primary ovarian insufficiency
TRANSCRIPT
Narmeen Hassan MS5
Final year medical student
Dow Medical College, Pakistan
Primary Ovarian Insufficiency
CaseIntroductionNormal Anatomy of the Female Genital TractPrevalenceCausesRisk FactorsClinical PresentationDiagnosisTestsTreatmentOther associated heath conditionsCounseling and follow-up
Contents
21 year Female Gravida 0 with primary amenorrhea and hot flushes. Endocrine studies have been normal (prolactin, thyroid and DHEA- Sulphate) with the exception of FSH and LH that were high in the postmenopausal range. Her thyroglobulin antibodies and ANA antibodies were negative. Her chromosomal karyotyping was 46XX which is normal. She is a non smoker, no history of hepatitis or renal disease. She is not diabetic.
O/E – BP 126/80 ,Weight 241 Lbs, Height 5 ft 11 inches. Thyroid gland is normal. No lymphadenopathies. Breast exam is normal. Abdomen was soft. No masses or tenderness in the abdomen. Pelvic Exam was normal.
Case
Diagnosis
Idiopathic Primary Ovarian Insufficiency
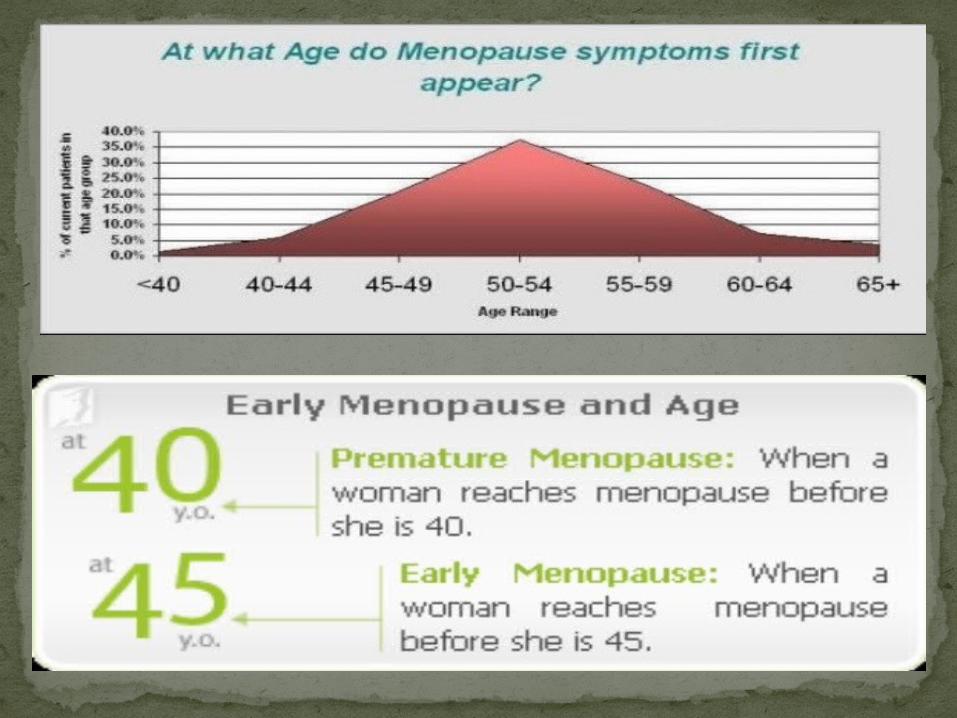
The depletion or dysfunction of ovarian follicles with cessation of menses before age 40 years
Also known as hypergonadotropic hypogonadismThe term “premature menopause” has fallen out of
favor. “Primary ovarian insufficiency” is the preferred term advocated by the National Institutes of Health because ovarian function is intermittent or unpredictable in many cases.
Because 5–10% of women with primary ovarian insufficiency experience spontaneous conception and delivery, primary ovarian insufficiency can be distinguished from natural menopause and also may be described as decreased ovarian reserve
What is Primary Ovarian Insufficiency
Depending on the cause, premature ovarian failure may develop as early as the teen years, or the problem may have been present from birth.
There is no consensus on criteria to identify primary ovarian insufficiency in adolescents, and delay in diagnosis is common.
Health care providers who make this clinical diagnosis should be mindful of the sensitive nature of this medical condition
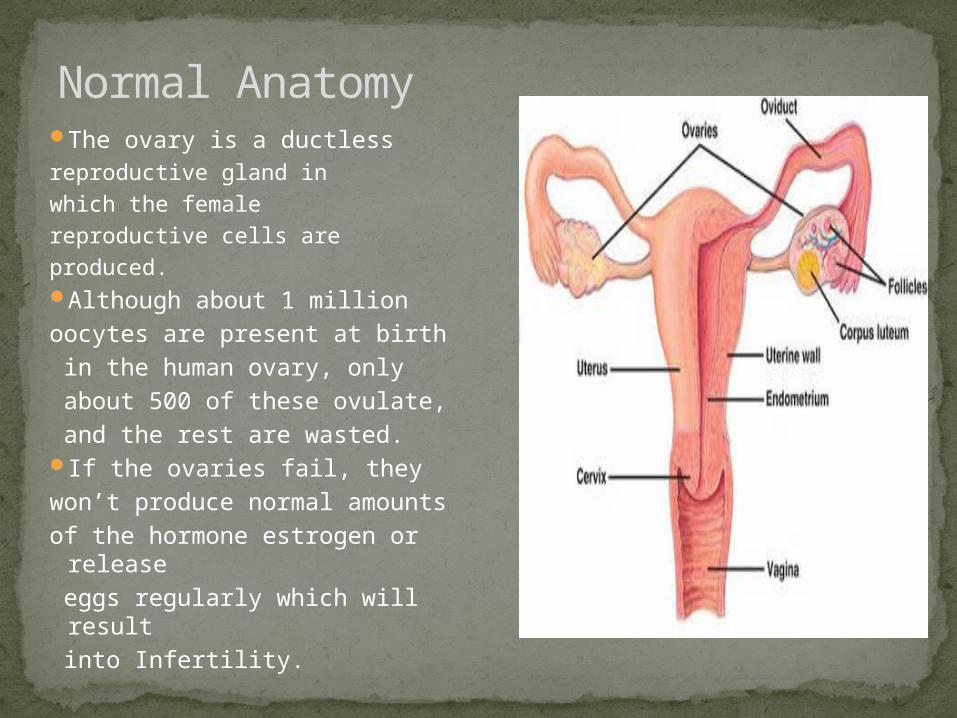
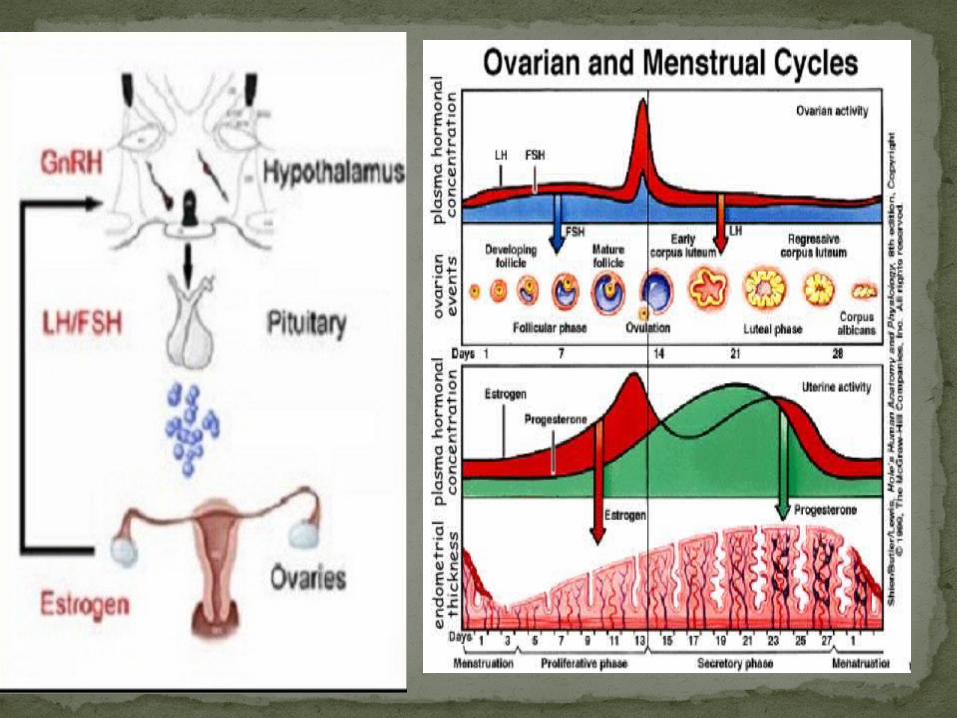
The ovary is a ductless reproductive gland in which the female reproductive cells are produced. Although about 1 million oocytes are present at birth in the human ovary, only about 500 of these ovulate, and the rest are wasted. If the ovaries fail, they won’t produce normal amounts of the hormone estrogen or
release eggs regularly which will result into Infertility.
Normal Anatomy
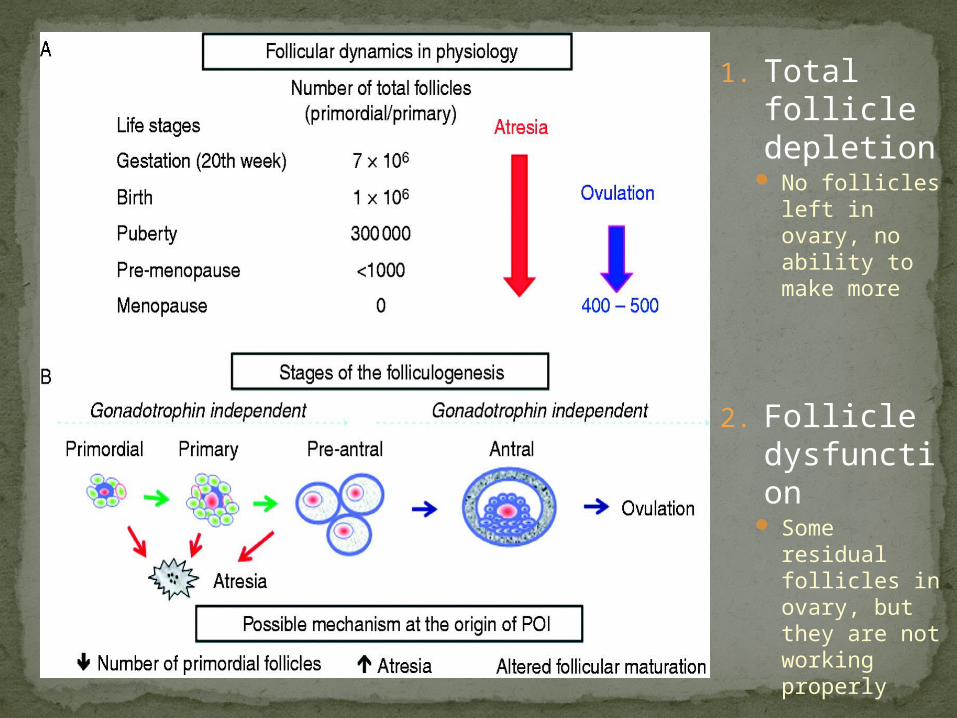
1. Total follicle depletion
No follicles left in ovary, no ability to make more
2. Follicle dysfunction
Some residual follicles in ovary, but they are not working properly
1/250 by age 351/100 by age 40
Prevalence
UnknownGenetic: 10-20 percent of women with POF have a family
historyAutoimmune: association with thyroid dysfunction,
hypoparathyroidism , hypoadrenalism and diabetes MUST SCREEN FOR THESE CO-MORBIDITIES!
ChemotherapyRadiationCigarette SmokeChemicalsPesticidesTuberculosis of the genital tract Ovarian failure following hysterectomyProlonged GnRH (Gonadatrophin Releasing Hormone) therapyEnzyme defects Resistant ovary Induction of multiple ovulation in infertility
Causes

Chromosomal DefectsCertain genetic disorders are associated which include
Turner's syndrome, a condition in which a woman has only one X chromosome instead of the usual two, and fragile X syndrome.
Toxins Chemotherapy and radiation therapy are the most
common causes of toxin-induced ovarian failure. These therapies may damage the genetic material in cells. Other toxins such as cigarette smoke, chemicals, pesticides and viruses may hasten ovarian failure.
Autoimmune Immune system may produce antibodies against own
ovarian tissue, harming the egg-containing follicles and damaging the egg. What triggers the immune response is unclear, but exposure to a virus is one possibility.
Age : The risk of ovarian failure rises sharply between age 35 and age 40.
Family history : Having a family history of premature ovarian failure increases your risk of developing this disorder
Risk factors
Most common first symptoms: irregular periods, Infertility
Symptoms similar to menopauseHot flashes, night sweatsIrritability, poor concentrationDecreased libidoVaginal dryness
Symptoms of Premature Ovarian Failure
Diagnosis and Initial Evaluation of Primary Ovarian Insufficiency
Menstrual irregularity for at least 3 consecutive monthsFollicle-stimulating hormone and estradiol levels (two
random tests at least 1 month apart)Prolactin and thyroid function test
If diagnosis is confirmed:KaryotypeFMR1 permutationAdrenal antibodies
— 21-hydroxylase (CYP21) by immunoprecipitationor
— Indirect immunofluorescence Pelvic ultrasonography
Antimüllerian hormone With further research, antimüllerian hormone testing may
become increasingly valuable in assessing ovarian reserve before and after chemotherapy for young women with cancer, before and after ovarian surgery, and for females at high risk of primary ovarian insufficiency
Inhibin B. There is significant variability in inhibin B levels between
menstrual cycles. This marker does not reliably predict a poor response to ovarian stimulation, and thus, inhibin B is not a recommended test.
Surrogate markers of ovarian reserve (presence of regular menses, serial serum estradiol levels, and antral follicle count by transvaginal ultrasonography) are highly variable and are not predictive of future fertility or hormonal production in young women who have undergone treatment for cancer , but are currently undergoing investigation.
Other Tests
No proven treatment to restore ovarian functionHRT for vasomotor symptoms, promotion of bone
health (can use OCPs)Estrogen is typically prescribed with progesterone. Adding progesterone protects the lining of your uterus
(endometrium) from precancerous changes caused by taking estrogen alone.
In older women, long-term estrogen plus progestin therapy has been linked to an increased risk of heart and blood vessel (cardiovascular) disease and breast cancer.
In young women with premature ovarian failure, however, the benefits of hormone replacement therapy for heart health may outweigh the potential risks.
Treatment
Calcium, Vitamin D are important for preventing osteoporosis.
A bone density test shall be suggested before starting supplements to get a baseline bone density measurement.
For women ages 19 through 50, the Institute of Medicine recommends 1,000 milligrams (mg) of calcium a day through food or supplements, increasing to 1,200 mg a day for women age 51 or older.
Monitor for development of hyperplasia, bleeding
OsteoporosisHypothyroidismAddison's diseaseDiabetesHeart diseaseDepression and AnxietyFragile X carriers more likely to develop
premature ovarian failure
Associated health conditions
5 – 10% of women with premature ovarian will become pregnant spontaneously
IVF with donor egg is only proven effective fertility treatment
Fertility
Patients and their families should be counseled on the effect of the patient’s condition on future fertility, on the risk of co morbidities associated with primary ovarian insufficiency, and on the condition’s potential for genetic inheritance. Psychological counseling also should be offered because impaired self-esteem and emotional distress have been reported after diagnosis of primary ovarian insufficiency.
Once primary ovarian insufficiency is diagnosed, patients should be evaluated at least annually
Referrals to a reproductive endocrinology and infertility specialist should be made when desired by the patient and family to further discuss available reproductive treatment
Counselling and Followup
American Society of Reproductive MedicineThe American Congress of Obstetricians and
Gynecologists MedscapeUptoDate
References
