prevalence of feeding difficulties objectives · pdf filemy baby is not eating ... lack of...
TRANSCRIPT

1
Colin Rudolph, MD, PhD
Vice-President, Global Medical Affairs & Chief Medical Officer Mead Johnson Nutrition
Conflict of Interest
• Employed by Mead Johnson Nutrition
• Board Member- POPSICLE
25% - 45% in children with normal development
33%-80% in children with developmental delays or chronic disease
Prevalence of Feeding Difficulties
To provide guidance on:
When to worry
When to refer
Where to refer
an infant or toddler with concerns about feeding
Objectives

2
My baby is not eating…
When did the problem start?
Acute onset in previously well
infant/child
Neurologic
Infection
Cardio-pulmonary
Metabolic
Other
Chronic problem
Subdural Hematoma
Meningitis
Cerebrovascular Event
Botulinum Toxin
Myasthenia Gravis
Guillain-Barre Syndrome
Arnold Chiari Malformation
Increased ICP
Vitamin A toxicity
Drug Tardive dyskinesia
Urinary Tract Infection
Bacteremia/Sepsis
Meningitis
Otitis Media
Hepatitis
Gastroenteritis
Pancreatitis
Esophagitis- Candida/Herpes
Neurologic Infection
Congestive Heart Failure
Pneumonia
Epiglotitis
Uremia
Hypercalcemia
Hypocalcemia
Hypomagnesiemia
Toxins
Cardio-pulmonary
Metabolic
Other
Foreign Body
Evaluation for Acute Changes in Feeding
• History and Physical Exam
– Is this infant sick? Directed laboratory exam
• Head MRI/CT?
• Sepsis work-up?
• Metabolic panel?
• No clear pathology
– Rule out Foreign Body
• UGI (water-soluble contrast)
• Upper endoscopy

3
My baby is not eating…
When did the problem start?
Acute onset in previously well
infant/child
Neurologic
Infection
Cardio-pulmonary
Metabolic
Other
Chronic problem
Presentations of Feeding Disorders
Inadequate growth due to inadequate intake
Inefficient feeding (prolonged time for each meal)
Delayed progression of normal feeding skills
(intake of pureed, chewing, etc)
Recurrent respiratory disease
Causes of Inadequate or Inefficient Intake
Decreased appetite drive
Disordered parent-child interaction
Inadequate suck/swallowing skills
Learned aversion due to pain or discomfort following feeds
Popsicle Queries
• Does your baby/child let you know when he is
hungry?
• Do you think your baby/child eats enough?
• Does your baby usually like to be fed?
• Do you enjoy feeding time with your baby/child?

4
ARC
POMC/
CART
AgRP/
NPY
Leptin
Appetite Appetite
Inhibition Stimulation
Environmental factors
(neglect, maternal depression) - +
Inflammatory
mediators
(TNFα)
-
Vagus -
Visceral
Pain
Medications
- +
Ghrelin +
CCK
Insulin
PYY
- +
Parent-Child Interactions
• Providing Food
• Positive Reinforcement
• Modeling Behaviors
• Is poor growth due to
“neglect” or “organic
factors”?
-Temperment
-Skills -Temperment
-Skills
Disordered parent-child interactions
“Feeding Traps”
Reinforced negative behaviors
Force feeding, food hunts, short-order cooking
Failure to set appropriate limits
grazing, multiple feeding environments, TV
Not attending to positive behaviors
ignoring child’s cues
Projecting parental food preferences
I don’t like it, therefore you won’t like it
“Infantile Anorexia”
• Infants characterized by: – refusal to eat adequate amounts of food for at least 1 month
– onset of the food refusal under 3 years of age, most commonly during the
transition to spoon- and self-feeding
– failure to communicate hunger signals, lack of interest in food, but strong
interest in exploration and/or interaction with caregivers
– significant growth deficiency
– no evidence that the food refusal followed a traumatic event or is associated
with an underlying medical illness.
Chatoor I et al, Pediatrics 2004;113:e440

5
Consequences of “Infantile Anorexia”
Compared to
• Picky eaters – Persistent refusal to eat all types of food or certain
types of food to cause concern to parents
– No growth deficiency
• Healthy eaters – No food refusal or concerns
– No growth deficiency
Chatoor I et al, Pediatrics 2004;113:e440
Consequences of “Infantile Anorexia”
• Although toddlers with infantile anorexia exhibit growth
deficiency, they performed within the normal range of
cognitive development
• The MDI scores of toddlers with infantile anorexia and that
of the normal weight picky eaters were, respectively, 11 and
14 points below that of the healthy eaters without feeding
problems
• Higher socio-economic status, maternal education, and
feeding reciprocity were related to higher MDI scores
• Higher levels of conflict and control struggles during feeding
interactions and maternal intrusiveness during play
interactions were related to lower MDI scores
Chatoor I et al, Pediatrics 2004;113:e440
Consequences of “Infantile Anorexia”
• Causality of this disorder remains unclear – Underlying cognitive issues or mild skill deficits may make establishment of
normal feeding relationship more problematic
– Parental worry over the effect of poor weight gain on development may lead
to coercive feeding which intensifies parent-child conflicts and impacts
development
Chatoor I et al, Pediatrics 2004;113:e440
-Temperment
-Skills
-Cognition
-Temperment
-Skills
-Cognition
Wolfson Screening Criteria for Behavioral
Causes of Infant Feeding Refusal
• Evaluated infant and parent behavior patterns or symptoms to
distinguish organic or behavioral causes or infant feeding refusal
– Infantile feeding disorder- Symptoms before age 2, persistent food aversion longer
than 1 month, and a response to behavioral intervention (n=83)
– Organic group (diagnosis of GERD, Milk Allergy, Nutritional FTT) responded to
medical or nutritional therapy alone (n=68)
• Poor intake, poor weight gain, or vomiting did not discriminate between
“organic” and “nonorganic” causes.
• Factors indicating the presence of a behavioral cause included:
– food refusal (p<0.0001)
– food fixation (p<0.0001)
– abnormal parental feeding practices (p<0.0001)
– onset after a specific trigger (p<0.0001)
– presence of anticipatory gagging (p<0.0001)
Levy Y et al, J Pediatr Gastroenterol Nutr 2009:48-355-62
6
More Popsicle Queries
• Do you often have to do anything special to help your
baby eat?
• Does your baby/child do any of the following when you
feed him?
– Refuses to eat
– Does not swallow
– Turns away from the breast/bottle/cup
– Gags, coughs, chokes
– Arches his body
– Cries/Tantrums
– Vomits after eating
Evaluation and Management of Possible
Behavioral Issues Impacting Feeding
• History and Physical Exam
– Query for underlying pathology since behavioral
issues may result from physical disorders
– Query for potential signs of behavioral factors
especially “anticipatory gagging”, onset after a
trigger
• No clear pathology
– Consider referral to psychologist/feeding team with
expertise in evaluating and treating behavioral
disorders.
– If not progressing with behavioral treatment,
reconsider other contributing factors
Evaluation and Management of Possible
Behavioral Issues Impacting Feeding
• Nutritional intervention (ng/gt) may be
advisable but there are no uniformly agreed
upon criteria (Wght for Height >2SD below
normal?)
• Often infants stop eating when supplemental
nutrition is provided and their hunger drive is
suppressed
• Follow-up on FTT infants shows they remain
small, and no study shows that intervention
alters long-term outcomes.
Popsicle Queries
• Skills limit the ability to ingest normal amounts
– Do you feed your baby more often than every two
hours?
– Do you think your baby eats enough?
– How long does it usually take to feed your baby?
• <5min; 5 to 30 min; >30 min
– Does your baby
• Turn blue, become limp or worn out before the end of
feedings, falls asleep before the end of feeing, make loud
breathing noises during/after feeding, etc….
7
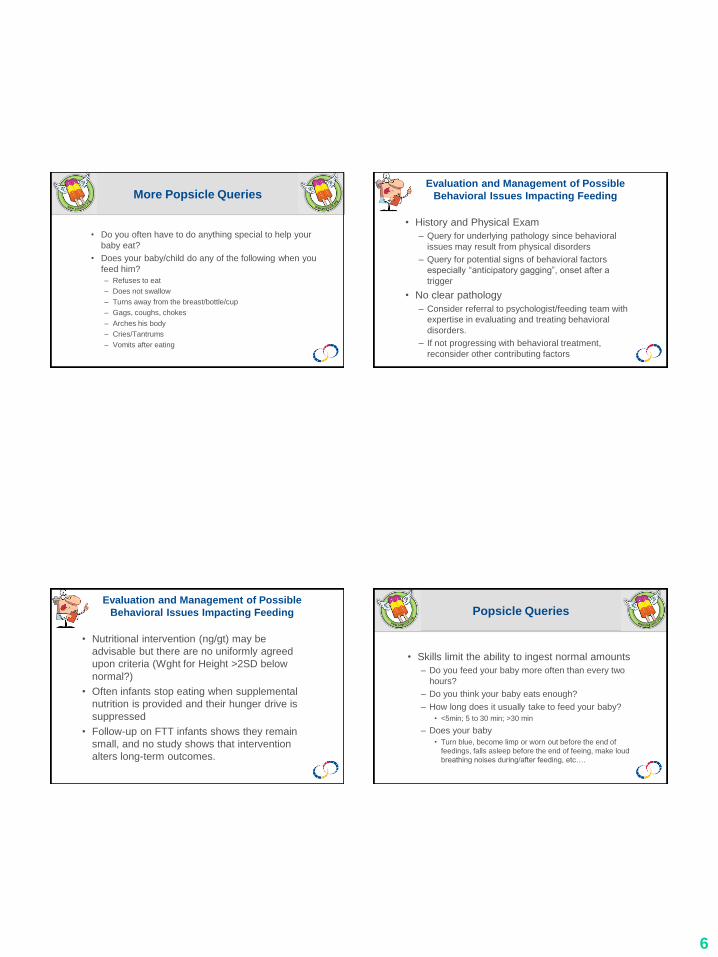
Causes of inadequate suck/swallow skills
Anatomic disorders
Poor coordination of suck-swallow-breathing sequence
Neurologic disorders
Oropharyngeal
Generalized
Inadequate experience during critical sensitive periods of development
Infant Adult
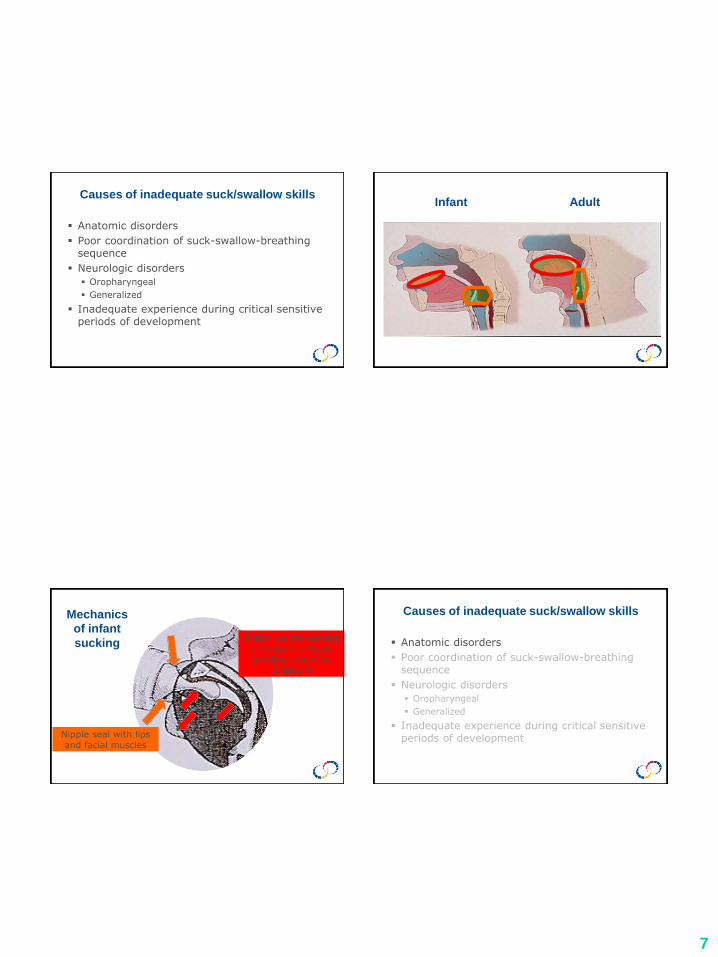
Mechanics
of infant
sucking Pistonlike movement of tongue and jaw produce negative
pressure
Nipple seal with lips and facial muscles
Causes of inadequate suck/swallow skills
Anatomic disorders
Poor coordination of suck-swallow-breathing sequence
Neurologic disorders
Oropharyngeal
Generalized
Inadequate experience during critical sensitive periods of development

8
Examples of anatomic disorders
• Cleft lip and palate
• Mass such as Lingual tonsil
• Laryngeal cleft
• Tracheo-esophageal fistula
• Esophageal stenosis, web or ring
• Choanal atresia or stenosis
Causes of inadequate suck/swallow skills
Anatomic disorders
Poor coordination of suck-swallow-breathing sequence
Neurologic disorders
Oropharyngeal
Generalized
Inadequate experience during critical sensitive periods of development
Milk flow
Expired CO2
Relationship of breathing and swallowing
in normal newborn infant
Infant coordinates suck-swallow-breath sequence
Respiration ceases during swallowing
In children with tachypnea (due to pulmonary, cardiac or neurologic disease) coordination is often poor
Causes of inadequate suck/swallow skills
Anatomic disorders
Poor coordination of suck-swallow-breathing sequence
Neurologic disorders
Oropharyngeal
Generalized
Inadequate experience during critical sensitive periods of development

9
Popsicle Queries
• Does your baby usually turn to take the breast or
bottle into the mouth? (rooting reflex)
• Do you usually hold your baby in your arms when you
feed him? (tone)
• Does your baby (after 9mo) sit up to eat?
• Does your child (over 15mo) pick up food with his
fingers?
• How long does it usually take to feed your baby?
• Do you often have to do anything special to help your
baby eat?
Neuromuscular disorders
Generalized
Myasthenia gravis
Muscular dystrophy
Congenital myopathies
Cerebral palsy
Polymyositis or Dermatoyositis
Infant botulism
Guillan-Barre
Oropharyngeal
Arnold-Chiari Malformation
Bulbar atresia
Ocular-Pharyngeal Dystrophy
Brain Stem Tumor
Drug-Tardive Dyskinesia
Moebius Syndrome
Cricopharyngeal achalasia
Other disorders associated with feeding
difficulties
Familial Dysautonomia
Prader-Willi
Hypothyroidism
Trisomy 18 & 21
Velocardiofacial syndrome
Rett syndrome
Evaluation for Neurologic Issues
Impacting on Feeding
• History and Physical Exam
– h/o or suspicion of seizures?
– Family history of developmental delays?
– Prematurity?
– Careful neurologic exam
• Consider speech pathology and/or
physical/occupational therapy referral
• Consider video-fluoroscopic swallowing
study
• Consider genetic/metabolic studies

10
Inadequate oropharyngeal skills
Anatomic disorders
Poor coordination of suck-swallow-breathing sequence
Neurologic disorders Oropharyngeal
Generalized
Inadequate experience during critical sensitive periods of development
Critical Sensitive Periods for Development
The infant nervous system is programmed to acquire certain skills at specific times in development.
Skill acquisition at these “critical sensitive periods” is relatively effortless
Later skill acquisition is difficult
Infant Behavior and Learning
1937- Lorenz observed that young chicks “imprint” on the first brightly colored object they encounter and attempt to maintain proximity to that object.
Imprinting would not occur after 25 hours of age
• Deprivation of visual input at critical periods results in a lack of development of associated visual cortex

11
Mechanical Skill Acquisition
Experiment: Post-weaning mice fed a soft-powdered diet versus the usual pelleted-hard diet
Result: Fewer synapses developed in the hippocampus and parietal cortex.
As adults, the spatial learning ability (tested in 8 arm radial maze) of the soft-diet fed group was reduced compared to the pelleted-hard diet fed group
Yamamoto & Hirayama, Brain Res 2001;902:255
Causes of Inadequate or Inefficient Intake
Decreased appetite drive
Disordered parent-child interaction
Inadequate suck/swallowing skills
Learned aversion due to pain or discomfort following feeds
Learned Aversions Learned aversion due to pain or
discomfort following feeding
Pharyngo-esophageal
Inflammation
Candida
Herpes
Crohn’s
Behcet’s
Caustic Burns
Reflux esophagitis
Eosinophilic esophagitis
Other gastrointestinal disorders
Achalasia
Foreign Body
Esophageal stricture
Peptic ulcer disease
Biliary tract disease
Dumping syndrome
Gastroparesis
Severe constipation

12
Presentations of Pediatric Feeding Disorders
Inadequate growth due to inadequate intake
Prolonged time for feedings (but provides adequate calories for growth)
Delayed progression of normal feeding skills
(textures, variety, etc)
Recurrent respiratory disease
Popsicle Queries
• How long does it take to feed your baby/child?
– <5min; 5-30min; >30 min (20-30 min is normal)
• Do you feed your baby more than every two hours?
• Do you often feed your child during the night?
• Do you think your baby/child eats enough?
• Does your baby often do any of the following when you
feed him?
– Refuses to eat, does not swallow, becomes limp or
worn out before the end of feeding
Prolonged time for feedings
Can be due to:
Inefficient feeding, inadequate skills
Behavioral feeding disorder
Parental-Child interaction issues
Underlying disorder causing discomfort
Evaluation of Prolonged Feeding Time
• History and Physical Exam
• Consider speech pathology and/or
physical/occupational therapy referral (can
the infant/child eat more efficiently?)
• If skills appear appropriate, consider
behavioral therapy and/or multidisciplinary
feeding team referral
• May consider further diagnostic evaluation
including VSS and/or upper endoscopy

13
Presentations of Pediatric Feeding Disorders
Inadequate growth due to inadequate intake
Prolonged time for feedings (but provides adequate calories for growth)
Delayed progression of normal feeding skills
(textures, variety, etc)
Recurrent respiratory disease
Popsicle Queries
• Age specific questions:
– 9-11mo
• Is giving your baby new solid foods going well
• Does your baby eat a variety of foods?
• Does your baby usually like having things in or near his mouth?
– 12-14mo
• Does your child eat a variety of food textures?
– 15mo and older
• Most of the time, do you give your child the same food the family
eats?
• Does your child pick up food with his fingers?
• Does your child drink from a cup?
Evaluation of Delayed Progression of
Textures
• History and Physical Exam
• Consider speech pathology and/or
occupational therapy referral
• If skills appear appropriate consider
anatomic abnormality (esophageal ring,
web) Esophagram?
• Consider Eosinophilic Esophagitis
especially if child otherwise normal or FH
of atopy Upper endoscopy with biopsy
Management strategies when intake is
inadequate include:
Nutrition guidelines
Amounts & types of food
Alterations of food Texture, Taste,
Caloric density Changes in route of
nutrition/hydration NG, Gastrostomy,
GJ
Changes in feeding schedule & pacing
Utensil changes
Position & posture changes
Oral sensorimotor program with food
Nonnutritive oral sensorimotor program
Behavioral Therapies

14
Presentations of Pediatric Feeding Disorders
Inadequate growth due to inadequate intake
Prolonged time for feedings (but provides adequate calories for growth)
Delayed progression of normal feeding skills
(textures, variety, etc)
Recurrent respiratory disease
Popsicle Queries
• Does your baby do any of the following
when you feed him?
– choke, cough, gag
– make loud breathing noises
– turn blue
• No questions on recurrent pneumonia or
asthma- these are for the MD
Recurrent
Pneumonia
• Defined as 2 pneumonia episodes in 1 yr or 3 episodes overall
• Retrospective review of 2,952
pneumonia admissions over 10 yrs
• 238 were recurrent pneumonia
Owayed AF et al, Arch Pediatr Adolesc Med, 2000
Evaluation of Infant or Child with Recurrent
Pneumonia
Aspiration with swallow
48% Respiratory tract anomalies
8%
Immune disorder 14% GER 6%
Cong Heart disease 9% Unknown 8%
Asthma 8%
Owayed AF et al, Arch Pediatr Adolesc Med, 2000

15
Evaluation of Recurrent Respiratory Disease
• History and Physical Exam
• Rule out anatomic disorders (tracheo-
esophageal fistula or laryngeal cleft)
• Evaluate for aspiration (VSS, FEES,
Bronchoscopy with lavage, Chest CT?)
• Consider trial of nasogastric or nasojejunal
feeds
Conclusions
Feeding disorders present in various manners and determining the underlying cause can be difficult
A parent questionnaire screens for abnormalities but often does not provide help in identifying the underlying cause of feeding difficulties
Behavioral, anatomic, and physiologic disorders often coexist, complicating diagnosis and management such that a interdisciplinary approach to diagnosis and management is helpful