presented by: ragunathan kanagaretnam ceo quality ... · pdf file1. checklist, 2. structured...
TRANSCRIPT
Presented by:
RAGUnathan Kanagaretnam CEO
Quality Associates, Malaysia
RANJINI Ragunathan Perioperative Fellow, Process Excellence Hospital For Special Surgery New York
1
19 Feb 2012
No matter how competent healthcare professionals are, errors will occur.
The question then is: What can we do?

2
THE AVIATION CRASH OF THE CENTURY:
The beginning of CREW RESOURCE MANAGEMENT (CRM)
Tenerife (Canary
Islands) 03/27/1977
two fully loaded
Boeing 747 jumbo jets
collided
on a fog-blanketed
runway – visibility
700m
claiming the lives of
583 people.
http://www.youtube.com/watch?v=9Zfw3w3FRMA&feature=related

3
were totally SUBORDINATE in their interaction with the Captain
were not encouraged to QUESTION the Captain freely
A. The First Officer & Flight Engineer:
were clearly INTIMIDATED by the Captain’s
overbearing and authoritative style
Q. Why did the First Officer and the Flight Engineer not assert their concerns,
even in the face of impending disaster?
Q. Why did the Captain not seek input from the other professional crew members
(First Officer & Flight Engineer) when making decisions?
Simple answer is:

4
A REGRETFUL INTROSPECTION – 1976 Pre CRM
Chief
Flight Engineer
Chief Pilot
Training
Chief Pilot
Development
Acceptance Flight Testing of MALAYSIA AIRLINES 1st DC-10-30
LONG BEACH, CALIFORNIA, 1976
TECHNICALLY COMPETENT but DEFICIENT in COCKPIT TEAMWORK SKILLS
Oh Yes! An Abhorrent Culture
A shameful Past

Post Tenerife: An Intense Examination on Causes of Aviation Accidents
60-80 % of aviation accidents (Shappell & Wiegmann,1996)
were caused by:
5
and not
TECHNICAL INCOMPETENCY
A STARTLING REVELATION THAT
Fallibility of Decision Makers
6
Humans are imperfect organisms and will necessarily make errors,
particularly under conditions of overload, stress and fatigue. Thus:
That Lead to the Realization that:

7
The Federal Aviation Administration Defines Crew Resource Management
(FAA, 2009) As:
The effective use of all the resources available to crew members,
including each other, to achieve a safe and efficient flight.

8
1. recognizing the human factors that cause errors
2. recognizing that in complex, high-risk settings, teams rather than
individuals are the most effective operating units
3. instilling practices that use all available resources to reduce the adverse impacts of those
human factors
CRM trains crew team members from multiple disciplines to
work together in a coordinated, safety-conscious environment
by (Marshall, 2009):

The Result of Using CRM in Aviation
AVIATION ACCIDENT TRENDS
9 CRM has helped the aviation industry to be safer in all aspects of the industry.
According to the National Transportation Safety Board, the fatality risk fell to 68 per billion
fliers this decade, less than half the risk in the 1990s. Since 2002, the risk fell to 19 per
billion, an 86 percent drop since the 1990s. This improvement can be partially attributed to
CRM and the Federal Aviation Administration requires that all commercial airline and
military pilots undergo CRM training.
10

A Confidence Wrecking 1999 Institute of Medicine (IOM) study
‘To Err is Human’ reported:
44,000—98,000 annual deaths occur as a result of medical errors.
Medical errors are the leading cause, followed by surgical
mistakes and complications.
More Americans die from medical errors than from breast cancer,
AIDS, or car accidents.
7% of hospital patients experience a serious medication error.
11

12
Ref.: Annual Report on Quality & Safety, Joint Commission, 2007
Root Causes of Sentinel Events 1995 – 2005, By the Joint Commission
66% Communication Failures:
The leading causes of inadvertent
patient harm (Leonard et al, 2004)
Communication is essential to workplace efficiency and for the delivery of
high quality and safe work.
Communication and Patient Safety
and difficulties of transmitting information within and between large
organisations (e.g. safety alerts).
status effects inhibiting junior staff from speaking up;
Communication failures relate
to the following:
shift or patient handovers;
the quality of information
recorded in patient files,
case notes and incident reports;

CRM Programs for Healthcare is recommended
by these and other healthcare agencies
Australian Institute
of Health Innovation
Accreditation Council for
Graduate Medical Education

14
“As a conclusion it is clear that this process [CRM] would reduce errors, cut the
costs of litigation, reduce wasted capacity and reduce the patients stay in
hospital” (East Cheshire Hospitals NHS Trust, 2002).
CRM success evidences found in peer-reviewed healthcare publications.
A 50% reduction in surgical counts errors (Rivers, Diane & Nixon, 2003)
Clinical error rate reduction from 30% to 4.4% (Morey, et al., 2002)
Teamwork and communication skills, more than previous surgical experience,
determine how quickly medical personnel develop expertise with new technology,
e.g. robotics for minimally invasive cardiac surgery, (Pisano, 2001).

15

16
Aviation and Health Care Have Much in Common
5. Both are entrusted with the safety of others
6. In both human factors are cause of the majority of errors and accidents
1. Both are extremely complex industries
2. Both require highly skilled and trained crew members
4. Both need to function ably under stressful conditions
3. Both should work effectively as a team to reduce errors
17
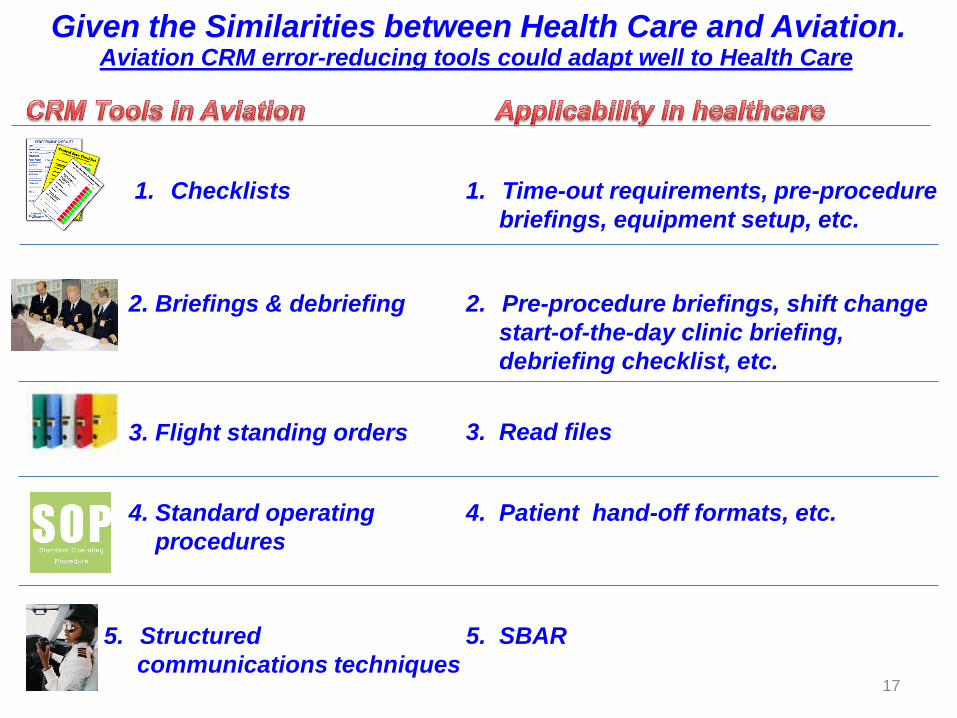
1. Checklists
2. Briefings & debriefing 2. Pre-procedure briefings, shift change
start-of-the-day clinic briefing,
debriefing checklist, etc.
3. Flight standing orders
4. Standard operating
procedures
5. Structured
communications techniques
3. Read files
4. Patient hand-off formats, etc.
5. SBAR
1. Time-out requirements, pre-procedure
briefings, equipment setup, etc.
Given the Similarities between Health Care and Aviation. Aviation CRM error-reducing tools could adapt well to Health Care

The Fundamentals of Health Care CRM Philosophy
18
1. checklist,
2. structured communication techniques, SBAR
3. briefing - WHO surgery checklist
4. debrief,
5. handoff, cross-monitoring, feedback, etc.
1. leadership,
2. mutual support,
3. situation monitoring, and
4. communication.
These CRM tools to be
discussed next.

19

20
Example of a ‘Normal Landing’ ‘Do & Read’ Checklist in Aviation
The UBIQUITIOUS CHECKLIST How things get done in Aviation
The ‘Do & Read’ Checklist
Captain: “Before Landing Checklist”
Captain: “Checked” (Double checking that all flaps are in the full landing configuration)
Flight Engineer: “ Roger, Flaps 30, 30, Green light” (This statement confirms he has the command to execute the Before Landing Checklist)
Co-Pilot: “Flaps, 30, 30 Green light” (Confirms the flap handle is at the 300 detent, the flap indicator gauge shows 300 on
both the inboard and outboard flaps, and the cockpit light indicating that all the flaps are
down is illuminated)

21
The consequences of missing a single item can be tragic
Example of an Emergency Checklist
Engine Fire or Severe Damage
‘Read and Do’ Checklist
The UBIQUITIOUS CHECKLIST How things get done in Aviation
The ‘Read & Do’ Checklist

22
In 2001 a critical-care specialist at Johns Hopkins Hospital named Peter Pronovost decided to give “Checklist” a try. He designed a checklist to tackle just one problem: LINE INFECTIONS
Over a 27 month period only two line infections occurred.
In 2001 a critical-care specialist at Johns Hopkins Hospital named Peter Pronovost decided to give “Checklist” a try. He designed a checklist to tackle just one problem: LINE INFECTIONS
Central Line Insertion
Checklist in Healthcare

23

The Tenerife crash in 1977 changed aviation communication
As a result of this accident an increased emphasis was
placed on using standardized phraseology in ATC
communication.
KLM Copilot: “We are now at take-off”
(he meant on the take run)
Air Traffic Control understood it to mean that KLM
was static at take-off position and so replied: “OK”.
For example:
“Take-off” was changed to “Taxi into position and hold”
“Take-off” is only used when actual take-off clearance is given.
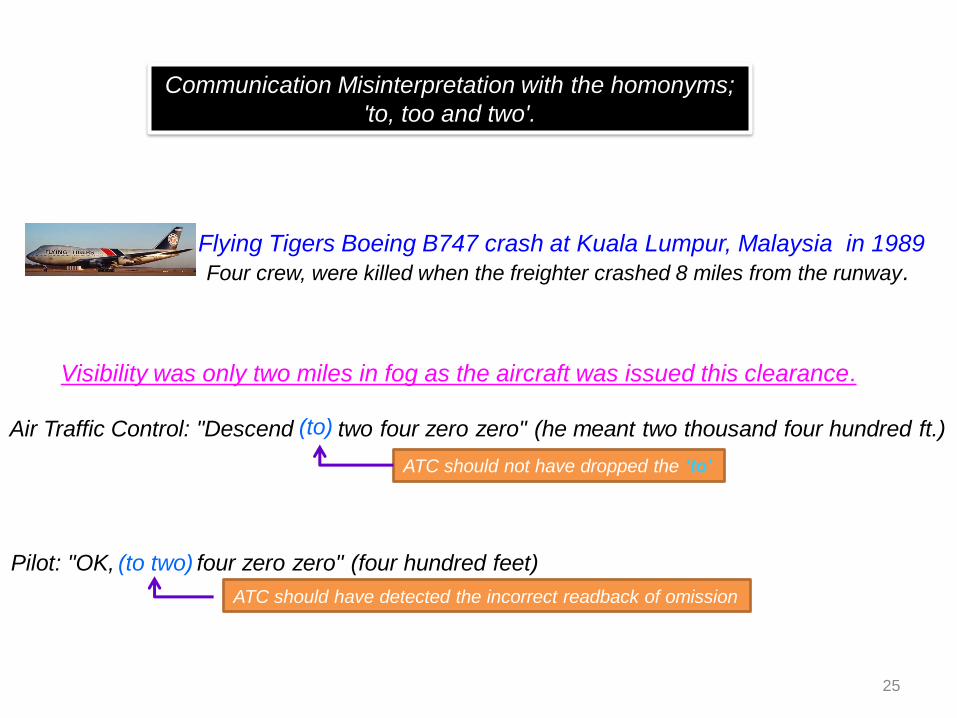
25
Flying Tigers Boeing B747 crash at Kuala Lumpur, Malaysia in 1989
Four crew, were killed when the freighter crashed 8 miles from the runway.
Air Traffic Control: "Descend two four zero zero" (he meant two thousand four hundred ft.)
Visibility was only two miles in fog as the aircraft was issued this clearance.
ATC should not have dropped the ‘to’
(to)
Pilot: "OK, four zero zero" (four hundred feet)
ATC should have detected the incorrect readback of omission
(to two)
Communication Misinterpretation with the homonyms;
'to, too and two'.

CRM Based Approach: Communication Model
for Inter-Professional Communication Among Clinicians
Must understand
the motivation
of the Receiver.
Nurses – descriptive
Doctors - factual
Message Information sender wants
to convey
Feedback Sender should confirm
message has been received
Receiver interprets
the message
and responds
For CRM based
approach
repetition
& reinforcement
is essential.
Repeat The Medium
2
6
Hierarchy
Sex
Knowledge Skills
Past experiences
Paradigms, etc.
Assumptions
Not sharing information
Poor documentation
Confusion
Work overload
Too busy
Fatigue
Stress
Conflict

Example of aviation communication based on the CRM
Communication Model: Clear, concise and standardized
Station calling Vegas Ground
say again your callsign
Vegas Ground, BIGJET 347,
radio check 118.3
BIGJET 347, Vegas Ground,
readability 5
Ground, BIGJET 347, stand 24,
information bravo, QNH 1011,
request start up
BIGJET 347, start up approved
Flight Start Up Approval
Vegas Ground, BIGJET 347,
radio check 118.3
Reference: CAP 413, Radiotelephony Manual, Edition 20
1. PRECISE COMMUNICATION
(Communication skill)
2. STANDARD TERMINOLOGY
(Safety tool)
27

28
What do you see?
1. A young woman
2. An old woman
Mental Models
People act according to their “mental models” ,i.e.
different conclusions of the same subject.
“Mental models are deeply ingrained assumptions, generalizations, or … images that influence how we
understand the world and how we take action.” Peter Senge – The Fifth Discipline

“Mental models are deeply ingrained assumptions, generalizations, or … images that influence how we
understand the world and how we take action.” Peter Senge – The Fifth Discipline
What are Mental Models? C
an a
lso b
e b
etw
een
Docto
r to
Docto
r O
r N
urs
e t
o N
urs
e
“Two people with different mental models
can observe the same event and describe it
differently.” Ragunathan K. Externalizing Tacit Knowledge For Training
Effectiveness: A Cognitive Model Of Knowledge Conversion.
PhD Thesis, Kuala Lumpur, July 2002.
29
Nurse
Vision of
The
World
Doctor
Vision of
The
World
Joint Commission 2007
Humans tend to
consider that their
vision of the world is
correct whenever
events happen in
accordance with their
expectations.
The Joint Commission notes that in 66% of
sentinel events, communication is a
contributing factor in medical errors.

30
SBAR is a tool to share clinicians MENTAL
MODELS of a patient’s clinical condition.
State what you think is the problem. Provide patient
A - Assessment
State your name and briefly the patient related issue you
are concerned about
Describe the
S – Situation
State what you like to do to correct the problem. Make or ask for
R - Recommendation
Describe the clinical background or context. Provide the
B – Background
SBAR enhances the effectiveness of communication through an established structure that;
improves safety, clarity, efficiency, and respect for the message sender and receiver.

31
Nurses like the SBAR tool, as it gives them the
“authority” to make a recommendation & their
contribution is valued.
Doctors are delighted to get straight to the point
facts rather than the usual descriptive version
said to be typical of nurses.
32
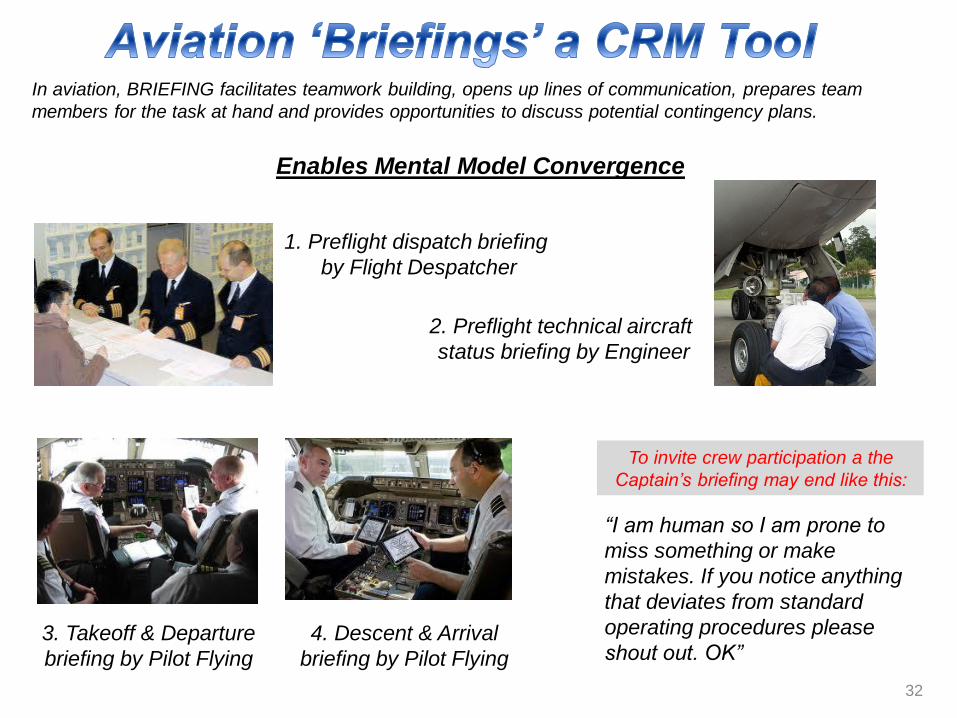
In aviation, BRIEFING facilitates teamwork building, opens up lines of communication, prepares team
members for the task at hand and provides opportunities to discuss potential contingency plans.
Enables Mental Model Convergence
1. Preflight dispatch briefing
by Flight Despatcher
2. Preflight technical aircraft
status briefing by Engineer
3. Takeoff & Departure
briefing by Pilot Flying
4. Descent & Arrival
briefing by Pilot Flying
To invite crew participation a the
Captain’s briefing may end like this:
“I am human so I am prone to
miss something or make
mistakes. If you notice anything
that deviates from standard
operating procedures please
shout out. OK”

33
0
10
20
30
40
50
60
70
80
1 2 3 4 5
%
Characterizing Teamwork in the OR
26%
73%
39%
28%
10%
Anesthesiologists Surgical
Nurses
Anesthesia
Nurses
Anesthesia
Residents
Attending
Surgeons
Survey Question: “Rate the quality of teamwork and communication or
cooperation with consultant surgeons”
Communication & Teamwork in Medicine: A Research Findings
(Sexton, Thomas & Helmreich, 2000)
Although attending surgeons perceive that teamwork in their operating rooms
is quite good, the rest of the team members disagree, proving that one should
never ask the leader about the quality of teamwork!
Can you imagine this happening in
a flight cockpit.

34
Surgical Checklist by the World Health Organization (WHO) Promotes effective teamwork and prevents wrong site, wrong procedure
and wrong person surgery from occurring.
A 2007-2008 WHO study on the use of the Surgical Safety Checklist worldwide
confirms that at least half a million deaths per year could be prevented.

35
.
Before skin incision, the checklist coordinator should ask the surgeon if
imaging is needed for the case. If so, the coordinator should verbally confirm
that the essential imaging is in the room and prominently displayed for use
during the operation.
The checklist coordinator should ask each person in the room to introduce
him or herself by name and role.
The checklist co-ordinator will ask everyone in the operating room to confirm
the name of the patient, the surgery to be performed and the site of surgery
The checklist co-ordinator will ask out loud whether prophylactic antibiotics
were given during the previous 60 minutes.
Effective team communication is a critical component of safe surgery,
efficient teamwork and the prevention of major complications. To ensure
communication of critical patient issues, the checklist coordinator leads a
swift discussion among the surgeon, anaesthesia staff and nursing staff of
critical dangers and operative plans.
A Pre - Surgery Briefing: A ‘Page’ from Aviation CRM (WHO, 2009)

36

37
Loss of authority – concern of physicians.
(Goal of CRM is to make better decisions … enhances the physicians authority)
What if I speak up and get yelled at?
(The organization must not accept hostility and if it happens it should deal with it.)
I do not buy CRM and I am not going to do it.
(Patient safety is not optional.)
CRM, not in an emergency.
(Errors are more likely to occur in emergencies when
departing from well-trained standard procedures)

38
Marshall, David. Crew Resource Management: From Patient Safety to High Reliability.
Colorado: Safer Healthcare Partners, 2009. p. 19
Federal Aviation Administration, Department of Transportation, Part 121, Subpart Y, Section 121-907. 2009
Rivers R.M., Diane S. & Nixon B. Using aviation safety measures to enhance patient outcomes. Association of
PeriOperative Registered Nurses (AORN) 2003; 77:158.
Morey J.C., et al. Error reduction and performance improvement in the emergency department through
formal teamwork training: Evaluation results of the MedTeams project. Health Service Results 2002; 37:1553.
Pisano G.P. et al. Organizational differences in rates of learning: Evidence from the adoption of minimally invasive
cardiac surgery. Management Science 47, No.6 (June 2001):752.
East Cheshire Hospitals NHS Trust. Error Prevention Programme Conclusion & Recommendations Report, 22/10/02.
Gaffney F.A., Harden S.W., Seddon R. Crew Resource Management: The Flight Plan for Lasting Change in Patient Safety.
HCPro, Inc.: Marblehead. 2005.
Sexton, Thomas & Helmreich . Error, Stress and Teamwork in Medicine and Aviation: Cross Sectional Surveys.
BMJ Volume 320. 2000.
References
World Health Organisation. Implementation Manual WHO Surgical Safety Checklist 2009: Safe Surgery Saves Lives.
Geneva: WHO, 2009. Print.
Leonard, M., Graham, S. & Bonacum, D. (2004) The human factor: the critical importance of effective teamwork and
communication in providing safe care. Quality and Safety in Health Care, 13, 85-90.
Shappell, S. & Wiegmann, D. (1996). U.S. naval aviation mishaps 1977-92: Differences between single- and dual-
piloted aircraft. Aviation, Space, and Environmental Medicine, 67(1), 65-9.

Ragunathan Kanagaretnam, PhD
Ranjini Ragunathan, BS (ISyE)
39
Conclusion:
If humans are involved, error is inevitable.
Health Care! It Is Time To File Your Aviation
CRM Flight Plan For Patient Safety