probiotics from theory to practice in allergy
TRANSCRIPT

1
This presentation aims at getting allergists acquainted with the concept of probiotics and
their use in clinical practice, based on the evidences available to date.

Dr. Pedro Ojeda received honoraria from Allergy Therapeutics to give this
talk.
2

This slide stands out the National Microbiome Initiative promoted and
endorsed by the White House in which $400 Million will be invested in
research on the human microbiome, highlighting the importance that the
microbiome is acquiring in science and therefore scientists and particularly
physicians cannot remain unaware of this emerging field and the world of
probiotics. They should at least be knowledgeable and then decide by
themselves whether they embrace it or not.
3

4
5

As an allergist, for me, the fields of probiotics and immunotherapy share
important periods and concepts.
Dr. Élie Metchnikoff may be regarded as one of the fathers of Probiotics. In
1907 he published “The prolongation of life” in which he stated that the
putrefaction of food in the gut could be the origin of toxins that could shorten
individual’s life. He observed that Bulgarian people lived longer than others
and related this fact to their consumption of sour milk, as a source of
beneficial bacteria. This book may be considered the starting point of
probiotics science.
Not much later, in 1911, Leonard Noon and John Freeman published their
pivotal study “Prophylactic inoculation against hay fever”, in which they
established the basis for current allergen immunotherapy, although the concept
at that time was that hey fever was caused by a toxin and this inoculation
consisted of an “anti-toxin”.
6

The 1960´s were another important period for both fields. In 1965 Dr. Daniel
Lilly and Dr. Rosalie Stillwell coined the term probiotic as a growth-
promoting factors produced by microorganisms to facilitate the proliferation
of specific bacteria in the gut.
In 1967, three independent research groups got to the discovery of the
immunoglobulin E, one of the key elements in allergic reactions.
7

The end of the 20th and beginning of the 21st centuries are important dates as
well. In 1998, in a worldwide referenced position paper, the WHO endorsed
allergen immunotherapy and allergen avoidance as the only treatments that
may have an impact on the natural course of allergic diseases, by contrast with
pharmacological therapies. Three years later, the WHO and FAO set up an
expert panel to discuss for the first time on probiotics and how to better
scientifically assess their effects on human health.
8

9

10

11

12

13

14
Prebiotics are essentially sugars; most of them are inulin-type fructans or inulin oligo or
polymers, galactans or mixtures of fructans and galactans; new prebiotics are being investigated.
Prebiotics are mainly used to feed the bacteria included in a probiotic product.
In some patients with intestinal bacterial overgrowth (SIBO), prebiotics may be badly
tolerated so a prebiotic-free product may be selected to treat them.

It is important to know that prebiotics have biological effects by themselves,
including immune regulation functions.
15

16
Synbiotics are just a mixture of prebiotics and probiotics.

Again the parallelism with allergen immunotherapy: In the same way it is
important the quality of the allergenic extract as well as the kind of adjuvant
used in an allergy vaccine, it is important to kwon the genus and strain of the
probiotics, and the type of prebiotic included in this kind of products.
17
18

The study of Hunt et al published in 1978 in the NEJM clearly showed that
immunotherapy with whole body hymenoptera extract was no better, even
worse, than placebo to treat hymenoptera sting allergy: the rate of reactors
after hymenoptera sting following a course of immunotherapy was very
similar in the group of patients having received whole body extract and
placebo. However, the rate of reactors was 10 times lower in the patients
receiving pure hymenoptera venom extract. Since then, allergy vaccines for
hymenoptera allergy are only produced from pure hymenoptera venom, and
the cure rate in theses patients may be as high as 98% for wasp allergy.
This is a clear example of the importance of conducting properly designed
studies to show the efficacy of a particular treatment in a specific disease.
Therefore, if we want to assess the efficacy and safety of probiotics-containing
products, properly designed trials must be conducted.
19

These are the results of a PubMed search looking for “probiotics” and
“human”, and filtering by any kind of article, clinical trials, or meta-analysis.
Although publications on probiotics started already in the 1960s, it was not
until the 1980s that the scientific production started to blossom. Similarly, the
publication of clinical trials on probiotics in humans began to increase by the
end of the 20th Century, and meta-analyses began to be conducted by the mid-
first decade of the 21st Century.
20

However, probiotics are living organisms and as proposed in this publication,
several factors of the host and the product and production process have to be
taken into account when carrying out clinical trials.
21

In 2002, the FAO and the WHO put together a Working Group to establish the
guidelines for the evaluation of probiotics in foods.
22

The steps included in these guidelines are summarized in this slide.
23

However, in 2008, Hoffman et al published in Clinical Infectious Diseases the
main needs that still have to be met in order to properly establish the efficacy
of probiotics in human health and diseases. One of the key points is the
importance of properly differentiating the characteristics and effects that may
be generalized to a genus or species and which other are specific of a strain.
24

In 2010, Dr. Gregor Reid, who was the chairman of the 2001 WHO/FAO
Expert Panel on probiotics, criticized the policies of both the FDA and the
EFSA about the evaluation of probiotic-containing products, setting up
excessively stringent standards for the authorization of these products, and
proposed, in this publication, a new way of evaluating probiotics.
29

To date, the FDA requires the opening of a New Investigational Drug (NID)
file for every product for use in the diagnosis, cure, mitigation, treatment or
prevention of any disease; in this example, the product Polagen by Allergy
Therapeutics, sold in Spain as a “synbiotic food supplement, based on
probiotics, indicated for the treatment of grass pollen-induced allergic rhinitis”
should undergo an NID process of evaluation in order to obtain the license to
be sold in the US market.
30

The implications of an NID file are shown in this slide.
31

A group of experts put together by the School of Law of the University of
Maryland published a report with recommendations for change in the
assessment process and regulation of probiotics. Among other proposals, the
considered the creation of a new category less regulated than drugs and
medical devices for probiotics.
33

In the EU, the Regulation No. 1924/2006 establishes the rules dictating the
labeling and health claims of functional foods, including probiotics and
probiotic-containing foods. It is clearly established that sound scientific works
must endorsed the health claims of these products.
34
35

The rationale for the use of probiotics in allergic diseases derives from the
basic and experimental studies in animals that have shown a potential to
down-regulate Th2-type (pro-allergenic) immune responses and promote Th1-
type responses and the population of regulatory T lymphocytes, along with
some other immunological and non-immunological, but important effects such
as increased mucosal IgA, anti-inflammatory effects and improvement of the
epithelial barrier that may be paramount for allergen exclusion at the skin and
intestinal barriers.
36

One of the first RCT on the use of probiotics for the prevention of allergic
diseases using L. reuteri vs placebo during the last month in utero and the first
year of life failed to demonstrate an effect on the prevention of allergic
sensitization or any other allergic disease up to 7 years of follow-up.
37

Some other trials and meta-analyses have been performed later on and I focus
on the latest two published, respectively in the Journal of Allergy and Clinical
Immunology (2015) and Allergy (2015). In the first one, it was shown that
probiotics reduced the risk of eczema when introduced prenatally, during
breast-feeding and when given to infants during the first year of live; however,
the certainty of this results was low.
38
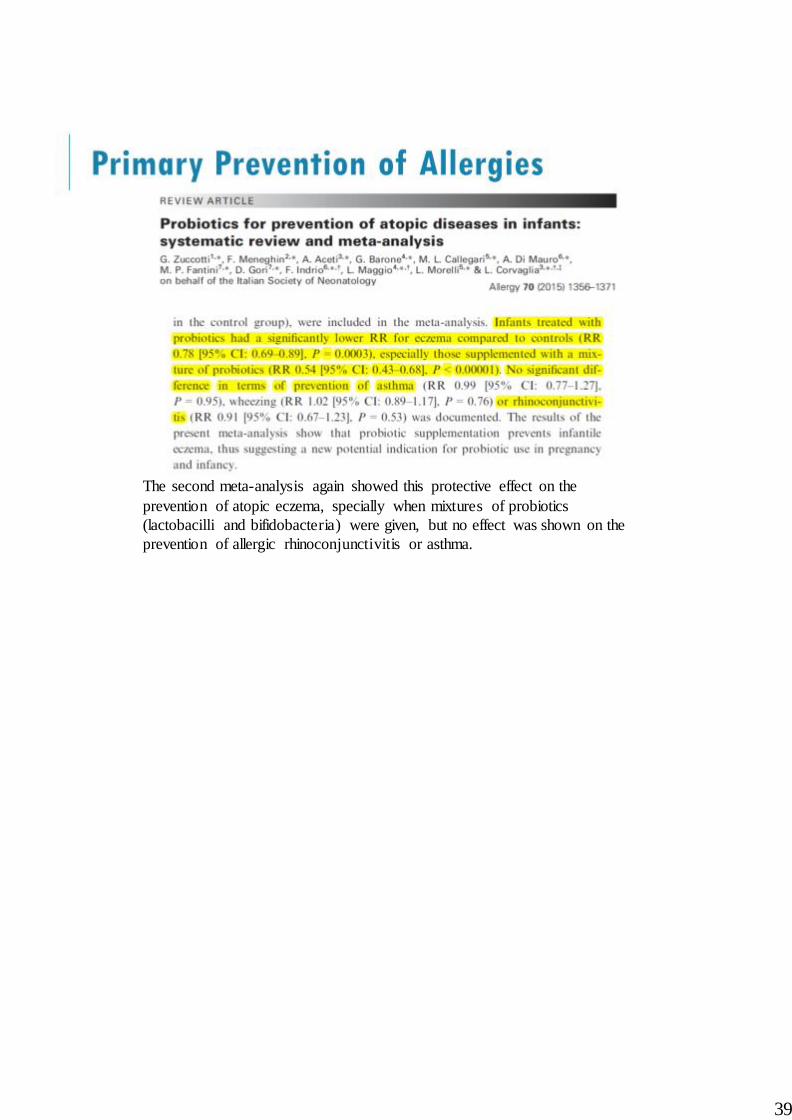
The second meta-analysis again showed this protective effect on the
prevention of atopic eczema, specially when mixtures of probiotics
(lactobacilli and bifidobacteria) were given, but no effect was shown on the
prevention of allergic rhinoconjunctivitis or asthma.
39

However, letters to the editor were written criticizing both meta-analyses: in
the first case, because of pooling data from studies using different species and
strains of probiotics, arguing that studies and meta-analysis should be done
with specific strains for particular health effects; the authors argued it would
be the same as carrying out a meta-analysis to show whether any kind of
antibiotic is useful to treat pneumonia.
In the second case, the authors disagreeing state that the studies included in the
meta-analysis are the same but taken at different periods of their lives and
published in different studies and, again, the argue against the heterogeneity of
the species of probiotics used in the different studies analyzed.
40

This other meta-analysis has shown, however, a protective effect on
sensitization (positive skin prick tests) to inhalant and food allergens when
probiotics are administered prenatally to the mother and postnatally to the
infants.
41

Regarding the treatment (not prevention) of atopic eczema the evidence shows
that the use of probiotics may help improve the course of the disease both in
children and adults with moderate to severe disease. The use of probiotic
mixtures, and particularly Lactobacilli showed the greatest benefit.
42

Two meta-analyses have shown that probiotic used pre-and co-seasonally for
allergic rhinitis helps reducing the symptoms score and improve quality of life
results.
43

Besides, the second one have shown immunological changes favoring the
skewing of the immunological response towards a Th1 response. Moreover, it
seems that Lactobacillus paracasei strain 33 yields the more consistent
benefits.
44

Several meta-analyses have been carried out and none of them has shown a
benefit of probiotics in the prevention or treatment of asthma or wheezing, so
there is no evidence supporting their use for this condition.
45
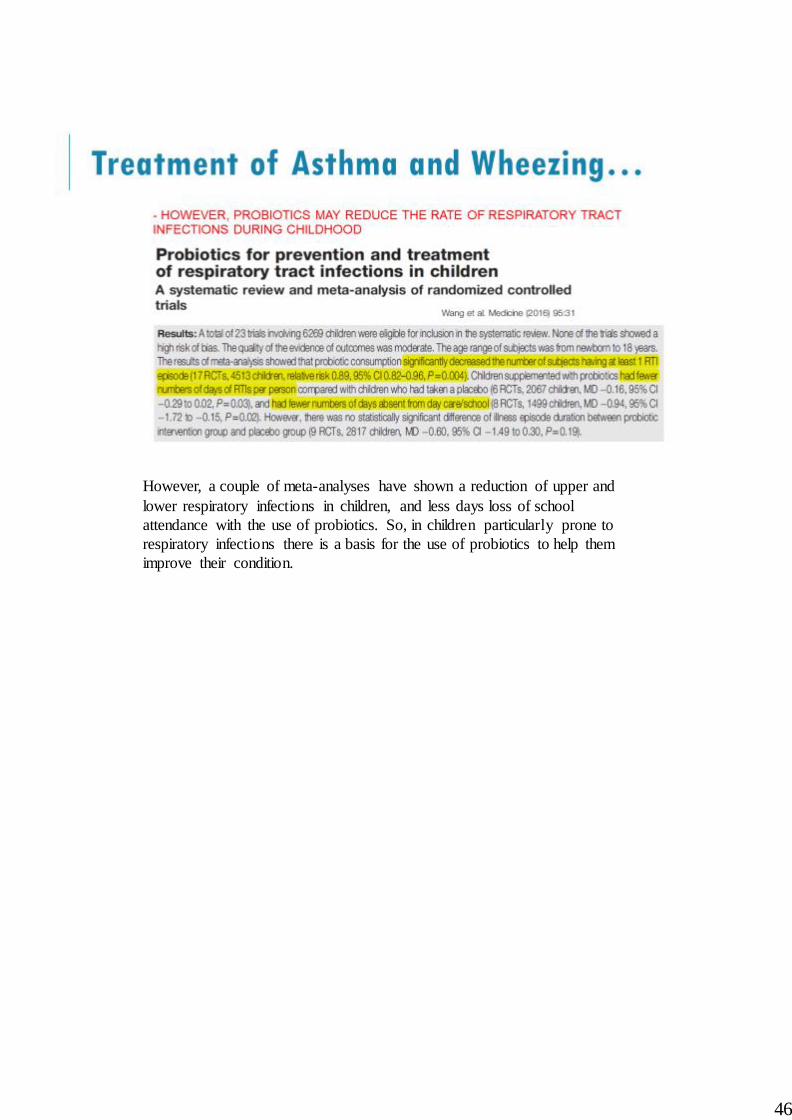
However, a couple of meta-analyses have shown a reduction of upper and
lower respiratory infections in children, and less days loss of school
attendance with the use of probiotics. So, in children particularly prone to
respiratory infections there is a basis for the use of probiotics to help them
improve their condition.
46

The different meta-analyses have failed to show a beneficial effect of the use
of probiotics for the prevention of food allergies and the latest EAACI
guidelines on food allergy and anaphylaxis do not recommend their use for
this purpose; however, as mentioned a few slides before, one meta-analysis
have shown a reduction in the rate of positive SPT with food allergens.
47

Notwithstanding, there is one study showing that the addition of Lactobacillus
rhamnosus (LGG) to an extensive hydrosilate of cow’s milk proteins
considerably and significantly improves the rate of natural acquisition of
cow’s milk tolerance at one year of age in both milk allergic and intolerant
infants.
48

Another study has shown that the combination of probiotics (LGG) to oral
tolerance induction therapy with peanut clearly improves the tolerance to this
food, even when interrupting peanut ingestion for 4-5 weeks after acquisition
of tolerance, as compared to a control group of peanut-allergic children treated
with sham OTI+placebo. In my opinion, the design could have been better if
two groups of peanut-OTI treated patients were compared, one using probiotic
and the other group using placebo.
49

This is a very rapidly changing area of research and this is reflected in the
recommendations of the World Allergy Organization (WAO) since in 2012 in
its position paper this Institution did not recommended the use of probiotics in
allergy clinical practice given the lack of sufficient evidence and three years
later, this same scientific society did recommend the use of probiotics pre and
postnatally, and in breastfeeding mothers for the prevention of atopic eczema
in high risk infants (those with mother and/or father and/or siblings) with
allergic diseases.
50
51

52