prevention of maternal mortality_stanton
TRANSCRIPT

USAID’s Maternal Health Vision for Action: How Can It Inform Programs?

Ending Preventable Maternal Mortality: USAID Maternal Health Vision for Action June 2014
Ending Preventable Maternal Mortality: USAID Maternal Health Vision for Action Evidence for Strategic Approaches January 2015
Ending Preventable Maternal Mortality: USAID Vision
A world where no woman dies from preventable maternal causes and maternal and fetal health are
improved
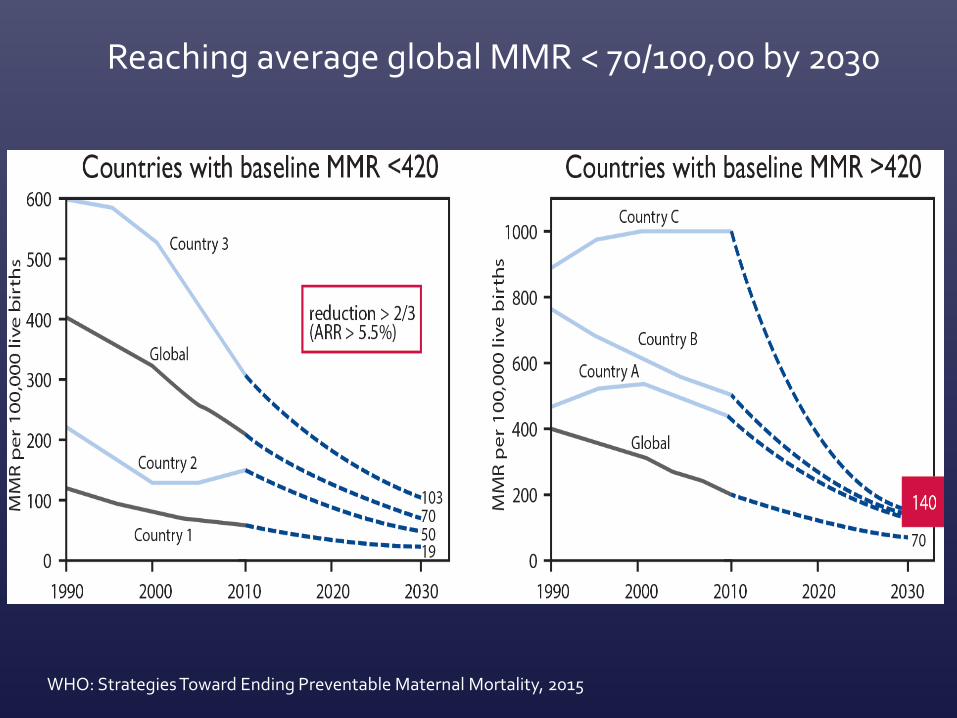
Reaching average global MMR < 70/100,00 by 2030
WHO: Strategies Toward Ending Preventable Maternal Mortality, 2015


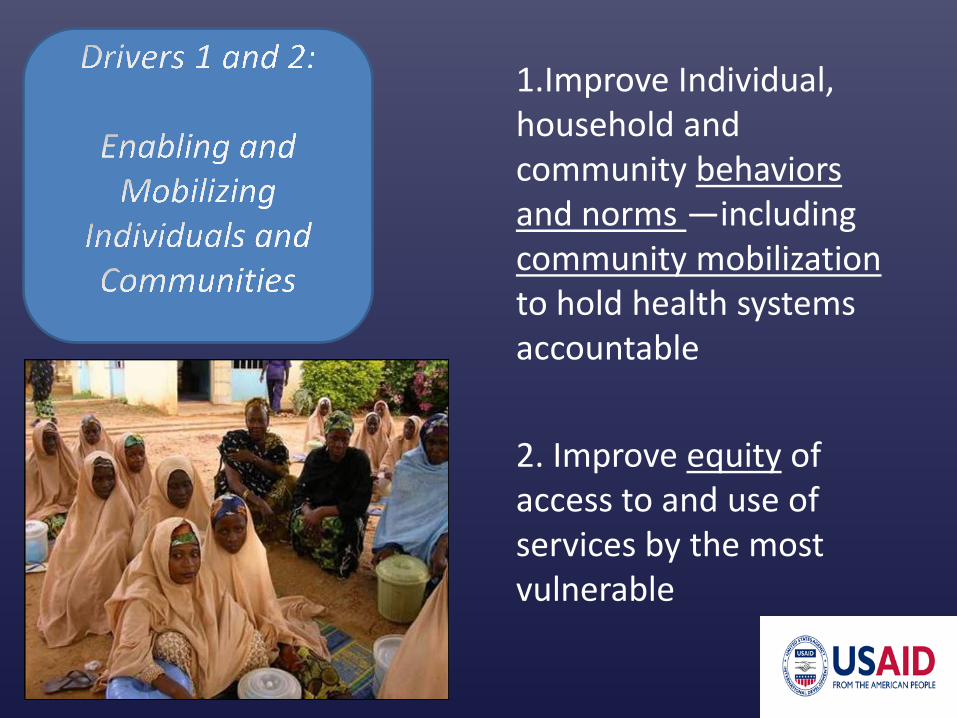
1.Improve Individual, household and community behaviors and norms —including community mobilization to hold health systems accountable 2. Improve equity of access to and use of services by the most vulnerable

Despite progress in coverage of maternal health services, economic disparities are significant

Address the knowledge/ information barrier
• Health education that imparts knowledge through dialogue and problem solving • Provided through community participation or empowerment
approaches in which communities are actively involved in shaping their health
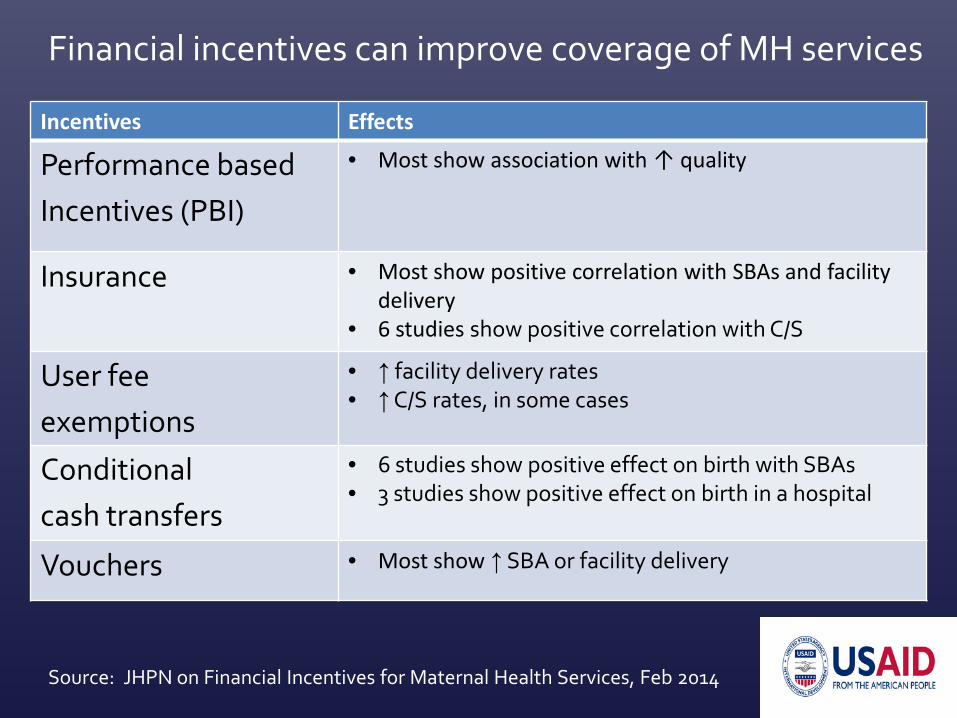
Financial incentives can improve coverage of MH services
Incentives Effects
Performance based Incentives (PBI)
• Most show association with ↑ quality
Insurance • Most show positive correlation with SBAs and facility delivery
• 6 studies show positive correlation with C/S
User fee exemptions
• ↑ facility delivery rates • ↑ C/S rates, in some cases
Conditional cash transfers
• 6 studies show positive effect on birth with SBAs • 3 studies show positive effect on birth in a hospital
Vouchers • Most show ↑ SBA or facility delivery
Source: JHPN on Financial Incentives for Maternal Health Services, Feb 2014

3. Strengthening integration of maternal services with family planning 4. Scale up quality maternal and fetal health care 5. Prevent diagnose and treat indirect causes of maternal mortality and poor birth outcomes 6. Increase focus on averting and addressing maternal morbidity and disability 7. Advance choice and respectful maternity care – and improve working conditions for providers
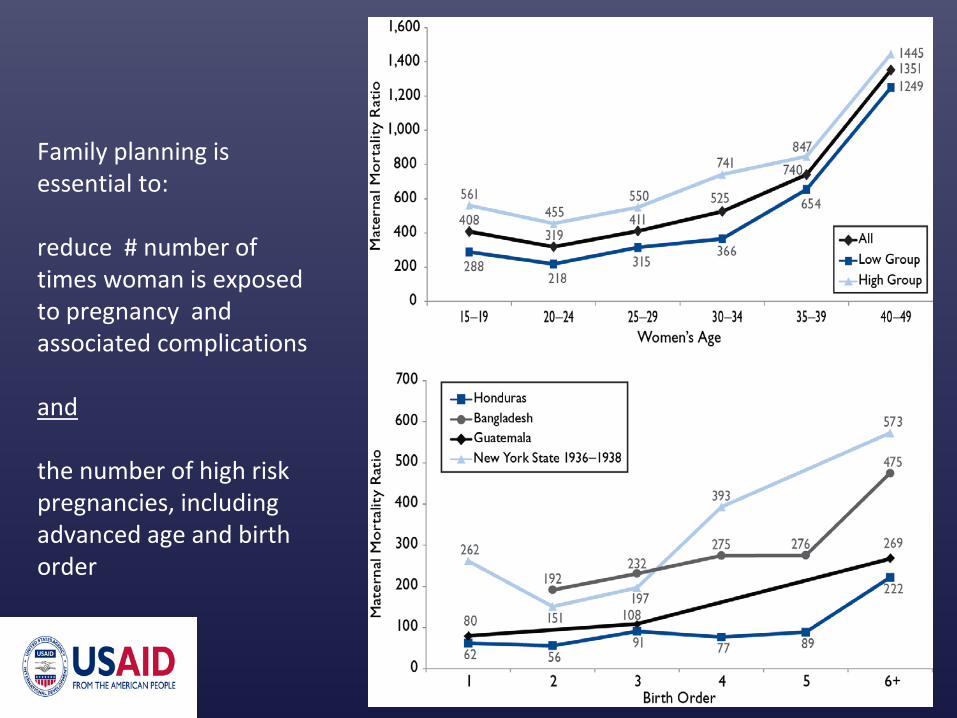
Family planning is essential to: reduce # number of times woman is exposed to pregnancy and associated complications and the number of high risk pregnancies, including advanced age and birth order

Reducing maternal and fetal mortality & morbidity requires quality care for prevention, complication identification, and prompt treatment
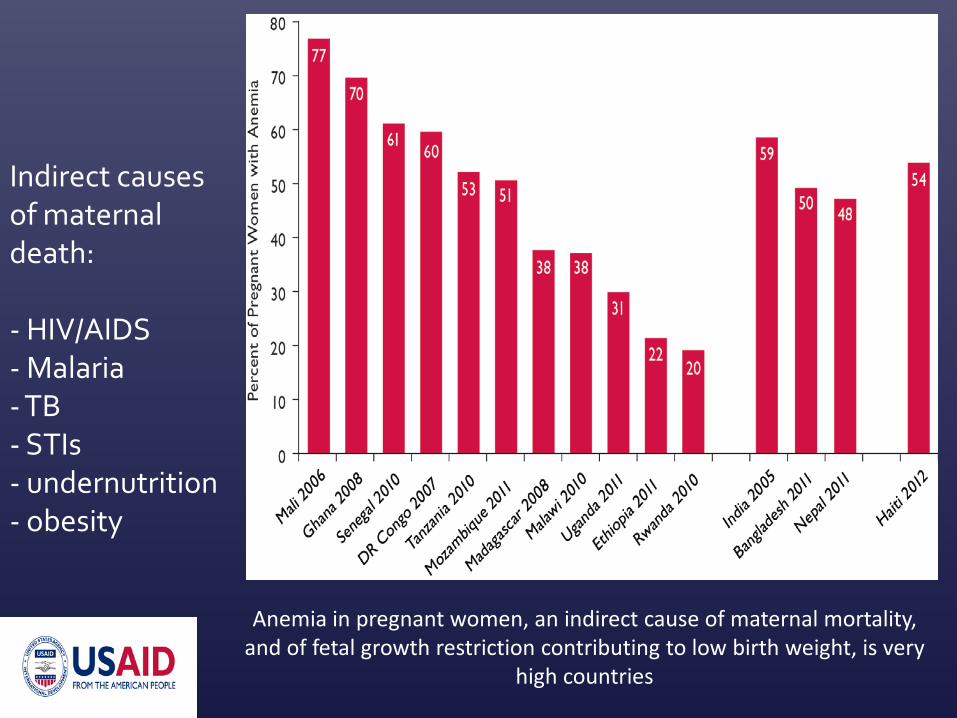
Indirect causes of maternal death: - HIV/AIDS - Malaria - TB - STIs - undernutrition - obesity
Anemia in pregnant women, an indirect cause of maternal mortality, and of fetal growth restriction contributing to low birth weight, is very
high countries

Elements of disrespect and abuse…
• Lack of informed consent • Lack of confidentiality • Discrimination • Physical Abuse • Undignified Care → Humiliation • Abandonment of Care • Demand for payments → Detention in Facilities
Disrespect and abuse of women in childbirth has been reported in every
region of the world – it is a human rights and a quality
of care issue

8. Strengthen and support health systems 9. Promote data for decision-making and accountability 10. Promote innovation and research for policy and programs

Use of private sector care for childbirth, Asia, Decade 2000-2012
Beyond the health system “pillars”, we need to understand and work within evolving contexts including: -- urbanization -- privatization -- decentralization
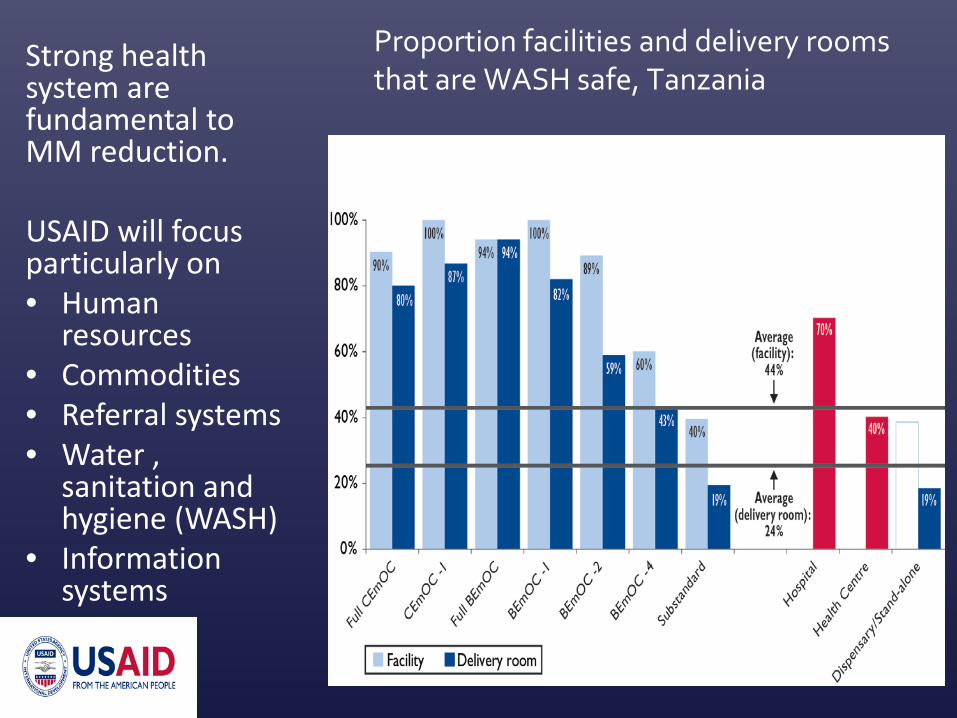
Proportion facilities and delivery rooms that are WASH safe, Tanzania
Strong health system are fundamental to MM reduction.
USAID will focus particularly on • Human
resources • Commodities • Referral systems • Water ,
sanitation and hygiene (WASH)
• Information systems

Barrier to care: Lack of data for decisions and accountability

Ghana substantial regional variation, with Upper East and Volta regions with highest mortality ratios
Innovation New technology to report, analyze and display subnational data to propel problem solving and decisions

Baseline 2013
Target 2020
ANC x 1 80% 90%
ANC x 4 44% 65%
SBA 51% 60%
Facility delivery 34% 60%
Facility delivery, rural 25% 45%
Facility deliver, 2 lowest wealth quintiles
7% 20%
Cesarean section, rural 3.7% 5%
Cesarean section, 2 lowest wealth quintiles
0.87% 3.5%
PNC within 2 days of birth, regardless of location
38.7% 55%

Annual Burden of Maternal and Newborn Mortality and Morbidity
Beyond maternal mortality… to maternal and fetal health
… Mahmoud Fathalla