prevention of diabetes and cvd: it can be done dr christine connors director, preventable chronic...
TRANSCRIPT
Prevention of diabetes and CVD:it can be done
Dr Christine Connors
Director, Preventable Chronic Disease Program
Department Health & Families
Overview
• Burden of disease
• Prevention works
• Current policy environment
• What’s happening in CA
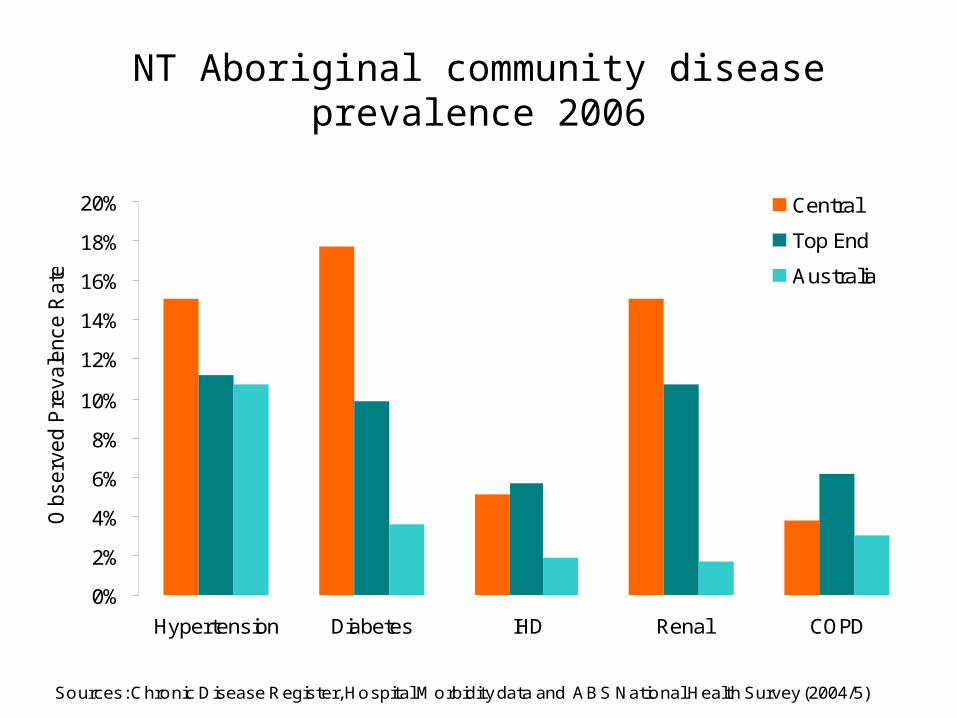
NT Aboriginal community disease prevalence 2006
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
Hypertension Diabetes IHD Renal COPD
Observ
ed P
revale
nce R
ate
s
Central
Top End
Australia
Sources: Chronic Disease Register, Hospital Morbidity data and ABS National Health Survey (2004/5)

Diabetes by region and age
0%
10%
20%
30%
40%
50%
60%
<15 15-34 35-49 >=50
Age Group (Years)
Observ
ed P
revale
nce R
ate
Central
Top End
Australia
Sources: Chronic Disease Register, Hospital Morbidity data and ABS National Health Survey (2004/5)

Trends in avoidable hospitalisation
NT Indigenous
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
1998
/99
1999
/00
2000
/01
2001
/02
2002
/03
2003
/04
2004
/05
2005
/06
Hospital separations per 100 000
NT non-Indigenous
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
1998
/99
1999
/00
2000
/01
2001
/02
2002
/03
2003
/04
2004
/05
2005
/06
Hospital separations per 100 000
Vaccine Vaccine
Acute Acute
ChronicChronic
Li SQ et al. (2009) Avoidable Hospitalisation in Aboriginal and non-Aboriginal people in the Northern Territory MJA

Vic Tobacco
Act
Pack health
labelling regulations introduced
NRT available for sale in Australia
MCG Smokefree
C/W implement tax by stick
Smokefree dining
Gaming venue bans
1st QUIT Campaigns
4 rotating
pack health
warnings
Smoking banned on domestic airlines
Tobacco Ads
banned Print Media
in excise duty
Federal bans on tobacco sponsorship of sports & arts
Age for sale of cigarettes 16 to 18
Health warnings on packs
Remaining tobacco sponsorship removed (exc.
Significant international events)
POS advertising bans
No Butts Campaign
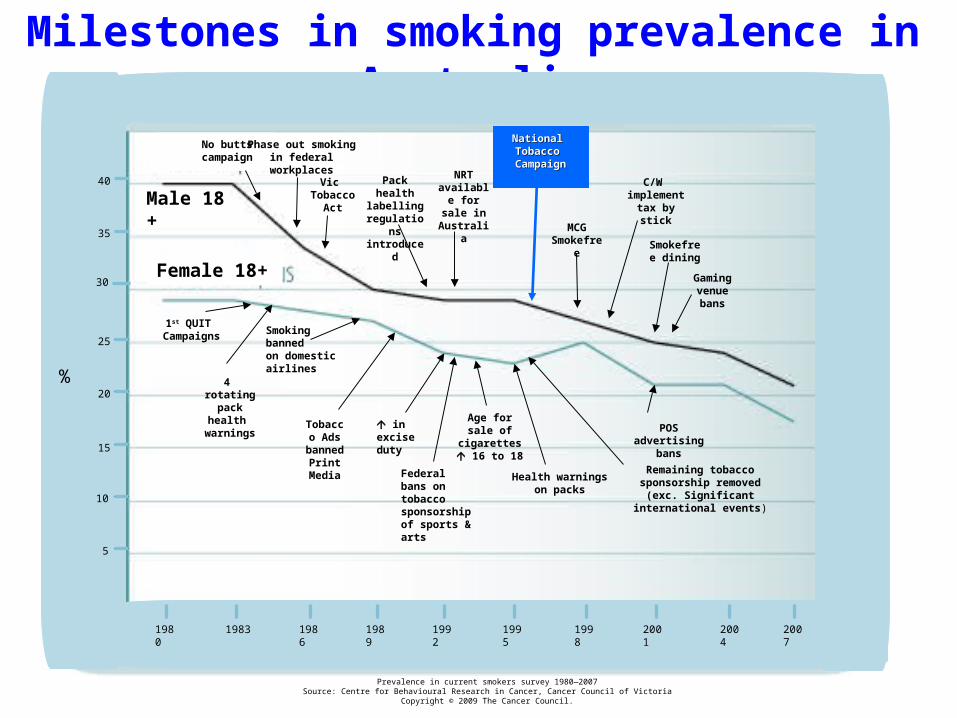
Milestones in smoking prevalence in Australia
Male 18 +
National National Tobacco Tobacco CampaignCampaign
1980 1983 1986 1989 1992 1995 1998 2001 2004
10
5
20
15
30
25
35
40
%
Prevalence in current smokers survey 1980—2007Source: Centre for Behavioural Research in Cancer, Cancer Council of Victoria
Copyright © 2009 The Cancer Council.
2007
Phase out smoking in federal
workplaces
Female 18+
No butts campaign
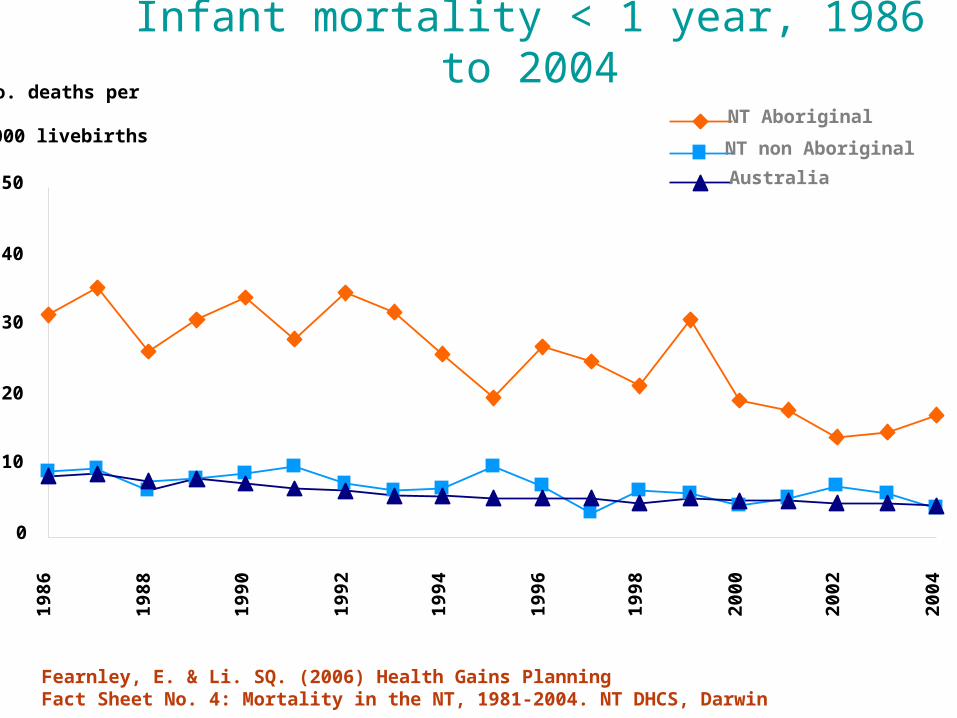
Infant mortality < 1 year, 1986 to 2004
0
10
20
30
40
50
198
6
198
8
199
0
199
2
199
4
199
6
199
8
200
0
200
2
200
4
No. deaths per
1000 livebirthsNT Aboriginal
NT non Aboriginal
Australia
Fearnley, E. & Li. SQ. (2006) Health Gains Planning Fact Sheet No. 4: Mortality in the NT, 1981-2004. NT DHCS, Darwin

Trends in % children underweight
0
5
10
15
20
25
30
1999 2000 2001 2002 2003 2004
EA
DR
Kath
Bark
CA
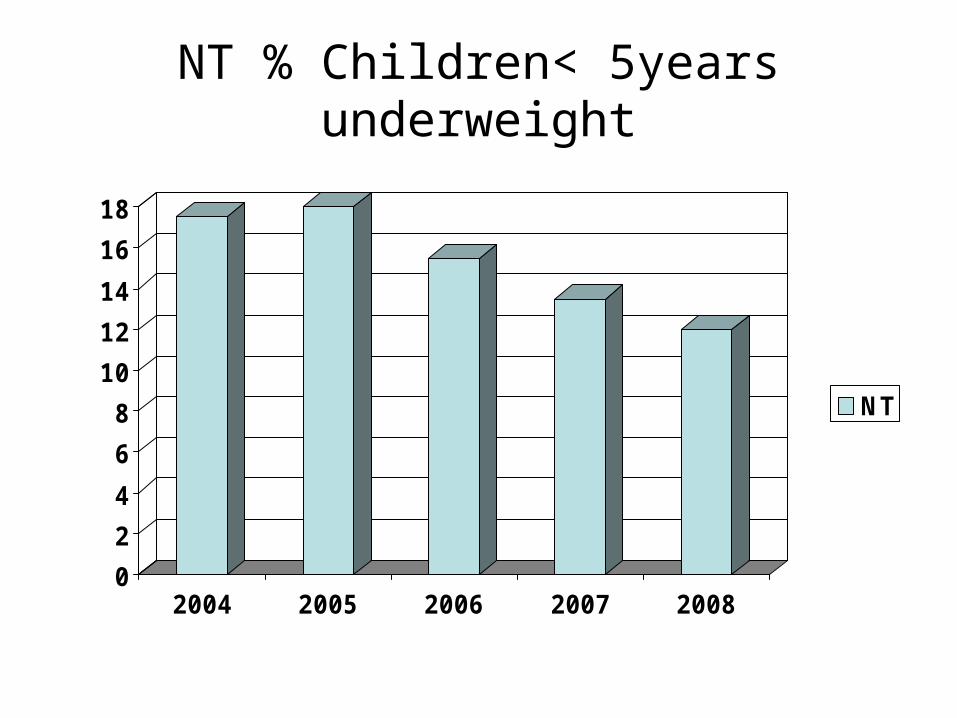
NT % Children< 5years underweight
0
2
4
6
8
10
12
14
16
18
2004 2005 2006 2007 2008
NT
Social determinants
– NTG Closing the gap– COAG Close the gap
– NT intervention• PHC expansion and reform (EHSDI)• Education• Housing• Employment and business opportunities
– Private sector support jobs

NTG Closing the Gap
• “Budget 2009 delivers more housing, health, education and child protection services in remote areas”
• “Tackling Indigenous disadvantage is a key focus of the Northern Territory Government and $63.5 million delivered as part of Budget 2009 is part of our five-year $286 million closing the gap package.

“Little Children Are Sacred”
Report recommendations included:
Use PHC centres as service hubs as part of the development of integrated health and welfare responses in remote communities
Successful submission from NT• $200 million PHC services
2008/09-2011/12

PHC expansion and reform
• Transition to community control
• Expanded services– focus on population health programs– Core services including prevention
• Reform– Community control– CQI– Hub services
NT Department Health & Families Corporate Plan 2009-2012
Six Priority Action Areas
1. Promoting and Protecting Good Health and Wellbeing and Preventing Injury
– Focusing on health promotion and minimising unhealthy behaviours and their impacts
– Improving health awareness to reduce cost pressures on the health system that are derived from preventable chronic diseases
– Assist in ‘closing the gap’ in health outcomes and life expectancy between Aboriginal and non Aboriginal populations in the NT

NT Chronic Conditions Prevention and Management Strategy 2010-2020
Social determinants of health
Primary Prevention
Secondary prevention and early intervention
Self management support
Care for people with chronic conditions
Workforce planning and development
Information, communication and disease management
systems
Continuous quality improvement

COAG Preventative Health Partnership agreement
2009-2014• Focus on obesity• Community programs through Local government• Early childhood: child care settings• Schools: physical activity and nutrition policies• Workplaces: healthy worker programs• Social marketing: national• Incentive payments linked to ambitious targets
The Healthiest Country by 2020The Healthiest Country by 2020

Obesity - Priorities for Action Drive environmental changes throughout the community
Drive change within the food supply
Embed physical activity and healthy eating in everyday life
Encourage people to improve their levels of physical activity and healthy eating
Reduce exposure of children and others to marketing of energy-dense nutrient-poor foods and beverages

Local government, community, NGO’s•Healthy Places and Spaces planning guidelines adopted•COAG Healthy Communities initiative implemented
State and Territory Governments•Health Impact Assessment in all policy development•Fund programs that promote health eating in schools, workplaces and community
Food and Beverage Industry•Partner in Healthy Food Compact to drive change in food supply•Work with AG to implement national food labelling
Individuals and Families•Positive role modelling for children•Turn off TV and be active as a family•Eat one healthy meal together each day•Use active transport•Reduce sitting time•Limit eating food with high sugar, fat and salt
Australian Government•Research economic barriers and tax incentives promote production, access and consumption of healthy foods
•Reduce advertising before 9pm of high fat energy dense food•Review legislation to promote and support workplace programs
Indigenous communities•Work with community organisations and government to implement comprehensive programs that promote healthy eating and physical activity•Strengthen maternal and child health services
Advertising industry•Increase marketing of healthy food and beverages•Work with government to promote physical activity and healthy eating through social marketing
Schools•Incorporate Health and Physical education into National Curriculum•Support active transport•Provide community access to school recreation facilities after hours
Workplaces•Implement policies that promote healthy eating and physical activity•Support active transport•Offer employees access to workplace programs
OBESITY: Shared responsibility

Tobacco: priorities for action Make tobacco significantly more expensive Social marketing Eliminate exposure to second hand smoke in public places Ensure all smokers in contact with health services are
supported and encouraged to quit Work in partnership with Indigenous groups to boost
efforts to reduce smoking and exposure to tobacco products
Boost efforts to discourage smoking amongst disadvantaged groups
Assist parents and educators to discourage tobacco use and protect young people from second hand smoke

Prevention activities in CA

Health promotion approach
• Needs assessment• Understand contributing factors and where
public health staff can assist• Use evidence to identify most effective
actions– PHT technical papers
• Planning and evaluation– Public health bush book– QIPPS
Ottawa Charter Health Promotion Actions
Use them all, all of the time• Create Supportive Environments• Strengthen Community Actions• Develop Personal Skills• Build Healthy Public Policy• Reorient Health Services• Mediate• Advocate

Diabetes in pregnancy
• Screening for diabetes in pregnancy• Limited knowledge and confidence amongst PHC staff• Pre-existing undiagnosed DM has significant complications• Management by local PHC team• Supported by outreach midwives, Obstetrician
• Diabetes Antenatal clinic (DANCE) at ASH• Weekly clinic with Obstetrician, midwife and diabetes
educator at ASH• Virtual clinic• Limited specialist staff • High prevalence (approx 20% pregnancies)

Schools
• Mooditj program– Target group: children aged 10-14 years
• Delivered in schools and also weekend sessions, 10 week program
– Wellness program• Focuses on developing self esteem, body image, puberty,
resilience, goal setting, problem solving, sexual issues
– Need dedicated Coordinators to expand delivery
• Alukura: womens health education program: high schools, teenage girls
• Headspace: work with young people in Alice Springs, tobacco
• The Gap youth centre’; physical activities
Schools• Nutritionists assist school canteen staff to implement new school
canteen policy• Ad hoc nutrition sessions in classrooms
– Local and visiting staff– Nutrition curriculum in DET but not being delivered
• Red Cross Breakfast program• School nutrition program (mainly lunches) funded by DEEWR, AGI
– Local women run the program at Tara and Wilora• Remote stores
– Many have local policies to refuse service to children during school hours
– Usually close 1200-2.00pm• School holiday program: “Deadly Treadlies”
– Recycle old bikes and teach kids to maintain– Recently defunded

Community programs
• Women’s centres– Cookbooks, cooking for elderly, frail &
disabled
• Wok cooking• Store tours
• Cooking demonstrations• “Eat Better Move More” program

Community programs: physical activity
• Limited infrastructure– Basketball courts but often no night lights– 35 communities:5-6 have gym equipment– Limited numbers of Sport & recreation officers
• Previously often focused on kids• Recently working with Heart Foundation
– Active After School program: frequently unqualified staff
• Group activities– Organised sport– Walking groups– Dance classes

Population approaches
• Improving food availability and quality– Outback Stores– 8 stores in CA– employ dietician
• Cost and food security major issue• Mae Wirru store policy NPY Lands
– Nutrition policy, healthy product placement, ban on soft drinks
• Remote Indigenous Stores and Takeaways project

Smoking rates in pregnancyAboriginal women 2005
0
10
20
30
40
50
60
70
1st visit` 36 wks
East Arnhem
Dwn remote
Katherine
Barkly
Alice remote
NT NA

Tobacco control
Limited comprehensive programs to datePerception “not a problem in CA”Taxation and social marketing most effectiveBut…
BI, NRT, smoke free policies, Quit programsCommunity education and local social marketingLocal smoke free outdoor policies: • card games, social gatheringsNT Tobacco Action PlanNew legislation 2 January 2010

Prevention: it can be done
• Systematic organised approach
• Resourced
• Evidence based
• Community development
• Evaluation and research