primary eye care manual
TRANSCRIPT

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 1/81
Interprofessional Fostering of Ophthalmic Care for Underserved Sectors
a non-profit organization promoting “eye care for all"
Primary Eye Care and Training Manual
reaching out to
eople and
rograms near
and far to
romote healthy
eyes and
clear vision
or all

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 2/81
a non-profit organization promoting “eye care for all" Interprofessional Fostering of Ophthalmic Care for Underserved Sectors
Named “Outstanding Project 1998” by the American Public Health AssociationVision Care Section
Member of World Health Organization Partnership Committee of Non-governmentalOrganizations dedicated to the Preventionof Blindness
Dr. Ian Berger President
InFOCUS
19728 Saums Rd., PMB #136Houston, Texas 77084Ph: 281 398 7525Fax: 281 398 7428
Email: [email protected] Website: www.infocusonline.org

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 3/81
ACKNOWLEDGEMENTS
Ms. Diane Baker Dr. Ian B. Berger Ms. Mary DipboyeMs. Del GarciaDr. Simon Gould
Ms. Diana GrigsbyDr. Jean-Paul HeldtMs. Jillian HopewellDr. Ravi KankariaMs. Barbara KazdanDr. Christoph Lengwiler Dr. Valerian LyimoDr. Patrick McColloster Dr. Kavita MistryMs. Vasu MistryDr. Nghiem Pham
Ms. Jan RuebMs. Victoria SheffieldDr. Larry SpitzbergDr. Scott SwannDr. Jerry Vincent
And the students of theUniversity of HoustonCollege of Optometry
Overall objective of this training seminar is to:
Promote a high standard of practice for all engaged in primary eye care, especially for non-eye care professionals and volunteers
working with medically underserved and economically disadvantaged populations

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 4/81

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 5/81
“Primary Eye Care Training and Reference Manual”Contents
Introduction ..............................................................................................1
Module 1 Eye Anatomy, Functions & Common Sight
Problems ................................................................................................5 Anatomy of the Eye ....................................................................................6
How the Eye Works ....................................................................................8
Common Sight Problems............................................................................9
• Visual Acuity
• Refractive Errors
• Other Problems
Professional Eye Exams...........................................................................11
• Recommended Schedule and Benefits
Module 2 Vision Assessment ...........................................................................13
Protocol for Primary Eye Care Examination .............................................13
Patient Record Form ................................................................................14
Visual Acuity Charts .................................................................................15
• Measuring Distance Vision..................................................................16
• Measuring Near Vision........................................................................17
• Pinhole Occluder.................................................................................19
Screening for Binocular Dysfunction.........................................................20
Screening for Coordinated Eye Movement...............................................21
Screening for Limitations of Visual Field...................................................22 Screening Color Vision.............................................................................23
Screening for Acanthosis Nigricans..........................................................24
Measuring Refractive Errors using FOCOMETER® .................................25
• FOCOMETER® Fact Sheet ................................................................25
• How to Read FOCOMETER® .............................................................26
• Using FOCOMETER® for Refractive Error.........................................28
• Using FOCOMETER® for Astigmatism Error......................................30
• Clock Target........................................................................................33
• Care and Maintenance........................................................................34
Module 3 Eye Health and Safety ......................................................................35
Preventive Practices.................................................................................35
Basic Primary Eye Care Techniques........................................................36
Module 4 Eye Injuries & Disease .....................................................................39
Assessing Eye Conditions........................................................................39
Common Eye Diseases............................................................................42
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 6/81
Module 5 Referrals ...............................................................................................47
Criteria for Referring Patients to Eye Care and
Medical Care Professionals ................................................................47
Referral Procedure...................................................................................47
Module 6 Dispensing Eyeglasses...................................................................49
Eyeglass Frames & Lenses......................................................................49
Customized vs. Recycled Glasses...........................................................50
Protocol for Dispensing Customized Glasses ..........................................51
Recycled Eyeglasses – Sorting & Inventory.............................................52
Protocol for Dispensing Recycled Glasses...............................................53
Protocol for Dispensing Reading Glasses................................................54
Using FOCOMETER® to Neutralize the Corrective Power of Lenses.......55
Using Spherical Equivalent to Correct for Astigmatism ............................57
Sources of Inexpensive Eyeglasses ........................................................59Procedure for orienting cylinder axis when assembling
Instant Eyeglasses™ .........................................................................60
Measuring Pupillary Distance (PD) .........................................................61
How to Read a Prescription......................................................................62
Module 7 Record Keeping .................................................................................63
Maintaining Clinical and Fiscal Records...................................................63
Appendix
Glossary...................................................................................................65
Eye Care Websites ..................................................................................69
Equipment / Materials List for Primary Eye Care......................................73

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 7/81
1
Introduction
Introducing InFOCUSInFOCUS (Interprofessional Fostering of Ophthalmic Care for Underserved Sectors) began in 1987 asan outreach project of the University of Houston College Optometry. The project produced theFOCOMETER®, an affordable refracting device appropriate to areas without access to professionapersonnel, electricity or costly equipment. This device became the centerpiece of a unique program
designed to help medically underserved communities achieve self-reliance for basic vision care.
In 1995 InFOCUS was chartered as a non-profit 501c3 organization with a mission to provide eye careto all populations, beginning with those most in need and hardest to serve due to poverty or geographicremoteness. Its strategy is to train local service providers to provide primary eye care. Its goals are toimprove vision, prevent blindness and promote health.
Why is InFOCUS Needed? As many as 900 million children and adults in the world today are visually impaired due to refractiveerrors that could be corrected by prescription eyeglasses. The World Health Organization estimatesthat 75% of the world’s blindness could be prevented or treated. Toward that goal, InFOCUS helpslarge, medically isolated populations acquire basic vision services and the capacity to link patients toprofessional care.
What Does InFOCUS Do?Working with health care providers and other agencies serving low-income communities InFOCUS
• Fosters sustainable, community-based eye care services
• Promotes eye health through education
• Helps disadvantaged people gain access to basic vision services and preventive health education
In the United States, InFOCUS trains health and social service providers and community volunteers topromote preventive practices, assess vision, and refer patients to qualified practitioners for eye examsand eyeglass prescriptions. InFOCUS helps its program partners set up “vision stations” offering low-cost, quality eyeglasses to individuals who could otherwise not afford them. InFOCUS also trains andequips clinicians and volunteers to offer eye care on short-term mission trips.
In other countries, InFOCUS provides the technology, training, and an initial supply of low-cost lensesand frames to help communities set up vision stations. Community eye care providers measurerefractive errors, dispense glasses, and use the proceeds of spectacle sales to defray operating costs.
InFOCUS works with program partners to
• Establish and sustain a vision station
• Provide an appropriate standard of care
• Provide health education to promote the prevention of eye and other diseases
• Refer patients with serious eye conditions to appropriate medical resources
The InFOCUS Center for Primary Eye Care Development
Based in Houston, Texas, the InFOCUS Center for Primary Eye Care serves as the hub of globaefforts to expand access to vision care. Working with universities, professionals and healthorganizations, the Center
• Provides training, information resources and technical assistance to service providers
• Promotes awareness of primary eye care needs and program strategies
• Fosters research on clinical methods and technologies
• Initiates and participated in collaborative projects; and
• Develops and implements programs to respond to critically unmet needs.
InFOCUS reaches out to people and programs near and far to promote healthy eyes and clear visionfor all.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 8/81
2
Primary Eye Care and FOCOMETRY
Primary eye care is considered the “first encounter” with eye care. Often, the only eye careoffered to many people in poor and rural communities is a vision screen. About one billionpeople need an eye exam but do not have access to an eye care provider.
The Need for Eyeglasses
One of the most widespread eye problems is simply the need for eyeglasses. At least 900million people in the world today need a correction for visual refractive errors (i.e., needeyeglasses). However, many are unable to obtain a prescription because of geographic or financial barriers. Despite abundant good will on the part of eye care professionals andmedical institutions to reach out beyond their usual service areas to individuals andpopulations in need, only a tiny fraction of the need is being met.
FOCOMETER ® Key to Removing Barriers
The FOCOMETER
®
is helping people to gain access to basic vision care. Because theFOCOMETER® is an accurate, affordable, and easy-to-use tool for measuring refractiveerrors, it is being used in 40 countries with medically underserved populations, includingcommunities in remote locations. InFOCUS is training and equipping health workers andnon-medical volunteers to measure refractive errors and dispense appropriate eyeglasses.
As a result, the burden of poor vision has been lifted from many people around the world.
The FOCOMETER® requires no electricity and has been found to be as accurate as the autorefractor in field trials that have been published in scientific journals. The FOCOMETER® enables the measurement of refractive errors of patients who need eyeglasses, and can alsobe used to determine the corrective power of prescription eyeglasses (neutralization).

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 9/81
3
Uses for This Manual
Primary Eye Care Assessment:
1. Measuring visual acuity, screening for binocular dysfunction and color vision
problems;2. Determining which patients have refractive errors and need eyeglasses;
3. Recognizing symptoms of eye diseases;
4. Determining prescriptions for eyeglasses using Focometry;
5. Promoting eye health; and
6. Making appropriate referrals.
Eyeglass Dispensing:
1. Managing and dispensing recycled eyeglasses;
2. Dispensing customized glasses;
3. Using a spherical equivalent for dispensing glasses to patients with astigmatic error;and
4. Maintaining clinical and fiscal records.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 10/81
4
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 11/81
5
Module 1 – Eye Anatomy, Functions & CommonSight Problems
Introduction to Anatomy of the Eye
The human eye is truly one of the most remarkable organs in the body. The sense of vision requires a light receptor (the eye), a pathway by which nerve impulses are conveyed(the optic nerve), and an area in the brain (the visual cortex) that transforms the nerveimpulses into images of color and form.
External Structure
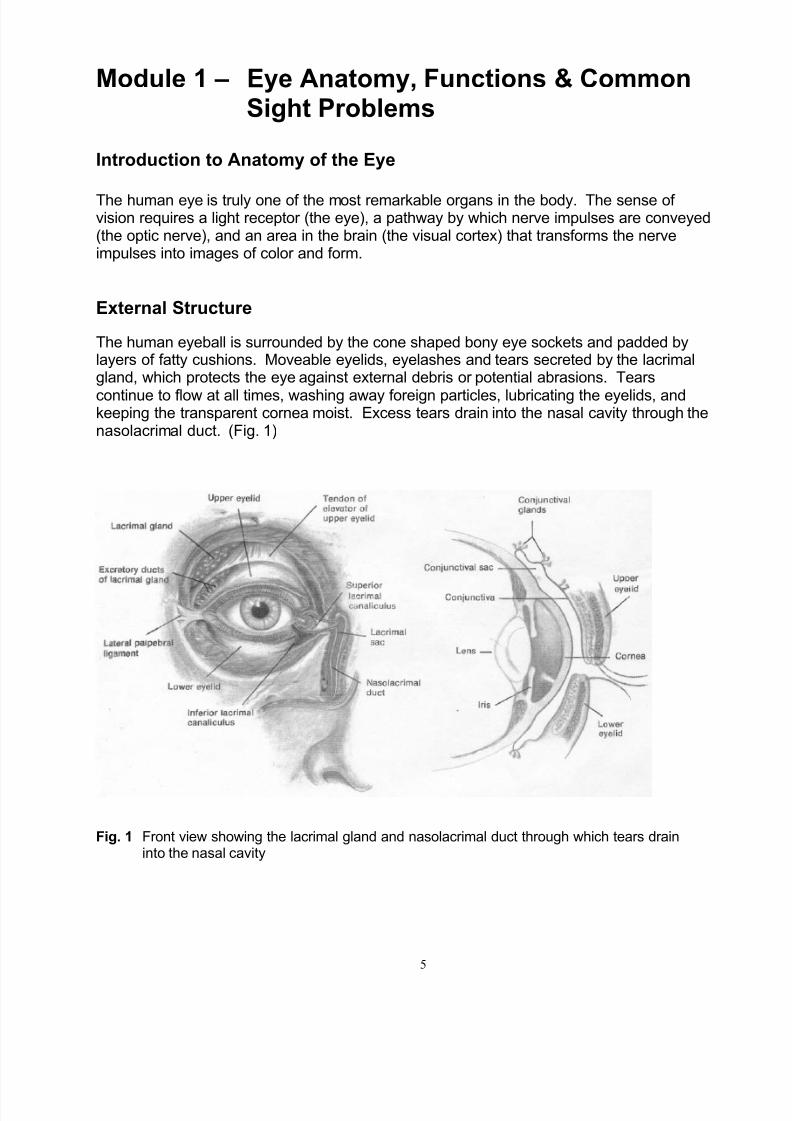
The human eyeball is surrounded by the cone shaped bony eye sockets and padded bylayers of fatty cushions. Moveable eyelids, eyelashes and tears secreted by the lacrimalgland, which protects the eye against external debris or potential abrasions. Tears
continue to flow at all times, washing away foreign particles, lubricating the eyelids, andkeeping the transparent cornea moist. Excess tears drain into the nasal cavity through thenasolacrimal duct. (Fig. 1)
Fig. 1 Front view showing the lacrimal gland and nasolacrimal duct through which tears draininto the nasal cavity
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 12/81
6
Anatomy of the Eye
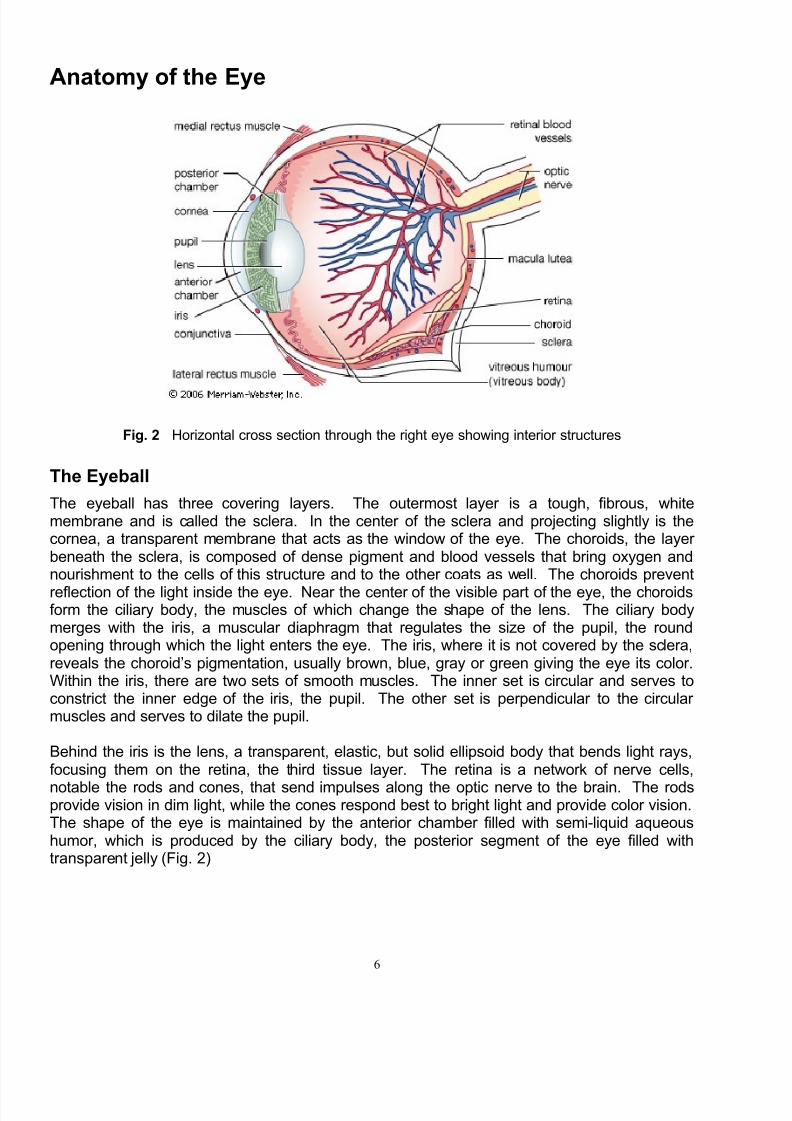
Fig. 2 Horizontal cross section through the right eye showing interior structures
The Eyeball
The eyeball has three covering layers. The outermost layer is a tough, fibrous, whitemembrane and is called the sclera. In the center of the sclera and projecting slightly is thecornea, a transparent membrane that acts as the window of the eye. The choroids, the layer beneath the sclera, is composed of dense pigment and blood vessels that bring oxygen andnourishment to the cells of this structure and to the other coats as well. The choroids prevent
reflection of the light inside the eye. Near the center of the visible part of the eye, the choroidsform the ciliary body, the muscles of which change the shape of the lens. The ciliary bodymerges with the iris, a muscular diaphragm that regulates the size of the pupil, the roundopening through which the light enters the eye. The iris, where it is not covered by the sclera,reveals the choroid’s pigmentation, usually brown, blue, gray or green giving the eye its color.Within the iris, there are two sets of smooth muscles. The inner set is circular and serves toconstrict the inner edge of the iris, the pupil. The other set is perpendicular to the circular muscles and serves to dilate the pupil.
Behind the iris is the lens, a transparent, elastic, but solid ellipsoid body that bends light rays,focusing them on the retina, the third tissue layer. The retina is a network of nerve cells,
notable the rods and cones, that send impulses along the optic nerve to the brain. The rodsprovide vision in dim light, while the cones respond best to bright light and provide color vision.The shape of the eye is maintained by the anterior chamber filled with semi-liquid aqueoushumor, which is produced by the ciliary body, the posterior segment of the eye filled withtransparent jelly (Fig. 2)

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 13/81
7
Eye Muscles
The movement of the eyes are controlled by the six extra ocular muscles. These musclesoriginate on the bones of the orbit and insert on the eyeball itself. Three pairs of striatedextra ocular muscles are responsible for each movement. Four of the muscles areattached to the superior, inferior, medial, and lateral surfaces of the eyeball and are namedaccordingly: superior rectus, inferior rectus, medial rectus and lateral rectus. They cause
the eyeball to turn up, down, inward, outward, respectively. The two remaining muscles arecalled superior and inferior obliques and they act alone to rotate the eyeball. (Fig. 3)
Fig. 3 Extraocular muscles of the eye

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 14/81
8
How the Eye Works
Your eyes and brain work together to make it possible for you to see. Light is reflected fromobjects onto the front surface of your eye, the cornea. The cornea bends the light, which thenpasses through fluid called the aqueous humor, through the pupil, and to the lens. The lens,which can change its shape, helps to focus light onto the retina at the back of the eye. On the
retina, light forms an upside-down image on the cones and rods, the light sensitive receptors inthe eye. The cones and rods send images to the brain via the optic nerve.
Shortly after leaving the eye, the optic nerves from each eye cross and separate, sending their fibers to receiving and analytical stations in the brain. In effect, the brain receives messagesfrom both eyes. Besides interpreting the visual input, if movement of both eyes is coordinated,the brain fuses images from each eye together to form one three-dimensional image.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 15/81
9
Common Sight Problems
Visual Acuity
Normal(Emmetropia)
Sight - Objects appear clear from a distance of 20’ (or 6 meters) and atreading distance.Cause - Lenses of the eye can change shape, for the purpose of converginglight rays on the retina at the back of the eyeball, also called ‘accommodation’.
This capability enables clear vision at close range.
Refractive Errors
Farsightedness(Hypermetropia)
Sight - Difficulty seeing up close. In some cases, difficulty seeing at adistance.Cause - Eyeball is either shorter or smaller than average. Not a disease.Light rays do not converge at retina but rather at an angle that converges inback of retina.Corrective lenses – If only farsighted correction is needed, then sphericallenses will correct the refractive error. If patient is farsighted plus astigmatic,then compound lenses are needed. Compound lenses combine both spherical
and cylindrical correction.*
Nearsightedness(Myopia)
Sight - Difficulty seeing at a distance.Cause - The eyeball is longer or larger than average. Not a disease. Lightrays converge in front of the retina, rather than on the retina.Corrective lenses – If only nearsighted, then a spherical lens will correct. If patient is nearsighted plus astigmatic, then compound lenses containing bothspherical and cylindrical corrections are needed. *
Astigmatism
Sight - Difficulty seeing some objects while other objects are seen clearly.Difficulty seeing objects near and far.Cause –Non-round cornea results in uneven refraction of light.Corrective Lens –Cylinder. When patient is either near or farsighted thencompound lenses will be used that combine cylindrical and spherical
correction. *
Other Problems
Presbyopia
Sight – Difficulty seeing objects placed near the eyeCause – Loss of elasticity of the focusing lens inside the eye (loss of accommodation), commonly begins when patients reach their 40’s.Corrective Lens –If correction needed for reading or close work only, thenmagnification will be added to a spherical lens. When patients have blurreddistance vision in addition to presbyopia and want to wear glasses for bothnear and distance vision, then bifocals will be prescribed.
Binocular
Misalignment(Strabismus)
Sight –Double vision or suppressed vision in one eye.Cause – Poor coordination of muscles that move the eyes or inability to fuse
images from two eyes.Corrective Techniques –Vision training, glasses with prism components,surgery. Treatment before age six is important.
Color VisionDeficiency
Sight – Inability to see some colors, most commonly red and green.Cause – Usually genetic in origin. Affects 1 out of 8 males and 1 or 30females.Corrective Techniques – none unless due to either pathology or medication.
*When compound lenses are not available, then spherical lenses may be substituted which contain an additionalcorrection beyond the amount required to correct the patient’s nearsightedness. See “Using SphericalEquivalent” in Module 6.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 16/81
10
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 17/81
11
Professional Eye Exams
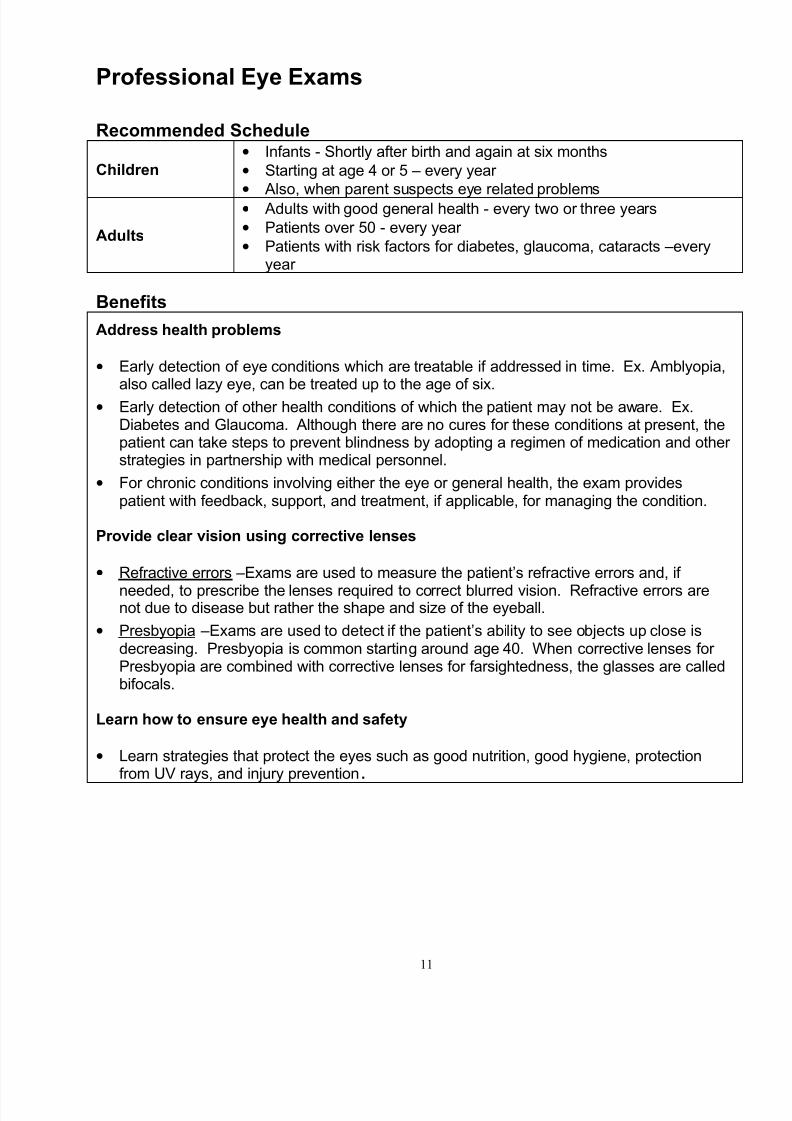
Recommended Schedule
Children• Infants - Shortly after birth and again at six months
• Starting at age 4 or 5 – every year
•
Also, when parent suspects eye related problems
Adults
• Adults with good general health - every two or three years
• Patients over 50 - every year
• Patients with risk factors for diabetes, glaucoma, cataracts –everyyear
Benefits
Address health problems
• Early detection of eye conditions which are treatable if addressed in time. Ex. Amblyopia,also called lazy eye, can be treated up to the age of six.
• Early detection of other health conditions of which the patient may not be aware. Ex.Diabetes and Glaucoma. Although there are no cures for these conditions at present, thepatient can take steps to prevent blindness by adopting a regimen of medication and other strategies in partnership with medical personnel.
• For chronic conditions involving either the eye or general health, the exam providespatient with feedback, support, and treatment, if applicable, for managing the condition.
Provide clear vision using corrective lenses
• Refractive errors –Exams are used to measure the patient’s refractive errors and, if
needed, to prescribe the lenses required to correct blurred vision. Refractive errors arenot due to disease but rather the shape and size of the eyeball.
• Presbyopia –Exams are used to detect if the patient’s ability to see objects up close isdecreasing. Presbyopia is common starting around age 40. When corrective lenses for Presbyopia are combined with corrective lenses for farsightedness, the glasses are calledbifocals.
Learn how to ensure eye health and safety
• Learn strategies that protect the eyes such as good nutrition, good hygiene, protectionfrom UV rays, and injury prevention.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 18/81
12

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 19/81
13
Module 2 – Vision Assessment
Protocol for Primary Eye Care Examination*
When to Use: • Examiner is assessing vision in a Vision Station, at a health center or in the field.
• Examiner may be trained to perform basic first aid.
1ReviewPatientHistory
• Record patient history on Patient Record form.
• Determine time of last professional eye exam.
• Ask patient if he/she is taking any medications
• Ask patient if he/she has concerns or questions.
2Assess Visual
Acuity
• Check distance vision and near vision. See procedures on pages 16-17.Record results on Patient Record form.
• If both distance AND near vision are clear (20/30 or better for distance vision),then skip step 4 with adult patients. In the case of children, include step 4 in allexams. Children have a strong ability to focus their eyes and yet may have
refractive errors that could be corrected with lenses.• If either distance OR near vision is blurred (worse than 20/30 for distance vision),
then conduct pinhole test on page 19 and record.
• If vision improves during pinhole test, be sure to include step 4
• If vision does not improve, skip step 4.
3Screen for Binocular Dysfunction
• Cover Test and Versions Test. See pages 20 and 21
• Record results on form.
4MeasureRefractive Errors
• Use FOCOMETER®
to determine eyeglass prescription needed, if any. For correcting refractive errors, including astigmatism, see pages 30 and 31. Recordresults on form.
5Check eye for disease or injury
• Check all eye and surrounding structures for evidence of disease or trauma.See Module 4, “Eye Injuries and Diseases”.
• Screen for color vision defects. Procedure on page 23.
• Examine nape of neck for Acanthosis Nigricans (Type II Diabetes).Procedure on page 24.
• If problem(s) is identified, then record on form and refer.
6Give eye healthand safetyinformation
• Provide information on hygiene, nutrition, UV protection, and injury prevention.See Module 3, “Eye Health and Safety.”
7Make referral asneeded
• Review “Criteria for Referring Patients to Eye Care Professional” and make areferral if any of the criteria is met. See Module 5, “Referrals”.
.
8Wrap-upInterview
• Review findings of exam with patient. If giving a referral, give patient the reason.Discuss the patient’s concerns and questions.
• Schedule next appointment with patient. Encourage patient’s family and friendsto make appointments. (See schedule recommendation on page 11.)
• Complete “Patient Record” form and retain in patient files.
*In the United States, prescriptions for corrective lenses can only be filled if written by either an optometristor ophthalmologist. InFOCUS advises anyone providing vision services to respect all regulations applicableto the area in which services are provided.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 20/81
14
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 21/81
15
Visual Acuity Charts
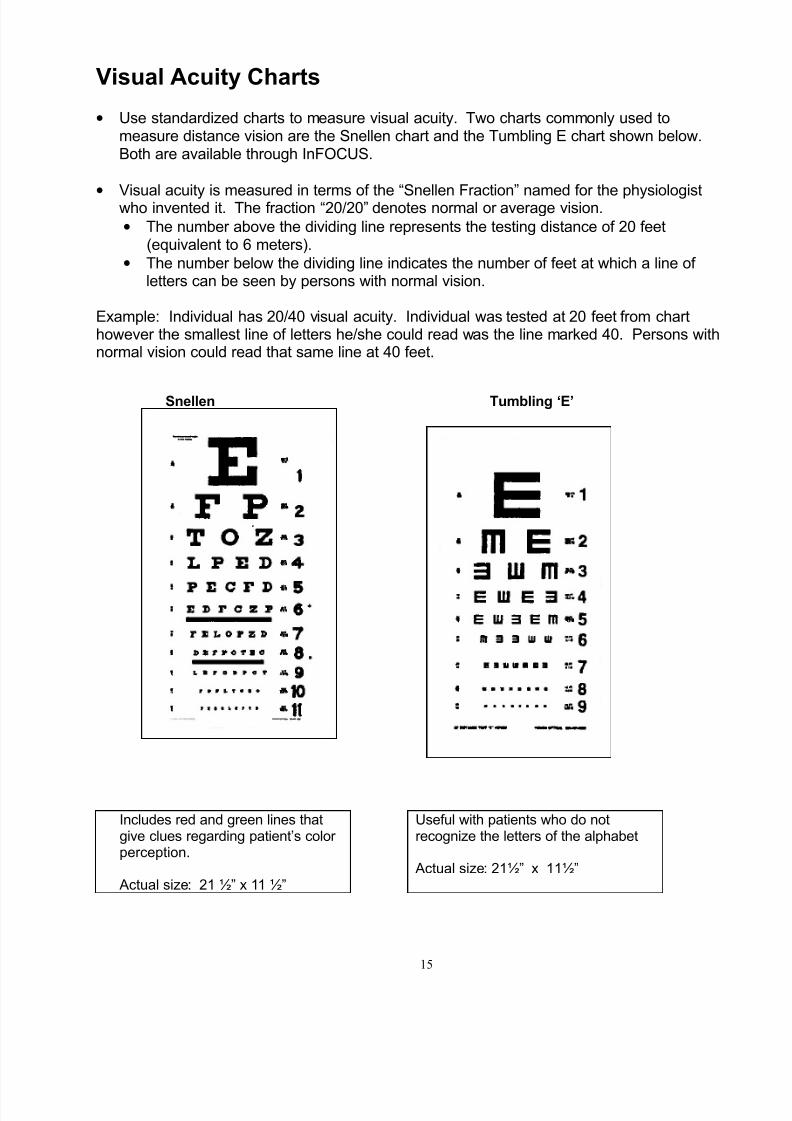
• Use standardized charts to measure visual acuity. Two charts commonly used tomeasure distance vision are the Snellen chart and the Tumbling E chart shown below.Both are available through InFOCUS.
•
Visual acuity is measured in terms of the “Snellen Fraction” named for the physiologistwho invented it. The fraction “20/20” denotes normal or average vision.
• The number above the dividing line represents the testing distance of 20 feet(equivalent to 6 meters).
• The number below the dividing line indicates the number of feet at which a line of letters can be seen by persons with normal vision.
Example: Individual has 20/40 visual acuity. Individual was tested at 20 feet from charthowever the smallest line of letters he/she could read was the line marked 40. Persons withnormal vision could read that same line at 40 feet.
Snellen Tumbling ‘E’
Includes red and green lines thatgive clues regarding patient’s color perception.
Actual size: 21 ½” x 11 ½”
Useful with patients who do notrecognize the letters of the alphabet
Actual size: 21½” x 11½”
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 22/81
16
Procedure: Measuring Distance Vision
Purpose: To determine the smallest line of letters the patient is able to read at a specified distancewith each eye. Children, starting at age 4, can take this test as well as adults.
Illumination: Make sure the eye chart is well lit and no reflection is coming off the chart.
Target: Snellen Chart (Ex. Letters, Tumbling E, numbers, pictures, Landolt C). See examples onpage 15.
Distance: 20’ or 6 meters from chart to patient
Lenses: Patient first reads chart without corrective lenses. Test is repeated with patient wearingcorrective lenses as needed.
Equipment: Opaque Occluder
Form: Patient Record form and pencil to record results
Instructions toPatient:
If patient is wearing prescription glasses, then ask him/her to take them off.Explain to patient that you will indicate the letters (numbers, Tumbling E’s, etc.) ondifferent lines of the chart one at a time. He/she should tell you what they see. In thecase of Tumbling E charts, it is helpful to give the patient a large cut out letter “E” and askthem to respond by turning the letter to match the direction of the letter they see on thechart. (This method works well when the examiner and patient do not speak the samelanguage.)
Steps: 1. Test right eye first. Cover left eye with occluder. Be sure that patient is using only the right eye.2. Test vision by starting with the largest letters first. Proceed down the chart to the smallestletters the patient can see. It is advisable to skip lines so as to identify the smallest line that thepatient can read.
3. Record the smallest line in which the patient can see at least half of the letters. See Recordsection below.
4. Repeat the test with the left eye.5. Repeat the test with patient wearing his/her corrective lenses.6. If patient cannot see largest letters, then follow the procedure in Notes section.
Interpretation of Test Results: • Normal Vision: 20/30 or better* • Subnormal Vision: worse than 20/30
• Blindness: 20/400 or less
*Patient may benefit from glasses, if available. 20/30 or better is an “acceptable” level of visual acuity but withthe proper resources vision may still be improved.
Notes:If the patient cannot read the largest letters, then use the following test sequence. Failure at one level of thetest requires testing at the next level.
1. Ask the patient to walk toward the chart and report when the largest letter is legible. The distance fromthe chart would be the number of the acuity fraction, i.e. 3/400.
2. The patient is seated and asked to count the examiner’s hand. Record as “finger counting at 3 feet.”3. Ask the patient to tell whether the examiner’s hand is moving or still. Record as “hand movement at 3 feet.”4. The patient is asked to indicate whether a light source is on or off. If the patient is accurate, it is recorded
as “light perception”; if not, “no light perception.”
Record:The patient’s visual acuity is measured for the right eye, left eye and both eyes. Visual acuity is recorded inone of the following ways:
1. Smallest line patient can read at least half of the letters along with number of letters missed on that line.Ex. 20/40 –2 --or--
2. Smallest line patient can read completely, along with the number read correctly on that next line.Ex. 20/20 + 2 i.e. patient can read all the letters on the 20/20 line and can also read 2 letters on the20/15 line. So credit is given for the 2 letters read on the line below the 20/20 line.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 23/81
17
Procedure: Measuring Near Vision
Purpose: To assess visual acuity using objects at a reading distance. This procedure isused with adults and children, starting at age 4.
Illumination: Make sure the eye chart is adequately lit and that no reflection is coming off thechart.
Target: Near Point Card (Reduced Snellen chart) or usual reading material. Young
children may require a card with symbols (drawings of animals etc.) withoutletters.
Distance: 14” - 16” or normal distance for patient to use when he/she reads or works atclose range
Lenses: First test without corrective lenses and then with corrective lenses.
Equipment: Opaque Occluder
Form: Patient Record form and pencil to record results.
Instructions toPatient:
If patient is wearing corrective lenses, then ask him/her to take them off. Ask patient to read the Near Point Card (Reduced Snellen chart) or readingmaterial at 14” – 16” with one eye at a time, then with both eyes. Repeatwearing glasses.(Hyperopes, persons with blurred near vision, cannot see close without them.)
Steps: Using Near Point Card
1. Test right eye first. Cover left eye with occluder. Be sure that patient is using only the right eye.
2. Test vision by starting with the largest letters first. Proceed down the chart to the smallest lettersthe patient can see. It is advisable to skip lines so as to identify the smallest line that the patientcan read.
3. Record the smallest line in which the patient can see at least half of the letters.
4. Repeat the test with the left eye.
5. If patient wears corrective lenses, have patient wear glasses and repeat steps 1 – 4.
6. Record results on Patient Record form.
Using Other Targets
1. Same as above
2. Test vision by asking patient to hold target at range in which material is clear.
3. If patient reports that he/she cannot clearly see target at any range when holding the target,then record on the form that patient needs magnification lenses to see at near.
4. If patient reports that he/she can see target clearly, ask patient to demonstrate the distance(s).Record on the form the smallest line seen clearly on the Near Point card
Interpretation When using the near point card- When using reading material -of Test Results: Normal Vision = 20/20 normal = able to see familiar reading
Subnormal Vision: Less than 20/20 material without magnificationdepending on age When using non reading material
normal = able to see target atreading distance (approx. 14”-16)
Notes:Nearsighted patients will generally see better at near without glasses. Farsighted patients havedifficulty seeing up close or cannot see at all up close without their glasses. Therefore, patientsshould be tested both with and without their glasses. Presbyopes who are also myopic may beable to see clearly at near while not wearing their prescription for distance.
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 24/81
18
Near Vision Assessment
The smallest type (4.5 pt. type) on a near point card should be seen clearly through theindividual’s prescription glasses, or without glasses for those with 20/20 vision, when thecard is viewed at 14 inches in moderate lighting conditions. In order to see the small typeclearly, older adults may need to increase the distance between the eyes and the card, or
use magnification (plus power lenses). Plus lenses may be an “add” applied to the distanceprescription with bifocal eyeglasses, or reading glasses may be indicated for those notneeding a distance prescription.
To find the appropriate power of lenses to dispense to adult patients, refer to the section‘Protocol for Dispensing Reading Glasses’ in this manual. For children, dispense the lowestpower of lenses that offer the best clarity when the card is viewed at 14 inches.
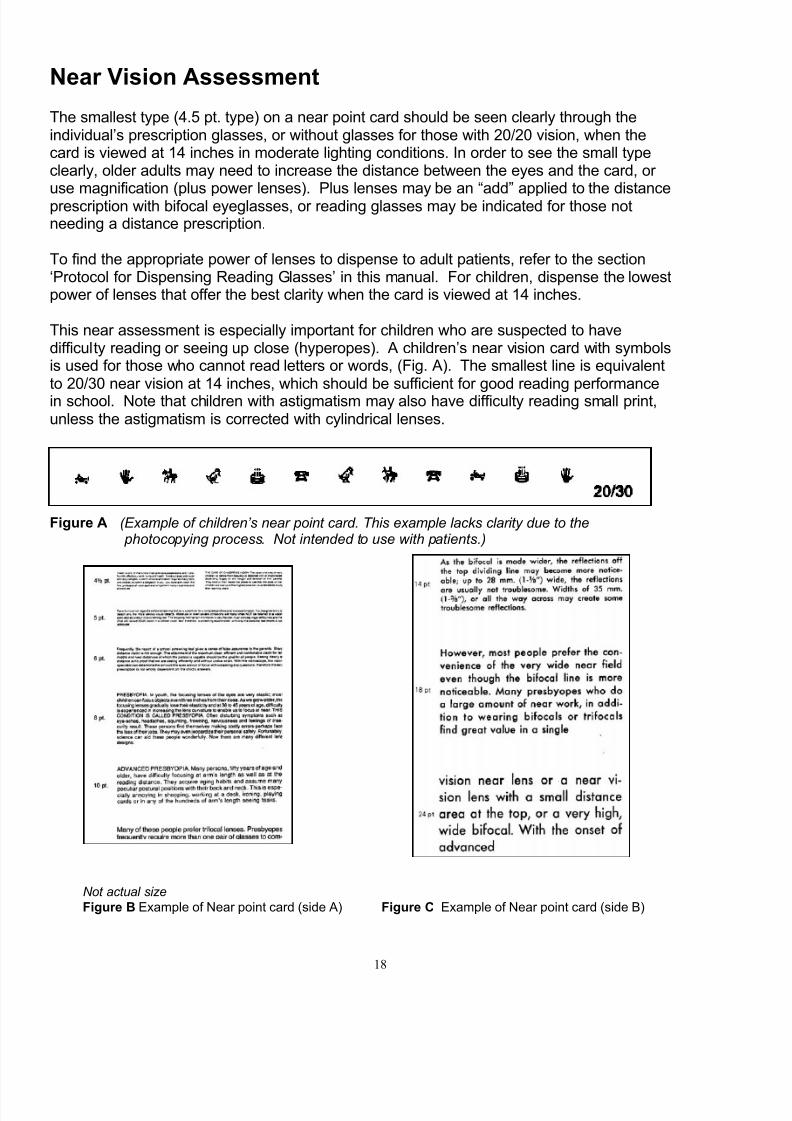
This near assessment is especially important for children who are suspected to havedifficulty reading or seeing up close (hyperopes). A children’s near vision card with symbolsis used for those who cannot read letters or words, (Fig. A). The smallest line is equivalentto 20/30 near vision at 14 inches, which should be sufficient for good reading performancein school. Note that children with astigmatism may also have difficulty reading small print,unless the astigmatism is corrected with cylindrical lenses.
Figure A (Example of children’s near point card. This example lacks clarity due to the photocopying process. Not intended to use with patients.)
Not actual size Figure B Example of Near point card (side A) Figure C Example of Near point card (side B)

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 25/81
19
Procedure: Pinhole Occluder Test
Purpose:
To determine if patient’s visual acuity would be improved usingcorrective lenses.Improved sight when viewing through the occluder indicates patientwould benefit from corrective lenses.
Illumination:Make sure the eye chart is well lit and that no reflection is coming off the chart.
Target: Standard acuity chart such as Snellen, Tumbling ‘E’, etc.
Distance: 20’ or 6 meters
Lenses: Read without corrective lenses. Repeat wearing corrective lenses.
Equipment: Pinhole occluder
Form: Patient Record form and pencil to record results
Instructions toPatient:
If patient is wearing prescription glasses, then ask him/her to takethem off.
Steps:
1. Test right eye first. Cover left eye with cardboard or cup. Ask patient to read a line onvisual acuity chart such as Snellen or Tumbling ‘E’. Ask patient if his/her sight is thesame through the occluder.
• If improved, then patient could probably benefit from corrective lenses.
• If not improved, then patient would not benefit from corrective lenses.
2. Test left eye.
3. Repeat steps 1 and 2 wearing corrective lenses.
4. Record results on Patient Record form.
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 26/81
20
Procedure: Screening for Binocular Dysfunction(Cover / Uncover Test)
Purpose:
To observe how well the eyes work together. Early detection andtreatment of problems with binocular coordination can preventamblyopia (reduced visual perception). The test for binocular vision iscalled the Cover/Uncover Test. This test should be performed after thevisual acuity test.
Illumination: Ordinary room light
Target: Standard acuity chart such as Snellen, Tumbling ‘E’, etc.
Distance: 20’ (or six meters) from patient to acuity chart
Lenses: Patient wears corrective lenses, if applicable
Equipment: Acuity chart such as Snellen or Tumbling ‘E’
Instructions toPatient:
When asked, fixate on target, don’t move head and don’t look away.
Steps: Cover/Uncover Test
1. Test right eye first. The patient is asked to look at the target, the large “E” on top line of the acuity chart at 20’ and maintain fixation with both eyes.
2. The left eye is then covered while telling the patient not to lose fixation with theuncovered (right) eye. The right eye is observed for movement.
3. Note if any movement is detected, and if possible, indicate whether the movement isconsistently towards the nose, or towards the ear.
4. Test the left eye. Repeat steps 1 –3 with the right eye covered and look at possiblemovement in the left eye.
5. Then repeat for each eye using the near target (examiner’s nose at a distance of 3’ to5’).
6. Any movement of either uncovered eye should be recorded on form and a referralshould be made to an eye doctor for full assessment of binocular function.
7. The examiner records “pass” or “fail” on Patient’s Record form, and those who fail arereferred for a complete eye exam.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 27/81
21
Procedure: Screening for Coordinated Eye Movement(Versions Test)
Purpose:
To observe how well the eyes work together. Early detection andtreatment of problems with binocular coordination can preventamblyopia (reduced visual perception). The test for coordinated eyemovement is called the Versions Test. This test should be performedafter the visual acuity test.
Illumination: Ordinary room light
Target: Standard acuity chart such as Snellen, Tumbling ‘E’, etc.
Distance: Versions – 3’ to 5’ from patient
Lenses: Patient wears corrective lenses, if applicable
Equipment: Acuity chart such as Snellen or Tumbling ‘E’
Instructions toPatient:
When asked, fixate on target, don’t move head and don’t look away
Steps: Versions Test
1. The patient is asked to look at the examiner’s finger and follow the finger with botheyes without moving the head as a wide rectangle is traced through the air. For children,use a puppet.
2. The examiner watches the patient’s eyes, to ascertain that both eyes follow the finger and work together throughout the sideways and up and down movements.
3. Refer to appropriate eye professional if eyes don’t follow together.
4. The examiner records either “unrestricted” or “restricted” on Patient’s Record form.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 28/81
22
Procedure: Screening for Limitations of Visual Field
Purpose: To assess whether limitations are present in the field of vision
Illumination: Ordinary room light
Target: Standard acuity chart such as Snellen, Tumbling ‘E”, etc.
Distance: 1 to 2 feet from patient’s head
Lenses: Patient does not wear corrective lenses
Equipment: Not applicable
Instructions toPatient:
Ask patient to report when fingers are seen and how many fingers arevisible
Steps:
1. Test right eye first. Tell patient to close or cover left eye. Patient stares straight ahead
to the large letter at the top of the acuity chart.
2. Examiner places one of his/her hands behind the patient’s head. With either one or twofingers showing, the examiner brings his/her hand around the side of the patient’s headto the front.
3. Patient reports when the number of fingers is visible and the number seen.
4. Examiner repeats the same movement on the other side of patient’s head. Themovement is repeated two more times
• over patient’s head
• under patient’s head
In this way, each quadrant of the patient’s potential field of vision is tested, one quadrantat a time.
5. Repeat with left eye.
6. Record any difficulties with visual field on Patient Record form. If found, refer to an eyedoctor for a full assessment.
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 29/81
23
Procedure: Screening Color Vision
Purpose:To determine whether a complete color vision assessment isnecessary.
Illumination: Ordinary room light
Target: Color Vision test plates
Distance: Near, about 14” to 16”
Lenses: Patient wears corrective lenses, if applicable
Equipment: Color vision test plates
Instructions toPatient:
Read numbers or letters on test plates and tell examiner
Steps:
1. Patient is instructed to inspect various standardized color vision plates and respond toexaminer’s questions.
2. Examiner asks the patient to say the number or letter seen.
3. If patient makes one or more errors in reading plates or any complaint about color vision, then refer to eye doctor for complete examination.
4. Examiner records either “pass” or “refer” on Patient’s Record.
Notes:
Color Vision PlatesColor vision plates may be ordered from any ophthalmic supply firm. Request pseudo-
isochromatic plates for testing color perception. Care should be taken when handlingthe plates so that they are not smudged with fingerprints. If Color Vision Plates arenot available, test whether the patient correctly identifies the red and green lineson the Eye Chart. Red-green color deficiency is the most common type of color blindness.
Causes of Color BlindnessColor blindness is usually caused by a genetic defect in the cone cells in the retina.If color blindness is detected in only one eye, then cause may be pathology instead of genetics. If color blindness develops, the cause may be medication the patient is taking.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 30/81
24
Procedure: Screening for Acanthosis Nigricans
Purpose:To detect early symptom of Type II Diabetes Mellitus, a major cause of blindness
Illumination: Moderate
Instructions toPatient:
Explain to patient that the back of the neck will be examined.
Steps:
1. Look at the nape (back) of the patient’s neck for a darkened band.
2. Distinguish between birthmarks and Acanthosis Nigricans, which has a raised velvetytexture.
3. If Acanthosis is present, alert the patient that this mark is often an early sign of Type IIDiabetes. Encourage patient to see a doctor to learn how to manage the disease and
prevent blindness. Patient should also have their eyes examined regularly by an eyeprofessional.
4. Examiner records either “pass” or “refer” on patient’s record.
Note: See Diabetic Retinopathy in the Module 4, “Eye Injuries & Diseases”.This darkened band is often mistaken for a birthmark or dirt.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 31/81
25
Measuring Refractive Errors using the FOCOMETER ®
Fact Sheet
The FOCOMETER ® was developed by Drs. Ian Berger and Larry Spitzberg at theUniversity of Houston College of Optometry in Houston, Texas to provide asubjective refraction without the need for electricity or complicated protocol. Theportable, hand-held instrument is highly appropriate for use in poor and remoteareas.
Based on Badal optics, the FOCOMETER® allows the patient to view a real unmagnifiedtarget and bring it into focus, with a direct reading of spherical correction on a linear diopter scale.
Measurement of cylinder for stigmatism is easily accomplished, utilizing a ‘clock’ targetsupplied with the instrument.
‘Add’ power requirements for presbyopes can also be measured, simply by first obtainingthe distance correction and then adding plus power in small increments until a target at thedesired ‘near’ distance is clear.
In extensive field-testing, the FOCOMETER® was found to be as accurate as other methodsof subjective refraction and retinoscopy. Field test data were published in Optometry andVision Science (April 1993).
The FOCOMETER® is patented and is registered with the F.D.A 510(k)
Utilized in over 40 countries, the FOCOMETER® is manufactured by InFOCUS, a non-profitorganization based in Houston, Texas.
The design eliminates the need for many pieces, which could be lost or broken and difficultto replace.
Many clinicians in the USA and other developed countries find the FOCOMETER®
useful for over-refraction of contact lens wearers and for patients ordinarily difficult to refract, such aspatients with keratoconus.
Contact InFOCUS to order a FOCOMETER®, to learn about donating FOCOMETER® to acolleague in a developing country, or with any questions that you may have about theFOCOMETER® or primary eye care.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 32/81
26
How to Read the FOCOMETER ®
The FOCOMETER ® provides a readout of spectacle prescription.
• Prescriptions are measured in units called diopters. See Glossary in Appendix for a description.
• A diopter scale is found on the threaded barrel of the FOCOMETER®. The scale is calibrated andlinear. The range of the scale is +10 to –10. Note only even numbers are printed on the barrel.
• A reading of 0.00 indicates that the person has no refractive error.• The plus (+) or minus (-) sign in front of the numbers represent the power of the plus lens
or minus lens needed to correct the refractive error of the patient.
• Plus correction improves farsightedness or Hyperopia.
• Minus correction improves nearsightedness or Myopia.
• The rotating collar of the FOCOMETER® contains four equally spaced lines with three dots betweeneach line. The lines represent whole diopters and the dots represent quarter and half diopters.Note: Some models do not have dots on the scale, only straight lines indicating whole and half diopters.
To take a reading….
• The reading should bemeasured to the nearest quarter on the diopter scale.
• To take a reading, look straightdown on the diopter scale. The
reading is taken on the diopter scale where the collar crossesthe diopter scale.
• Patients are instructed to stoprotating the collar as soon as
the clock target is clearly seenthrough the FOCOMETER
®.
• When a straight line on thecollar is found directlyabove the diopter scale on
the barrel, then the diopter reading is a whole number.
ex. –2.00, 0.00, or +1.00
• When a dot on the collar isfound directly above the
diopter scale, then thediopter reading will includea quarterly fraction of a
diopter.ex. –2.25, -2.50, or -2.75
See examples on next page.
Side view
Flexibleeye piece
LookThroughThisend
CalibratedLinear scale
Rotatingcollar
Lens(front)
Stationarycollar Threaded
barrel
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 33/81
27
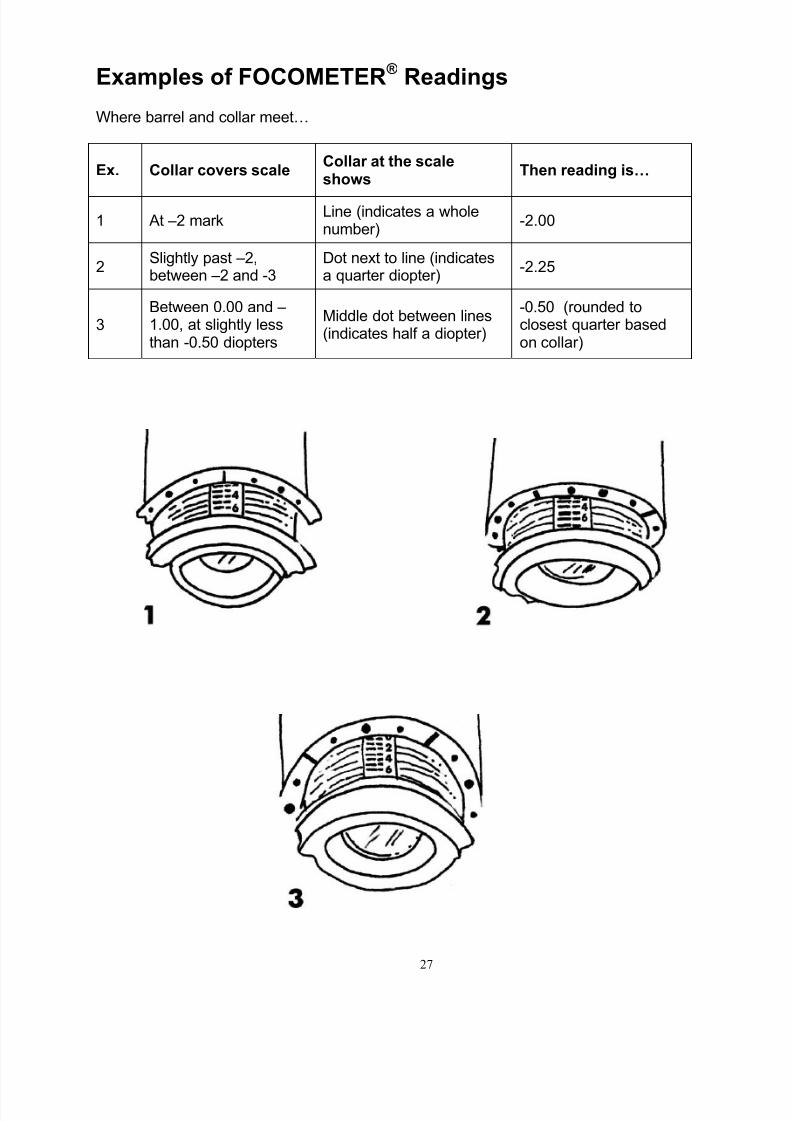
Examples of FOCOMETER ® Readings
Where barrel and collar meet…
Ex. Collar covers scaleCollar at the scaleshows
Then reading is…
1 At –2 markLine (indicates a wholenumber)
-2.00
2Slightly past –2,between –2 and -3
Dot next to line (indicatesa quarter diopter)
-2.25
3Between 0.00 and –1.00, at slightly lessthan -0.50 diopters
Middle dot between lines(indicates half a diopter)
-0.50 (rounded toclosest quarter basedon collar)
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 34/81
28
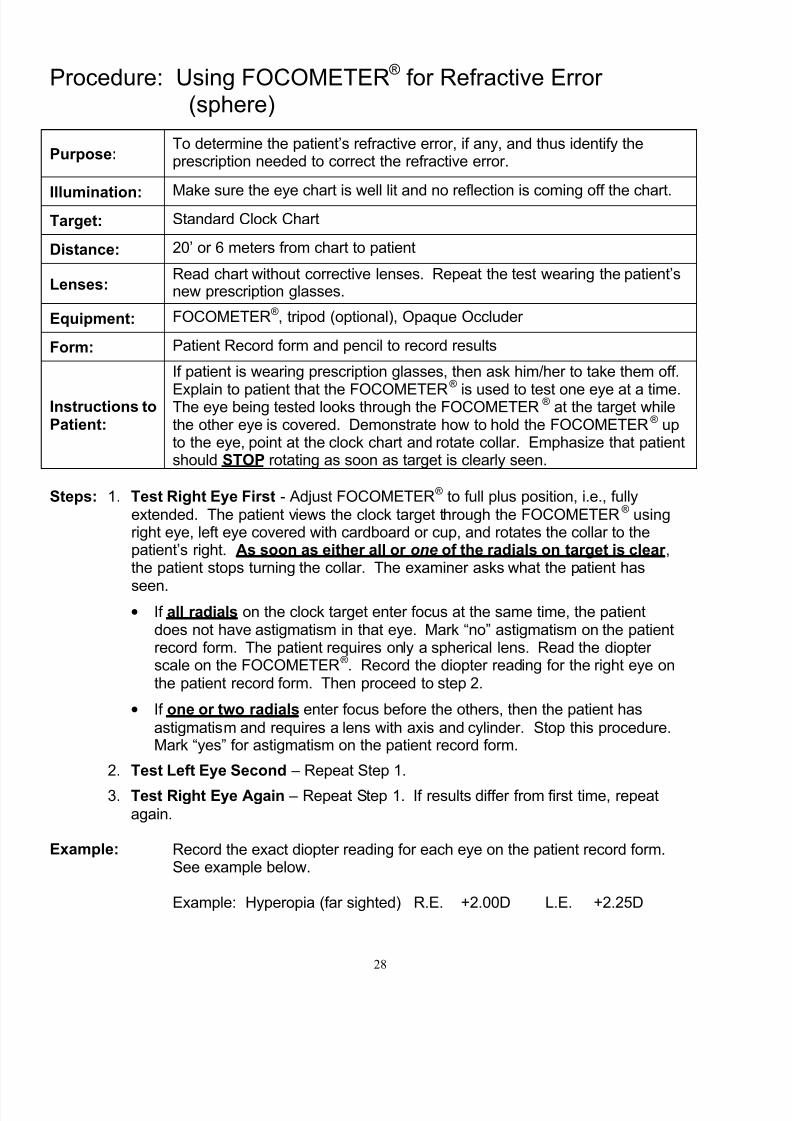
Procedure: Using FOCOMETER® for Refractive Error (sphere)
Purpose:To determine the patient’s refractive error, if any, and thus identify theprescription needed to correct the refractive error.
Illumination: Make sure the eye chart is well lit and no reflection is coming off the chart.
Target: Standard Clock Chart
Distance: 20’ or 6 meters from chart to patient
Lenses:Read chart without corrective lenses. Repeat the test wearing the patient’snew prescription glasses.
Equipment: FOCOMETER®, tripod (optional), Opaque Occluder
Form: Patient Record form and pencil to record results
Instructions toPatient:
If patient is wearing prescription glasses, then ask him/her to take them off.
Explain to patient that the FOCOMETER®
is used to test one eye at a time.The eye being tested looks through the FOCOMETER® at the target whilethe other eye is covered. Demonstrate how to hold the FOCOMETER® upto the eye, point at the clock chart and rotate collar. Emphasize that patientshould STOP rotating as soon as target is clearly seen.
Steps: 1. Test Right Eye First - Adjust FOCOMETER® to full plus position, i.e., fullyextended. The patient views the clock target through the FOCOMETER® usingright eye, left eye covered with cardboard or cup, and rotates the collar to thepatient’s right. As soon as either all or one of the radials on target is clear ,the patient stops turning the collar. The examiner asks what the patient has
seen.• If all radials on the clock target enter focus at the same time, the patient
does not have astigmatism in that eye. Mark “no” astigmatism on the patientrecord form. The patient requires only a spherical lens. Read the diopter scale on the FOCOMETER®. Record the diopter reading for the right eye onthe patient record form. Then proceed to step 2.
• If one or two radials enter focus before the others, then the patient has
astigmatism and requires a lens with axis and cylinder. Stop this procedure.Mark “yes” for astigmatism on the patient record form.
2. Test Left Eye Second – Repeat Step 1.
3. Test Right Eye Again – Repeat Step 1. If results differ from first time, repeat
again.
Example: Record the exact diopter reading for each eye on the patient record form.See example below.
Example: Hyperopia (far sighted) R.E. +2.00D L.E. +2.25D

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 35/81
29
Interpretationof TestResults:
0.00 diopters - Normal vision, no need for corrective lensesPlus diopters - Far vision correction available with prescription lensesMinus diopters - Near vision correction available with prescription lenses
All radials appear at same time - only spherical lenses needed, noastigmatism presentOne or two radials appear first - astigmatism present

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 36/81
30
Procedure: Using FOCOMETER ® for Astigmatic Error
Purpose:To determine the patient’s astigmatic error, if any, and thus identify theprescription needed to correct the astigmatic error.
Illumination: Make sure the eye chart is well lit and no reflection is coming off the chart.
Target: Standard Clock Chart
Distance: 20’ or 6 meters from chart to patient
Lenses:Read chart without corrective lenses. Repeat the test wearing the patient’snew prescription glasses when they become available.
Equipment: FOCOMETER® tripod (optional), Opaque Occluder
Form: Patient Record form and pencil to record results
Instructions toPatient:
Tell patient to look through FOCOMETER® at the clock chart while the other eye is covered. Instruct patient to turn FOCOMETER® collar to the right
and then STOP as soon as the first radial comes into view. Once thereading is taken, the patient should resume viewing through theFOCOMETER® and continue rotating the collar UNTIL the second radial,perpendicular to the first, comes into view. For example, If the first radialseen clearly is 11 - 5 line on the clock target, tell the patient to continuerotating the collar until the 8 - 2 line on the clock target is seen clearly.Make a note of the reading on the FOCOMETER®.
Steps:
1. Complete Steps 1 and 2 of “Using FOCOMETER® for Refractive Error”. If patient reportsthat one or two radials become clear before the rest of the radials, then proceed with thisprocedure.
2. Test Right Eye First - Adjust FOCOMETER® to full plus position, i.e., fully extended.The patient views the clock target through the FOCOMETER® using right eye, left eyecovered with occluder, cardboard or cup, and rotates the collar to the patient’s right.
• As soon as one of the radials on target is clear*, the patient stops turning thecollar. The examiner asks the patient which radial(s)* were seen first. The examiner records the number of degrees (30 to 180 degrees) associated with the radial. Inaddition, the examiner records the number and sign of diopters on the barrel of theFOCOMETER®. This first radial is called the Spherical correction.
Ex. First Radial (Spherical) +3.00 D @ 150 degrees

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 37/81
31
• The examiner tells the patient to stop as soon as the second radial* comes intofocus. Then the patient looks through the FOCOMETER® again, and continues torotate the collar to the right until the second radial, perpendicular to first radial, comesinto focus. This second radial is always 90 degrees away from the first and alwayshas a diopter reading that is in the more minus direction on the scale than the firstradial. The examiner records degrees and diopters again.
Ex. Second Radial +2.50 (diopters) @ 60 (degrees)
3. Calculate the Cylinder required to correct astigmatism by finding the difference indiopters between the first and second perpendicular radials
Ex. (First Radial) +3.00 minus (Second Radial) +2.50 = 0.50(recorded as -0.50D)
4. Prescription for this eye is written as: +3.00 - 0.50 x 060(sphere) (cylinder) (axis) (degrees)
+3.00 is 3.00 diopters of Sphere from first radial reading-0.50 diopters is the cylinder power from the difference between the powers
of the two radials60 degrees is the axis of the perpendicular (second) radial
5. Test Left Eye Second – Repeat Steps 2 – 4.
More examples:
Ex. #2 1st Radial is -2.00 @ 90 (12 o’clock)2nd Radial is -4.00 @ 180 (3-9 o’clock)
-2.00 minus -4.00 = -2.00Then the cylinder is -2.00Rx is written as -2.00 - -2.00 x 180
(sphere) - (cylinder) (axis) (degrees)
Ex. #3 1st Radial is +1.00 @ 120 (1 o’clock)2nd Radial is -3.00 @ 30 (10 o’clock)+1.00 minus -3.00 = -4.00Then the cylinder is -4.00Rx is written as +1.00 - -4.00 x 030
(sphere) - (cylinder) (axis) (degrees)
Ex. #4 1
st
Radial is 0.00 at 180 (3-9 o’clock)2nd Radial is -2.00 @ 900.00 minus -2.00 = -2.00Then the cylinder is -2.00Rx is written as plano - -2.00 x 090
(sphere) - (cylinder) (axis) (degrees)

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 38/81
32
Remember the Scale – You always turn the Focometer sleeve to get the cylinder power in the more minus direction
Sphere power is always the most plus direction
+10 +9 +8 +7 +6 +5 +4 +3 +2 +1 0 -1 -2 -3 -4 -5 -6 -7 -8 -9 -10
Cylinder power is always the more minus direction
Prescriptions are always written in the minus form so we can only go in one direction frommost plus to minus.
In the examples above:
Sphere reading Cylinder reading Cylinder Power on Focometer on Focometer
Ex. 1 +3.00 D +2.50 D -0.50 DEx. 2 -2.00 D -4.00 D -2.00 DEx. 3 +1.00 D -3.00 D -4.00 DEx. 4 0.00 (pl) -2.00 D -2.00 D
Plug these numbers on the scale above and see how we derived the cylinder power.
The above scale is the same as on the Focometer except that this scale is flat on a pieceof paper instead of a tube.
*If two radials become clear at the same time, then it is okay to estimate the radial
between them. Eg. If both the 10 o’clock line and 11 o’clock line look equally clear thenthe axis will be between 30° (10 o’clock radial) and 60° (11 o’clock radial) which is 45°
Interpretation of Test Results: All radials appear at same time. Normal vision, no need for astigmatic
correction
One or two of the radials appear at the same time - Astigmatic vision
Record: Record readings for each eye on Patient Record form.Sphere in diopters with plus or minus sign
Cylinder in minus diopters and axis of cylinder in degrees
Ex. R.E. +2.75 -2.00 x 120L.E. +3.00 -2.25 x 150
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 39/81
33
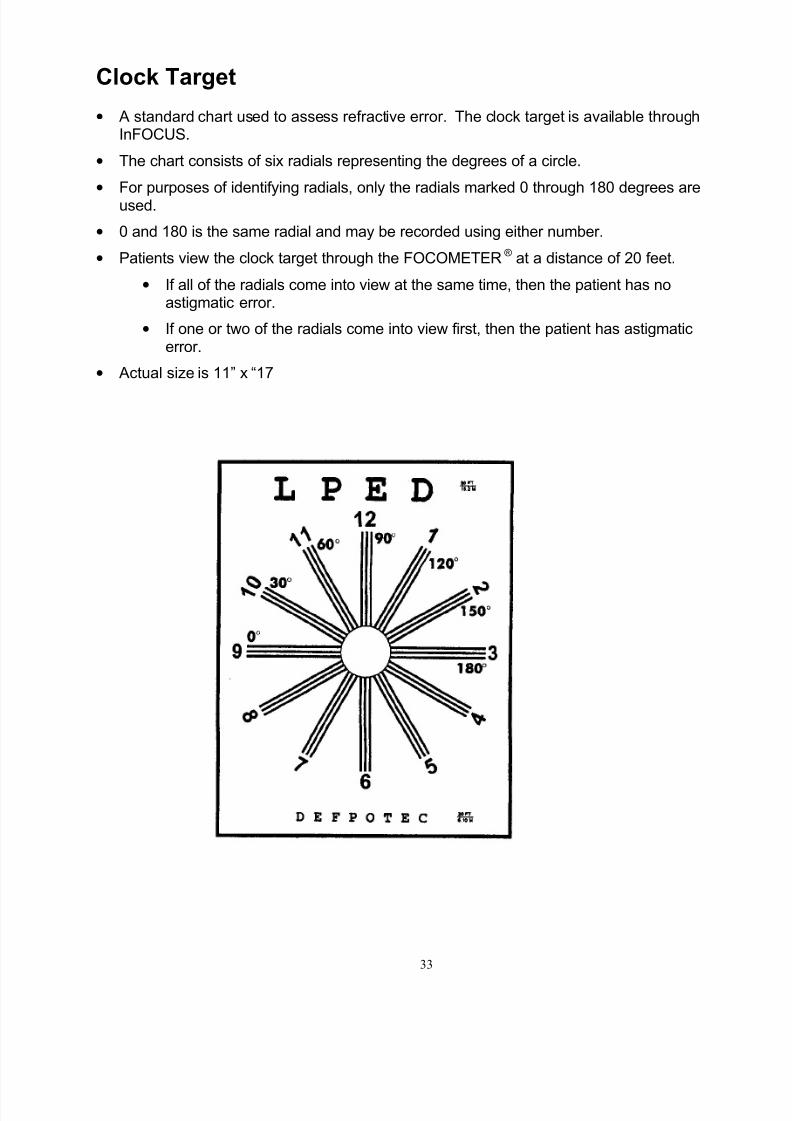
Clock Target
• A standard chart used to assess refractive error. The clock target is available throughInFOCUS.
• The chart consists of six radials representing the degrees of a circle.
• For purposes of identifying radials, only the radials marked 0 through 180 degrees areused.
• 0 and 180 is the same radial and may be recorded using either number.
• Patients view the clock target through the FOCOMETER® at a distance of 20 feet.
• If all of the radials come into view at the same time, then the patient has noastigmatic error.
• If one or two of the radials come into view first, then the patient has astigmaticerror.
• Actual size is 11” x “17
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 40/81
34
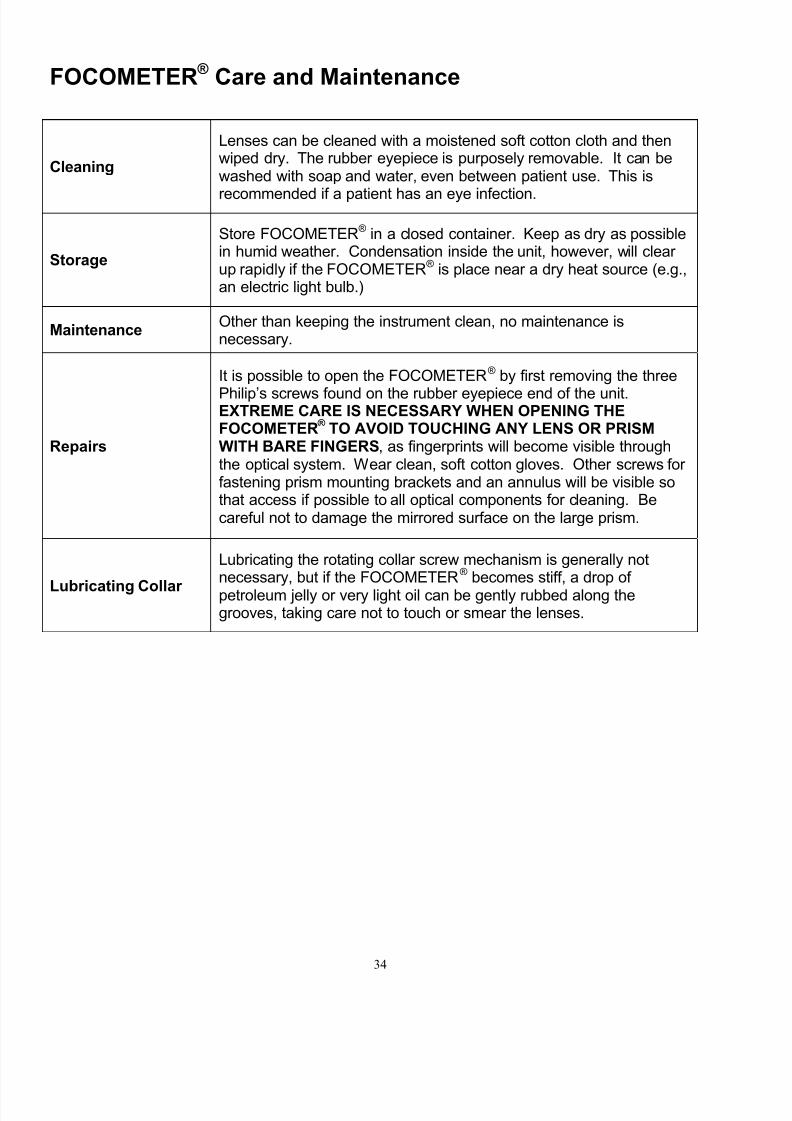
FOCOMETER ® Care and Maintenance
Cleaning
Lenses can be cleaned with a moistened soft cotton cloth and thenwiped dry. The rubber eyepiece is purposely removable. It can bewashed with soap and water, even between patient use. This is
recommended if a patient has an eye infection.
Storage
Store FOCOMETER® in a closed container. Keep as dry as possiblein humid weather. Condensation inside the unit, however, will clear up rapidly if the FOCOMETER® is place near a dry heat source (e.g.,an electric light bulb.)
MaintenanceOther than keeping the instrument clean, no maintenance isnecessary.
Repairs
It is possible to open the FOCOMETER® by first removing the three
Philip’s screws found on the rubber eyepiece end of the unit.EXTREME CARE IS NECESSARY WHEN OPENING THEFOCOMETER ® TO AVOID TOUCHING ANY LENS OR PRISMWITH BARE FINGERS, as fingerprints will become visible throughthe optical system. Wear clean, soft cotton gloves. Other screws for fastening prism mounting brackets and an annulus will be visible sothat access if possible to all optical components for cleaning. Becareful not to damage the mirrored surface on the large prism.
Lubricating Collar
Lubricating the rotating collar screw mechanism is generally notnecessary, but if the FOCOMETER® becomes stiff, a drop of petroleum jelly or very light oil can be gently rubbed along thegrooves, taking care not to touch or smear the lenses.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 41/81
35
Module 3 – Eye Health & Safety
Preventive PracticesMany of the problems that affect the eyes are preventable by practicing appropriatehygiene, good nutrition and basic preventative steps. Prevention is directly related to
people’s behavior and the choices they make in how they live their lives. Good healtheducation can lead to making healthier behavior choices.
Hygiene
Risk – Eye infections and maternal gonorrhea. Note: Maternal gonorrhea isa venereal disease; blindness in the newborn is prevented with antiseptic or antibiotic therapy.Preventive Steps –Do not share: towels, handkerchiefs, bandannas, bed pillowcases andlinens, or cosmeticsWash hands: prior to and after touching the eye or playing with childrenDo not wipe sweat from eye using work shirts or other work clothing toprevent exposure to dust, pesticides and contaminants.
Face Washing: frequent washing of face will discourage face-seeking flieswhich carry trachoma in many parts of the world.Household: Proper disposal of rubbish and feces and moving livestock awayfrom houses will reduce the number of flies.Entire family needs to cooperate regarding household hygiene.
UV Protection
Risk - Excessive and unprotected exposure to ultraviolet (UV) radiation maycontribute to or worsen Pterygium, cataracts and macular degeneration.Preventive Steps – Wear sunglasses or safety glasses with 100% UVblockage and wide brim hat
Injury Prevention
Risk – Burns that damage cornea are caused by household cleaners,
pesticides, fungicides and fertilizers. Also debris in the eye, traumas to thehead and infections resulting from traumas.Preventive Steps – Use safety equipment properly:
• Wear ANSI-approved, impact-resistant safety glasses or work goggles
• Use 100% Ultraviolet blockage sunglasses or goggles
• Use well fitting cap with a strong brim
• Stay alert and do not using audio equipment that hinders hearing
Nutrition
Risk – Vitamin A deficiency leads to night blindness, dry eyes, and pain inthe eyes. Vitamin A deficiency is the leading cause of non-infectiousblindness in children worldwide. Deficient diets also impair healing and
recovery from injuries and infections.Preventive Steps - Eat foods rich in Vitamin A such as red, yellow, andgreen vegetables, fruits and diary products. Eat a well balanced diet overall,including an adequate daily intake of protein. Diabetics should eat foodsrecommended to manage their disease.
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 42/81
36
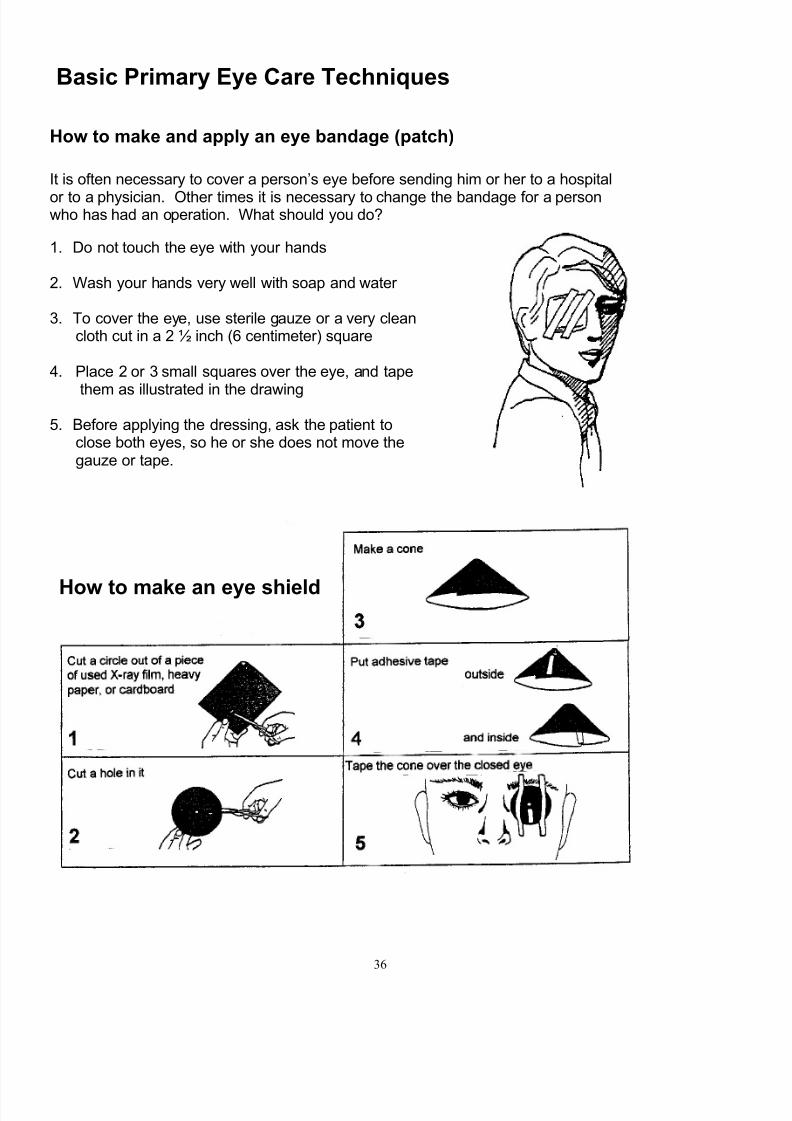
Basic Primary Eye Care Techniques
How to make and apply an eye bandage (patch)
It is often necessary to cover a person’s eye before sending him or her to a hospital
or to a physician. Other times it is necessary to change the bandage for a personwho has had an operation. What should you do?
1. Do not touch the eye with your hands
2. Wash your hands very well with soap and water
3. To cover the eye, use sterile gauze or a very cleancloth cut in a 2 ½ inch (6 centimeter) square
4. Place 2 or 3 small squares over the eye, and tape
them as illustrated in the drawing
5. Before applying the dressing, ask the patient toclose both eyes, so he or she does not move thegauze or tape.
How to make an eye shield

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 43/81
37
How to evert (turn out) the upper eyelid
1. Look for the foreign body on the eyeball withoutlifting the upper eyelid
2. If you cannot find it, take the upper eye lid
between the thumb and forefinger 3. Lift the eye lid so it stays on the match stick and
with the entire conjunctiva in view, look for theforeign body
4. When you have found it, carefully remove with aclean cotton swab or the tip of a clean cloth
How to apply drops and / or ointment to the eye
Portions of this chapter, including illustrations,are adapted from ‘Primary Eye Care manual’,World Health Organization, Scientific
Publication No. 490 1985

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 44/81
38
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 45/81
39
Module 4 – Eye Injuries & Diseases
Assessing Eye Conditions
Eye injuries are common and a leading cause of preventable unilateral blindnessworldwide. The causes vary, but drawing upon experience from The Gambia and Senegal,trauma is more common during the farming season and among small-scale metal workersworking without eye protection. Stick injury is common in children and farmers, sometimescausing a penetrating injury that can result in the affected eye quickly becoming infected.Blunt trauma is common among children, who can be injured with a catapult or stone. Thedusty environment is a common cause of corneal, conjunctival and sub-tarsal foreignbodies injuries.
Injuries are often preventable which makes education at the community level important.Village health workers and community-based volunteers (such as ‘Nyateros‘ or ‘Friends of the Eye’ in The Gambia) are important promoters of good eye health practices.
A network of community ophthalmic nurses can provide appropriate first aid and refer fromvillage level to secondary or tertiary care. This can significantly reduce visual impairmentand blindness resulting from injuries. Health facilities should be ready to deal with eyeinjuries by:
• ensuring that staff know how to assess eye injuries and perform basic first aidprocedures appropriate to their level of training
• ensuring a supply of equipment, drugs and consumables required to assess andprovide first aid for eye injury
• having a plan of how to refer patients, including nearest referral facilities, and
options for transporting patients in an emergency.
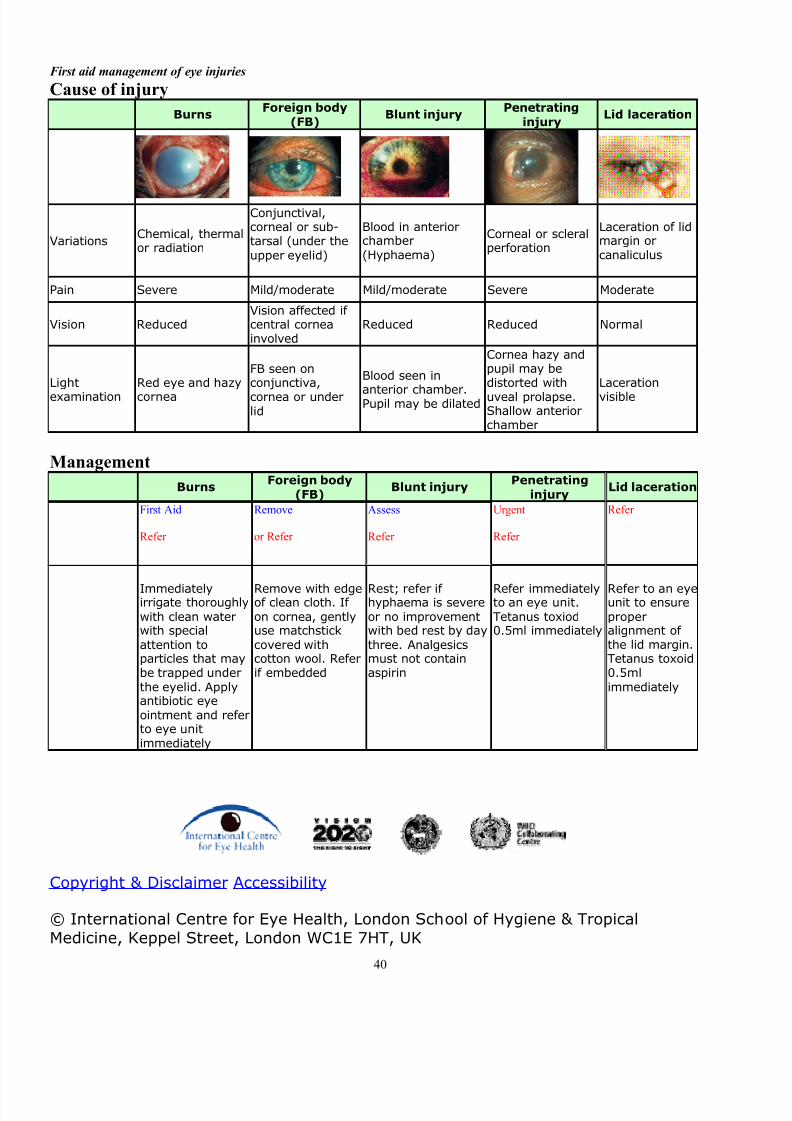
The chart below provides an easy reference for community level workers faced with an eyeinjury in their clinic or community.
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 46/81
40
First aid management of eye injuries
Cause of injury
BurnsForeign body
(FB)Blunt injury
Penetrating
injuryLid laceration
VariationsChemical, thermalor radiation
Conjunctival,corneal or sub-tarsal (under theupper eyelid)
Blood in anteriorchamber(Hyphaema)
Corneal or scleralperforation
Laceration of lidmargin orcanaliculus
Pain Severe Mild/moderate Mild/moderate Severe Moderate
Vision ReducedVision affected if central corneainvolved
Reduced Reduced Normal
Light
examination
Red eye and hazy
cornea
FB seen onconjunctiva,
cornea or underlid
Blood seen in
anterior chamber.Pupil may be dilated
Cornea hazy andpupil may bedistorted with
uveal prolapse.Shallow anteriorchamber
Laceration
visible
Management
BurnsForeign body
(FB)Blunt injury
Penetrating
injuryLid laceration
First Aid
Refer
Remove
or Refer
Assess
Refer
Urgent
Refer
Refer
Immediatelyirrigate thoroughlywith clean waterwith specialattention toparticles that maybe trapped underthe eyelid. Applyantibiotic eyeointment and referto eye unitimmediately
Remove with edgeof clean cloth. If on cornea, gentlyuse matchstickcovered withcotton wool. Referif embedded
Rest; refer if hyphaema is severeor no improvementwith bed rest by daythree. Analgesicsmust not containaspirin
Refer immediatelyto an eye unit.Tetanus toxiod0.5ml immediately
Refer to an eyeunit to ensureproperalignment of the lid margin.Tetanus toxoid0.5mlimmediately
Copyright & Disclaimer Accessibility
© International Centre for Eye Health, London School of Hygiene & Tropical
Medicine, Keppel Street, London WC1E 7HT, UK

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 47/81
41
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 48/81
42
Most Common Eye Diseases
Some eye problems are minor and fleeting. But some lead to a permanent loss
of vision. Common eye problems include:
• Cataracts - clouded lenses•
Glaucoma - damage to the optic nerve from too much pressure in the eye• Retinal disorders - problems with the nerve layer at the back of the eye• Conjunctivitis - an infection also known as pink eye
Your best defense is to have regular checkups, because eye diseases do not always havesymptoms. Early detection and treatment could prevent vision loss. See an eye careprofessional right away if you have a sudden change in vision or everything looks dim or if you see flashes of light. Other symptoms that need quick attention are pain, double vision,fluid coming from the eye and inflammation.
Cataract
A cataract is a clouding of the lens in your eye. It affects your vision. Cataracts are verycommon in older people. By age 80, more than half of all people in the United States either have a cataract or have had cataract surgery.
Common symptoms are:
• Blurry vision• Colors that seem faded• Glare• Not being able to see well at night• Double vision• Frequent prescription changes in your eye wear
Cataracts usually develop slowly. New glasses, brighter lighting, anti-glare sunglasses or magnifying lenses can help at first. Surgery is also an option. It involves removing thecloudy lens and replacing it with an artificial lens. Wearing sunglasses and a hat with a brimto block ultraviolet sunlight may help to delay cataracts.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 49/81
43
Glaucoma
Glaucoma damages the eye's optic nerve. It is a leading cause of blindness inthe United States. It usually happens when the fluid pressure inside the eyesslowly rises, damaging the optic nerve. Often there are no symptoms at first,
but a comprehensive eye exam can detect it.
People at risk should get eye exams at least every two years. They include
• African Americans over age 40• People over age 60, especially Mexican Americans• People with a family history of glaucoma
Early treatment can help protect your eyes against vision loss. Treatments
usually include prescription eye drops and/or surgery.
Diabetic Retinopathy
Diabetes is a disease that occurs when the pancreas does not secrete enough insulinor the body is unable to process it properly. Insulin is the hormone that regulates thelevel of sugar (glucose) in the blood. Diabetes can affect children and adults.
How does diabetes affect the retina?
Patients with diabetes are more likely to developeye problems such as cataracts and glaucoma,but the disease’s affect on the retina is the mainthreat to vision. Most patients develop diabetic
changes in the retina after approximately 20years. The effect of diabetes on the eye is calleddiabetic retinopathy.
Over time, diabetes affects the circulatory systemof the retina. The earliest phase of the disease isknown as background diabetic retinopathy. In thisphase, the arteries in the retina become
weakened and leak, forming small, dot-like hemorrhages. These leaking vessels often leadto swelling or edema in the retina and decreased vision.
The next stage is known as proliferative diabetic retinopathy. In this stage, circulationproblems cause areas of the retina to become oxygen-deprived or ischemic. New, fragile,vessels develop as the circulatory system attempts to maintain adequate oxygen levelswithin the retina. This is called neovascularization. Unfortunately, these delicate vesselshemorrhage easily. Blood may leak into the retina and vitreous, causing spots or floaters,along with decreased vision.
In the later phases of the disease, continued abnormal vessel growth and scar tissue maycause serious problems such as retinal detachment and glaucoma.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 50/81
44
Retinal Disorders
The retina is a layer of tissue in the back of your eye that senses light and sends images toyour brain. In the center of this nerve tissue is the macula. It provides the sharp, centralvision needed for reading, driving and seeing fine detail.
Retinal disorders affect this vital tissue. They can affect your vision, and some can be
serious enough to cause blindness. Examples are
• Retinal detachment - a medical emergency, when the retina is pulled away from theback of the eye
• Macular pucker - scar tissue on the macula• Macular hole - a small break in the macula that usually happens to people over 60• Floaters - cobwebs or specks in your field of vision
Eye Infections
Your eyes can get infections from bacteria, fungi or viruses. Eye infections canoccur in different parts of the eye and can affect just one eye or both. Two
common eye infections are
Conjunctivitis - also known as pink eye. Conjunctivitis is often due to an infection. Childrenfrequently get it, and it is very contagious.
Stye - a bump on the eyelid that happens when bacteria from your skin get into the hair follicleof an eyelash.
Symptoms of eye infections may include redness, itching, swelling,discharge, pain, or problems with vision. Treatment depends on thecause of the infection and may include compresses, eye drops, creamsor antibiotics.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 51/81
45
Pterygium is a wedge-shaped, raised outgrowth of
the conjunctiva. It is a fibrous, vascularized, andopaque tissue that forms at the junction betweenepisclera and the clear cornea. Pterygium is typicallyseen in the 20-30-year age group and ispredominately in males. Living in a tropical climate aswell as exposure to ultraviolet light, dust, wind, and
noxious chemicals contribute to the spontaneoustriangular outgrowth. With time, some pterygia willspontaneously become inactive, whereas in other cases the growth affects vision byinvading the central cornea. This condition requires surgical excision.
What can be done to prevent pterygia and invasion of the cornea?Protecting eyes from sun, dust and wind is essential. Artificial tears may be helpfulto reduce irritation, and topical steroids may be used to diminish inflammation.
Subconjunctival hemorrhage occurs when a small blood vesselunder the conjunctiva breaks and bleeds. It may occur spontane-ously or from coughing, heavy lifting, or vomiting. In some cases,it may develop following eye surgery or trauma. Subconjunctivalhemorrhage tends to be more common among those with diabetesand hypertension.
While it may look frightening, a subconjunctival hemorrhage is essentially harmless.The blood becomes trapped underneath the clear conjunctival tissue, much like a bruise.The blood is visible because it shows through the thin, clear conjunctiva. The bloodnaturally absorbs within one to three weeks and no treatment is required.
Signs and Symptoms• Red, bloody patch on the white of the eye• Painless• No change in vision
Treatment
Although it may look like an emergency, a subconjunctival hemorrhage does not affect thevision and no treatment is required.
Pterygium (early)
Possible Signs and Symptoms• Irritation/Redness• Sensitivity to light• Tearing• Foreign body sensation
• Diplopia (double vision)• Increased astigmatism (cylindrical
distortion)
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 52/81
46
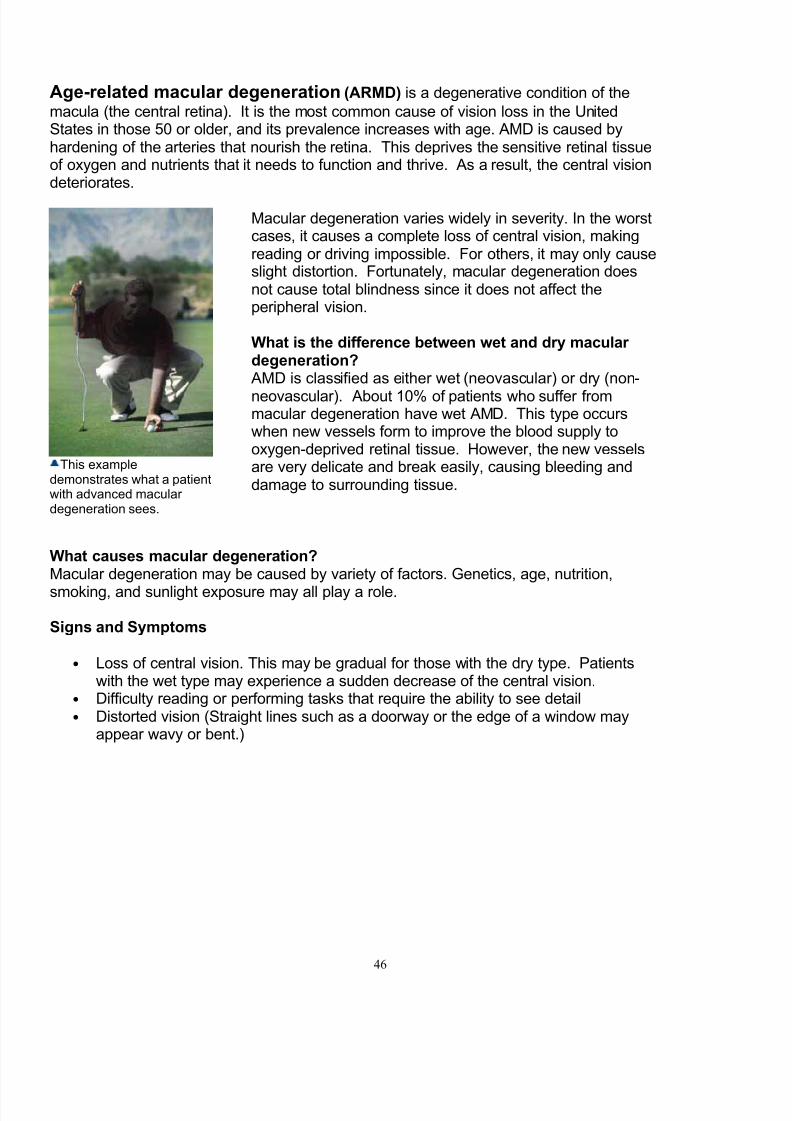
Age-related macular degeneration (ARMD) is a degenerative condition of the
macula (the central retina). It is the most common cause of vision loss in the UnitedStates in those 50 or older, and its prevalence increases with age. AMD is caused byhardening of the arteries that nourish the retina. This deprives the sensitive retinal tissueof oxygen and nutrients that it needs to function and thrive. As a result, the central visiondeteriorates.
Macular degeneration varies widely in severity. In the worstcases, it causes a complete loss of central vision, makingreading or driving impossible. For others, it may only causeslight distortion. Fortunately, macular degeneration doesnot cause total blindness since it does not affect theperipheral vision.
What is the difference between wet and dry macular degeneration?
AMD is classified as either wet (neovascular) or dry (non-
neovascular). About 10% of patients who suffer frommacular degeneration have wet AMD. This type occurswhen new vessels form to improve the blood supply tooxygen-deprived retinal tissue. However, the new vesselsare very delicate and break easily, causing bleeding anddamage to surrounding tissue.
What causes macular degeneration? Macular degeneration may be caused by variety of factors. Genetics, age, nutrition,
smoking, and sunlight exposure may all play a role.
Signs and Symptoms
• Loss of central vision. This may be gradual for those with the dry type. Patientswith the wet type may experience a sudden decrease of the central vision.
• Difficulty reading or performing tasks that require the ability to see detail• Distorted vision (Straight lines such as a doorway or the edge of a window may
appear wavy or bent.)
This exampledemonstrates what a patientwith advanced macular degeneration sees.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 53/81
47
Module 5 – Referrals
If patient meets any of the following criteria, then a vision exam is necessary. If theexaminer is unable to resolve the problem, or is unsure of the results, a referral toappropriate eye care professional is strongly recommended.
CriteriaRecommended Schedule - Patient is due or overdue for a professional eye exam. SeeRecommended Schedule Guidelines on page 11.
History – History or signs of glaucoma, diabetes and hypertension in patient or patient’s family
Visual Acuity
• Distance – 20/30 or worse in either eye.
• Near - 20/40 or worse in either eye or inability to see clearly at a comfortable readingdistance. Vision is blurred and patient is under 40.
• Child – passed distance vision with 20/30 or lower but strained, squinted, or tilted head, etc.May indicate astigmatism.
• Astigmatism – evident. Patient reports some areas of the clock target are blurred and others
are clear. Note that astigmatism can be confirmed with the FOCOMETER ® . Refractive Error – Patient’s refractive error indicates a need for eyeglasses. Diopter readingswere more than plus or minus 0.50 diopters.
Color Vision – Patient showed difficulty in recognizing colors
Binocular Coordination – Patient’s failed Versions Test and/or Cover/Uncover Test.
Eye Condition - Patient’s eyes do not appear as follows and examiner is not trained to treat.
• Cornea is clear
• Pupil is black
• White part (conjunctiva) white
• Eyelids open and close properly
Other (specify) any complaint or concern, especially regarding pain, expressed by patient or theparent of young patient.
Referral Procedure
Referral Sources
Types - May be a general referral in which the patient chooses theeye care professional or a specific referral chosen by the examiner and/or the examiner’s organization.Barriers - The patient’s lack of financial assets may act as a barrier toeither seeing an eye care professional or to obtaining glasses. Prior tomaking a referral, investigate how this barrier might be overcome.
Patient InvolvementTell patient the reason for the referral and why it is important tofollow-up on the referral. Ask patient if he/she has any concerns or
questions.
Provide WrittenReferral
Some organizations may use referral forms. Ideally, the patientshould be provided with a name, address and phone number of aneye care professional that is willing to accept the referral on a timelybasis.
Document Referral
Record on patient’s form and retain in patient’s file:
• Referred to
• Referred on date
• Reason for referral

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 54/81
48

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 55/81
49
Module 6 – Dispensing Eyeglasses
Eyeglass FramesPurpose: Frames hold corrective lenses in their proper place before the eyes.
Types:1. Plastic2. Metal3. Combination plastic and metal4. Rimless
Materials:1. Plastics2. Metals3. High Tech
Eyeglass Lenses
Purpose:Correct blurred vision by bending light rays entering the pupil so that the raysconverge at the back of the eyeball
Materials:1. CR-392. Polycarbonate or “poly” – safest high impact lenses on the market,
require anti-scratch coating because poly is soft
Lens Surfaces:
1. Spherical, round like a basketball, two types
• Convex – corrects hyperopia or farsightedness
• Concave – corrects myopia or nearsightedness2. Cylindrical, round like a football or an egg, two types
• Cylindrical only – corrects astigmatism
• Compound, i.e., cylindrical & spherical -- corrects astigmatism andeither hyperopia or myopia
Prism: Used to correct faulty eye-muscle imbalances in which eyes do not act as ateam. Unless present in strong amounts, prisms will not be conspicuous.
Number of Corrections:
1. Single vision – same focal power throughout the entire lens.2. Bifocals – upper part has correction for distance vision and lower part has
correction for close vision tasks3. Trifocals – three segments; upper part corrects distance vision;
intermediate segment corrects arms-length vision and lower part correctsclose work
4. Reading glasses – lower part corrects for close vision and upper part hasno correction
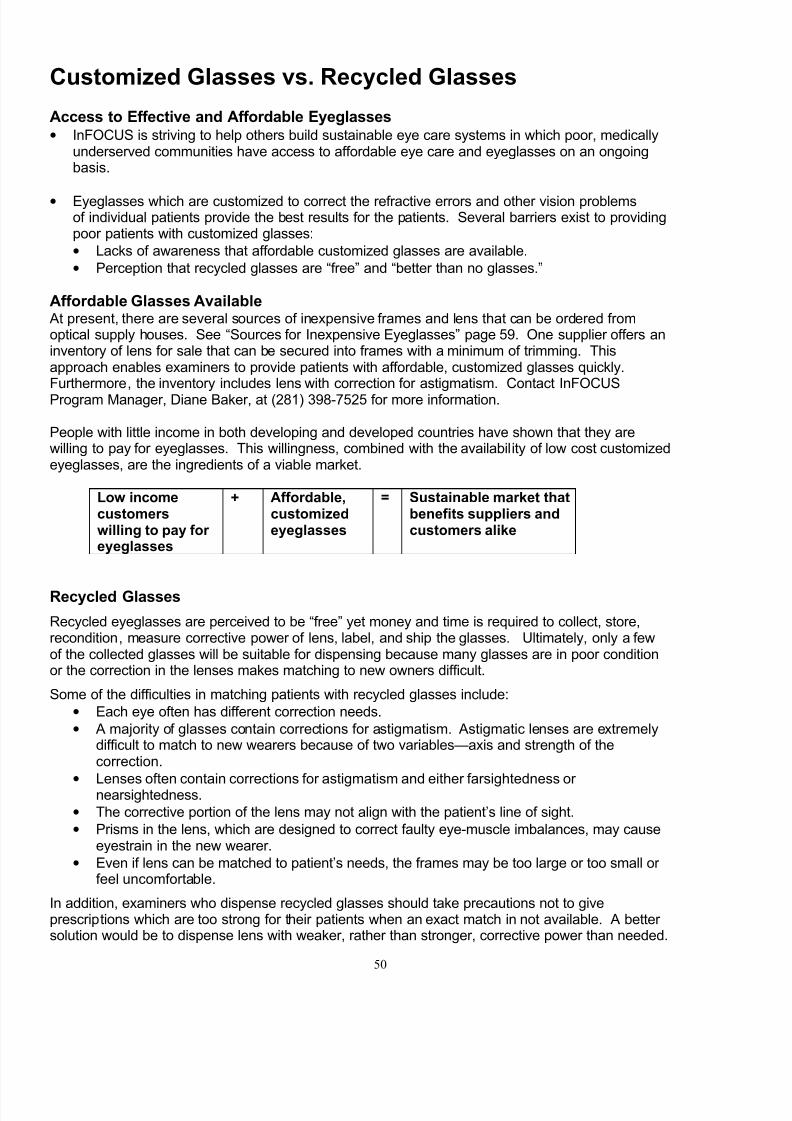
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 56/81
50
Customized Glasses vs. Recycled Glasses
Access to Effective and Affordable Eyeglasses• InFOCUS is striving to help others build sustainable eye care systems in which poor, medically
underserved communities have access to affordable eye care and eyeglasses on an ongoingbasis.
• Eyeglasses which are customized to correct the refractive errors and other vision problemsof individual patients provide the best results for the patients. Several barriers exist to providingpoor patients with customized glasses:
• Lacks of awareness that affordable customized glasses are available.
• Perception that recycled glasses are “free” and “better than no glasses.”
Affordable Glasses Available At present, there are several sources of inexpensive frames and lens that can be ordered fromoptical supply houses. See “Sources for Inexpensive Eyeglasses” page 59. One supplier offers aninventory of lens for sale that can be secured into frames with a minimum of trimming. Thisapproach enables examiners to provide patients with affordable, customized glasses quickly.Furthermore, the inventory includes lens with correction for astigmatism. Contact InFOCUSProgram Manager, Diane Baker, at (281) 398-7525 for more information.
People with little income in both developing and developed countries have shown that they arewilling to pay for eyeglasses. This willingness, combined with the availability of low cost customizedeyeglasses, are the ingredients of a viable market.
Low incomecustomerswilling to pay for eyeglasses
+ Affordable,customizedeyeglasses
= Sustainable market thatbenefits suppliers andcustomers alike
Recycled Glasses
Recycled eyeglasses are perceived to be “free” yet money and time is required to collect, store,recondition, measure corrective power of lens, label, and ship the glasses. Ultimately, only a fewof the collected glasses will be suitable for dispensing because many glasses are in poor conditionor the correction in the lenses makes matching to new owners difficult.
Some of the difficulties in matching patients with recycled glasses include:
• Each eye often has different correction needs.
• A majority of glasses contain corrections for astigmatism. Astigmatic lenses are extremelydifficult to match to new wearers because of two variables—axis and strength of thecorrection.
•
Lenses often contain corrections for astigmatism and either farsightedness or nearsightedness.
• The corrective portion of the lens may not align with the patient’s line of sight.
• Prisms in the lens, which are designed to correct faulty eye-muscle imbalances, may causeeyestrain in the new wearer.
• Even if lens can be matched to patient’s needs, the frames may be too large or too small or feel uncomfortable.
In addition, examiners who dispense recycled glasses should take precautions not to giveprescriptions which are too strong for their patients when an exact match in not available. A better solution would be to dispense lens with weaker, rather than stronger, corrective power than needed.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 57/81
51
Protocol for Dispensing Customized Eyeglasses
When to Use• Patient’s prescription for corrective lenses has been determined and
affordable, customized eyeglasses are available to the patient.
1Stock andDisplay Frames
• Provide samples of the frames available. Have a mirror available.
• Stock an eyeglass repair kit.
2 Interview Patient• Determine the activities of the patient, i.e., sedentary or active.
• Examine patient’s prescription.
• Start a Patient’s Record form.
3
Locate BestAvailable Lensand Frames for
Patient
• Based on patient’s activities, prescription and preferences, help thepatient to identify possible matches with the lenses and framesavailable.
•
Check the fit of frame on patient. Adjust if needed. If comfortable fitcannot be achieved, it is unlikely that patient will wear the glasses.
4
Order andReceive Framesand Lenses fromOptical SupplyHouse
• Place order. Retain copy of order.
• Receive order. Check eyeglasses against order. Return if eyeglassesdo not comply with order.
• Call patient to return when eyeglasses are ready.
5
MeasurePatient’sVisual Acuitywhile WearingGlasses
• Check distance vision and near vision while patient is wearing glasses.
• If both distance and near vision are clear, then go to step 6.
• If blurred for either distance or near vision, then record the difficultyon Patient Record form. Determine the source of the problem—prescription or eyeglasses. Return eyeglasses to optical supplyhouse and reorder.
• Check frames for comfort and fit. Adjust if needed.
6Give eye healthand safetyinformation
• Provide patient with information on hygiene, nutrition, UV protection,and injury prevention.
• Provide patient with instructions for wearing and caring for theeyeglasses.
7Completepaperwork.
• Complete Patient Record form re: prescription dispensed andinstructions given patient for wearing glasses. Maintain forms in
Patient Record files.
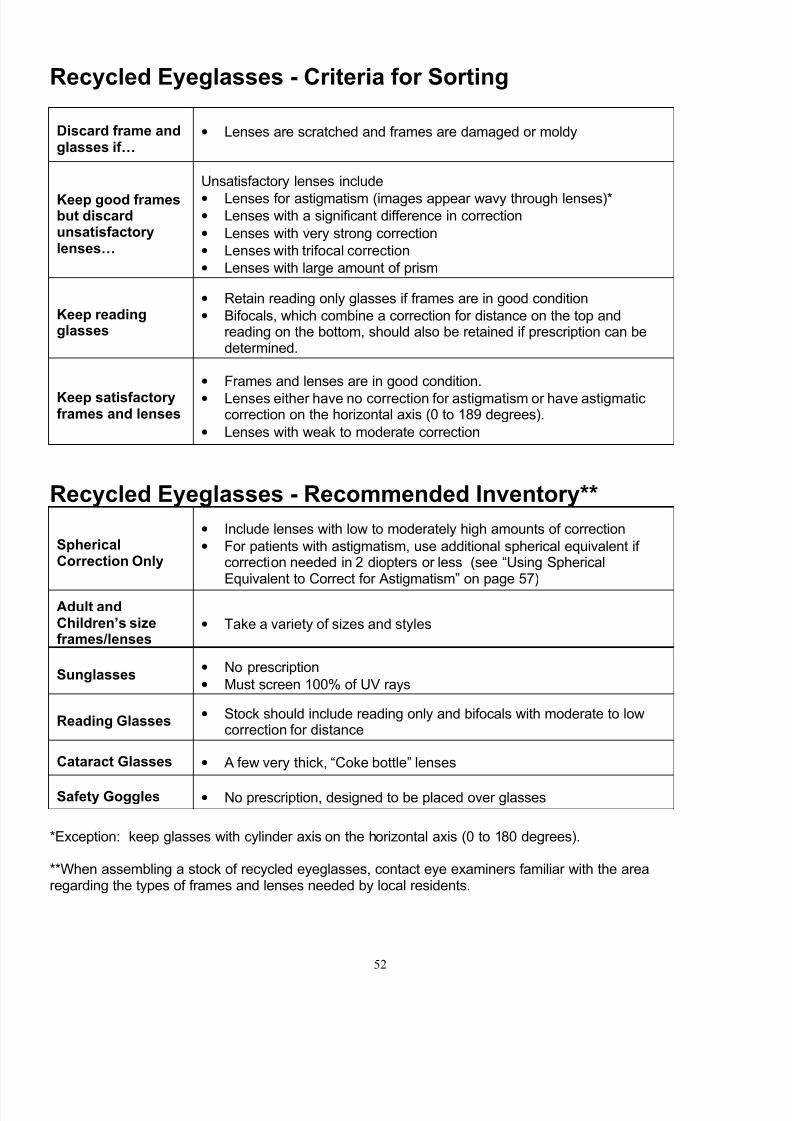
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 58/81
52
Recycled Eyeglasses - Criteria for Sorting
Discard frame andglasses if…
• Lenses are scratched and frames are damaged or moldy
Keep good framesbut discardunsatisfactorylenses…
Unsatisfactory lenses include
• Lenses for astigmatism (images appear wavy through lenses)*• Lenses with a significant difference in correction
• Lenses with very strong correction
• Lenses with trifocal correction
• Lenses with large amount of prism
Keep readingglasses
• Retain reading only glasses if frames are in good condition
• Bifocals, which combine a correction for distance on the top andreading on the bottom, should also be retained if prescription can bedetermined.
Keep satisfactoryframes and lenses
• Frames and lenses are in good condition.
• Lenses either have no correction for astigmatism or have astigmaticcorrection on the horizontal axis (0 to 189 degrees).
• Lenses with weak to moderate correction
Recycled Eyeglasses - Recommended Inventory**
SphericalCorrection Only
• Include lenses with low to moderately high amounts of correction
• For patients with astigmatism, use additional spherical equivalent if correction needed in 2 diopters or less (see “Using SphericalEquivalent to Correct for Astigmatism” on page 57)
Adult andChildren’s sizeframes/lenses
• Take a variety of sizes and styles
Sunglasses• No prescription
• Must screen 100% of UV rays
Reading Glasses• Stock should include reading only and bifocals with moderate to low
correction for distance
Cataract Glasses • A few very thick, “Coke bottle” lenses
Safety Goggles • No prescription, designed to be placed over glasses
*Exception: keep glasses with cylinder axis on the horizontal axis (0 to 180 degrees).
**When assembling a stock of recycled eyeglasses, contact eye examiners familiar with the arearegarding the types of frames and lenses needed by local residents.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 59/81
53
Protocol for Dispensing Recycled Eyeglasses
When to Use - Patient’s prescription for corrective lenses has been determined and affordable,
customized eyeglasses are not available to the patient
1. Sort Recycled Eyeglasses
• Examine stock of recycled eyeglasses to identify eyeglasses suitable for dispensing.Sort according to “Recycled Glasses- Criteria for Sorting”.
• Dispose of unsuitable eyeglasses as appropriate.
2. Identify Corrective Power of Lens
• On eyeglasses identified as suitable for dispensing, verify the prescription byperforming the procedure “Measuring the Corrective Power of Eyeglass Lenses” onpage 55.
• If corrective power of the eyeglasses still meets “suitability criteria”, then add toeyeglasses stock. If not, dispose of eyeglasses as appropriate.
3. Locate Best Available Lens and Frames for Patient• Examine patient’s prescription* and identify possible matches between patient’s
prescription and eyeglasses in stock.
• For patients with astigmatism, use “spherical equivalent” calculation on page 58 toidentify suitable eyeglasses.
• Check fit of frame on patient. Adjust if possible. If comfortable fit cannot be achieved,it is unlikely that patient will wear glasses.
4. Measure Patient’s Visual Acuity while Wearing Recycled Glasses
• Check distance vision and near vision using procedures on pages 16 and 17.
• If both distance and near vision are clear, then go to step 5.
• If blurred for either distance or near vision, then try other pairs of eyeglasses withcorrective powers appropriate for patient.
• Check frames for comfort and fit.
5. Give eye health and safety information
• Provide information on hygiene, nutrition, UV protection, & injury prevention.
• Provide patient with instructions for wearing and caring for the eyeglasses.
6. Complete paperwork.
• Complete “Patient Record” form re: prescription dispensed and instructions given topatient for wearing glasses. Maintain forms in patient record files.
**See “How to Read a Prescription” page 62.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 60/81
54
Protocol for Dispensing Reading Glasses
When to Use
• Patient, age 40 or older, experiencing difficulty seeing objects that arenear, such as newspaper, or at low illumination.
• This condition is called Presbyopia. It is caused by a reduction inelasticity of the focusing lens inside the eye.
1Stock andDisplayFrames
• Retain a stock of reading glasses. Include with magnification power rated at +1.00, +1.25, +1.50, +1.75, +2.00, +2.50.
• If dispensing recycled glasses, then include in inventory some glasseswith correction for reading only and other glasses with two corrections,
i.e., for reading and distance vision problems.
2InterviewPatient
• Determine the patient’s age.
• Ask the patient if he/she has other sight difficulties.
• Start a Patient’s Record Form.
3CheckDistanceVision
• Check the patient’s distance vision using Snellen or other standardizedchart.
• Record results.
• If patient has blurred distance and near vision, then he/she has twooptions. He/she can use either bifocals or two pairs of eyeglasses:one for distance vision and another for reading. Do not proceed withthis procedure. Rather go to the applicable Dispensing Protocol(Customized or Recycled Eyeglasses) in this Module.
If patient has clear distance vision and blurred near vision, then go tonext step.
4Select ReadingGlasses basedon Age
• Try out lenses based on age and adjust as needed.
40 years +1.0045 +1.2550 +1.5060 +2.0065 (and above) +2.50 (or as needed)
5Advice Patienton wearinginstructions
• Tell patient that reading glasses are designed for close reading andwork.
• The magnification portion of the reading glasses should not be used tosee distant objects.
6
Give eyehealth andsafetyinformation
• Provide patient with information on hygiene, nutrition, UV protection,and injury prevention.
• Provide patient with instructions for wearing and caring for theeyeglasses.
7Completepaperwork.
• Complete Patient Record form re: prescription dispensed andinstructions given to patient for wearing glasses. Maintain forms inPatient Record files.
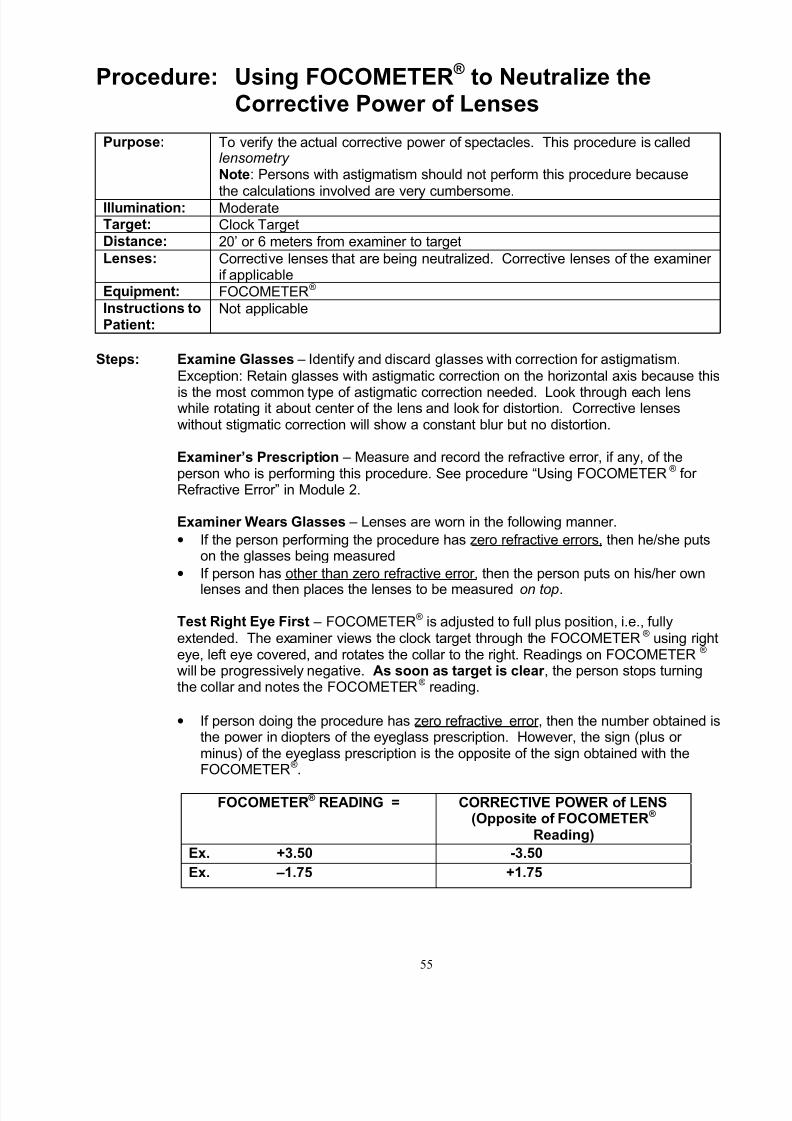
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 61/81
55
Procedure: Using FOCOMETER ® to Neutralize theCorrective Power of Lenses
Purpose: To verify the actual corrective power of spectacles. This procedure is calledlensometry Note: Persons with astigmatism should not perform this procedure because
the calculations involved are very cumbersome.Illumination: ModerateTarget: Clock TargetDistance: 20’ or 6 meters from examiner to targetLenses: Corrective lenses that are being neutralized. Corrective lenses of the examiner
if applicableEquipment: FOCOMETER® Instructions toPatient:
Not applicable
Steps: Examine Glasses – Identify and discard glasses with correction for astigmatism.Exception: Retain glasses with astigmatic correction on the horizontal axis because this
is the most common type of astigmatic correction needed. Look through each lenswhile rotating it about center of the lens and look for distortion. Corrective lenseswithout stigmatic correction will show a constant blur but no distortion.
Examiner’s Prescription – Measure and record the refractive error, if any, of theperson who is performing this procedure. See procedure “Using FOCOMETER® for Refractive Error” in Module 2.
Examiner Wears Glasses – Lenses are worn in the following manner.
• If the person performing the procedure has zero refractive errors, then he/she putson the glasses being measured
• If person has other than zero refractive error, then the person puts on his/her own
lenses and then places the lenses to be measured on top.
Test Right Eye First – FOCOMETER® is adjusted to full plus position, i.e., fullyextended. The examiner views the clock target through the FOCOMETER® using righteye, left eye covered, and rotates the collar to the right. Readings on FOCOMETER® will be progressively negative. As soon as target is clear , the person stops turningthe collar and notes the FOCOMETER® reading.
• If person doing the procedure has zero refractive error, then the number obtained isthe power in diopters of the eyeglass prescription. However, the sign (plus or minus) of the eyeglass prescription is the opposite of the sign obtained with theFOCOMETER®.
FOCOMETER ® READING = CORRECTIVE POWER of LENS(Opposite of FOCOMETER ®
Reading)
Ex. +3.50 -3.50
Ex. –1.75 +1.75
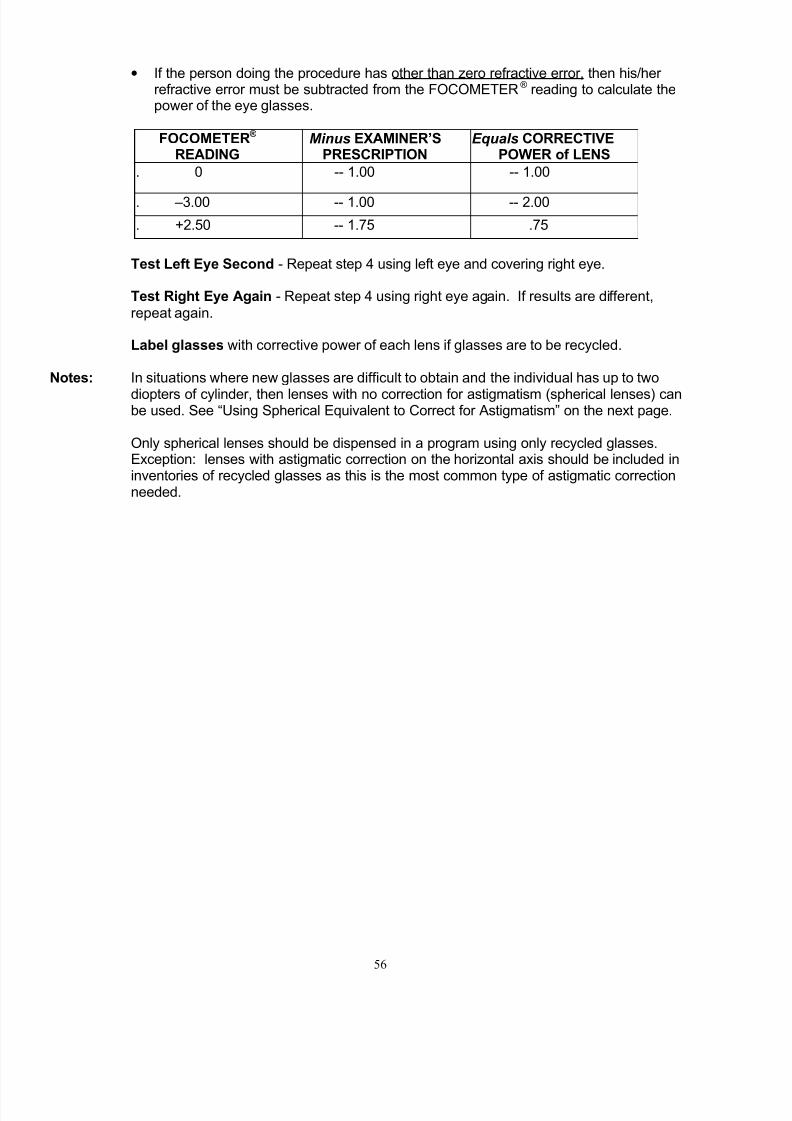
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 62/81
56
• If the person doing the procedure has other than zero refractive error, then his/her refractive error must be subtracted from the FOCOMETER® reading to calculate thepower of the eye glasses.
FOCOMETER ® READING
Minus EXAMINER’SPRESCRIPTION
Equals CORRECTIVEPOWER of LENS
. 0 -- 1.00 -- 1.00
. –3.00 -- 1.00 -- 2.00
. +2.50 -- 1.75 .75
Test Left Eye Second - Repeat step 4 using left eye and covering right eye.
Test Right Eye Again - Repeat step 4 using right eye again. If results are different,repeat again.
Label glasses with corrective power of each lens if glasses are to be recycled.
Notes: In situations where new glasses are difficult to obtain and the individual has up to two
diopters of cylinder, then lenses with no correction for astigmatism (spherical lenses) canbe used. See “Using Spherical Equivalent to Correct for Astigmatism” on the next page.
Only spherical lenses should be dispensed in a program using only recycled glasses.Exception: lenses with astigmatic correction on the horizontal axis should be included ininventories of recycled glasses as this is the most common type of astigmatic correctionneeded.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 63/81
57
Procedure: Using Spherical Equivalent to Correct for Astigmatism
Purpose:
To correct for astigmatism by using additional spherical power instead of cylinder. This procedure is used when lenses with astigmatic correctionare not available and patient’s cylinder in his/her prescription is no more
than two diopters. Over 90% of patients will have a major improvement invisual acuity when spherical power is increased using spherical equivalent
Formula:Spherical measurement + half of the cylinder measurement =spherical equivalent
Steps: 1. Identify patient’s astigmatic error. If not already known, measure astigmatic error using the FOCOMETER® as described in Module 2 – Using FOCOMETER® for
Astigmatic Error.
2. Right Eye First – Review patient’s data on radials.
• First radial (called SPHERE) – Ex. -2.00 diopters at AXIS of 30 degrees
• Second, Perpendicular radial – Ex. -3.50 at AXIS of 120 degrees (always 900 from first radial)
3. Calculate CYLINDER by finding the difference in diopters between the two radials
• Ex. ((-3.50) – (-2.00)) = ((-3.50) + 2.00) = -1.50 diopters
4. Prescription for this eye then requires the following lens:
• Ex. SPHERE –2.00 CYLINDER –1.50 diopters AXIS 120 degrees
5. Calculate SPHERICAL EQUIVALENTSpherical measurement + half of the cylinder measurement
• Ex. -2.00 + -.75 = -2.75 diopters
Correct notation is:
• Ex. R: -2.75 S
6. Left Eye – Repeat steps 2 - 5.
See another example on next page.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 64/81
58
Using Spherical Equivalent to Correct for Astigmatism
Example: Clock Target
Calculating Cylinder
•
First radial (spherical correction).• Second radial perpendicular to first radial.
• CYLINDER calculated by subtractingFOCOMETER® reading at second radial minusFOCOMETER® reading at first radial.
Diopters +1.00 - 1.00 -1.00 – (+1.00)=-1.00 - +1.00=
-2.00Axis 120 degrees 30 degrees 30 degrees
Prescription (Rx) written as follows:
Sphere (SPH) Cylinder (CYL) Axis
+1.00 -2.00* 30 degrees
Spherical Equivalent for same prescription recorded as: +2.00S. Calculation
follows:
Sphere(SPH)
plus ½ of Cylinder
equalsSpherical Equivalent
+1.00 -1.00 0.00plano
*Patients with cylinder of up to 2.00 diopters can be helped using spherical equivalent
1st radial(sphere) Difference between
2nd radial minus 1stradial = Cylinder 2nd radial

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 65/81
59
Sources of Inexpensive Eyeglasses
New Eyeglasses
InFOCUS can offer Eye Deal Eyewear’s Instant Eyeglasses™ at special low prices.Instant Eyeglasses™ are a unique design that allows assembly of frames and lenses
so that individual’s prescription can be dispensed in only a few minutes following theeye exam.
These eyeglasses are optically accurate and correct for myopia, hyperopia, presbyopia,and astigmatic conditions. Lenses are single vision, including correction for astigmatism.
Instant Eyeglasses™ are ideal to use in rural and remote areas with little or no access toan optical lab, or when patients are seen on a one-time basis.
Frame styles are designed to accommodate a broad range of interpupillary distances.Pre-molded round lenses fit into frames that come in sizes to fit almost any face. The sizes
available are large (46mm) and small (42mm) in gold metal frames.
For more information contact Eye Deal Eyewear, Inc. 2620 Manatee Ave W., Ste ABradenton, FL 34205-4944; Phone 866-221-6790.
Example of Instant Eyeglass™ available from InFOCUS
Recycled (used) Glasses
The SBC Pioneers Eyeglass Bank, 1714 Ashland Avenue, Room 23, Houston, Texas 77008;Contact: Wanda Schoellkopf; Ph: 713 865 5713
Lions Clubs Eyeglass Recycling Centers, Visit www.lionsclubs.org to locate a recyclingcenter near you or contact Multi-district Coordinator Denisa Marston, at Texas LionsEyeglass Recycling Center, Midland, Texas Ph: 915 683 3611;Email: [email protected]

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 66/81
60
Procedure for orienting cylinder axis when assemblingInstant Eyeglasses™
Remove demo lenses, if installed, from the frames to be used
1. Place right eyewire of the frame on the clock target below
2. Be sure that the frame bridge and other eyewire is placed parallel to the 3-9 o’clock or 180degree axis, or parallel to the bottom of the page
3. Mark the prescription axis on the frame rim with a dot or line
4. Align the lens axis mark with the frame mark
5. Install the right eye prescription in the right lens frame
6. Repeat procedure for the left lens
eyewire
nosepad
Bridge
frame front
Front of frame
hinges
temples

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 67/81
61
Procedure: Measuring Pupillary Distance (PD)
Purpose: To determine the distance between the pupils when fixated on a distanceobject (Distance PD) and on a near object (Near PD). When eyeglassesmatch the PD of the patient, the patient sees through the optical center of the lenses without straining.
Illumination:Moderate
Target: Penlight
Distance: 14”
Lenses: None
Other materials: Millimeter ruler, pen, and patient record
Instructions: Tell patient to fixate at the penlight with both eyes open and to stay still.
To measure Near Pupillary Distance (P.D.)1. Examiner holds penlight close to his/her left eye 14” in front of the patient. Examiner closes
his/her right eye.
2. Examiner tells patient to look at the penlight with both eyes open.3. Examiner holds a centimeter ruler in front of the patient and aligns the zero on the ruler with
the outer edge of the patient’s right iris.4. Examiner finds the Near P.D. by noting the distance between
• the outer edge of the patient’s right iris and
• the inner edge of the patient’s left iris. See diagram below.5. Record the Near P.D.Examiner and Patient: Be careful not to move ruler or head between measuring Near P.D.and Distance P.D.
To measure Distance Pupillary Distance (P.D.)
1. Examiner moves penlight to just below his/her right eye. Examiner closes his/her left eye.2. Examiner tells patient to keep looking at the penlight with both eyes open.3. Examiner finds the Distance P.D. by noting the distance between
• the outer edge of the patient’s right iris where the ‘zero’ on the ruler is placed as shownin the diagram below.
• the inner edge of the patient’s left iris.This is the ‘Distance P.D.’ Without moving the ruler now the patient is asked to look at thepenlight just below the examiner left eye.
4. Examiner records the Distance P.D. (Same two points as in step 3)
Notes: P.D. is usually within a range of 55 to 75 centimeters. Near P.D. is always less thanDistance P.D. and the difference is typically approximately 3 centimeters.
Record: Near P.D. Distance P.D.
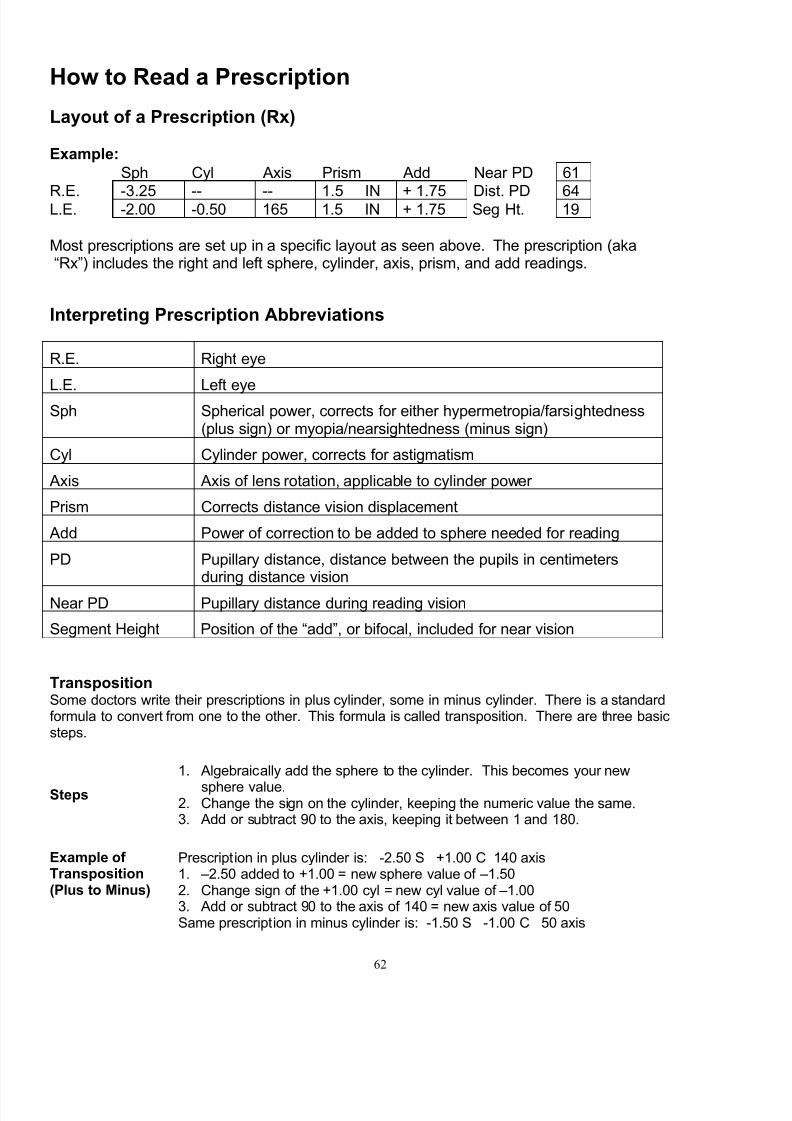
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 68/81
62
How to Read a Prescription
Layout of a Prescription (Rx)
Example:
Sph Cyl Axis Prism Add Near PD 61
R.E. -3.25 -- -- 1.5 IN + 1.75 Dist. PD 64L.E. -2.00 -0.50 165 1.5 IN + 1.75 Seg Ht. 19
Most prescriptions are set up in a specific layout as seen above. The prescription (aka“Rx”) includes the right and left sphere, cylinder, axis, prism, and add readings.
Interpreting Prescription Abbreviations
R.E. Right eye
L.E. Left eyeSph Spherical power, corrects for either hypermetropia/farsightedness
(plus sign) or myopia/nearsightedness (minus sign)
Cyl Cylinder power, corrects for astigmatism
Axis Axis of lens rotation, applicable to cylinder power
Prism Corrects distance vision displacement
Add Power of correction to be added to sphere needed for reading
PD Pupillary distance, distance between the pupils in centimetersduring distance vision
Near PD Pupillary distance during reading vision
Segment Height Position of the “add”, or bifocal, included for near vision
TranspositionSome doctors write their prescriptions in plus cylinder, some in minus cylinder. There is a standardformula to convert from one to the other. This formula is called transposition. There are three basicsteps.
Steps
1. Algebraically add the sphere to the cylinder. This becomes your new
sphere value.2. Change the sign on the cylinder, keeping the numeric value the same.3. Add or subtract 90 to the axis, keeping it between 1 and 180.
Example of Transposition(Plus to Minus)
Prescription in plus cylinder is: -2.50 S +1.00 C 140 axis1. –2.50 added to +1.00 = new sphere value of –1.502. Change sign of the +1.00 cyl = new cyl value of –1.003. Add or subtract 90 to the axis of 140 = new axis value of 50Same prescription in minus cylinder is: -1.50 S -1.00 C 50 axis
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 69/81
63
Module 7 – Record Keeping
Maintaining Clinical and Fiscal Records
Record keeping is key to:
• Providing good service to patients
• Monitoring the use and cost/benefit of services and products provided
Clinical Records
• Use a Patient Record form designed to capture information about the patient’s history,vision check, health check, etc.
• Require that Patient Record form be used with every patient and signed by the personperforming the exam.
•Require that the Patient Record form is filed in an accessible and secure place and thateither a person or position is designated to maintain the files.
• Periodically, check to ensure that Patient Record forms are being completed and retainedfor each patient.
• At least once a year, compile statistics from the Patient Record forms to determine patternsand to identify possible areas of improvement.
Referral Forms
• When referring the patient to a specific provider, provide them with a written referral formon which the provider’s name, location, and phone number is listed.
• Record referral information on Patient’s Record.
Inventory Forms
• Document orders placed and shipments received for frames and lenses
• Review periodically to identify trends and areas for improvement
Fiscal Records
• Identify the costs and revenues associated with the eye-related activities.
• Identify how each cost and revenue will be tracked. Document in writing.
• Implement tracking system and create monthly reports of cost vs. revenue.• At least once a year, review tracking system to identify areas for improvement.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 70/81
64

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 71/81
65
Appendix
Glossary
Add - The add power is the amount of correction to be added to the sphere for a
reading or near power. The add power assists the weakened eye muscles to viewcloser objects. It is usually a value between +1.00 and +3.00. We commonly use abifocal for this. A bifocal is a lens that has the distance correction in the normal viewingarea and a smaller segment for reading lower in the lens. We commonly use a Flat top28 (FT – 28). A FT –28 is a half circle segment add with a 28mm diameter
Astigmatism – a condition caused by an irregularity in the shape of the cornea whichprevents light from focusing correctly on the retina thereby causing blurred vision.Symptoms may include headaches, fatigue, eye strain, or blurred vision at certain or alldistances.
Axis – the location of the cylinder component in the compound lens. Written as adegree of rotation from 0-180 degrees.
Bifocal - a lens that is designed with two different prescription areas to correct for bothnear and distance vision.
Bridge - the part of a spectacle frame that extends across the nose.
Compound lens – a lens which combines both spherical and cylinder lenses.
Cylinder - The amount of correction needed beyond the sphere to correct for astigmatism. This could be written in two forms, either plus or minus cylinder. It is
identified by a “+” or “-“ in front of the value. There is a formula that allows you toconvert from plus to minus or minus to plus. It is called transposition. See below for theformula. Minus cylinder is most commonly used and is the conversion preferred byoptometrists. Plus cylinder is often used by ophthalmologists.
Cylinder lens – a lens with a surface shaped like a rod (cylinder). Used in combinationwith spherical lenses for patients with astigmatism and spherical error.
Diopter (D) - Unit to designate the refractive power of a lens.
Hyperopia - farsightedness; vision of nearby objects is impaired, while distance objects
remain in relative focus. Light is focused on a point that lies behind the retina.
Iris - Pigmented tissue lying behind the cornea that gives color to the eye (e.g., blueeyes) and controls amount of light entering the eye by varying the size of the pupillaryopening.
Lens - transparent structure within the eye that focuses light rays upon the retina.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 72/81
66
Myopia - nearsightedness; close objects are in relative focus while distant objects areblurred. Light is focused on a point that lies in front of the retina.
Ophthalmologist - a doctor of medicine (M.D.) or doctor of osteopathy (D.O.) whospecializes in both the medical treatment and surgical care of the eyes and the visualsystem. Ophthalmologists must complete four or more years of medical school, oneyear of internship, and three or more years of specialized training and experience.
Optician - state licensed professionals who interpret and fill a prescription from an
optometrist or ophthalmologist for corrective eyewear. An optician is trained in theselection and fitting of eyeglasses and contacts (with special license). Qualifications for licensure include successful completion of a 2 year college program in optical scienceor a 2 year apprenticeship under a licensed optician or optometrist, followed by a statelicense examination. Opticians must also attend continuing education classes each year to maintain their license.
Optometrist - doctors of optometry (O.D.) who specialize in the examination of theeyes and the visual system as well as the diagnosis and treatment of certain ocular
diseases, injuries, and other health problems. An optometrist can prescribe manyophthalmic medications, but cannot perform surgery. They may, however, participate inpre-operative and post-operative care relating to eye surgery. Optometrists mustcomplete four years of post-graduate optometry school.
PD - The PD is the distance between the pupils in centimeters. Near PD is measuredwhen the eyes are fixated on a close object. Because the eyes must turn in to viewnearby objects, Near PD is always smaller than Distance PD. The normal differencebetween Near PD and Distance PD is approximately 3 centimeters. See Appendix for procedure on how to measure PD.
Plus and minus notation for lenses that correct astigmatism - compound lenses aremanufactured by combining a spherical lens with a cylinder lens. The cylindricalcompound lens may be considered either a negative or positive diopter lens. Theconvention that is used must be indicated by a plus (+) or negative (-) sign before thepower of cylinder correction.
Prism – a wedge shaped component of an optical lens is used in prescription glassesfor correcting near vision and or for correcting a patient with strabismus.
Presbyopia – an inability to see items clearly at reading distance. The natural lens inthe eye is unable to focus due to structural changes as a result of aging.
Pupil - the adjustable opening at the center of the iris that allows variable amounts of light into the eye. The pupil will expand or dilate in response to low light conditions in anattempt to bring more light into the eye and will reduce in size when intense light ispresent.
Refraction - test to determine an eye's refractive error and the best corrective lenses tobe prescribed. Series of lenses in graded powers are presented to determine whichprovide sharpest, clearest vision.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 73/81
67
Refractive error - optical defect in an unaccommodating eye; parallel light rays are notbrought to a sharp focus precisely on the retina, producing a blurred retinal image. Canbe corrected by eyeglasses, contact lenses, or refractive surgery.
Retina - a thin layer of light sensitive nerve tissue lining the interior of the eye that
translates light waves into nerve impulses that are sent to the brain.
Retinal detachment - occurs when the retina separates from the rear wall of the eye.Vision loss occurs at these detached areas.
Sclera - the outer layer of the eye that forms the visible white area of the eye and
extends from the cornea in the front of the eye to the back of the eye where it meetsand surrounds the optic nerve.
Sphere - The amount of correction needed to correct for near (myopia) or far
sightedness (hypermetropia). There is no limit to what the correction could be. Thenormal range is +6.00 to –6.00.
Spherical lens – either concave (minus or negative power) or convex (plus or positivepower) in shape used to correct visual refractive errors. Concave lenses correct myopia(nearsightedness) by causing light to diverge. Convex lenses correct hyperopia(farsightedness) by causing light to converge.
20/20 - Normal visual acuity. Upper number is the standard distance (20 feet) betweenan eye being tested and the eye chart; lower number indicates that a tested eye cansee the same small standard-sized letters or symbols as a normal eye at 20 feet.
Visual acuity – how clearly a person can see either at distance or near. Visual acuitymeasurements are assessed with visual targets at standard distances of 20 feet or 6
meters at distance and 14 inches at near.

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 74/81
68

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 75/81
69
Eye Care Links
The following resources will help you make informed decisions, but they are not asubstitute for medical care. Discuss information provided in these links with your healthcare provider. If you are experiencing problems with your vision or eyes, visit aneye care professional immediately.
I. How Vision Systems Work
1. American College of Chiropractic Rehabilitation Science ..................www.accrs.org 2. Anchorage Health Online.................................................www.anchoragehealth.org 3. American Psychological Association.................................................... www.apa.org 4. CenterWatch Clinical Trials Listing Service............................www.centerwatch.com 5. University of Texas Dept of Computer Sciences ........................ www.cs.utexas.edu 6. Jacob L. Driesen. Ph.D. Neuropsychology & Medical Resources . www.driesen.com 7. Galaxy Search Engine.....................................................................www.galaxy.com 8. How Stuff Works ................................................................ www.howstuffworks.com 9. The Hybrid Vigor Institute..........................................................www.hybridvigor.net
10. International Society of Refractive Surgery ...........................................www.isrs.org 11. The Vision Correction Website.....................................................www.lasersite.com 12. Worldwide Directory of Eye Care [email protected] 13. Macular Degeneration Support ................................................. www.mdsupport.org 14. New York Online Access to Health ......................................... www.noah-health.org 15. Sola Eyeglass Lenses for the Way you Live ...................................... www.sola.com 16. St. Luke’s Cataract & Laser Institute........................................www.stlukeseye.com 17. University of Rochester Medical Center ................................ www.stronghealth.com 18. SUNY State College of Optometry ................................................www.sunyopt.edu 19. Think Quest...............................................................................www.thinkquest.com 20. Vision Channel ......................................................................www.visionchannel.net
21. York University ....................................................................................www.yorku.ca
II. General Eye Care
1. Meredith W. Morgan University Eye Center ..............................www.caleyecare.org 2. Caring for Kids ..................................................................www.caringforkids.cps.ca 3. Centers for Disease Control and Prevention........................................ www.cdc.gov 4. Center Watch Clinical Trails Listing Service...........................www.centerwatch.com 5. Eye Care Office of Ofner & Fleming.................................www.eugeneeyecare.com 6. NJSOP Society of Optometric Physicians......................................www.eyecare.org 7. Eye care India .......................................................................www.eyecareindia.com
8. EyeMDLink..............................................................................www.eyemedlink.com 9. The Stanford Health Library..................................... www.healthlibrary.stanford.edu 10. Health on the Net Foundation ................................................................www.hon.ch 11. The Eye Site A Real Site for Sore Eyes.............................................www.i-care.net 12. Laser Eye Surgery Doc Shop............................ www.lasereyesurgerydocshop.com 13. Physician-Patient Communications Network.................................www.medem.com 14. Methodist Health Care System.........................................www.methodisthealth.com 15. My Healthy Eyes ...............................................................www.myhealthyeyes.com 16. National Eye Institute ......................................................................www.nei.nih.gov 17. Internet Ophthalmology.....................................................................www.opthal.org
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 76/81
70
18. Optometrists Association Australia ....................................www.optometrists.asn.au 19. ORBIS Saving Sight Worldwide.....................................................www.orbis.org-hk 20. Royal National Institute of the Blind.................................................www.mib-org.uk 21. St. Luke’s Cataract & Laser Institute.......................................www.stlukes-eye.com 22. Sports Vision Institute .......................................................... www.vision4sports.com 23. The Cornea and Laser Eye Institute .................................. www.vision-institute.com 24. Vision Therapy....................................................................www.vision-therapy.com
III. Common Vision Problems
1. Adult Strabismus................................................................www.adultstrabismus.org 2. Alan Optics ............................................................................www.alanoptics.per.sg 3. All About Vision................................................................... www.allaboutvision.com 4. Bausch & Lomb..............................................................................www.bausch.com 5. Canadian Pediatric Society............................................... www.caringforkids.cps.ca 6. Cascade Eye Center................................................................www.cascadeye.com 7. The Low Vision Centers of Indiana.................................... www.eyeassociates.com 8. EyeMAC Development, LLC.........................................................www.eyemac.com
9. Eyesite Canadian Ophthalmological Society ....................................www.eyesite.ca 10. American Academy of Family Physicians ............................... www.familydoctor.org 11. Discovery Health Channel .............................................. www.health.discovery.com 12. Eye & Vision Care Health Ctr..... www.health.yahoo.com/health/centers/eye_vision /13. Health On the Net Foundation ............................................................... www.hon.ch 14. University of Michigan Kellogg Eye Center..........................www.kellogg.umich.edu 15. Very Best Kids! .......................www.wywy.essortment.com/kidsinformatio_rsdh.htm 16. Mayo Clinic .............................................................................. www.mayoclinic.com 17. American Academy of Ophthalmology..........................................www.medem.com 18. Methodist Health Care System ........................................www.methodisthealth.com 19. Myopia Manual by Dr. Klaus Schmid .................................. www.myopia-manual.de
20. British Columbia Association of Optometrists ......................www.optometrists.bc.ca 21. Patanol.......................................................................................... www.patanol.com 22. Parents Active for Vision Education........................................... www.pave-eye.com 23. Prevent Blindness America..............................................www.preventblindness.org 24. Sola International................................................................................www.sola.com 25. St. Luke’s Cataract & Laser Institute.......................................www.stlukes-eye.com 26. The Med Guide – Eye Care ....................................www.themeguide.com/docs/eye 27. University Health Services .....................................................www.uhs.berkeley.edu 28. Colorado Optometric Association................................................www.visioncare.org 29. The Vision Help Network .......................................................... www.visionhelp.com 30. Vision Therapy....................................................................www.vision-therapy.com
31. Vision World Wide........................................................................ www.visionww.org 32. Vision, Reading and Computer Users.........................................www.webword.com
IV. Refractive Surgery
1. Laser Eye Center of Silicon Valley.........................................www.2020eyesite.com 2. Alcon..........................................................................................www.alconlabs.com 3. All About Vision................................................................... www.allaboutvision.com 4. American Society of Cataract & Refractive Surgery........................... www.ascrs.org 5. Ask Lasik Doctors.................................................................www.asklasikdocs.com

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 77/81
71
6. The Harman Eye Clinic ...................................................www.cascaderegional.com 7. The Cleveland Clinic ........................................................... www.clevelandclinic.org 8. Clinica Reinoso ...................................................................www.clinicareinoso.com 9. Hayden & Kovach Eye Center................................. www.eyelaser-chicagoland.com 10. Eye Search The Ultimate Eye & vision Portal .......................... www.eyesearch.com 11. International Society of Refractive Surgery ...........................................www.isrs.org 12. The Vision Correction Website.................................................... www.lasersite.com
13. Laser Surgery for Eyes.............................................. www.lasersurgeryforeyes.com 14. LASIK Institute ........................................................................www.lasikinstitute.org 15. U.S. National Library of Medicine...................................................www.nlm.nih.gov 16. Pacific Cataract and Laser Institute..................................................... www.pcli.com 17. Park and Lasik Today ..........................................................................www.prk.com 18. Refractec.....................................................................................www.refractec.com 19. Refractive Source............................................................ www.refractivesource.com 20. Review of Refractive Surgery............................www.reviewofrefractivesurgery.com 21. Slack Inc. Healthcare Specialty....................................................www.slackinc.com 22. Council for Refractive Surgery Quality Assurance ........................www.usaeyes.org
V. Eyewear
1. All About Vision...................................................................www.allaboutvision.com 2. Andersen Eye Associates ....................................................www.anderseneye.com 3. Bausch & Lomb............................................................................. www.bausch.com 4. CIBA Vision...............................................................................www.cibavision.com 5. Contact Lens Manufacturers Association............................................www.clma.net 6. UK Internet Shopping......................................................www.come-shopping.co.uk 7. Contact Lens Council ....................................................www.contactlenscouncil.org 8. Guide from Contact Lens Manufacturers Association .......... www.contactlenses.org 9. University of Tennessee Dept of Ophthalmology .....................www.eye.utmem.edu
10. Eyewear Concepts........................................................www.eyewearconcepts.com 11. Paul Adler Optometrist UK........................................................ www.eyezone.co.uk 12. Frames Direct........................................................................www.framesdirect.com 13. InFOCUS Interprofessional Fostering of Ophthalmic Care for Underserved Sectors
.............................................................................................. www.infocusonline.org 14. Knighton Optical................................................................www.knightonoptical.com 15. LensCrafters........................................................................... www.lenscrafters.com 16. Lens Express .........................................................................www.lensexpress.com 17. My Eye Net................................................................................ www.myeyenet.com 18. Novelty Contact Lenses ........................................ www.novelty-contact-lenses.com 19. Optima..................................................................................www.optima-hyper.com
20. Outpost Optical ...................................................................www.outpostoptical.com 21. Renton Vision Source ............................................................www.rentonvision.com 22. Prescription Dive Mask............................................................www.rxdivemask.com 23. The Eye Center.....................................................................www.sandiegoeye.com 24. Virginia Beach Eye Surgery ............................................................ www.vbeye.com 25. Vision 1 to 1 ..............................................................................www.vision1to1.com 26. Vision Colored Contact Lenses...................... www.visioncoloredcontactlenses.com 27. Vision RX ......................................................................................www.visionrx.com 28. Vision Web................................................................................ www.visionweb.com 29. WPS Optometrists UK...................................................www.wpsoptometrists.co.uk
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 78/81
72
30. Contact Lenses and Lens Wear Information Portal....................www.wwwcops.com
VI. Eye Diseases
1. American Academy of Ophthalmology..................................................www.aao.org 2. American Health Assistance Foundation ............................................www.ahaf.org 3. All About Vision................................................................... www.allaboutvision.com
4. American Optometric Association....................................................www.aoanet.org 5. The American Society of Cataract & Refractive Surgery ...................www.ascrs.org 6. American Society of Ophthalmic Plastic & Reconstructive Surgery.www.asoprs.org 7. Home Foundation Fighting Blindness ......................................... www.blindness.org 8. The Harman Eye Clinic ...................................................www.cascaderegional.com 9. Dr. Angela Howell, Optometrist......................................... www.drangelahowell.com 10. eMedicine Clinical Knowledge Base .........................................www.emedicine.com 11. Eye Atlas of Ophthalmology.........................................................www.eyeatlas.com 12. Eye Cancer Network .................................................................www.eyecancer.com 13. Eye Disease Online: Your Eye Disease Information Center ..www.eye-disease.com 14. Eye MD Link..............................................................................www.eyemdlink.com
15. Glaucoma Research Foundation ................................................www.glaucoma.org 16. Glaucoma Foundation...............................................www.glaucomafoundation.com 17. Health Library at Stanford ........................................ www.healthlibrary.stanford.edu 18. Center for Keratoconus...................................................................www.kcenter.org 19. Lighthouse International............................................................. www.lighthouse.org 20. The Low Vision Gateway .............................................................www.lowvision.org 21. Understanding & Coping with Macular Diseases ............................www.macula.org 22. American Macular Degeneration Foundation............................... www.macular.com 23. Macular Degeneration Network................................www.macular-degeneration.org 24. Macular Degeneration Support ..................................................www.mdsupport.org 25. Medem Inc. ...................................................................................www.medem.com
26. Free Medical Dictionary ..........................................................www.medfriendly.com 27. The Merck Manual of Medical Information ...................................... www.merck.com 28. Karolinska Institute.......................................http://www.mic.ki.se/Diseases/c11.html 29. My Eye World.........................................................................www.myeyeworld.com 30. National Association for Visually Handicapped...................................www.navh.org 31. New England Eye Center.................................................................. www.neec.com 32. National Eye Institute...................................................................... www.nei.nih.gov 33. New York Institute for Special Education........................................... www.nyise.org 34. Prevent Blindness America..............................................www.preventblindness.org 35. Red Atlas – Recognizing Eye Disease......................................... www.redatlas.com 36. All About Retinitis-Pigmentosa...................................www.retinitis-pigmentosa.com
37. American College of Rheumatology......................................www.rheumatology.org 38. International Surgical Eye Expeditions............................................. www.seeintl.org 39. St Luke’s Cataract & Laser Institute......................................... www.stlukeseye.com 40. Retina Information Source ................................................www.theretinasource.com 41. Helen Keller International Trachoma Program........................ www.trachomahki.org 42. Vision Channel......................................................................www.visionchannel.net 43. Vision Works, Inc. .............................................................www.visionworksusa.com 44. Vitreous-Retina-Macula Consultants............................................... www.vrmny.com 45. Washington Academy of Eye Physicians & Surgeons ............... www.wa-eyemd.org
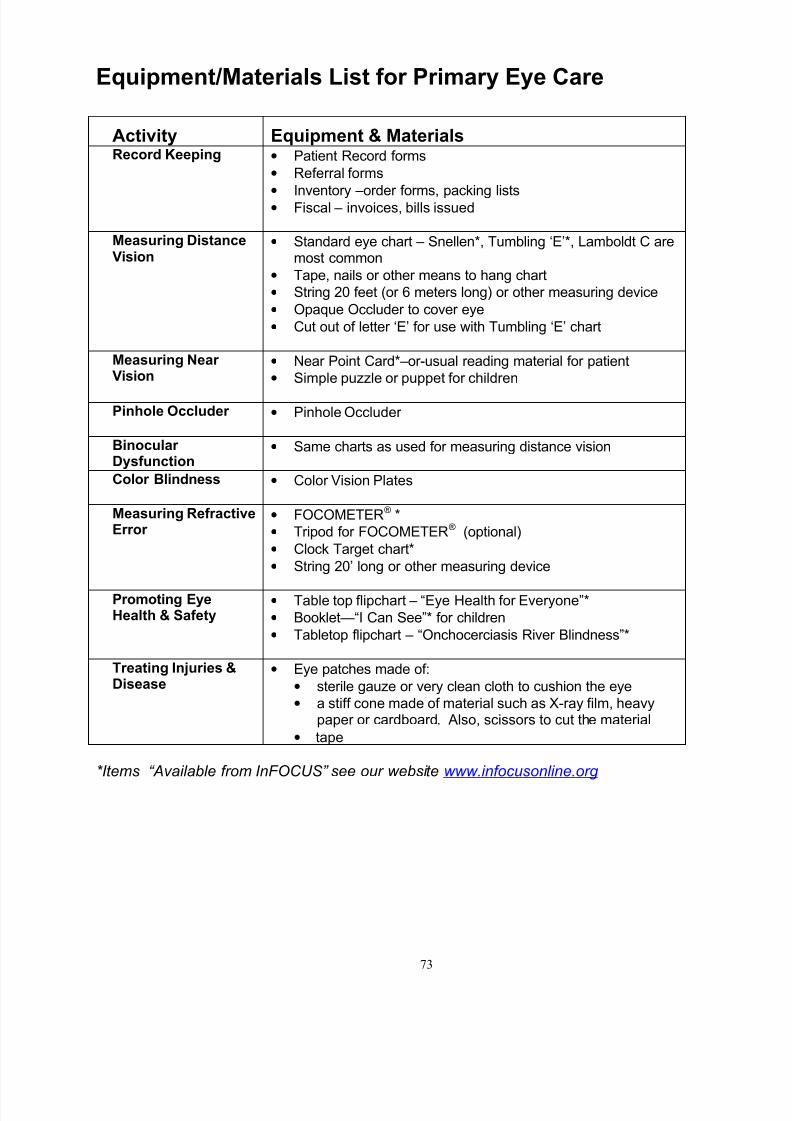
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 79/81
73
Equipment/Materials List for Primary Eye Care
Activity Equipment & MaterialsRecord Keeping • Patient Record forms
• Referral forms
•
Inventory –order forms, packing lists• Fiscal – invoices, bills issued
Measuring DistanceVision
• Standard eye chart – Snellen*, Tumbling ‘E’*, Lamboldt C aremost common
• Tape, nails or other means to hang chart
• String 20 feet (or 6 meters long) or other measuring device
• Opaque Occluder to cover eye
• Cut out of letter ‘E’ for use with Tumbling ‘E’ chart
Measuring Near Vision
• Near Point Card*–or-usual reading material for patient
• Simple puzzle or puppet for children
Pinhole Occluder • Pinhole Occluder
Binocular Dysfunction
• Same charts as used for measuring distance vision
Color Blindness • Color Vision Plates
Measuring RefractiveError
• FOCOMETER® *
• Tripod for FOCOMETER® (optional)
• Clock Target chart*
• String 20’ long or other measuring device
Promoting EyeHealth & Safety
• Table top flipchart – “Eye Health for Everyone”*
• Booklet—“I Can See”* for children
• Tabletop flipchart – “Onchocerciasis River Blindness”*
Treating Injuries &Disease
• Eye patches made of:
• sterile gauze or very clean cloth to cushion the eye
• a stiff cone made of material such as X-ray film, heavypaper or cardboard. Also, scissors to cut the material
• tape
*Items “Available from InFOCUS” see our website www.infocusonline.org
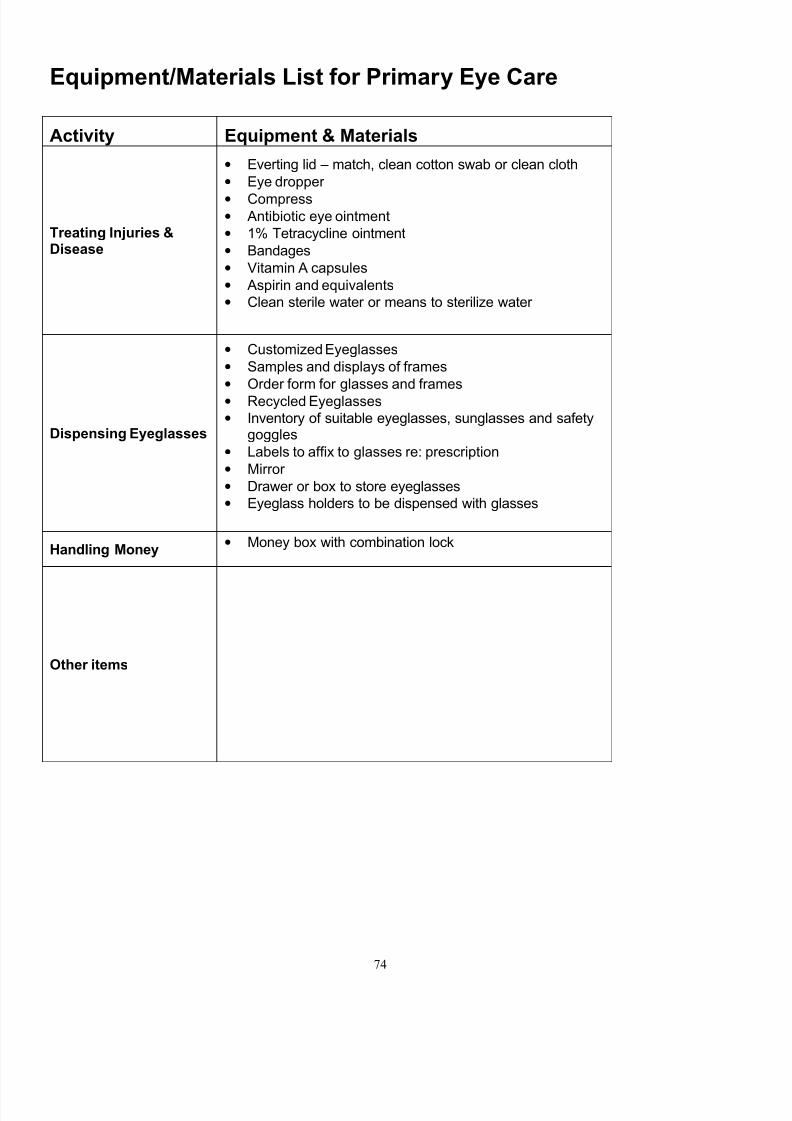
7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 80/81
74
Equipment/Materials List for Primary Eye Care
Activity Equipment & Materials
Treating Injuries &Disease
• Everting lid – match, clean cotton swab or clean cloth
• Eye dropper
• Compress• Antibiotic eye ointment
• 1% Tetracycline ointment
• Bandages
• Vitamin A capsules
• Aspirin and equivalents
• Clean sterile water or means to sterilize water
Dispensing Eyeglasses
• Customized Eyeglasses
• Samples and displays of frames
• Order form for glasses and frames
• Recycled Eyeglasses
• Inventory of suitable eyeglasses, sunglasses and safetygoggles
• Labels to affix to glasses re: prescription
• Mirror
• Drawer or box to store eyeglasses
• Eyeglass holders to be dispensed with glasses
Handling Money• Money box with combination lock
Other items

7/29/2019 Primary Eye Care Manual
http://slidepdf.com/reader/full/primary-eye-care-manual 81/81