presentation - university of montana · type 2 diabetes and obesity: evolving treatment stragies...
TRANSCRIPT
3/27/2013
1
Type 2 Diabetes and Obesity:Evolving Treatment Stragies
Christopher Sorli, MD/PhD, FACEChair, Department of Diabetes, Endocrinology and Metabolism
Billings ClinicBillings, MT
Pathogenesis of Type 2 Diabetes
HGP=hepatic glucose production.
Islet -cell
ImpairedInsulin Secretion
IncreasedHGP
Decreased GlucoseUptake
Metformin
SUsInsulin
Insulin
NHANES1988-1994
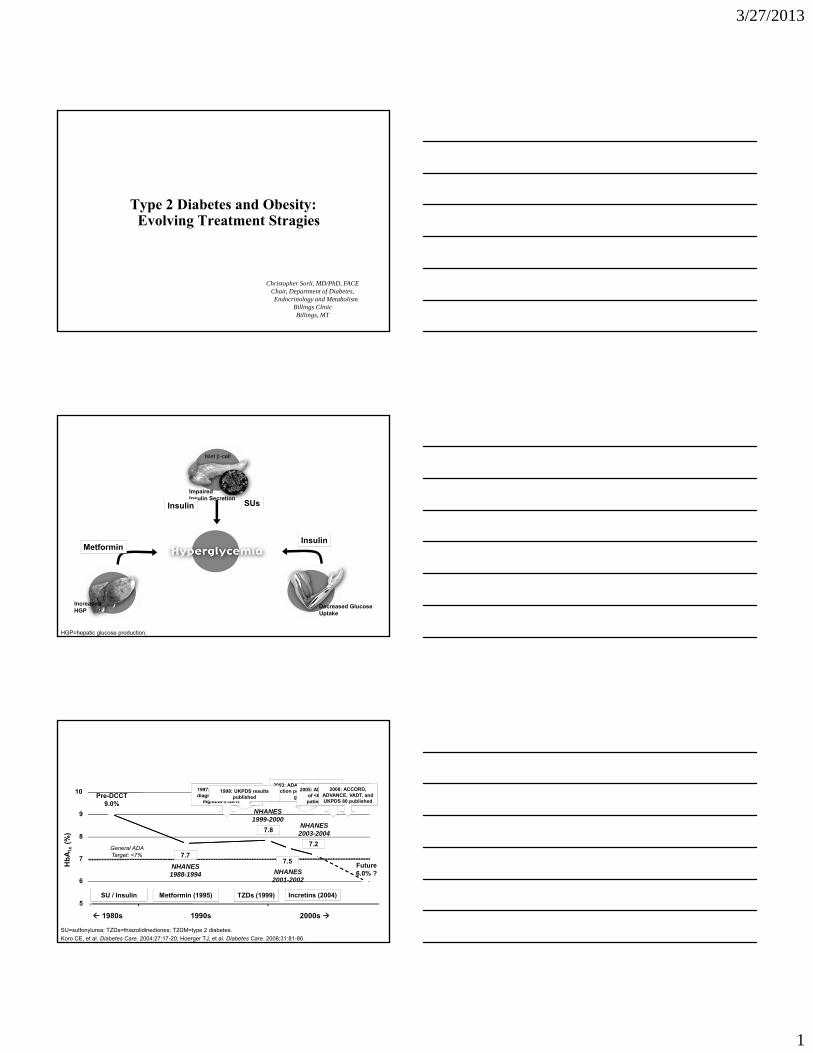
Advances in Therapy, but Falling Short of Goals
5
6
7
8
9
10
1980s 1990s 2000s
Hb
A1c
(%)
SU / Insulin Metformin (1995) TZDs (1999) Incretins (2004)
Pre-DCCT9.0%
7.7
NHANES1999-2000
7.8
NHANES2001-2002
7.5
NHANES2003-2004
7.2
Future6.0% ?
1997: ADA lowered T2DM diagnosis from FPG ≥140
mg/dLto ≥126 mg/dL
2003: ADA eliminated HbA1c
“action point” of <8% from guidelines
SU=sulfonylurea; TZDs=thiazolidinediones; T2DM=type 2 diabetes.
Koro CE, et al. Diabetes Care. 2004;27:17-20; Hoerger TJ, et al. Diabetes Care. 2008;31:81-86.
2005: ADA added HbA1c goal of <6% for “individual patients” to guidelines
General ADA Target: <7%
1998: UKPDS results published
2008: ACCORD, ADVANCE, VADT, and UKPDS 80 published

3/27/2013
2
Type 2 Diabetes Evolving Treatment Strategies
Mortality
intensive
standard
HR = 1.22(95% CI =1.01-1.46)
p = 0.04
NHANES1988-1994
Advances in Therapy, but Falling Short of Goals
5
6
7
8
9
10
1980s 1990s 2000s
Hb
A1c
(%)
SU / Insulin Metformin (1995) TZDs (1999) Incretins (2004)
Pre-DCCT9.0%
7.7
NHANES1999-2000
7.8
NHANES2001-2002
7.5
NHANES2003-2004
7.2
Future6.0% ?
SU=sulfonylurea; TZDs=thiazolidinediones; T2DM=type 2 diabetes.
Koro CE, et al. Diabetes Care. 2004;27:17-20; Hoerger TJ, et al. Diabetes Care. 2008;31:81-86.
General ADA Target: <7%
2009: ADA added “less stringent” HbA1c goal for patients with significant comorbidities or risk of hypoglycemia, or short
life expectancy
3/27/2013
3
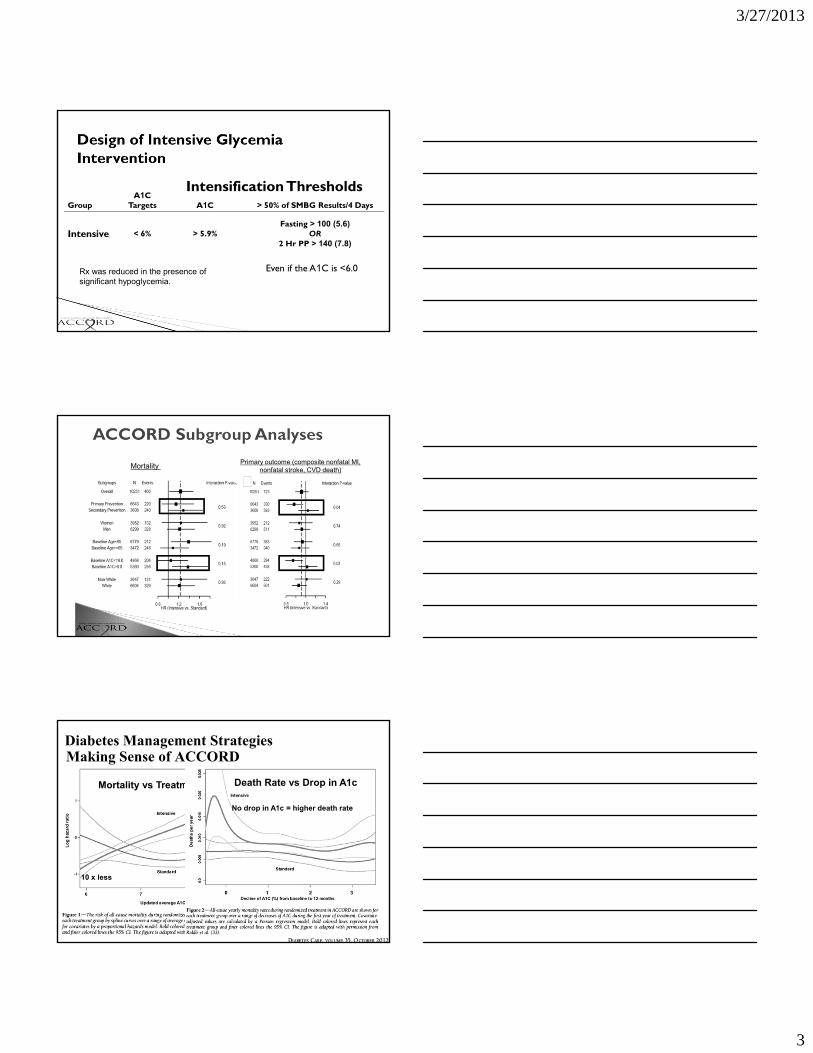
GroupA1C
Targets
Intensification ThresholdsA1C > 50% of SMBG Results/4 Days
Intensive < 6% > 5.9%Fasting > 100 (5.6)
OR2 Hr PP > 140 (7.8)
Even if the A1C is <6.0Rx was reduced in the presence of significant hypoglycemia.
Mortality Primary outcome (composite nonfatal MI,
nonfatal stroke, CVD death)
Diabetes Management StrategiesMaking Sense of ACCORD
Mortality vs Treatment A1c
10 x less
10 x more
Death Rate vs Drop in A1c
No drop in A1c = higher death rate

3/27/2013
4
Pathogenesis of Type 2 Diabetes
HGP=hepatic glucose production.
Islet -cell
ImpairedInsulin Secretion
IncreasedHGP
Decreased GlucoseUptake
The Ominous Octet
Islet -cell
ImpairedInsulin Secretion
NeurotransmitterDysfunction
Decreased GlucoseUptake
Islet -cell
IncreasedGlucagon Secretion
IncreasedLipolysis
Increased GlucoseReabsorption
IncreasedHGP
DecreasedIncretin Effect
Metabolic syndrome Hyperglycemia
Failing -cellFunctional -cell
Heine RJ, Spijkerman AM. 2006.
Insulin resistance Insulin resistance
Type 2 Diabetes: A HeterogeneousDisorder
CVD
Cancer
Retinopathy
Neuropathy
Nephropathy
70-80% of
population
20-30% of
population

3/27/2013
5
DIABETES/OBESITYManagement Strategies
Insulin ResistanceMetabolic Syndrome
Energy Storage
Insulin SupplyBeta Cell Dysfunction
Hyperglycemia
Insulin Resistance
β cell function
Years of Diabetes/Metabolic Syndrome
RelativeFunction 100 (%)
-20 -10 0 10 20 30
β cell mass
Adapted from IDC, Minneapolis, MN
Macrovascular Risk/ Cancer Risk
Prevention!Intensive managment of
Insulin resistanceβ cell dysfunction
CVD risks
Damage Control!Less intensive glycemic goals
Avoid hypoglycemia
History of Diabetes Therapy:What More Could We Possibly Want?
Animal Insulin
1922 1950’s 1982-85 1995 1996 2001 2003 2005 2007 2009
Sulfonylurea
Human Insulin
Metformin
Lispro
Glitazones
Glinides
Aspart
Exenatide
Pramlintide
Detemir
Sitagliptin
Bromocriptine
Saxagliptin
2013
Liraglutide
SGLT-2 inhib
11-β-HSD1 inhib
The End of Protocol Driven Therapy
Weekly Exenatide
DegludecGlucagon R antangonists
Management of Hyperglycemia in Type 2Diabetes: A Patient-Centered ApproachPosition Statement of the American Diabetes Association (ADA) and
the European Association for the Study of Diabetes (EASD)

3/27/2013
6
ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
3. ANTI‐HYPERGLYCEMIC THERAPY
• Glycemic targets
- HbA1c < 7.0% (mean PG 150‐160 mg/dl [8.3‐8.9 mmol/l])
- Pre‐prandial PG <130 mg/dl (7.2 mmol/l)
- Post‐prandial PG <180 mg/dl (10.0 mmol/l)
- Individualization is key:
Tighter targets (6.0 ‐ 6.5%) ‐ younger, healthier
Looser targets (7.5 ‐ 8.0%+) ‐ older, comorbidities, hypoglycemia prone, etc.
- Avoidance of hypoglycemia
PG = plasma glucose Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
Figure 1 Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print](Adapted with permission from: Ismail-Beigi F, et al. Ann Intern Med 2011;154:554)
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

3/27/2013
7
ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
• Weight
- Majority of T2DM patients overweight / obese
- Intensive lifestyle program
- Metformin
- GLP‐1 receptor agonists
- ? Bariatric surgery
- Consider LADA in lean patients
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
Adapted Recommendations: When Goal is to Avoid Weight GainDiabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
Stomach
Islet
GI Tract
Brain
HypothalmusHind Brain
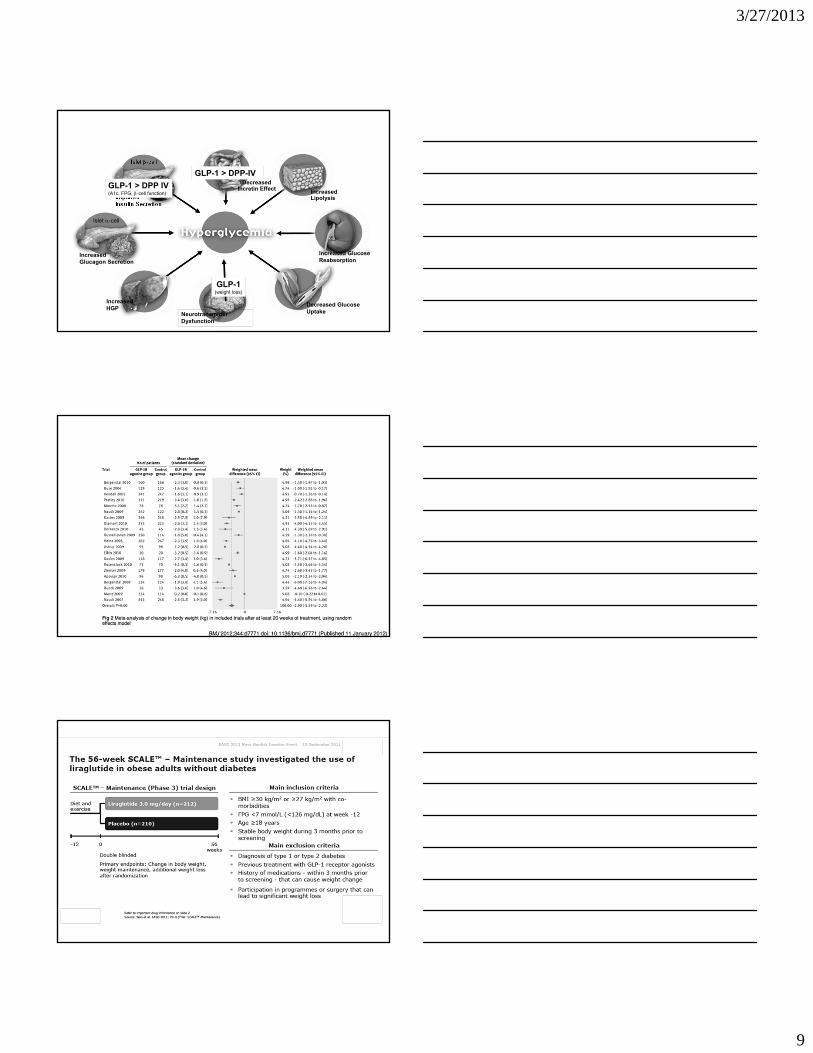
Peptide Therapeutics:Incretins (GLP-1 and GIP)
Visceral Fat Cell
Vagal Afferents
Leptin
Amylin
InsulinGLP-1
GlicentinOxyntomodulin
Ghrelin
GIP
Adiponectin
Visfatin
Resistin
Glucagon
CCK
Adapted from Badman MK and Flier JS; Science 2006: 307, 1909-1914
PYY3-36
Incretins (injectables)
Exenatide – Bydureon, ByettaLiraglutide - Victoza
DPP-IV Inhibitors(orals)
Sitagliptin – JanuviaLinagliptin – TradjentaSaxagliptin - Onglyza

3/27/2013
8
Incretins:GLP-1 Agonists vs. DPP-IV Inhibitors
Pharmacology vs PhysiologyDPP-IV – increases endogenous
GLP-1GLP-1 agonist – super physiologic
effect
…Not quite that simple
Differential Effects:Glycemic ControlEnergy Balance
T2DM – Treatment Strategies
Islet -cell
ImpairedInsulin Secretion
NeurotransmitterDysfunction
Decreased GlucoseUptake
Islet -cell
IncreasedGlucagon Secretion
IncreasedLipolysis
Increased GlucoseReabsorption
IncreasedHGP
DecreasedIncretin EffectGLP-1 > DPP IV
(A1c, FPG, -cell function)
GLP-1 > DPP-IV
Incretins (Exenatide):Sustained Efficacy- Improved Beta Cell Function
Buse et.al., Oct 2012, EASD, Berlin
3/27/2013
9
T2DM – Treatment Strategies
Islet -cell
ImpairedInsulin Secretion
NeurotransmitterDysfunction
Decreased GlucoseUptake
Islet -cell
IncreasedGlucagon Secretion
IncreasedLipolysis
Increased GlucoseReabsorption
IncreasedHGP
DecreasedIncretin EffectGLP-1 > DPP IV
(A1c, FPG, -cell function)
GLP-1(weight loss)
GLP-1 > DPP-IV
Incretin TherapyEffect on Energy Homeostasis

3/27/2013
10
T2DM– Treatment Strategies
Islet -cell
ImpairedInsulin Secretion
NeurotransmitterDysfunction
Decreased GlucoseUptake
Islet -cell
IncreasedGlucagon Secretion
IncreasedLipolysis
Increased GlucoseReabsorption
IncreasedHGP
DecreasedIncretin EffectGLP-1 > DPP IV
(A1c, FPG, -cell function)
GLP-1(weight loss)
GLP-1 > DPP-IV
GLP-1 > DPP IV(glucagon inhibition, FPG,
Prandial control)
GLP-1 > DPP IV(Glucagon inhibition, FPG,
Prandial control)
Incretins:Expanding Role in Treatment Strategies
Pediatric Type 1 Diabetics (n=8)
Insulin dose reduced 20%with exenatide dosing – mixed meal
3/27/2013
11
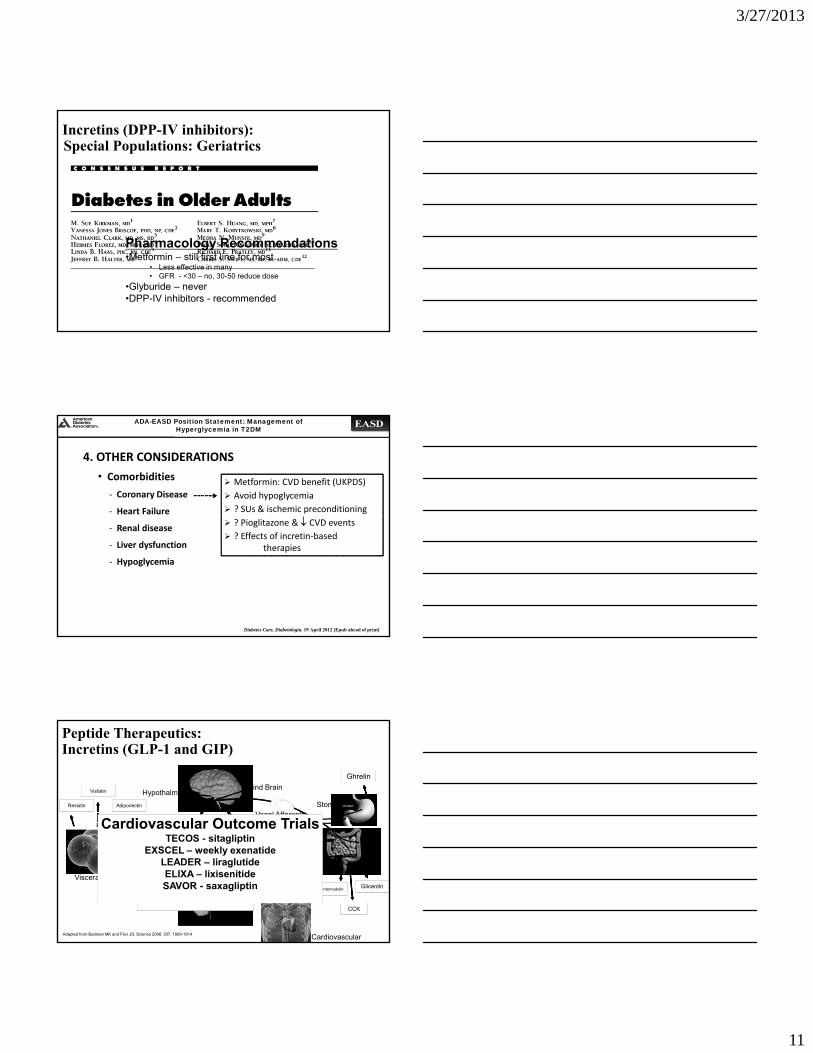
Incretins (DPP-IV inhibitors):Special Populations: Geriatrics
Pharmacology Recommendations•Metformin – still first line for most
• Less effective in many• GFR - <30 – no, 30-50 reduce dose
•Glyburide – never•DPP-IV inhibitors - recommended
ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
• Comorbidities
‐ Coronary Disease
‐ Heart Failure
‐ Renal disease
‐ Liver dysfunction
‐ Hypoglycemia
Metformin: CVD benefit (UKPDS)
Avoid hypoglycemia
? SUs & ischemic preconditioning
? Pioglitazone & CVD events
? Effects of incretin‐based therapies
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
Stomach
Islet
GI Tract
Brain
HypothalmusHind Brain
Peptide Therapeutics:Incretins (GLP-1 and GIP)
Visceral Fat Cell
Vagal Afferents
Leptin
Amylin
InsulinGLP-1
GlicentinOxyntomodulin
Ghrelin
GIP
Adiponectin
Visfatin
Resistin
Glucagon
CCK
Adapted from Badman MK and Flier JS; Science 2006: 307, 1909-1914
PYY3-36
Cardiovascular
IncretinsExenatide – Bydureon, Byetta
Liraglutide - Victoza
DPP-IV InhibitorsSitagliptin – Januvia
Linagliptin – TradjentaSaxagliptin - Onglyza
Cardiovascular Outcome TrialsTECOS - sitagliptin
EXSCEL – weekly exenatideLEADER – liraglutideELIXA – lixisenitideSAVOR - saxagliptin

3/27/2013
12
ACCORD:Mortality Hazard Ratios for Post-Randomization Prescription of Glycemia Medications
Adjusted for Baseline Participant CharacteristicsACCORD Study Group. Presented at the ADA Scientific Sessions, San Francisco, June 2008
RR
Peptide Therapeutics:Incretins (GLP-1 and GIP)
Exenatide vs. Non-Exenatide – Cardiovascular Events
ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
• Comorbidities
‐ Coronary Disease
‐ Heart Failure
‐ Renal disease
‐ Liver dysfunction
‐ Hypoglycemia
Metformin: CVD benefit (UKPDS)
Avoid hypoglycemia
? SUs & ischemic preconditioning
? Pioglitazone & CVD events
? Effects of incretin‐based therapies
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
Glyburide (and older) – Should never be usedGlimepiride or Glipizide if any SU

3/27/2013
13
ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
• Comorbidities
‐ Coronary Disease
‐ Heart Failure
‐ Renal disease
‐ Liver dysfunction
‐ Hypoglycemia Emerging concerns regarding
association with increasedmortality
Proper drug selection in the hypoglycemia prone
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
Adapted Recommendations: When Goal is to Avoid HypoglycemiaDiabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
T2DM– Treatment Strategies
Islet -cell
ImpairedInsulin Secretion
NeurotransmitterDysfunction
Decreased GlucoseUptake
Islet -cell
IncreasedGlucagon Secretion
IncreasedLipolysis
Increased GlucoseReabsorption
IncreasedHGP
DecreasedIncretin Effect
TZDs
TZDs
TZDs
TZDsTZDs
TZDs

3/27/2013
14
Slide Source:Lipids Online Slide Librarywww.lipidsonline.org
Time to Fatal/Nonfatal MI(Excluding Silent MI)
Kapl
an-M
eier
Eve
nt R
ate
Prespecified Analysis
0 6 12 18 24 30 36
Time from Randomization (Months)
Time to Acute Coronary Syndrome
Kapl
an-M
eier
Eve
nt R
ate
Post Hoc Exploratory Analysis
0 6 12 18 24 30 36
Time from Randomization (Months)
–28% –37%
Reprinted with permission from Erdmann E et al. J Am Coll Cardiol. 2007;49:1772-1780.Copyright © 2007 American College of Cardiology Foundation. All rights reserved.
Pioglitazone (65/1230)Placebo (88/1215)
Pioglitazone (35/1230)Placebo (54/1215)
PROactive: Pioglitazone Reduced “Hard”Coronary Heart Disease Endpoints
Pioglitazone vs Placebo:HR 0.72 (95% CI 0.52–0.99);
p=0.045
Pioglitazone vs Placebo:HR 0.63 (95% CI 0.41–0.97);
p=0.035
Type 2 Diabetes: Benefits vs Risks of TZDs
Type 2 Diabetes: Benefits vs Risks of TZDs
But????Actos causes Bladder Cancer!!!...Right?
3/27/2013
15
T2DM Anti‐hyperglycemic Therapy: General RecommendationsDiabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
The Ominous Octet – Treatment Strategies
Islet -cell
ImpairedInsulin Secretion
NeurotransmitterDysfunction
Decreased GlucoseUptake
Islet -cell
IncreasedGlucagon Secretion
IncreasedLipolysis
Increased GlucoseReabsorption
IncreasedHGP
DecreasedIncretin Effect
Insulin
Insulin
Insulin
InsulinInsulin
Insulin
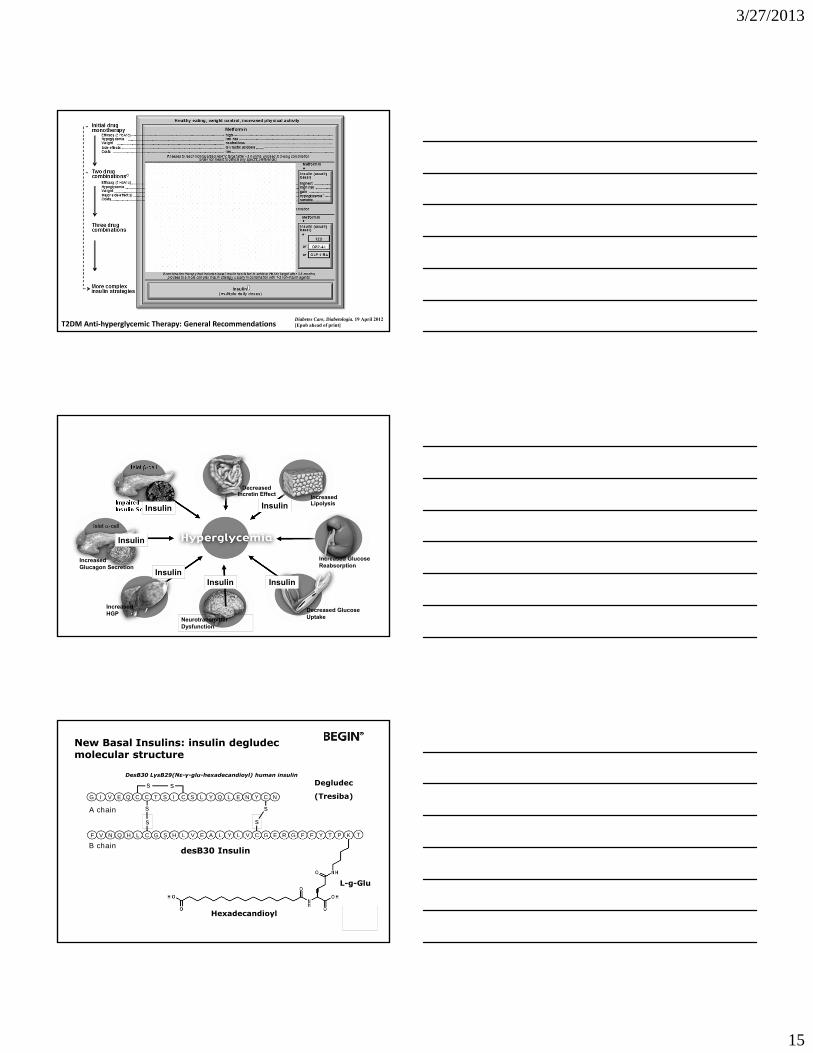
New Basal Insulins: insulin degludec molecular structure
DesB30 LysB29(Nε-γ-glu-hexadecandioyl) human insulinDegludec
(Tresiba)
s
s
s
F V N Q H L C G S H L V E A L Y L V C G E R G F F Y T P
G I V E Q C T S I C S L Y Q L E N Y C NC
s
s s
A chain
B chainK
Hexadecandioyl
L-g-Glu
desB30 Insulin
T

3/27/2013
16
Multi-hexamer formation after injection
Insulin degludec in pen
Long multi-hexamer chains assemble
[ Phenol; Zn2+]
Injection site
Jonassen I et al. Diabetes. 2010;59(suppl 1):A11
Insulin degludec multi-hexamers
Main picture shows elongated IDeg structures in absence of phenol; inset (white box) shows absence of elongated IDeg structures in presence of phenol.
Kurtzhals P et al. ADA 2011;32-LB (MoP + NN1250-1993)Kurtzhals P. EASD 2011; 092-P #1049 (MoP + NN1250-1993)
Following injection
[Zn2+ ]
Insulin degludec multi-hexamers
Subcutaneous depot
Monomers are absorbed from the depot into the circulation
- zinc
As zinc slowly diffuses out of the multi-hexamers, insulin degludec
monomers are formed
Jonassen I et al. Diabetes. 2010;59(suppl 1):A11

3/27/2013
17
Clamp profile in type 2 diabetes: ultra-long, flat and consistent
Glu
cose
infu
sion
rat
e (m
g/(k
g*m
in))
5
4
3
2
1
0
Treatment
IDeg 100 U/mL 0.4 U/kg
IDeg 100 U/mL 0.8 U/kgIDeg 100 U/mL 0.6 U/kg
Nosek L et al. ADA 2011;49-LB (NN1250-1987)Nosek L. EASD 2011; 093-P #1055 (NN1250-1987)
Consistently lower within-subject variability over time for insulin degludec
Heise et al. Diabetes 2011;60(Suppl. 1):A263c
IDeg
Consistently lower within-subject variability over time for insulin degludec
IDegIGlar
Heise et al. Diabetes 2011;60(Suppl. 1):A263c

3/27/2013
18
IDeg OD+ metformin ±DPP-4 (n=773)
IGlar OD + metformin ±DPP-4 (n=257)
Insulin-naïve patients with type
2 diabetes(n=1030)
0 52 weeksInclusion criteria• Type 2 diabetes ≥6 months• Insulin naïve treated with
metformin ± SU, DPP-4 or acarbose for ≥3 months
• HbA1C 7.0–10.0%• BMI ≤40 kg/m2
• Age ≥18 years
Study designONCE LONG (3579)
Randomized 3:1 (IDeg OD:IGlar OD)Open label
NN1250-3579; IDeg OD vs IGlar OD in T2DM.
DPP-4: dipeptidyl peptidase-4 inhibitorSU: sulphonylureaOD: once-daily
Nocturnal confirmed hypoglycemiaONCE LONG (3579)
36% lower ratewith IDeg OD
p<0.05
NN1250-3579; IDeg OD vs IGlar OD in T2DM.
IDeg OD (n=766)IGlar OD (n=257)
SAS Comparisons: Estimates adjusted for multiple covariates
JM2
Reduction in confirmed hypoglycemia with
degludec (all IDeg vs. IGlar studies,
maintenance period)
*statistically significant improvement
Overall
NocturnalT1 and T2 32%*
T2 basal only 49%*
16%*T1 and T228%*T2 basal only
http://www.novonordisk.com/images/investors/investor_presentations/2011/CMD2011/04_Diabetes_treatment_tomorrow_CMD2011.pdf’
Maintenance period
Pre-specified hypoglycemia meta-analyses Type 1 & type 2 diabetes

Slide 53
JM2 Graph is picture. SDM will source slide with graph as graph.Jackson, Meryn, 2/23/2012
3/27/2013
19
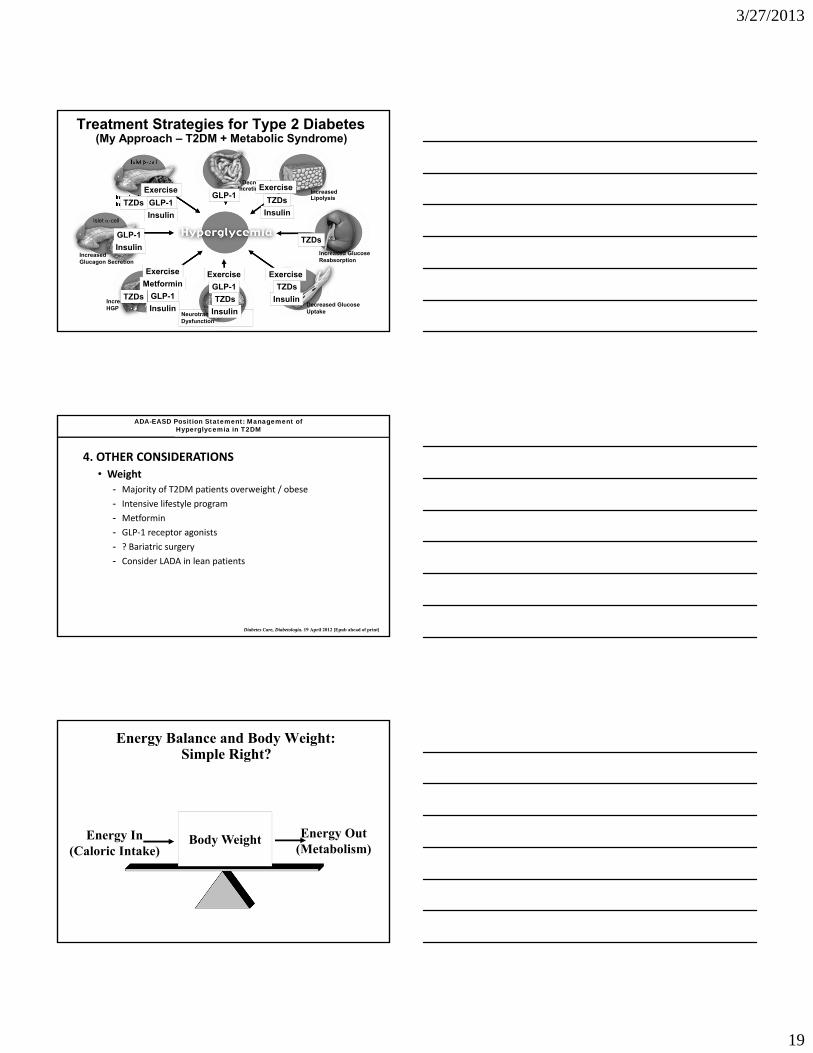
Treatment Strategies for Type 2 Diabetes (My Approach – T2DM + Metabolic Syndrome)
Islet -cell
ImpairedInsulin Secretion
NeurotransmitterDysfunction
Decreased GlucoseUptake
Islet -cell
IncreasedGlucagon Secretion
IncreasedLipolysis
Increased GlucoseReabsorption
IncreasedHGP
DecreasedIncretin Effect
GLP-1
GLP-1
GLP-1
GLP-1
GLP-1
Insulin
Insulin
Insulin
Insulin
Insulin
Insulin
Metformin
Exercise
Exercise
Exercise
Exercise Exercise
TZDs
TZDs
TZDs
TZDs TZDs
TZDs
ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS
• Weight
- Majority of T2DM patients overweight / obese
- Intensive lifestyle program
- Metformin
- GLP‐1 receptor agonists
- ? Bariatric surgery
- Consider LADA in lean patients
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
Energy Balance and Body Weight:Simple Right?
Body WeightEnergy In(Caloric Intake)
Energy Out(Metabolism)
3/27/2013
20
Stomach
Islet
GI Tract
Brain
HypothalmusHind Brain
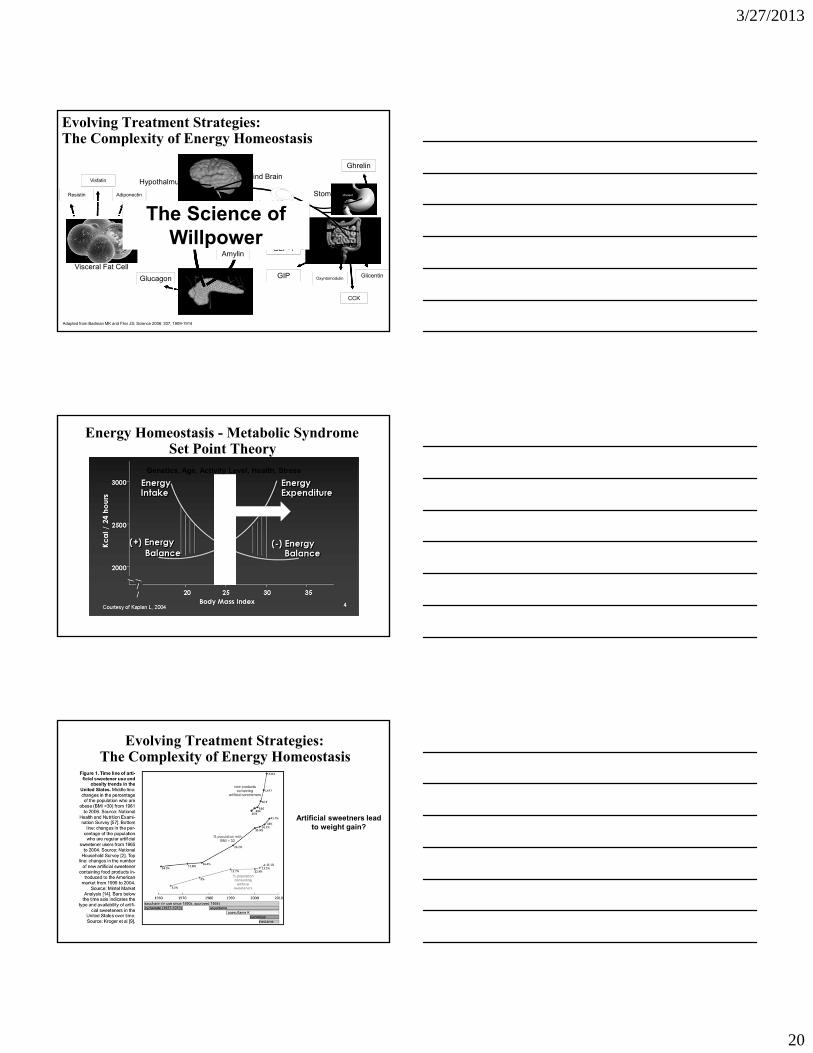
Evolving Treatment Strategies:The Complexity of Energy Homeostasis
Visceral Fat Cell
Vagal Afferents
Leptin
Amylin
InsulinGLP-1
GlicentinOxyntomodulin
Ghrelin
GIP
Adiponectin
Visfatin
Resistin
Glucagon
CCK
Adapted from Badman MK and Flier JS; Science 2006: 307, 1909-1914
PYY3-36
The Science ofWillpower
Energy Homeostasis - Metabolic Syndrome Set Point Theory
Genetics, Age, Activity Level, Health, Stress
Evolving Treatment Strategies:The Complexity of Energy Homeostasis
Artificial sweetners lead to weight gain?

3/27/2013
21
Energy Balance and Body Weight:What is Metabolism?
Body WeightEnergy In(Caloric Intake)
Energy Out(Metabolism)
Energy Homeostasis:The Quick Fix?
The Diet StrategyFailure Rate of Diet Alone 90-98%
Weight
Baseline
Counter-Regulation
New Set Point
↓ 5-10%

3/27/2013
22
Weight ManagementCounter-Regulation and the Failure of the “Diet” – HCG Diet
Weight LossCounter-Regulation and the Failure of the “Diet” –
Ideal Protein
295
Ideal Protein Diet↓ 28%
211
308
Fatigue, Depression, Fibromyalgia,Sleep Disorder,
“Must be something hormonal”
Energy Balance and Body Weight:What is Metabolism?
Body WeightEnergy In(Caloric Intake)
Energy Out(Metabolism)

3/27/2013
23
Low MetabolismHow Do I Fix It? – “Get Your Ducks in a Row”
• Sleep Problems – Sleep Apnea
• Vitamin D Deficiency
• Thyroid
• Vitamin B12
• Low Testosterone (male)
• Medications (centrally acting)
Energy Homeostasis:The Miracle Pill?
3/27/2013
24
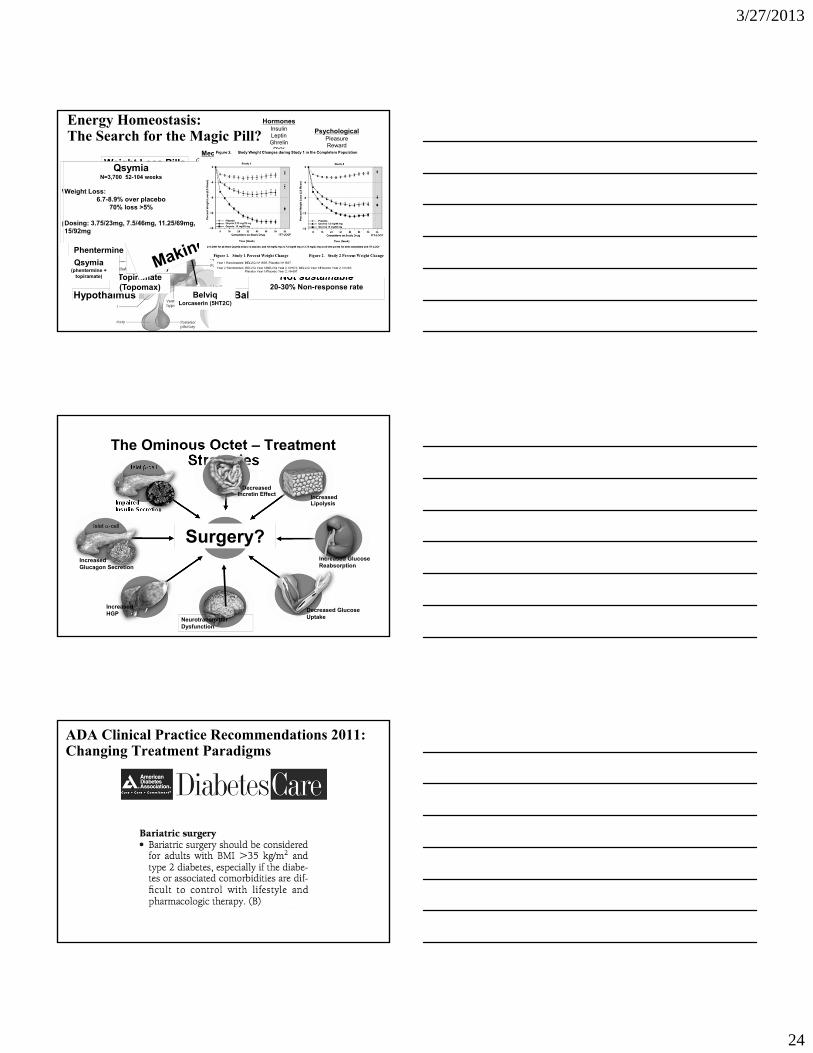
Energy Homeostasis:The Search for the Magic Pill?
SubstratesGlucose
AminoacidsFree Fatty Acids
Lipids
HormonesInsulinLeptinGhrelin
PYYCCK
Adiponectin
MechanicalGastric Distension
NeuralVagal Afferents
PsychologicalPleasureRewardVisual
OlfactoryTaste
Hypothalmus
Dopamine, CannabanoidsNorepinephrine, NPY
Serotonin, POMC,GABA etc…
Sibutramine(Meridia)
Topiramate(Topomax)
Phentermine
Rimonobant
Qsymia(phentermine +
topiramate)
Contrave(bupropion + naltrexone)
Energy Balance CenterBelviqLorcaserin (5HT2C)
BelviqLorcaserin (5HT2C)
Weight Loss Pills
Empatic(bupropion + zonisamide)
Tesofensine(NS2330) 4-8% Total body weight loss
Not sustainable20-30% Non-response rate
BelviqN=8,000 52-104 weeks
Weight Loss: 3-3.7% over placebo
47% loss >5%
Dosing: 10mg BID
QsymiaN=3,700 52-104 weeks
Weight Loss: 6.7-8.9% over placebo
70% loss >5%
Dosing: 3.75/23mg, 7.5/46mg, 11.25/69mg, 15/92mg
The Ominous Octet – Treatment Strategies
Islet -cell
ImpairedInsulin Secretion
NeurotransmitterDysfunction
Decreased GlucoseUptake
Islet -cell
IncreasedGlucagon Secretion
IncreasedLipolysis
Increased GlucoseReabsorption
IncreasedHGP
DecreasedIncretin Effect
Surgery?
ADA Clinical Practice Recommendations 2011:Changing Treatment Paradigms
3/27/2013
25
Energy Homeostasis:A Role for Surgery?
Lap BandRestriction of caloric intake
Gastric Bypass (Roux-En-Y)Restriction of caloric intakeMalabsorption of nutrients
X
Gastric Bypass: Five Operations
CONFIDENTIAL
Gastric Bypass: Five Operations
1. Isolation of gastric cardia
CONFIDENTIAL

3/27/2013
26
Gastric Bypass: Five Operations
2. Exclusion of distal stomach
CONFIDENTIAL
Gastric Bypass: Five Operations
3. Exclusion of duodenum and proximal jejunum
CONFIDENTIAL
Gastric Bypass: Five Operations
4. Exposure of distal jejunum to undigested nutrients
CONFIDENTIAL

3/27/2013
27
Gastric Bypass: Five Operations
5. Partial vagotomy
CONFIDENTIAL
Energy Homeostasis:A Role for Surgery?
Sleeve GastrectomyStomach becomes a “sleeve”Alters signaling mechanismsIndependent glycemic effect
Metabolic Surgery: The STAMPEDE Trial
Type 2 DM, A1c > 7.0%, BMI 27 - 43
N = 150, single center, one surgeon
Intensive Medical Therapy
No Surgery
Sleeve Gastrectomy
Gastric Bypass
Primary Outcome: Proportion with A1c < 6.0% at 12 months

3/27/2013
28
Metabolic Surgery: The STAMPEDE Trial
Metabolic Surgery: The STAMPEDE Trial

3/27/2013
29
THE END
Metabolic Surgery: The STAMPEDE Trial -Results