prognosis of luxated permanent teeth — the development of pulp necrosis
TRANSCRIPT

Prognosis of luxated permanent teeth - thedevelopment of pulp necrosisAtidreasen EM, Vestergaard Pedersen B. Prognosis of luxatedpermanent teeth - tbe development of pulp necrosis. EndodlDent Traumatol 1985; 1: 207-220.
Abstract - A population of 400 patients, eomprising 637 luxatedpermanent teeth was studied prospeetively with respect to thedevelopment of pulp necrosis after luxation injuries. The patientswere treated for traumatic dental injuries over a period of 10years. While initial treatment was provided according to estab-lished treattnent guidelines by the attending oral surgeoti at theemergency room, foUow-tip examination and treatment was pro-vided by one oral surgeon. It ap]3eared th;tt pulp necrosis occtn-redsoon after injury, within 3 tnonths after conctission, wilhin (he1st yr after subluxation and extrusion, and might be diagnosedu p to 2 yr after lateral- and intrtisive ltixatioti. While tnanyfactors, when considered one at a tintc, were Ibund to have asignifteant or nearly significant ellect on the devclo]imcnt o( ptilpnecrosis (i.e. type of injtn-y, age of jxttient, stage of root develop-m e n t , degree of dislocation, reducli(3n/rc|3ositioning j^roccdurc,t y p e of fixation, restorations in place at the lime of injtiry), amullivariate regression analysis revealed lluil when ihe type ofinjury (diagnosis) and stage of foot development were takeni n t o account, (he elfecl of other factors was no longer significant."ri ie risk of pulp neerosis increased witfi the extent of injury, i.e.concussion and subluxation represented the least risk, followedi n ascetiding order by extrusive-, lateral-, and ititrusive lux-a t ion . Moreover, teeth wilfi (om|)letcd root formation detnon-s t ra ted a greater risk of pul]5 necrosis than teeth witfi iticotnpleter o o t fbrmation. No treattnent effect could be demonstrated. How-ever, as treatment was perfortned accotding to established guideli-n e s , which might introduce bias, it would appear justifted toconduc t randomized elinieal sttidies in oider to determine thev a l u e of different forms of treatment (e.g. reduction and ftxationo f luxated teeth) to improve tlie prognosis with respect to thedevelopment of pulp necrosis after injury. In conclusion, thema jo r faetors influencing dcveloi^ment of pul]3 necrosis after hix-a t i o n injuries appear to be the extent of the initial injury to thep u l p and periodontium, as reflected by the type of luxation,a n d the repair potential of the injtu'ed tooth, as reflected by thes t a g e of root dcvefoi^ment.
Frances iVI. Andreasen* and Bo Vester-gaard Pedersen**'Department of Oral Medicine and Oral Surgery,University Hospital (Rigshospitalet), and Departmentof Pedodontics, Royal Denial College, Copenhagen."Statistical Research Unit, Copenhagen Univer-sity and the Danish Breast Cancer CooperativeGroup, Finsen Institute, Copenhagen, Denmark
Key words: luxation injuries, prognosis, pulp necro-sis, root development, proportional hazards re-gression model, grouped survival data.R M. Andreasen, nD.S., Department of Oral Medi-cine and Oral Surgery, University Hospifal (Rigsho-spitalet), Tagensvej 18, DK 2200 Copenhagen N,Denmark.
Accepted for publication 13 May 1985.
Desj^ite many chnical and experinienlal sltidies, theetiology of pulp tiecrosis after luxation injuries isst i l l uncertain (1 14). The general outcome of theseinvestigations has been the idetitiflcation of clinicalfactors wliich, (o a greater or lesser degree, werefound to \)c associated with the developtnent of pttlp
neci'osis after injury. These factors include: age ofthe patient (1, 3, 8, 9), stage of root development(1, 3, 5 12, 27), type of luxation injury (3, 6, 8, 9,11, 12, 27), mobility of the injured tooth at the timeofinjtiry (1, 2, 6, 8, 13), degree of dislocation (14),initial positive reaction to pulp testing (1, 5, 6, 13),
207
Andreasen and Pedersen
tenderness to percussion at the time of injury (13,15), the type of reduction procedure (2, 16), fixationperiod (2), and delayed initial treatment (1, 5, 6,8). These results imply a rather complex etiology ofpulp neerosis after luxation injuries. However, inmany of these studies, only the Jrequency of pulpnecrosis in relation to one factor at a time wasstudied. Sueh analyses neglect the time from injuryto occurrence of pulp necrosis and cannot accountfor the possible close associations between factorsstudied, sueh as between age and root developmentor mobility and displacement of an injured toothand the type of luxation. A multivariate analysis isrequired to identify the smallest set of factors whicficontains the greatest amount of prognostie infor-mation with respeet to development of pulp necrosisafter luxation injuries.
It is therefore the aim of the present investigationto answer the following questions using a populationof patients whieh has been uniformly treated forluxation injuries to the permanent dentition andfollowed prospeetively for up to 10 yr:
1. Which types of luxation injuries are followedl)y pulp neerosis and to what extent? 2. What is thechronologieal relationship between type of luxationinjury and the diagnosis of pulp necrosis? 3. Wfiichfactors associated with injury or subsequent treat-ment determine the development of pulp necrosisalter ltjxation injuries?
Material and methodsMaterial
'fhe material eomprises 400 patients with 637 lux-ated teeth and 414 non-injured (control) teeth selec-ted from 3260 referred to and treated fbr luxationinjuries at the Department of Oral Medicine andOral Surgery, University Hospital, Copenhagen.Details concerning selection of patient material, di-agnostic criteria for luxation injuries and treatmentl^rocedures have been described elsewhere (17).
Only teeth which fulOllcd the criteria for luxationinjuries (18) were admitted to the study; that is,concussion, subluxation, extrtisive luxation, lateralluxation and intrusion.
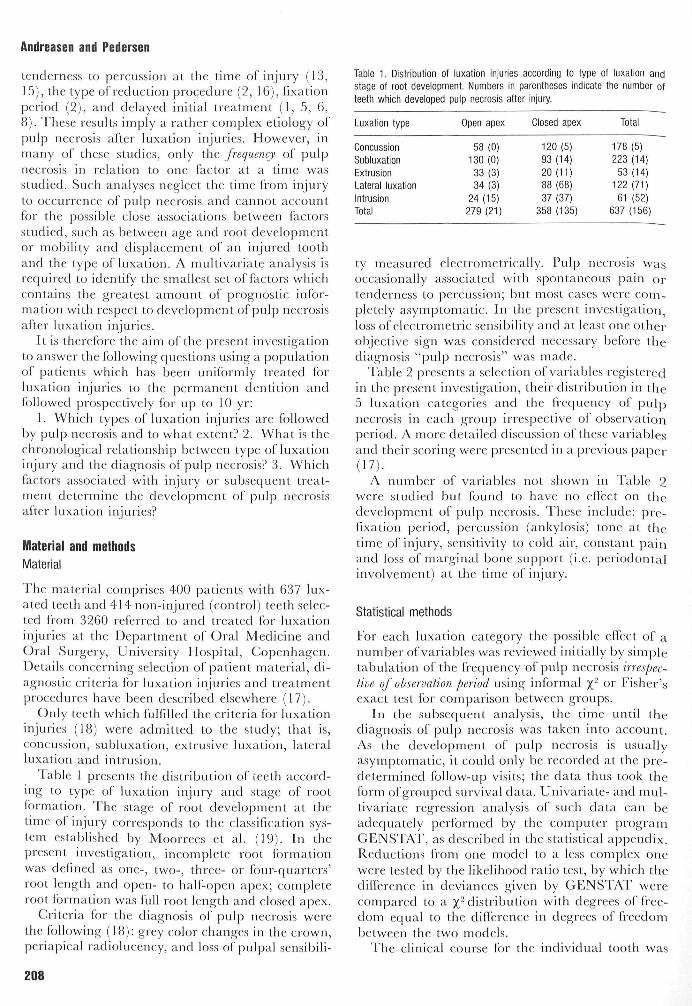
lable 1 presents the distribution of teeth accord-ing to type of luxation injury and stage of rootformation. 'I'he stage of root development at thetime oi injury corresponds to the classification sys-tem established by Moorrees et al. (19). In thepresent investigation, ineomplete root formationwas defined as one-, two-, three- or four-quarters'root length and open- to half-open apex; comjiletcroot formation was full root length and closed apex.
Criteria for the diagnosis of pulp neerosis werethe following (18): grey color changes in the crown,periapical radiolueency, and loss of pulpal sensibih-
Table 1. Distribution of luxation injuries according to type of luxafion andstage of root development. Numbers In parentheses indicate fhe number ofteeth which developed pulp necrosis after injury.
Luxation type
ConcussionSubluxafionExtrusionLateral luxafionIntrusionTotal
Open apex
58 (0)130 (0)
33 (3)34(3)
24(15)279 (21)
Closed apex
120 (5)93 (14)20 (11)88 (68)37 (37)
358 (135)
Total
178(5)223 (14)
53 (14)122 (71)61 (52)
637 (156)
ty measured electromctrically. Pulp necrosis wasoccasionally associated with spontaneous pain ortenderness to percussion; but most cases were com-pletely asymptomatic. In the present investigation,loss of electrometrie sensibility and at least one otherobjective sign was considered necessary before tbediagnosis "pulp necrosis" was made.
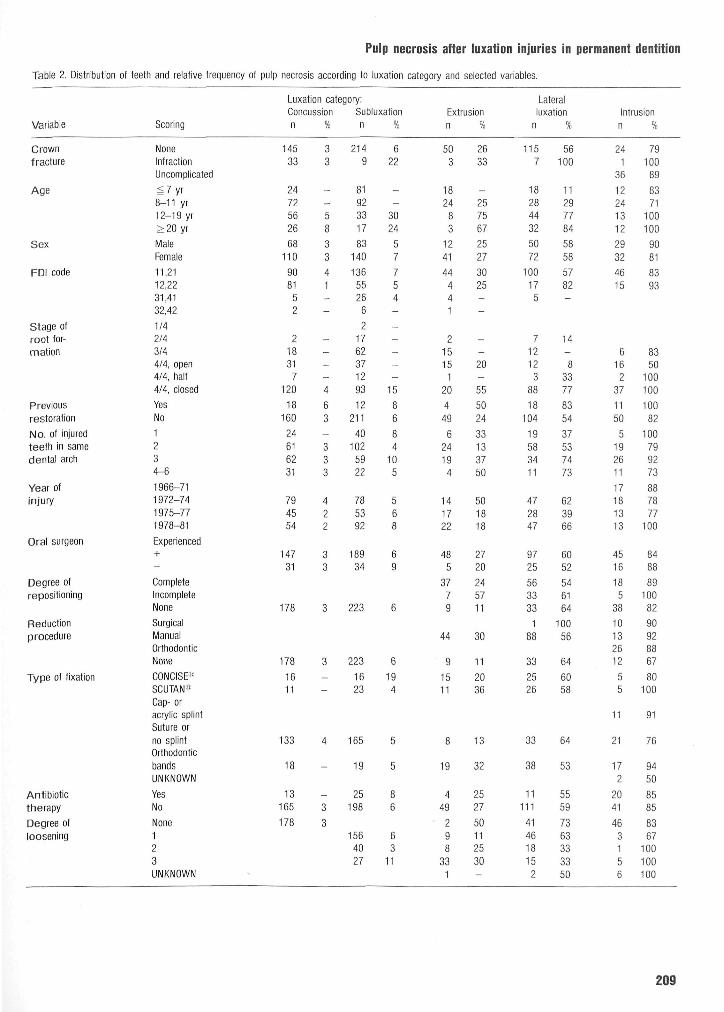
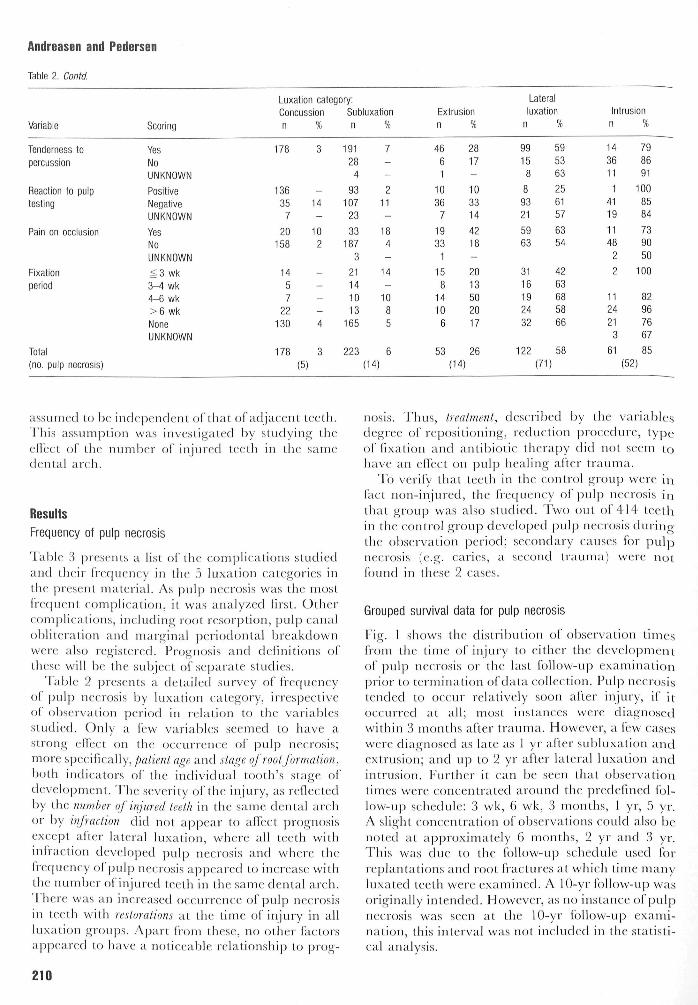
Table 2 presents a seleetion of variables registeredin the present investigation, their distribution in tbe5 luxation categories and the frec[ueiicy of pulpnecrosis in each group irrespective of observationperiod. A more detailed discussion of these variablesand their scoring were presented in a previous paper(17).
A number of variables not shown in Table 2were studied but found to have no effect on thedevelopment of pulp necrosis. These include: jare-fixation period, percussion (ankylosis) tone at thetime of injury, sensitivity to eold air, constant |3ainand loss of marginal bone support (i.e. |:)ci iodontalinvolvement) at the time of injury.
Statistical methods
Eor each luxation category the possible elfect of anumber of variables was reviewed initially by simpletabulation of the frequency of pulp necrosis irrespec-tive of observation period using informal %' or Eisher'sexact test for comparison between groups.
In the subsequent analysis, the time until tbediagnosis of pulp necrosis was taken into account.As the development of pulp necrosis is usuallyasymptomatic, it could only be recorded at the pre-determined fbllow-up visits; the data thus took theform of grouped survival data. Univariate- and mul-tivariate regression analysis of such data can beadequately performed by the computer programCENSTAT, as described in the statistical a]5penclix.Reductions from one model to a less eomplex onewere tested by the likelihood ratio test, by which thedilTert nce in deviances given by GENS'lAT wereeomjjared to a c distribution with degrees ol free-dom equal to the difference in degrees of freedombetween the two models.
The elinieal eourse for the individual tooth was
208
Pulp necrosis after luxation injuries in permanent dentition
Table 2. Distribution of feefh and relative frequency of pulp necrosis according fo luxation category and selected variables.
Variable
Crowntracfure
Age
Sex
FDI code
Stage ofroof for-mation
Previousrestoration
No. of injuredteefh in samedental arch
Year ofinjury
Oral surgeon
Degree ofrepositioning
Reducfionprocedure
Type of fixation
AntibiotictherapyDegree ofloosening
Scoring
NoneInfracfionUncomplicated
g7 yr8-11 yr12-19 yr>20yrMaleFemale
11,2112,2231,4132,42
1/42/43/44/4. open4/4, half4/4, closed
YesNo1234-6
1966-711972-741975-771978-81
Experienced
+-CompleteIncompleteNone
SurgicalManualOrthodonticNone
CONCISE*
SCUTAN"
Cap- or
acrylic splinfSuture orno splinfOrfhodonfic
bandsUNKNOWN
YesNo
None
123UNKNOWN
Luxafion cafegory:Concussionn
14533
2472562668
1109081
52
21831
7120
18160
24616231
794554
14731
178
178
1611
133
18
13165
178
%
33
.--583341_-
----4
63
—
333
422
33
3
3
_-
4
_
_
3
3
Subluxationn
2149
81923317
83140
13655266
21762371293
12211
40102
5922
785392
18934
223
223
1623
165
19
25198
1564027
%
622
--
3024
57754-
-----
15
86
84
105
568
69
6
6
194
5
5
86
63
11
Extrusionn
503
1824
83
124144441
215151
20
449
624194
141722
485
3779
44
9
1511
8
19
449
298
331
%
2633
-
257567
25273025--
--20-
55
5024
33133750
501818
2720
245711
30
11
2036
13
32
2527
50112530-
Laferalluxation
n
1157
18284432
5072
100175
712123
88
18104
19583411
472847
9725
563333
188
33
2526
33
38
11111
414618152
%
56100
11291184
5858
5782-
14-
83311
8354
37537473
623966
6052
546164
10056
64
6058
64
53
5559
7363333350
Intrusionn
241
36
12241312
2932
4615
6162
37
1150
5192611
17181313
4516
185
38
10132612
55
11
21
172
2041
4631
56
%
7910089
8371
100100
9081
8393
8350
100100
10082
100799273
887811
100
8488
89100
82
90928867
80100
91
76
9450
8585
8367
100100100
209
Andreasen and
Table 2. Contd.
Variable
Tenderness fopercussion
Reaction fo pulpfesfing
Pain on occlusion
Fixationperiod
Total(no. puip necrosis)
Pedersen
Scoring
YesNoUNKNOWN
PositiveNegativeUNKNOWN
YesNoUNKNOWN
g 3 wk3-4 wk4-6 wk>6 wkNoneUNKNOWN
Luxafion cafegory:Concussionn
178
136357
20158
1457
22130
178
%
3
-
14-
102
_-——
4
3
(5)
Subluxafionn
19128
4
93107
23
33187
3
21141013
165
223
%
7-
-
211-
184-
14.-
1085
6(14)
Extrusionn
4661
10367
1933
1
158
14106
53
%
2817-103314
4218-
2013502017
26(14)
Lateralluxation
n
9915
8
89321
5963
3116192432
122
%
595363
256157
6354
4263685866
58
(71)
Intrusionn
14
3611
14119
1148
22
112421
3
61
%
79
8691
1008584
7390
50100
82967667
85(52)
assumed to be inde|x'ndent ol that of adjacent teeth.I his assumption was investigated by studying theeflect of the number of injured teeth in the samedental areh.
ResultsFrequency of pulp necrosis
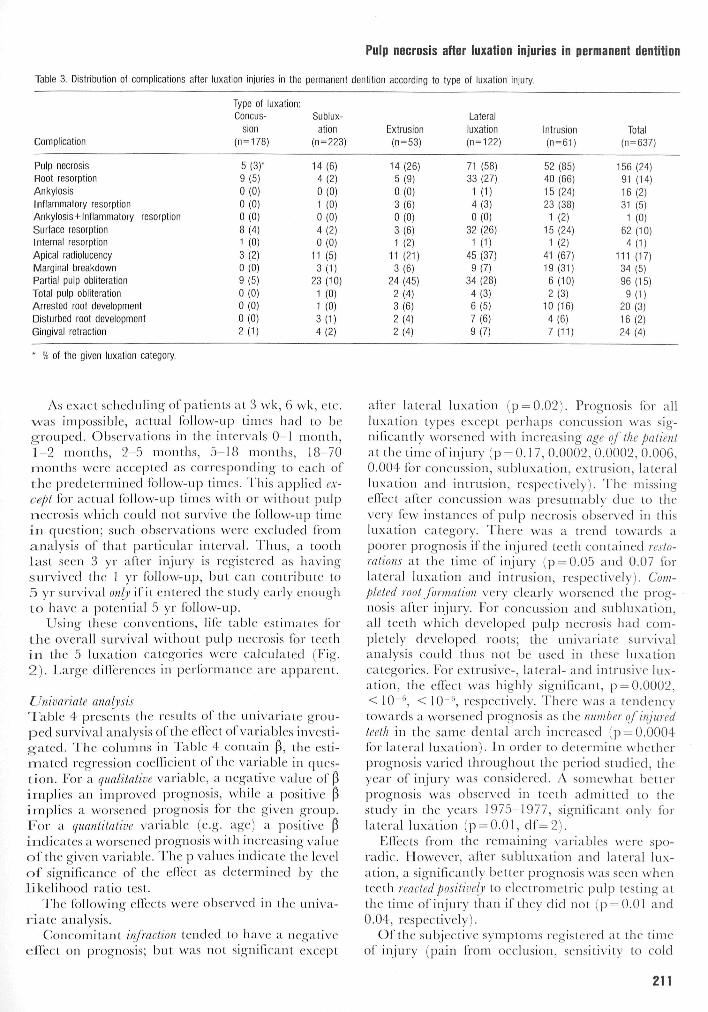
Table 3 presents a list of the e(MTipli( ations studiedand their frequency in the .5 luxation categories inthe present material. As pulp necrosis was the mostfrequent complication, it was analyzed first. Othercomplications, including root resorption, pulp canalobliteration and marginal periodontal breakdownwere also registered. Prognosis and definitions ofthese will be the subject of separate studies.
Table 2 presents a detailed survey of frec|ueneyof ptilp necrosis by luxation category, irrespectiveof observation ]:)eriocl in relation to the variablesstudied. Only a few variables seemed to have astrong effect on the occurrence oi |3ulp necrosis;more speeifically, patient age and stage of root forma lion,both indicators of the individual tooth's stage ofdevelopment. The severity of the injury, as reflectedby the number of injured teeth in the same dental archor by infraetioit did not a|Dpeai- to allect prognosisexcept after lateral luxation, where all teeth withinfraction developed ijulj) neerosis and where thefrequency of pulp necrosis appeared to increase withthe number of injured teeth in the same dental arch.There was an increased occurrence of pulp necrosisin teeth with restorations at the time of injury in allluxation groups. Apart from these, no other factorsappeared to have a notieeable relationship to prog-
nosis. Thus, Ireatmenl, described by the variablesdegree of repositioning, redtution procedure, typeof fixation and antibiotic th<~rapy did not seem tohave an elfect on |)ulp healing after trauma.
To verify that teeth in the control group were infact non-injured, the frequeney of pulp necrosis inthat grou|5 was also studied. Two out of 4H- teetbin the control group developed pulp necrosis during-the observation period; secondary causes for pulpnecrosis (e.g. caries, a second trauma) w(-re notfound in these 2 cases.
Grouped survival data for pulp necrosis
lMg. I shows the distribution of observation timesfrom the time of injury to cither the devel()])mentof |:)ulp neerosis or the last follow-ti]i examination]:)rior to termination of data cx)llection. Pi\\p necrosistended to occur relatively soon after injury, if itocctured at all; most instances were diagnosedwithin 3 months after trauma. However, a few caseswere diagnosed as late as 1 yr after subluxation andextrusion; and up to 2 yr after lateral luxation andintrusion. Etnlher it can be seen tha( observationtimes were concentrated around the predefined fol-low-u]3 sehedule: 3 wk, G wk, 3 months, 1 yr, 5 yr.A slight concentration of observations eould also benoted at approximately (3 months, 2 yr and 3 yr.This was due to the follow-u]3 schedule used forreplantations and root (racttues at which time manyluxated teeth were examined. A 10-yr follow-up wasoriginally intended. However, as no instance of ]3ulpnecrosis was seen at the 10-yr follow-up exami-naticjn, this interval was not included in the statisti-cal analysis.
210
Pulp necrosis atter luxation injuries in permanent dentition
Table 3. Oisfribufion of complications after luxafion injuries in fhe permanenf denfifion according fo fype of luxafion injury.
Complicafion
Pulp necrosisRoof resorptionAnkylosisInflammatory resorpfionAnkylosis-i-Inflammafory resorpfionSurface resorpfionInfernal resorpfionApical radiolucencyMarginal breakdownParfial pulp obliterationTofal pulp obliferafionArresfed roof developmenfDisturbed roof developmenfGingival refraction
* % of fhe given luxation category.
Type of luxafion:Concus-
sion(n=178)
5(3)-9(5)0(0)0(0)0(0)8(4)1 (0)3(2)0(0)9(5)0(0)0(0)0(0)2(1)
Sublux-afion
(n=223)
14(6)4 ( 2 )
0(0)1 (0)0(0)4(2)0(0)
11 (5)3(1)
23 (10)1 (0)1 (0)
3(1)4(2)
Exfrusion(n=53)
14(26)5(9)0(0)3(6)0(0)3(6)1 (2)
11 (21)3(6)
24 (45)2(4)3(6)2(4)2(4)
Laferalluxation(n=122)
71 (58)33 (27)
1 (1)4(3)0(0)
32 (26)
1 (1)45 (37)9(7)
34 (28)4(3)6(5)7(6)9(7)
Infrusion(n=61)
52 (85)40 (66)15(24)23 (38)
1 (2)15(24)1 (2)
41 (67)19 (31)6(10)2(3)
10 (16)4(6)7(11)
Total(n = 637)
156 (24)91 (14)16(2)31 (5)
1 (0)62 (10)4(1)
111 (17)34(5)96(15)9(1)
20(3)16(2)24(4)
As exact scheduling of patients at 3 wk, t) wk, etc.was impossible, actual fbllow-iii^ times had to begrouped. Observations in the intervals 0 1 month,1-2 months, 2-5 months, 5-18 months, 18 70months were acce|5ted as corrcspcjiiding to each ofihe predetermined follc)w-ti|3 times. This ajjplied ex-cept for acttial fbllovv-ti|3 times with or withotil pulpnecrosis which could not stir\ i\e fhe fbllow-up timein question; such observations were excluded fromanalysis of that particulai' interval. Thus, a toothlast seen 3 yr after injury is registered as havingsurvived the 1 yr follow-up, but can contribute to5 yr survival onlv if it entered the study early enoughto have a potential 5 yr IOIIOW-UJD.
Using these conventions, life tabfe estimates fbrthe overall survival without pulp necrosis for teethin the 5 Itixation categories were calctilated (Eig.2) . Large diirerences in performance are apparent.
Urtivariate analysisTable 4 presents the results of the uui\ ariate grou-ped survival analysis of the elfect of variables investi-g-ated. The columns in 'Jable 4 contain 0, the esti-mated regression cocllicient of the variable in ques-tion. Eor a qualitative variable, a negative value of 0implies an improved prognosis, while a jjositive 3implies a worscncxl ]jrc)gnosis fbr the gi\'en group.For a quanlitalive variable (e.g. age) a positive (5indicates a worsened prognosis with iiu-rcasing vahieof the given variable. The p values indicate the levelo f significance of the effeet as determined by thelikelihood ratio test.
The fbllowiiig effecUs were observed in the univa-r ia te analysis.
Ccjiicomitant infraction tended to have a negativeeffect on pi'ognosis; but was not significant cxc:ept
after lateral luxation (p = 0.02). Prcjgnosis for allluxation t)pes except perhaps concussion was sig-nificantly worsened with increasing age of the patientat the time of injury (p = 0.1 7, 0.0002, 0.0002, 0.006,O.OO-l fbr concussion, subluxation, extrusion, lateralluxation and intrusion, respectix'ely). The missingeflect after concussion was presumably dtie to thevery few instances of ])tilp neerosis obscr\ed in thisItixation category. There was a trend towards apoorer prognosis if the injured teeth contained resto-rations at the time of injury (p = 0.05 and 0.07 forlaferal luxation and intrusion, respectively). Com-pleted root formation very clearly worsened the prog-nosis after injury. Eor eoneussion and subluxation,all teeth whieh de\eloped pulp necrosis had com-]Dletely developed roots; the univariate survivalanalysis could thus not be used in these luxationeategories. Eor extrusive-, lateral- and intrusi\ e lux-atic:>n, the effect was highly significant, p = 0.0002,< 10 '', < 10"'', respecti\'ely. There was a tendencytowards a worsened prognosis as the number of injuredteeth in the same dental arch increased (p = 0.0004for lateral luxation). In order to determine whetherprognosis varied throughotit the period studied, theyear of injtii')' was considered. A somewhat belterprognosis was observed in teeth admitted fo thesttidy in the years 1975-1977, significant only forlateral luxation (p = 0.01, df=2) . '
Efibcts from (he remaining variables were spo-radic. However, after subhixation and lateral lux-ation, a significantly better prognosis was seen whenteeth reactedposilively to electrometrie ptilp testing atthe time of injury than if they did not (p = 0.01 aiul0.04, respectively).
Of the subjective symptoms registered at the timeof injury (pain from occlusion, sensitivity to cold
211

Andreasen and Pedersen
PULP SURVIVAL AFTER LUXATION INJURIES.Total material.
Fig. t. Distribulioii ol observation times Irom injury to citherthe dcvelo])rn(Mil of pulp necrosis (solid, black columns) or (hefast fbllow-iip cxamiiKilion |)rior lo lerniinalion ol data collection(elonijjated 1 's). i'.acii li( on the Y axis niduales 5 instances oleilher pulp necrosis or survixal vvilhoul pnlp necrosis.
air, constant pain), only pain from occlusion seemedto be aecompanied by a worsened i^rognosis, signifi-cant for subluxafion and extrusion (]3 = 0.01, 0.05,respectively).
Multivariale analysisThe following is a review of the mtiltivariate anttlysisfor each luxation category based on simultaneousinelusion of thcise variables fbund to be of interestin the univariate analysis described above.
According to the univariate analysis (Table 4),the two most important variables with respect tothe development CDI |3ulp necrosis were age and rootformation. These two variables, however, were closelyassociated. It was only in the group 8-1 1 yr of age(Table 2) that there were teeth with both completeand incomplete root formation. The group ^ 7 yrcontained only teeth with incomplete root forma-tion, while the group ^12 yr contained only teethwith completed root formation. In order to deter-mine whether age contained other prognostic infor-mation than that contained in stage ol root forma-tion, the possible interaction between rocjt ibrmationand age was investigated. Because of the limitedrange of ages for teefh with incomplete root forma-tion, only the effect of age on teeth with completedroot formation was analyzed.
Coticussioti and subluxation
'1 he frccjueney of ]julp necrosis for both luxationcatcgcjrics was very low. Moreover, all ]5ul|i necrosis
a concussjone subluxation
extrusion
laL lux.
intrusion
No. at risk during interval;
173
subluxation o 212 „ 73
extnjsion
laL lux.
intnjsion
53
_L22_ 1 1 3 I 7 4 I C)1
Fig. 2. Life lalile esliniales olsnivival wilhoul pnlp neerosis ofleeth in (he .') luxalion categories.
occurred in teeth with coinpleled root formation: thus,the elfect of root development could not be includedin the analysis, and an independent multivariateanalysis cjf ecjncussicjti and subluxatiou was, there-fore, not perfbrmed.
Extrusion
From Eig. 1, it appears that no pulp neci'osis oc-curred at the 3-incjnth or 5-yr follow-up; these inter-vals were, therefore, excluded from the analysis.Because of the limited material in this luxation cate-gory, only the effeets of root formation and age wereconsidered, lable 5 shows that when the cflects ofroot formation and age (either age for all teeth orage for teeth with completed root (brmation only)were eonsidered simultaneously, neither elfect wassignificant. In the final model, the elfeet of completedroot formation was highly significant for the develc^p-ment of pul]:) necrosis (p = 0.0002).
Lateral luxation
There were several variables which, when con-sidered individually, had a signifieant elTect cjn thedevelopment of pulp necrosis. 1 hese were con-sidered in the multivariate analysis. Table 6 reviewsthe results of the analysis of variables where com-plete information was available.
212

Pulp necrosis after luxation injuries in permanent dentition
Table 4. Univariafe survival analysis. The esfimafed regression coefficienf and level of significance are given for eacfi variable and each fype of luxafion, Empfycolumns represenf irrelevanf analyses (see Table 2).
Variable
Crownfracfure
Afle
Previousresforafion
Complefed roofformafion
No. of injured teeth In samedenfal arch
Year of injury
InfrusionExfrusionRefrusion
Degree of repositioning
Reducfionprocedure
Type of fixafion
Anfibiofictherapy
Pre-fixation period
Degree of loosening
Tenderness fopercussion
Reacfion fopulp fesfing
Pain on occlusion
Scoring
NoneInfracfionUncomplicafed
(in yr)
YesNo
YesNo
(quanfifafive)
<19751975-771978-81
(mm)(mm)(mm)
ComplefeIncomplefeNone
SurgicalManualOrfhodonticNone
CONCISE""SCUTAN'"Cap- or acrylic splinfSufure or no splintOrfhodonfic bands
YesNo
< 3 hg 3 h
None123
YesNo
PosifiveNegafive
YesNo
Luxafion
Concussion
3 P
0.11
.05
.790
.27
0-.55- .74
1.730
.92
.17
.52
.57
.77
.09
cafegory:
Subluxafion
P P
01.52
.07
.280
.10
0.11.39
1.29-.23
0-.04
.290
0-.91
.57
-1.69
0
1.510
.09
.0002
.75
.65
.78
.35
.65
.35
.or
.01*
Exfrusion
P P
0.47
.20
1.020
2.160
.45
0-1.28-1.25
-.07- 0 3
.791.96
0
1.03
0
.451.15
0.98
- 0 80
0-.21
0-2.10-1.23-.91
.600
-1.350
1.050
.67
.0002
.24
.0002
.82
.07
.56
.86
.11
.51
.60
.92
.74
.45-
.53*
.11*
.05*
Laferal
luxation
P P
01.16
.02
.600
2.780
.39
0-.87.02
.04
.00
- 3 4-.21
0
-.29
0
-.33-.12
0-.25
-.170
0.19
0-.18
-1.06-1.16
.240
-1.230
.270
.02
.006
.05
<io-«
.0004
.01
.65
.95
.50
.27
.75
.65
.53
.01*
.57*
.04*
.25
Intrusion
P P
0-.28.41
.02
.700
1.720
.08
0-.31.69
.09
.05
.84
.810
1.311.47.850
.462.29.680
.90
-.250
0.76
0-.36- 1 3.95
-.020
2.64
0
-.270
.32
.004
.07
<10-f'
.53
.06
.08
.53
.02
.01
.01*
.37
.12
.35*
.95*
.17*
.48*
* Variables which are not registered for all feefh in invesfigafion.
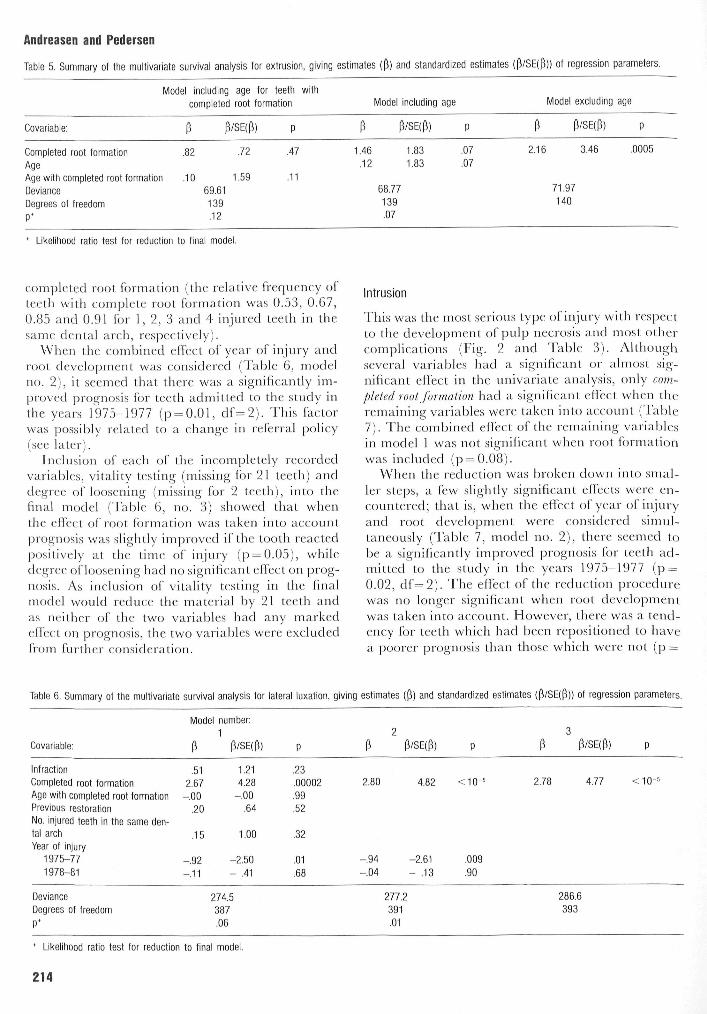
In the full statistical model (Table 6, model no.1), it api^eared that only completed root formation hada highly signifieant eifect on the development ofpulp necrosis. The remaining variables did not addsignificant information (p = 0.06) when root fbrma-tion was considered. Although the number of in-
jured teeth in fhe same dental arch had a stronglysignifieant effect on prognosis in the uni\ariateanalysis, its elfect was not sigtiificanf in fhe muhi\a-riate analysis (p = 0.32). fhis might be explainedby the close association that was found between theluiniber of iiijtn ed teeth in the same dental arc h and
213
Andreasen and Pedersen
Table 5. Summary of fhe mulfivariafe survival analysis for exfrusion, giving esfimates (p) and sfandardized esfimafes (p/SE(p)) of regression parameters.
Covariable:
Complefed roof formafionAge
Model includingcomplefed
P P.82
Age wifh complefed roof formafion .10DevianceDegrees of freedom
P*
69.61139.12
ageroof
/SE(f
.72
1.59
for feefh wifhformafion
>) P
.47
.11
P1.46.12
Model including
P/SE(p)
1.831.83
68.77139.07
age
P
.07
.07
Model excluding age
P P/SE(P) p
2.16 3.46 .0005
71.97
140
likelihood rafio fesf for reduction fo final model.
completed root formation (the relative frequency ofteeth with complete root formation was 0.53, 0.67,0.85 and 0.91 for 1, 2, 3 and 4 injured teeth in thesame dental arch, respectively).
When the combined effect of year of injury androot development was considered (Table 6, modelno. 2), it seemed that there was a significantly im-proved progncjisis for teeth admitted to the study inthe years 1975-1977 (p = 0.01, df=2). This factorwas possibly related to a change in referral policy(see later).
Inclusion of each of the incompletely recordedvariables, vitality testing (missing fbr 21 teeth) anddegree of loosening (missing for 2 teeth), into thefinal model (Table 6, no. 3) showed that whenthe effect of root formation was taken into acc:ountprognosis was slightly improved if the tooth reactedpositively at the time of injury (p = 0.05), whiledegree of loosening had no signifieant effect on Jjrog-nosis. As inelusion of vitality testing in the finalmodel would reduce the material by 21 teeth andas neither of the two variables had any markedeffect on prognosis, the two variables were excludedfrom further consideration.
Intrusion
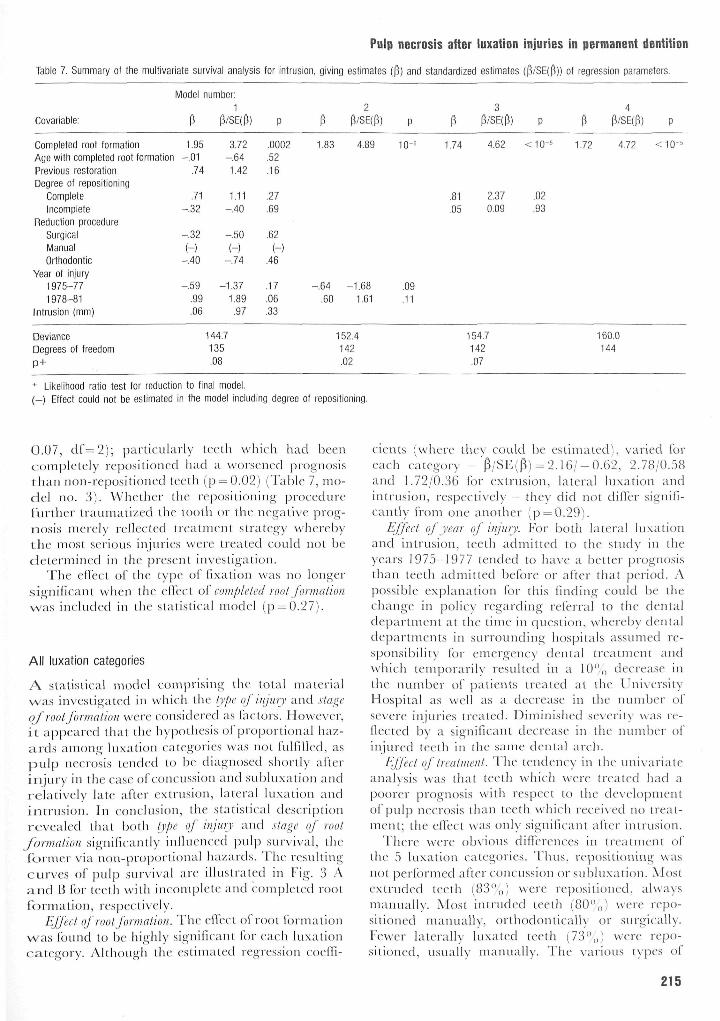
'fhis was the most serious type of injury with respectto the development of pulp necrosis and most othercomplications (Fig. 2 and Table 3). Althoughseveral variables had a significant or almost sig-nificant effect in the univariate analysis, only com-pleted root formation had a significant effeet when theremaining variables were taken into account (Table7). The combined effect of the remaining variablesin model 1 was not significant when root fbrmationwas included (p = 0.08).
When the reduction was broken down into smal-ler steps, a few slightly significant effeets were en-countered; that is, when the effect of year of injuryand root develo]3ment were considered sinnil-taneously (Table 7, model no. 2), there seemed tobe a significantly improvc;d prognosis fbr teeth ad-mitted to the study in the years 1975 1977 (p =0.02, df=2). J he elTect of the reduction piocedtn-ewas nc3 longer significant when root developmentwas taken into aeeount. However, there was a tend-ency Ibr teeth which had been repositioned to havea, |)oorer |3rognosis than those which were not (]:) =
Table 6. Summary of fhe mulfivariafe survival analysis for laferal luxafion, giving esfimates (f!) and standardized esfimates (p/SE(p)) of regression parameters.
Covariable:
Model number:1
P P/SE(P) P/SE(P) P/SE(P)
Infracfion .51 1.21 .23Completed roof formafion 2.67 4.28 .00002 2.80 4.82 <10-5 2.78 4.77 < 1 0 -Age wifh complefed roof formafion -.00 -.00 .99Previous resforafion .20 .64 .52No. injured feefh in fhe same den-tal arch .15 1.00 .32Year of injury
1975-77 - J 2 -2.50 .01 -.94 -2.61 .0091978-81 -.11 - .41 .68 -.04 - .13 .90
DevianceDegrees of freedom
P'
274.5387.06
277.2391.01
286.6393
* Likelihood rafio fesf for reducfion fo final model.
214
Pulp necrosis after luxation injuries in permanent dentition
Table 7. Summary ot the muitivariate survival analysis for intrusion, giving estimates (0) and standardized estimates (p/SE(P)) ot regression parameters.
Model number:1
Covariable:
Completed root formationAge with completed root formationPrevious restorationDegree of lepositioning
CompleteIncomplete
Reduction procedureSurgicaiManualOrthodontic
Year of injury1975-771978-81
Intrusion (mm)
1.95-.01
.74
.71-.32
-.32
(-)-.40
-.59.99.06
372-.641.42
1.11-.40
-.50
(-)-.74
-1.371.89.97
.0002
.52
.16
.27
.69
.62(-)
.46
.17
.06
.33
1.83 4.89
-.64 -1.68.60 1.61
10-'
.09
.11
1.74 4.62
.81 2.37
.05 0.09
1.72 4.72
.02
.93
DevianceDegrees of freedom
P+
144.7135.08
152.4142.02
154.7142.07
160.0144
* Likelihood ratio test for reduction to tinal model.( - ) Ettect could nof be estimated in the model including degree of repositioning.
O.07, cli"=2); i)articuhu'ly teeth which had beencompletely ropositioncd liad a worsened prognosisthan non-repositioiicd teetli (p = 0.02) (Table 7, mo-del no. 3). VN'hetlu-r the re]3ositioning iDroccdiirefurtlirr traumatized the toolh or the negative prog-nosis merely rellected treatment strategy wherebythe most serious injuries were treated could not bedetermined in the present investigalion.
The effect of the type ol' lixation was no longersignilicant when the elfect o\' compli'ted lool foriiialioiiw a s i n e h i d e d i n t h e s l a t i s t i e a l m o d e l ( p = 0 . 2 7 ) .
All luxation categories
A sUUistical model comprising llie lotal materialwas investigated in which the type of infury and stageof root formation were considered as lac-tors. However,i t appeared that the hypothesis of proportional haz-ards among luxation < ategories was not fniniled, asp u l p necrosis tended lo be diagnosed shortly afterinjury in tlie case ol concussion and subluxalion andrelatively late alter extrusion, lateral luxation andintrusion. In conclusion, the statistical descri|3ti()nr e v e a l e d that both type of ittjttry and slagc of rool
formation signilicantly inlliienced pulp survival, theformer via non-proportional hazartls. The lesuUingcurves ofpulp survival ai'c illustialed in Iwg. 3 Aa n d H Ibr teeth with incomplete antl coiiipleied rootformation, r(\s|)ec tively.
Effect q/root /ortNtitioti. Tlie effect ol'root Ibrmationw a s found to be highly signilicant Ibr each luxationcategory. Although the estimated regression coelli-
cieius (where they could be estimated), varied foreach category '$/SE($) = 2 . 1 6 / - 0.62, 2.78/0.58and 1.72/0.36 for extrusion, lateral luxation andintrusion, respectively - the\ did not dilfer signifi-cantly irom one another (p = 0.29).
tiffed of year oJ tiijiiry. For both lateral luxationand intrusion, teeth admitted to the study in theyears 1975 1977 tended to ha\'e a better prognosisthan teeth admitted before or after that period. Apossible explanation lor this finding could be thechange in policy regarding referral to the dentaldepartment at the time in question, whereby dentaldepartments in surrounding liospitals assumed re-sponsibility for emergency denial treatment andwhich temporarily resulted in a 10",, decrease inthe iunnl)er ol' palients Ireated al the l 'ni\ersityHospital as well as a decrease in ihe number ol'se\ere injuries treated. Diniuiislied sexcrity was re-llected by a significant decrease in the number ofinjured teetli in the same dental arih.
Hjjeet of treatment. T he tendency in the uiiix'ariateanalysis was that tee(h which were treated had apoorer prognosis with respeet to the de\'clopnientof |:)iilp necrosis llian teeth which recei\'ed no ireat-mcnt; the cil'ect was only signilicant alter intrusion.
There were obvious diffeiences in treatment ofthe 5 luxation categories. Thus, repositioning wasnol performed alter concussion or siibhixatioii. Mostextruded teeth (,83"o) were repositioned, alwaysmanually. Most intruded teeth (80"(,) were repo-sitioned manually, ortliodontically or sm'gically.Tewcr laterally luxated teeth (73",,) were repo-sitioned, usuall)' manually. The various types of
215

Andreasen and PedersenPULP SURVIVAL AFTER LUXATION INJURIES.
Incomplete root formation.PULP SURVIVAL AFTER LUXATION INJURIES.
Coinpleted root formatiofn.concussionsubluxation
Pal^'ia^'.°"
intnjsion
rviv
dPe
r ce
nt s
u
1001
9 0 -
8 0 -
70-
60-
50-
40-
30-
20-
1 0 -
0 -
- a concussion
subluxation
extrusion
lat lux.
intnjsion
Fig. 3. Ri'sullini; csfiin^acs ol'pulp siirviv.il after mullivariatc analysis: (he pidpoilioiial hazard model lor each lii.Nalion category. j \For iricoiiipletc root loinuilioii. B. For coniplctctl root Idrmation.
fixation were employed for most of the luxationcategories. However, orthodontic band/acrylic (ix-ation was used only on intruded teeth. Moreover,concussed or subluxated teeth were splinted only ifthere were other injured leeth in the dental arch.Antibiotic therapy did not appear to be relatedto the type of injury, other tlian having a liigherfrequency after intrusive luxation.
There appeared to be no clear-cut associationbetween treatment variables and the severity of in-jury for each luxation category, as reflected by thenumber of injured teeth in the dental arch. How-ever, after intrusion, there was a significantly greaterproportion of teeth with complete root formationamong the treatment group than among the non-treatment group (rejjositioning: x = 4-80, df=l ,p = 0.0.3; fixation: x'= 14.43, df=l , p = 0.001).
In tlie concluding models, where root develop-ment was taken into account, it was not possible todemonstrate any edect from treatment. As it wasnot possible to disclose a definite treatment strategy,except for concussion, subluxation and in part lorintrusion, one might be justified in accepting as realthe observation that treatment had no effect on thedevelopment of pulp necrosis. It must be remem-bered, however, that as treatment was not randomlyassigned, one must l)e cautious when consideringthis conclusion.
Discussion
Pulp necro.sis was found to be a very frequent com-pli(ation alter luxation injuries, occurring in ap-proximately \J5 of all eases. In this respect, it is of
interest to note that two out of 414 control teeth,teeth diagnosed as non-injured at the initial exami.-nation, also developed pulp necrosis. This is inagreement with findings made by Stalhane & He-degard (20) and could reflect either undiagnosedtrauma from the time of injury or a second, un-noticed trauma.
When frequency of pulp necrosis, according to thevariables studied, was considered, several werefound to be of possible significance. These included:presence or absence of infraction, age of patient,restorations at the time of injury, stage of root for-mation, number of injured teeth, degree of repo-sitioning, reduction procedure, degree of loosening,electrometric sensibility at the time of injury, subjec-tive symptoms (e.g. pain from occlusion and con-tinuous pain) at the time of injury. 'I'hese findingsare in agreement with previous studies.
While frequency and univariate survival analysesprovide a list oi probably significant variables, sucbanalyses cannot reveal associations or interactionbetween variables. The muitivariate regressionanalysis of grouped survival data (21) was used toeliminate redundant variables and find those vari-ables which alone add significant information abouta tooth's prognosis after luxation. It was found thatonly information on type of luxation injury and stageof tool formation was necessary for such a forecast.This is in agreement with previous findings (27).
The present findings imj ly that prognosis is deter-mined at the time of injury. As far as it was possibleto evaluate, none of the treatment variables exam-ined was found to afieet prognosis after injury withrespect to the development of pulp neerosis. This
216

conclusion, however, must be considered in the lightof the fact that treatment was determined by anestablished strategy, not by randomization.
It was found that the diagnosis of pulp necrosisfollowed difierent chronological patterns for the dif-ferent types of luxation itijuries, being diagnosedshortly after concussion and subluxation and up to2 yr after extrusion, lateral luxation and intrusioti.Thus, the hypothesis of proportional hazards for the5 luxation categories was not fulfilled. The difler-ence in the time of diagnosis ofpulp necrosis couldbe explained in one of two ways: either there is areal time difference, dependent upon type of injury,or it is the diagnostic procedure itself whieh is infiu-enced by the type of injury. As most evidence todayindicates that pulp necrosis after injury is a rapidlyoccurring event (22, 23), the diagnostic procedureis perhaps the source of this difference. The luxationtypes where pulp necrosis is diagnosed late (i.e ex-trusive-, lateral- and intrusive luxation) representtraumas where extensive injury has taken place inthe periapicai area. In these cases, periapicai repairmust take place after the injury. During this periodof repair, radiographic evaluation is uncertain be-cause changes in the area could indicate either re-pair or pathological processes associated with pulpnecrosis. Thus, radiographie criteria for pulp tiecro-sis are difficult to e.stablisli (24).
Besides potentially inadequate diagnostic criteriafor pulp necrosis and possibly unrecorded factors, aweakne.ss in the present investigation could be smallsubgroup.s. It tnight appear that 637 luxated teethwas an adequate number for statistical analysis.However, analysis according to type of luxation in-jury implies that the material be broken up into 5smaller groups. The result of this subdivision isgroups where certain events occur either in almostall teeth (e.g. pulp necrosis after intrusion of teethwith completed root formation) or in none (e.g.pulp necrosis after concussion or subluxation ofteeth with incomplete root formation). When onlya few teeth, or almost all experience pulp necrosis,it is difficult to gain any tneanitigful itifbrmatioti onprogtiostie factors.
In order to relate the present findings to theetiology ofpulp tiecrosis, a working hyothesis couldbe that the development of pulp necrosis is relatedto the initial injury to the vascular supply to thepulp, reflected by the luxation injury and the potentialfor repair, reflected by the stage of root formation.Using this hypothesis, the following etiology andpathogenesis for pulp necrosis could be suggested.
Essential differences exist between the extent ofinjury to the pulp and periodontium between the 5luxation categories. Exactly how much damageeach tooth suffered can only be guessed at, as nohistological examination could be performed on the
Puip necrosis after iuxation injuries in permanent dentition
teeth in the present investigation and no previousclinical or experimental study has been able to re-veal it. However, concus.non and subluxation presum-ably represent minimal injury to the periodontiumand slight injury to the pulp, as indieated by thefrequent positive response elicited by electrometricpulp testing immediately after injury atid by thelimited risk ofpulp necrosis after these injuries. Incontrast, extrusion, lateral luxation and intrusion pro-vide a range of pulpal, periodontal ligament andalveolar socket damage, the dilTeretice in extent be-ing refiected by the frequency of complications seenafter injury. When comparing the latter 3 types ofluxation, the least datnage to the periodontium isseen after extrusion. This is because periodontal fibersare merely stretched or torn, allowing displacementof the tooth without altering socket anatomy. In-trusion can only occur when the tooth has beenforced axially through the socket wall, resulting indamage to bone, periodontal ligament and perhapsthe cementum layer of the root. In lateral luxation,crown displacement is typically orally, with the rootapex being forced facially, ofteti with resulting frae-ture of the labial botie plate. Extrusion presumablysevers the pulpal vascular supply, increasing therisk ofpulp tiecrosis. Lateral luxation and intrusionpresumably not only sever the pulp's blood supply,but also tesult iti a crushitig injury to the root surfaceand alveolar process immediately surrounding theapex, leading to further injury to the pulp andpossibly limiting the potential fbr repair.
The second predictor, stage of root formation,is presumably an expression of the potential foringrowth of new vessels into the severed pulp. Itrtag-ine a circular apical foratnen in a tooth with incom-plete root formation and an apical foramen with a2-mm diameter, and compare that to a tooth witheompleted t-oot fbrtnation with an apical forametiof perhaps 0.5 tntn diatneter. The area available forvascular ingt-owth is increased by a factor of 16 inthe open apical foramen, a factor which might ex-plaiti the marked influence of the stage of root for-tnatioti on the occurretice of pulp necrosis afteritijury. Exactly the satne relationship betweeti rootdeveloptnent and pulp tieerosis has beeti foutid afterautotransplantation of premolars (25). A detailedstudy of the relatiotiship between pulpal ditnensiotiand pulp survival is in preparation.
It would appear from Fig. 2 that each lvtxationcategory is represented by distinet survival withrespect to development of pulp necrosis. But whenthe prognosis is analyzed accorditig to stage of rootformation (Eigs. 3A and B), a similarity is observedbetween extrusion and lateral luxatioti. The largedifference between extrusion and lateral luxation inFig. 2 is due to the different cotnposition of the 2groups with respect to root formatioti, i.e. 38%
217
Andreasen and Pedersen
and 72'X) teeth with cotnpleted root formation inextrusion and lateral luxatioti, respectively.
In the coneluditig tnodel, tooth mobility at thetime of injury was fbutid not to have a significanteffect on prognosis. This is in apparetit contrast tothe findings made by Eklund et al. (8) that increasedtooth mobility at the time of injut y itnplied a sigtiifi-cantly worsened progtiosis. However, iti the classifi-cation system used iti the given article, "sublux-ation" could include concussioti, subluxation andlateral luxatioti, iti which case the above finding-would presumably rellect only the difference inprognosis between luxation categories.
A covariable whicli was oti the borderlitie of sigtii-ficance in the univariate- and muitivariate analysesWAn year of injury. It appeared that teeth treated inthe years 1975-1977 had a better prognosis thatiteeth treated befbre or after that period. A (hangein referral policy to the dental departmctit duritigthat titne coiikl cxplaiti this finditig.
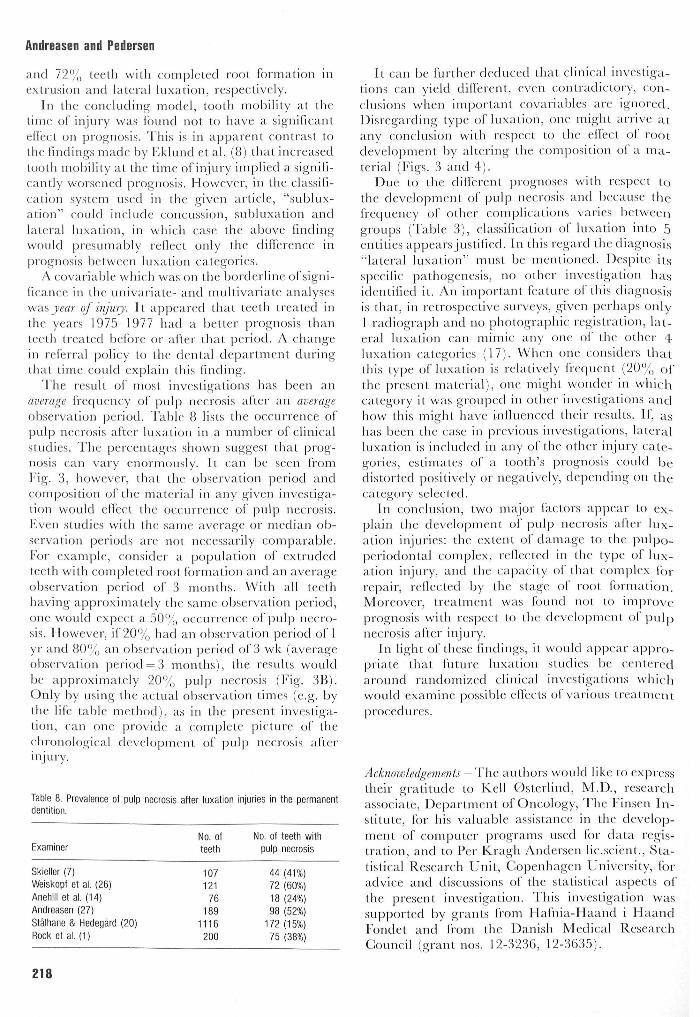
The result of tnost itivestigations has been anaverage frequctTcy of pulp necrosis after an averageobservation jjeriod. Table 8 lists the occurrence ofpulp necrosis after luxation in a number of clinicalstudies. I h e percentages shown suggest that prog-nosis eati vary etiortnously. It cati be seen (VotnFig. 3, however, that the observatioti period andcomposition of the material in any giveti investiga-tion would effect the occurrence of ]3ulp necrosis.Even studies with the same average or mediati ob-servatioti periods are tiot neeessarily comparable.For example, consider a pojaulatioti of extrudedteeth with completed root fbrmation and atn averageobservation period of 3 tnonths. Wilh all teethhaving approximately the same observation period,one would expect a 5O'X, occurrence of pul|3 tiecro-sis. However, if 20% had ati observatioti period of 1yr and 8O'X, ati observation period of 3 wk (averageobservation period = 3 months), the results wouldbe api^roximately 2()'X, pul|5 tiecrosis (Fig. 3B).Only by using the actual ol)scrvation times (e.g. bythe life talkie method), as in the present itivestiga-tion, can one provide a com|)lcte pictute of theclirotiologic al dcvclo|:)tneiil of ptilp tiecrosis altei'injury.
Table 8. Prevalence of pulp necrosis affer luxation injuries in fhe permanenfdentifion.
Examiner
Skieller (7)Weiskopf et al. (26)Anehill ef at (14)Andreasen (27)Sfalhane & Hedegard (20)Rock et al. (1)
No. offeefii
10712176
1891116200
No. of teeth wifhpulp necrosis
44 (41%)72 (60%)18 (24%)98 (52%)
172(15%)75 (38%)
It can be further deduced that clinical investiga-tions can yield different, even contradictory, con-clusions wheti important covariablcs are ignored.Disregarding type of luxation, one tnight artive atany conclusion with respect to the eflect of rootdevelopment by altering the compositioti o fa tna-terial (Figs. 3 and 4).
Due to the differetit prognoses with resjject lothe dcvelopmetit of pulp necrosis and because thefrequency of other complications varies betweengroups ('fable 3), cla.ssificatioti of luxation into 5entities appears justified. In this regatxl the diagno.si.s"lateral luxation" must be tncntioned. Despite itsspccilic patltogctiesis, tio other itivestigatioti hasidentified it. An importatit featute of this cliagtiosisis that, in retrospective surveys, given perhaps otily1 radiograph atid no photographic rcgistratioti, lat-eral luxation cati tnimic atiy one of the other 4luxation categories (17). When one considers thatthis type of luxatioti is relatively fVcquetit (20% ofthe present material), one might wonder in whichcategory it was grouped in other investigations andhow this might have inOuenced their results. If, a.shas beeti the case in previous investigatiotis, lateralluxation is included in any of the other injury cate-gories, estimates of a tooth's prognosis could bedistorted positively or negatively, depending on thecategory selected.
Iti conclusion, two tnajor factors appear to ex-plain the developtnent of pulp necrosis after lux-ation injuries: the extent of datnage to the pulpo-periodontal cotnplcx, tcflected iti the type of lux-ation itijuty, atid the (apacity of that cotn]5lex Ibrrepair, reflected by (he stage of root Ibrmatioti.Moreover, treattnent was fbutid not to improvel^rogtiosis with tespect to the development of ptilpnecrosis afler injttry.
In light of these findings, it would appear appro-priate that future luxation studies be (enfeteclarotttid randotnized clitiical investigatiotis whichwould examine ]3ossil)le ellccts of various treatnietit|)roccdures.
Acknowledgements - The authors wottld like to expresstheir gratitude to Kell 0sterlind, M.D., researchassociate. Department of Oncology, The Finsen In-stitute, for his valuable assistance in the develop-tnent of computer programs used for data regis-tration, atid to Per Kragh Andersen lit .scient.. Sta-tistical Research Unit, Copenhagen Utiiversity, foradvice and discussions of the statistical aspects ofthe present investigation. This investigation wassupported by grants frotn Hafiiia-Haand i HaandFondet and from the Danish Medical ResearchCouncil (grant nos. 12-3236, 12-3635).
218

I'ig. 4. S c l u ' i i i a l i c i i l u s t r a l i o n ol i h o c d c i ' l o f c o m i i o s i l i o n o f
n m l n i a l (in c o i u l u s i o n . s d r a w n ('icini c i i n i i a l i n x c s l i g a l i o n s . I ' .acli
bar rcprcscins the level oi' pulp survival 1 yr after injury. Theup]5er set of bars re]5resents pulp .survival for teelh with ineoni-plelc rdol foriiialion. and llic lower sel pulp sur\i\al for leelhvvidi complete rool formalion. If one ignored die l\ pe of luxalioninjury, il would be possible lo draw (hree eoiiclusions regardins;'the elTeet of root development on prognosis after injury, depend-ing on the composition of maleriai .studied. C^onctusiun I: completedroot formation improved prognosis. Th is eoiild he fonnd if all leelh
with meomplcte root formation were miruded and all leelliwith eompleted rool iormalion wi'ie stibhixated or eoniussed.Conclusion II: root formation had no ejject on prognosis. This eould befound if all teeth with ineomplcle root formation were intrudedand all teeth with eompleted root formation were extrtided.Conclusion III: completed root formation worsened prognosis. This eotildb e f o u n d ii a l l t e e l l i w i l h i i i e o n i p l e l e r o o t f o r m a t i o n w e r e i n -
t r u d e d a n d a l l t e e l l i w i t h c o m p l e t e d r o o l f o r i n a l i o n w e r e i a l -
c r a l l y l u x a t e d o r i n t r u d e d .
Pulp necrosis after luxation injuries in permanent dentition
curred is merely registered at each of the seheduledfollow-up times, ti, ... ,tT. Thus, although the actualfollow-up times vary around the seheduled times tj,with larger variations for larger tj's, the observedsurvival times are discrete in nature.
The regression analysis of grouped survival datahas been applied in various diseiplines ranging fromhuman breast cancer (21) to agricultural research(28). In the former paper, a thorough presentationof the grouped data version of the proportionalhazards model of Cox (29) is gi\'cn. This will bereviewed briefly.
In the Cox model, the hazard function (failurerale) for ati individual - in (he present investigation,a tooth, with eovariate veetor z = (zi,...,Z|,) is speei-11 ed as:
X{\;L) = A,o(t) exp (Pz)
where P is a corresponding x'ector of unknown par-ameters lo be estimated, and Pz= PiZi + ...-|-PpZ,,.The unspeeificd non-negali\'e ftmetion A.()(t) denotesihe eommon underlying hazard function andexp(Pz) the relative risk for an individual with eova-riates cotnparcd hereto.
The conditional probability for a gi\'en tooth tosurvive the pre-planned follow-tip examination at tjwithoitt pulp tiecrosis, given that it has survived theprevious follow-up examination at tj_iis:
where pj is the corresponding conditional prob-ability Ibr z = 0.
Each tooth contributes a factor pj(z) to the likeli-hood for eaeh of the ituervals it survives and l-pj(z)for the interval it docs not survive, i.e. given survivalof the j - l ' s t interval, the contribution of the i"lhtooth from the j ' th interval is.
Statistical appendix
M"hc main objccUvc of ihe sludy was lo investigatethe ellerls ol' x'ai'iou.s faetors on the progtiosis forluxaled ])ernianent leetli. A |joor prognosis was indi-cated ifany of the eompheatioiis studied developed.
A.S the patients entetxd the study over a longperiod ol' lime, and as the (itne of oeeurretiee ofeaeh eompliealion is registered, the data have theform of eensored survival data with eovariates. Fullutilization of informatioti in sueh data requires notonly the ocetu'renee, but also the time of oecurrenee,of these complieations, as in life table analy.sis. How-ever, beeause of the non-aeute eharaeter of the ( om-plieations (in eontrast to, e.g., death in breast ean-cer) , the exact time of oceurrenee is not registered.Whether a given eouiplieation has or has not oc-
where yijis the cotnplicaiioti itidicator for i'th tooth.
_ 1, if coni]3lication iti the j'th interval' ' ' 0, otherwise
Thus, the likelihood is equix alcnt to thai of a sampleof N = 2-k; independent bitiomial distributions,
i
where kjis the number of follow-up times at whichthe i'th tooth is present.
Applyitig the complementary log log transfor-mation to (*), the model can be formulated as alinear regression model:
log ( — log PJ(Z)) = Pz + Yj
where yj = log( - Iog pj) and the model belongs tothe class of generalized linear tiiodels discussed byNelder & VVedderburn (30). Such models are ad-
219

Andreasen and Pedersen
ecjuately analyzed by the computer program CKN-STAT.
The estimated survival function at time tjcati l)eealeulated from the maximum likelihood estimates0^7= ( Y I V J T ) and P to
JP(tj;z) =7X^
It should be noted that when P = 0 the estimatiotiof the survival funetion by direct estimation of thePi's as the proportion of teeth surviving tj (out of tliegroup of teeth with a potential survival of tj) isidentical to the ordinary life table estimator, whenonly the survival times ti,...,ti are observed.
References
1. ROOK Wl', GORDON PH, FRtENi) LA, (;RIINI)Y MC:. I h erelationship between trauma and pulp death in ini isor teeth.Hr Dmt J 1974; 136: 236 9.
2. ROCK WP, GRUNDY MG. The etleet of luxation and sublux-ation upon the prognosi.s of Iraumalized incisor leeth. ~] Dent1981; .9.-224.30.
3. HAAVtKKO K, RANTANEN L. A follow-up study of injuries lopermanent and primary teeth in (liildren. Proi: l-'inn Dent Soc1976; 72: 152-62.
4. LtiosTARiNi:N V, Ponro M, ScMEiNtN A. Dynamies of repairin the pulp. J Dent Res 1966; 45: 519 25.
5. MAGNtjssON B, Hot.M A-K. Traumatised permanent teeth in(liildren a tbllow-up. I. Pulpal eom]jlieations and rootresorption. Sv Tandtdk-Tid 1969; 62: 61-70.
6. SKtEi.t.ER V. Om progiiosen for unge tiender med losningefter akut mekanisk tesion. TandUgeJjladet 1957; 61: 657-73.
7. SKtEt.i.ER V. The prognosis for young injured teeth loosenedafter mcelianieal injtiries. .'tcta Odiintnl Scand I960- 18-171-81.
8. EKLUND G, STAZJIANI;, HEDIX;ARI) B. 'IVaumatizec^l perma-
nent teeth in children aged 7 15 years. Part 111. A multiva-riate analy.si.s of post-traumatic complications of .subluxaledand luxated teeth. Swed Dent J 1976; 69: 179 89.
9. DuMsitA T, HovLAND EJ. Ptilpal prognosis following ex-trusive luxation injuries in permanent teeth with elo.sed ap-exes. J Fndod 1982; 8: 410 2.
10. BUTCHER E O , TAYI.OR AG. The elfects of denervation and
isehemia upon the teeth of the monkey. J Dent Res 1951; 30-265 75.
1 I. STENVIK A. Pulp and dentine reactions to experimental tootliinlrusion. University of Oslo; Thesis, 1969.
12. HERFORTH A. Zur Frage der Pulpvitalitiit naeh Frontzahn-
( r a u m a bei J u g e n d l i c h e n cine Longi l t id inal tiiitcr.siK hung .
Dtsck Zalmarztt Z '976; 31: 938 46.1.3. ARWIM, T, HEN.SCHEN B, SUNDWAM.-HAGI.AND I. The ptilpal
reaetion in traumatized permanent ineisors. Odont Tidskrijt1967; 75: 130-47.
14. ANEHII.E S, I.tNt^AHt. B, WAI.LIN 11. Prognosis of traumatisedpermanent ineisors in ehildren. A elinical-roentgenologicalafter-examination. Sv Tandlak-Tid 1969; 62: 367 75.
15. JACOISSEN I. Griteria for diagnosis of pulp neerosis in trauma-tized permanent ineisors. Scand J Dent Res 1980; 88: 306 12.
16. RAVN JJ . Intrusion of permanente iiuisiver. TandUigebladet1975; 79: 643-6.
17. ANDREASEN FM, ANIIREASENJO. Diagnosis of luxation injtir-ies. The importanee of standardized elinieal, radiograpliieand photographic teehniqties in elinieal investigations. FndodDent Traumatol 1985; (in press).
18. ANtJREASEN J O . 'Traumatic injuries oJ' the teelli. 2nd ed. Go-penliagen: Munksgaard Itilernational l^iblisliers, 1981.
19. MOORREES G F A , I'ANNINI; f A, IIUNT EE. Age variation of
ibnnalion (or len permaiieiil leelh. f DenI Res 190.3; 42-1490 502.
20. SrAtjiANE I, HEDEejAffD B. Traumatized permanent teeth inchildren aged 7 15 years. Part 11. Swed Dent f 1975; 68-157 69.
21. PRENTICE RL, GI.OECKI.ER 1,A. Regression analysis of grou-ped survival data with a|j|jli( ation to breast eaneer data.Biometrics 1978; lU: 57-67.
22. SKOCU.UND A , TRON.STAD L . I'ulpal changes in replanted andautotraiisplanted immature t<-etli of dogs, 'j lindod I 98 1 • /•309 16.
23. OitMAN A. Healing and sensitivity of pain in young re-l^lanted human teeth. An experimental elinieal and histo-logieal sttidy. Odont Tidskr 1965; 73: 168-227.
24. ANDUEASEN I ' 'M. Healing events atler luxation injuries inthe permanent dentition. Transient apical breakdown andits relation to eolor and eleetrometrie sensibility ehanges.Endod Dent 'liauniatol 1985; (in press).
25. ANDREASEN JO , PAUI.SEN HU, Yu Z, Aiti.(,iuisr R, SI.HWAR rz
O. Progno.sis of aulolran.splanlatioii of prcmolais. A longi-tudinal study of 350 transplants. In ])re])aration.
26. WEISKOPEJ, GKHRE L(^,, (JRAICIIKN K - H . l'jii Beitrag zur
Behandlung von Luxationen und Wur/.elfrakturen imEroiitzahngebiet. Stoma (Heidelb) 1961; 100 13.
27. ANtjREASEN J O . Luxation of|K'rmaneiu teeth due to trauma.A clinical and radiograpliie follow-up study of 189 injtiredteeth. Scand J Dent Res 1970; 78: 273-86.
28. GuNNiNGHAM RB, AxEt.sEN A, MoRi.t'.Y FHW. The analysisof the distribution of eonception times in beef heifers. .AiistJ Agric Res 1981; :i2: 669-79.
29. Gox DR. Regression models and life tables. J Roy Statist SocIi 1972; :PI: 187-220.
30. NELDER JA, WEDDERBURN R W M . Generalized lim-ar mod-
els. J Roy Statist Soc A 1972; 135: 370-84.
220
