presented by: kwavi agbeyegbe, sam ruffing, michael peterson med inf 406-dl fall 2010
TRANSCRIPT

USING CDSS FOR APPROPRIATE DOSING OF ANTIBIOTICS WITH
REDUCED RENAL FUNCTIONPresented By:
Kwavi Agbeyegbe, Sam Ruffing, Michael Peterson
MED INF 406-DL FALL 2010

Identify the Problem
Antibiotics are one of the most widely used classes of drugs in hospitals and account for one-third of total pharmacy cost.
Suboptimal dosing decisions are the most common reason for inappropriate antibiotic prescribing in the hospital setting, with the majority of errors occurring in the prescribing phase.
It is believed 25-50% of all prescribed antibiotics are inappropriate in respect of drug choice, dose administered or duration of treatment (Ena,1998)

Identify the Problem
Antibiotics which are eliminated from the human body by renal excretion, are inappropriately dosed in an estimated 18-26% of patients (Nicholas,2009).
The estimated prevalence of impaired renal function (GFR<60 ml/min/1.73m2) is 13% for men and 36% for women over the age of 65.
Dosing of renal cleared antibiotics is very complex, it requires complicated dosing algorithms and pharmacokinetic monitoring.

Antibiotics
Antibiotics are eliminated from our bodies by basically two routes.
* Renal elimination * Metabolized by the liver Antibiotics can be cleared by one route, both
routes, or any proportion of either route. Our CDSS will focus on antibiotics that
required a reduction in dosage or kinetic monitoring when renal function is diminished.
Examples: Quinolones , Aminoglycosides and Vancomycin.

Renal Function
Renal Function Decreasing as patients get older (COOK, 2007)
Different Calculation Methods: Glomular Filtration Rate (GFR), Creatinine Clearance (CrCl)

Negative Effects
Adverse Drug Events: Nephrotoxicity, Ototoxicity, Cardiotoxicity….
Economic Cost: Increased length of stay, higher cost for monitoring, increased medication costs.
Societal Cost: Increased Insurance cost, Loss of antibiotic efficacy, lower quality of care.

Antibiotic Dosing Model
Our CDSS Antibiotic dosing model requires data from multiple sources: ADT, Lab, Pharmacy, EMR, Clinics
Baseline data required: Age, sex, height, allergies, diagnosis, infection site, current drug therapy, WBC with diff, albumin.
Lab work-up: Scr, BUN, cultures Loading dose based on ideal body weight,
and dosing interval determined by renal function.

Monitoring Parameters
Trough and Peak levels at steady state Measuring SrCr every two days or every
day in unstable renal function Weigh patient every two to seven days Measure and monitor urine output daily When the patient is on an aminoglycoside
baseline and weekly audiograms, and check for tinnitus or vertigo daily.
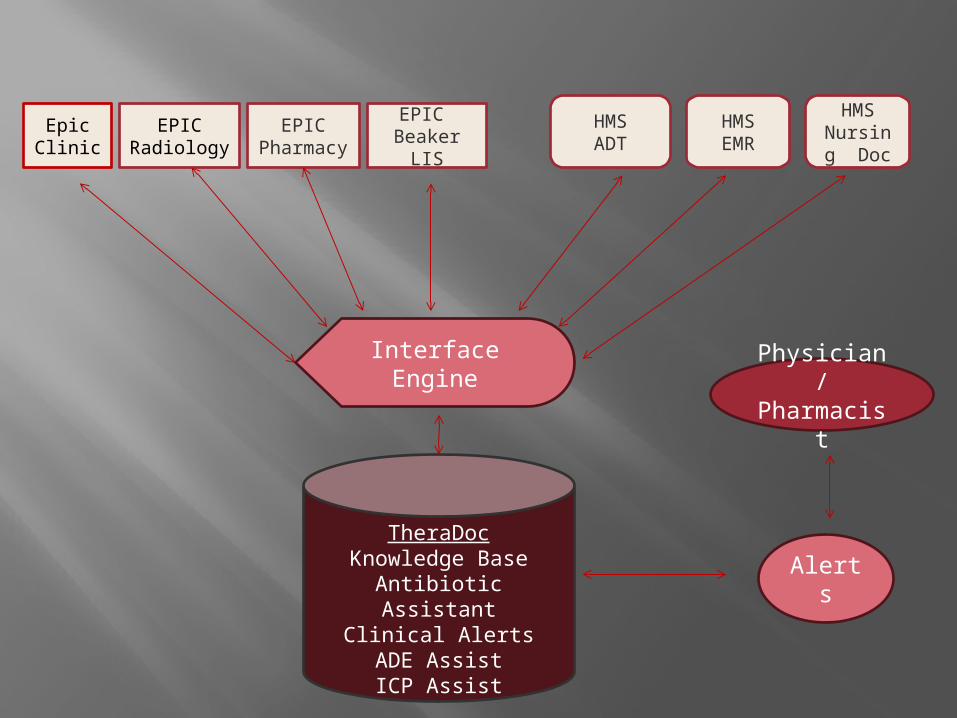
EPIC Pharmac
y
EPIC Beaker LIS
HMSADT
HMS EMR
HMS Nursing
Doc
EPICRadiology
TheraDocKnowledge Base
Antibiotic AssistantClinical Alerts
ADE AssistICP Assist
Interface Engine
Alerts
Physician/Pharmacist
EpicClinic

EPIC uses HL7, ANSI X 12, XML
HMS is ODBCcompliant
TheraDoc-HL7, LOINC, NHSN, PHIN, MS,
SNOMED-CT and Rx Norm
CCOW
Real time interface

1. Physician selects an Antibiotic-Initial Order
2. All known needed data elements are pulled to one screen:•Allergies•Current/Past Renal Dx•Serum Creatinine, BUN, WBC w/diff and albumin results•Demographics•Radiology results-Chest X-rays findings•Pathology findings if relevant
3. Recommendations includeAntibiotic dosage/ selectionPeak / trough levels orderedRepeat BUN/Creatinine ordered
4. Physician selects agree/change
If order selection is changed drop down box with reasons will require completion
Once order is completed:
Peak and trough dates and times will be ordered
eMAR will populate Antibiotic Selections with peak and trough draw times
To : Physician and PharmacistMicro results on culture and sensitivity with new recommendations for Antibiotic choice, if appropriate
To: Nurses/phlebotomistAlerts for peak and trough times for drawing
To: Physicians Alerts from nursing documentation/Lab that may signal signs and symptoms of toxicity
Alerts

Evaluation
To implement a knowledge-based clinical decision support system for clinical information systems, it is crucial to verify and validate the knowledge base. (Kim, Kim, Cho, Lee, & Kim, 2010).

Evaluation
The requirements of the CDSS should meet the user requirements and also satisfy all the regulatory specifications.
Methods and techniques used in the Verification and Validation should be designed carefully with verification taking place before validation.
Software validations should not be left to the closing phases of the project.

Verification and Validation
Building the system right
Building the right system
Verification
Requirements Specification gathering
Functional design
Internal systems design
Code verification

Verification
Walk through
Buddy Checks
Inspection

ValidationTesting Strategy
Black box testing
Equivalence partitioning testing

Validation
User Acceptance Testing/Validation
Functional Testing/Validation
Integration Testing/Validation
Code Validation

Requirement Specification gathering
Requirement Specification Verification
Coding
User Acceptance Testing (UAT)
Validation
Functional Design
Functional Design Verification
Integration Testing
Validation
Functional Testing
Validation
Internal System Design Specification
Internal System Design Specification Verification
Code Verification Code Validation
Verify
Verify
Verify
Verification levels with corresponding Validation tests.
Verify

However, the FDA is realistic enough to recognize that a developer cannot test forever. Under-testing vs. Over-testing
Under-testing vs Over-testing

Benefits of Verification and Validation
Benefits of Verification and Validation(Chojnowski, 2008)

System limitations
Physician autonomy
Computer literacy
IT Support Availability
Impact on workflow
System limitations
Training
Buy-in from clinicians and administrative staff
Lack of standards for CDSS development

Future Extensions
Study the prescribing behavior and structure of errors when physicians override the default value.
Open source Standard for development of CDSS
Post-implementation review

Conclusion Stakeholders have to be informed and
involvedprior, during and after implementation.
CDSS is more effective when combined with CPOE.
CDSS System review concludes aided drug dosing provides an overall benefit.
To increase adoption, CDSS should be integrated into existing workflow.