problems of abdominal aortic aneurysm associated with ... · tioli a. aneurisma dell'aorta...
TRANSCRIPT
Eur J Vasc Endovasc Surg 14, 75-78 (1997)
C A S E R E P O R T
Problems of Abdominal Aortic Aneurysm Associated with Horseshoe Kidney
D. Y. Artioukh 1, P. N. Wake 1, P. R. Edwards 2 and A. P. Moody 1
1Department of Surgery, Warrington Hospital, Warrington, Cheshire, WA5 IQG and 2Department of Surgery, Countess of Chester Hospital, Chester, CH2 1BQ, U.K.
Introduction
Horseshoe k idney (HSK) is an unusual abnormali ty occurring in 0.15--0.25% of the population. 1'2 In its most common form fusion is be tween the lower poles, creating an isthmus of variable size and shape anterior to the aorta and inferior vena cava. This may consist of a simple fibrous band or may contain a significant amount of functioning renal pa renchyma and part of the collecting system. In up to three-quarters of cases it is associated with abnormalities of the renal vas- culature.
The coexistence of abdominal aortic aneurysm (AAA) wi th HSK is rare, being present in only 0.12% of patients undergoing aneurysm replacement. 3 Technical problems related to exposure, vascular access and preservat ion of renal tissue may trap the unwary.
We report two cases of successful reconstruction of the aorta in patients with AAA and HSK and review the literature to date.
Case 1
A 71-year-old lady was investigated for loin pain and recurrent ur inary tract infections by intravenous urography, which revealed a functioning HSK with a calculus in the left lower calyx. Extracorporeal shock wave li thotripsy was p lanned and subsequently aban- doned after an AAA was discovered on ul t rasound scan (USS). A spiral computed tom0graphy (CT)
* Please address all correspondence to: Mr A. P. Moody, MD, FRCS, Consultant Surgeon, Warrington Hospital, Lovely Lane, Warrington, Cheshire, WA51QG, U.K.
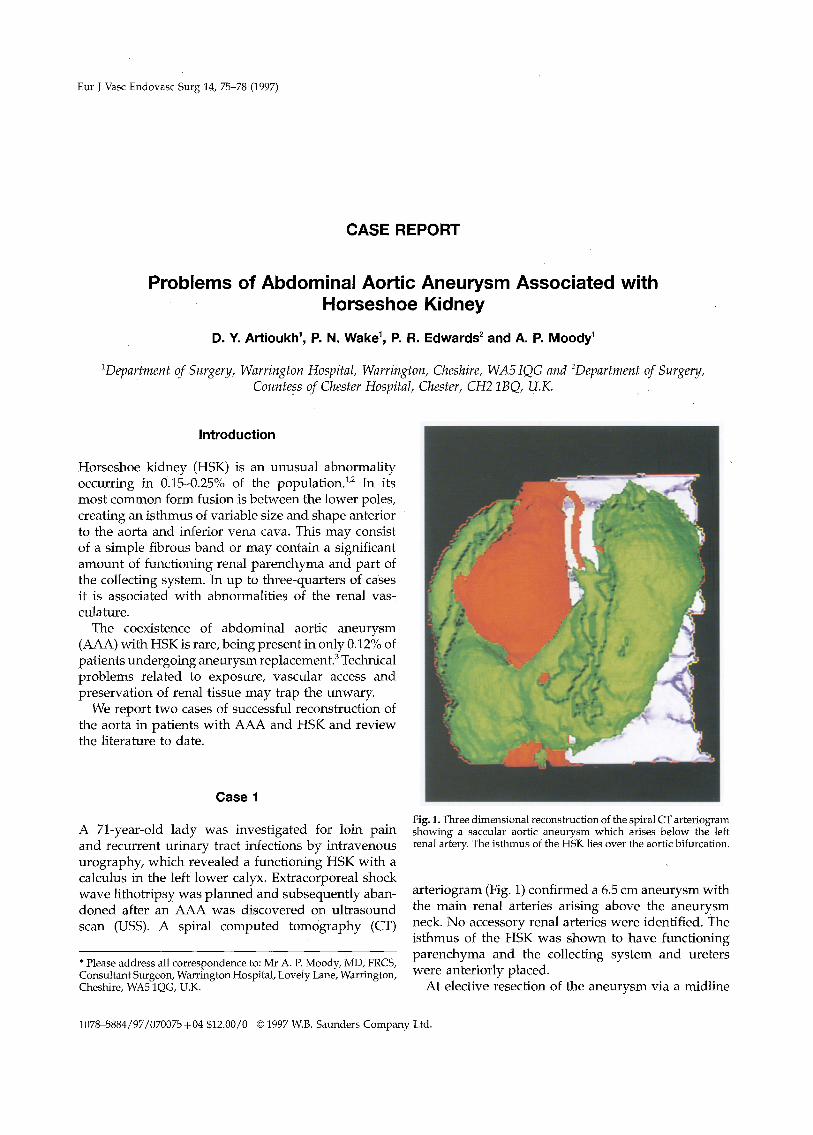
Fig. 1. Three dimensional reconstruction of the spiral CT arteriogram showing a saccular aortic aneurysm which arises below the left renal artery. The isthmus of the HSK lies over the aortic bifurcation.
ar ter iogram (Fig. 1) confirmed a 6.5 cm aneurysm with the main renal arteries arising above the aneurysm neck. No accessory renal arteries were identified. The isthmus of the HSK was shown to have funct ioning parenchyma and the collecting system and ureters were anteriorly placed.
At elective resection of the aneurysm via a midline
1078-5884/97/070075+04 $12.00/0 © 1997 W.B. Saunders Company Ltd.

76 D.Y. Artioukh et al.
inci.sion and transperitoneal exposure of the aorta, the aneurysm was found to be inflammatory with the duodenojejunal flexure and left renal vein densely applied to its anterior surface. The thick isthmus of the HSK was also densely adherent to the aneurysm sac below the inferior mesenteric artery (IMA) origin. The bifurcation of the aorta lay behind the renal isth- mus.
In order to gain proximal control the left renal vein was divided and oversewn, and the aorta cross- clamped above the right but below the left renal artery. Distal control was obtained by clamping the left common iliac and the right exterrial iliac arteries after ligation of the right internal iliac artery. The sac was opened longitudinally and a bifurcated graft anastomosed to the neck. The graft was tunnelled, with difficulty, beneath the isthmus and the distal end- to-end anastomoses were constructed to the external iliac arteries in a standard fashion. Throughout the procedure troublesome bleeding was encountered from the aortic lumen behind the isthmus, arising from the median sacral artery. This was eventually controlled by oversewing both common iliac arteries, packing the distal aorta with haemostatic sponge and oversewing the stump. Postoperatively, the patient's renal function remained normal and she was allowed home, without complications, on the ninth day.
Case 2
A 74-year-old gentleman, followed-up for carcinoma of the bladder, was found to have an asymptomatic AAA measuring 8cm in its maximum diameter on USS. The kidneys and bladder were reported as ultra- sonically normal and elective surgery for AAA was arranged.
A transverse supraumbilical laparotomy was per- formed and exposure of the infrarenal aorta revealed an unsuspected HSK with a substantial isthmus lying below the IMA. Dissection of the aortic neck below the renal arteries was performed and an infrarenal clamp was applie d which caused immediate de- vascularisation of approximately two-thirds of the renal tissue. Renal perfusion was restored after prompt clamp removal. The procedUre was abandoned and the patient underwent arteriography a few days later to clarify the renal arterial anatomy. Thi s demonstrated apparently normally sited main renal arteries which fed the upper poles of the HSK. A large aberrant artery was seen arising from the anterior wall of the aorta
Fig. 2. Lateral view of aortogram demonstrating an infrarenal an- eurysm and a large aberrant renal artery which arises from the anterior wall of the aorta (arrow).
(below the IMA) and feeding the isthmus and a large part of the kidney moieties (Fig. 2).
Re-exploration was performed 2 weeks later and the neck was clamped as before. The common iliac arteries were controlled with balloon occlusion catheters and the IMA was oversewn. The aberrant renal artery was perfused with Ringer lactate and the proximal anastomosis was constructed. A tube graft was tun- nelled below the renal isthmus and the distal ana- stomosis was completed. The lower limbs were reperfused and the aberrant renal artery was then anastomosed to the anterior surface of the graft. Renal function remained normal postoperatively and the patient made an uneventful recovery, going home on the tenth day.
Discussion
Since the first operation performed by Phelan and colleagues in 19564 over 100 cases of abdominal aortic reconstruction in the presence of HSK have been re- ported. The major challenges during surgery are posed firstly by the isthmus of the HSK lying anterior to the great vessels, and secondly by associated renovascular
Eur J Vasc Endovasc Surg Vol 14, July 1997

Abdominal Aortic Aneurysm and Horseshoe Kidney 77
abnormalities. Up to 25% of cases of HSK 5'6 are not diagnosed preoperatively, and this adds significantly to the difficulties encountered, especially in the emer- gency setting. 7
At present, CT scanning is the most accurate imaging modality for the diagnosis of HSK s and also provides important information about the AAA itself, thus ob- viating the need for any other imaging. 6"s USS alone is disappointing and frequently underdiagnoses HSK, as illustrated by our second case. Intravenous uro- graphy is reliable in 88% of cases 6 and is extremely helpful in the delineation of the renal collecting sys- tem. It is not routinely used in aneurysmal disease. Arteriography has an accuracy varying from 258 to 67%, 6 but is the principal tool for assessing the renal arterial pattern. We report the use of spiral CT ar- teriography as an additional modality, which in our first case gave accurate data regarding renal vas- culature and isthmus.
The surgical exposure for aortic reconstruction re- mains controversial. The optimal approach should provide access to the aortic neck, bifurcation and iliac arteries, and allow reimplantation of aberrant renal vessels. It should also minimise the risk of injury to the renal collect!ng system, s
The midline laparotomy is the most widely used 5'7'8 and its proponents feel that it meets these criteria. In the majority of reported cases the isthmus of the HSK was left intact and the graft was simply tunnelled behind it. Our experience with the first case, however, illustrates that a bulky isthmus, if undivided, may make the distal aorta inaccessible and the control of lower lumbar or median sacral arteries difficult. The isthmus has, therefore, been divided by some to im- prove exposure and to gain control in cases of rupture. 9 Opponents of midline laparotomy suggest that di- vision of the isthmus increases the risks of urinary fistula and, since infection is common in HSK, graft sepsis is a potential risk. 6 Severe complications, how- ever, are exceptionaP and division of the isthmus is not necessarily associated with increased morbidity and mortality. 9
Midline incision may be combined with a right retroperitoneal dissection to facilitate visualisation and reimplantation of aberrant renal arteries. 1° Pre- servation of these vessels is essential and, as the pat- terns of supply are highly variable, it is of paramount importance to anticipate the likely reconstructive pro- cedure, otherwise renal failure may ensue following simple arterial ligation.
A left thoracoabdominal retroperitoneal approach is preferred by some because it avoids the collecting system 6'11 and is useful in patients who have had
previous surgery for congenital renal abnormalities. Its main disadvantage is the restriction of access to the right external iliac artery requiring sometimes an additional extraperitoneal incision a few centimetres above the right inguinal ligament. 12
Case 1 required a bifurcated graft because of an inaccessible distal aorta, although a tube graft would have been performed. Current advances in technology have now made endovascular stenting of aortic an- eurysms a reality, which would have been a viable option for this case. However, in most other cases the use of endovascular stenting will be limited by the need to protect renal function by preserving aberrant renal arteries.
We report two cases of successful repair of AAA associated with HSK. In one case the aneurysm was inflammatory and that has not been previously re- ported. The HSK may be missed by USS and therefore CT scan, as the most reliable diagnostic modality, is necessary. Our current practice is to perform spiral CT arteriography for assessment of all aneurysms. This technique may prove useful in delineating renal ar- terial afiatomy and, as further experience is ac- cumulated, may replace conventional arteriography.
Acknowledgements
The authors are grateful to Dr C. C. Yeong for his help in the preparation of illustrations.
References
1 BAUER SB, PERLMUTTER AD, RETIK AB. Anomalies of the upper urinary tract. In: Walsh PC, ed. Campbell's urology. 6th ed. Phila- delphia: WB Saunders, 1992: 1357-1442.
2 BERTIN F I CHRISTIDES C, CORNU E et al. Dissection aigue de l'a0rte sous renale et rein en fer a cheval. Apropos d 'un cas et revue de la litterature. ] Chir (Paris) 1992; 129: 330-334.
3 GIORDANENGO F, VANDONE P, PIZZOCARI P, DE MONTI M, MAT- TIOLI A. Aneurisma dell'aorta addominale e rene a ferro di cavallo. Contributo clinico. Minerva Cardioangiol 1991; 39: 97-102.
4 PHELAN JT, BERNATZ PE, DE WEERD JH. Abdominal aortic an- eurysm associated with horseshoe kidney: report of a case. Mayo Clin Proc 1957; 32: 77-81.
5 JULIA P, HANOTEL MC, GHALAYINI B, FABIANI JN. Abdominal aortic aneurysm associated with horseshoe kidney and du- plication of the inferior vena cava. Ann Vasc Surg 1993; 7: 587-589.
60'HARA PJ, HAKAIM AG, HERTZER NR, KRAJEWSKI LP, COX GS, BEVEN EG. Surgical management of aortic aneurysm and coexistent horseshoe kidney: review of a 31-year experience. J Vasc Surg 1993; 17: 940-947.
7 YAMAN M, WOOSTER D, BOJANOWSKI V, LoucI-I R. Two patients with horseshoe kidney and ruptured abdominal aortic aneurysm. Can ] Surg 1991; 34: 238-241.
8 SHORTELL CK, WELCH EL, OURIEL K, GREEN RM, DEWEESE JA. Operative management of coexistent aortic disease and horse- shoe kidney. Ann Vasc Surg 1995; 9: 123-128.
Eur J Vasc Endovasc Surg Vol 14, July 1997

78 D.Y. Artioukh et aL
9 TAPPER SS, MARTIN RS 3rd, EDWARDS WH, MEACHAM PW. Ruptured abdominal aortic aneurysm and horseshoe kidney. South Med f 1990; 83: 224-226.
10 DA¥IDSON BR, GARDHAM R. Selective use of a right retro- peritoneal approach to abdominal aortic aneurysm. Br J Surg 1992; 79: 639-640.
11 MASON RA, KVILEKVAL KH, HARTMAN A, GIRON E The retro- peritoneal approach to aortic surgery associated with horseshoe kidney. ] Cardiovasc Surg (Torino) 1991; 32: 763-766.
12 SHEPARD AD, TOLLEFSON DF~ REDD'd DJ et al. Left flank retro- peritoneal exposure: a technical aid to complex aortic re- construction. J Vasc Surg 1991; 14: 283-291.
Accepted 11 September 1996
Eur J Vasc Endovasc Surg Vol 14, July 1997