presentación de powerpoint -...
TRANSCRIPT

DILI (Hepatotoxicidad)
Raúl J Andrade Gastroenterology Service,
University Hospital,
Department of Medicine, University of
Málaga, IBIMA and CIBERehd
October 31, 2015

Relatively uncommon, potentially severe
-Chief cause of ALF
-Rank among main reasons for drug atrittion
Diagnosis after exclusion of alternative causes
-No diagnostic biomarkers
-A wide range of phenotypes
Many drugs involved
Drug-induced liver injury

916
220
142
36
137 112
25 15 18
134
245
0
100
200
300
400
500
600
700
800
900
1000
AP
AP
Dru
g
Hep
B
Hep
A
Auto
imm
Isch
em
ic
Wils
on's
Bu
dd
-Ch
iari
Pre
gn
an
cy
Oth
er
Inde
ter
Etiology of Acute Liver Failure in the USA Adult Registry (n = 2,000)
ALF Study Group, Jan 2013
46%
11% 12%

Drug-induced liver Injury
Proper case definition and reliable epidemiology
Identification of susceptible subjects and mechanisms
Clinical and histological phenotypic characterization
Prediction of severe outcomes Diagnosis

Proper case definition and reliable epidemiology Identification of susceptible subjects and
mechanisms
Clinical and histological phenotypic characterization
Prediction of severe outcomes Diagnosis

Drug-induced liver injury (DILI)
Criteria for liver injury (Benichou, J Hepatol, 1990)
> 2 xULN ALT > 2 xULN conjutated BL Combined increase in AST, ALP and total BL, with at least one being > 2 xULN Criteria for DILI qualification case (Aithal et al, Clin Pharmacol
Ther, 2011)
≥ 5 xULN ALT ≥ 2 xULN ALP ≥ 3 xULN ALT + > 2 xULN TBL
R= ALT/AP (ULN) Hepatocellular > 5 Mixed >= 2=< 5 Cholestatic < 2

DILI incidence rate
Population based studies
UK (de Abajo et al, 2004)**
2.4 per 100 000 person-year France (Sgro et al, 2002)* 13.9 per 100 000 person-year
Iceland (Björnsson et al, 2013)*
19.1 per 100 000 person-year *prospective study, **retrospective study

Prescrip
tion
rate p
er perso
n
15-24
Epidemiology of Drug-induced Liver injury in Iceland n=251,860
Annual Incidence of DILI 19.1 per 100.000
Björnsson et al Gastroenterology 2013; 144(7):1419-1425
Case qualification: ALT > 3N
96 patients (27% jaundiced,
23% hospitalized)

DILI demographics and clinical features
Spain1 Latin
America2 USA3
DILI patients 603 73 300
Male/female (%) 51/49 40/60 40/60
Age, mean (range) 54 (13-88) 52 (15-86) 48 (ND)
Jaundice, % 69 71 69
Hospitalization, % 54 54 60
Type of injury
Hepatocellular, % 55 50 57
Cholestatic, % 25 32 23
Mixed, % 20 18 20
Liver related death or transplantation, %
3.8 5.1 6.0
1Lucena et al, 2009
2Bessone et al, 2013
3Chalasani et al, 2008

Causative agents
ATC system group code
*Fontana et al, Gastroenterology 2014

Drug Patients treated,
n
Prescription, n
Cases, n
Proportion Per 100,000
95% CI 95% CI
Amoxicillin /clavulanate 35,252 83,379 15 2350 43 24 70
Diclofenac 54,889 112,801 6 9148 11 4 24 Azathioprine 532 3054 4 133 752 205 1914 Infliximab 593 a 4 148 675 184 1718 Nitrofurantoin 5476 12,034 4 1369 73 20 187 Isotretinoin 2169 7978 3 732 138 29 404 Atorvastatin 7385 34,171 2 3693 27 4 98 Doxycycline 32,677 54,232 2 16339 6 1 22
Only drugs associated with at least 2 cases of DILI are shown.
CI, confidence interval.
a Most patients on infliximab received continuous prescriptions
Epidemiology of Drug-induced Liver injury in Iceland n=251,860
Björnsson et al Gastroenterology 2013; 144(7):1419-1425

Proper case definition and reliable epidemiology Identification of susceptible subjects and
mechanisms
Clinical and histological phenotypic characterization
Prediction of severe outcomes Diagnosis

Hepatocyte
Drug 3 DAMPs
HMGB1 RNA HSPs
DNA
Toxicity
(drug, T/B cell mediated)
Toll-Like Receptors
Antigen Presenting cell
Drug
Drug
Drug
Drug 1
5
2
4
TH B
CTL
IL-6, TNFα
Co- stimulation
Neo- antigen
MHC TCR
IL-13
IL-17 IL-21
Metabolism CYP,GSH
GSHT
Lymphocytes
Perforin Granzyme
Pathogenesis and progression of drug-induced liver injury
De Lemos et al Semin Liver Dis 2014;34:194–204.

Genome-wide association (GWA)
studies
201 amoxicillin-clavulanate DILI patients (96 English,
56 American and 49 Spanish cases) and 532 controles

Chromosome 6, HLA associations
HLA-DRB1*1501-DQB1*0602 (classII)
HLA –A*0201 (class I)
Lucena et al, Gastroenterology 2011

Flucoxacillin: HLA-B57*01
A-C and lumiracoxib: HLA-
DRB1*1501-DQB1*0602
HLA –A*0201
Ximelagatran
Daly et al Nat Genet 2009 Lucena et al Gastroenterology 2011
OR= 80 , low predictive positive value
High predictive negative value
GWAS: chromosome 6 (HLA genes)
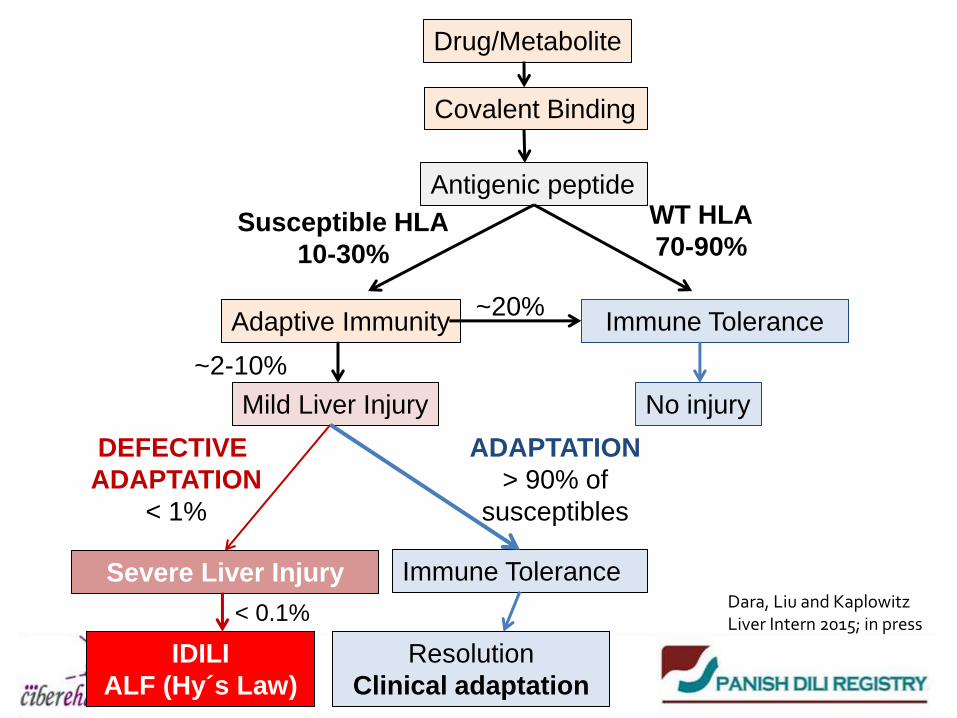
Drug/Metabolite
Covalent Binding
Antigenic peptide
Adaptive Immunity Immune Tolerance
No injury Mild Liver Injury
Severe Liver Injury Immune Tolerance
IDILI
ALF (Hy´s Law)
Resolution
Clinical adaptation
Susceptible HLA
10-30%
WT HLA
70-90%
~20%
~2-10%
DEFECTIVE
ADAPTATION
< 1%
ADAPTATION
> 90% of
susceptibles
< 0.1% Dara, Liu and Kaplowitz Liver Intern 2015; in press

Clinical manifestation and outcome
Immune/ inflammation
RepairTissue injury
Drug
Host factors
Genetic variantsRace/ethnicity
AgeGender
Reproductive statenutrition, alcohol, smoking
Lifestyles Disease conditions
MedicationsGut flora
Drug properties
PhysiochemicalPharmacological
ToxicologicalBio-physiological effects
Host response to injury insult
Cellular injury initiation
Pharmacological responsesReactive metabolites, drug elimination
Toxicological responsesCovalent binding, haptenization,
oxidative stress, mitochondrial injury, ER stress
Cell deathApoptosis, necrosis, DAMP release
Chen et al J Hepatol 2015 Apr 22. pii: S0168-8278(15)00299-8. doi: 10.1016/j.jhep.2015.04.016

-Doses ≥ 50 mg/daily associated with death, liver failure
and liver transplantation1
•-Majority (77%) of the drugs incriminated in DILI in the
SADRAC and Spanish DILI Registry were prescribed at
doses ≥ 50 mg/daily1,2
•-Many false positives
Toxic potential of the drug in IDILI: the effect of dose
1 Lammert et al Hepatology 2008; 47: 2003-2009,
2 Lucena et al Hepatology 2009; 49: 2001-2009.
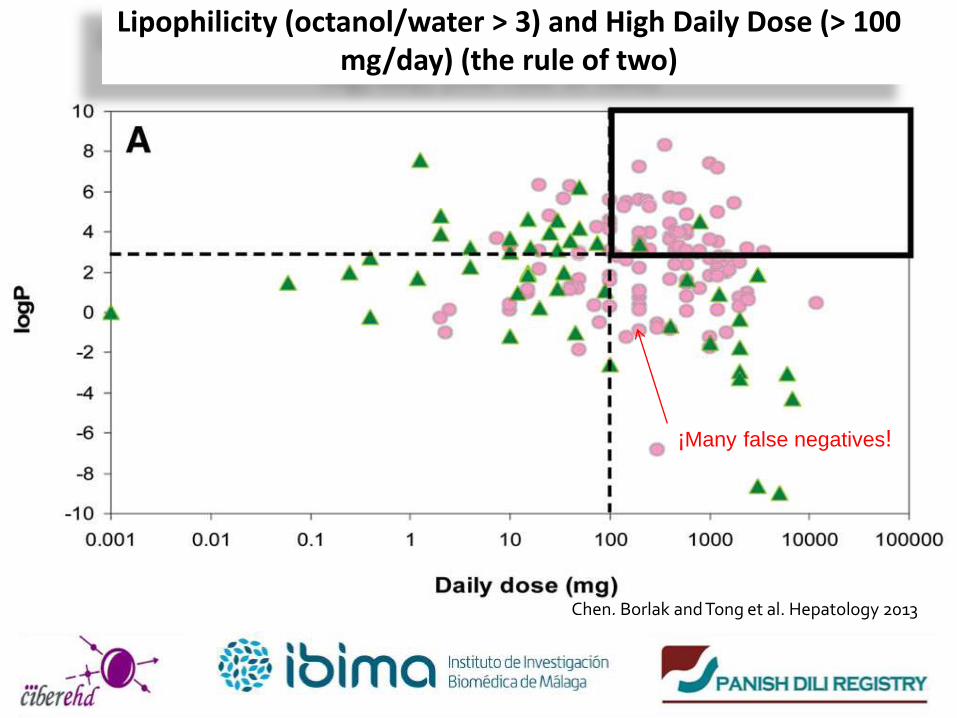
Chen, Borlak and Tong et al. Hepatology 2013
Lipophilicity (octanol/water > 3) and High Daily Dose (> 100 mg/day) (the rule of two)
¡Many false negatives!
Morgan et al Toxicol Sci 2010
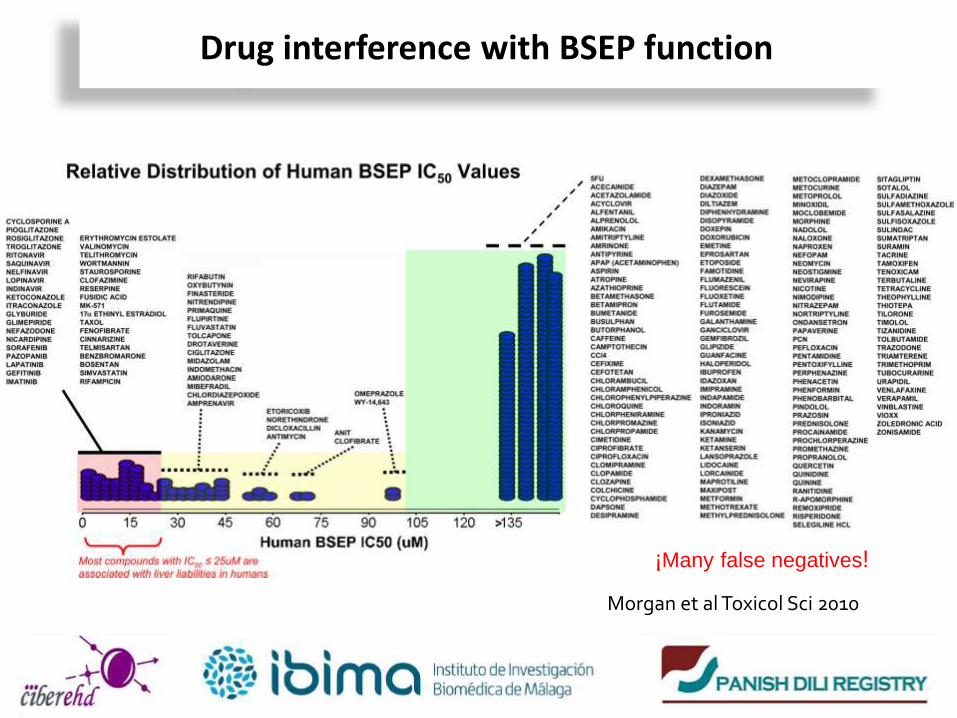
Drug interference with BSEP function
¡Many false negatives!

Proper case definition and reliable epidemiology Identification of susceptible subjects and
mechanisms
Clinical and histological phenotypic characterization
Prediction of severe outcomes Diagnosis

Type of liver injury and gender

• Liver biopsies from 249 cases of suspected DILI blindly reviewed – 18 DILI patterns identified
Kleiner et al., Hepatology, 2014 ;59:661-70
.1
1
10
100
1 2 3 4 5 10
Acute
Hepatitic
Chronic
Hepatitic
Acute
Cholestatic
Chronic
Cholestatic
Cholestastic
Hepatitic
Zonal
Necrosis
R
8 74 25 23 35 51

Age and gender as DILI risks
N
umbe
r of
cas
es
DILI according to age and gender
Age (years) Type of liver injury according to age and gender
Peak age of DILI
occurs earlier in
women (40-49 vs
60-69 years)
Women <60 years are
more prone to develop
hepatocellular DILI,
while men >60 years
cholestatic DILI
Lucena et al, Hepatology 2009

DAÑO HEPATOCELULAR DAÑO COLESTÁSICO
*p<0.001 †p<0.001 **p=0.012
††p=0.01
Test de Kruskal-Wallis: *p<0.001 AAS vs resto de clases terapéuticas, **p=0.012 AAS vs CNS y HDS, †p<0.001 AAS vs resto
de clases terapéuticas, ††p=0.01 AAS vs amoxicilina clavulánico, antineoplásicos y cardiovasculares.
Proper case definition and reliable epidemiology Identification of susceptible subjects and
mechanisms
Clinical and histological phenotypic characterization
Prediction of severe outcomes Diagnosis

Risk of drug-induced acute liver failure (ALF)
Predictive risk factors of ALF
TBL (at recogntion, peak ALT and peak TBL
AST/ALT (recognition, peak ALT, peak TBL)
Hepatocellular damage (recognition, peak TBL)
Female gender
Logistic regression analysis of demographic, clinical and laboratory parameters in
DILI cases with (31) and without (774) ALF resulting in death or OLT
Gastroenterology 2014; 147: 109-118
ALF incidence rate: 32 of 771 DILI patients (4.2%)

Robles-Díaz M et al Gastroenterology 2014; 147(1):109-118.
Prognostic algorithm for ALF in DILI Chi-squared automatic interaction detection (CHAID)
Specificity 82%
Sensitivity 80%
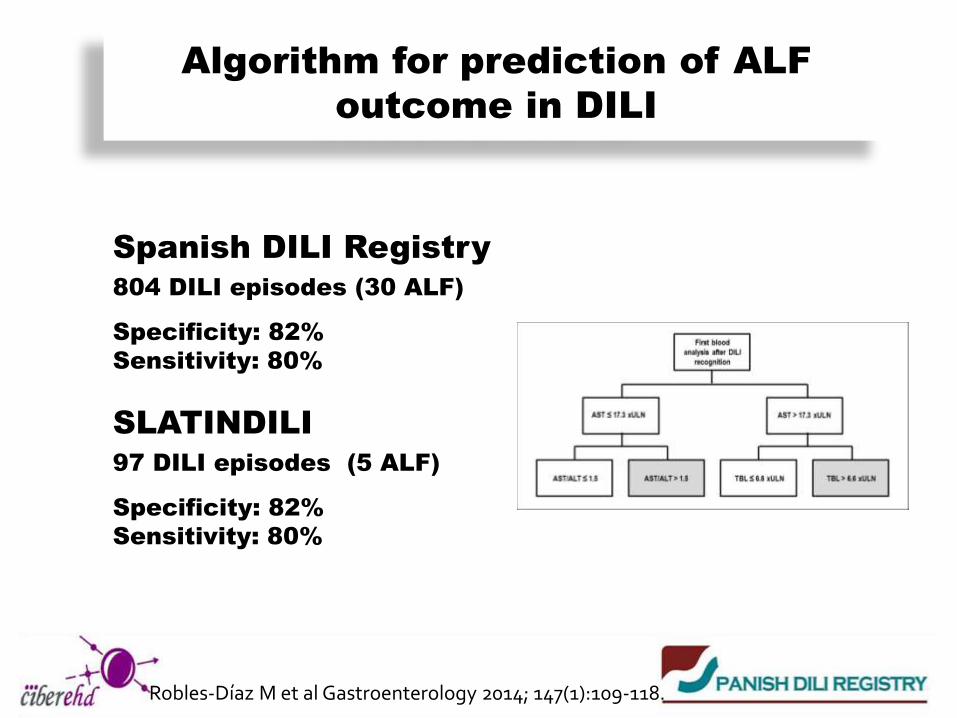
Algorithm for prediction of ALF
outcome in DILI
Spanish DILI Registry
804 DILI episodes (30 ALF)
Specificity: 82%
Sensitivity: 80%
SLATINDILI
97 DILI episodes (5 ALF)
Specificity: 82%
Sensitivity: 80%
Robles-Díaz M et al Gastroenterology 2014; 147(1):109-118.

(better Hy’s Law ?)
Need to improve prediction of severe DILI outcome?

Days to resolution
0-60 61-90 91-180 181-365 366-730 731-1095 1096-2000 2001-3020
Hepatocellular cases (N=193)
71 30 57 27 4 3 1 -
Cholestatic cases (N=46)
9 8 17 10 - - 2 -
Mixed cases (N=46)
15 13 12 4 1 - - 1
The inset shows the same data on an enlarged y axis
p=0.4 by long-rank
test
Chol, p= 0.95
HC, p= 0.9
Mix , p= 0.97
348 d
Abbreviations: Chol: cholestatic, HC: hepatocellular, Mix: mixed
Chronicity definition
Robles-Díaz et al unpublished data 2015

Proper case definition and reliable epidemiology Identification of susceptible subjects and
mechanisms
Clinical and histological phenotypic characterization
Prediction of severe outcomes Diagnosis

Step-by-step approach
for suspected DILI
cases
*García-Cortés M, Stephens C, Lucena MI, Fernández-Castañer A, Andrade RJ.. Causality Assessment Methods in Drug Induced Liver Injury: Strengths and Weaknesses. Journal of Hepatology, 2011; 55: 683-691
¡There is an urgent need of
Specific biomarkers!

•Bacterial Hepatitis •Wilson´s Disease
•Deficit of α- 1antitrypsin
•Haemocromatosis
A, B, C, E
Viral
hepatitis Biliary
obstruction
Autoinmune
Hepatitis.
PBC
Alcoholic
Hepatitis
Isquemic
Hepatitis
Diseases
Dalton et al Aliment Pharmacol Ther 2007 Davern et al Gastroenterology 2011


• Temporal relationship (0 to 2) • Course (-2 to 3) • Risk factors (0 to 2) • Concomitant drug (0 to -3) • Non-drug causes (-3 to 2) • Prior reports/ information (0 to 2) • Re-challenge (-2 to 3) Score (-8 to 14) Highly probable >8 Possible 3-5 Excluded ≤0 Probable 6-8 Unlikely 1-2
Danan et al J Clin Epidemiol 1993;46:1323-1330
CIOMS/RUCAM

Causality scales: Weaknesses
Often complex and time consuming
Lack of clear user instructions
Lack of case information or follow-up data can lead to reduced probability
Do not discriminate among concomitant drugs
Evaluation of atypical cases remains challenging
Restrictive criteria and arbitrary weighting of factors may lead to incorrect evaluations
Do not substitute clinical judgement
García-Cortés M et al J Hepatol, 2011; 55: 683-691

Summary
DILI is not so rare as formerly thought
Idiosyncratic DILI results from complex drug-host interactions and the failure to adapt to minor degree of injury
DILI phenotype is influenced by age and sex
Demographics and routine liver biochemistry can be of help in predicting fulminant course
Causality assessment is complex and uncertain and current
diagnostic scales are imperfect

H. Torrecárdenas, Almería: MC Fernández, G Peláez, M Casado
H. Virgen Macarena, Sevilla: JA Durán, M Villar
H. Universitario Virgen de Valme, Sevilla: M Romero,
H. Central de Asturias, Oviedo: L Rodrigo-Saez, R Perez-Alvarez
H. de Puerto Real, Cádiz: JM Pérez-Moreno, M Puertas
H. Universitario San Cecilio, Granada: J Salmerón, A Gila
H. Germans Trias i Puyol, Barcelona: I Barriocanal, Eva Montané, J Costa
H. Costa del Sol, Málaga: JM Navarro, JF Rodríguez
H. 12 de Octubre, Madrid: T. Muñoz-Yagüe, JA Solis-Herruzo
H. Marqués de Valdecilla, Santander: F Pons, J Crespo
H. Sant Pau, Barcelona: C Guarner, G Soriano
H. Carlos Haya, Málaga: M Jiménez, R González-Grande
H. Xeral-Calde, Lugo: S Avila-Nasi
H. Puerta de Hierro, Madrid: JL Calleja, J de la Revilla
H. Nuestra Sra. de Aranzazu, San Sebastián: M García-Bengoechea, J Arenas
H. de Mendaro, Guipuzcuoa: A Castiella, E Zapata
H. Alto Deba, Mondragón, Guipuzcuoa: P Otazua
H. de Basurto, Bilbao: S Blanco, P Martinez Odriozola
H. Clínico Provincial: M Bruguera, P Ginés
H. Morales Messeguer: H Hallal
H. de Albacete, Albacete: JM Moreno
H. Puerta del Mar, Cádiz: P Rendón
H. de Salamanca: F González
H. De Alcorcón: C Fernández
H. De Sagunto: J Primo
H. La Fe: M Prieto
Collaborating hosptial units in the Spanish DILI Registry
