodegib
Erivedge - SmPC
Roche
Licensed indication: Basal cell carcinoma, metastatic or locally advanced.
Guidance: None.
Reviews: LCNDG Feb 2013.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 66 No responsibility is accepted for the content of documents derived from this original publication.
Table 3. Recent UK drug launches or licence extensions (Sep 2012 to Aug 2013)
Generic and brand name.
Company. Indication and relevant guidance. Full prescribing information can be found on the electronic medicines compendium at medicines.org.uk via brand name link.
BNF 9. Nutrition and blood
Deferasirox
Exjade - SmPC
Novartis
Licence extension: Treatment of chronic iron overload in patients aged at least 10 years with non-transfusion-dependent thalassemia syndrome.
Guidance: SMC: Not approved. AWMSG: Not endorsed.
Reviews: None.
Ferumoxytol
Rienso - SmPC
Takeda
Licensed indication: Iron deficiency anaemia in chronic kidney disease (CKD).
Guidance: NICE: Anaemia in CKD pathway. SIGN: CKD. SMC: Restricted use. AWMSG:
Restricted use.
Reviews: LNDG Oct 2012, NIHR HSC Jan 2011.
BNF 10. Musculoskeletal and joint diseases
Abatacept
Orencia - SmPC
Bristol Myers Squibb
New formulation: Rheumatoid arthritis (RA), moderate-to-severe active, subcutaneous formulation.
Guidance: NICE: RA pathway. SIGN: RA. SMC: Restricted use.
Reviews: None.
Canakinumab
Ilaris - SmPC
Novartis
Licence extension: Gouty arthritis – second-line.
Guidance: SMC: Not approved. AWMSG: Not endorsed.
Reviews: NICE-MPC Jul 2013.
Etanercept
Enbrel - SmPC
Pfizer
Licence extension: Paediatric use in juvenile idiopathic arthritis, oligoarticular, enthesitis-
related or psoriatic.
Guidance: NICE: Etanercept. SMC: Restricted use. AWMSG: In progress.
Reviews: None.
Tocilizumab
RoActemra - SmPC
Roche
Licence extension: Rheumatoid arthritis (RA) – monotherapy in inadequate responders to DMARDs or methotrexate.
Guidance: NICE: RA pathway. SIGN: RA. SMC: Restricted use.
Reviews: None.
Tocilizumab
RoActemra - SmPC
Roche
Licence extension: Juvenile idiopathic polyarthritis, polyarticular – second-line after methotrexate.
Guidance: None.
Reviews: NIHR HSC Jul 2012.
BNF 11. Eye
Aflibercept
Eylea - SmPC
Bayer
Licensed indication: Wet age related macular degeneration (AMD).
Guidance: NICE: Wet AMD. SMC: Approved.
Reviews: LNDG Mar 2013, NETAG Dec 2012.
Fluocinolone acetonide
Iluvien - SmPC
Alimera Sciences
Licensed indication: Diabetic macular oedema - second-line.
Guidance: NICE: Fluocinolone. SMC: Not approved.
Reviews: LNDG Feb 2011.
Ocriplasmin
Jetrea - SmPC
Alcon
Licensed indication: Symptomatic vitreomacular traction, including macular hole.
Guidance: NICE: Ocriplasmin due Oct 2013. SMC: Due Sep 2013.
Reviews: NIHR HSC Sep 2011.
Ranibizumab
Lucentis - SmPC
Novartis
Licence extension: Visual impairment due to choroidal neovascularisation secondary to pathologic myopia.
Guidance: SMC: Due Nov 2013.
Reviews: NIHR HSC Aug 2011.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 67 No responsibility is accepted for the content of documents derived from this original publication.
Table 3. Recent UK drug launches or licence extensions (Sep 2012 to Aug 2013)
Generic and brand name.
Company. Indication and relevant guidance. Full prescribing information can be found on the electronic medicines compendium at medicines.org.uk via brand name link.
BNF 12. Ear, nose and oropharynx
Azelastine hydrochloride/ fluticasone propionate
Dymista - SmPC
Meda
Licensed indication: Moderate to severe seasonal and perennial allergic rhinitis.
Guidance: SMC: Due Dec 2013.
Reviews: None.
BNF 13. Skin
Aminolaevulinic acid
Ameluz - SmPC
Spirit Healthcare
Licensed indication: Actinic keratosis of mild to moderate intensity on the face and scalp.
Guidance: SMC: Approved. AWMSG: In progress.
Reviews: None.
Imiquimod 3.75%
Zyclara - SmPC
MEDA
Licensed indication: Actinic keratosis on the face and scalp in immunocompetent adults.
Guidance: None.
Reviews: MTRAC Jun 2013, RDTC Apr 2013.
Ingenol mebutate
Picato - SmPC
LEO Pharma
Licensed indication: Actinic keratosis in adults – first-line.
Guidance: SMC: Approved. AWMSG: Recommended.
Reviews: MTRAC Jun 2013, RDTC Apr 2013, NICE-MPC Mar 2013.

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 68 No responsibility is accepted for the content of documents derived from this original publication.
Patent expiries 2013 - 2015
Generic medicines have a significant impact on prescribing budgets and can offset, to some extent, costs
associated with the introduction of new medicines. Generic products can be marketed once the patent on the
original product has expired although manufacturers may apply for a Supplementary Protection Certificate (SPC) to
extend the effective patent life by up to 5 years (5½ years if it includes a Paediatric Investigation Plan). Expiry dates
below take account of SPCs. The table highlights those drugs where there is a greater potential for the availability
of a generic/biosimilar product. In addition, the table indicates where a licence for a generic/biosimilar product is in
the latter stages of the EU licensing process or is already available in the EU. However, it does not follow that the
generic/biosimilar product will be available in the UK as patent issues may differ between countries. Patent
legislation is complex and the information below should be used as a guide only.
* Drugs which have the greatest potential for generic/biosimilar preparations becoming available.
# Drugs where generic/biosimilar products are in later stages of EU licensing or are licensed in EU (see also over the page).
Patent extended by 6 months (paediatric extension).
Expiry date
Drug
2013
Feb Montelukast
Fosphenytoin sodium
Ganirelix
Mar Dorzolamide/ timolol #
Zidovudine/ lamivudine
Daclizumab
Apr Basiliximab
May Nelarabine
Tirofiban
Zoledronic acid #
Jun Capecitabine #
Nevirapine #
Sildenafil #
Jul Etonogestrel
Aug Raloxifene HCl #
Rizatriptan #
Clopidogrel hydrogen
sulphate
Oct Irbesartan/ hydrochlorothiazide
Nov Efavirenz
Rituximab *
Dec Telmisartan #
Expiry date
Drug
2014
Feb Alemtuzumab
Temoporfin
Zanamivir *
Mar Somatropin (synthetic hGH)
Apr Memantine HCl
May Anakinra
Escitalopram oxalate
Jun Abacavir
Hydroxyethyl starch
Moxifloxacin
Ulipristal acetate *
Jul Trastuzumab
Verteporfin
Aug Palivizumab
Sep Cetuximab *
Panitumumab
Oct Aripiprazole *
Nelfinavir mesylate
Paliperidone
Nov Insulin glargine
Icatibant acetate
Dec Almotriptan
Bevacizumab
Brinzolamide *
Omalizumab
Expiry date
Drug
2015
Feb Infliximab *
Mar Darifenacin
Tegafur/ uracil
Apr Aripiprazole *
May Clofarabine
Glatiramer
Insulin glargine
Jun Nepafenac
Tenecteplase
Jul Etanercept
Rasburicase
Aug Bivalirudin
Strontium ranelate
Sep Etoricoxib
Nateglinide
Sirolimus
Tiotropium *
Oct Alitretinoin
Nov Palonosetron
Pimecrolimus
Dec Eletriptan
Frovatriptan
Lopinavir/ ritonavir
Pemetrexed

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 69 No responsibility is accepted for the content of documents derived from this original publication.
Biosimilar developments
What are biosimilars?
Biosimilars are ‘generic’ biological medicines. Unlike conventional pharmaceuticals, which are generally low molecular weight organic compounds with a defined chemical structure, biologicals are large complex proteins that cannot be copied exactly. To gain a licence, the manufacturer must provide the EMA with adequate data to show that their biosimilar is physically, chemically, biologically and clinically similar to the approved originator product. This data will be derived from extensive laboratory analysis of molecular characteristics, in vitro and in vivo studies in multiple species of animals and phase I studies in humans to define pharmacokinetics, pharmacodynamics and toxicity. In addition, phase III studies are performed to show clinical efficacy and safety; post-marketing risk management plans and phase IV studies assess safety in routine practice. Consequently, development of a biosimilar is more costly and protracted (up to eight years) compared to that of a standard generic medicine.
What biosimilars are currently available or will soon be available?
Three drugs are currently available in the UK in biosimilar formulations: filgrastim, epoetin and somatropin. These are reasonably simple protein structures compared to monoclonal antibodies. The first monoclonal antibody biosimilar to be submitted for marketing approval in the EU, infliximab, is in the final stages of the licensing process; two brands of the same infliximab biosimilar (Inflectra and Remsima) were recommended for approval by the EMA in June 2013 with all the same indications as the originator product, Remicade, even though clinical studies have only been carried out in adults with ankylosing spondylitis (PI studies) and rheumatoid arthritis (PIII studies). Launch of infliximab biosimilar, if licensing is confirmed, will be delayed until the patent protecting the originator product expires.
What is the impact of biosimilars?
Marketed biosimilars are currently 5-20% cheaper than the originator products. Celltrion has stated that Remsima will cost at least 30% less than Remicade. Originators will no doubt seek to retain their market share; for example, by making their products more attractive by reformulating to simplify administration, or by offering competitive discounts.
What other biosimilars are in the pipeline?
The table below gives details of those medicines identified elsewhere in this document (Patent expiries) for which biosimilars are in clinical development. Further information on biosimilars that could be licensed in the UK in the near future is given in the table on the following page.
Drug name Patent expiry
Biosimilar Disease/Indication Highest development stage relevant to EU
Company
Bevacizumab 2014 BI 695502 Cancer PI Boehringer Ingelheim
Etanercept 2015 SB4 Rheumatoid arthritis PIII Samsung Bioepis
GP 2015 Plaque psoriasis PIII Sandoz
AFOLIA Pre-registration Finox
Infliximab 2015 CT P13 (Inflectra,
Remsima)
All inflammatory indications for which the originator is licensed
Recommended for approval Jun 2013
Celltrion, Hospira
Insulin glargine
2015 LY 2963016 Diabetes Pre-registration Eli Lilly/ Boehringer Ingelheim
Rituximab 2013 BI 695500 Rheumatoid arthritis PIII Boehringer Ingelheim
BI 695500 Non-Hodgkin's lymphoma PIII Boehringer Ingelheim
SAIT-101 Rheumatoid arthritis PIII Samsung
MK-8808 Follicular lymphoma PIII Merck
GP 2013 Follicular lymphoma PIII Sandoz
Trastuzumab 2014 ABP-980 Breast cancer PIII Amgen
CT P06 (CT-P6)
Breast cancer PIII Celltrion/ Hospira
Gastric cancer Celltrion/ Hospira

UKMi September 2013 Solely for use within the NHS and not for commercial use. page 70 No responsibility is accepted for the content of documents derived from this original publication.
Infliximab
CT P13 injection
Inflectra/ Remsima
Hospira/ Celltrion
Indication:
Rheumatoid arthritis, adult and paediatric Crohn’s disease, adult and paediatric ulcerative colitis, ankylosing spondylitis, psoriatic arthritis and psoriasis.
Current status:
Recommended for approval in EU Jun 2013. First monoclonal antibody to have gone through the EU biosimilar regulatory process.
Predicted UK launch:
2014/2015
(Patent expiry 2015)
Pharmacology: Monoclonal tumour necrosis factor alpha (TNF-a) inhibitor. Originator product - Remicade.
Efficacy: Rheumatoid arthritis: CT P13 was compared to Remicade in a 54-week PIII study in 606 patients also receiving methotrexate. At all assessment points, there were no clinically significant differences between the two groups in efficacy or safety outcomes. In a PIII trial, safety was similar to that of the branded product, and in particular there was no statistically significant difference in the ratio of patients who developed anti-drug antibodies.
Follitropin alfa XM 17 injection
Ovaleap
Teva
Indication:
Fertility disorders: anovulation unresponsive to clomifene citrate; stimulation of multifollicular development in women undergoing assisted reproduction; with luteinising-hormone (LH) for stimulation of follicular development in severe LH and FSH deficiency; stimulation of spermatogenesis in men.
Current status:
Recommended for approval in EU Jul 2013.
Predicted UK launch:
2013
(Patent expired 2009)
Pharmacology: Human recombinant follicle stimulating hormone (FSH). Originator product – Gonal-f.
Efficacy: An international PIII study in 280 women undergoing assisted reproductive technologies compared XM17 to Gonal-f, administered for up to three cycles. The primary outcome was number of cumulus oocyte complexes retrieved.
Follitropin alfa AFOLIA injection
Bemfola
Finox
Indication:
Fertility disorders.
Current status:
Filed in the EU in Dec 2012.
Predicted UK launch:
2014
(Patent expired 2009)
Pharmacology: Human recombinant follicle stimulating hormone (FSH). Originator product – Gonal-f. Uses a different injector device to Gonal-f that reduces administration to three steps.
Efficacy: A single-blind European PIII study comparing Bemfola vs. Gonal-f in 410 women during the first or second cycle of assisted reproductive treatment has been completed. The primary outcome was the number of retrieved oocytes. A second PIII study vs. Gonal-f started in the US in May 2013. It is enrolling 1,106 women undergoing in vitro fertilisation and has a primary outcome clinical pregnancy rate.
Insulin glargine
LY 2963016 injection
Eli Lilly/ Boehringer Ingelheim
Indication:
Diabetes mellitus type 1 and 2 (T1DM, T2DM)
Current status:
Filed in the EU in Jul 2013.
Predicted UK launch:
2014/2015
(Patent expiry 2015)
Pharmacology: Recombinant human insulin analogue. Originator product - Lantus.
Efficacy: Two PIII studies vs. Lantus have been completed: ELEMENT 1 in 400 adults with T1DM in which it was used in combination with insulin lispro and ELEMENT 2 in 606 adults with T2DM used in combination with oral hypoglycaemics.
Trastuzumab
CT P06 injection
Hospira/ Celltrion
Indication:
Breast cancer, HER 2 positive, early and metastatic. Gastric cancer, HER2 positive.
Current status:
PIII.
Filed in Korea in Jun 2013 for the range of indication for which Herceptin is licensed.
Predicted UK launch:
2014/2015
(Patent expiry 2014)
Pharmacology: Anti-HER2 monoclonal antibody. Originator product - Herceptin.
Efficacy: A PIII study in 383 patients with HER2+ metastatic breast cancer showed CT-P6 and trastuzumab, both in
combination with paclitaxel, to have equivalent efficacy in terms in overall response rate and safety profile when given as first-line therapy every 3 weeks.
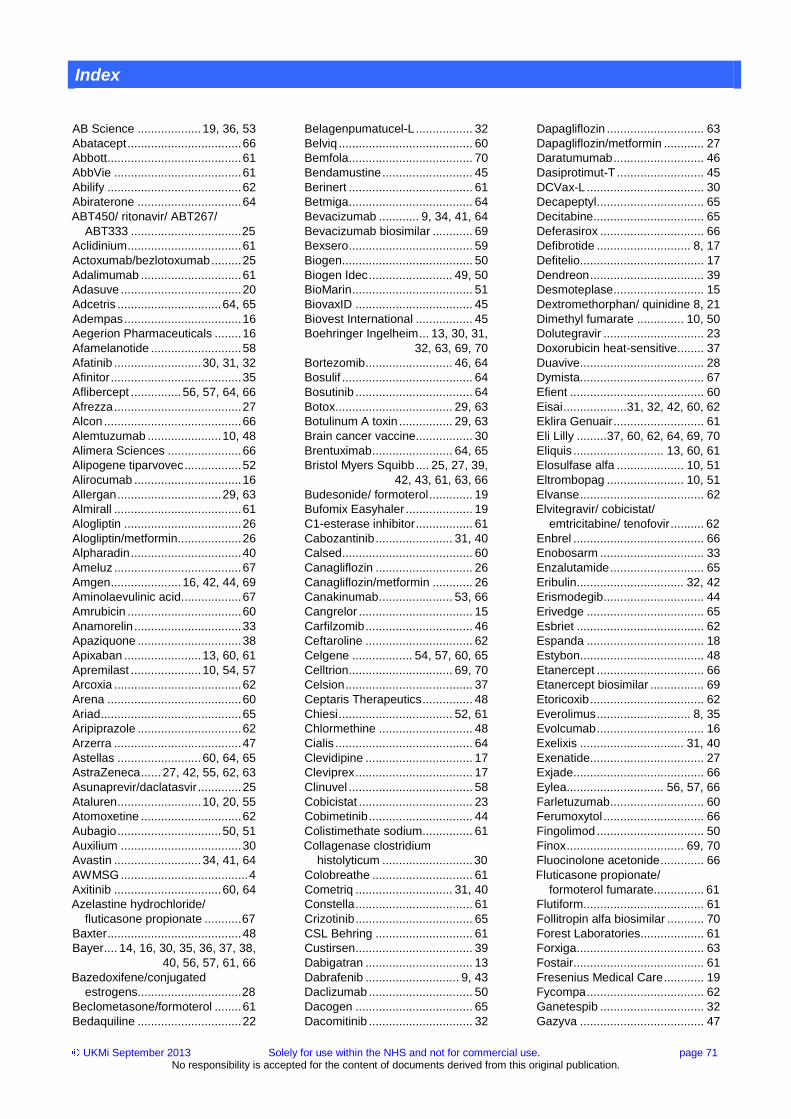
UKMi September 2013 Solely for use within the NHS and not for commercial use. page 71 No responsibility is accepted for the content of documents derived from this original publication.
Index
AB Science ................... 19, 36, 53
Abatacept .................................. 66
Abbott ........................................ 61
AbbVie ...................................... 61
Abilify ........................................ 62
Abiraterone ............................... 64
ABT450/ ritonavir/ ABT267/
ABT333 ................................. 25
Aclidinium .................................. 61
Actoxumab/bezlotoxumab ......... 25
Adalimumab .............................. 61
Adasuve .................................... 20
Adcetris ............................... 64, 65
Adempas ................................... 16
Aegerion Pharmaceuticals ........ 16
Afamelanotide ........................... 58
Afatinib .......................... 30, 31, 32
Afinitor ....................................... 35
Aflibercept ............... 56, 57, 64, 66
Afrezza ...................................... 27
Alcon ......................................... 66
Alemtuzumab ...................... 10, 48
Alimera Sciences ...................... 66
Alipogene tiparvovec ................. 52
Alirocumab ................................ 16
Allergan ............................... 29, 63
Almirall ...................................... 61
Alogliptin ................................... 26
Alogliptin/metformin ................... 26
Alpharadin ................................. 40
Ameluz ...................................... 67
Amgen ..................... 16, 42, 44, 69
Aminolaevulinic acid .................. 67
Amrubicin .................................. 60
Anamorelin ................................ 33
Apaziquone ............................... 38
Apixaban ....................... 13, 60, 61
Apremilast ..................... 10, 54, 57
Arcoxia ...................................... 62
Arena ........................................ 60
Ariad .......................................... 65
Aripiprazole ............................... 62
Arzerra ...................................... 47
Astellas ......................... 60, 64, 65
AstraZeneca ...... 27, 42, 55, 62, 63
Asunaprevir/daclatasvir ............. 25
Ataluren ......................... 10, 20, 55
Atomoxetine .............................. 62
Aubagio ............................... 50, 51
Auxilium .................................... 30
Avastin .......................... 34, 41, 64
AWMSG ...................................... 4
Axitinib ................................ 60, 64
Azelastine hydrochloride/
fluticasone propionate ........... 67
Baxter ........................................ 48
Bayer .... 14, 16, 30, 35, 36, 37, 38,
40, 56, 57, 61, 66
Bazedoxifene/conjugated
estrogens............................... 28
Beclometasone/formoterol ........ 61
Bedaquiline ............................... 22
Belagenpumatucel-L ................. 32
Belviq ........................................ 60
Bemfola ..................................... 70
Bendamustine ........................... 45
Berinert ..................................... 61
Betmiga ..................................... 64
Bevacizumab ............ 9, 34, 41, 64
Bevacizumab biosimilar ............ 69
Bexsero ..................................... 59
Biogen ....................................... 50
Biogen Idec ......................... 49, 50
BioMarin .................................... 51
BiovaxID ................................... 45
Biovest International ................. 45
Boehringer Ingelheim ... 13, 30, 31,
32, 63, 69, 70
Bortezomib .......................... 46, 64
Bosulif ....................................... 64
Bosutinib ................................... 64
Botox ................................... 29, 63
Botulinum A toxin ................ 29, 63
Brain cancer vaccine ................. 30
Brentuximab ........................ 64, 65
Bristol Myers Squibb .... 25, 27, 39,
42, 43, 61, 63, 66
Budesonide/ formoterol ............. 19
Bufomix Easyhaler .................... 19
C1-esterase inhibitor ................. 61
Cabozantinib ....................... 31, 40
Calsed ....................................... 60
Canagliflozin ............................. 26
Canagliflozin/metformin ............ 26
Canakinumab ...................... 53, 66
Cangrelor .................................. 15
Carfilzomib ................................ 46
Ceftaroline ................................ 62
Celgene .................. 54, 57, 60, 65
Celltrion ............................... 69, 70
Celsion ...................................... 37
Ceptaris Therapeutics ............... 48
Chiesi .................................. 52, 61
Chlormethine ............................ 48
Cialis ......................................... 64
Clevidipine ................................ 17
Cleviprex ................................... 17
Clinuvel ..................................... 58
Cobicistat .................................. 23
Cobimetinib ............................... 44
Colistimethate sodium ............... 61
Collagenase clostridium
histolyticum ........................... 30
Colobreathe .............................. 61
Cometriq ............................. 31, 40
Constella ................................... 61
Crizotinib ................................... 65
CSL Behring ............................. 61
Custirsen ................................... 39
Dabigatran ................................ 13
Dabrafenib ............................ 9, 43
Daclizumab ............................... 50
Dacogen ................................... 65
Dacomitinib ............................... 32
Dapagliflozin ............................. 63
Dapagliflozin/metformin ............ 27
Daratumumab ........................... 46
Dasiprotimut-T .......................... 45
DCVax-L ................................... 30
Decapeptyl ................................ 65
Decitabine ................................. 65
Deferasirox ............................... 66
Defibrotide ............................ 8, 17
Defitelio ..................................... 17
Dendreon .................................. 39
Desmoteplase ........................... 15
Dextromethorphan/ quinidine 8, 21
Dimethyl fumarate .............. 10, 50
Dolutegravir .............................. 23
Doxorubicin heat-sensitive ........ 37
Duavive ..................................... 28
Dymista ..................................... 67
Efient ........................................ 60
Eisai ...................31, 32, 42, 60, 62
Eklira Genuair ........................... 61
Eli Lilly ......... 37, 60, 62, 64, 69, 70
Eliquis ........................... 13, 60, 61
Elosulfase alfa .................... 10, 51
Eltrombopag ....................... 10, 51
Elvanse ..................................... 62
Elvitegravir/ cobicistat/
emtricitabine/ tenofovir .......... 62
Enbrel ....................................... 66
Enobosarm ............................... 33
Enzalutamide ............................ 65
Eribulin ................................ 32, 42
Erismodegib .............................. 44
Erivedge ................................... 65
Esbriet ...................................... 62
Espanda ................................... 18
Estybon ..................................... 48
Etanercept ................................ 66
Etanercept biosimilar ................ 69
Etoricoxib .................................. 62
Everolimus ............................ 8, 35
Evolcumab ................................ 16
Exelixis ............................... 31, 40
Exenatide .................................. 27
Exjade ....................................... 66
Eylea............................. 56, 57, 66
Farletuzumab ............................ 60
Ferumoxytol .............................. 66
Fingolimod ................................ 50
Finox ................................... 69, 70
Fluocinolone acetonide ............. 66
Fluticasone propionate/
formoterol fumarate ............... 61
Flutiform .................................... 61
Follitropin alfa biosimilar ........... 70
Forest Laboratories................... 61
Forxiga ...................................... 63
Fostair ....................................... 61
Fresenius Medical Care ............ 19
Fycompa ................................... 62
Ganetespib ............................... 32
Gazyva ..................................... 47
UKMi September 2013 Solely for use within the NHS and not for commercial use. page 72 No responsibility is accepted for the content of documents derived from this original publication.
Gentium .................................... 17
Genzyme ....................... 20, 48, 60
Gilead ...................... 23, 24, 25, 62
Gilead Sciences ........................ 47
Gilenya ...................................... 50
Giotrif ............................ 30, 31, 32
GlaxoSmithKline ..... 18, 40, 43, 44,
47, 51, 65
Glybera ..................................... 52
Glycopyrronium bromide ........... 61
Golimumab .......................... 11, 53
Grupo Ferrer ............................. 20
GTXi .......................................... 33
Halaven ............................... 32, 42
Helsinn ...................................... 33
Herceptin ................................... 34
Hidrasec .................................... 61
Hospira ................................ 69, 70
Humira ...................................... 61
Hydrocortisone .......................... 63
Ibrutinib ..................................... 47
Iclusig ........................................ 65
Idebenone ................................. 56
Idelalisib .................................... 47
Ilaris .................................... 53, 66
Iluvien ........................................ 66
Imatinib ..................................... 60
Imiquimod ................................. 67
Imnovid ..................................... 65
Indacaterol/ glycopyrronium ...... 18
Inflectra ..................................... 70
Infliximab biosimilar ............. 69, 70
Ingenol mebutate ...................... 67
Inlyta ................................... 60, 64
Insulin inhaled ........................... 27
Insulin degludec ........................ 63
Insulin degludec/ insulin aspart .. 8,
27
Insulin glargine .......................... 63
Insulin glargine biosimilar .... 69, 70
Intarcia therapeutics .................. 27
Intercept .................................... 12
InterMune .................................. 62
Invokana ................................... 26
Ipilimumab ....................... 9, 39, 42
Ipsen ......................................... 65
Ivacaftor .................................... 62
Jakavi ........................................ 65
Janssen-Cilag .. 22, 24, 26, 46, 47,
48, 54, 64, 65
Jenson ...................................... 21
Jentadueto ................................ 63
Jenzyl ........................................ 60
Jetrea ........................................ 66
Kadcyla ............................... 33, 34
KAEL-GemVax .......................... 60
Kalydeco ................................... 62
Kinaction ................................... 36
Komboglyze .............................. 63
Krystexxa .................................. 55
Kynamro .................................... 60
Kyprolis ..................................... 46
L(C)NDG ..................................... 4
Lantus ....................................... 63
Lapatinib ................................... 65
Laquinimod ......................... 10, 49
Latuda ....................................... 20
LDK378 ..................................... 32
Lemtrada ................................... 48
Lenalidomide ............................ 65
Lenvatinib ................................. 31
LEO Pharma ............................. 67
Lesinurad .................................. 55
Levact ....................................... 45
Linaclotide ................................. 61
Linagliptin .................................. 63
Linagliptin/ metformin ................ 63
Liraglutide ................................. 21
Lisdexamfetamine dimesylate ... 62
Lixisenatide ............................... 63
LNDG .......................................... 4
Lojuxta ...................................... 16
Lomitapide ................................ 16
Lorcaserin ................................. 60
Loxapine ................................... 20
Lucane Pharma ........................ 52
Lucanix ..................................... 32
Lucentis .................................... 66
Lumacaftor ................................ 20
Lundbeck ............................ 15, 62
Lurasidone ................................ 20
Lyxumia .................................... 63
MabThera ................................. 45
MannKind Corporation .............. 27
Martindale ................................. 62
Masitinib .................... 9, 19, 36, 53
Meda ......................................... 67
Medroxyprogesterone acetate .. 63
Mekinist ..................................... 44
Meningococcal group-B vaccine 59
Merck .................................. 60, 69
Mipomersen .............................. 60
Mirabegron ................................ 64
MSD 11, 15, 25, 41, 53, 55, 62, 64
MTRAC ....................................... 4
Nalfurafine ................................ 19
Nalmefene ................................ 62
Naloxone ................................... 62
Napp ................................... 45, 61
Neoquin .................................... 38
NETAG ....................................... 4
Nexavar .................. 30, 35, 37, 38
NHSC .......................................... 4
NICE ........................................... 4
NICE-MPC .................................. 4
Nomegestrol acetate/ estradiol . 64
Norgine ..................................... 63
Northwest Biotherapeutics ........ 30
Novartis 17, 18, 19, 28, 32, 35, 44,
50, 53, 54, 58, 59, 60, 61, 63,
65, 66
NovaRx Corporation ................. 32
Novo Nordisk ................ 21, 27, 63
NPC ............................................ 4
NPS Pharmaceuticals ............... 12
Nuedexta .................................. 21
Oasmia ..................................... 41
Obeticholic acid......................... 12
Obinutuzumab .................... 10, 47
Ocriplasmin ............................... 66
Odanacatib ............................... 55
Ofatumumab ....................... 10, 47
Olaparib .................................... 42
Omacetaxine meppesuccinate . 46
Omalizumab ............................. 19
Omontys ................................... 60
OncoGenex .............................. 39
Onyx ......................................... 46
Orencia ..................................... 66
Orion Pharma ........................... 19
Ostarine .................................... 33
Otsuka ...................................... 62
Otsuka Pharmaceuticals ........... 29
Ovaleap .................................... 70
Paclical ..................................... 41
Paclitaxel .................................. 41
Palbociclib ................................ 35
Pari Pharma .............................. 22
Pasireotide .......................... 28, 63
Pazopanib ............................. 9, 40
Peginesatide ............................. 60
Peginterferon beta-1a ............... 49
Pegloticase ............................... 55
Perampanel .............................. 62
Perjeta ...................................... 65
Pertuzumab .............................. 65
Pfizer .... 13, 28, 32, 35, 57, 60, 61,
62, 63, 64, 65, 66
Pheburane ................................ 52
Phentermine/ topiramate .......... 60
Picato ........................................ 67
Pierre Fabre .............................. 58
Pirfenidone ............................... 62
Plegridy ..................................... 49
Plenadren ................................. 63
Pomalidomide ........................... 65
Ponatinib ................................... 65
Pradaxa .................................... 13
Prasugrel .................................. 60
Prenoxad .................................. 62
Propranolol ............................... 58
Protelos .................................... 60
Provenge .................................. 39
PTC Therapeutics ..................... 55
Qsiva ........................................ 60
Racecadotril .............................. 61
Radium-223 .............................. 40
Ramucirumab ........................... 37
Ranibizumab ............................. 66
RDTC .......................................... 4
Regorafenib .................... 9, 36, 37
Remsima .................................. 70
Revestive .................................. 12
Revlimid .................................... 65
Revolade .................................. 51
Ridaforolimus ............................ 60
Rienso ...................................... 66
Rifaximin ................................... 63
Rigosertib ................................. 48
Riociguat ................................... 16
Rituximab ........................ 9, 45, 65
Rituximab biosimilar.................. 69
Rivaroxaban ............. 8, 14, 15, 61
RoActemra ................................ 66
Roche ... 33, 34, 41, 44, 45, 47, 64,
65, 66
Ruvise ....................................... 60
Ruxolitinib ................................. 65
UKMi September 2013 Solely for use within the NHS and not for commercial use. page 73 No responsibility is accepted for the content of documents derived from this original publication.
Ryzodeg .................................... 27
Samsca ..................................... 29
Samsung ................................... 69
Samsung Bioepis ...................... 69
Sandoz ...................................... 69
Sanofi ................ 16, 50, 51, 63, 64
Savient ...................................... 55
Saxagliptin/metformin ................ 63
Sayana ...................................... 63
Scenesse .................................. 58
Sebelipase alfa.......................... 52
Secukinumab ................ 53, 54, 58
Seebri Breezhaler ..................... 61
Selincro ..................................... 62
Serelaxin ................................... 17
Servier ....................................... 60
Shire .......................................... 62
SIGN ........................................... 4
Signifor ................................ 28, 63
Simeprevir ................................. 24
Simponi ............................... 11, 53
Sipuleucel-T .............................. 39
Situro ......................................... 22
SMC ............................................ 4
Sodium phenylbutyrate ............. 52
Sofosbuvir ................................. 24
Sofosbuvir/ledipasvir ................. 25
Sorafenib ................. 30, 35, 37, 38
Sovrima ..................................... 56
Spectrum ................................... 38
Spirit Healthcare ........................ 67
Stelara ....................................... 54
Stivarga ............................... 36, 37
Strattera .................................... 62
Stribild ....................................... 62
Strontium ranelate ..................... 60
Sunesis ..................................... 47
Synageva BioPharma ............... 52
Synribo ...................................... 46
Synta ......................................... 32
Tadalafil .................................... 64
Tafamidis .................................. 62
Tafinlar ...................................... 43
Takeda . 11, 12, 20, 26, 56, 60, 64,
65, 66
Talimogene laherparepvec ....... 44
Targaxan ................................... 63
Tecfidera ................................... 50
Teduglutide ............................... 12
Teriflunomide ................ 10, 50, 51
Tertomotide ............................... 60
Teva .............................. 46, 49, 70
The Medicines Company .... 15, 17
ThermoDox ............................... 37
Tivozanib .................................. 60
Tobramycin ............................... 22
Tocilizumab ............................... 66
Tofacitinib ........................... 57, 60
Tolvaptan .............................. 8, 29
Trajenta ..................................... 63
Trametinib ............................. 9, 44
Translarna ................................. 55
Trastuzumab biosimilar ....... 69, 70
Trastuzumab emtansine . 8, 33, 34
Trastuzumab/ hyaluronidase . 9, 34
Trebananib ................................ 42
Tresiba ...................................... 63
Triptorelin .................................. 65
Tybost ....................................... 23
Tyverb ....................................... 65
UKMi ........................................... 4
Ultibro Breezhaler ..................... 18
Umeclidinium ............................ 18
Umeclidinium/ vilanterol ............ 18
Ustekinumab ............................. 54
Valchlor ..................................... 48
Vantobra ................................... 22
Vedolizumab ....................... 11, 12
Velcade ............................... 46, 64
Vertex ................................. 20, 62
Victoza ...................................... 21
ViiV healthcare UK ................... 23
Vimizim ..................................... 51
Vintafolide ............................. 9, 41
Vipdomet .................................. 26
Vipidia ....................................... 26
ViroPharma ............................... 63
Vismodegib ............................... 65
Vivus ......................................... 60
Vosaroxin .................................. 47
Votrient ..................................... 40
Vyndaqel ................................... 62
Vynfinit ...................................... 41
Winfuran ................................... 19
Xalkori ....................................... 65
Xarelto ................................ 14, 61
Xeljanz ...................................... 57
Xiapex ....................................... 30
Xolair ........................................ 19
Xtandi ....................................... 65
Yervoy ................................ 39, 43
Zaltrap ...................................... 64
Zenapax .................................... 50
Zinforo ...................................... 62
Zoely ......................................... 64
Zyclara ...................................... 67
Zytiga ........................................ 64
Acknowledgements
Key contributors:
Helen Davis, North West MI Centre.
Alexandra Denby, London MI Service - Northwick Park.
Stephen Erhorn, Regional Drug & Therapeutics Centre, Newcastle.
Jim Glare, West Midlands MI Service.
Peter Golightly, Trent MI Centre.
Sue Gough, Wessex Drug & MI Centre.
Justine Howard, North West MI Centre.
Joanne McEntee, North West MI Centre.
Christine Proudlove, North West MI Centre.
Jill Rutter, North West MI Centre.
The following are acknowledged for commenting on draft versions, providing professional advice or technical and quality assurance support:
Alison Alvey, South West MI and Training Centre.
Liz Arkell, University Hospital of South Manchester NHS Foundation Trust.
Lindsay Banks, North West MI Centre.
David Erskine, London and South East MI Centre.
Simone Henderson, North West MI Centre.
Ashley Marsden, North West MI Centre.
Helen Potter, Cheshire, Warrington & Wirral Area Team NHS England.
Christine Randall, North West MI Centre.
Gail Woodland, Welsh MI centre and All Wales Medicines Strategy Group.