present - bayes-pharma
TRANSCRIPT

A Bayesian Dose De-Escalating Design With Stratified Minimax Regret Roland Fisch*, Georg Gutjahr†, Jean Lecot‡
Bayes 2012, Aachen, May 11, 2012 * Novartis Pharma AG; [email protected] † Universität Bremen; [email protected] ‡ Medstat; [email protected]

Outline
Motivation: Dose finding in a rare benign cancer indication
Outcomes of interest: Tumor size reduction; remission rate, stabilizing rate
Dose de-escalation design
Bayesian de-escalation design parameters
Design performance measures
What is an «optimal» design?
Regret, minimax regret, stratified minimax regret
Simulations
Summary
2 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret

Dose finding in a rare benign cancer indication
3 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Virtual «generic» example, for motivation and illustration
Indication
Rare tumor
benign, i.e. no metastases
There is an effective, but quite invasive standard treatment; however, the tumor may grow again afterwards
Proof of Concept (PoC) trial has been done, with a new treatment (an oral tablet), at one dose (vs Placebo):
Small sample size, e.g. 8
demonstrated tumor size reduction of 92% on average at 4 weeks,
75% of patients with a ≥80% reduction
dose cannot be increased beyond the chosen dose = MTD, due to safety and/or tolerability issues (as established in a first in human healthy volunteer trial); assume MTD = 10 mg
Dose finding in a rare benign cancer indication
4 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Design a dose finding trial:
Find an efficient loading dose <=MTD to be used in pivotal phase 3 trial
Find an efficient maintenance dose to be used in pivotal phase 3 trial
Small maximal sample size, e.g. ≤ 20
Minimize number of patients with sub-therapeutic doses

Outcomes of interest
5 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Tumor size reduction: Using imaging techniques (MRI, CT), a tumor size can be determined, at baseline, and during treatment at different time points
Clinicians prefer to dichotomize the outcome:
Remission:
Tumor size reduction to at most x% (e.g. 20%), of its original size at baseline, at 4 weeks, as a consequence of treating the patient with a «loading dose»
Remission rate = Proportion of patients achieving a remission
Relapse: After remission, the tumor grows back to more than y% (e.g. 40%) of its original size
Stabilize: After remission/relapse, treat with a «maintenance dose» to achieve another remission

Outcomes of interest: Relapse, remission, stabilize
6 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Inference on remission / relapse / stabilizing rates can be derived from inference on the continuous outcome

Outcomes of interest: Relapse (remission, stabilize)
7 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
In this presentation: Concentrate on relapse rate, i.e. dose finding for loading dose

Adaptive dose de-escalation design (loading dose)
8 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Start with a high loading dose, e.g. MTD
De-escalate the loading dose, in steps, in cohorts of one or more patients
Data analysis: Bayesian analysis on tumor size at 4 weeks (absolute or in % change); parametric (sigmoidal dose-response model) or ANOVA (i.e. no parametric assumption for dose-response shape)
After each cohort, update the Bayesian analysis
Use PoC data to derive an informative prior
Need to define:
Target/objective: what do we mean by efficient loading dose ?
Decision criteria: i.e. when to de-escalate, or stop ?

Target / objective
9 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Remission rate at dose d: πd
Posterior densities for remission rate πd can be derived from the tumor size model, given data
Potential objectives for loading dose: Find smallest loading dose d with the following property (with a given level of confidence = level of proof)
πd > PRR (for a predefined target remission rate PRR, e.g. PRR = 70%)
πd > π10 – DRR (for a predefined difference DRR relative to MTD=10, e.g. DRR = 10%)
πd > π10 * RRR (relative difference RRR relative to MTD=10, e.g. RRR = 0.8)

De-escalation decision criteria
10 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Decision criteria, in words:
If we have high confidence that the current loading dose is sufficiently effective, we try the next lower dose
If we are still uncertain whether current loading dose is effective, we allocate another cohort at this dose
If we have low confidence that the current loading dose is sufficiently effective, we stop and select the last effective dose (i.e. the previous, higher dose)

De-escalation decision criteria
11 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
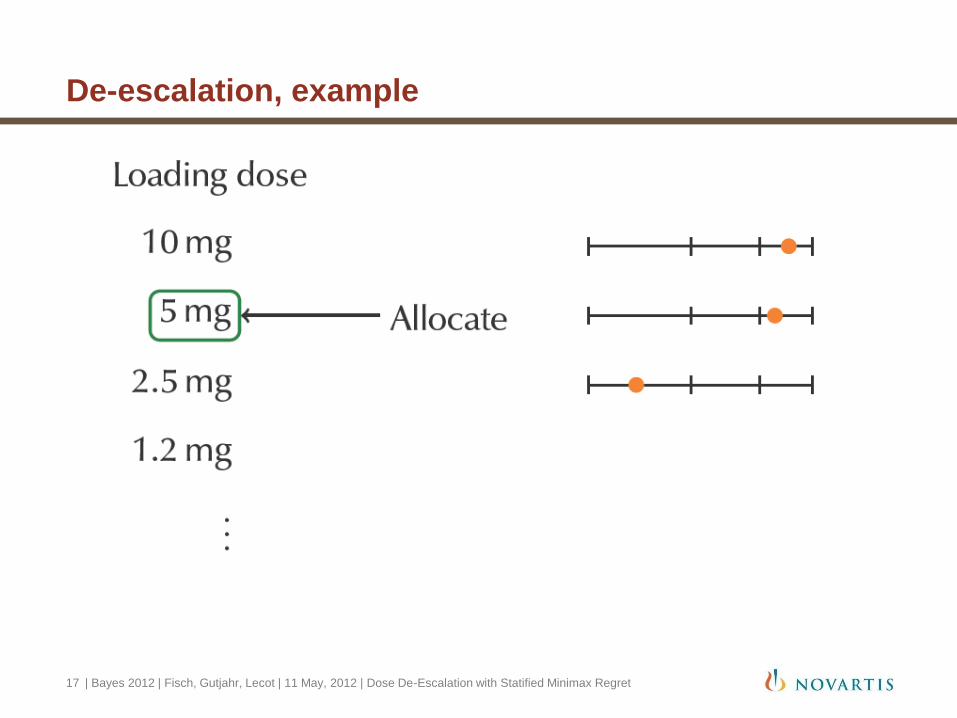
Decision criteria, in probabilities (with parameters δ1, δ2):
For the current dose d (i.e. the one most recently applied), calculate the (posterior) probability qd = prob(πd > PRR)
If qd ≥ δ2 then goto next lower dose
If δ1 ≤ qd < δ2 then assign another cohort to dose d
If qd < δ1 then stop, and declare the next higher dose as the minimally effective one

De-escalation, example
12 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret

De-escalation, example
13 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret

De-escalation, example
14 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret

De-escalation, example
15 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret

De-escalation, example
16 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
De-escalation, example
17 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret

Adaptive dose de-escalation design
18 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Advantages of the design:
Find target loading dose quickly, with a small number of patients
Expected number of patients receiving an ineffective dose is small
Quantified by running simulations
Disadvantages:
Essentially unblinded
Logistically more demanding, as compared to fixed design
What is an optimal design?
Can we do simulations to find an «optimal» design?
What are reasonable criteria for optimality?
What are the scenarios to optimize over?
Find the «overall» optimal design parameters δ1, δ2

General simulation model
19 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Elucidate biological/clinical assumptions
Build a temporal random effects dose-response model (to allow for simulating loading dose and maintenance dose effects)
For loading dose only: dose-response model (at week 4)

Loading dose simulation model
20 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Reduce temporal model to 4 weeks: Emax-like model
Parameters with informative prior Q(μ10,σ2), from PoC trial
Effect μ10 and variance σ2 at dose 10μg, at 4 weeks
Assume homoscedasticity
Other dose-response parameters θ: Unknown
Define a design performance measure («utility») as a function of δ, θ, μ10, σ2
Overall design performance measure:
integrate out over dQ(μ10,σ2)*dP(θ) -> solution strongly depends on the choice of uninformative P(θ)
integrate out over dQ(μ10,σ2); choose a plausible metric of overall performance, under reasonable scenarios for θ: (θ1, θ2, θ3, ...)
Find the parameters δ which optimize the overall design performance
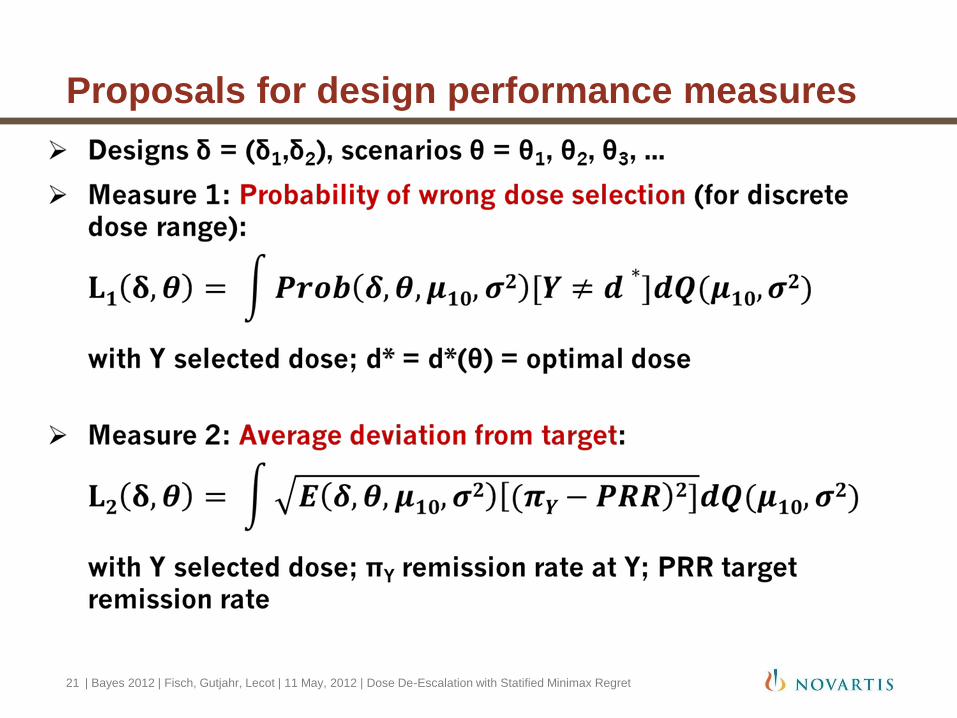
Proposals for design performance measures
21 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret

Optimality criterion, first try: Minimax regret
22 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Regret:
Maximal regret of design δ, over θ:
Minimax regret: Minimum (over all δ’s), of maximal regret (over θ) (for simulation: 0 ≤ δ1 ≤ 0.5 ≤ δ2 ≤ 0.95, in 0.05 increments)

Optimal minimax regret design
23 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Highest values for δ1,δ2 chosen: Almost never de-escalate ??

Optimal minimax regret design
24 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Highest value for δ2 chosen: Almost never de-escalate?? Does not make sense!
What’s wrong?
For scenarios where the highest dose is optimal, not de-escalating is the best design; this seems to dominate the minimax criterion
Need to downweight the regret for scenarios where the highest dose is optimal, in favor of the ones for lower target doses

Minimax regret design: stratified
25 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret

Optimality, second try: Stratified minimax regret
26 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Stratify the set of scenarios Θ into subsets Θ1U Θ2U Θ3U ..., such that Θi contains scenarios where the i-th dose is optimal
Stratified regret:
Standardize stratified regret to [0,1]:
Stratified minimax regret:

Optimality, second try: Stratified minimax regret
27 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret

Design optimality
28 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Minimax regret produces nonsensical optimal design
Stratified minimax seems reasonable: δopt = (δ1=0.15,δ2=0.85),
In general:
Need a design performance measure as a function of design and scenario R(δ,θ) (e.g. Regret)
Need a way to summarize R(δ,θ) over scenarios θ (e.g. maximization, stratified maximization, expectation)
Minimize over δ

Design optimality
29 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
Refine optimality / design performance measure, i.e. utility
Stratified minimax regret is just a try
Consider refining the utility:
Ideally, in units of Net Present Value
Incorporate number of patients
Incorporate number of patients on sub-therapeutic dose
Based on simulations, report aspects of design performance in tabular and graphical form
Use Decision Analysis tools to discuss utility / optimality with the team

Summary
30 | Bayes 2012 | Fisch, Gutjahr, Lecot | 11 May, 2012 | Dose De-Escalation with Statified Minimax Regret
De-esclation seems to be a reasonable approach
Stratified minimax optimal design seems to perform well
Project specifics influence design choices:
Target dose definition (PRR, DRR, RRR)
Design performance measures (L1, L2, ..)
Optimality criteria
needs a lot more work!
Additional complexity when looking at loading dose + maintenance dose