presentazione di powerpoint · 2019-11-05 · key telemedicine components in diabetes 1. accurate...
TRANSCRIPT
FRANCESCO GIORGINO
DIPARTIMENTO DELL’EMERGENZA E DEI TRAPIANTI DI ORGANI
SEZIONE DI MEDICINA INTERNA, ENDOCRINOLOGIA, ANDROLOGIA E MALATTIE METABOLICHE
Glucose Monitoring: why?
• Evaluate the efficacy of current therapy
• Make insulin and medication dose adjustments
• Monitor treatment safety
• Enable patients to better understand the impact of diet,
exercise, illness, stress, and medications on glucose
levels
• Enable patients to recognize and treat hypoglycemic
and hyperglycemic episodes
• Select the most appropriate drug therapy
modified from Bailey T.S., et al. AACE/ACE GM Consensus Statement 2016

Monitoraggio GlicemicoLa Tecnologia al Servizio della Cura
• Telemedicina
• CGM/FGM
Quale tra le seguenti ritenete la modalità più
efficace/appropriata per l’implementazione della
telemedicina in Diabetologia?
1. Real-time video conferencing
2. Comunicazione tramite websites
3. Comunicazione tramite e-mail
4. SMS e messaggi via smartphone
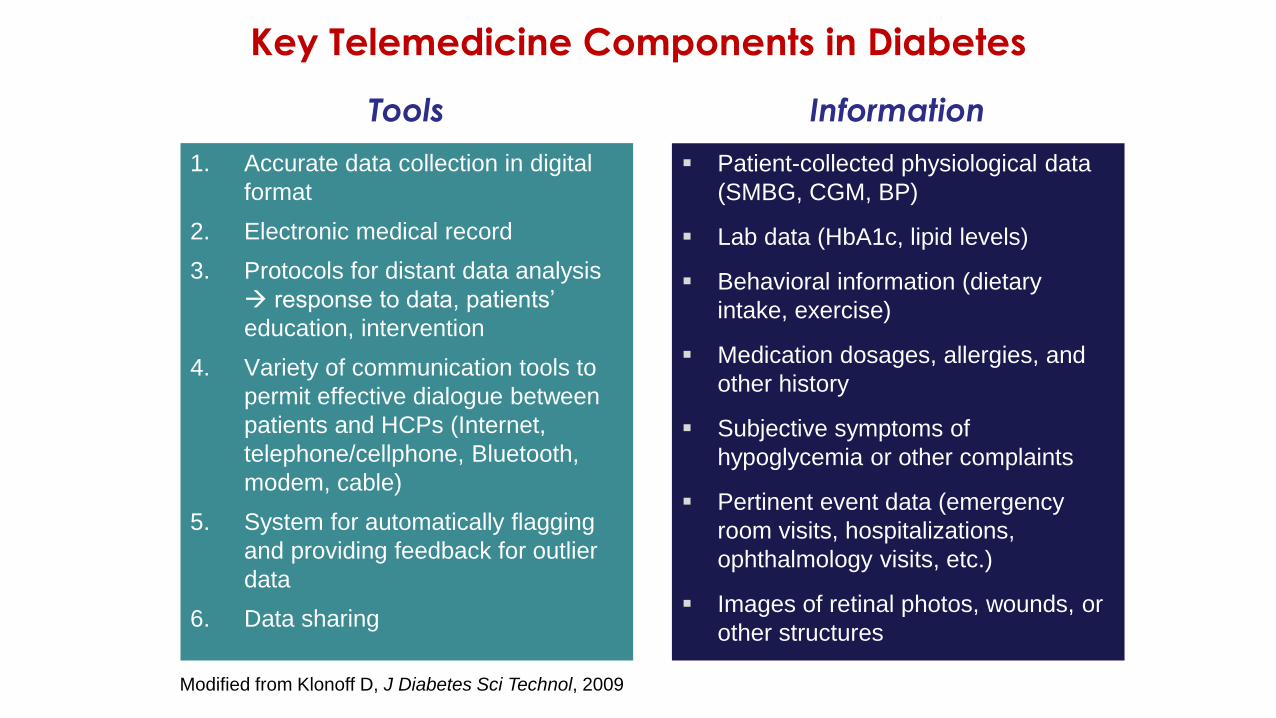
Key Telemedicine Components in Diabetes
1. Accurate data collection in digital
format
2. Electronic medical record
3. Protocols for distant data analysis
→ response to data, patients’
education, intervention
4. Variety of communication tools to
permit effective dialogue between
patients and HCPs (Internet,
telephone/cellphone, Bluetooth,
modem, cable)
5. System for automatically flagging
and providing feedback for outlier
data
6. Data sharing
Modified from Klonoff D, J Diabetes Sci Technol, 2009
▪ Patient-collected physiological data
(SMBG, CGM, BP)
▪ Lab data (HbA1c, lipid levels)
▪ Behavioral information (dietary
intake, exercise)
▪ Medication dosages, allergies, and
other history
▪ Subjective symptoms of
hypoglycemia or other complaints
▪ Pertinent event data (emergency
room visits, hospitalizations,
ophthalmology visits, etc.)
▪ Images of retinal photos, wounds, or
other structures
Tools Information
Internal
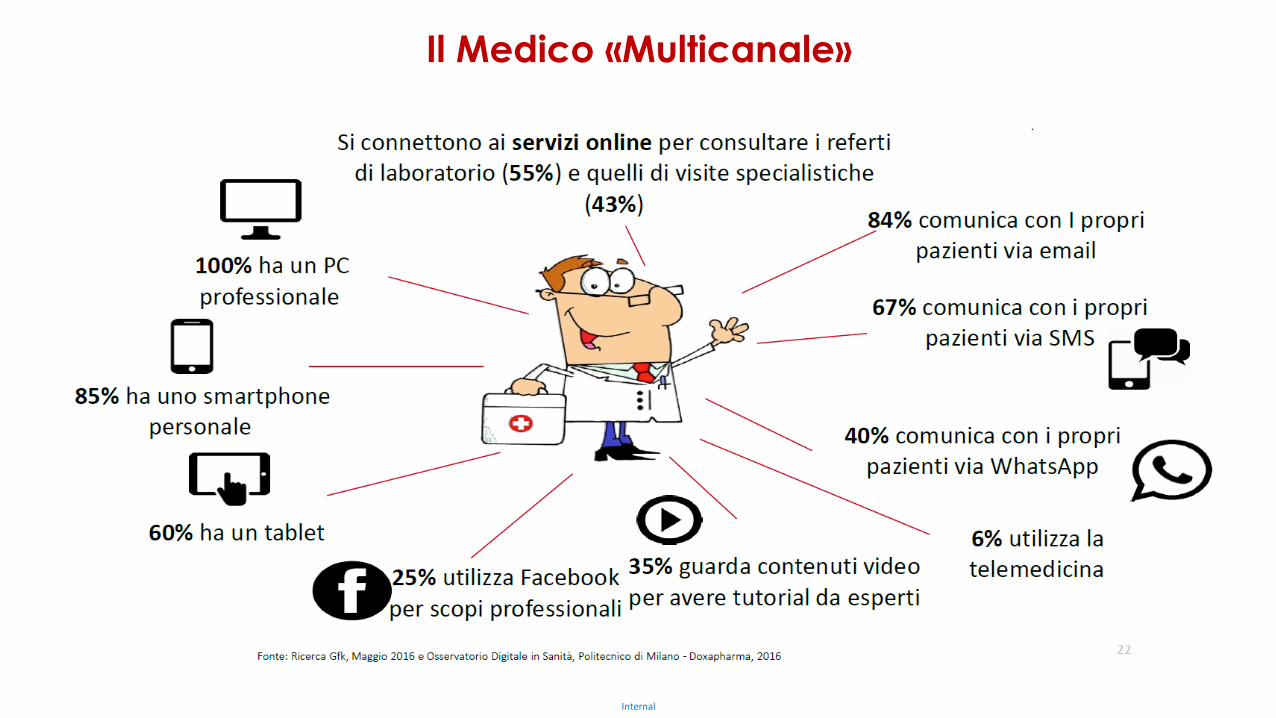
Il Medico «Multicanale»

Quale entità di riduzione di HbA1c può essere ottenuta
con l’uso della telemedicina nel diabete?
1. Non apprezzabile
2. 0,5%
3. 1%
4. 1,5%
5. Si è osservata solo una riduzione dei casi di marcato
scompenso glicemico
Risposta esatta: 2
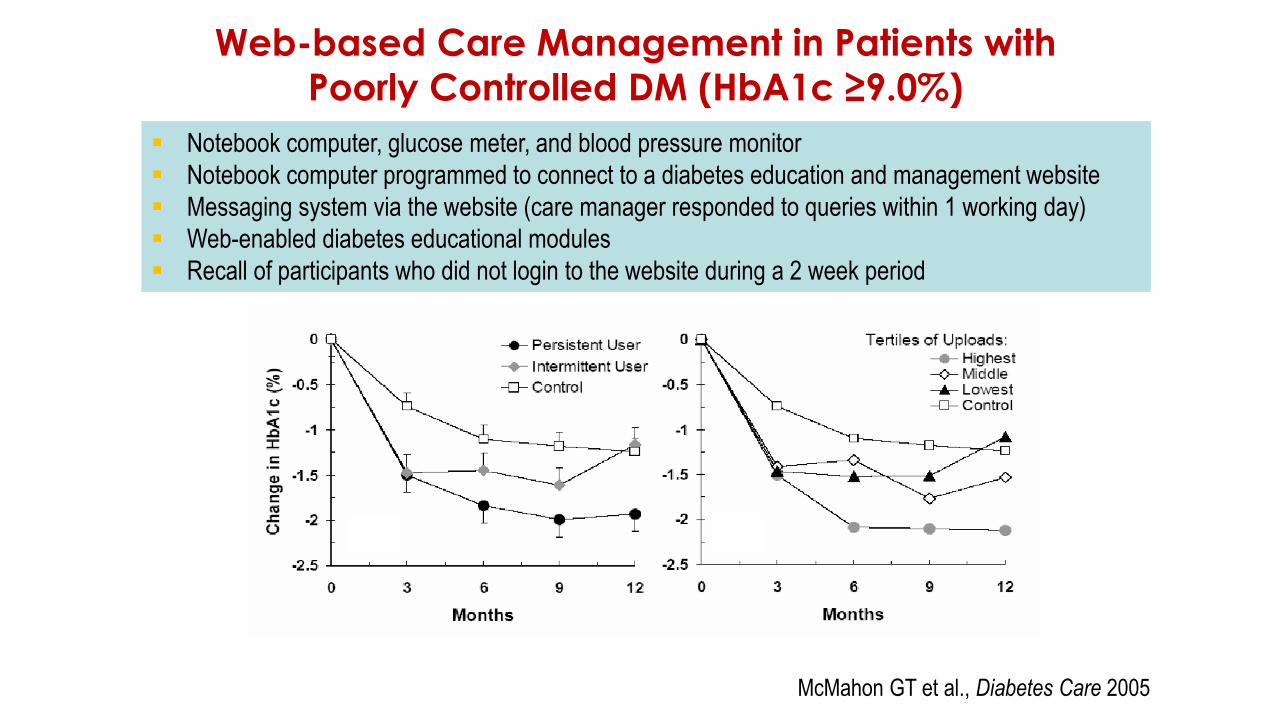
Web-based Care Management in Patients with
Poorly Controlled DM (HbA1c ≥9.0%)
▪ Notebook computer, glucose meter, and blood pressure monitor
▪ Notebook computer programmed to connect to a diabetes education and management website
▪ Messaging system via the website (care manager responded to queries within 1 working day)
▪ Web-enabled diabetes educational modules
▪ Recall of participants who did not login to the website during a 2 week period
McMahon GT et al., Diabetes Care 2005
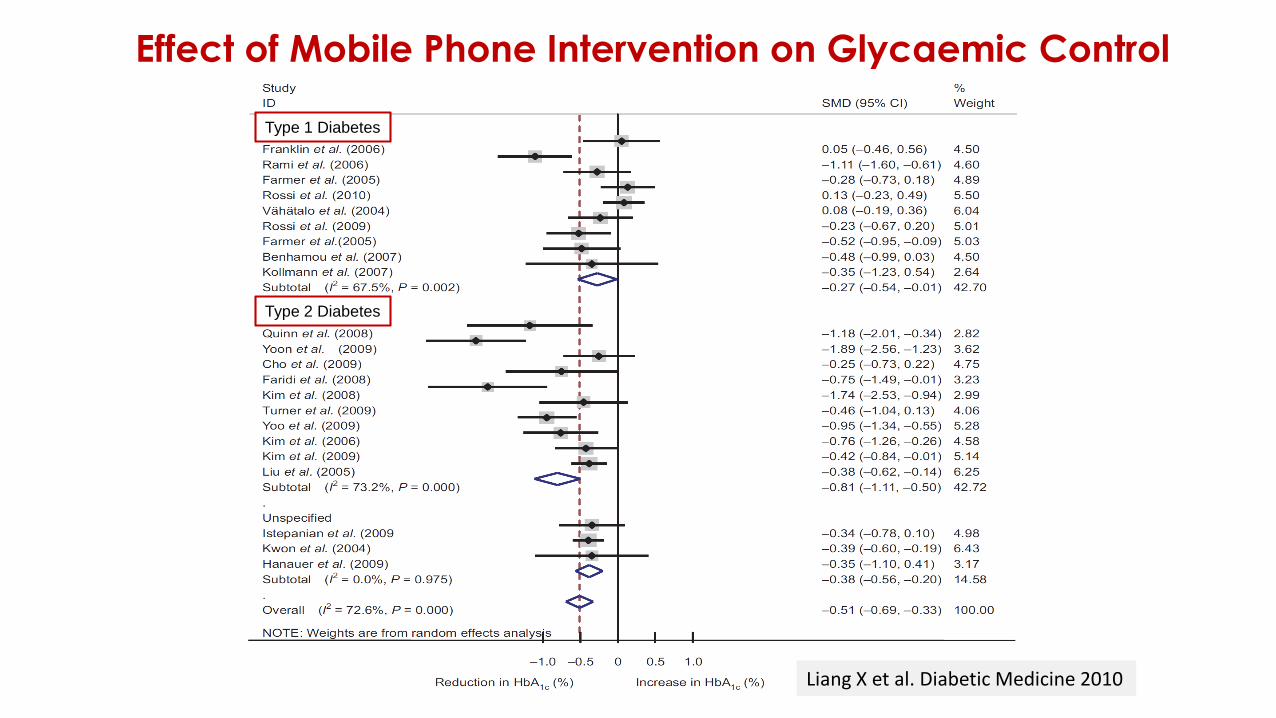
Effect of Mobile Phone Intervention on Glycaemic Control
Liang X et al. Diabetic Medicine 2010
Type 1 Diabetes
Type 2 Diabetes
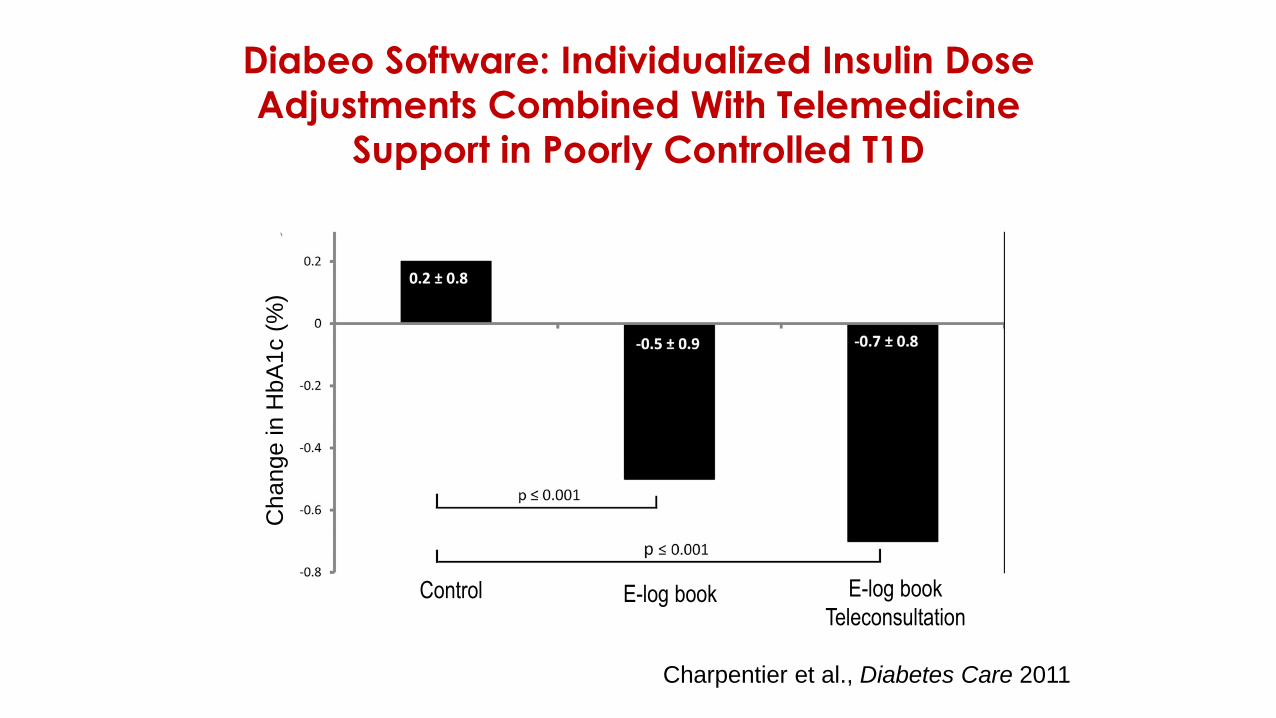
Diabeo Software: Individualized Insulin Dose
Adjustments Combined With Telemedicine
Support in Poorly Controlled T1D
Charpentier et al., Diabetes Care 2011
Change
in H
bA
1c (
%)
E-log bookControl E-log book
Teleconsultation
Medicine, December 2014
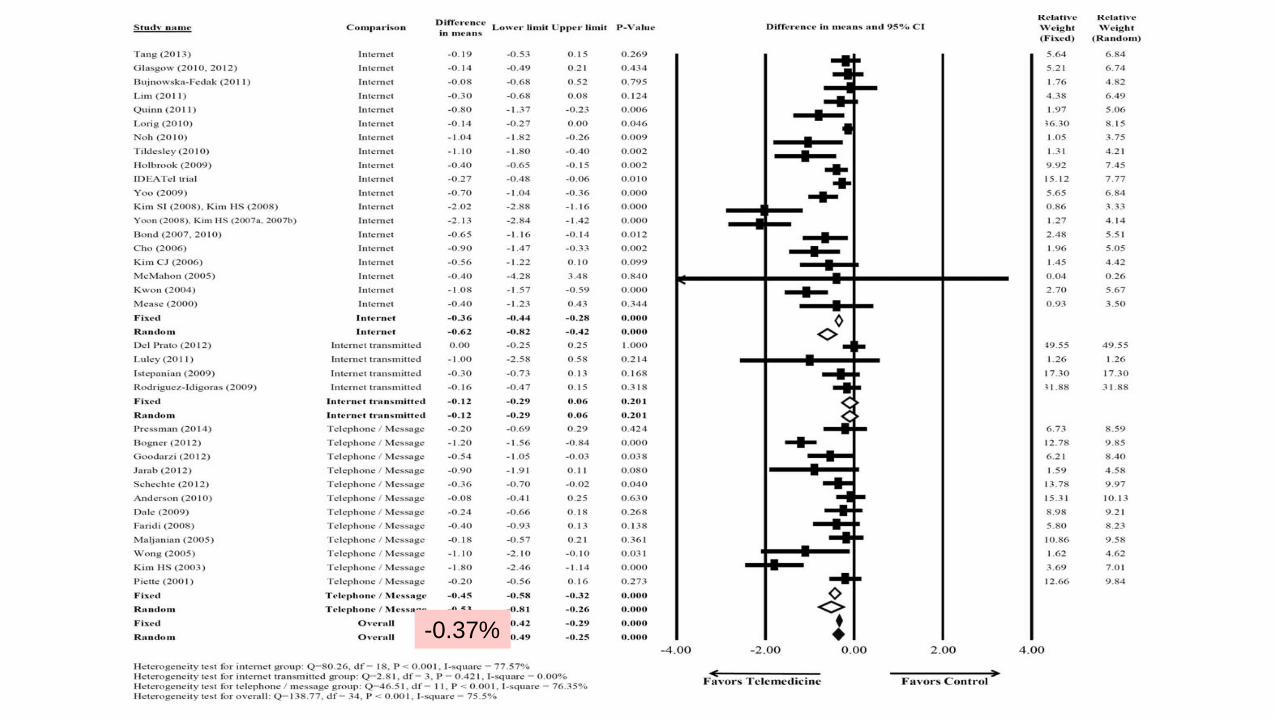
-0.37%

L’uso della telemedicina nel diabete ha mostrato:
1. Un miglioramento del controllo glico-metabolico
2. Un miglioramento della qualità di vita
3. Una riduzione degli episodi di ipoglicemia
4. Un potenziale impatto su parametri lipidici e pressori
5. Tutte le precedenti
Risposta esatta: 5
Impact of the "Diabetes Interactive Diary" Telemedicine on
Metabolic Control, Risk of Hypoglycemia, and QoL in T1DRossi MC et al., Diabetes Technol Ther. 2013 Aug;15:670-9
▪ Diabetes Interactive Diary (DID): carbohydrate/bolus calculator
promoting the patient-physician communication via SMS
▪ 127 T1D patients not previously educated on carbohydrate counting
assigned to DID or standard of care
▪ No between-group difference in HbA1c levels
▪ Lower risk of grade 2 hypoglycemia with DID
▪ DID improved the "perceived frequency of hyperglycemic
episodes" scale of the DTSQ and the "social relations" and the
"fear of hypoglycemia" dimensions of the DSQLS

Web-based Intervention and Physical Outcomes
Associated with Diabetes among Adults > 60 yrsBond GE, et al., Diabetes Technol Ther. 2007;9:52–9
▪ RCT, 62 subjects (87% with T2D), 6-month follow-up
▪ Nurse-based
▪ Computer experience or computer literacy not required for eligibility
▪ Several behavioral strategies (coaching, motivational, and social
support)
▪ Mean HbA1c level decreased in the intervention group from
7.0% to 6.4% and in the control group from 7.1% to 7.0% (P =
0.01)
▪ Significant reductions in SBP, DBP, total cholesterol and weight
in the intervention group
“this study disproves the myth that seniors will not be attracted to the
Internet as a way of communication”
Interactive Telemedicine (TM): Effects on
Professional Practice and Health Care OutcomesFlodgren G et al., Cochrane Database Syst Rev 2015
• 93 eligible trials (N = 22,047 participants)
• 21 in patients with diabetes
• Education and advice for self-management, specialist consultations for
diagnosis and treatment decisions
• Telephone, e-mail, SMS
• Lower HbA1c with TM: -0.31% (95% CI -0.37 to -0.24; P < 0.00001)
at a median of nine months follow-up
• Some evidence for a decrease in LDL (4 studies, N = 1692; -12.45,
95% CI -14.23 to -10.68; P < 0.00001) and blood pressure (4
studies, N = 1770: SBP:-4.33, 95% CI -5.30 to -3.35, P < 0.00001;
DBP: -2.75 95% CI -3.28 to -2.22, P < 0.00001) with TM
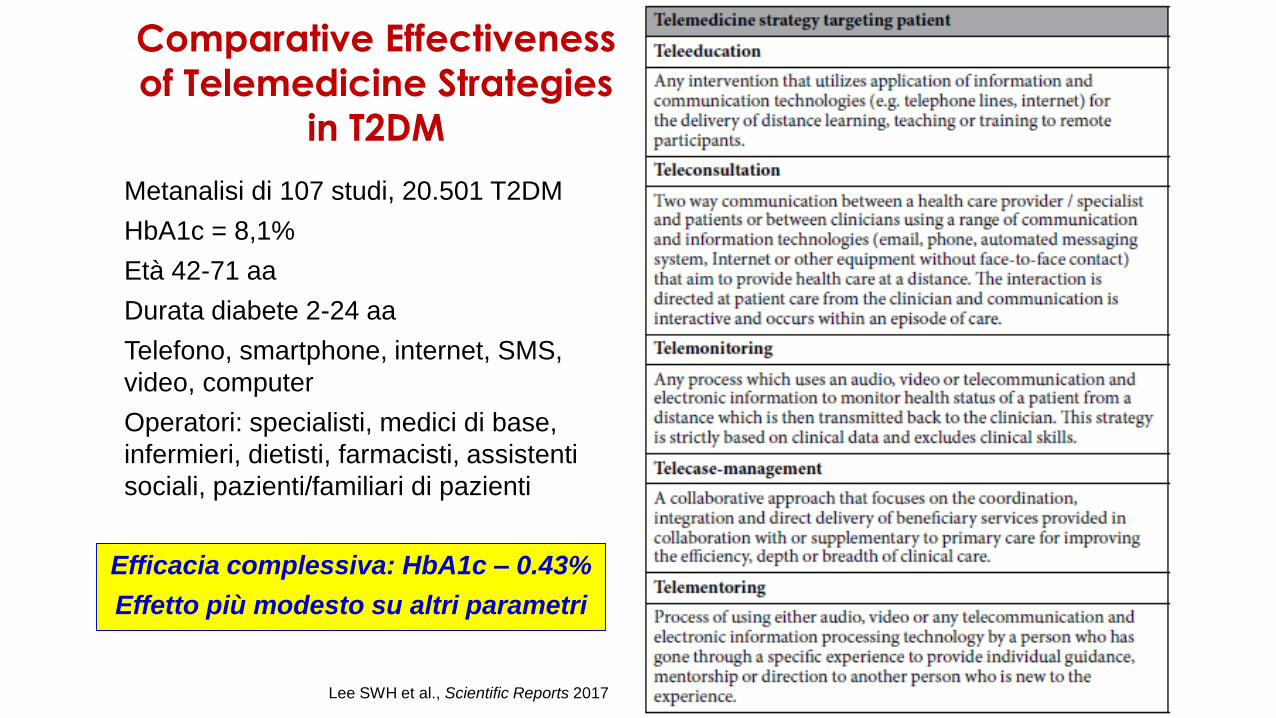
Comparative Effectiveness
of Telemedicine Strategies
in T2DM
Lee SWH et al., Scientific Reports 2017
Metanalisi di 107 studi, 20.501 T2DM
HbA1c = 8,1%
Età 42-71 aa
Durata diabete 2-24 aa
Telefono, smartphone, internet, SMS,
video, computer
Operatori: specialisti, medici di base,
infermieri, dietisti, farmacisti, assistenti
sociali, pazienti/familiari di pazienti
Efficacia complessiva: HbA1c – 0.43%
Effetto più modesto su altri parametri
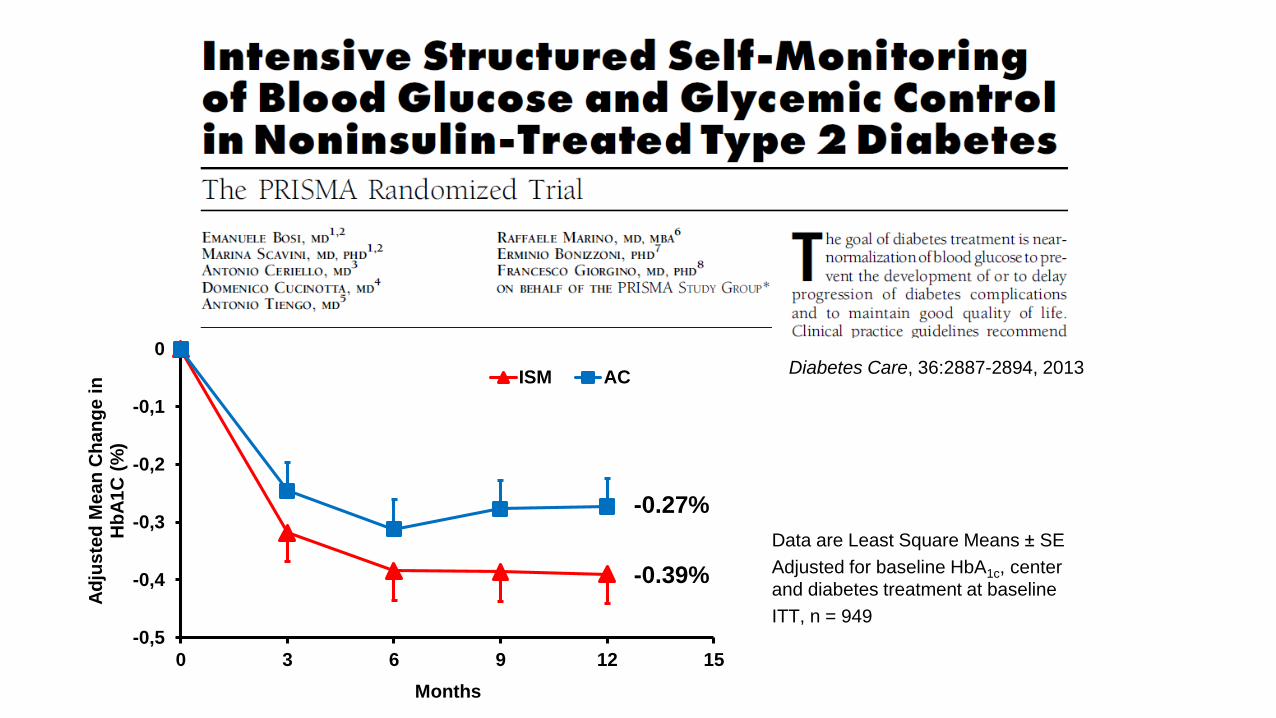
Diabetes Care, 36:2887-2894, 2013
-0,5
-0,4
-0,3
-0,2
-0,1
0
0 3 6 9 12 15
Ad
juste
d M
ean
Ch
an
ge i
n
Hb
A1
C (
%)
Months
ISM AC
-0.39%
-0.27%
Data are Least Square Means ± SE
Adjusted for baseline HbA1c, center
and diabetes treatment at baseline
ITT, n = 949
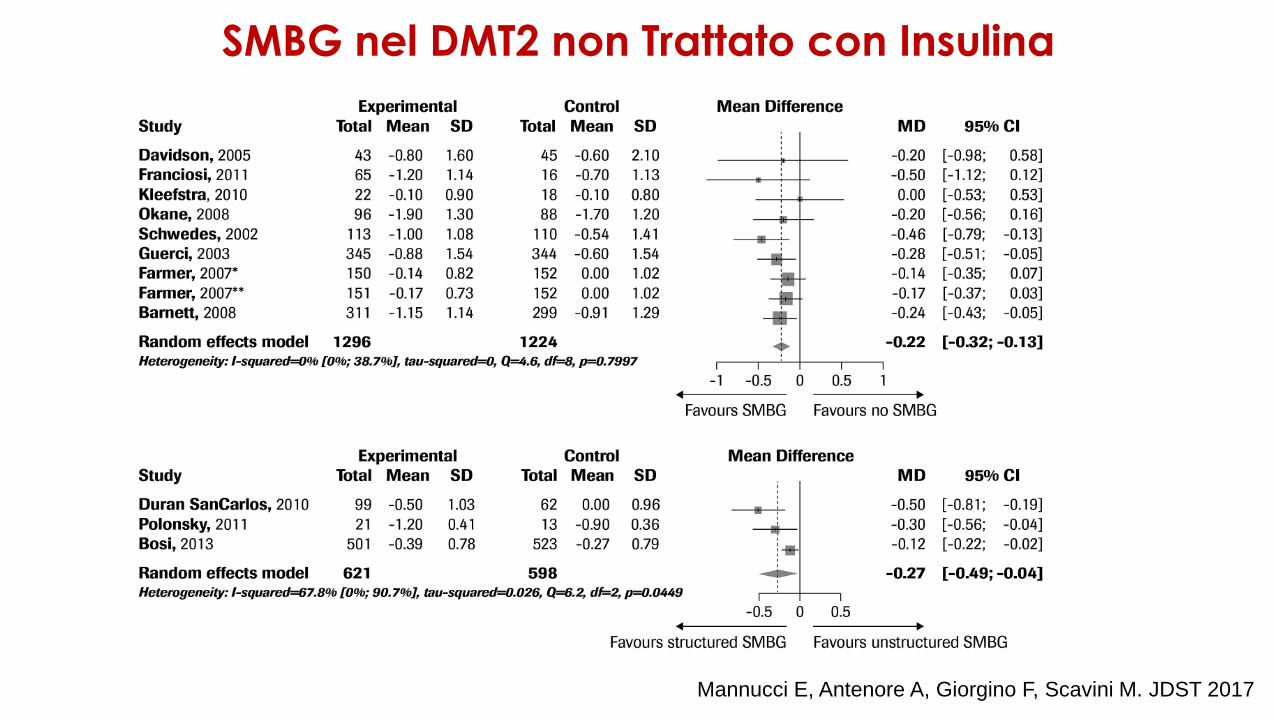
Mannucci E, Antenore A, Giorgino F, Scavini M. JDST 2017
SMBG nel DMT2 non Trattato con Insulina
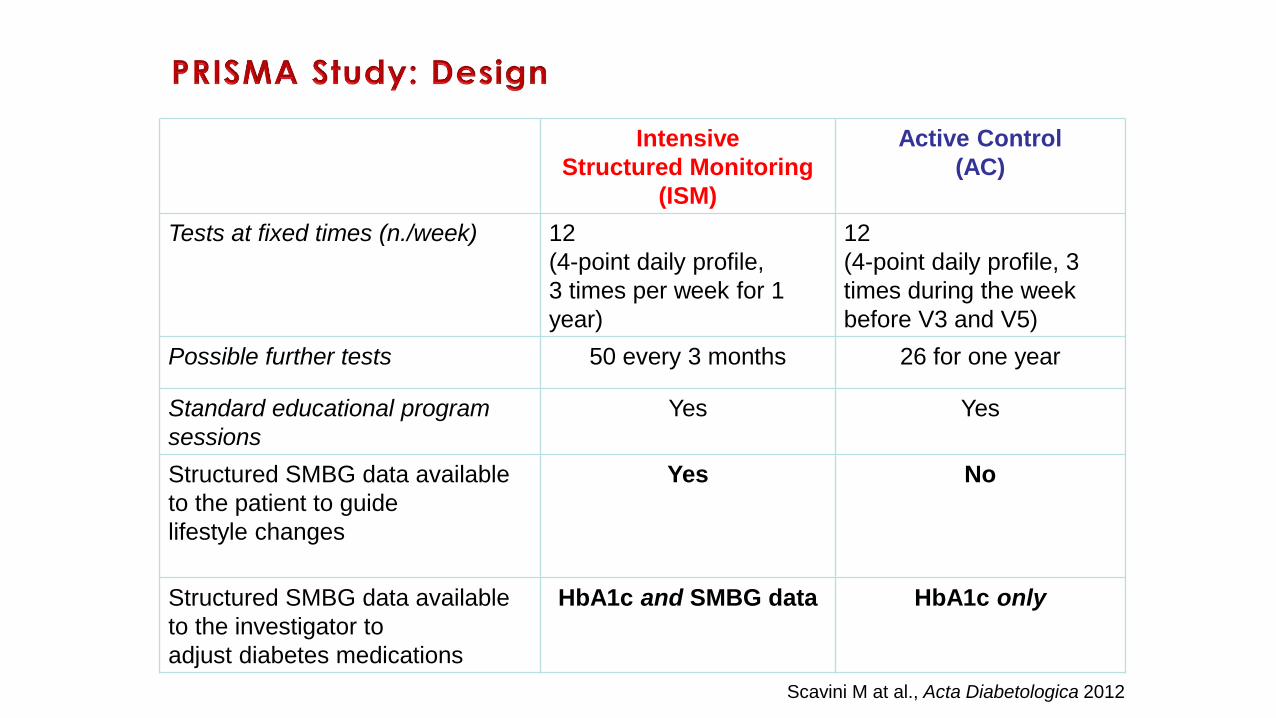
Intensive
Structured Monitoring
(ISM)
Active Control
(AC)
Tests at fixed times (n./week) 12
(4-point daily profile,
3 times per week for 1
year)
12
(4-point daily profile, 3
times during the week
before V3 and V5)
Possible further tests 50 every 3 months 26 for one year
Standard educational program
sessions
Yes Yes
Structured SMBG data available
to the patient to guide
lifestyle changes
Yes No
Structured SMBG data available
to the investigator to
adjust diabetes medications
HbA1c and SMBG data HbA1c only
Scavini M at al., Acta Diabetologica 2012
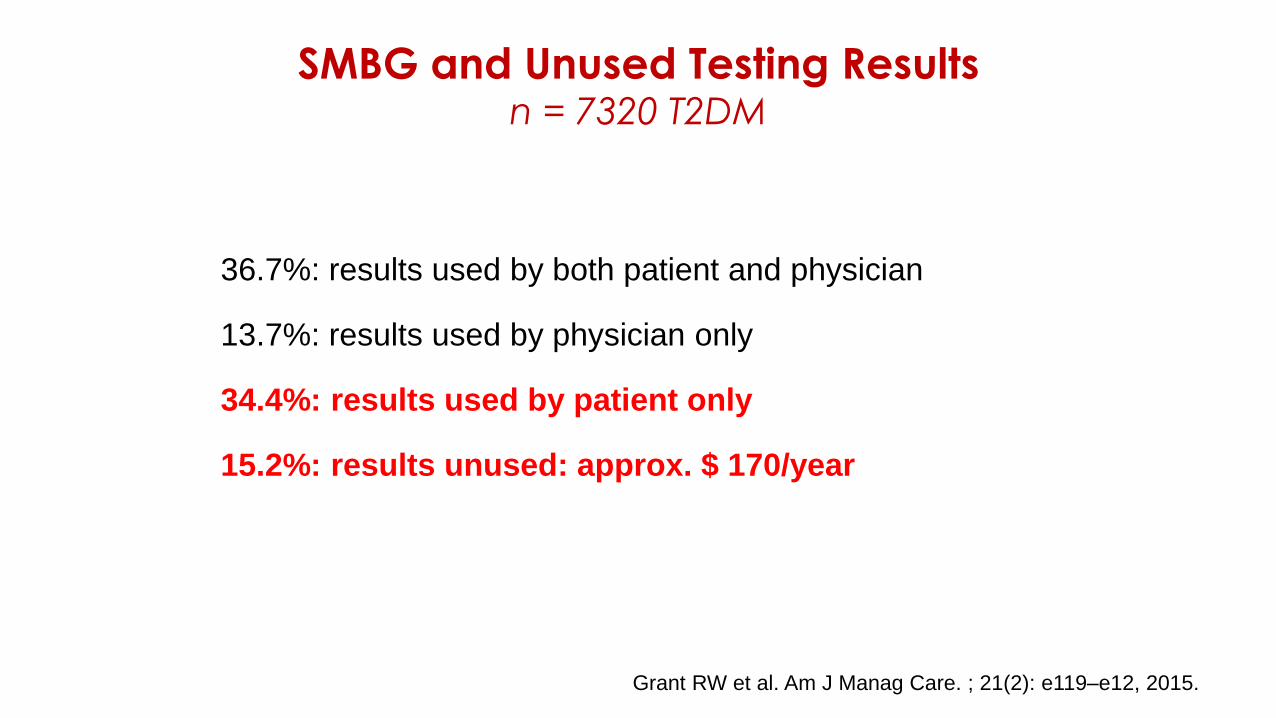
Grant RW et al. Am J Manag Care. ; 21(2): e119–e12, 2015.
SMBG and Unused Testing Resultsn = 7320 T2DM
36.7%: results used by both patient and physician
13.7%: results used by physician only
34.4%: results used by patient only
15.2%: results unused: approx. $ 170/year
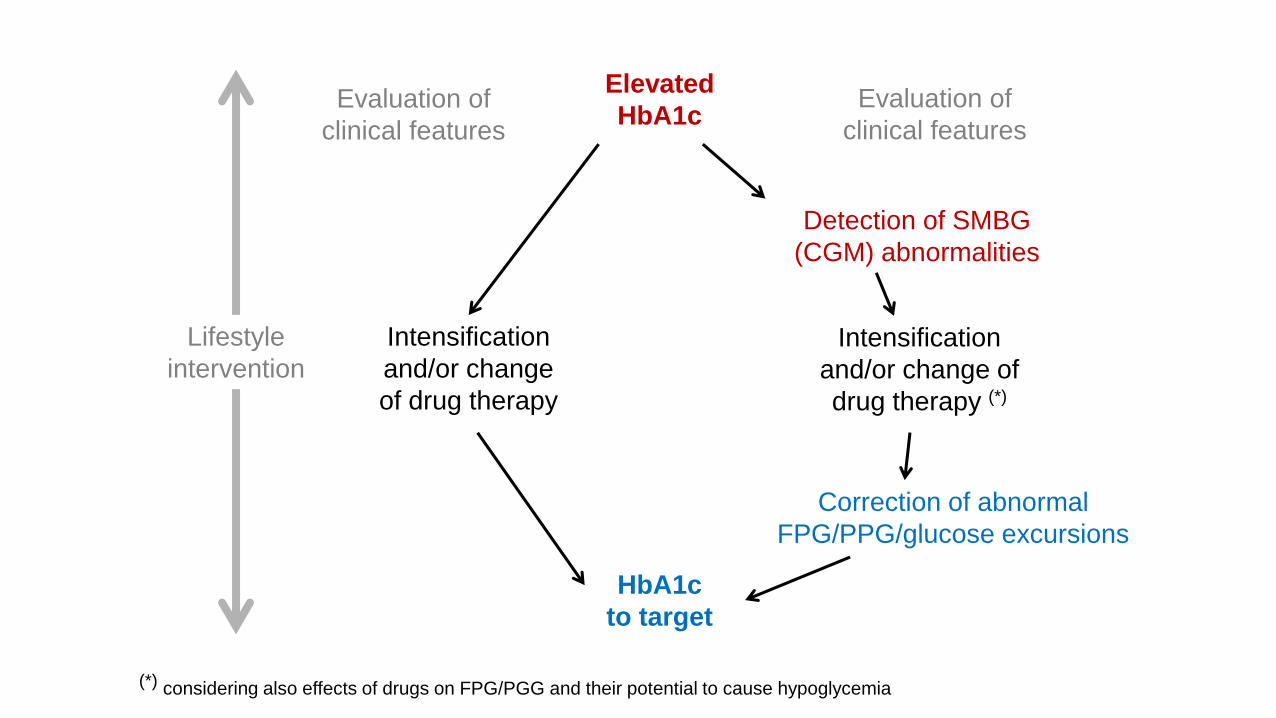
Elevated
HbA1c
HbA1c
to target
Intensification
and/or change
of drug therapy
Lifestyle
intervention
Evaluation of
clinical features
Evaluation of
clinical features
Detection of SMBG
(CGM) abnormalities
Intensification
and/or change of
drug therapy (*)
Correction of abnormal
FPG/PPG/glucose excursions
(*) considering also effects of drugs on FPG/PGG and their potential to cause hypoglycemia
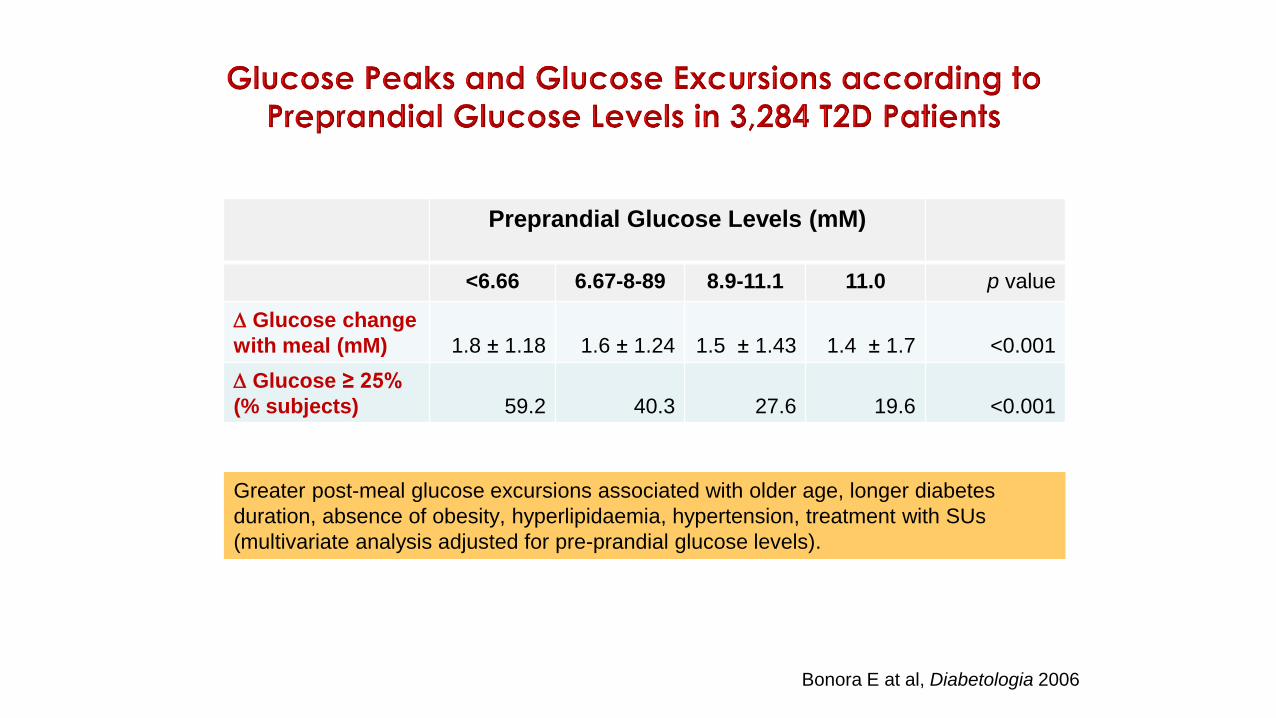
Greater post-meal glucose excursions associated with older age, longer diabetes
duration, absence of obesity, hyperlipidaemia, hypertension, treatment with SUs
(multivariate analysis adjusted for pre-prandial glucose levels).
Preprandial Glucose Levels (mM)
<6.66 6.67-8-89 8.9-11.1 11.0 p value
Glucose change
with meal (mM) 1.8 ± 1.18 1.6 ± 1.24 1.5 ± 1.43 1.4 ± 1.7 <0.001
Glucose ≥ 25%
(% subjects) 59.2 40.3 27.6 19.6 <0.001
Bonora E at al, Diabetologia 2006
Monitoraggio GlicemicoLa Tecnologia al Servizio della Cura
• Telemedicina
• CGM/FGM
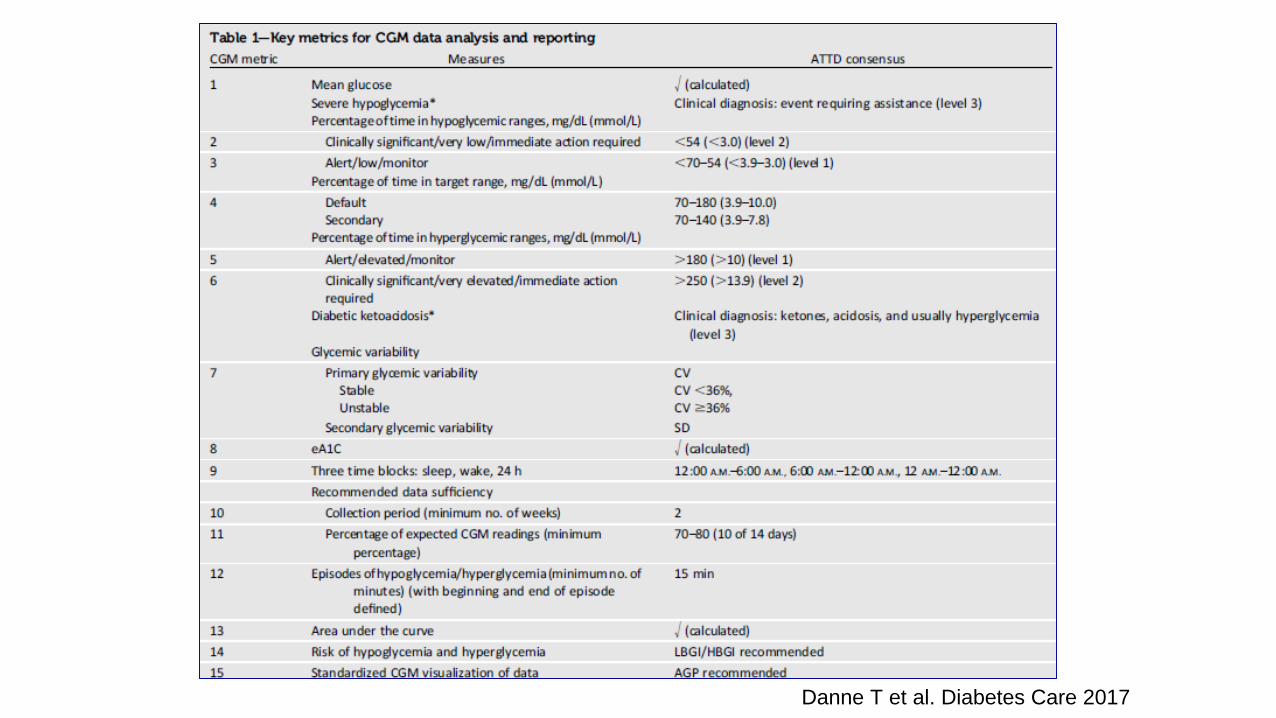
Non-HbA1c Glucose Metrics
Maahs DM et al. Diabetes Care 2016Danne T et al. Diabetes Care 2017
Quale dei seguenti parametri ottenibili con il CGM
ritenete più utile dal punto di vista clinico?
1. Media della glicemia
2. Media delle glicemie a digiuno, pre-prandiali e post-prandiali
3. Deviazione Standard (DS), Coefficiente di variazione (CV), range
interquartile (IQR)
4. TIR (Time in Range)
5. TATR (Time Above Target Range)
6. TBTR (Time Below Target Range)
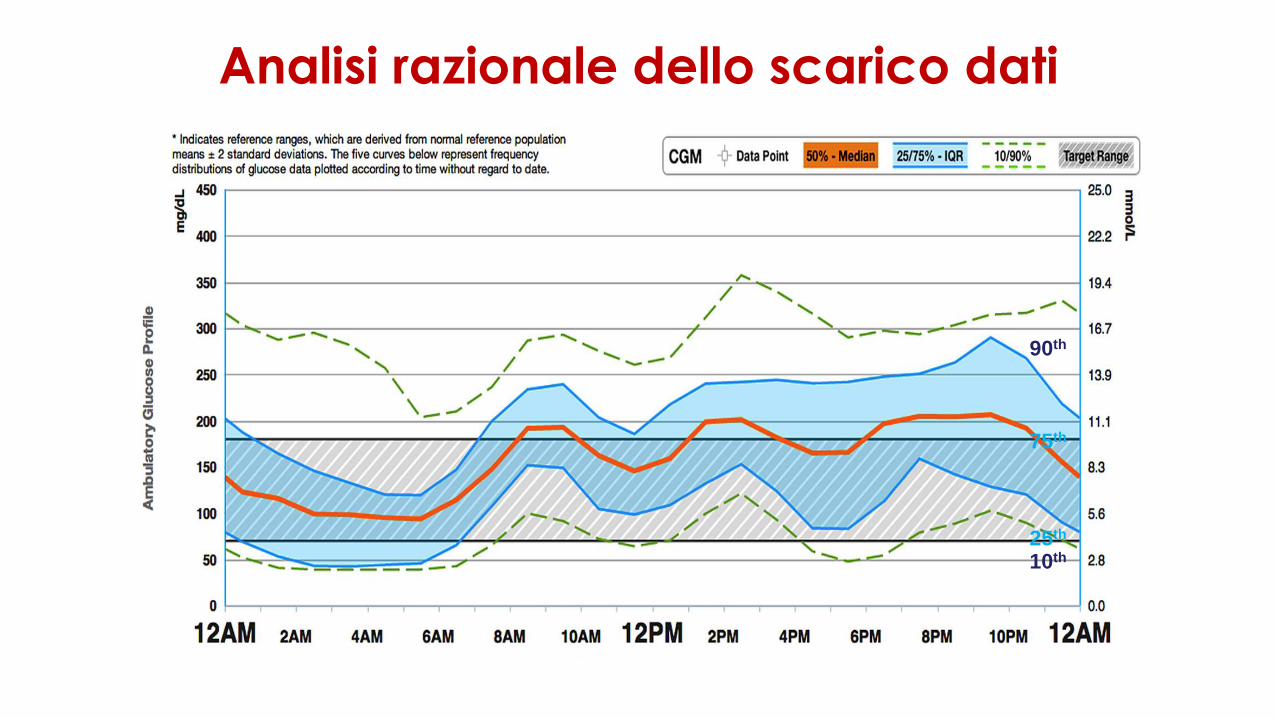
Analisi razionale dello scarico dati
10th
25th
75th
90th
▪ HbA1c stabilmente superiore al target desiderabile
▪ Ipoglicemia problematica (no FGM in ipoglicemia inavvertita)
▪ Disponibilità all’impiego costante (>70%)
▪ Training (iniziale + refresh periodico)
▪ Adeguato periodo di «prova»
▪ Capacità di gestione del dato (paziente)
▪ Capacità di interpretazione del dato (team)
CGM/FGM: qualche spunto per l’appropriatezza
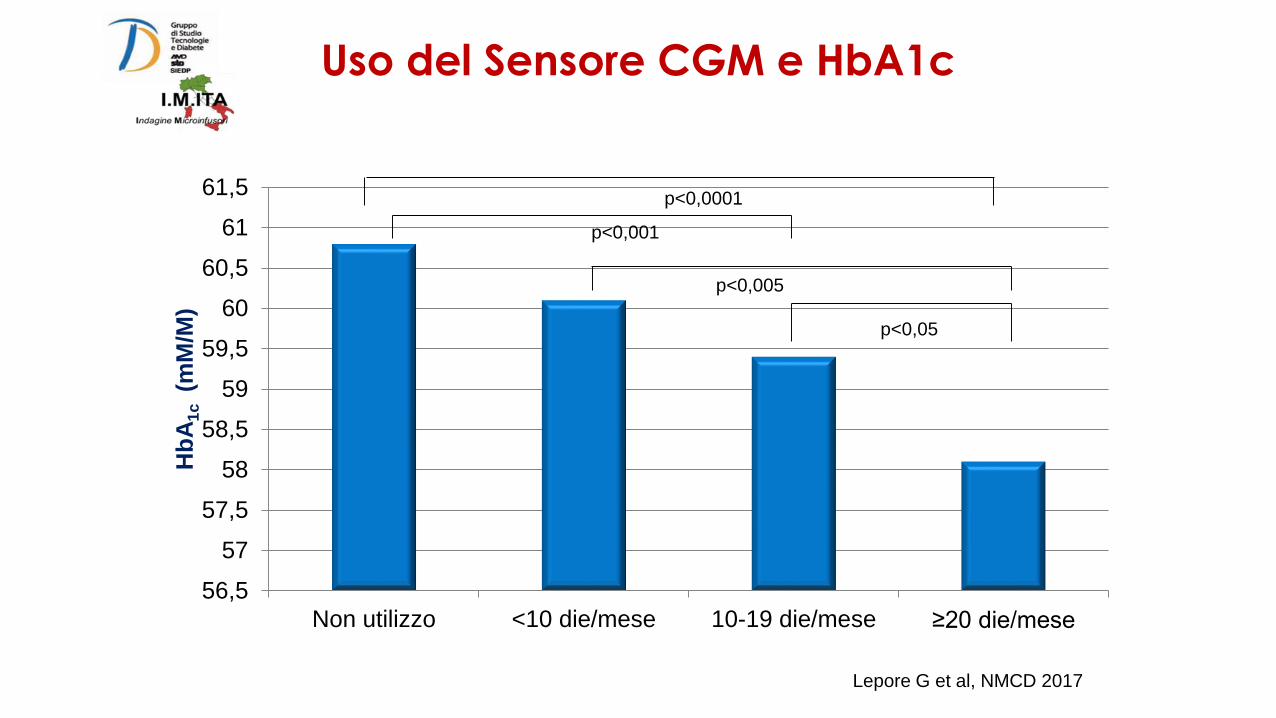
56,5
57
57,5
58
58,5
59
59,5
60
60,5
61
61,5
Non utilizzo <10 die/mese 10-19 die/mese ≥20 die/mese
Hb
A1
c (m
M/M
)p<0,0001
p<0,001
p<0,05
p<0,005
Uso del Sensore CGM e HbA1c
Lepore G et al, NMCD 2017
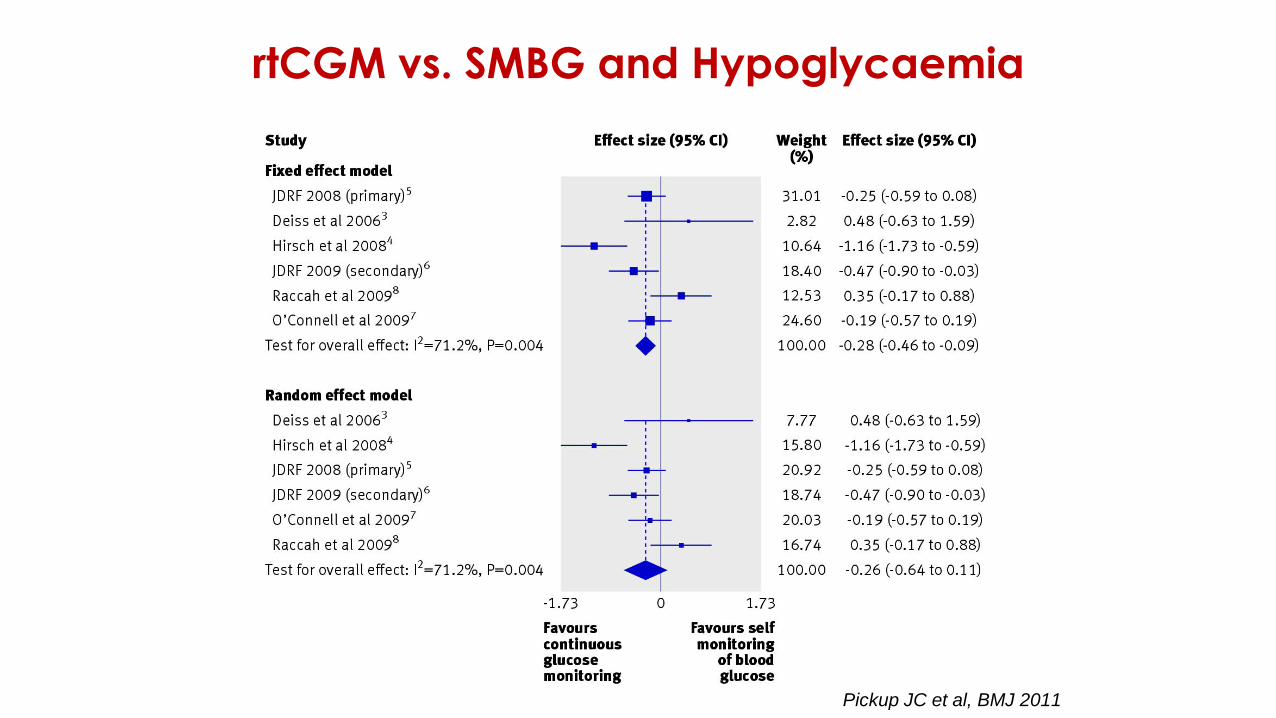
Pickup JC et al, BMJ 2011
rtCGM vs. SMBG and Hypoglycaemia
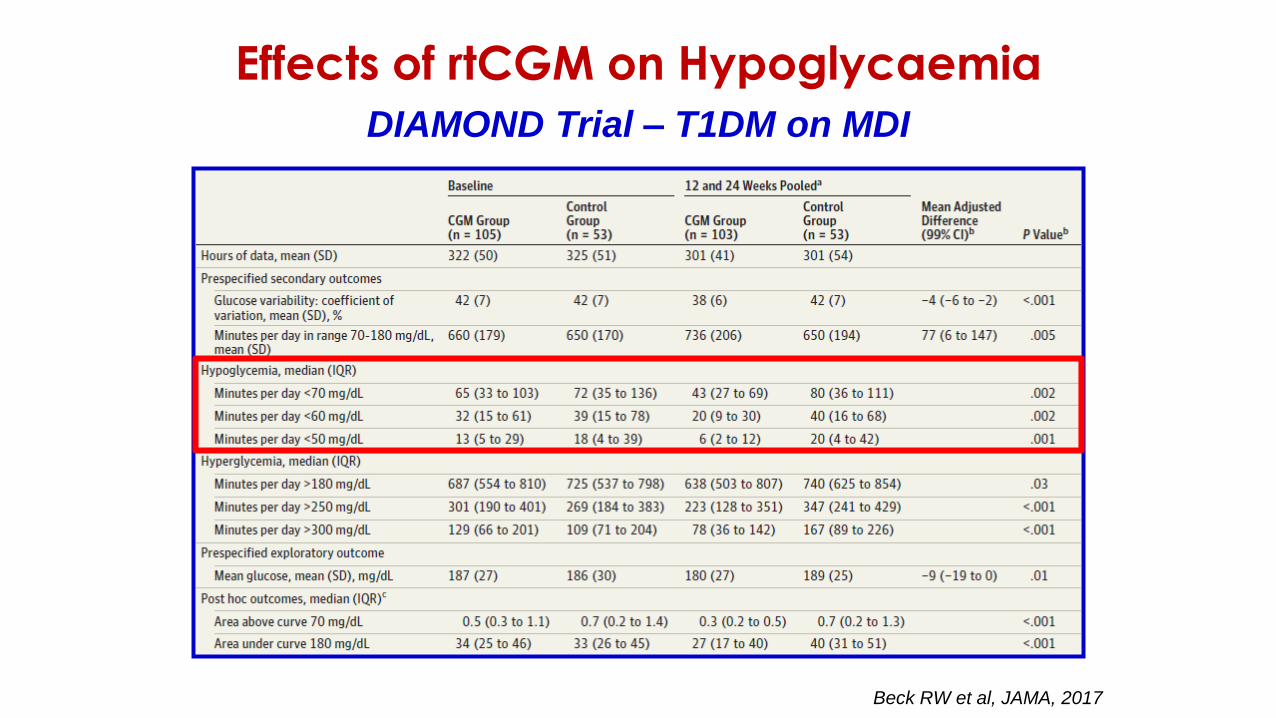
Beck RW et al, JAMA, 2017
DIAMOND Trial – T1DM on MDI
Effects of rtCGM on Hypoglycaemia
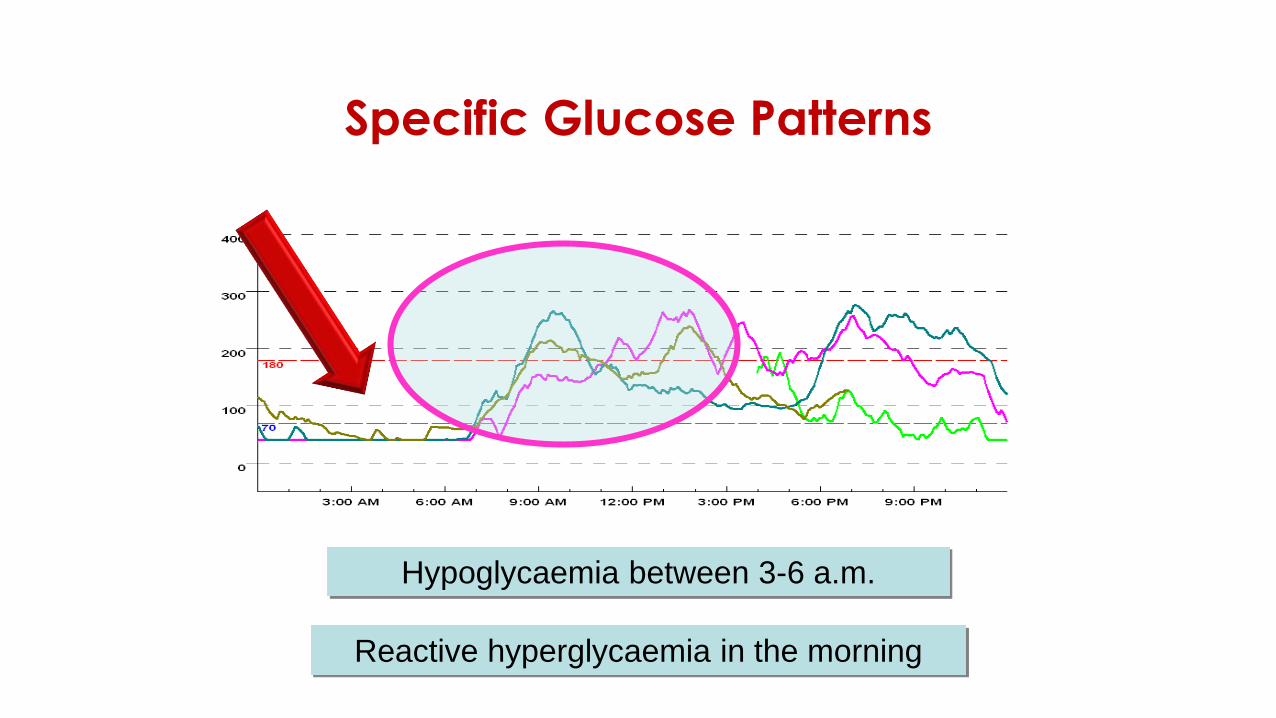
Specific Glucose Patterns
Hypoglycaemia between 3-6 a.m.
Reactive hyperglycaemia in the morning
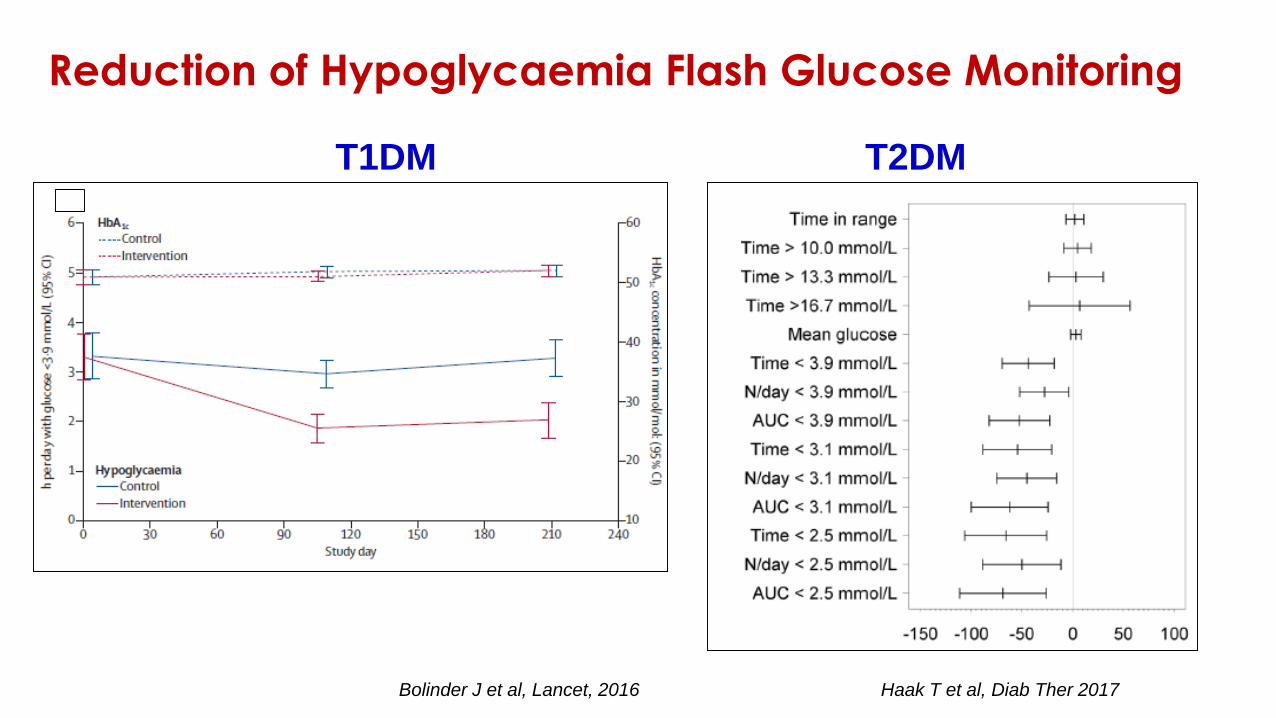
Bolinder J et al, Lancet, 2016 Haak T et al, Diab Ther 2017
T1DM T2DM
Reduction of Hypoglycaemia Flash Glucose Monitoring
Le informazioni ottenibili con il sistema rtCGM
sono:
1. valore assoluto della concentrazione di glucosio
2. valore assoluto della concentrazione di glucosio, frecce di
tendenza
3. valore assoluto della concentrazione di glucosio, frecce di
tendenza, allarmi
4. valore assoluto della concentrazione di glucosio, HbA1c stimata
Risposta esatta: 3
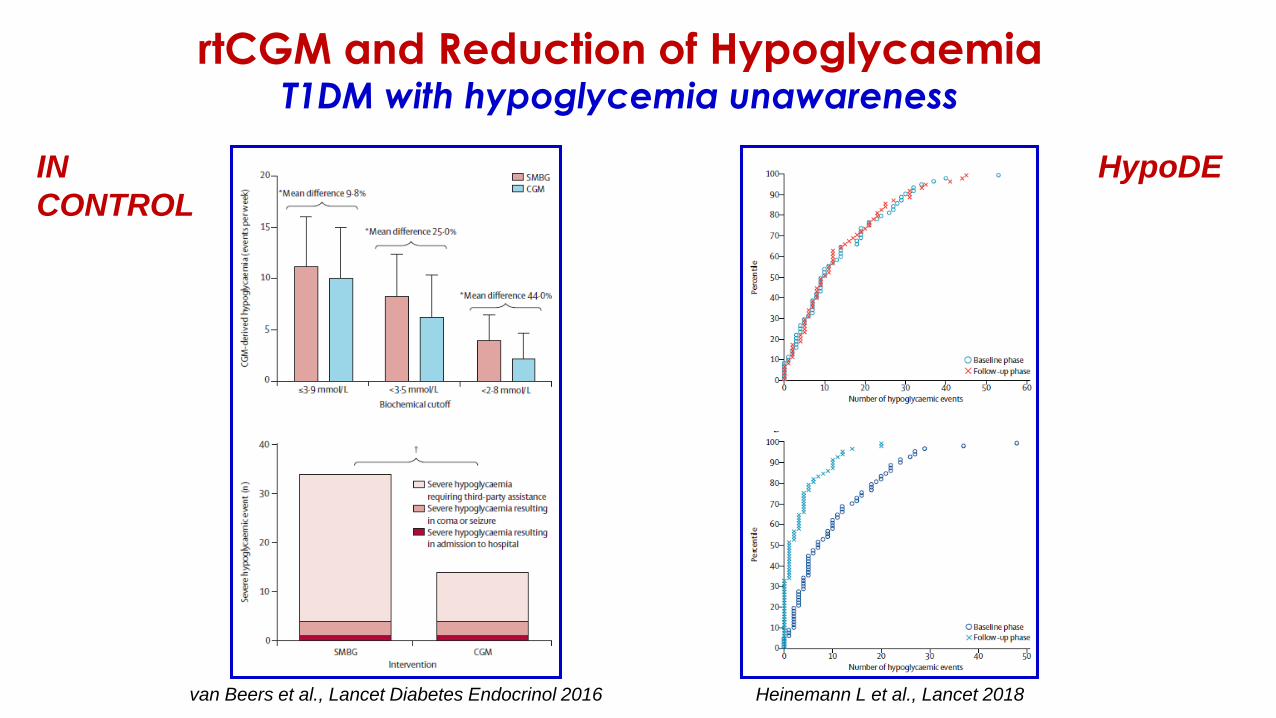
van Beers et al., Lancet Diabetes Endocrinol 2016 Heinemann L et al., Lancet 2018
rtCGM and Reduction of HypoglycaemiaT1DM with hypoglycemia unawareness
IN
CONTROL
HypoDE
Frecce di tendenza
• Le tendenze sono indicate dalle frecce
• La tendenza si genera in base all’andamento che la glicemia
ha avuto negli ultimi 15-20 minuti e cioè se è stata stabile, se
sta aumentando o se sta diminuendo
• Essa predice ciò che accadrà nei successivi 30 min se non ci
sono nuove variazioni
• Ciascun sistema ha un sua definizione di tendenza.

Quali decisioni prendere in basealle frecce di tendenza?
Pre
esercizioIntervento convenzionale Frecce Intervento appropriato
125
mg/dLAssumere 10-15 gr di CHO ➞ stabile
Assumere 10-15 gr di
CHO
125
mg/dLAssumere 10-15 gr di CHO
⬊⬇ lenta discesa Assumere 20-30 gr di
CHO
125
mg/dLAssumere 10-15 gr di CHO ⬇⬇ rapida discesa
Assumere 30-40 gr di
CHO
125
mg/dLAssumere 10-15 gr di CHO ⬈⬆ lenta salita Non è necessario snack
125
mg/dLAssumere 10-15 gr di CHO ⬆⬆ rapida salita
Controllare BG dopo 15-
20 e se necessario
effettuare bolo
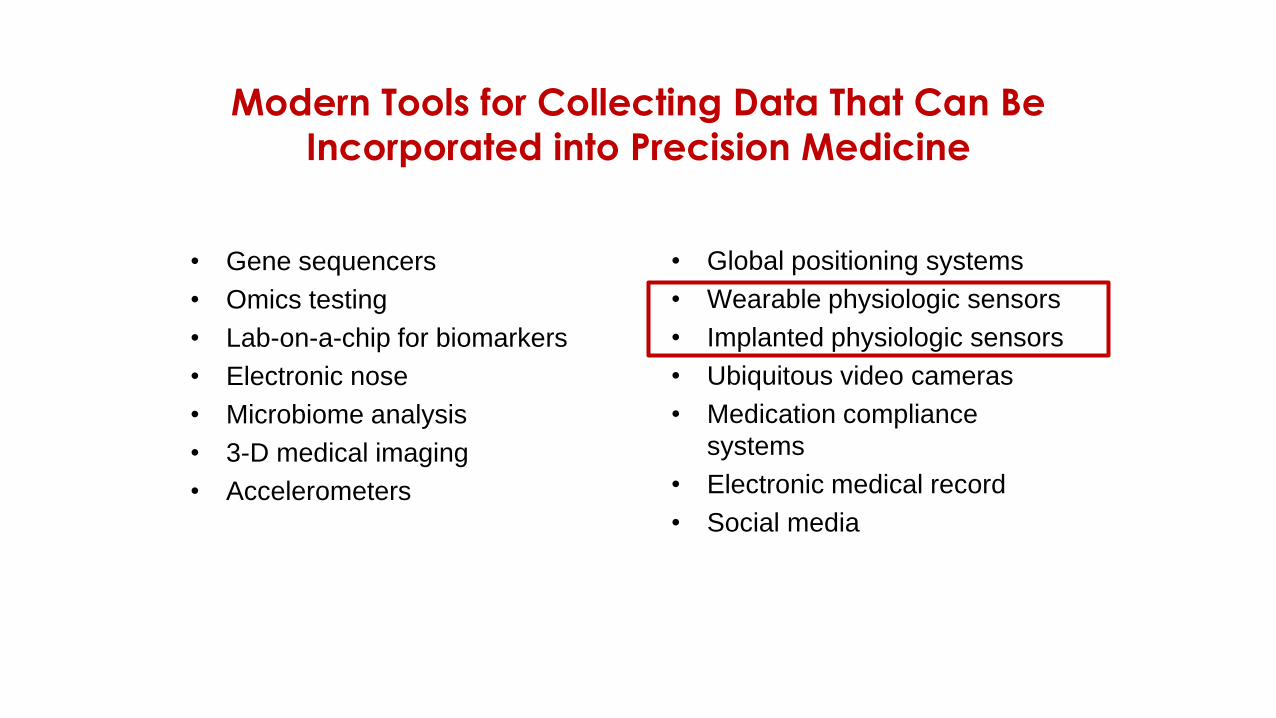
Modern Tools for Collecting Data That Can Be
Incorporated into Precision Medicine
• Gene sequencers
• Omics testing
• Lab-on-a-chip for biomarkers
• Electronic nose
• Microbiome analysis
• 3-D medical imaging
• Accelerometers
• Global positioning systems
• Wearable physiologic sensors
• Implanted physiologic sensors
• Ubiquitous video cameras
• Medication compliance
systems
• Electronic medical record
• Social media
Klonoff DC, J Diabetes Sci Technol 2015
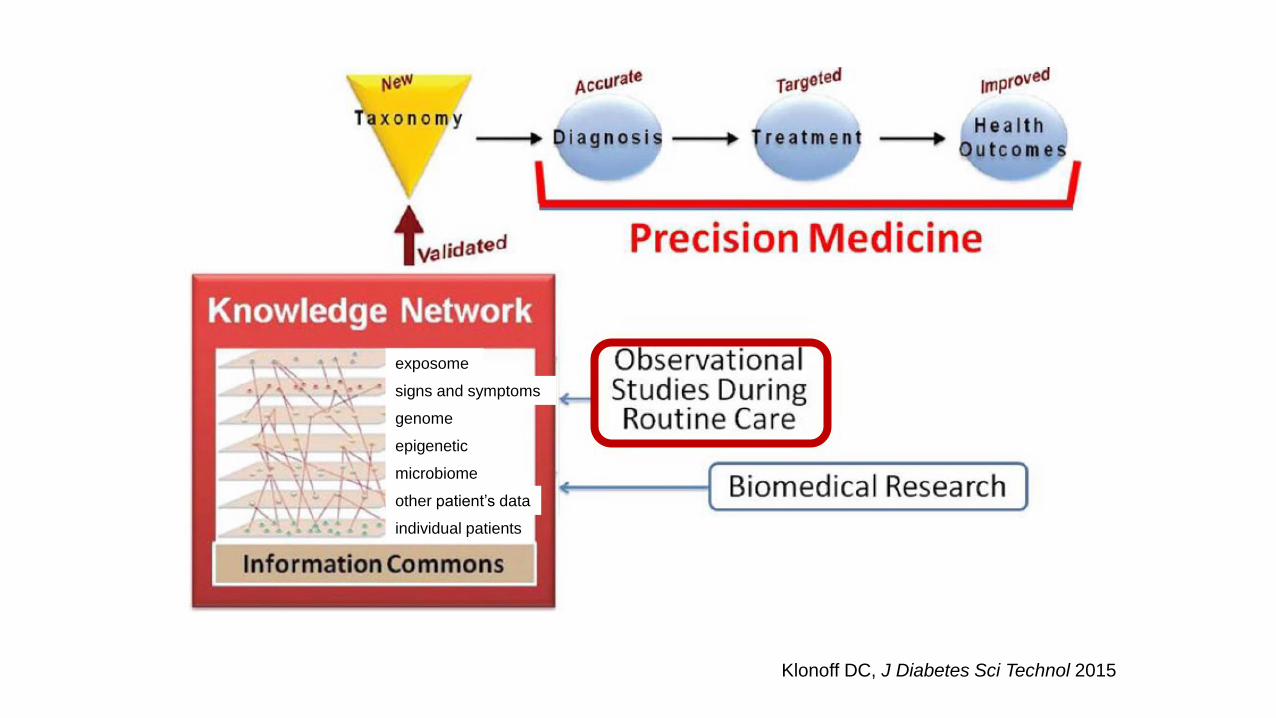
exposome
signs and symptoms
genome
epigenetic
microbiome
other patient’s data
individual patients
“Each patient may become a big-data producer. The data we generate at home or in the wild will vastly exceed what we accumulate in clinical care”.“We’re trying to create these big collages of different data modalities — from the genomic to the environmental to the clinical — and link them back to the patient.”