problematic marijuana use (addiction): characteristics ...problematic marijuana use (addiction):...
TRANSCRIPT
Problematic Marijuana Use (Addiction): Characteristics,
Prevalence, Treatment Outcomes
Alan J. Budney, Ph.D. Dartmouth College, Geisel School of Medicine
National Debate on Marijuana,
Cancun, Mexico January 26, 2016
My Background
• Treatment Research for Substance Use
(cannabis) problems for over 25 years
• Lab & Survey Studies: Cannabis Withdrawal
• DSM-5 Substance Use Disorders Workgroup
Goals / Conclusions for Today
1. Characterize cannabis use, misuse, or addiction
- substantial abuse potential and consequences
2. Clinical Epidemiology: Prevalence of Problems
- comparable or greater than other substances
3. Treatment Responsivity
- “efficacious” treatments
- but, like other substances: limited efficacy
4. Importance of dealing with cannabis in ways similar to other substances
Can Cannabis Use Lead to Addiction?
Behavioral and Biological Evidence
• Functions as a reinforcer in the human laboratory
• People meet dependence criteria
• People seek help for marijuana problems
• Cannabinoid system in the brain
• Effects of administration and cessation on the brain are similar to that with other drugs of abuse
• Evidence for a Withdrawal syndrome
• It is difficult for those with problems to quit
Defining Addiction (Problem Use)
Is Cannabis / Marijuana Addictive?
DSM and ICD definitions
Cannabis Use Disorder criteria are not
different from other substances
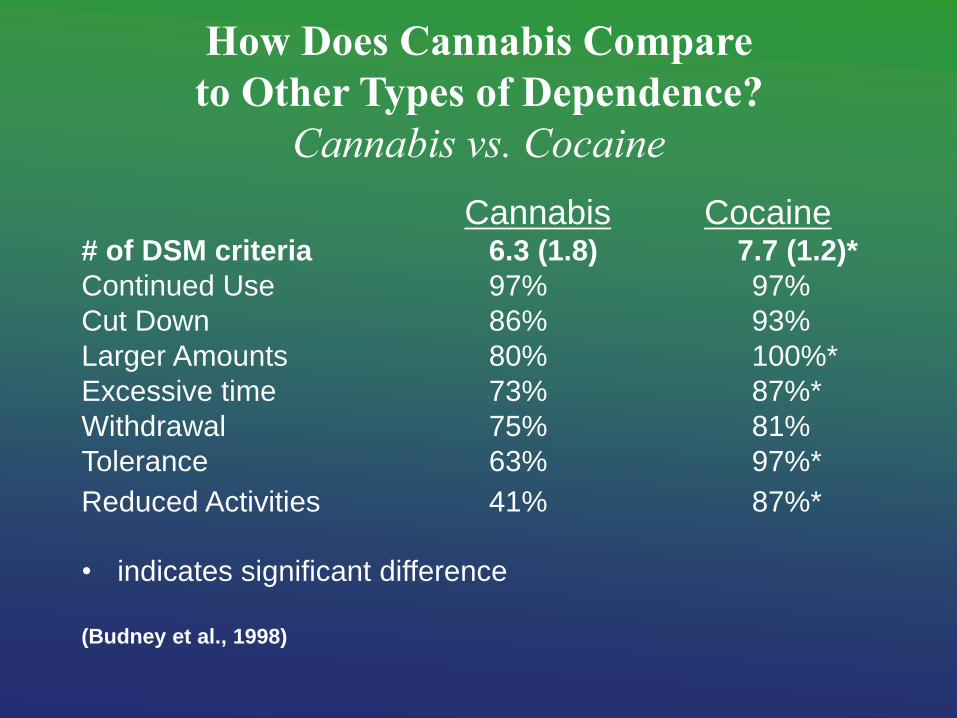
How Does Cannabis Compare
to Other Types of Dependence?
Cannabis vs. Cocaine
Cannabis Cocaine # of DSM criteria 6.3 (1.8) 7.7 (1.2)*
Continued Use 97% 97%
Cut Down 86% 93%
Larger Amounts 80% 100%*
Excessive time 73% 87%*
Withdrawal 75% 81%
Tolerance 63% 97%*
Reduced Activities 41% 87%*
• indicates significant difference
(Budney et al., 1998)
How Does Cannabis Dependence Compare to Other Types of Dependence?
Treatment seekers meet 4.7 - 5.9 of the 7 DSM-IV
criteria…reflects a lower severity syndrome
The “structure” of cannabis dependence is more similar than different than others
- unidimensional, factor structure
- full range of criterion items are endorsed
- generally less severe Budney (2006)
Cannabis Use Disorder Similar to other SUDs Shmulewitz et al. 2015; Hasin et al. 2013
Review: Multiple International Studies (n > 30), large population-based studies
Cannabis Use Disorder highly similar to other SUDS
- unidimensional construct
- full range of criterion are endorsed
- most prevalent behind alcohol and tobacco
Cannabis Withdrawal
Cannabis Withdrawal demonstrated in:
– Non-human studies (primate, rodent, dog)
– Clinical survey studies
– Human inpatient/outpatient laboratory studies
Budney et al. 2004
True Withdrawal Syndrome (Hughes 1990)
• Reliable abstinence symptoms
• Not Rare
• Onset, with Transient Timecourse
• Pharmacological Specificity
• Clinical Importance
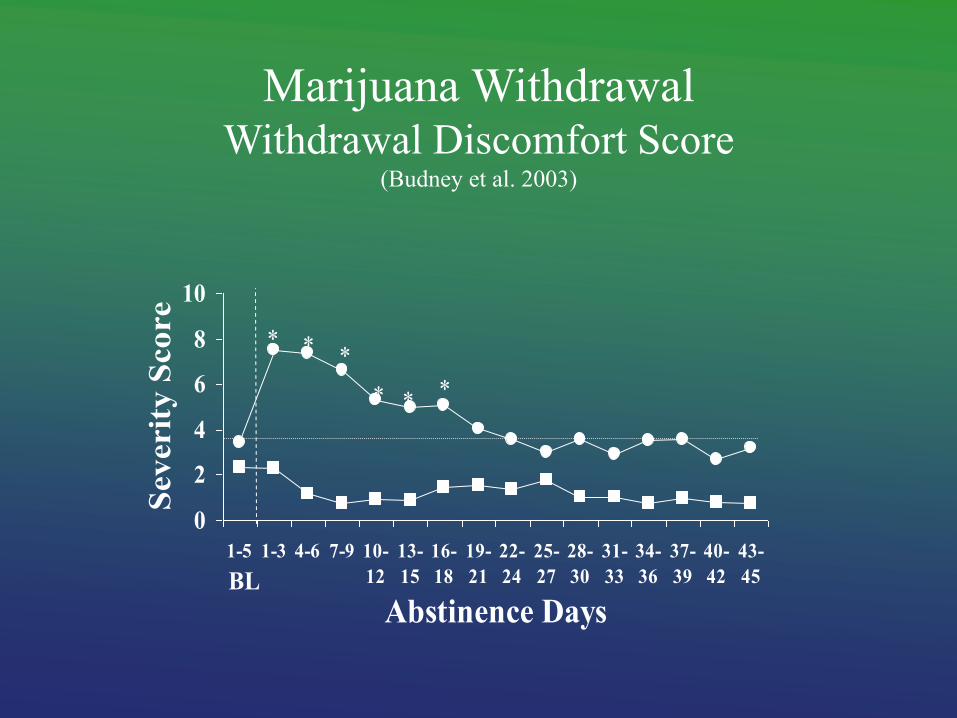
Marijuana Withdrawal Withdrawal Discomfort Score
(Budney et al. 2003)
0
2
4
6
8
10
1-5 1-3 4-6 7-9 10-
12
13-
15
16-
18
19-
21
22-
24
25-
27
28-
30
31-
33
34-
36
37-
39
40-
42
43-
45
Abstinence Days
Severit
y S
core
*
*
* *
*
BL
*
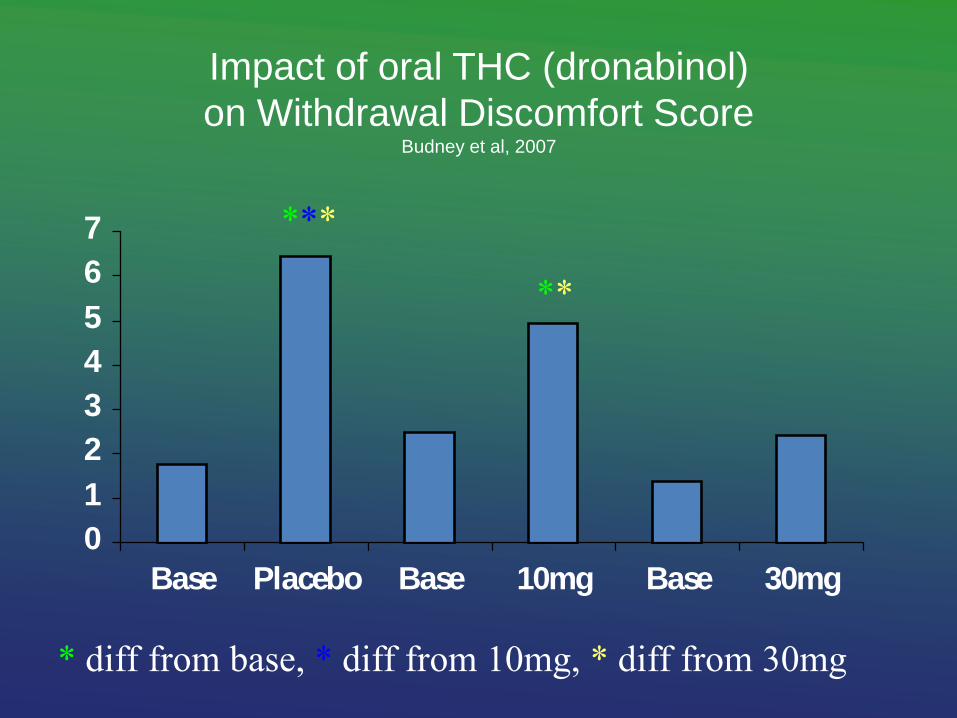
Impact of oral THC (dronabinol)
on Withdrawal Discomfort Score Budney et al, 2007
0
1
2
3
4
5
6
7
Base Placebo Base 10mg Base 30mg
***
**
* diff from base, * diff from 10mg, * diff from 30mg
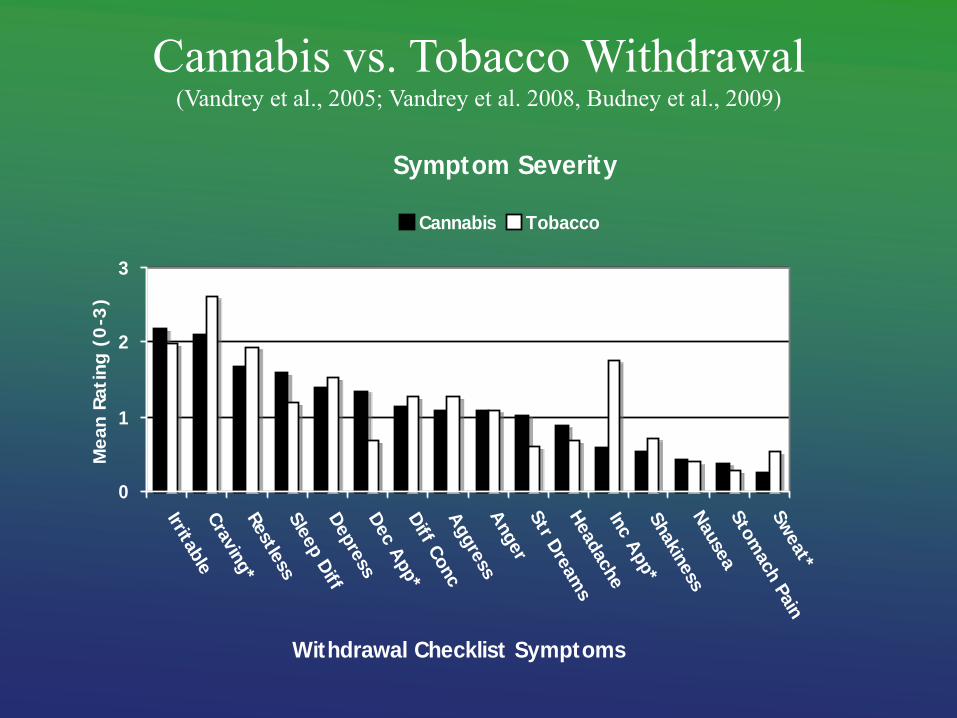
Cannabis vs. Tobacco Withdrawal (Vandrey et al., 2005; Vandrey et al. 2008, Budney et al., 2009)
Symptom Severity
0
1
2
3
Irritable
Cra
vin
g*
Restle
ssSle
ep D
iffD
epre
ssD
ec A
pp*
Diff C
onc
Aggre
ssA
nger
Str D
ream
sH
eadache
Inc A
pp*
Shakin
ess
Nause
aSto
mach P
ain
Sw
eat*
Withdrawal Checklist Symptoms
Me
an
Rati
ng
(0
-3)
Cannabis Tobacco
Clinical Importance of Cannabis WD
Similar in magnitude and severity to Tobacco Withdrawal
- similar attributions about impact on quitting & relapse
Cannabis users report using cannabis (or other substances) to relieve WD symptoms
Patients complain of WD; indicate it makes quitting difficult
# of WD symptoms predicts dependence severity 1-yr later and WD severity predicts rapid relapse (adolescents)
Cannabis Use Disorder is real, and when it occurs, it looks
much the same as other types of SUDs
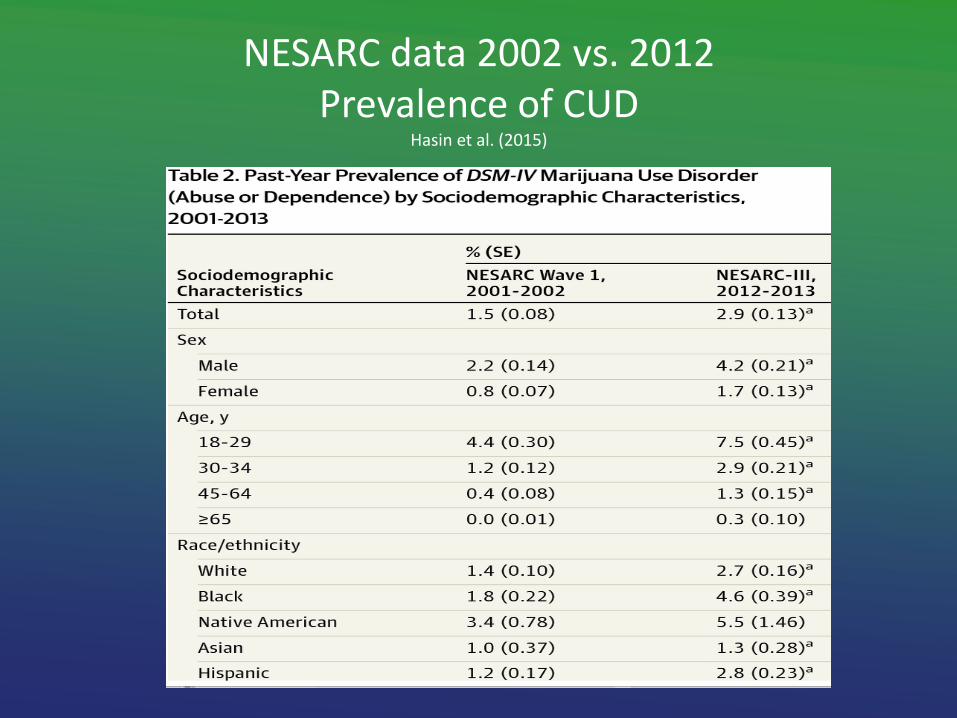
NESARC data 2002 vs. 2012 Prevalence of CUD
Hasin et al. (2015)
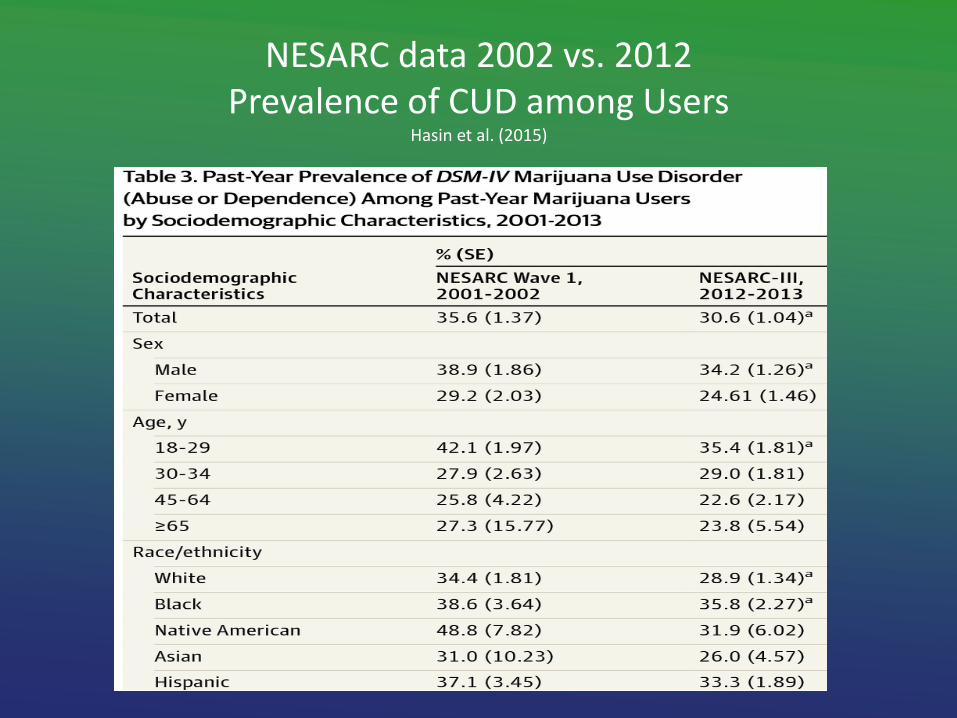
NESARC data 2002 vs. 2012 Prevalence of CUD among Users
Hasin et al. (2015)
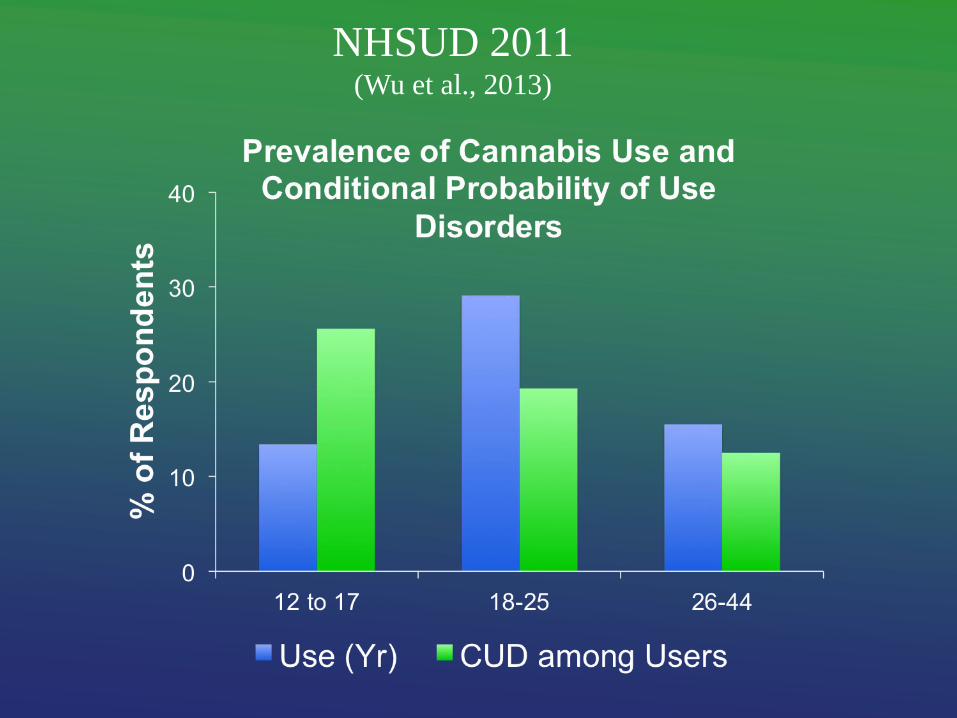
NHSUD 2011 (Wu et al., 2013)
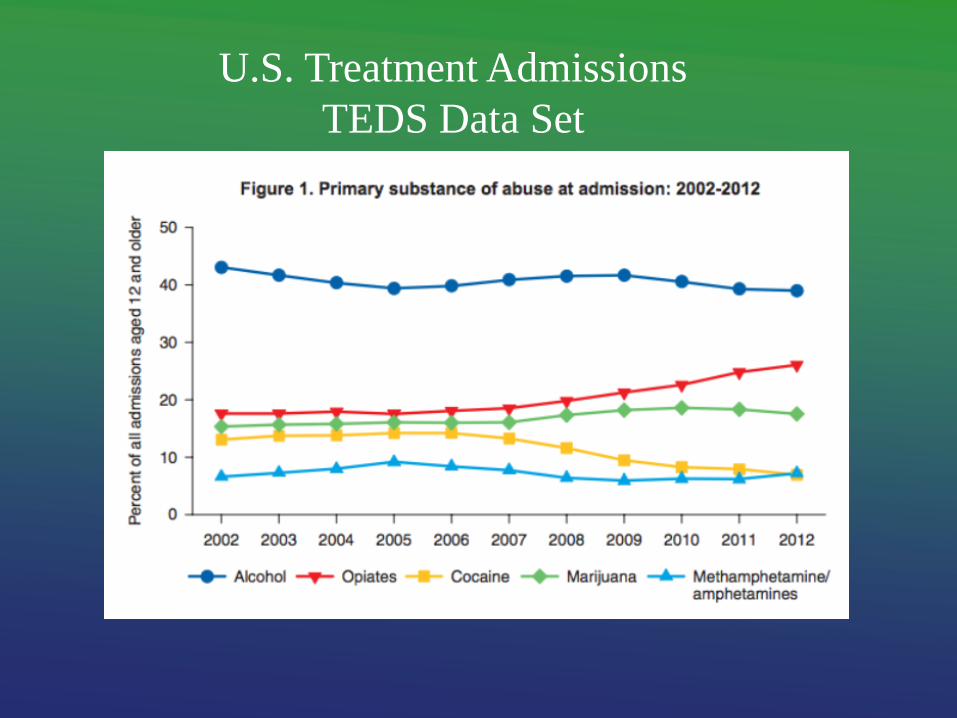
U.S. Treatment Admissions
TEDS Data Set
Cannabis Use Disorder is “common” and it makes up a
substantial proportion of treatment admissions!

How Effective is Treatment?
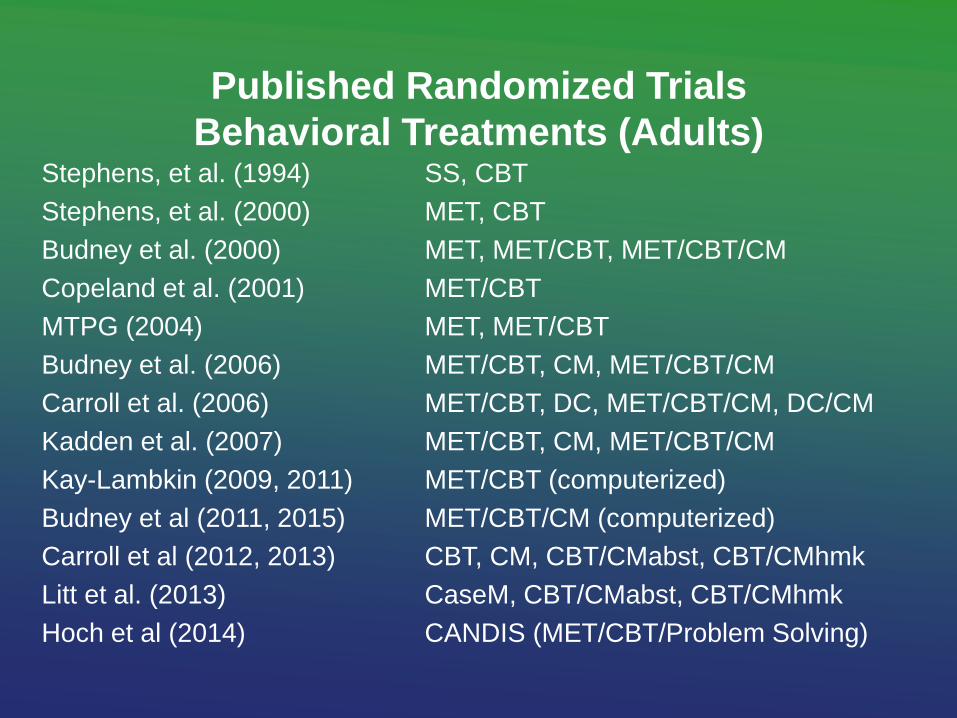
Published Randomized Trials
Behavioral Treatments (Adults) Stephens, et al. (1994) SS, CBT
Stephens, et al. (2000) MET, CBT
Budney et al. (2000) MET, MET/CBT, MET/CBT/CM
Copeland et al. (2001) MET/CBT
MTPG (2004) MET, MET/CBT
Budney et al. (2006) MET/CBT, CM, MET/CBT/CM
Carroll et al. (2006) MET/CBT, DC, MET/CBT/CM, DC/CM
Kadden et al. (2007) MET/CBT, CM, MET/CBT/CM
Kay-Lambkin (2009, 2011) MET/CBT (computerized)
Budney et al (2011, 2015) MET/CBT/CM (computerized)
Carroll et al (2012, 2013) CBT, CM, CBT/CMabst, CBT/CMhmk
Litt et al. (2013) CaseM, CBT/CMabst, CBT/CMhmk
Hoch et al (2014) CANDIS (MET/CBT/Problem Solving)
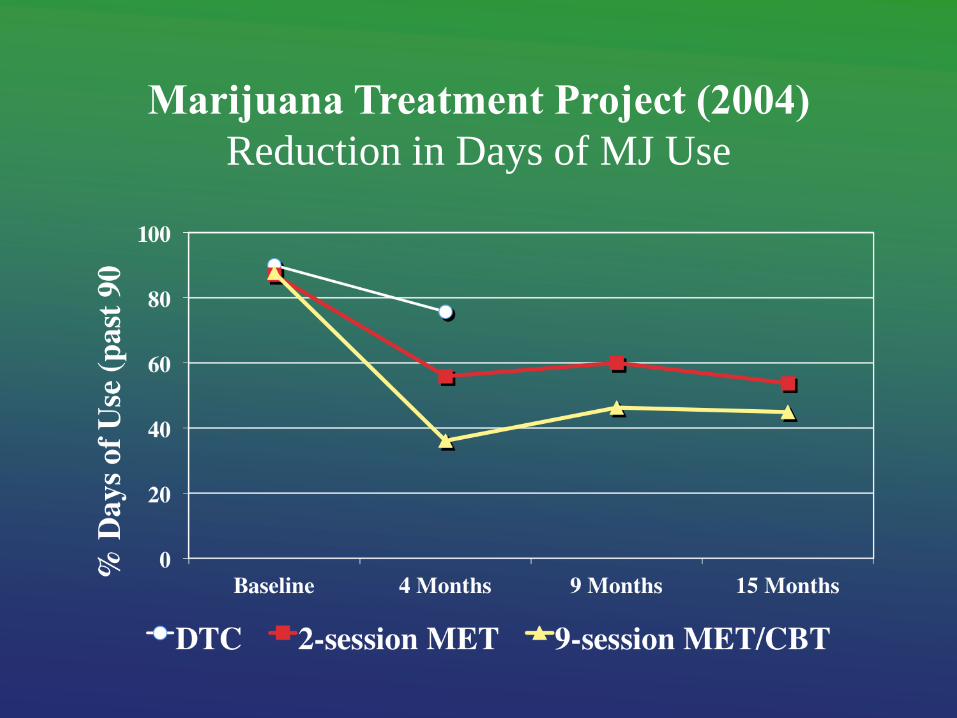
Marijuana Treatment Project (2004)
Reduction in Days of MJ Use
0
10
20
30
40
50
60
70
80
4 Months 9 Months 15 Months
% P
art
icip
an
ts A
bst
inen
t
DTC MET MET/CBT
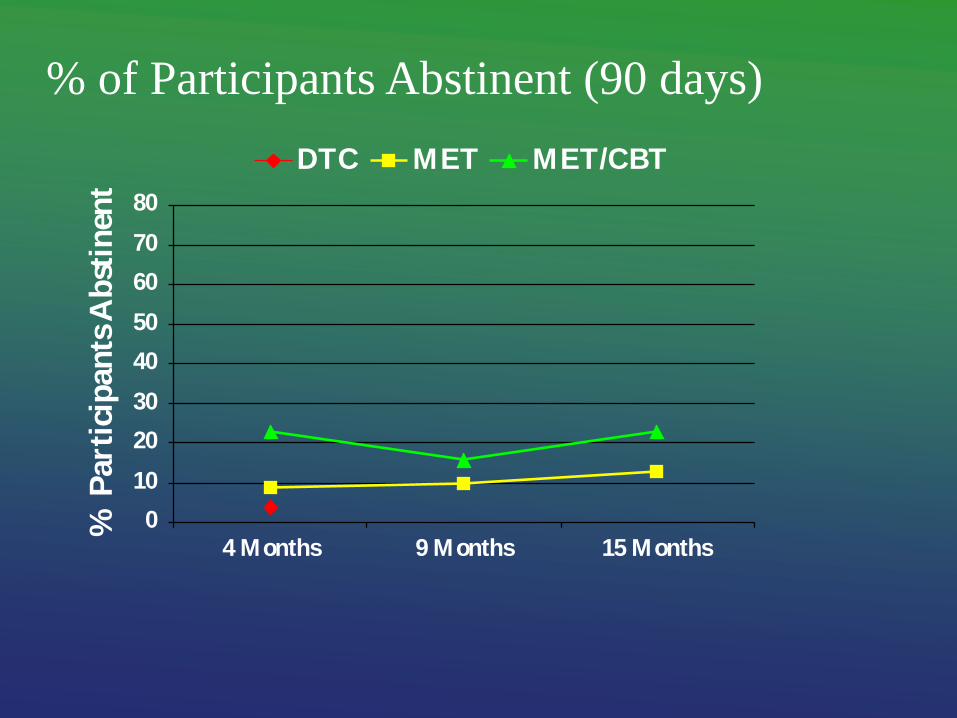
% of Participants Abstinent (90 days)
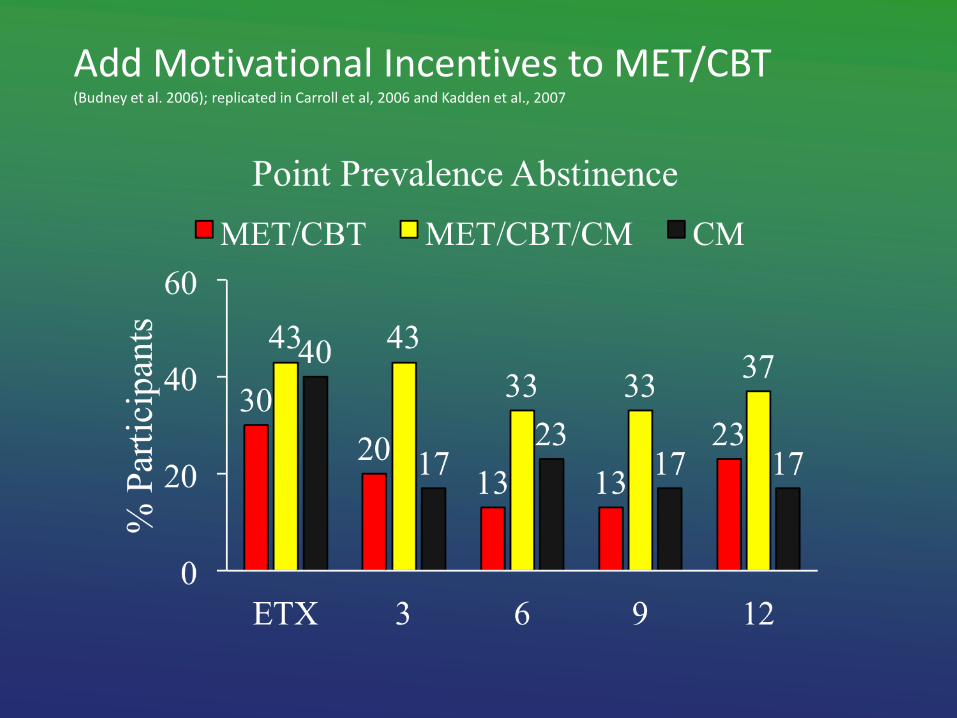
Add Motivational Incentives to MET/CBT (Budney et al. 2006); replicated in Carroll et al, 2006 and Kadden et al., 2007
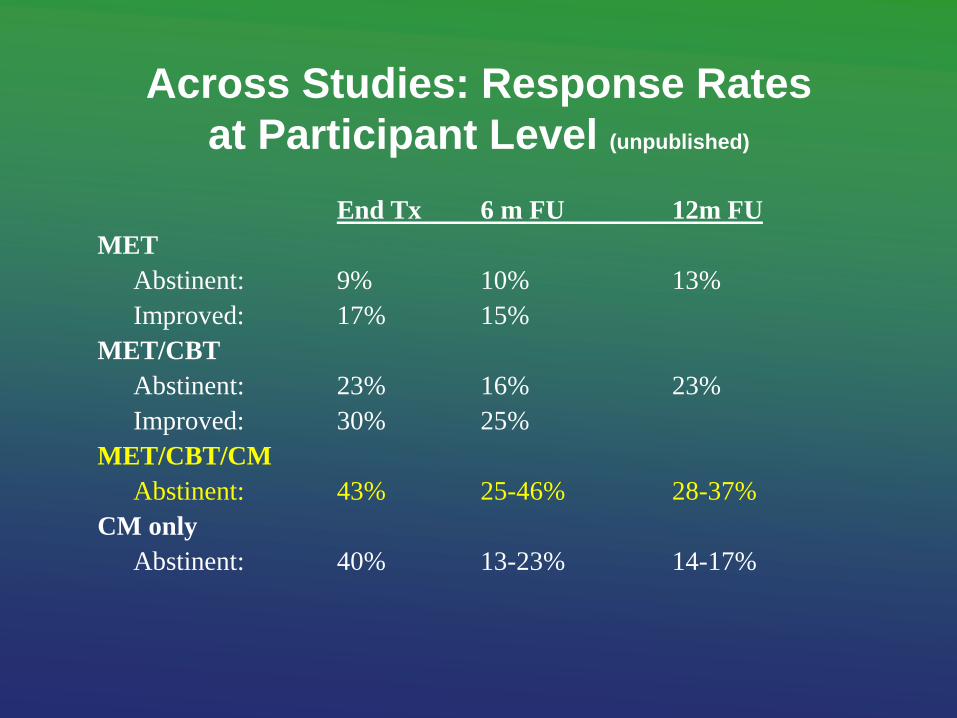
Across Studies: Response Rates
at Participant Level (unpublished)
End Tx 6 m FU 12m FU
MET
Abstinent: 9% 10% 13%
Improved: 17% 15%
MET/CBT
Abstinent: 23% 16% 23%
Improved: 30% 25%
MET/CBT/CM
Abstinent: 43% 25-46% 28-37%
CM only
Abstinent: 40% 13-23% 14-17%
Summary of Adult Trials for CUD
- MET, CBT, CM, MET/CBT are efficacious
- Abstinence incentives (CM) enhance outcomes
- Many people do not respond to these treatments
** Still much room for Improvement
Adolescent Treatment Literature
Multiple types of family-based and group / individual
behavioral efficacious interventions (Waldron 2008: review)
Waldron et al. FFT, CBT, combo
Liddle et al. MDFT
Henggeler et al. MST
Dennis et al./Godley et al. MET/CBT, ACRA, FSN
Kaminer et al. MET/CBT
Szapocznik et al. BSFT
Stanger, Budney et al. CM
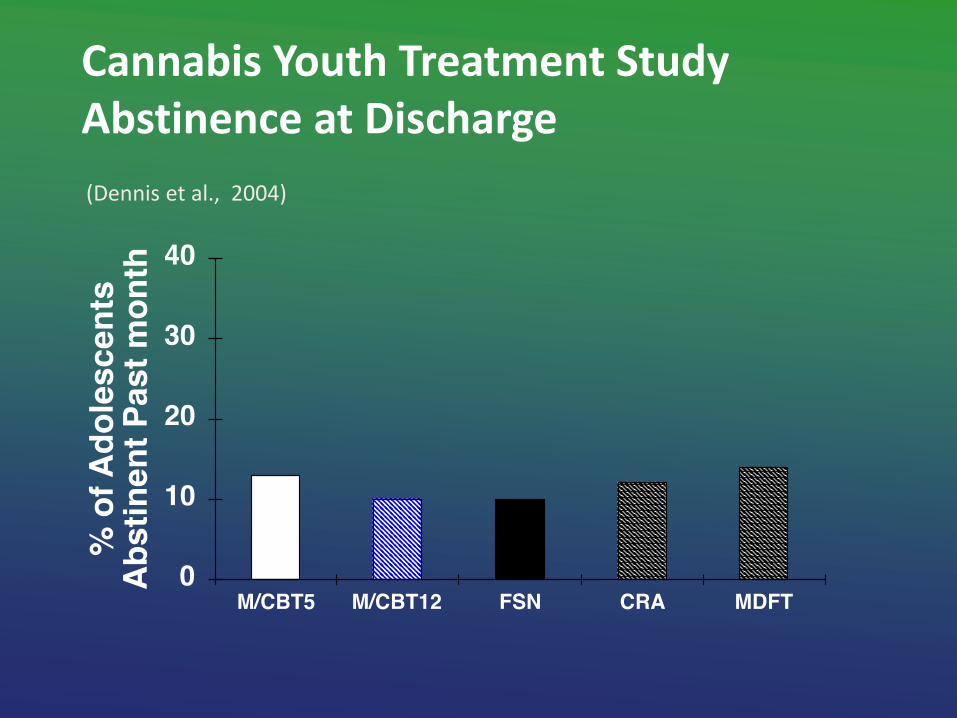
Cannabis Youth Treatment Study Abstinence at Discharge
(Dennis et al., 2004)
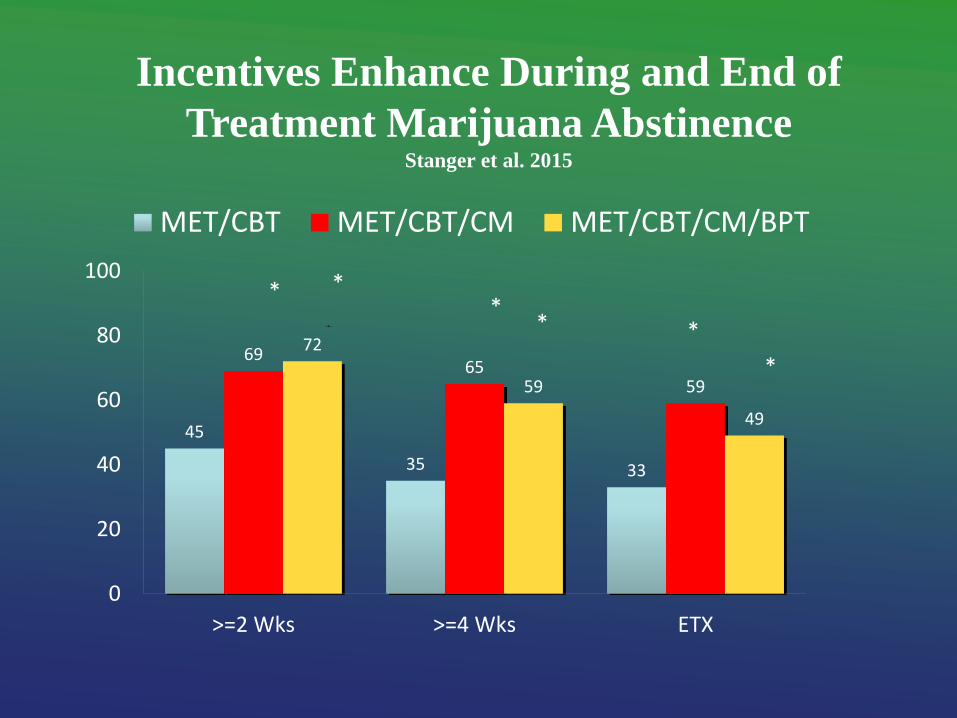
Incentives Enhance During and End of
Treatment Marijuana Abstinence Stanger et al. 2015
45
35 33
69 65
59
72
59
49
0
20
40
60
80
100
>=2 Wks >=4 Wks ETX
MET/CBT MET/CBT/CM MET/CBT/CM/BPT
*
* * *
* *
*
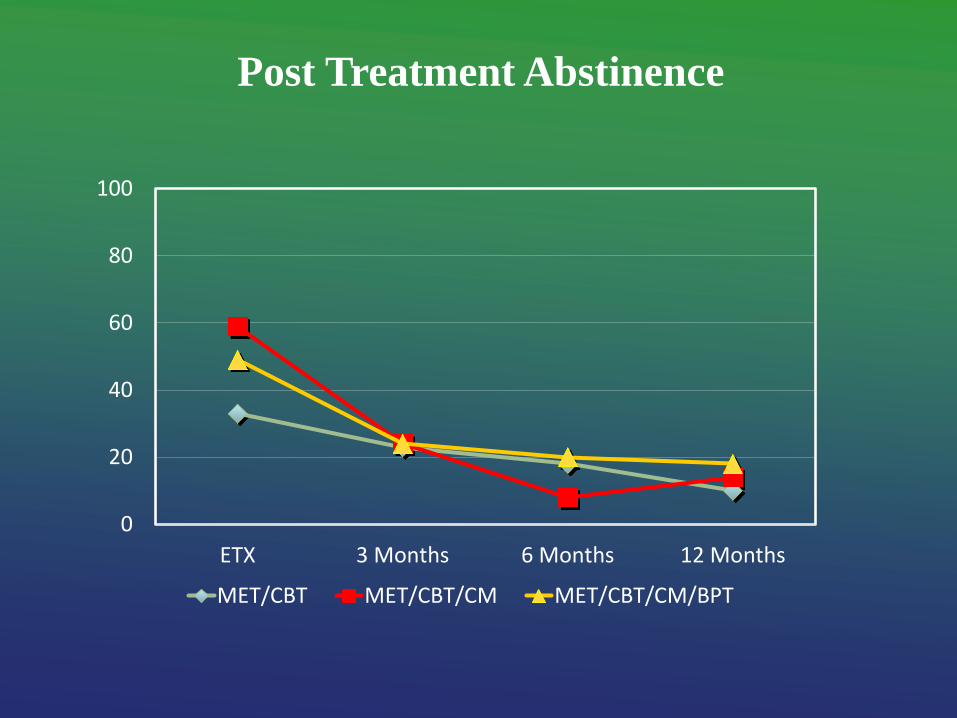
Post Treatment Abstinence
0
20
40
60
80
100
ETX 3 Months 6 Months 12 Months
MET/CBT MET/CBT/CM MET/CBT/CM/BPT
Summary of Teen Trials for CUD/SUD
- Multiple interventions are “efficacious”
- Abstinence incentive (CM) enhance outcomes
- % of teens improved appears lower than that observed
with adults
- Success rates in disadvantaged populations are low
** Still much, much room for Improvement

How Do We Improve?
Behavioral and Neuro-science Provide Targets
- Enhance Delivery Systems / Improve Access
- Endogenous Cannabinoid System; Withdrawal Syndrome
- Genetics
- Impulsivity/Delay Discounting
- Brain Function
- Innovative Incentive Programs
- Concurrent Tobacco Use
- Target Non-responders
- Innovative Use of Technology
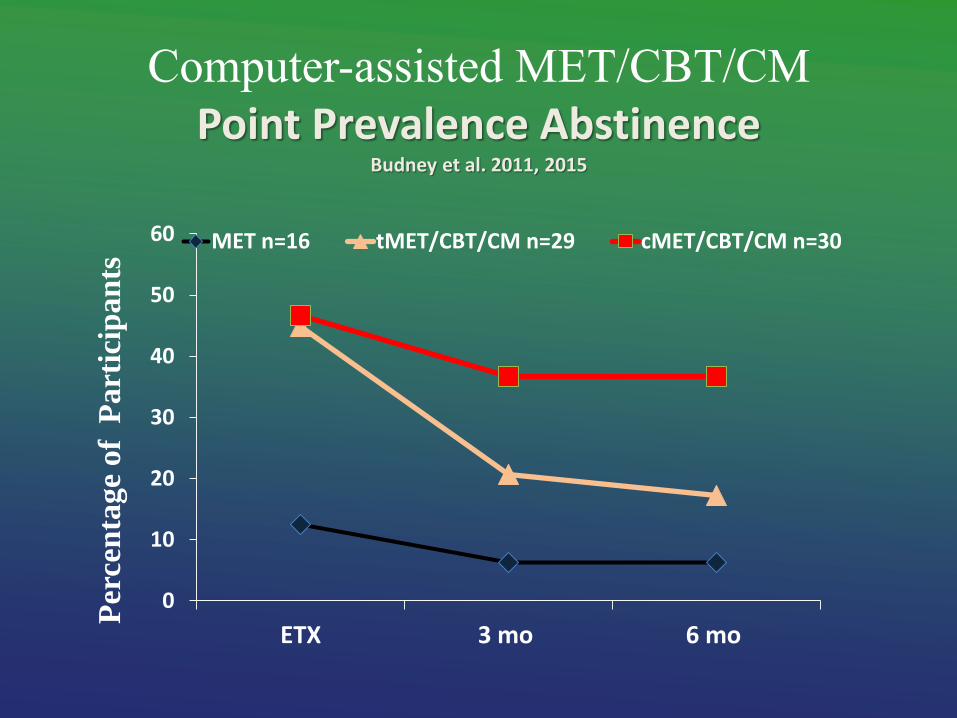
Computer-assisted MET/CBT/CM Point Prevalence Abstinence
Budney et al. 2011, 2015
0
10
20
30
40
50
60
ETX 3 mo 6 mo
MET n=16 tMET/CBT/CM n=29 cMET/CBT/CM n=30
P
erce
nta
ge
of
Part
icip
an
ts
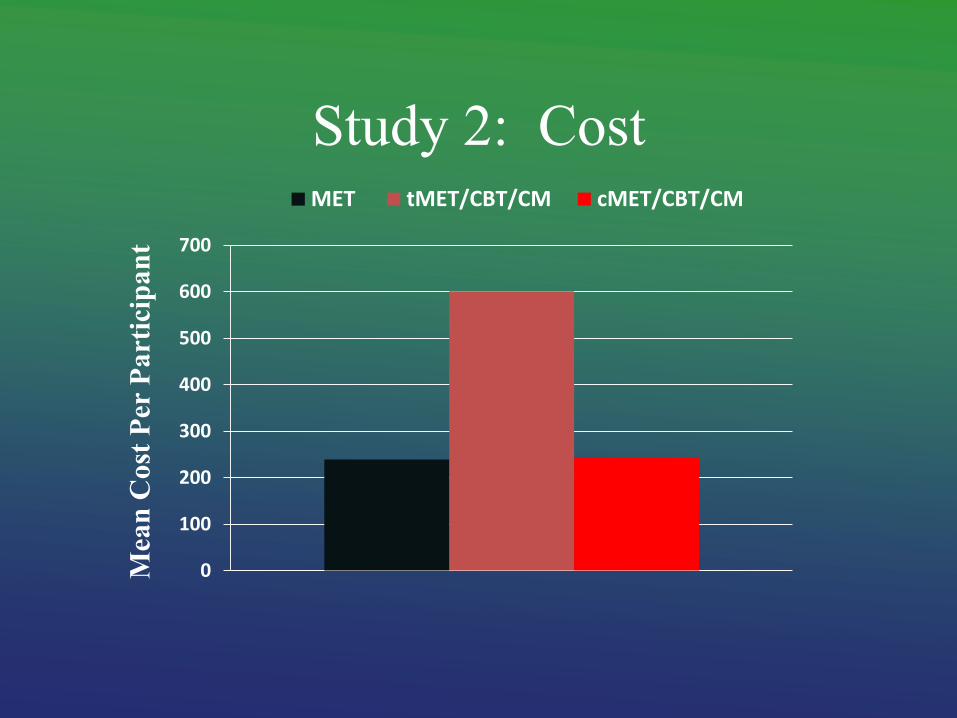
Study 2: Cost
0
100
200
300
400
500
600
700
Mea
n C
ost
Per
Pa
rtic
ipa
nt
MET tMET/CBT/CM cMET/CBT/CM
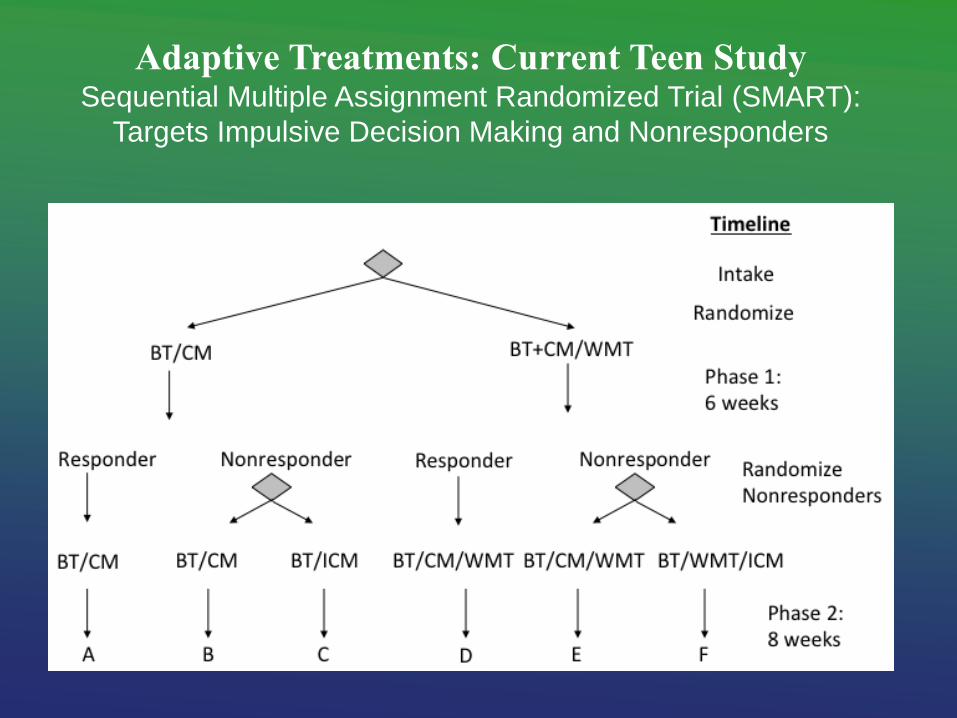
Adaptive Treatments: Current Teen Study Sequential Multiple Assignment Randomized Trial (SMART):
Targets Impulsive Decision Making and Nonresponders

Cannabis Use Disorders are not easily treated. Like for other SUDs, we have efficacious
treatments, but many adults and teens do not respond.
We need to find more effective treatments
and treatment strategies!
CONCLUSIONS
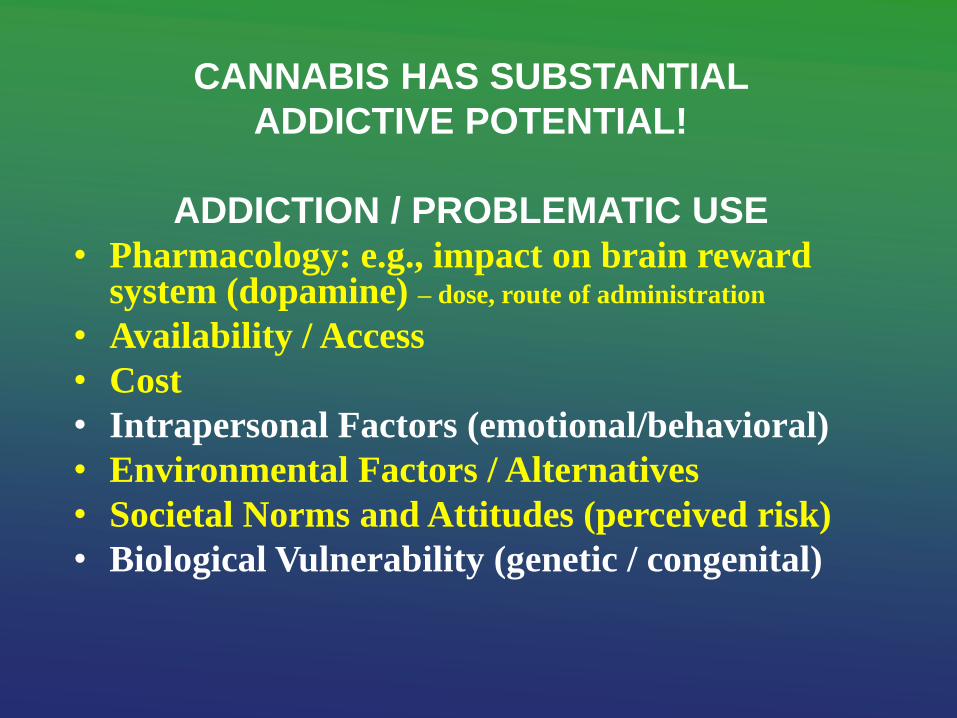
CANNABIS HAS SUBSTANTIAL
ADDICTIVE POTENTIAL!
ADDICTION / PROBLEMATIC USE
• Pharmacology: e.g., impact on brain reward system (dopamine) – dose, route of administration
• Availability / Access
• Cost
• Intrapersonal Factors (emotional/behavioral)
• Environmental Factors / Alternatives
• Societal Norms and Attitudes (perceived risk)
• Biological Vulnerability (genetic / congenital)
Cannabis is more similar than dissimilar to other substances that are considered “substances of abuse”
Like other substances, cannabis is used primarily for its positive (and negative) reinforcing effects
• a subset of those who use cannabis will develop problems
• problems will range from mild to severe

Funding and Support
National Institute on Drug Abuse: – multiple research and training awards
University of Vermont
University of Arkansas for Medical Sciences
Dartmouth College, Geisel School of
Medicine

THANKS!!!! Faculty/Trainees Staff / Therapists Cathy Stanger Patty Costello
Stephanie Fearer Eliza Wessinger
Brent Moore Gray Norton
Ryan Vandrey Leanna Delhey
John Hughes Lee Whetstone
Steve Higgins Doris Ogden
Warren Bickel Jonathan Young
Denise Walker Heath Rocha
Roger Roffman Andrea Meier
Bob Stephens Merrie Vannucci
Pam Brown, Jen VanScoyoc Marlo Lowe
Stacy Ryan Bobby Ward
Amanda Elton / Clint Kilts Sarah Clark
Jody Kamon Nancy Culbertson
Dustin Lee, Jacob Borodovsky Stanley See, Hao Yang
Ben Crosier Nick Tacke, Samantha Auty
James Sargent Jennifer Darsie
Additional Slides
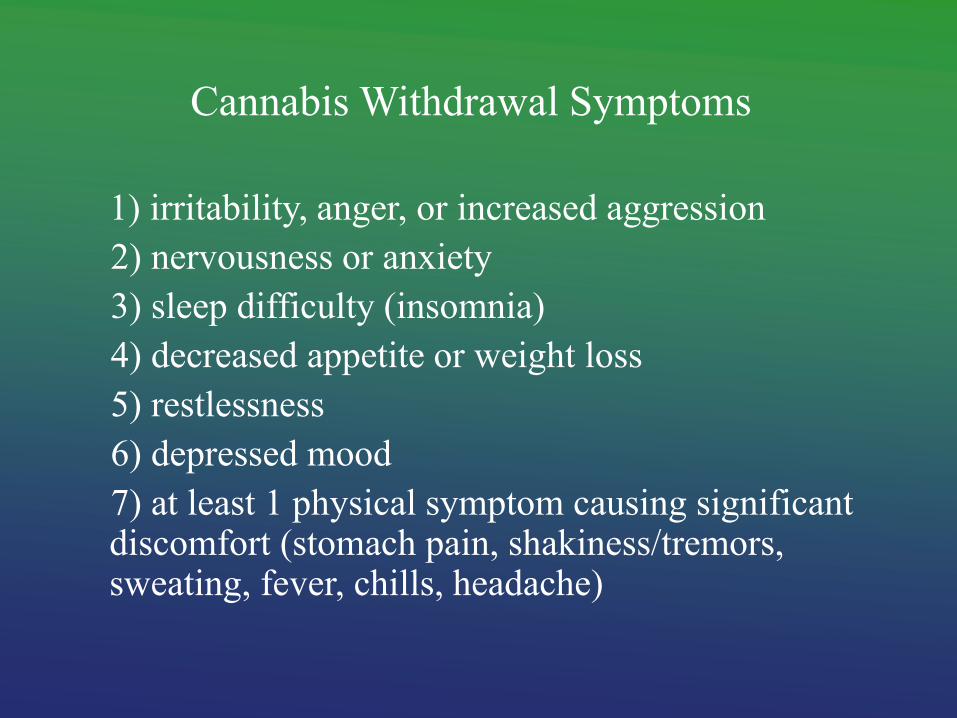
Cannabis Withdrawal Symptoms
1) irritability, anger, or increased aggression
2) nervousness or anxiety
3) sleep difficulty (insomnia)
4) decreased appetite or weight loss
5) restlessness
6) depressed mood
7) at least 1 physical symptom causing significant discomfort (stomach pain, shakiness/tremors, sweating, fever, chills, headache)
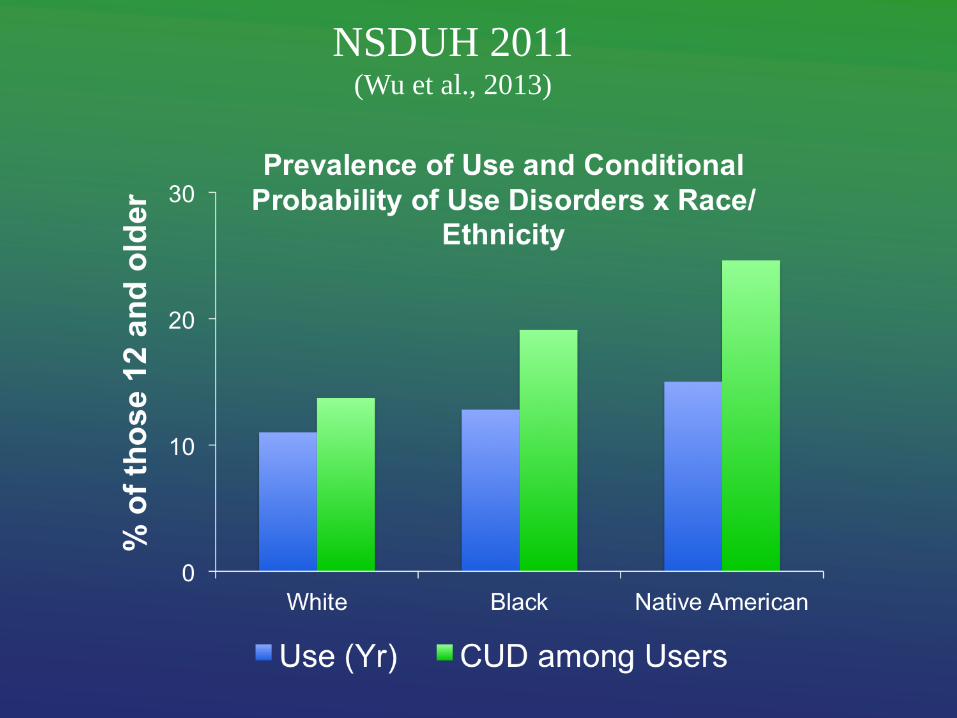
NSDUH 2011 (Wu et al., 2013)
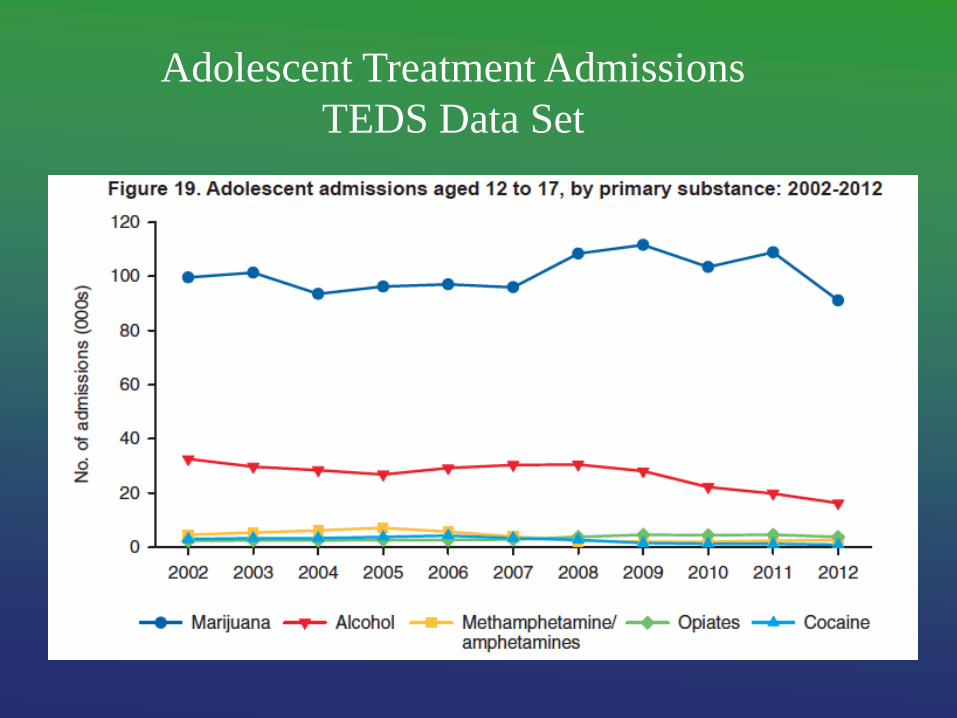
Adolescent Treatment Admissions
TEDS Data Set
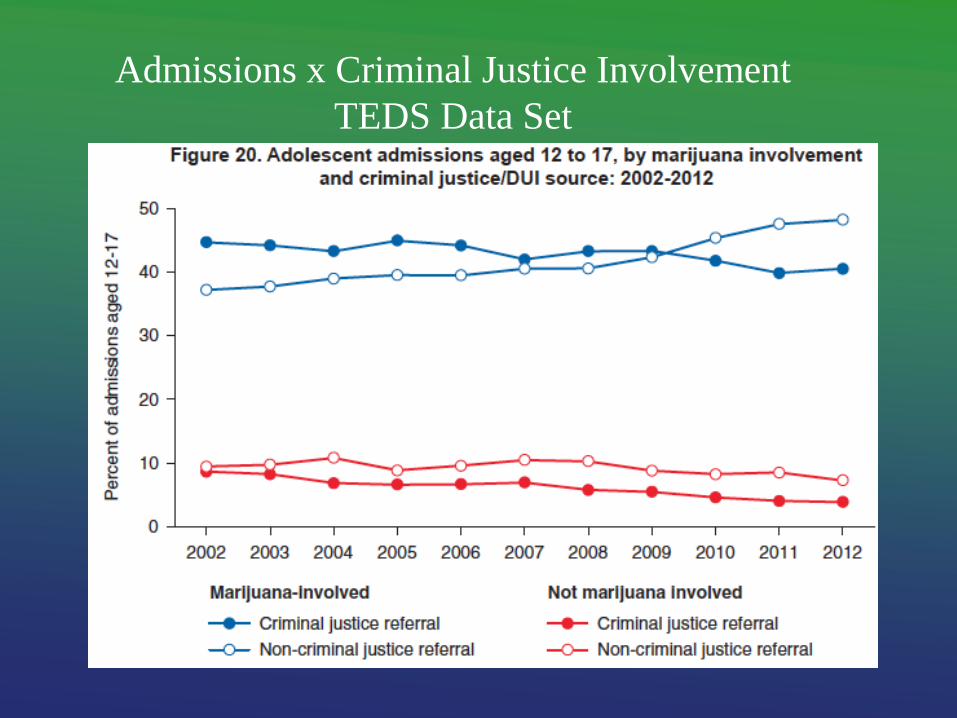
Admissions x Criminal Justice Involvement
TEDS Data Set