presentation - reviews of the medicare benefits schedule ... · reviews of the medicare benefits...
TRANSCRIPT

Reviews of the Medicare Benefits Schedule and the NHMRC Professor Bruce Robinson Chair, MBS Review Taskforce Chair, NHMRC
Sydney 18 April 2016

| 1
Today’s presentation
▪ The case for review and change in health and medical research
▪ Overview and update on the work of the MBS Review Taskforce
▪ NHMRC and translational research
▪ Key points from the Primary health Care Advisory Group report

| 2
What motivates me?
▪ Health care has advanced and the MBS has not kept pace ▪ The MBS contains anomalies and is not consistent with current clinical practice
guidelines ▪ There is a significant amount of low or no-value care, some of which is driven by the
MBS ▪ The MBS is not a driver of quality care and data collection is inadequate ▪ Belief in health and medical research to better inform health systems and individual
patient care
| 3
What’s the gap?
▪ The MBS is seen as a funding instrument, not as a tool for better care ▪ There is frustration that the MBS has not been over-hauled in 30 years ▪ Clinicians are aware of the anomalies and variations in use of the MBS ▪ Clinicians are frustrated by the ‘waste’ ▪ NHMRC success rates are only 13%, career structures are very poor
| 4
How will we address these issues?
▪ A clinician-lead review of the MBS and a review of Primary Health Care ▪ A review of the NHMRC – specifically to look for solutions to a very complex strategic
and funding dilemma which has long-term implications for health and medical research in Australia
▪ Solutions require assistance from all of the people who work in this area and the people who pay for, and benefit!

| 5
Why do I believe this is going to work? Who else believes this?
▪ Clinicians and consumers are supportive ▪ The Colleges are supportive ▪ The AMA is supportive ▪ The Minister is supportive ▪ The process is using evidence, data, clinician opinion and consumer input ▪ We are proceeding methodically, with good support from the Department of
Health ▪ The NHMRC review is being lead by Steve Wesselingh and supported by a
range of levels of researchers
| 6
What’s in it for you?
▪ Health consumers – better health care ▪ Community/society – better value for taxes ▪ Clinicians – satisfaction that the care is more efficient, appropriate, effective
and the ‘best and latest’ ▪ Corporates – costs aligned to rebates, not dependent on ‘cross-subsidies’ ▪ Less time wasted on unsuccessful research applications, better career
structures for researchers, assistance with commercialization and innovation, clearer delineation of roles of NHMRC, MRFF and other funding agencies
The Medicare Benefits Schedule Review
Our objectives, methodology, and state of play
7
| 8
The MBS Review
▪ Established by Health Minister Sussan Ley in June 2015
▪ At $20 billion per annum, MBS is the largest single health program – around 30 per cent of Commonwealth health expenditure – Overall health expenditure exceeds $150 billion per annum
▪ More than 5,700 services funded – many haven’t been re-examined or evaluated since listing
| 9
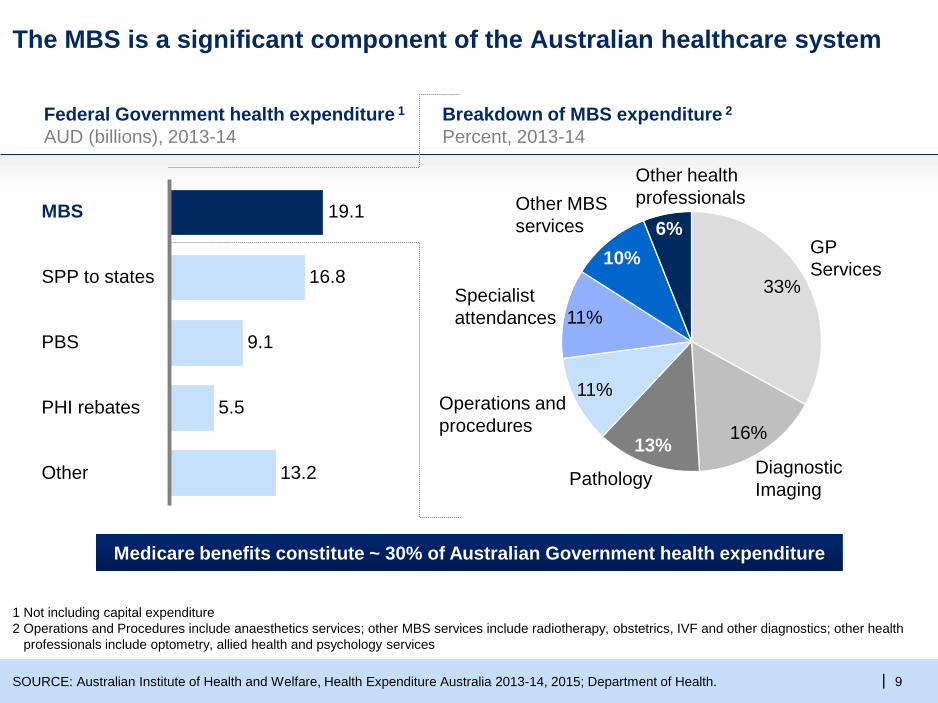
The MBS is a significant component of the Australian healthcare system
Federal Government health expenditure 1 AUD (billions), 2013-14
1 Not including capital expenditure 2 Operations and Procedures include anaesthetics services; other MBS services include radiotherapy, obstetrics, IVF and other diagnostics; other health
professionals include optometry, allied health and psychology services
Medicare benefits constitute ~ 30% of Australian Government health expenditure
Other 13.2
5.5
PBS
SPP to states
19.1
16.8
MBS
9.1
PHI rebates
Breakdown of MBS expenditure 2
Percent, 2013-14
GP Services
33%
Operations and procedures
11%
6%
11%
Pathology Diagnostic Imaging
16%
Other MBS services
Other health professionals
10%
13%
Specialist attendances
SOURCE: Australian Institute of Health and Welfare, Health Expenditure Australia 2013-14, 2015; Department of Health.
| 10
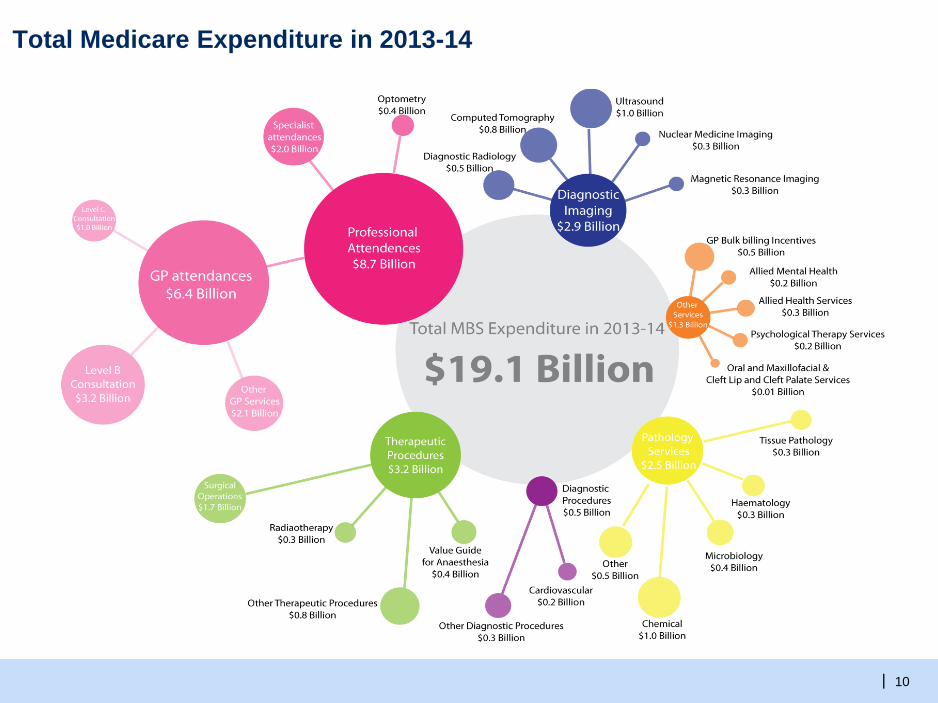
Total Medicare Expenditure in 2013-14

| 11
Expenditure through Medicare since 1984
| 12
Terms and references for the MBS review
Out of Scope In scope
▪ All current MBS items and the services they describe
▪ Increasing the value derived from services
▪ Concerns about safety, clinically unnecessary service provision and concurrence with guidelines
▪ Evidence for services, appropriateness, best practice options, levels and frequency of support
▪ Legislation and rules that underpin the MBS
▪ Division of responsibilities between Government – Federation White Paper
▪ Innovative funding models for chronic and complex disease – Primary Health Care Advisory Group
| 13
What will this review mean for patients and consumers?
More evidence-based care
More appropriate referrals and appointments
Better use of best-practice health care services
Prevention of unnecessary treatments and tests
Increased access to valuable, yet underutilised, treatments
1
2
3
4
5
| 14
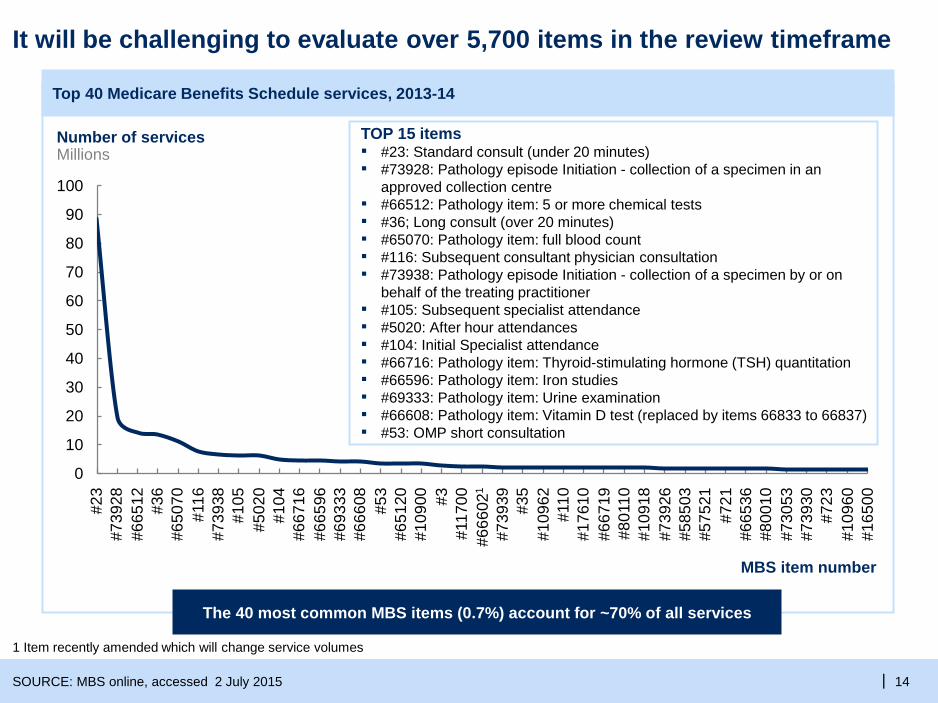
It will be challenging to evaluate over 5,700 items in the review timeframe
0
10
20
30
40
50
60
70
80
90
100
#585
03
#165
00
#721
#667
19
#739
30
#730
53
#665
36
#3
#651
20
#693
33
#667
16
#666
08
#739
39
#109
60
#800
10
MBS item number
#723
#575
21
#739
26
#109
18
#801
10
#176
10
#110
#35
#666
021
#109
62
#117
00
#109
00
Number of services Millions
#665
96
#739
28
#116
#6
5070
#665
12
#53
#739
38
#36
#23
#105
#5
020
#104
The 40 most common MBS items (0.7%) account for ~70% of all services
SOURCE: MBS online, accessed 2 July 2015
Top 40 Medicare Benefits Schedule services, 2013-14
1 Item recently amended which will change service volumes
TOP 15 items ▪ #23: Standard consult (under 20 minutes) ▪ #73928: Pathology episode Initiation - collection of a specimen in an
approved collection centre ▪ #66512: Pathology item: 5 or more chemical tests ▪ #36; Long consult (over 20 minutes) ▪ #65070: Pathology item: full blood count ▪ #116: Subsequent consultant physician consultation ▪ #73938: Pathology episode Initiation - collection of a specimen by or on
behalf of the treating practitioner ▪ #105: Subsequent specialist attendance ▪ #5020: After hour attendances ▪ #104: Initial Specialist attendance ▪ #66716: Pathology item: Thyroid-stimulating hormone (TSH) quantitation ▪ #66596: Pathology item: Iron studies ▪ #69333: Pathology item: Urine examination ▪ #66608: Pathology item: Vitamin D test (replaced by items 66833 to 66837) ▪ #53: OMP short consultation

| 15
Review methodology
▪ Clinician-led review and significant consultation with stakeholders o Clinicians o Consumers o Industry o Other health disciplines, including public health
▪ Clinical Committees o Discipline-specific clinical committees o Subordinate working groups for reviews of particular services o Membership is broad-based:
• Clinicians, requestors, generalists, academics with public health and health economics expertise, consumers
o Members are an expert in their own right and not a ‘representative’ of an organisation
| 16
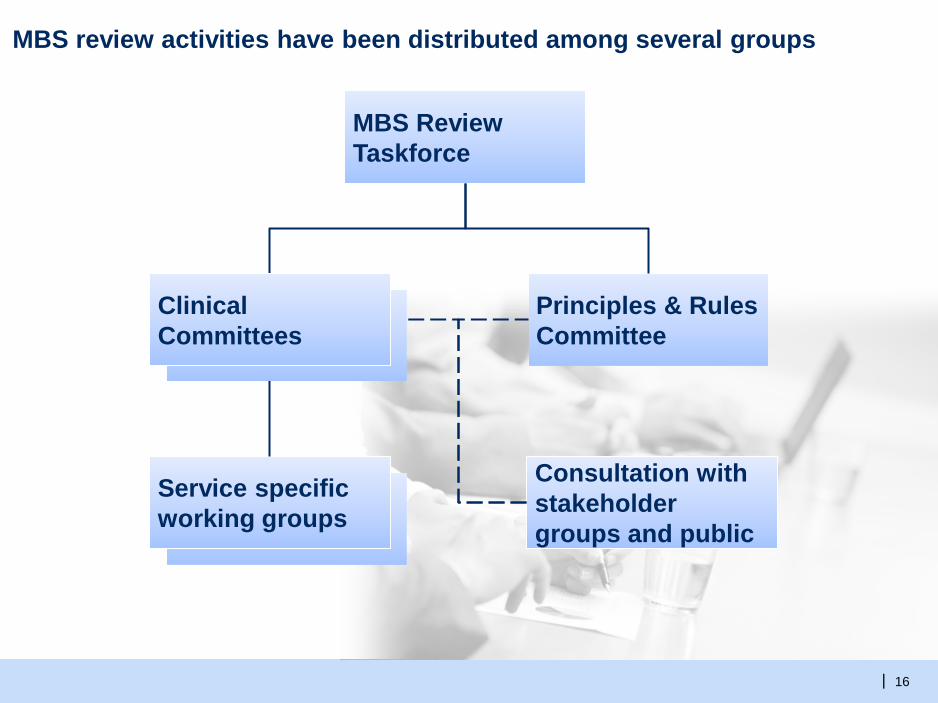
MBS review activities have been distributed among several groups
MBS Review Taskforce
Principles & Rules Committee
Service specific working groups
Consultation with stakeholder groups and public
Clinical Committees

| 17
The Clinical Committees are following a consistent five-step approach
Propose changes to items and articulate rationale
Taskforce finalises recommendations to Government
Conduct rapid evidence reviews and targeted analyses as needed for each item
Examine item descriptors and usage patterns to identify items requiring detailed investigation
Colleges, peak bodies and other affected stakeholders are notified of the recommended changes and invited to contribute feedback
Triage 1
Evaluation 2
Clinical Committee Recommendation
3
Taskforce Recommendation
5
Consultation 4

| 18
The Principles and Rules Committee examines issues which affect many or all Clinical Committees
Examples of issues raised by stakeholders
Description of the Principles and Rules Committee
▪ The Taskforce will recommend updates to the legislation which underpins the MBS
▪ The Committee contains a broad range of participants, including Taskforce members clinicians, and others
▪ Stakeholders are invited to actively contribute to the refinement of Rules
▪ Referral regulation: how can the current model be optimised for patients and providers
▪ MBS item descriptors: how can MBS items be more clearly defined and user-friendly?
▪ MBS principles: e.g., complete medical service, aftercare etc.

| 19
New services
▪ The focus is on existing items, but the Taskforce may recommend new items or services
▪ MSAC remains the primary gateway for health technology assessment and new MBS services o Where good clinical practice requires addition of a service, Minister might ask
MSAC for expedited advice o For a completely novel treatment or technology, Minister might choose a full MSAC
review of the evidence
▪ Existing item/s can be combined to form new item/s to better describe the service o Normally will not need MSAC review
▪ Rapid reviews undertaken by a clinical committee may reduce the time required by MSAC in adding new items o Onus is on clinical committee to commission rapid review and make
recommendation

| 20
Obsolete items – first tranche
▪ 23 MBS items were identified by Clinical Committees as obsolete. o Diagnostic Imaging: 58706, 58924, 59503, 59715, 59736, 59760, 61465 o Ear, Nose and Throat Surgery: 11321, 18246, 41680, 41695, 41758, 41761, 41846,
41849, 41852 o Gastroenterology:13500, 13503, 30493, 32078, 32081 o Obstetrics: 16504 o Thoracic Medicine: 11500
▪ Public consultation from 18 December 2015 to 8 February 2016
▪ Amendments to some recommendations after taking into account feedback
▪ Government consideration of Taskforce recommendation
| 21
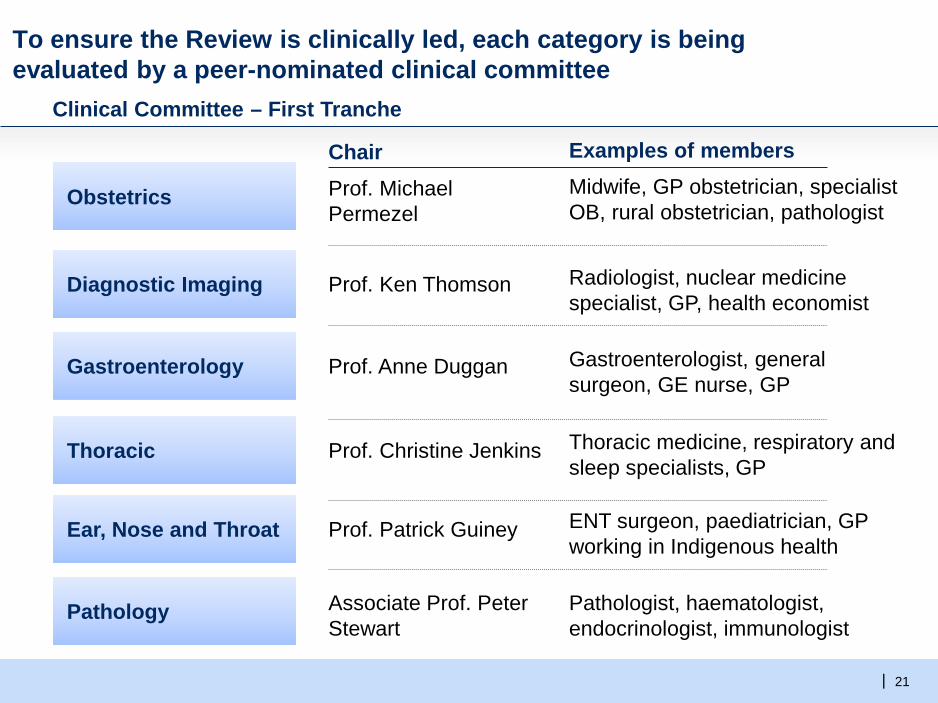
To ensure the Review is clinically led, each category is being evaluated by a peer-nominated clinical committee
Chair Examples of members
Obstetrics Prof. Michael Permezel
Midwife, GP obstetrician, specialist OB, rural obstetrician, pathologist
Prof. Ken Thomson Radiologist, nuclear medicine specialist, GP, health economist
Prof. Anne Duggan Gastroenterologist, general surgeon, GE nurse, GP
Prof. Christine Jenkins Thoracic medicine, respiratory and sleep specialists, GP
Prof. Patrick Guiney ENT surgeon, paediatrician, GP working in Indigenous health
Clinical Committee – First Tranche
Diagnostic Imaging
Thoracic
Ear, Nose and Throat
Pathology
Gastroenterology
Associate Prof. Peter Stewart
Pathologist, haematologist, endocrinologist, immunologist
| 22
Clinical Committees – Second tranche
▪ The second tranche of Clinical Committees is underway ▪ This tranche includes: o Cardiac Services
• Cardiology and cardiothoracic surgery
o Dermatology, Allergy & Immunology • Skin conditions and allergy testing (skin cancer surgery review completed)
o Endocrinology • Includes endocrine surgery
o Intensive Care and Emergency Medicine • Includes neonatology
o Oncology • Chemotherapy and radiation oncology (not cancer surgery)
o Renal Medicine • Includes dialysis

| 23
Public consultations
▪ The Taskforce is committed to engaging with all stakeholders and welcomes input into all aspects of the review o Consultation will occur regularly throughout 2016
▪ Public consultation will follow recommendations from Clinical Committees o Recommendations including obsolete items, rapid reviews, changes to existing
items, new services o Detailed information to provide context and rationale o Targeted consultation by directly contacting organisations with relevant interests o Broad consultation by publishing on website, media release, and newsletter
▪ Taskforce considers recommendations from Clinical Committee and feedback from public consultation, prior to making recommendations to Minister
| 24
The Clinical Committee program for 2016
▪ The third tranche of clinical committees will commence in the next few months ▪ Items specific to pain management will be considered in this review by a Pain
Management clinical committee – commencement will be later in the year ▪ As with all committees, this committee will have a broad based membership including
clinicians, requestors, generalists, academics with public health and health economics expertise, and health consumers
▪ The items specific to pain management include: – GP and specialist consultation – Specific pain management procedures (including nerve blocks) – Multidisciplinary care plans – Allied health services – Mental health services
The NHMRC Review
25
| 26
Scope and terms of reference
The Review will examine and provide advice to the CEO of NHMRC about: the structure of the grant programme, including: 1. The impact of the grant programme on the health and medical research sector;
2. The flexibility of the grant programme to meet future needs for health and medical research in Australia; and 3. Alternative models and their potential to overcome the current challenges. The Review will consider relevant overseas experience with medical research grant programmes. NHMRC will also consider feedback provided in response to its Fellowship Consultation. Chaired by Prof Steve Wesselingh, SAHMRI
| 27
Should we have a National Institute for Health Research?
• In the UK the NIHR undertakes research in health systems and health care delivery
• Funds provided by the health system (NHS Trusts)
• Competitive funding of projects which can be pilots but must be able to be ‘scaled up’
• Would free up significant research $ for clinical and basic research
• Could be linked to MBS with some clinical trials being part funded using temporary
item numbers.
Primary Health Care

|
• The Advisory Group delivered its final report, Better Outcomes for People with Chronic and Complex Health Conditions, to Government on 3 December 2015.
• The final report was released on 31 March 2016 and can be found on the Department of Health’s website at www.health.gov.au/healthiermedicare
• The PHCAG made 15 key recommendations designed to establish a Health Care Home model of care for patients with chronic and complex conditions.
• Government have accepted the findings of the PHCAG report and is
beginning staged implementation of the Health Care Home model.
PHCAG Final Report

|
• Eligible patients will voluntarily enrol with a participating medical practice known as their Health Care Home
• This practice will provide a patient with a ‘home base’ for ongoing coordination, management and support.
• Care coordination and team-based care
• Regional clinical ‘patient pathways’
• Patient participation
Health Care Home model
|
• Care coordination is critical to ensure that patients with high care needs can navigate the health care system
• Patients enrolled in the Health Care home may also be eligible to receive support services through other programs that can improve their ability to manage their care
• Approximately 59% of practices employ an additional staff member to coordinate their patients’ care
• These resources need to be effectively targeted to those patients who have the greatest need
Care Coordination

|
A New Payment Mechanism
• A new blended payment mechanism will provide flexibility in the delivery of care and incentivise delivery of high quality care. Health Care Homes will be paid a quarterly bundled
payment to provide care related to a patient’s chronic and complex condition.
Fee for service payments will be maintained for care not
relating to the enrolled patient’s chronic conditions. Existing MBS items for allied health services will remain in
place for patients enrolled in a Health Care Home.
• Pursue collaborative approaches to planning and allocation of health system resources, including joint and pooled funding with State and Territory governments and private health insurers.

|
• As a first step Health Care Homes will be rolled out in up to seven Primary Health Network regions across the country.
• Up to 200 Health Care Homes will offer services to up to 65,000 people with chronic and complex conditions.
• Health Care Home services will be delivered in these regions from 1 July 2017.
• Any national roll out of Health Care Homes will be informed by the results of a rigorous evaluation of the first stage of implementation and consideration by Government.
Evaluation of the Health Care Home model

| 34
[email protected] Email :
www http://www.health.gov.au/internet/main/publishing.nsf/Content/MBSReviewTaskforce Website :