prevalence and clinicopathological...
TRANSCRIPT

Prevalence and Clinicopathological Characteristics ofIslet Amyloid in Chinese Patients With Type 2 DiabetesHai-Lu Zhao,
1Fernand M.M. Lai,
2Peter C.Y. Tong,
1Ding-Rong Zhong,
3Di Yang,
4Brian Tomlinson,
1
and Juliana C.N. Chan1
Islet amyloid has been suggested to be an important linkbetween insulin resistance and �-cell dysfunction intype 2 diabetes. To investigate the prevalence andclinicopathological characteristics of islet amyloid, weexamined consecutive autopsies of 235 Chinese pa-tients with type 2 diabetes and 533 nondiabetic sub-jects. Islet amyloid deposits were identified usingCongo red staining and quantitated by image analysis.We found that 3.0% of the nondiabetic subjects versus39.6% of the diabetic patients displayed islet amyloid(P < 0.001). In diabetic patients, the amyloid depositsoccupied a mean islet area of 36.2%, which was posi-tively associated with BMI, blood pressure, and glyce-mic control. Pancreatic fibrosis and fat infiltration weremore frequently found in diabetic patients with isletamyloid than those without islet amyloid, whereas pan-creatic arteriosclerosis was identified in all diabeticpatients. These findings suggest that islet amyloid de-posits reflect greater insulin resistance and islet failurein a subgroup of type 2 diabetic patients. Islet failuremay also have been exacerbated by fat infiltration,fibrosis, and arteriosclerosis. Optimal blood pressureand metabolic control may reduce these pathologicalchanges and help preserve islet cell mass. Diabetes 52:2759–2766, 2003
Type 2 diabetes is characterized by insulin resis-tance and progressive islet �-cell dysfunction(1,2). However, the link between insulin resis-tance and �-cell failure is unclear (2,3). Islet
amyloid has been considered by many as a pathologicalhallmark of type 2 diabetes (4,5). In diabetic monkeys, theextent of islet amyloid is proportional to the degree of lossof islet mass and insulin secretion (6). In type 2 diabeticpatients, islet amyloid is associated with severity of �-celldysfunction (7). Islet amyloid is most diffuse and abundantin type 2 diabetic patients on insulin therapy (8,9). All
these findings point to an intimate association betweenislet amyloid and �-cell dysfunction in type 2 diabetes(5,10,11).
Islet amyloid is a relatively common feature of type 2diabetes across different ethnic groups, including Cauca-sians (11–13), Pima Indians (14), Asian Indians (15), andJapanese (16), with prevalence ranging from 50 to 100%.This wide range in reported prevalence may reflect trueethnic differences or sampling heterogeneity. However,most of these autopsy studies included �100 diabeticcases and thus might not have been truly representative ofactual prevalence.
Furthermore, the clinicopathological characteristics ofislet amyloid in type 2 diabetes have seldom been docu-mented. An increase in islet amyloid deposits has beenreported in Japanese type 2 diabetic patients with longdisease duration and obesity (17). However, other autopsystudies have shown that islet amyloid developed indepen-dent of duration of diabetes over 2–40 years (11,18).Hence, the relation between islet amyloid and clinicalphenotypes of type 2 diabetes remains to be clarified.
Because not all type 2 diabetic patients harbor isletamyloid, other underlying pathologies may also contributeto �-cell failure in type 2 diabetes. Pancreatic fibrosis,chronic inflammation, and fat infiltration have been de-scribed in type 2 diabetic patients (11,18–20). However,the relation between these pathological changes and isletamyloid has not been defined. Therefore, we conducted amulticenter study of 768 consecutive autopsies to estimatethe prevalence of islet amyloid in Chinese type 2 diabeticpatients and characterize the clinicopathological featuresof islet amyloid in type 2 diabetes.
RESEARCH DESIGN AND METHODS
Case selection. Over a 6-year period (1994–1999), 5,298 consecutive autop-sies of adult Chinese subjects were performed at two medical centers inBeijing and one medical center in Hong Kong. Candidate cases were firstidentified through review of the autopsy databases in all three medicalcenters. Autopsy cases meeting the following criteria were included: 1)performance of a full autopsy within 24 h of death; 2) availability of clinicaldata on blood pressure, fasting plasma glucose, HbA1c, and fasting serumlipids (total cholesterol, triglycerides, and LDL and HDL cholesterol); and 3)availability of sufficient pancreatic tissue, with at least one representativeblock resected from the tail/body region. Cases were excluded if 1) pancreatictissue had undergone autolysis, 2) diabetes was secondary to a known causeof hyperglycemia such as Cushing’s syndrome, or 3) patients had type 1diabetes, defined by presentation with ketoacidosis, requirement of insulintherapy from disease onset, or the presence of autoimmune markers of islet�-cell.
The patients’ hospital records, including autopsy reports, were reviewed,and relevant data including BMI, glycemic and lipid measurements, and causeof death were obtained. The lipids were measured routinely using enzymaticmethods. Cut-off values used for BMI were �23.0 kg/m2 to indicate patient
From the 1Department of Medicine and Therapeutics, The Prince of WalesHospital, Chinese University of Hong Kong, Shatin, Hong Kong SAR, China;the 2Department of Anatomical and Cellular Pathology, The Prince of WalesHospital, Chinese University of Hong Kong, Shatin, Hong Kong SAR, China;the 3Department of Pathology, Chinese PLA General Hospital, Beijing, China;and 4Department of Pathology, Peking Union College Hospital, Beijing, China.
Address correspondence and reprint requests to Hai-Lu Zhao, MD, Depart-ment of Medicine and Therapeutics, The Prince of Wales Hospital, ChineseUniversity of Hong Kong, Shatin, N.T., Hong Kong. E-mail: [email protected].
Received for publication 18 March 2003 and accepted in revised form 30July 2003.
H-E, hematoxylin-eosin; IAPP, islet amyloid polypeptide; PAS, periodic acidSchiff.
© 2003 by the American Diabetes Association.
DIABETES, VOL. 52, NOVEMBER 2003 2759

was overweight and �25.0 kg/m2 to indicate obesity in Asian patients (21). Alldiabetic subjects had been treated with oral antidiabetic drugs or insulin,whereas nondiabetic subjects were identified using a fasting plasma glucose�7 mmol/l and absence of treatment with antidiabetic medications. Usingthese criteria, we selected 235 type 2 diabetic patients and 533 age- andsex-matched nondiabetic subjects with biochemical parameters and sufficientpancreatic tissues for comparison. The type 2 diabetic patients were furtherclassified as islet amyloid positive or negative based on Congo red stainingwith polarization.Tissue sampling and staining. Pancreatic tissues were taken at postmortemexamination, fixed in 10% buffered formalin, and embedded in paraffin blocks.Tissue sections (6 �m) were cut from these paraffin blocks and stained byhematoxylin-eosin (H-E), periodic acid Schiff (PAS), and Congo red.
Congo red is a reliable, practical, and sensitive technique for detecting amyloiddeposits containing islet amyloid polypeptide (IAPP) or amylin (22,23). IAPP isthe building block of islet amyloid deposits (5,10,24). Although Congo red is nota specific marker for IAPP, it is as sensitive a marker for islet amyloid as IAPPimmunolabeling (22). In this study, we identified islet amyloid using a Congo redtechnique (25), the specificity of which was further confirmed in thyroid medul-lary carcinoma, Alzheimer’s disease, and insulinoma (26). Briefly, all 6-�m thickpancreatic sections were treated with 1% sodium chloride-hydroxide solution for20 min and stained with alkaline Congo red solution for another 20 min. All theCongophilic amyloid deposits exhibited characteristic green/yellow birefringenceunder the polarizing microscope.Morphometry of islet amyloid. For each patient, representative tissue slidesfor the pancreatic tail, body, and head were examined. The severity of type 2diabetes�associated islet amyloid was assessed by the distribution, fre-quency, and degree of the amyloid deposits. The distribution described thelocalization of islet amyloid deposits in different pancreatic regions (i.e.,pancreatic head, body, and tail). The frequency of islet amyloid was defined asthe ratio of the number of amyloid-affected islets to the total number of isletsin 10 randomly selected objective fields (magnification �20). The degree ofislet amyloid was quantitated on representative Congo red�stained sectionsfrom pancreatic tail/body at an objective magnification of �20 (AutomaticNikon Integrated Biological Imaging Microscope with Digital CCD Camera;Nikon, Tokyo, Japan; MetaMorph 4.0 image acquisition program for Windows1999; Universal Imaging, Downingtown, PA). For each case, 10 fields of thesection were randomly selected. Morphometric data were expressed as theproportion of area of Congo red�positive islet amyloid to the total pancreaticislet area examined.Statistics. Data are expressed as means � SD or percent. Student’s t test wasused to compare means (Statistics Package for the Social Sciences 10.0.7 forWindows 2000; SPSS, Chicago, IL). The association between two sets ofparametric data was evaluated using the Pearson correlation coefficient.Differences in frequencies were assessed using the �2 test (GraphPad InStatversion 3.00 for Windows; GraphPad Software, San Diego, CA). A two-tailedP � 0.05 was considered significant.
RESULTS
Prevalence of islet amyloid. The prevalence of isletamyloid was higher in type 2 diabetic than in nondiabetic
subjects (39.6 vs. 3.0%; P � 0.001). Islet amyloid depositswere identified in 93 of the 235 type 2 diabetic cases and in16 of the 533 nondiabetic cases. All the 16 nondiabeticsubjects with islet amyloid were older than age 60 years.Clinical demographic data. The clinical demographicdata of the 235 type 2 diabetic patients are depicted inTable 1. The mean BMI was 23.5 � 4.9 kg/m2 and 25.5% ofthe diabetic subjects were obese (BMI �25 kg/m2) (21). Ofthe 235 diabetic patients, �80% were elderly (age 65years).
The mean age of the 533 nondiabetic patients was 71.9 �10.7 years (range 26–95 years). The male-to-female ratiowas not significantly different between the diabetic andnondiabetic subjects (1.9 vs. 1.6; P 0.3301). Hyperten-sion was noted in �60% of the type 2 diabetic andnondiabetic subjects. The three leading causes of death inthe type 2 diabetic and nondiabetic cases were cardioce-rebrovascular diseases (42.1 and 43.6%, respectively), can-cers (22.1 and 20.2%), and respiratory diseases (9.8 and11.6%). No significant differences in the major causes ofdeath were found between patients with and those withoutislet amyloid (P 0.05).Clinical characteristics of islet amyloid in type 2
diabetes. The clinical characteristics of islet amyloid intype 2 diabetes are summarized in Table 1. Patients withislet amyloid had greater mean BMI than those withoutislet amyloid (P 0.019). The prevalence of islet amyloidwas 26.5, 45.2, and 58.3% in diabetic patients with BMI�23, 23–24.9 kg/m2, and �25 kg/m2, respectively (P �0.001).
The type 2 diabetic patients with islet amyloid also hadhigher mean HbA1c levels than those without islet amyloid(P � 0.001). However, the mean fasting plasma glucoselevels were not significantly different between the twogroups (P 0.669). Compared with the type 2 diabeticpatients without islet amyloid, the diabetic patients withislet amyloid had higher mean blood pressure and preva-lence of hypertension, had a shorter duration of disease,and formed a larger proportion of male subjects (all P �0.05) (Table 1) . No differences were found in the mean ageor lipid levels between the two groups (all P 0.05).
TABLE 1Demographic characteristics of type 2 diabetic patients in relation to the presence of islet amyloid
Total patients withtype 2 diabetes
Patients withislet amyloid
Patients withoutislet amyloid P
n 235 93 142 —Age (years) 71.9 � 10.7 71.7 � 9.7 72.1 � 11.4 0.756Male:female 155:80 69:24 86:56 0.044BMI (kg/m2) 23.5 � 4.9 24.2 � 4.9 23.1 � 4.9 0.019Fasting plasma glucose (mmol/l) 12.8 � 4.8 12.6 � 4.1 12.9 � 5.2 0.669HbA1c (%) 9.6 � 2.2 11.7 � 2.3 8.6 � 2.2 �0.001Known duration of diabetes (months) 128 � 41 118 � 46 135 � 38 0.004Hypertension (%) 57.9 66.7 52.1 0.038Systolic blood pressure (mmHg) 146 � 36 149 � 29 144 � 39 0.042Diastolic blood pressure (mmHg) 78 � 17 80 � 15 77 � 19 0.039Total cholesterol (mmol/l) 4.7 � 1.1 4.8 � 0.9 4.6 � 1.2 0.070Triglyceride (mmol/l) 1.9 � 1.4 1.9 � 0.9 2.4 � 1.7 0.660LDL cholesterol (mmol/l) 2.5 � 0.4 2.6 � 0.5 2.5 � 0.3 0.133HDL cholesterol (mmol/l) 1.0 � 0.7 1.2 � 0.6 0.9 � 0.8 0.595
Data are n or means � SD.
ISLET AMYLOID IN TYPE 2 DIABETES
2760 DIABETES, VOL. 52, NOVEMBER 2003

Histopathological characteristics of islet amyloid in
type 2 diabetes. The pancreatic histopathological fea-tures associated with islet amyloid in type 2 diabetes areshown in Table 2. Islet amyloid was often accompanied bypancreatic fibrosis, fat infiltration, and arteriosclerosis(Fig. 1).
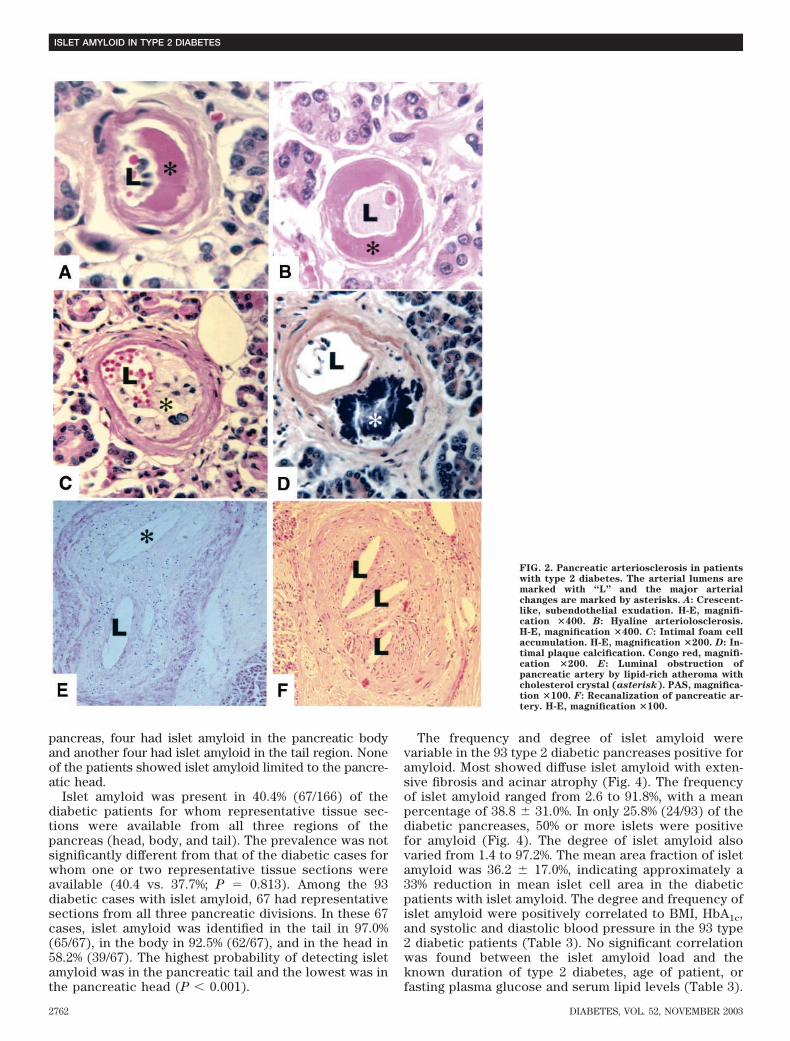
Type 2 diabetic patients displayed a full spectrum ofarteriosclerotic changes (Fig. 2). Changes in arterioles andsmall arteries, included hyaline arteriolosclerosis withsubendothelial exudation, intimal foam cell accumulation,and calcification (Fig. 2). Atherosclerotic lesions in pan-creatic large arteries showed prominent intimal lipid ac-cumulation in the form of foam macrophages andcholesterol crystals (Fig. 2). Some arteries were obliter-ated by atheroembolism (Fig. 2). The prevalence of arte-riosclerotic changes was slightly, albeit not significantly,higher in pancreases with than without islet amyloid.
Both fat infiltration and fibrosis were more common indiabetic pancreases with than without islet amyloid (all
P � 0.01) (Table 2). Pancreatic fat infiltration was detectedin 50.6% of the diabetic patients. Adipocytes were predom-inantly distributed in the exocrine acini and occasionallyfound in islets (Fig. 3). Fibrotic tissue was distributedirregularly throughout the diabetic pancreases, but exten-sive fibrosis often occurred in areas surrounding isletswith amyloid, ducts, and arteries with hyaline changes(Fig. 4). Chronic pancreatitis was found in 7.7% of thediabetic patients, in whom diffuse pancreatic fibrosis wasusually accompanied by acinar atrophy, chronic inflamma-tory infiltrates, and islet amyloid (Fig. 5).Severity of islet amyloid in type 2 diabetes. Theseverity of type 2 diabetes�associated islet amyloid wasassessed by the distribution, frequency, and degree of theamyloid deposits. The distribution of islet amyloid depos-its was not uniform; 88.6% (62/70) of the diabetic patientsshowed islet amyloid in more than one anatomical regionof the pancreas. Among the diabetic subjects with isletamyloid detected in only one anatomical region of the
FIG. 1. In patients with type 2 diabetes, isletamyloid (asterisks) is often accompanied byfat infiltration (A), fibrosis (F), and hyalinearteriolosclerosis (arrow). H-E, magnifica-tion �200.
TABLE 2Association of islet amyloid with pancreatic histopathology in type 2 diabetic patients
Totaldiabetic
pancreasesPancreases with
islet amyloidPancreases without
islet amyloid P
n 235 93 142 —Arteriosclerosis
Hyaline arteriolosclerosis 100 100 100 —Pancreatic atherosclerosis 34.0 40.9 29.6 0.077Arterial calcification 31.9 31.2 32.3 0.959Atheroembolism 13.2 12.9 13.4 0.927
Pancreatic fat infiltration 50.6 62.4 43.0 0.005Pancreatic fibrosis 57.9 76.3 45.8 �0.001Chronic pancreatitis 7.7 7.0 8.6 0.803
Data are n or %. P values were determined using the �2 test.
H.-L. ZHAO AND ASSOCIATES
DIABETES, VOL. 52, NOVEMBER 2003 2761
pancreas, four had islet amyloid in the pancreatic bodyand another four had islet amyloid in the tail region. Noneof the patients showed islet amyloid limited to the pancre-atic head.
Islet amyloid was present in 40.4% (67/166) of thediabetic patients for whom representative tissue sec-tions were available from all three regions of thepancreas (head, body, and tail). The prevalence was notsignificantly different from that of the diabetic cases forwhom one or two representative tissue sections wereavailable (40.4 vs. 37.7%; P 0.813). Among the 93diabetic cases with islet amyloid, 67 had representativesections from all three pancreatic divisions. In these 67cases, islet amyloid was identified in the tail in 97.0%(65/67), in the body in 92.5% (62/67), and in the head in58.2% (39/67). The highest probability of detecting isletamyloid was in the pancreatic tail and the lowest was inthe pancreatic head (P � 0.001).
The frequency and degree of islet amyloid werevariable in the 93 type 2 diabetic pancreases positive foramyloid. Most showed diffuse islet amyloid with exten-sive fibrosis and acinar atrophy (Fig. 4). The frequencyof islet amyloid ranged from 2.6 to 91.8%, with a meanpercentage of 38.8 � 31.0%. In only 25.8% (24/93) of thediabetic pancreases, 50% or more islets were positivefor amyloid (Fig. 4). The degree of islet amyloid alsovaried from 1.4 to 97.2%. The mean area fraction of isletamyloid was 36.2 � 17.0%, indicating approximately a33% reduction in mean islet cell area in the diabeticpatients with islet amyloid. The degree and frequency ofislet amyloid were positively correlated to BMI, HbA1c,and systolic and diastolic blood pressure in the 93 type2 diabetic patients (Table 3). No significant correlationwas found between the islet amyloid load and theknown duration of type 2 diabetes, age of patient, orfasting plasma glucose and serum lipid levels (Table 3).
FIG. 2. Pancreatic arteriosclerosis in patientswith type 2 diabetes. The arterial lumens aremarked with “L” and the major arterialchanges are marked by asterisks. A: Crescent-like, subendothelial exudation. H-E, magnifi-cation �400. B: Hyaline arteriolosclerosis.H-E, magnification �400. C: Intimal foam cellaccumulation. H-E, magnification �200. D: In-timal plaque calcification. Congo red, magnifi-cation �200. E: Luminal obstruction ofpancreatic artery by lipid-rich atheroma withcholesterol crystal (asterisk). PAS, magnifica-tion �100. F: Recanalization of pancreatic ar-tery. H-E, magnification �100.
ISLET AMYLOID IN TYPE 2 DIABETES
2762 DIABETES, VOL. 52, NOVEMBER 2003

DISCUSSION
We have reported the prevalence and clinicopathologicalcharacteristics of islet amyloid in Chinese patients withtype 2 diabetes. In this multicenter autopsy study, isletamyloid occurred in �40% of the Chinese patients withtype 2 diabetes who were on antidiabetic treatments, and
the amyloid deposits occupied a mean islet area of 36.2% inaffected patients. The type 2 diabetes�associated isletamyloid was positively associated with BMI, blood pres-sure, glycemic control, pancreatic fibrosis, and fat infiltra-tion. Our findings suggest that islet amyloid deposits mayreflect greater insulin resistance and �-cell failure in a
FIG. 3. Fat infiltration in pancreases oftype 2 diabetic patients. Adipocytes (a) areshown in exocrine acini (A; H-E, magnifica-tion �100), islet (B; PAS, magnification�400), adjacent to islet amyloid deposits inred color (C; Congo red, magnification�400, ordinary light), or green/yellow bire-fringence (D; Congo red, magnification�400, polarizing light).
FIG. 4. Diffuse fibrosis (white birefrin-gence; arrows) and islet amyloid deposits(green/yellow birefringence; asterisks) inpancreases of type 2 diabetic patients.Congo red magnification �200, polarizinglight microscope.
H.-L. ZHAO AND ASSOCIATES
DIABETES, VOL. 52, NOVEMBER 2003 2763

subgroup of type 2 diabetic patients (27,28). In agreementwith other reports, this study also confirmed the pheno-typic heterogeneity of type 2 diabetes and the associationof islet amyloid deposits with loss of islet cells (8,11,29).
A limitation of our study is that not all selected autopsycases had representative sections from all three regions(head, body, and tail) of the pancreas. This approach mayhave predisposed us to underestimate islet amyloid depos-its (8). However, most (88.6%) of the diabetic patients hadislet amyloid in more than one anatomical region of thepancreas. Only �3% of pancreases contained amyloid in�1% of the islets (8,30). The prevalence of islet amyloid inthe diabetic patients for whom representative sectionswere available from all three divisions of the pancreas wasnot significantly different from that of the diabetic casesfor whom one or two representative tissue sections wereavailable (40.4 vs. 37.7%; P 0.813). To minimize the biasof underestimation, we included autopsy subjects who had
at least one representative tissue block resected from the�-cell-rich region (tail/body) of the pancreas (22,29).
Islet amyloid deposits are present in only a portion ofpatients with type 2 diabetes. Because of differences insample size and diagnostic criteria, the prevalence of isletamyloid reported in type 2 diabetic patients varies sub-stantially (4,5,10). For example, the widely cited study byWestermark and Wilander (31) showed that islet amyloidwas found in 100% of their sample of only 12 Caucasianpatients with adult onset of diabetes. However, the prev-alence of islet amyloid in the nondiabetic subjects, definedas such by the absence of clinical signs of diabetes and oneor several negative tests for glucose in the urine in thesame study, was 60% (9/15) (31). In an early study, Bell(12) reviewed over 1,000 autopsy cases and found isletamyloid in 44% of diabetic subjects over age 40 years.Using more objective diagnostic criteria, we found isletamyloid in 39.6% of type 2 diabetic patients and 3.0% ofnondiabetic subjects. These data indicate that islet amy-loid occurs only in a subgroup of type 2 diabetic patients.
In this study, type 2 diabetic patients with islet amyloiddisplayed greater insulin resistance (presumed because ofhigher BMI and blood pressure) and insulin deficiency(higher HbA1c). The islet amyloid load has been reportedto be proportional to the severity of type 2 diabetes (6,8).In our study, islet amyloid deposits occupied a mean isletarea of 36.2%, and the frequency and degree of isletamyloid was correlated with HbA1c in 93 patients withtype 2 diabetes. In type 2 diabetic patients, there was aninverse relation between the degree of islet amyloid andintracellular IAPP immunoreactivity (22). Several in vitroand in vivo (transgenic mouse) studies have revealed thatsmall amyloidogenic human IAPP aggregates induce �-celldeath and, subsequently, insulin deficiency (4,29,32–34).All these data imply that the formation of extracellularislet amyloid deposits and the loss of �-cells may beassociated through a common shared precursor, amyloi-dogenic human IAPP aggregates (35). These aggregates
FIG. 5. Chronic pancreatitis characterizedby broad-band fibrotic tissues, extensiveacinar atrophy, inflammatory infiltrates,and islet amyloid deposits (asterisk). H-E,magnification �100.
TABLE 3Pearson’s correlation of islet amyloid with clinical characteris-tics in 93 type 2 diabetic patients
Frequency Degreer P r P
Known duration ofdiabetes 0.050 0.835 0.065 0.786
BMI 0.319 0.013 0.313 0.015Systolic blood pressure 0.326 0.011 0.235 0.028Diastolic blood pressure 0.523 0.008 0.430 0.010HbA1c 0.226 0.033 0.311 0.016Fasting plasma glucose 0.167 0.162 0.151 0.176Total cholesterol 0.163 0.167 0.153 0.175Triglycerides 0.136 0.230 0.132 0.239LDL cholesterol 0.119 0.332 0.116 0.431HDL cholesterol �0.067 0.621 �0.061 0.801Age 0.214 0.071 0.175 0.158Degree of islet amyloid 0.998 �0.001 1 —Frequency of islet amyloid 1 — 0.998 �0.001
ISLET AMYLOID IN TYPE 2 DIABETES
2764 DIABETES, VOL. 52, NOVEMBER 2003

may cause �-cell death by disrupting plasma membranesor/and causing oxidative stress (33,36) while they grow asextracellular islet amyloid deposits (35).
On the other hand, islet amyloid might be a result ofobesity-associated insulin resistance (5). We found thearea of islet amyloid deposits correlated significantly withBMI and blood pressure. Aging-related weight gain innormal rats and genetic obesity in Wistar fatty rats areassociated with elevated IAPP secretion (37). Althoughhemizygous transgenic mice expressing human IAPP inpancreatic �-cells have no diabetic phenotype, type 2diabetic phenotypes such as islet amyloid deposition anddecreased �-cell mass occurred when the hemizygousmice were crossed with an obese, insulin-resistant strainsuch as agouti viable yellow (38). In support of theseexperimental studies, patients with obesity and hyperten-sion have high basal and stimulated levels of plasma IAPP(39,40). Taken together, it is plausible that insulin resis-tance may cause intracellular IAPP amyloidogenesis and,subsequently, �-cell death and extracellular amyloid de-posits (29,33). In contrast to our findings, a recent autopsystudy in 124 Caucasians revealed that islet amyloid load(presence, frequency, and extent) was not increased intype 2 diabetic patients with BMI �27 kg/m2 comparedwith lean patients with BMI �25 kg/m2, nor was it in-creased in obese subjects with impaired glucose tolerancecompared with either obese or lean nondiabetic subjects(29). This discrepancy may reflect ethnic or phenotypicdifferences between the study populations.
Apart from amyloid deposits, �-cell failure in type 2diabetes may also result from other pancreatic his-topathologies, such as pancreatic fat infiltration and fibro-sis (19,20,31). In the current study, 50% of the pancreasesexhibited extensive fibrosis, fat infiltration, and severearteriosclerosis in either exocrine acini or islets. More-over, the frequency of fat infiltration and fibrosis indiabetic pancreases was higher in those with islet amyloid.Pancreatic arteriosclerosis and atherosclerosis were ascommon in diabetic patients with as in those without isletamyloid (41). These observations suggest that pancreaticremodeling induced by arteriosclerosis, islet amyloidosis,fat infiltration, fibrosis, and chronic inflammatory changesmight cause islet and �-cell failure in type 2 diabetes(19,41).
In summary, the prevalence of islet amyloid was �40%in autopsies of Chinese patients with type 2 diabetes. Onaverage, islet amyloid deposits occupied 36% of islet areain these patients. The presence of islet amyloid wasassociated with greater BMI, higher blood pressure,shorter duration of disease, and worse glycemic control indiabetic patients. Islet amyloid was also frequently accom-panied by pancreatic arteriosclerosis, fibrosis, and fatinfiltration. Optimal control of blood pressure and meta-bolic indexes may prevent some of these pathologicalchanges, reduce loss of islet cells, and preserve �-cellfunction in type 2 diabetes.
ACKNOWLEDGMENTS
This study was partially funded by the Graduate Schooland the Hong Kong Foundation for Research and Devel-opment of Diabetes, under the auspices of the ChineseUniversity of Hong Kong.
We gratefully acknowledge the technical assistance ofMing-Chen Guan (Chinese PLA General Hospital). Wethank Dr. Shao C Lee, Dr. Simon KM Lee, Prof. Ho-KeungNg, and the late Prof. Julian A.J.H. Critchley (The ChineseUniversity of Hong Kong) and Prof. Jie Chen (PekingUnion Medical College Hospital) for their support andadvice.
REFERENCES
1. Weyer C, Bogardus C, Mott DM, Pratley RE: The natural history of insulinsecretory dysfunction and insulin resistance in the pathogenesis of type 2diabetes mellitus. J Clin Invest 104:787–794, 1999
2. Ferrannini E: Insulin resistance versus insulin deficiency in non-insulin-dependent diabetes mellitus: problems and prospects. Endocr Rev 19:477–490, 1998
3. Taylor SI, Accili D, Imai Y: Insulin resistance or insulin deficiency. Whichis the primary cause of NIDDM? Diabetes 43:735–740, 1994
4. Hoppener JW, Ahren B, Lips CJ: Islet amyloid and type 2 diabetes mellitus.N Engl J Med 343:411–419, 2000
5. Kahn SE, Andrikopoulos S, Verchere CB: Islet amyloid: a long-recognizedbut underappreciated pathological feature of type 2 diabetes. Diabetes
48:241–253, 19996. de Koning EJ, Bodkin NL, Hansen BC, Clark A: Diabetes mellitus in
Macaca mulatta monkeys is characterised by islet amyloidosis and reduc-tion in beta-cell population. Diabetologia 36:378–384, 1993
7. Clark A, Jones LC, de Koning E, Hansen BC, Matthews DR: Decreasedinsulin secretion in type 2 diabetes: a problem of cellular mass or function?Diabetes 50 (Suppl. 1):S169–S171, 2001
8. Maloy AL, Longnecker DS, Greenberg ER: The relation of islet amyloid tothe clinical type of diabetes. Hum Pathol 12:917–922, 1981
9. Westermark P: Amyloid and polypeptide hormones. What is their inter-relationship? Amyloid 1:47–60, 1994
10. Clark A, Charge SB, Badman MK, de Koning EJ: Islet amyloid in type 2(non-insulin-dependent) diabetes. APMIS 104:12–18, 1996
11. Clark A, Wells CA, Buley ID, Cruickshank JK, Vanhegan RI, Matthews DR,Cooper GJ, Holman RR, Turner RC: Islet amyloid, increased A-cells,reduced B-cells and exocrine fibrosis: quantitative changes in the pancreasin type 2 diabetes. Diabetes Res 9:151–159, 1988
12. Bell ET: Hyalinization of the islets of Langerhans in diabetes mellitus.Diabetes 1:341–344, 1952
13. Westermark P, Engstrom U, Johnson KH, Westermark GT, Betsholtz C:Islet amyloid polypeptide: pinpointing amino acid residues linked toamyloid fibril formation. Proc Natl Acad Sci U S A 87:5036–5040, 1990
14. Clark A, Saad MF, Nezzer T, Uren C, Knowler WC, Bennett PH, Turner RC:Islet amyloid polypeptide in diabetic and non-diabetic Pima Indians.Diabetologia 33:285–289, 1990
15. Vishwanathan KA, Bazaz-Malik G, Dandekar J, Vaishnava H: A qualitativeand quantitative histological study of the islets of Langerhans in diabetesmellitus. Indian J Med Sci 26:807–812, 1972
16. Saito K, Yaginuma N, Takahashi T: Differential volumetry of A, B and Dcells in the pancreatic islets of diabetic and nondiabetic subjects. Tohoku
J Exp Med 129:273–283, 197917. Ohsawa H, Kanatsuka A, Mizuno Y, Tokuyama Y, Takada K, Mikata A,
Makino H, Yoshida S: Islet amyloid polypeptide-derived amyloid deposi-tion increases along with the duration of type 2 diabetes mellitus. Diabetes
Res Clin Pract 15:17–21, 199218. Rahier J, Goebbels RM, Henquin JC: Cellular composition of the human
diabetic pancreas. Diabetologia 24:366–371, 198319. Pancreatic abnormalities in type 2 diabetes mellitus (Editorial). Lancet
ii:1497–1498, 198720. Clark A, de Koning EJ, Hattersley AT, Hansen BC, Yajnik CS, Poulton J:
Pancreatic pathology in non-insulin dependent diabetes (NIDDM). Diabe-
tes Res Clin Pract 28:S39�S47, 199521. International Obesity Task Forces: The Asia-Pacific Prospective: Redefin-
ing Obesity and Its Treatment. Sydney, Health Communications Australia,2000, p. 15–21
22. Rocken C, Linke RP, Saeger W: Immunohistology of islet amyloid polypep-tide in diabetes mellitus: semi-quantitative studies in a post-mortem series.Virchows Arch 421:339–344, 1992
23. O’Brien TD, Butler AE, Roche PC, Johnson KH, Butler PC: Islet amyloidpolypeptide in human insulinomas: evidence for intracellular amyloidogen-esis. Diabetes 43:329–336, 1994
24. Cooper GJ, Willis AC, Clark A, Turner RC, Sim RB, Reid KB: Purification
H.-L. ZHAO AND ASSOCIATES
DIABETES, VOL. 52, NOVEMBER 2003 2765

and characterization of a peptide from amyloid-rich pancreases of type 2diabetic patients. Proc Natl Acad Sci U S A 84:8628–8632, 1987
25. Puchtler H, Sweat F, Levine M: On the binding of Congo red by amyloid.J Histochem Cytochem 10:355–364, 1962
26. Kelenyi G: Thioflavin S fluorescent and Congo red anisotropic stainings inthe histologic demonstration of amyloid. Acta Neuropathol 7:336–348,1967
27. Hoppener JW, Oosterwijk C, Nieuwenhuis MG, Posthuma G, Thijssen JH,Vroom TM, Ahren B, Lips CJ: Extensive islet amyloid formation is inducedby development of Type II diabetes mellitus and contributes to itsprogression: pathogenesis of diabetes in a mouse model. Diabetologia
42:427–434, 199928. Hoppener JW, Nieuwenhuis MG, Vroom TM, Ahren B, Lips CJ: Role of islet
amyloid in type 2 diabetes mellitus: consequence or cause? Mol Cell
Endocrinol 197:205–212, 200229. Butler AE, Janson J, Bonner-Weir S, Ritzel R, Rizza RA, Butler PC: Beta-cell
deficit and increased beta-cell apoptosis in humans with type 2 diabetes.Diabetes 52:102–110, 2003
30. Erlich JC, Ratner IM: Amyloidosis of the islets of Langerhans: a restudy ofislet hyaline in diabetic and nondiabetic individuals. Am J Pathol 38:49–59,1961
31. Westermark P, Wilander E: The influence of amyloid deposits on the isletvolume in maturity onset diabetes mellitus. Diabetologia 15:417–421, 1978
32. Lorenzo A, Razzaboni B, Weir GC, Yankner BA: Pancreatic islet celltoxicity of amylin associated with type-2 diabetes mellitus. Nature 368:756–760, 1994
33. Janson J, Ashley RH, Harrison D, McIntyre S, Butler PC: The mechanism ofislet amyloid polypeptide toxicity is membrane disruption by intermediate-sized toxic amyloid particles. Diabetes 48:491–498, 1999
34. Janson J, Soeller WC, Roche PC, Nelson RT, Torchia AJ, Kreutter DK,Butler PC: Spontaneous diabetes mellitus in transgenic mice expressinghuman islet amyloid polypeptide. Proc Natl Acad Sci U S A 93:7283–7288,1996
35. Butler PC: Islet amyloid and its potential role in the pathogenesis of type2 diabetes mellitus. In Diabetes Mellitus: A Fundamental and Clinical
Text. 2nd ed. LeRoith D, Taylor SI, Olefsky JM, Eds. Philadelphia,Lippincott Williams & Wilkins, 2000, p. 141–146
36. Janciauskiene S, Ahren B: Fibrillar islet amyloid polypeptide differentiallyaffects oxidative mechanisms and lipoprotein uptake in correlation withcytotoxicity in two insulin-producing cell lines. Biochem Biophys Res
Commun 267:619–625, 200037. Pieber TR, Roitelman J, Lee Y, Luskey KL, Stein DT: Direct plasma
radioimmunoassay for rat amylin-(1–37): concentrations with acquired andgenetic obesity. Am J Physiol 267:E156�E164, 1994
38. Soeller WC, Janson J, Hart SE, Parker JC, Carty MD, Stevenson RW,Kreutter DK, Butler PC: Islet amyloid-associated diabetes in obese avy/amice expressing human islet amyloid polypeptide. Diabetes 47:743–750,1998
39. Kautzky-Willer A, Thomaseth K, Pacini G, Clodi M, Ludvik B, Streli C,Waldhausl W, Prager R: Role of islet amyloid polypeptide secretion ininsulin-resistant humans. Diabetologia 37:188–194, 1994
40. Kailasam MT, Parmer RJ, Tyrell EA, Henry RR, O’Connor DT: Circulatingamylin in human essential hypertension: heritability and early increase inindividuals at genetic risk. J Hypertens 18:1611–1620, 2000
41. Kauppila LI, Hekali P, Penttila A: Postmortem pancreatic angiography in 45subjects with non-insulin-dependent diabetes mellitus and 51 controls.Pancreas 16:60–65, 1998
ISLET AMYLOID IN TYPE 2 DIABETES
2766 DIABETES, VOL. 52, NOVEMBER 2003