principles of antimicrobial therapy - pharmacology
TRANSCRIPT


Antimicrobial therapy takes advantage of the biochemical differences between microorganisms and humans
Antimicrobial drugs should have selective toxicity towards the invading microorganism without harming the cells of the host
This selective toxicity is usually relative rather than absolute, requiring careful control of the drug concentration
Selection of an appropriate antimicrobial agent requires knowing:
1. The microorganism
2. The organism’s susceptibility to a particular agent
3. The site of infection
4. Patient factors
5. The safety of the drug
6. The cost of therapy
Some patients require empiric treatment
(Immediate administration of drugs prior to bacterial identification and susceptibility testing)


Bacteriostatic drugs arrest the growth and replication of bacteria, thus limit the spread of infection until the body’s immune system attacks and eliminates the organism◦ If the drug is removed before the immune system has
eliminated the organism, remaining viable organisms can begin a second cycle of infection
Bactericidal drugs kill bacteria, they are often used in seriously ill patients


Some antimicrobials can be bacteriostatic against one organism and bactericidal for another◦ Example: chloramphenicol is bacteriostatic against
gram-negative rods and is bactericidal against other organisms such as S. pneumoniae

Minimum inhibitory concentration (MIC): the lowest concentration of antibiotic that inhibits bacterial growth
Minimum bactericidal concentration (MBC): the minimum concentration of antibiotic that kills the bacteria under investigation


Patient factors taken into consideration when selecting an antimicrobial agent◦ Immune system
◦ Renal dysfunction
◦ Hepatic dysfunction
◦ Poor perfusion
◦ Age
◦ Pregnancy
◦ Lactation
Oral route is chosen for mild infections, and is favorable for outpatients
Parenteral route is used for more serious infections, or when the anti-microbial agent of choice has poor GI absorption such as vancomycin, amphotericin B and aminoglycosides
Pharmacodynamics of the drug (the relationship of drug concentrations to antimicrobial effects
Pharmacokinetics of the drug (ADME)
Concentration dependent killing
Time dependent (concentration-independent killing)
Postantibiotic effect

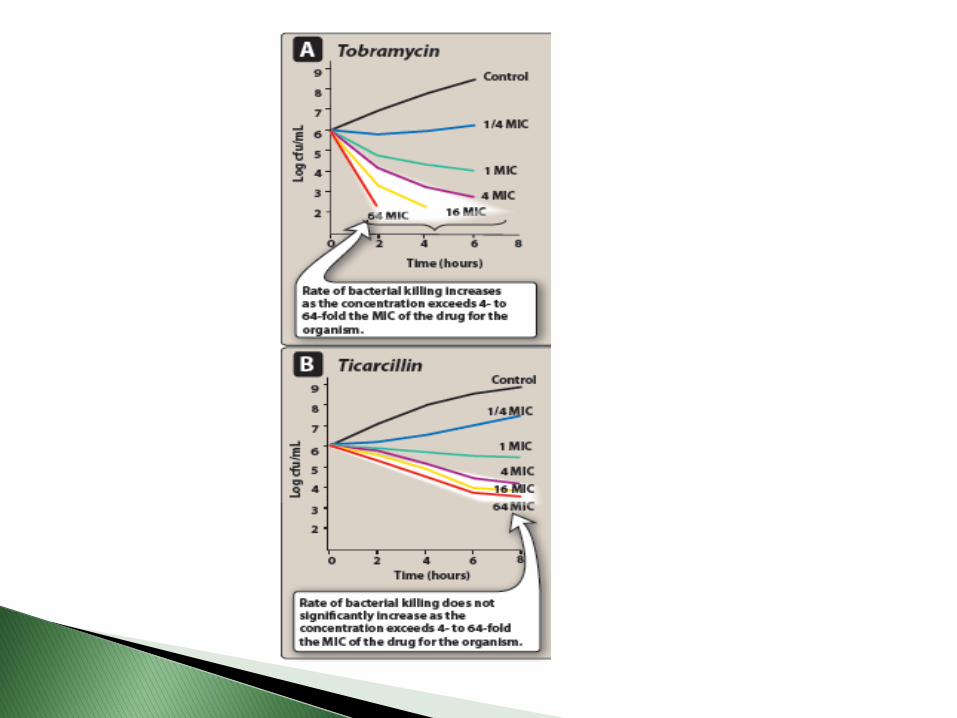
Concentration dependent killing
• Rate of bacterial killing increases as the concentration increases from 4-64 fold MIC
• e.g. aminoglycosides like tobramycin
• Administration by once-a-day bolus infusion achieves high peak levels, causing rapid killing of the pathogen
Time dependent (concentration-independent) killing
• Increasing concentration to higher multiplies of MIC does not increase the rate of killing
• e.g. β-lactams, glycopeptides, macrolides, clindamycin
• Administration by extended (3-4 hours) or continuous (24 hours) infusion achieves prolonged time above MIC and kills more bacteria

Penicillins
Cephalosporins
Tetracyclines
Aminoglycosides
Macrolides
Fluoroquinolones
Other

Narrow-spectrum antibioticsActing on a single or limited groupe.g. isoniazid is only active against mycobacteria Extended-spectrum antibioticsEffective against gram positive organisms ad also
against a significant number of gram negativee.g. ampicillin Broad-spectrum antibioticsDrugs affecting a wide variety of microbial species(Can cause superinfections)e.g. tetracycline and chloramphenicol

It is advisable to treat patients with a single agent that is more specific to the infecting organism to reduce possibility of superinfections, decrease resistance and toxicity
In certain situations combinations of antibiotics are needed for example treatment of tuberculosis requires the use of drug combinations

Bacteria is resistant to an antibiotic if the maximal level of the antibiotic does not stop their growth◦ Some organisms are inherently resistant to antibiotics
Ex. Gram negative bacteria are inherently resistant to vancomycin
◦ Microbial species that are normally responsive to a particular drug may develop more virulent or resistant strains through spontaneous mutation or acquired resistance and selection
◦ Some organisms may become resistant to more than one antibiotic
Antibiotics use for prevention is restricted to situations where the benefit outweighs the risks of bacterial resistance and superinfections such as:◦ Prevention of tuberculosis or meningitis
among individuals who are in close contact with infected patients
◦ Treatment prior to most surgical procedures to decrease the incidence of infection afterwards

Hypersensitivity◦ Penicillins can cause serious hypersensitivity problems
ranging from urticaria (hives) to anaphylactic shock
Direct toxicity◦ Aminoglycosides can cause ototoxicity by interfering with
membrane function in the hair cells of the organ of corti
Superinfections◦ Drug therapy especially broad spectrum antimicrobials
can lead to alterations to the normal flora of the upper respiratory, intestinal and genitourinary tracts permitting overgrowth of opportunistic organisms like fungi or resistant bacteria
◦ These infections are difficult to treat

Chemical structure
(β-Lactams or aminoglycosides)
Mechanism of action
(Cell wall synthesis inhibitors)
Their activity against a particular types of organisms
(Bacteria, fungi, viruses)
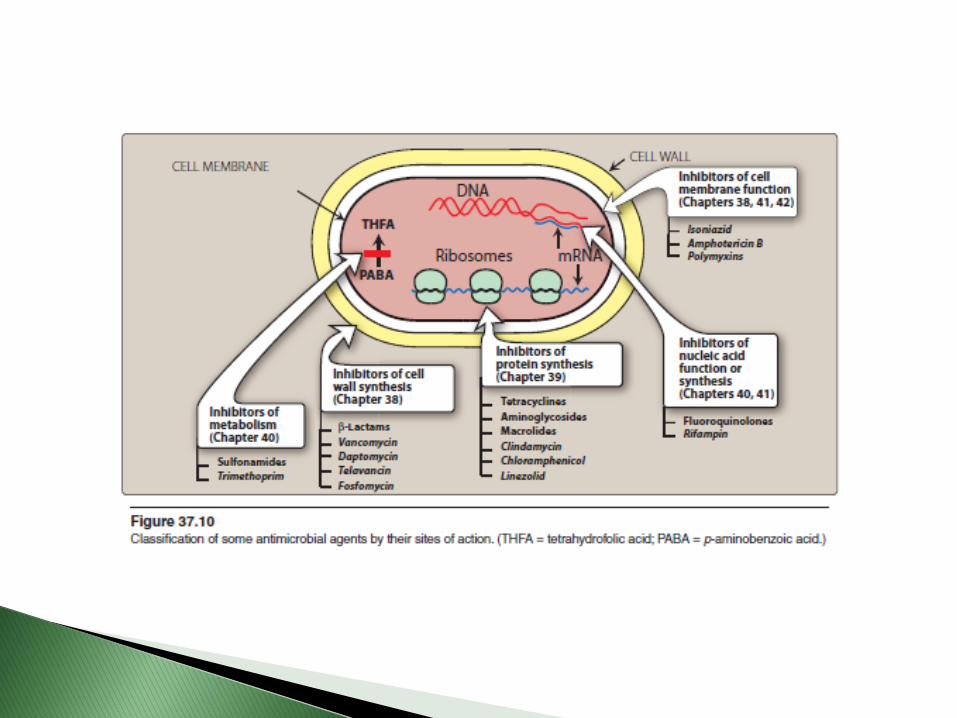


Interfere with bacterial cell wall synthesis(Mammalian cells do not have cell wall)
They are maximally effective in actively proliferating microorganismms
Have little or no effect on bacteria that are not growing and dividing
Include vancomycin and β-lactam antibiotics like penicillins and cephalosporins
Penicillins
Cephalosporins
Carbapenems
Monobactams
Other antibiotics
Amoxicillin (Amoxitid®, Amoxicare®, Moxepharm®, Moxypen®)
Ampicillin (Ampipharm®, Penibrin®)
Dicloxacillin
Oxacillin
Penicillin G
Penicillin V
Piperacillin
Ticarcillin

Widely effective and less toxic than other drugs
Resistance has limited their use
Nature of the side chain attached to aminopenicillanic acid determines:
Antimicrobial spectrum
Stability to stomach acid
Cross-hypersensitivity
Susceptibility to bacterial degradative enzymes
(β-lactamases)

Mechanism of action: ◦ Interfere with the last step of bacterial cell wall synthesis
(transpeptidation or cross linkage)
◦ The less osmotically stable cell membrane is exposed leading to cell lysis either through osmotic pressure or through activation of autolysins
◦ Bactericidal effect
Effective against rapidly growing organisms that synthesize a peptidoglycan cell wall
Inactive against organisms that lack peptidoglycan cell wall like mycobacteria, protozoa, fungi, and viruses

Bind to proteins on bacterial cell membrane, penicillin binding proteins (PBPs), bacterial enzymes involved in the synthesis of the cell wall and maintenance of bacterium morphology
This binding leads to morphological changes or lysis of bacteria
Alteration in some PBPs causes resistance(e.g. Methicillin resistant Saphylococcus aureus)
(MRSA)

Antibacterium spectrum depends on the ability of penicillin to cross the peptidoglycan wall and reach PBPs
Gram positive bacteria have cell walls easily penetrated by penicillins, in absence of resistance they’re susceptible to penicillins
Gram negative bacteria have an outer lipopolysacharidemembrane that represents a barrier for water soluble penicillins, which can cross through porins
Pseudomonas aeruginosa have restrictive porins and that’s why it’s resistant to many antimicrobials

Some organisms are naturally resistant to penicillins like organisms that lack cell wall such as mycoplasma
Acquired resistance to penicillins by plasmid transfer is a significant problem
Bacteria can gain resistance to multiple antibiotics after gaining resistant plasmids

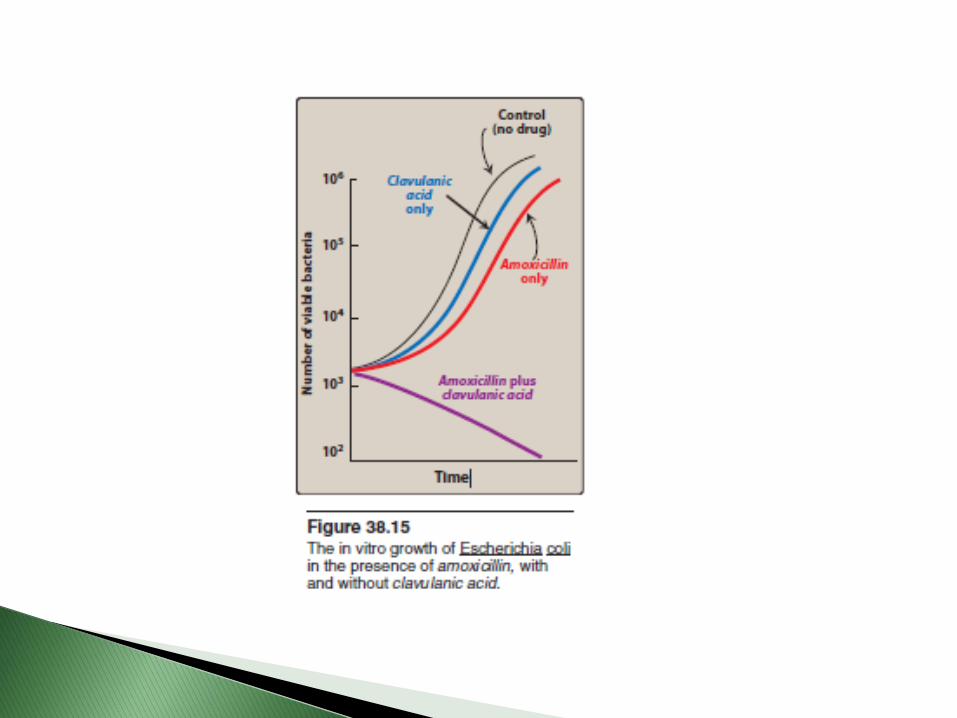
Clavulanic acid
Sulbactam
Tazobactam
Have no significant antibacterial activity by themselves
Bind to and inactivate β-lactamases protecting the coadministered antibiotic

Route of administration◦ Determined by stability to gastric acid
◦ Ticarcillin, piperacillin and the combination of ampicillinwith sulbactam and ticarcillin with clavulanic acid, and piperacillin with tazobactam must be administered IV or IM
◦ Penicillin V, amoxacillin and amoxacillin + clavulanic acid are available only orally
◦ Others are effective orally, IV or IM
◦ Procaine penicillin G and benzathine penicillin G are administered IM as depot forms, they are slowly absorbed into the circulation and persist over a long time period

Most are incompletely absorbed after oral administration except amoxicillin
Absorption of penicillinase resistant penicillins is decreased by food in stomach, taken 30-60 minutes before meals or 2-3 hours postprandial
Hypersensitivity◦ The most common adverse effect of penicillins
Diarrhea◦ Due to disruption of the normal balance of intestinal
microorganisms
Nephritis ◦ All penicillins can cause interstitial nephritis (Especially
methicillin that’s why it is no longer used)
Neurotoxicity◦ Penicillins are irritating to neuronal tissue and can provoke
seizures
Hematologic toxicity◦ Decreased coagulation may happen with high doses of
piperacillin, ticarcillin and nafacillin
Cation toxicity (administered as sodium or potassium salt)◦ Aqueous penicillin G has high K load◦ Ticarcillin has a high sodium load
β-Lactam antibiotics
Closely related to penicillins in structure and function
Have the same mechanisms of action and resistance as penicillins
More resistant to certain β-lactamases than penicillins
Cephalosporins are ineffective against MRSA, L. monocytogenes, Clostridium difficile and enterococci
Antimicrobial spectrum◦ Cephalosporins are classified based on their bacterial
susceptibility and resistance to β-Lactamases to: Firsts generation
Cefazolin Cefadroxil (Biodroxil®) Cephalexin (Keflex®, Jeflex®, Cefacare®)
Second generation Cefuroxime sodium (Zinacef®) Cefuroxime axetil (Zinnat®, Zinaxim®)
Third generation Cefixime Ceftazidime (Fortum®) Ceftriaxone (Rocephin®) Cefotaxime (Claforan®)
Fourth generation Cefepime

Firsts generation cephalosporins◦ Act as penicillin G substitutes
◦ Resistant to staphylococcal penicillinases
◦ Effective against Proteus mirabilis, Klebsiella pneumoniae
Second generation cephalosporins◦ Greater activity against 3 additional gram negative
organisms H. influenzae, Enterobacter aerogenes and some Neisseria species

Third generation cephalosporins◦ Have enhanced activity against gram negative bacilli
including most enteric organisms
◦ Ceftriaxone and cefotaxime are agents of choice for treatment of meningitis
◦ Should be use with caution, because of possible induction and spread of antimicrobial resistance
Forth generation cephalosporins◦ Cefepime
Administered parenterally
Wide antibacterial spectrum against streptococci and staphylococci (MSSA only)
Adverse effects◦ Allergic reactions
Patients who had anaphylactic response, Stevens-Johnson syndrome or toxic epidermal necrolysis to penicillins should not be given cephalosporins


Antibiotics that target bacterial ribosome which differs structurally from mammalian cytoplasmicribosome
Mammalian mitochondiral ribosome closely resembles bacterial ribosome and so high levels of these drugs can cause toxic effects
Tetracyclines
Glycylcyclines
Aminoglycosides
Macrolides/Ketolides
Others
Demeclocycline
Doxycycline (Doxylin® , Doxal®, Doxy®)
Minocycline (Minoclin® , Minocin®)
Tetracycline (Tevacycline® , Brimocycline®)

Mechanism of action: Bind reversibly to the 30S subunit of the bacterial ribosome blocking the binding of aminoacyl t-RNA to mRNA-ribosome complex and inhibiting bacterial protein synthesis
Antibacterial spectrum◦ Broad-spectrum bacteriostatic antibiotics
◦ Effective against gram-positive and gram-negative bacteria and other microorganisms like mycoplasma and chlamydia

Resistance◦ Due to inability of the organism to accumulate the
drug by Mg2+ dependent efflux of the drug
◦ Enzymatic inactivation of the drug
◦ Producing bacterial proteins that prevent tetracyclines from binding to the ribosome
Any organism resistant to one tetracycline is resistant to all

Should not be taken with diary products due to formation of nonabsorbable chelates of the tetracycline with Ca+2
Should not be taken with magnesium and aluminum antacids
Can bind to Ca in bones and teeth

Adverse effects◦ Gastric discomfort: epigastric distress due to irritation of
gastric mucosa, drug can be taken with food to reduce the discomfort (except diary)
◦ Effects on calcified tissues: deposition in bone and primary dentition in growing children causing discoloration and hypoplasia of the teeth and temporary stunting of growth
◦ Fatal hepatotoxicity
◦ Phototoxicity
◦ Vestibular problems: diziness, nausea and vomiting
◦ Superinfections
Contraindicated in pregnant or breast-feeding women or in children less than 8 years of age.
Contraindicated in renally impaired patients except doxycycline (excreted into bile)

Amikacin
Gentamicin
Tobramycin
Streptomycin
Neomycin

Have been used for serious infections
Being replaced due to their toxicities such as the third and forth generation cephalosporins
Diffuse through the porins in the outer membranes and have an oxygen-dependent system that transport the drugs through the cytoplasmic membrane
Mechanism of action: Bind to the 30S subunit and interferes with assembly of functional ribosomal apparatus or cause 30 S subunit misreading of genetic code
Aminoglycosides synergize with β-lactam antibiotics which enhance diffusion of aminoglycosides in to the bacterium due to their action of cell wall inhibition

Aminoglycosides are bactericidal, the exact mechanism is unkown
Effective in combination for the emperictreatment of infections suspected to be due to aerobic gram negative bacilli including P. aeruginosa, usually combined with β-lactamantibiotics or vancomycin
Resistance can be caused by◦ Decreased uptake of the drug◦ Plasmid associated synthesis of enzymes that inactivate
aminoglycosides
Adverse effects ◦ Ototoxicity◦ Nephrotoxicity◦ Neuromuscular paralysis◦ Allergic reactions (dermatitis in topically applied
neomycin)
serum levels should be monitored to avoid toxicity Contraindicated in pregnancy

Erythromycin (Erythro Teva® , Erythrotab® , Erythrolet®)
Azithromycin (Zmax® , Azimex® , Azicare® , Zitrocin®)
Clarithromycin (Klacid® , Klaridex® , Klaricare®)
Telithromycin (Ketolide)

Mechanism of action:◦ Irreversibly bind to the 50S subunit of the bacterial
ribosome inhibiting the translocation steps of protein synthesis
◦ Bacteriostatic, but may be bactericidal at higher doses
Adverse effects◦ Epigastric distress
◦ Cholestatic jaundice
◦ Ototoxicity

(Dalacin C®, Clindacin®)
Same mechanism of action as erythromycin
Effective against gram positive cocci including MRSA
Similar resistance mechanisms as erythromycin
Adverse effects◦ Skin rashes
◦ Potentially fatal pseudomembranous colitis due to overgrowth of C. difficile (vancomycin or metronidazole is used for this condition)

Fluoroquinolones 1st generation◦ Nalidixic acid
Fluoroquinolones 2nd generation◦ Ciprofloxacin (Floxin®, Ciprocare®, Ciprodex®)
◦ Norfloxacin
◦ Ofloxacin (Oflodex®)
Fluoroquinolones 3rd generation◦ Levoflaxin (Tavanic®, Levo®)
Fluoroquinolones 4th generation◦ Moxifloxacin (Megaxin®)

Newer fluorinated quinolones offer◦ Greater potency
◦ Broader spectrum of antimicrobial activity
◦ Greater in vitro efficacy against resistant microorganisms
◦ Sometimes a better safety profile
Compared to ciprofloxacin, newer compounds are more active against gram positive organisms and have favorable activity against gram negative organisms

Fluoroquinolones have wide antimicrobial spectrum, and favorable pharmacokinetic and adverse effects profiles
Their overuse has led to the emergence of resistant microorganisms

Mechanism of action◦ Enter the bacterium by passive diffusion through
porins
◦ Inhibit replication of bacterial DNA by interfering with the actions of DNA gyrase (topoisomerase II) and topoisomerase IV during bacterial growth and reproduction
◦ Binding of the quinolone to both enzymes and DNA forms a complex that inhibits the resealing step and can cause cell death by inducing cleavage of DNA
◦ Topoisomerase IV is required for cell division

DNA gyrase enzyme is a bacteriospecifictarget, cross-resistance with other antimicrobial drugs is rare. But resistance is increasing in multi-drug resistant microorganisms