pressure regulated volume control (prvc)
DESCRIPTION
PRVC mode on the Servo-i ventilator.TRANSCRIPT

PRESSURE REGULATED
VOLUME CONTROL (PRVC)
Charles S. Williams RRT, AE-C
PRVC
First introduced on the Servo 300 ventilator. Is now available
on the Servo-I ventilator.
PRVC is defined as pressure controlled ventilation with a
volume target. (Volume-targeted pressure control).
It is considered a form of Dual-Mode ventilation.
PRVC combines the advantages of both volume-controlled
(VC) and pressure-controlled (PC) ventilation.
Intro

PRVC
PRVC will attempt to deliver the desired set tidal volume using
the lowest possible pressure.
Use clinically as you would “standard” Volume Control (VC)
Similar modes on other ventilators include:
1. AutoFlow (Drager Evita),
2. Adaptive Support Ventilation (Hamilton Galileo)
3. Volume Ventilation Plus (Puritan Bennett 840)
Intro
Volume-Control Ventilation (VCV)
Assist-Control Ventilation
Set mandatory (min) rate
Every breath delivered, either ventilator initiated (control)
or patient initiated (assist), are identical.
Peak inspiratory pressure (PIP) will vary depending on
lung mechanics. (compliance and airway resistance)
Volume Control

Volume-Control Ventilation (VCV)
Shown here is standard Volume Control mode.
The set tidal volume is 500.
Volume Control
*Screenshots have been modified for illustration purposes

Volume-Control Ventilation (VCV)
In VC, flow remains constant during inspiration.
Flowrate is normally a set parameter in VC.
*Screenshots have been modified for illustration purposes
Volume Control

Volume-Control Ventilation (VCV)
Pressure will vary depending on lung compliance, airway resistance, etc.
*Screenshots have been modified for illustration purposes
Volume Control

PRVC
When switching to PRVC mode, the ventilator first delivers a volume “test”
breath along with an inspiratory “hold” maneuver.
This is also done anytime ventilation has been interrupted, (opening the vent
circuit, suctioning, etc.)
Inspiratory Hold
PRVC
*Screenshots have been modified for illustration purposes
PRVC
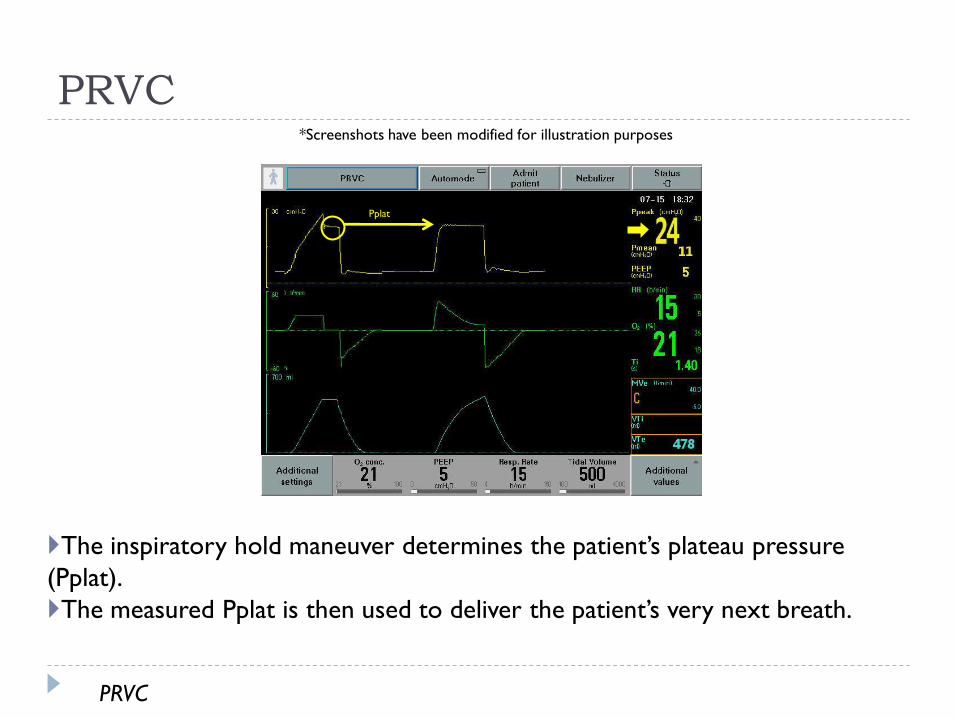
The inspiratory hold maneuver determines the patient’s plateau pressure
(Pplat).
The measured Pplat is then used to deliver the patient’s very next breath.
PRVC
*Screenshots have been modified for illustration purposes
Pplat
PRVC
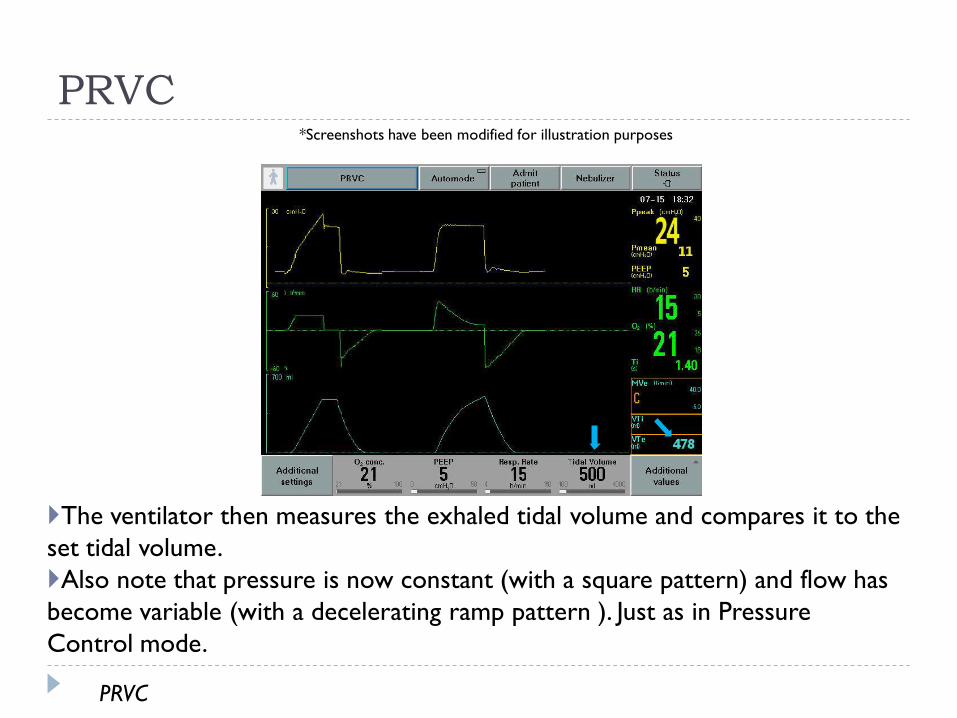
The ventilator then measures the exhaled tidal volume and compares it to the
set tidal volume.
Also note that pressure is now constant (with a square pattern) and flow has
become variable (with a decelerating ramp pattern ). Just as in Pressure
Control mode.
*Screenshots have been modified for illustration purposes
PRVC
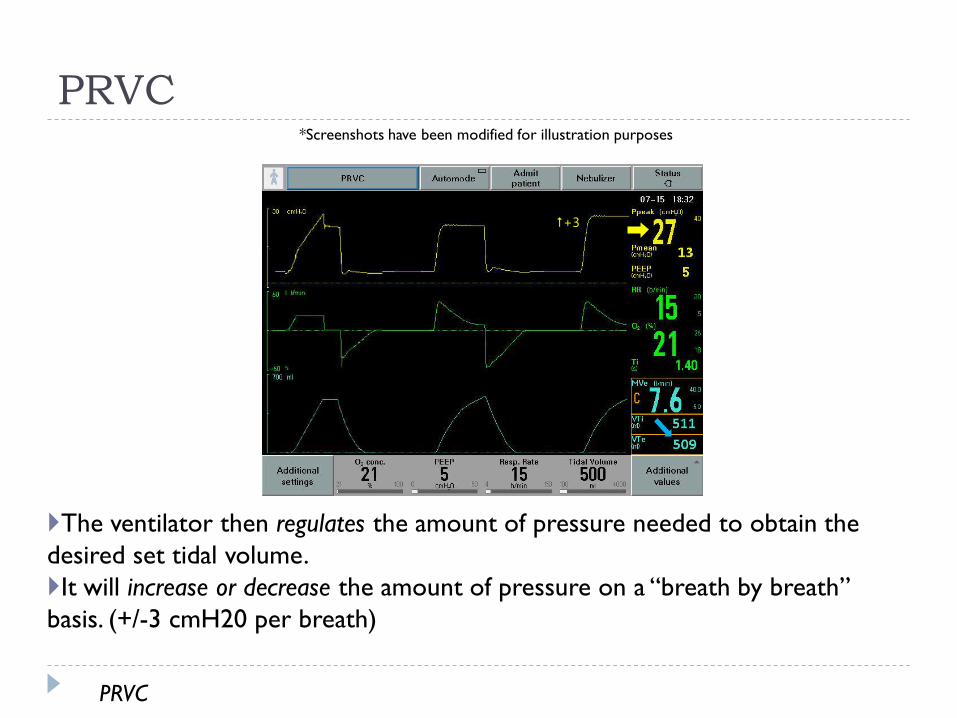
PRVC
The ventilator then regulates the amount of pressure needed to obtain the
desired set tidal volume.
It will increase or decrease the amount of pressure on a “breath by breath”
basis. (+/-3 cmH20 per breath)
+3
PRVC
*Screenshots have been modified for illustration purposes

PRVC
MeasureTidal Volume
Compare to
set
Tidal Volume
Give same
Inspiratory Pressure
Increase
Inspiratory
Pressure
Less
Equal
More
Decrease
Inspiratory
Pressure
Test Breath
PRVC Flowchart

PRVC
“Guarantees” delivery of desired tidal volume.
Minimizes risks of barotrauma due to high peak
pressures.
Decelerating flow pattern may provide better distribution
of ventilation and oxygenation.
Can better meet patients inspiratory flow demands.
Advantages:
Advantages

PRVC
The ventilator may potentially increase pressures to
dangerously high levels as it attempts to maintain the
desired tidal volume.
1) The maximum delivered pressure is limited to 5cmH2O
below the set High Pressure alarm limit.
2) High Pressure alarm limit should be set at 35-40 cmH20.
Disadvantages:
Disadvantages

PRVC
Pressure delivered is dependant on the tidal volume
achieved from the previous breath.
If the patient intermittently makes a significant inspiratory
effort, it can result in variable tidal volumes than can be
higher or lower than the setting.
Disadvantages:
Disadvantages
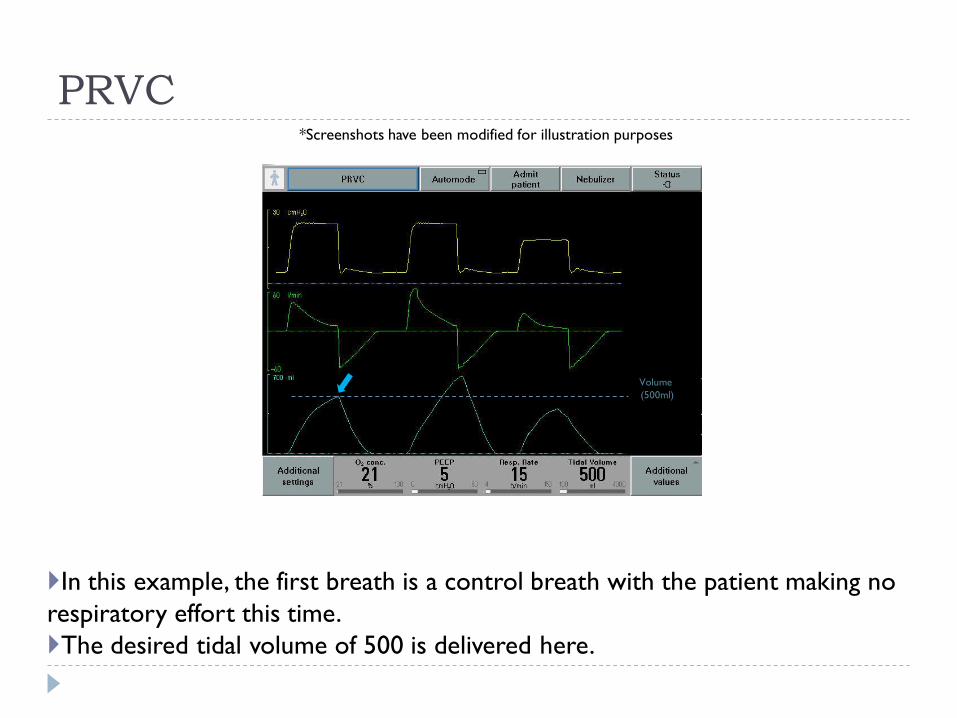
PRVC
In this example, the first breath is a control breath with the patient making no
respiratory effort this time.
The desired tidal volume of 500 is delivered here.
*Screenshots have been modified for illustration purposes
Volume
(500ml)

PRVC
The second breath is triggered by the patient who made a significant
inspiratory effort.
Although, PIP has remained the same as the first breath, a higher tidal volume
results because of higher transpulmonary pressure.
*Screenshots have been modified for illustration purposes
Volume
(500ml)

PRVC
The ventilator will then reduce the amount of pressure needed for the next
breath.
The patient doesn’t make any inspiratory effort with this breath, the result is a
tidal volume that is lower than the set tidal volume.
*Screenshots have been modified for illustration purposes
Volume
(500ml)
PRVC
Automode/Volume Support
For patients that are making intermittent inspiratory
efforts, or breathing spontaneously, switching to
Automode may be better.
In Automode, the ventilator will automatically switch
between PRVC and Volume Support mode.
PRVC breaths when there is no patient effort, and VS
breaths with patient effort).
Automode

PRVC
Automode/Volume Support
Volume Support (VS) mode works in the same way as
PRVC.
VS automatically adjusts the level of pressure support
needed to achieve a targeted tidal volume, based on
the amount of inspiratory effort given by the patient.
Volume Support is basically, Pressure Support that
guarantees a set tidal volume.
Volume Support

Sources:
PRVC Dr. Charles Gomersall, Dept of Anaesthesia & Intensive Care,
The Chinese University of Hong Kong,
Prince of Wales Hospital
Golden Moments In Mechanical VentilationMaqet, INC.
Servo-I: Modes of Ventilation, Pocket GuideMaqet, INC.
Evidence Base for Newer Modes of Mechanical Ventilation Charles B. Spearman, MSEd, RRT, FAARC
Assistant Professor
Respiratory Care Programs
Department of Cardiopulmonary Sciences
Loma Linda University