presentation given at the launch of countdown in cameroon
TRANSCRIPT

Le Compte à Rebours est Lancé !
Professors Louis-Albert Tchuem Tchuenté, Samuel Wanji & Russell Stothard

Overview and introduction
Helminth Infections Soil-transmitted helminth infections
• Ascariasis-Trichuriasis-Hookworm
Lymphatic filariasis
Onchocerciasis
Schistosomiasis
Dracunculiasis (guinea-worm disease)
Cysticercosis
Echinococcosis
Foodborne trematodes infections
and other "neglected zoonotic diseases"
Bacterial Infections Leprosy Trachoma Buruli ulcer Endemic treponematoses
Viral Infections Dengue Rabies
Protozoan Infections Human African trypanosomiasis Chagas disease Leishmaniasis
WHO focus on 17 Neglected Tropical Diseases
Soil-transmitted helminth infections
• Ascariasis-Trichuriasis-Hookworm
Lymphatic filariasis
Onchocerciasis
Schistosomiasis
Trachoma

Disease Intervention approaches Tool Availability AFR Goal
Soil-transmitted Helminthiasis
Preventive Chemotherapy (PC)
Tool-Ready
Control
Schistosomisis
Lymphatic Filariasis
EliminationOnchocerciasis
Blinding trachoma
Guinea worm disease
Innovative & Intensified Disease Management
(IDM)
Tool-Ready
Eradication
Leprosy EliminationHuman African Trypanosomiasis
(HAT)*
Tool-DeficientBuruli ulcer
ControlLeishmaniasis
10 Priority NTDs in WHO African Region

2015 2020Eradication • Dracunculiasis (guinea-worm disease) • Yaws
Global elimination
• Lymphatic filariasis• Blinding trachoma
Regional elimination
• Onchocerciasis in Latin America• Schistosomiasis in the Eastern
Mediterranean, Caribbean, Indonesia and Mekong River basin
• Schistosomiasis in the American and the Western Pacific regions
Country elimination
• Onchocerciasis in Yemen • Onchocerciasis in selected countries in Africa
• Schistosomiasis in selectedcountries in Africa
WHO NTD Roadmap: targets and milestones for 2015-2020 period
2012

694M
705M
711
M
729M
700M
0
10
20
30
40
50
60
70
80
90
100
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
Target date for full PC scale-up
20
20
go
als
WHO target of 75% coverage across diseases
%
Projected % of
people receiving
PC for at least
one disease
(including LF,
ONCH, SCH and
STH) out of total
number that
require PC
WHO identify scale-up of future PC to reach 2020 targets
Urgent need to address
bottlenecksin scale-up
of PC
and
to acceleratetowards
WHO 2020 targets

History behind NTD control programmes in Cameroon
NTD Control/EliminationProgramme
Datestarted
Onchocerciasis 1998
HAT 1998
Buruli Ulcer, Yaws, Leishmaniasis, Leprosy*
2001
Schistosomiasis and STH 2003
Lymphatic Filariasis 2008
Trachoma 2010
6 Existing NTD Control Programmes National NTD Master Plan 2012-2016Launched in Oct 2012
and currently been updated until 2020
Drug Distribution Channels for PC-NTDs
• School-based de-worming for Schistosomiasisand STH
• Community-based interventions for Onchocerciasis , Lymphatic Filariasis and Trachoma
• Vaccination campaigns for de-worming Pre-School Aged Children (<5 years)

• Insufficient few impact studies and need for better financial forecasting
• Period of school-based campaign too close to end of school year
• Delays in reporting treatment results from lower to higher levels
• Co-endemicity Lymphatic Filariasis/Onchocerciasis/Loa Loa Low treatment coverage
• Incentives issues for drug distributors demotivation and increase of attrition rates
• High reinfection rates (transmission dynamics) & limited vector control
Some key bottlenecks to NTD control in Cameroon

A broader perspective on COUNTDOWN
Professors Russell Stothard & Mark Taylor

Why was COUNTDOWN needed?
What will COUNTDOWN do?
What lasting legacy will COUNTDOWN leave?

Looking towards WHO’s 2020 Roadmap & SDG’s 2030 Targets
• Preventive chemotherapy • NTDs exacerbate poverty & suffering

Thinking further ahead 2015-2030: further domestic funding needed
The WHO/World Bank Framework & SDGs
• A minimum of 80% essential health services coverage
• 100% financial protection from out-of-pocket expenses
Control and elimination of NTDs is a ‘litmus test’ of progress
implementation research to optimise/strengthen performance
Reducing poverty in Africa with implementation science for NTD control
Programme of implementation research to inform the effective and sustainable scaling-up of integrated Neglected Tropical Disease (NTD) control initiatives
OJEU: 2013/S 181-312697
Open tender: one final application for £8M in the Nov. 2014 - Oct. 2019 period
In 2008, DfID committed £50M for to support control of NTDs
Implementation portfolio including:Sightsavers (Trachoma)Schistosomiasis Control Initiative (ICOSA)Filariasis Programmes Support Unit (LSTM)UNITED (Nigeria)
….with The Research and Evidence Division supporting

Why was COUNTDOWN needed?
What will COUNTDOWN do?
What lasting legacy will COUNTDOWN leave?

Rationale for research themes and approaches
PC NTDs
Diseases: ONCH*
LF
SCH
STH
(TRA)
Drugs: IVM/DEC/ALB/MEB/PZQ
(ZRT)
DOXY*

Q1) What are effective, cost-effective, sustainable and acceptable current and complementary strategies for scale-up?
Q4) How can integrating NTD programmes strengthen health systems and foster cross-sector working (e.g. sanitation & agriculture)?
Q2) What generalizable factors influence the acceptance, effectiveness, efficiency, and equity impact of scale-up within the health system?
Q3) What are the most effective strategies to work with CDDs and CHW to extend scale-up of MDA to include hard-to-reach communities?
Our IR questions were subsequently developed and are:
Multi-disciplinary studies: from social science to field epidemiology

How we will do it
IntegratedComplementary Strategy Theme
ICST 1
ICST 2
Liberia GhanaCameroon
MDA Scale-up Theme (MST 1 – 3)
elimination
: country & context-specific settings of MDA
MST 1: Evidence synthesisPaul Garner and Cochrane group
MST 2: Applied social scienceSally Theobald and Margaret Gyapong
MST 3: Health economicsLouis Niessen
ICST 1: ‘Hotspots’ and SAEs Mark Taylor, Lisa Riemer/Jo TurnerNana Biritwum and Sam Wanji
scale-up in Nigeria & responsive research
ICST 2: Access to MDA and CLTS Russ Stothard, Emily Adams, Kamal KarLouis Tchuem-Tchuente and Mike Osei
control

Impact and pathways to achievement
IMPACT: Reduced morbidity,mortality, and povertyassociated with NTDs throughincreased knowledge andevidence for cost effectivescale-up and sustainablecontrol and elimination of NTDsas a public health problem inline with the WHO 2020 NTDRoadmap
Community
Global
Regional
National
District

What are the COUNTDOWN expected results?
2: Provide rigorous and generalizable evidence to improve and support scale-up of MDA programmes, fostering optimal co-ordination
3: Develop knowledge management strategy and multi-sectoral platforms for cross-talk and dialogue, ensuring open access knowledge products
4: Increase research capacity and integrate multi-sectoral evidence for optimisation of NTD control programmes
Our results are framed in four outputs:
1: Form a vibrant multidisciplinary IR consortium engaged with national NTD programmes and international stakeholders

Why was COUNTDOWN needed?
What will COUNTDOWN do?
What lasting legacy will COUNTDOWN leave?

A successful launch on March 12th at LSTM, hosted policy positioning meetings

Formal research outputs already starting to change opinions and focus efforts

Launch of COUNTDOWN in Ghana 14th October
In October there are 4 key events before the end of inception year
Chairing 2 sub-meetings at COR-NTD in USA 22/23rd October
Cameroon launch 9th and RU uptake meeting on 12th October
Year 2 activities set to start with on-the-ground actions in country in 2016

Research structure in across two universities and interface with NTDs
- Buea Evidence synthesis, Social science, Health economics, ONCHO
- Yaounde Evidence synthesis, Social science, Health economics, SCH, STH
COUNTDOWN in Cameroon

New ways to rid Cameroon of River Blindness (Onchocerciasis)
Professor Samuel Wanji

Community-directed treatment with ivermectin (CDTI)

CDTi after 14 years in SW Region Cameroon
39 communities, 3 river basins, SW Cameroon

Poor coverage is linked to fear of severe adverse reactions from eye worm

Doxycycline, a proven safe Onchocerca cure targeting Wolbachia
0
10
20
30
40
50
Ivermectin Doxycycline
Active Worms

Community based intervention with doxycycline
Adopted as policy drug for alternative strategy by APOC, 2014
"many people are asking for the drugs in my community and those who have already been treated are still requesting for another treatment" CHI, Sanke
"I used to have a nodule on my knee, but it has disappeared after doxycycline treatment” Mbokambo community member
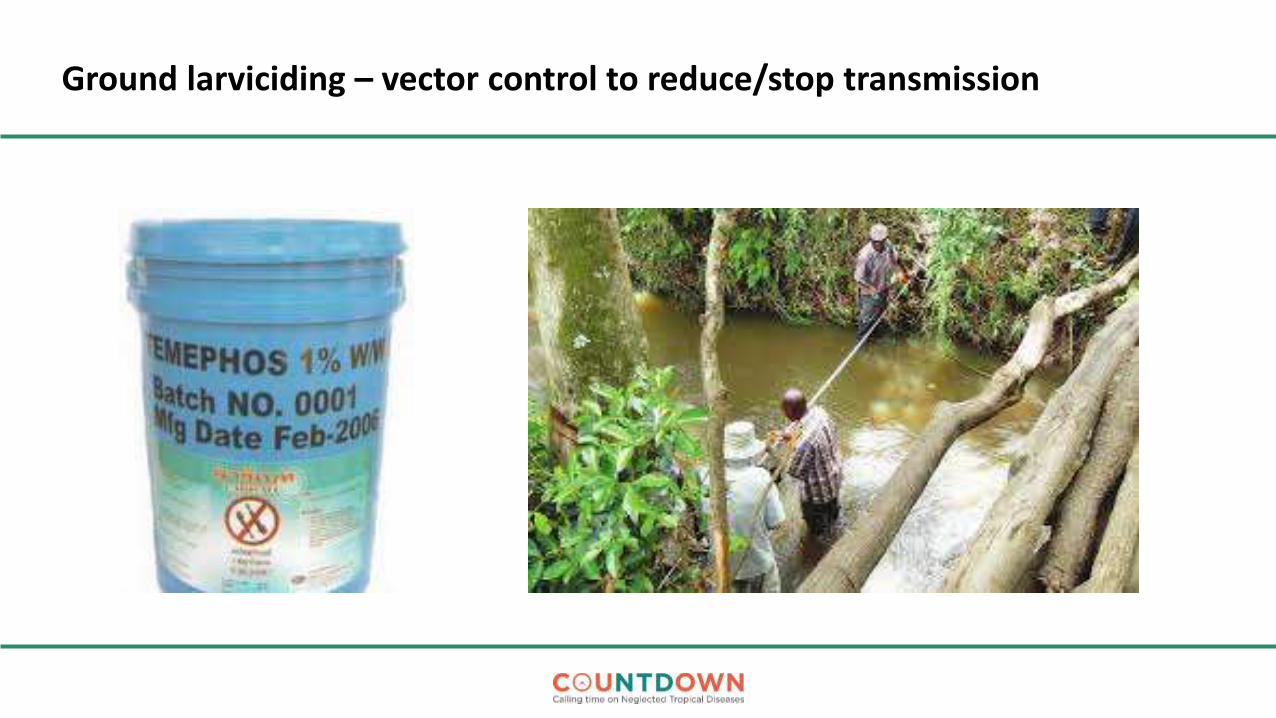
Ground larviciding – vector control to reduce/stop transmission

ICST-1
• How to implement these two alternative strategies?
• Test and treat with doxycycline in 10,000 people in Meme River Basin
• Combination with Temephos ground larviciding

Shifting from control to elimination of schistosomiasis
Professor Louis-Albert Tchuem Tchuenté

• Wide distribution of disease, 2M people infected
• Over 5 million people at risk of infection
• Highest endemicity in the Northern regions
• Occurrence of 3 schistosome species, several host snails
(S. haematobium, S. mansoni, S. guineensis)
• Various transmission dynamics, including single and mixed species infections
Schistosomiasis distribution
Main Features of schistosomiasis in Cameroon

Systematic deworming of school-age children and groups at risk …
Main Control Strategy: School-based delivery of PZQ
… in collaboration with the Ministry of Basic Education and the Ministry of Secondary Education

Steady Progress in SCH and STH treatments across Cameroon
0
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
6,000,000
7,000,000
8,000,000
9,000,000
2006 2007 2008 2009 2010 2011 2012 2013 2014
STH Schistosomiasis • MDA boosted by donated medicines
• Increase of Schistosomiasistreatment from 35 000 in 2006 to 2 818 604 in 2014
• Increase of STH treatment from 170 000 in 2006 to 8 252 171 in 2014

However, better access to PZQ and other Interventions are needed
• Pre-School-age children are not treated
• All SAC out-of-school are not reached
• Adults are not treated
• Rapid reinfection rates in high transmissionsettings, due to intense water contacts, requirealternative strategies
• Need to implement environment control: snailcontrol, sanitation improvement

ICST-2
• Scale-up of integrated access to Mass Drug Administration and Community Led TotalSanitation for the control and elimination of SCH and STH:
Equitable access to treatment for preschool-aged-children, out-of-school-children and adults Contribution to Universal Health Coverage
Improve of hygiene and sanitation in communities, snail monitoring
• Optimized strategies related to transmission dynamics:
Treatment twice per year Reduction of the impact of rapid reinfection rates in hightransmission settings
• Applied Social Science research to address impediments in control and scale-up
• Female genital schistosomiasis and capacity development for surveillance

In conclusion – implentation research of international importance
P C - NTDs
environment
COUNTDOWN will help moving from single intervention (treatment) to co-ordinated interventions optimizing impact.
PHASE approach:
Preventive chemotherapy,
Health education and behavioural change ,
Access to clean water and safe practices,
Sanitation and hygiene,
Environmental control

A New Asset: China-Africa Cooperation for Schistosomiasis Elimination
6th October signing the MOUIn Cape Town, South-Africa
Thank You for Your Attention
At the dawn of a new era of NTD control and a future
towards elimination