presentation title here presentation subtitle here clinical... · 1/4/2018 1 ©2017 mfmer | slide-1...
TRANSCRIPT

1/4/2018
1
©2017 MFMER | slide-1
Recent Clinical Advances in Vestibular Assessment
Devin L. McCaslin, Ph.D. Director, Vestibular and Balance Program
Minnesota Academy of Audiology February 24th, 2018
©2017 MFMER | slide-2
Disclaimer
• Salary supplemented by NIH
• Consultant for the American Academy of Audiology
©2017 MFMER | slide-3
Mayo Clinic Locations

1/4/2018
2
©2017 MFMER | slide-4
Outline of Presentation
• Assessment of the Semicircular Canals
• crHIT
• Suppression Head Impulse Paradigm
• Assessment of the Otoliths using Bone Conducted Stimuli
• B-81
• Skull Tapper
©2017 MFMER | slide-5
Current Challenges
• The clinical assessment of the peripheral vestibular system often consists of comparing the level of function from similar end-organs.
• In order to correctly interpret tests of vestibular function, the clinician must thoroughly understand the anatomical and physiological underpinnings of the tests.
©2017 MFMER | slide-6
• Caloric Test
• Video Head Impulse Test
Assessment of the Semicircular Canals

1/4/2018
3
©2017 MFMER | slide-7
The Problem!
• Halmagyi and Curthoys (1988)
• Doll’s eye test
©2017 MFMER | slide-8
©2017 MFMER | slide-9
Normal HIT Abnormal HIT

1/4/2018
4
©2017 MFMER | slide-10
Video Head Impulse Testing – Fixed Target
• The Video Head Impulse Test (vHIT) may, in some cases, make it possible to identify individual or multiple semicircular canals that are impaired.
• Instrumentation is video goggles and a computer.
M. Strupp, M.D. goggle system –
“Eyeseecam”
©2017 MFMER | slide-11
Responses from the Semicircular Canal Afferents
Goldberg and Fernandez, 1971
©2017 MFMER | slide-12
Saccade Classification
Weber et al., Neurology, 2008

1/4/2018
5
©2017 MFMER | slide-13
Video Head Impulse Test
©2017 MFMER | slide-14
Outline of Presentation
• Assessment of the Semicircular Canals
• “Suppression” Head Impulse Paradigm (SHIMP)
• crHIT
• Use of vHIT in Meniere’s Disease
• Assessment of the Otoliths using Bone Conducted Stimuli
• B-81
• Skull Tapper
©2017 MFMER | slide-15
SHIMP
• MacDougall et al. introduced a new complementary addition to HIMP referred to as the suppression head impulse paradigm (SHIMP). Video recordings were performed of responses to 20 random manually applied head impulse movements of between 1508 and 2508/s; these were done with attention to the corrective or compensatory saccades that followed.

1/4/2018
6
©2017 MFMER | slide-16
©2017 MFMER | slide-17
SHIMP
©2017 MFMER | slide-18
SHIMP

1/4/2018
7
©2017 MFMER | slide-19
SHIMP
©2017 MFMER | slide-20
SHIMP
©2017 MFMER | slide-21
SHIMP
• The study found that the compensatory saccade pattern responses for both HIMP and SHIMP were highly effective in distinguishing patients with unilateral or bilateral vestibular loss from controls, with 90% and 100% sensitivity and 100% specificity.
• This study is important for 2 reasons:
• (1) this is further support for use of HIMPs as techniques of diagnostic accuracy for characterizing peripheral
• vestibular function, and (2) it represents a fairly quick alternative to caloric

1/4/2018
8
©2017 MFMER | slide-22
SHIMP
• testing that is well tolerated by patients. The limits of this study include spectrum
• bias since the vestibular disorders studied did not span the full breadth that might
• be encountered in clinical practice. In addition, the number of participants was
• fairly small. Still, this technique shows promise as an alternative way to assess horizontal
• canal vestibular function in one or both ears. It remains to be seen whether
©2017 MFMER | slide-23
• HIMP and SHIMP may at some point supplant the more time-consuming and
• sometimes uncomfortable caloric testing that has been the mainstay of vestibular
• testing for much of the past century.2
©2017 MFMER | slide-24
SHIMP
• vHIT testing using a head-fixed rather than space-fixed visual target— the SHIMP paradigm —gives clearer results in patients with many covert saccades and in those with only low-level residual SCC function.

1/4/2018
9
©2017 MFMER | slide-25
Outline of Presentation
• Assessment of the Semicircular Canals
• “Suppression” Head Impulse Paradigm (SHIMP)
• The Computerized Rotational Head Impulse Test (crHIT) - Vertical
• Use of vHIT in Meniere’s Disease
• Assessment of the Otoliths using Bone Conducted Stimuli
• B-81
• Skull Tapper
©2017 MFMER | slide-26
The Problem!
• Halmagyi and Curthoys (1988)
• Doll’s eye test
©2017 MFMER | slide-27
Horizontal Canal
From Barber and Stockwell, 1981

1/4/2018
10
©2017 MFMER | slide-28
Description
• Measures horizontal eye movements in response to caloric stimuli (insert caloric eye video)
• Quick phases are directed according to the temperature (COWS).
• Diagnostic criterion (symmetry)
• Can stimulate both canals individually
• Possible to evaluate all three canals
©2017 MFMER | slide-29
• Caloric test technique developed by Aoki et al. 2009
• Concept: to bring to earth vertical position the…
• hSCC (head midline and anteflexed 30 deg.),
• pSCC (head anteflexed 30 deg and turned 45 deg. toward the stimulated ear) and the,
• aSCC (head anteflexed 30 deg and turned 45 deg away from midline)
©2017 MFMER | slide-30
Aoki et al. (2009)
N = 100 ears
Vertical
Channel
Cool caloric
creates DB
caloric
nystagmus
for pSCC and
UB
nystagmus in
the aSCC
1/4/2018
11
©2017 MFMER | slide-31
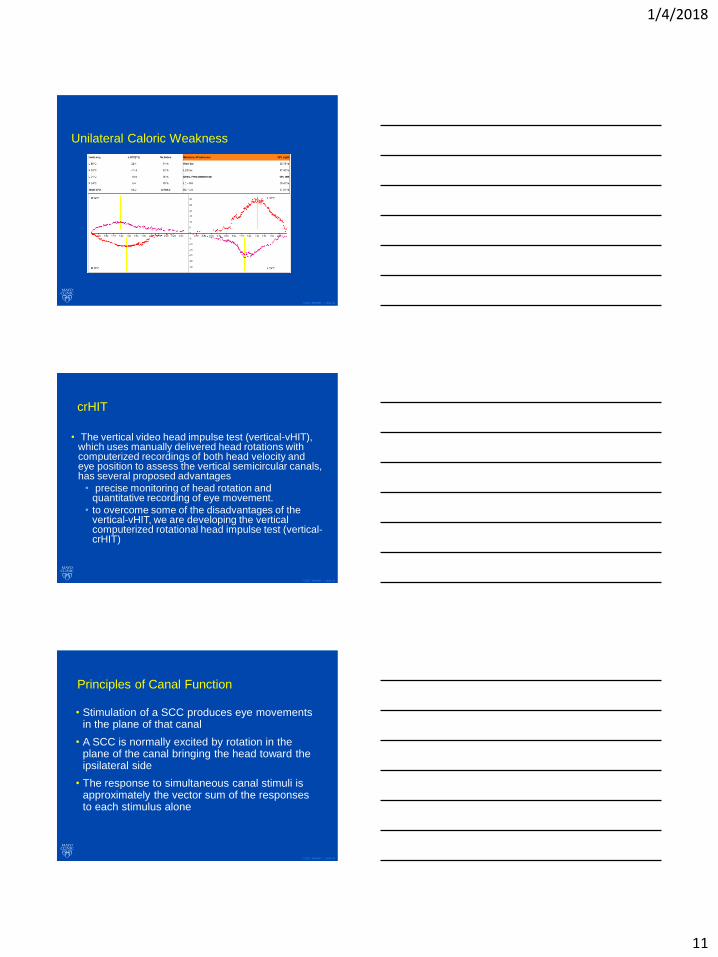
Unilateral Caloric Weakness
©2017 MFMER | slide-32
crHIT
• The vertical video head impulse test (vertical-vHIT), which uses manually delivered head rotations with computerized recordings of both head velocity and eye position to assess the vertical semicircular canals, has several proposed advantages
• precise monitoring of head rotation and quantitative recording of eye movement.
• to overcome some of the disadvantages of the vertical-vHIT, we are developing the vertical computerized rotational head impulse test (vertical-crHIT)
©2017 MFMER | slide-33
Principles of Canal Function
• Stimulation of a SCC produces eye movements in the plane of that canal
• A SCC is normally excited by rotation in the plane of the canal bringing the head toward the ipsilateral side
• The response to simultaneous canal stimuli is approximately the vector sum of the responses to each stimulus alone

1/4/2018
12
©2017 MFMER | slide-34
©2017 MFMER | slide-35
©2017 MFMER | slide-36

1/4/2018
13
©2017 MFMER | slide-37
©2017 MFMER | slide-38
Sensors and Eye Tracking
©2017 MFMER | slide-39
Head Positioning

1/4/2018
14
©2017 MFMER | slide-40
Head Positioning
©2017 MFMER | slide-41
Head Positioning
©2017 MFMER | slide-42
Phase I Procedures
• With the subject in one of the vertical canal planes, the subject was asked to look at a laser target in the primary position.
• The subject was then rotated sinusoidally about an earth-vertical axis at a frequency of 0.3 Hz with an amplitude of +/- 9 deg.

1/4/2018
15
©2017 MFMER | slide-43
Phase I Procedures
• The rotation about the head pitch axis and vertical eye position were used to calibrate the vertical component of the eye position recorded with the video goggles by assuming the visual-VOR gain was 1.0 for this low frequency rotation.
• While the subject looked at a small fixation target in the primary position in an otherwise darkened room, rotational impulses were delivered.
©2017 MFMER | slide-44
Rotational Trajectories
©2017 MFMER | slide-45
crHIT

1/4/2018
16
©2017 MFMER | slide-46
©2017 MFMER | slide-47
Results
• After preliminary testing and evaluation of design 1 vs design 2 options, the investigators came to the conclusion that option 2 is more acceptable secondary to the following factors:
• Patients feel more comfortable
• Head restraint during acceleration and deceleration is more robust;
• Head holder is more comfortable
©2017 MFMER | slide-48
Normal Response Data
150 deg/sec and a peak acceleration of about 750 deg/sec2. Gains for
responses were: RH=0.99; LH=0.98 ; RA =0.97; LA = 0.92; RP=0.96; LP =0.91.

1/4/2018
17
©2017 MFMER | slide-49
Left SVN Transection
RH=0.99; LH=0.60;
RA=0.89; LA=0.55;
RP=0.94; LP =0.92.
©2017 MFMER | slide-50
Report
©2017 MFMER | slide-51
Asymmetry
• crHIT: Average left VOR gain (GL), Average right VOR gain (GR), VOR weakness calculated as (GL-GR)/* (GL+GR)*100%,

1/4/2018
18
©2017 MFMER | slide-52
Conclusions
• As compared with the manual vertical-vHIT, the vertical-crHIT has the advantages of:
• Avoiding the small position limitations of a head-on-neck rotation
• Eliminating neck movement • Using a less abrupt movement and thus lowering
unpleasant jerk • Allowing random magnitude and direction of rotation
thus minimizing prediction • Controllable and repeatable motion stimulus • Eliminating the need for a highly trained examiner
The obvious disadvantage of the crHIT is the need for laboratory based equipment.
©2017 MFMER | slide-53
Outline of Presentation
• Assessment of the Semicircular Canals
• “Suppression” Head Impulse Paradigm (SHIMP)
• The Computerized Rotational Head Impulse Test (crHIT) - Vertical
• Use of vHIT in Meniere’s Disease
• Assessment of the Otoliths using Bone Conducted Stimuli
• B-81
• Skull Tapper
©2017 MFMER | slide-54
The Problem!
• Halmagyi and Curthoys (1988)
• Doll’s eye test

1/4/2018
19
©2017 MFMER | slide-55
Otolith Organs
©2017 MFMER | slide-56
Cervical VEMP
©2017 MFMER | slide-57
Nomenclature re: Cervical (scm) VEMP (aka cVEMP)
• 1st positive and negative waves are referred to as P13/N23 (or P1/N2).
• Positive waves represent inhibition of EMG
• Negative wave represents excitation of EMG

1/4/2018
20
©2017 MFMER | slide-58
Otolith Ocular Projections
• Electrical (to IVN), mechanical and acceleration stimuli result in eye movements.
• Excitatory activity in contralateral:
• inferior oblique, and
• and inferior rectus muscles
• Excitatory activity in ipsilateral:
• superior oblique
• and superior rectus muscles
• Activation of otolithic receptors should produce similar eye movements in humans
©2017 MFMER | slide-59
Ocular VEMP
Utricular afferents have a strong projection
to eye muscles.50,51
©2017 MFMER | slide-60
oVEMP Normal Response
• In response to 500 Hz tone burst
• N1: ~10 msec
• P1: ~15 msec
• Contralateral response occurs slightly earlier and is larger than ipsilateral response (contralateral pathway is faster)
Stim L, Rec R infraorbital
Stim L, Rec L infraorbital
N1
P1

1/4/2018
21
©2017 MFMER | slide-61
VEMPs and Bone Conduction Stimuli
• Bone conducted vibration applied to the head causes the skull to move by small amounts
• The pattern of displacement depends on (among other things:
• the location of the stimulator,
• stimulus frequency
• BCV results in rapid changes in linear acceleration at the mastoids that stimulates…
• Otolith irregular neurons that respond at intensity levels below ABR threshold
©2017 MFMER | slide-62
VEMPs and Air Conducted Stimuli
• Responses to air conducted stimuli are not as clear.
• Currently “believed” that a ‘shock wave’ initiated at the stapes footplate results in vestibular hair-cell receptors to be deflected.
• The mechanism is not understood
©2017 MFMER | slide-63
Mechanism by Which BCV and ACS Activate Otolith Receptors
• Bone Conducted Vibration
• Irregular otolith afferents originate from the central striolar region of the macula where chalice shaped nerve primary neurons connect to Type 1 receptors
• Irregular neurons are activated by changes in linear acceleration (jerk) and BCV is a preferred stimulus (repeated jerks)

1/4/2018
22
©2017 MFMER | slide-64
Case:
• Halmagyi and Curthoys (1988)
• Doll’s eye test
©2017 MFMER | slide-65
©2017 MFMER | slide-66
Results

1/4/2018
23
©2017 MFMER | slide-67
Outline of Presentation
• Assessment of the Semicircular Canals
• “Suppression” Head Impulse Paradigm (SHIMP)
• The Computerized Rotational Head Impulse Test (crHIT) - Vertical
• Use of vHIT in Meniere’s Disease
• Assessment of the Otoliths using Bone Conducted Stimuli
• B-81
• Skull Tapper
©2017 MFMER | slide-68
Mechanical skull tap device
• Intelligent Hearing Systems
• Universal Smart Box (USB)
• VEMP research software module enabled
• Additional hardware to route electrical current
• “Tapper” box with headband
©2017 MFMER | slide-69
Device coupling
• Adjustable soft band for coupling
• Force delivered may vary for different head circumferences due to band tightness
• Similar concerns with bone conduction ABR
• Utilized a dial spring scale to determine pressure was similar across subjects (Yang et al 1991)
• Target was 425-475grams

1/4/2018
24
©2017 MFMER | slide-70
Device output
• Verified output with Bruel & Kjaer artificial mastoid and sound level meter
• Maximum output of dial at 95 = 13-14N of force*
• Secondary verification with ATI Industrial Automation Gamma Force/Torque Sensor
• Band tension at 450g = 5N of force applied
• Maximum output of dial at 95 = 16N of force
©2017 MFMER | slide-71
Data collection
Conditions
1) Tapper on forehead
2) Tapper above right pinna
3) Tapper above inion
4) Tapper above left pinna
5) Right air conduction
6) Left air conduction
• oVEMP: 2 channel, eyes elevated ≥ 30°
• 2 visits 4-6 weeks apart
• 2 trials of 6 conditions
• n = 8
1 2
3 4
©2017 MFMER | slide-72
Test-Retest oVEMP
Condition
N10
latency
P15 latency N10-P15
Amplitude
1 Fair (.547)* Fair (.574)* Poor (.361)
2 Fair
(.548)*
Fair (.550)* Poor (.359)
3 Fair (.431)* Poor (.250) Excellent (.816)*
4 Fair (.573)* Fair (.550)* Fair (.680)*
• Excellent reliability found for amplitude with the tapper above the inion
• Reliability best for peak to peak amplitude, similar to Nguyen et al 2010 (n = 12)

1/4/2018
25
©2017 MFMER | slide-73
Next steps:
• Expand sample size of oVEMPs for normal group
• Determine optimal site for stimulus
• Expand sample size of cVEMPs for normal group
• Controlling for EMG activity
• Asymmetry characteristics
• Determine optimal site for stimulus
• Create additional groups
• Conductive hearing loss
• Otolith impairment UW/BW
• Multiple age groups
©2017 MFMER | slide-74
Summary
• Type your first bulleted point here type your first bulleted point here your first bulleted point here
• Type your second bulleted point here
• First subpoint first subpoint first subpoint first subpoint first subpoint first subpoint
• Second subpoint
• Type your third bulleted point here
• Etc, etc, etc…
• Etc, etc, etc…
©2017 MFMER | slide-75
Questions & Discussion